213
1

1

2
CONTENTS
Acronym Table 5
Message from the Chair and Chief Executive 8
Executive Summary 9
Part 1
Delivery of Our 2015/16 Plan
1.1 The New Clinical Response Model……………………………………............. 1.2 Quality and Operational Performance Trajectories…………………………... 1.3 2015/16 Strategic Change Portfolio …………………………………………… 1.4 Maturing Commissioning Arrangements and Increased Focus on Financial
Strategy……………………………………………………………………………
13
13 15 18
22
Part 2
Organisational and Strategic Context This section, coupled with Part 1, serves as a high level diagnostic of the context within which we operate – it answers the “where are we now?” question.
2.1 Profile of the Trust……………………………………………………………….. 2.2 Our Demand & Activity………………………………………………………….. 2.3 The Five-Step Ambulance Care Pathway, Commissioning Quality &
Delivery Framework, Understanding our Populations and Changes………. 2.4 National Policy Context………………………………………………………….. 2.5 Major Conditions, Older People and Frailty…………………………………… 2.6 Becoming a Listening and Learning Organisation………………………….... 2.7 NHS Wales Strategic Change Agenda………………………………………… 2.8 Service Change with Blue Light Partners……………………………………... 2.9 Ensuring Integration with Our Partners’ Three Year Plans………………….. 2.10 The Organisation and Prudent Healthcare……………………………………. 2.11 Treating People Fairly – Equality, Diversity & Human Rights………………. 2.12 Other Strategic Workforce and OD Drivers……………………………………
24
24 32
33 37 42 43 44 48 49 50 51 54
Part 3
Creating Our Strategic Framework This section sets the strategic framework for the organisation. It sets out our ambition and answers the “where do we want to go?” question.
3.1 Our Vision, Purpose and Behaviours………………………………………….. 3.2 Our Strategic Aims………………………………………………………………. 3.3 Our Priorities……………………………………………………………………… 3.4 Our Strategy Map………………………………………………………………… 3.5 Our Performance Ambitions………………………………………………......... 3.6 Developing a Frontline-Led Approach to Planning…………………………… 3.7 Becoming a Leading Ambulance Organisation: Where Do We Want to be
in 5 – 10 years? ...........................................................................................
57
57 58 59 63 65 78
84
Part 4
Quality and Prudent Healthcare – the Main Driver of Our Business This section sets out our ambition to put quality at the heart of our plans. It sets out the practical steps we are taking to move towards our vision, any milestones and intended impact of our actions - it answers the “what are we doing and how do we get there?” question.
86

3
4.1 Moving Forward 2016/19………………………………………………………... 4.2 Quality Themes and Improvements for 2016/17 and Beyond………………. 4.3 Quality Improvement, Measures and Assurance System………………....... 4.4 Quality Improvement and 1000 Lives Improvement…………………………. 4.5 Quality Governance………………………………………………………………
87 88 89 90 91
Part 5
Our Strategic Change Programmes – Our Service Focused Priorities This section gives an overview of our service change priorities, the practical steps we are taking to move towards our vision, any milestones and intended impact of our actions - it answers the “what are we doing and how will we make it happen?” question.
Emergency Medical Services: The Five-Step New Clinical Response Model………………………………………………………………………………
Non-Emergency Patient Transport……………………………………………..
94
95
108
Part 6
Our Enablers – the Building Blocks to Our Success This section gives an overview of the critical deliverables across our enabling functions and sets out how they will develop and strengthen to support service transformation- it answers the “what do we need in place to get there?” question.
6.1 Our People………………………………………………………………………... 6.2 Our Finances (Revenue and Capital)………………………………………….. 6.3 Our Estate………………………………………………………………………… 6.4 Our Fleet…………………………………………………………………............. 6.5 Research & Innovation…………………………………………………............. 6.6 Service Improvement……………………………………………………………. 6.7 Health Informatics and Business Intelligence……………………………........ 6.8 Information Communication and Technology……………………………........ 6.9 Partnerships and Engagement…………………………………………………. 6.10 Corporate Governance and Risk Management……………………………….
111
111 147 163 166 168 169 170 173 175 179
Part 7
Delivering the Plan This section sets out the delivery framework for our IMTP - it answers the “how do we know what we are delivering?” question.
7.1 Approach to Planning……………………………………………………………. 7.2 Plan Delivery……………………………………………………………………… 7.3 Risks and Issues to plan delivery………………………………………………. 7.4 Engagement and approval arrangements…………………………………….. 7.5 Internal Planning model and cycle……………………………………………...
182
182 182 187 190 190
APPENDICIES Appendix 1: Emerging Performance Issues Arising from the First Publication of the
Ambulance Quality Indicators……………………………………………………….
Appendix 2: CAREMORE® Service Change Ideas Currently Agreed with the
Emergency Ambulance Services Committee…………………………………......
192
193
195

4
Appendix 3: NHS Wales Strategic Change Agenda Milestones……………………………….
Appendix 4: Mid Wales Healthcare Collaborative (MWHC) – Key Actions…………………...
Appendix 5: Summary of Health Board and Trust IMTPs’ Integration with WAST………...
Appendix 6: Supporting Information Relating to Documented Actions…………………….....
Appendix 7: WAST 2016/17 Discretionary Capital Plan……………………………………......
Appendix 8: Strategic Change Programme Structures…………………………………………
197
198
204
207
208
211

5
Acronym Description
A&E Accident and Emergency Department
ABMU Abertawe Bro Morgannwg University Health Board
ACPs Alternative Care Pathways
AED Automated External Defibrillator
AEMTs Advanced Emergency Medical Technicians
AFSRC Ambulance and Fire Services Resource Centre
ALS Advanced Life Support
ABHB Aneurin Bevan University Health Board
AP Advanced Practitioner
APP Advanced Paramedic Practitioner
AQIs Ambulance Quality Indicators
ARC Ambulance Resource Centre
ARCH A Regional Collaboration for Health
AS Ambulance Station
AWW Ageing Well in Wales
BAF Board Assurance Framework
BCUHB Betsi Cadwaladr University Health Board
BME Black and Minority Ethnic
BJCs Business Justification Cases
CAD Computer Aided Dispatch System
CVUHB Cardiff and Vale University Health Board
CAS Clinical Assessment System
CASC Chief Ambulance Services Commissioner
CCA Civil Contingencies Act
CCC Clinical Contact Centre
CCG Clinical Commissioning Group
CCIS Community Care Information System
CE Chief Executive
CFR Community First Responder
CPADs Community Public Access Defibs
CPAG Clinical Pathways Advisory Group
CPAS Clinical Prioritisation Advisory Software Group
CPD Continuing Professional Development
CPR Cardiopulmonary Resuscitation
CQDF Commissioning & Quality Delivery Framework
CR Core Requirements
CRM New Clinical Response Model
CSD Clinical Support Desk
CSPT Call Streaming and Prioritisation Software
CTA Clinical Telephone Assessment (Hear & Treat)
CTL Clinical Team Leader
CW Central and West
CTUHB Cwm Taf University Health Board
DAV Dedicated Ambulance Vehicle
EAs Emergency Ambulances
EASC Emergency Ambulance Services Committee
EBR Established Based Responders
ED Emergency Department
EDCIMS Emergency Department Clinical Information Management System

6
EFL External Financing Limit
EMS Emergency Medical Services
EMT Executive Management Team
EMTs Emergency Medical Technicians
ENT Ear, Nose and Throat
EoL End of Life
EoLC End of Life Care
EPRR Emergency Preparedness, Resilience and Response
ESMCP Emergency Services Mobile Communication Programme
ESN Emergency Services Network
ESR Electronic Staff Record System
FC Frequent Callers
FRA Fire and Rescue Authorities
FRC Trust Board Finance and Resource Committee
GA General Anaesthetic
GP General Practitioner
GPOOH GP Out of Hours
HALO Hospital Ambulance Liaison Officers
HART Hazardous Area Response Team
HB Health Board
HCP Health Care Professional
HCSW Health Care Support Worker
HEI Higher Education Institute
HI Health Informatics
HQ Head Quarters
HR Human Resources
HDUHB Hywel Dda University Health Board
ICT Information Communications & Technology
IG Information Governance
IMTP Integrated Medium Term Plan
IPC Infection, Prevention & Control
IPR Integrated Performance Report
JET Joint Executive Team
KD Key Deliverable
KPI Key Performance Indicator
KSF Knowledge and Skills Framework
LDP Local Delivery Plan
LHB Local Health Board
LRF Local Resilience Forum
MBTI Myers Briggs Type Inventory
MFR Medical First Responders
MIU Minor Injury Unit
MPDS Medical Priority Dispatch System
MRD Make Ready Depot
MWFRS Mid Wales Fire and Rescue Service
MWHC Mid Wales Health Collaborative
NATC National Ambulance Training College
NEPTS Non-Emergency Patient Transport Services
NEPTSQIs Non-Emergency Patient Transport Services Quality Indicators
NHSDW NHS Direct Wales
NICU Neonatal Intensive Care Unit

7
NWFRS North Wales Fire and Rescue Service
NWSSP NHS Wales Shared Services Partnership
OD Organisational Development
OOH Out of Hours
PA Physicians’ Associates
PADR Personal Appraisal and Development Review
PCR Patient Care Records
PCRM Patient Centred Clinical Response Model
PCS Patient Care Services
PCT Primary Care Trust
PERU Pre-hospital Emergency Research Unit
PHEM Pre-hospital Emergency Medicine
PHW Public Health Wales
PIH Partners in Healthcare
POW Princess of Wales Hospital
PTHB Powys Teaching Health Board
PPF Paramedic Pathfinder
PPM Planned Preventative Maintenance
PTR Putting Things Right
QAIP Quality Assurance and Improvement Panel
QuESt Quality, Experience and Safety Committee
R&I Research & Innovation
RAPID Rapid Analgesia for Pre-hospital Hip Disruption
RLSS Royal Life Saving Society RNLI Royal National Lifeboat Institution
ROSC Return of Spontaneous Circulation
RRV Rapid Response Vehicle
SCCC Specialist and Critical Care Centre
SI Service Improvement
SLA Service Level Agreement
SMT Senior Management Team
SOC Strategic Outline Case
SOP Strategic Outline Programme
SORT Special Operations response Team
TASC The Alliance of Suicide Prevention Charities
TIA Transient Ischaemic Attack
TK Thomas-Kilmann Conflict Mode Tool
TRiM Psychological assessment of risk programme
TU Trade Union
UCS Urgent Care Services
UHP Unit Hour Production
UHW University Hospital of Wales
VPH Vantage Point House
WAST Welsh Ambulance Service NHS Trust
WEDS Welsh Education Development Services
WFIS Workforce Information System
WG Welsh Government
WHC Welsh Health Circular
WOD Workforce and Organisational Development
WTE Whole Time Equivalent

8
MESSAGE FROM THE CHAIR AND CHIEF EXECUTIVE
Welcome to our three-year Integrated Medium Term Plan (IMTP), which sets out our ambition for
the Welsh Ambulance Services NHS Trust (WAST) over the period 2016/17-2018/19.
The IMTP is the culmination of many months of engagement and planning underpinned by listening
to our staff, our patients and our stakeholders to develop our IMTP. We hope our IMTP clearly
articulates our purpose, vision, behaviours, strategic aims and priorities and helps everyone
understand the role the Ambulance Service plays within NHS Wales and the way we want to
develop over the coming years.
2015/16 was a significant year for the Trust, marked notably by the launch of a New Clinical
Response Model pilot that focuses on treating those in the most clinical need first and which helps
to establish the Welsh Ambulance Service very clearly as one which is clinically led and quality
driven.
This move towards a sound clinical basis for our services, be they Emergency Medical Services at
the forefront of the unscheduled care system; “Hear and Treat” services such as NHS Direct Wales
and our Clinical Desk supporting staff in our Clinical Contact Centres; or Non-Emergency Patient
Transport Services, which, from April 2016, will be delivered on a new, multi-agency basis, is
something that gives us a unique position as a bridge between the NHS in Wales and our blue-light,
emergency service partners.
The Welsh Ambulance Service is on a rapid improvement journey and the next three years will be
critical in ensuring that we are able to provide an ambulance service for people in Wales of which
they can be justly proud.
This means making bold decisions, reconfiguring our services to best meet the needs of
communities and reshaping our workforce to ensure our people can deliver what is needed to move
the Welsh Ambulance Service into the top tier of ambulance services, nationally and internationally.
Our services are all about people: those we serve and those who deliver care. We hope that this
IMTP describes how we all have a role to play in helping us deliver a dynamic and different
ambulance service that has a deserved reputation for consistently high standards of care,
compassion and performance.
We hope you find it an interesting and exciting document and that you will support us in whichever
way you can as we work hard to save and improve lives every day.
Share your thoughts with us on Twitter @welshambulance, find us on Facebook or email
Mick Giannasi Tracy Myhill
Chair Chief Executive

9
EXECUTIVE SUMMARY
Our Integrated Medium Term Plan (IMTP) covers a three-year period from 2016/17 to 2018/19. It
builds on our 2015/16 one-year plan and provides the framework for the organisation to:
provide a clear statement of ambition for the benefit of patients, the public of Wales, Trust
staff and NHS partners (together with other external stakeholders);
set out how it will deliver the Commissioning and Quality Delivery Framework (CQDF)
agreed with the Emergency Ambulance Services Committee (EASC);
outline the next phase of our clinical modernisation journey;
describe the modernisation of non-emergency patient transport services; and
describe the key enabling activities that will support front line staff to deliver good patient
care.
We in the Welsh Ambulance Service (WAST) have been through major change over the last 12
months.
2015 saw the introduction of the Commissioning and Quality Delivery Framework and we are now
working closely with both the Chief Ambulance Services Commissioner (CASC) and the Emergency
Ambulance Service Committee (EASC) to ensure this important framework agreement translates
into demonstrable service improvements for people in Wales who need and use our services.
The framework saw the introduction of a five-step Ambulance Care Pathway. This is a five-step
process for the delivery of emergency ambulance services within NHS Wales. The Ambulance
Care Pathway encourages us to focus on the patient journey i.e. patient flow, and a whole systems
approach.
Figure 1: Five-Step Ambulance Care Pathway
Transformational service changes have also taken place over the last year, including the New
Clinical Response Model (CRM) pilot that commenced in October 2015. The new model moves the
emergency element of our service from a time-based target system that has its origins in the 1970s,
when ambulance services were very different, towards an outcomes-based model.
Changes are also evident in the structure of the organisation. A permanent Chief Executive was
appointed in August 2015 and, following retirements and other departures, the Executive Team now
comprises a Director of Finance & ICT, a Medical Director, a new Director of Workforce & OD, a
new Director of Operations (interim), a new Director of Planning and Performance (interim), a new
Director of Quality, Safety & Patient Experience and a new Director of Partnership and
Engagement.
Our ambition is clear, and we have already made significant steps towards becoming a clinically-
focussed service rather than just a transport service. In so doing we are building a reputation as a
delivery-focused organisation that works through effective partnerships with staff, the public and

10
partner organisations. We want the public of Wales to have confidence in the Ambulance Service.
Whether patients are using non-emergency or emergency services, we want them to experience
excellent clinical care and customer service, over the telephone or face-to-face.
Such changes have meant the organisation has needed to review its purpose, vision, strategic aims
and priorities for the coming three years. These have been developed through widespread
engagement across the organisation, from the Board to frontline staff and will frame our plans going
forward.
By the end of year one of this plan we will have:
successfully transformed our Non-Emergency Patient Transport Services in line with the
Minister-approved business case;
implemented, with our partner organisations, the 111 Pathfinders in the Abertawe Bro
Morgannwg and Carmarthen areas;
made significant and quantifiable progress in transforming our Clinical Contact Centres,
including progressing the procurement of a new Computer Aided Dispatch system,
increasing the contribution of the clinical desk and implement learning from external and
benchmarking reports;
built on the progress made in 2015/16 and strengthened performance of our New Clinical
Response Model for emergency medical services (EMS), using the Five-Step Ambulance
Care Pathway, with a focus on reducing variation and moving focus from STEPS 4 and 5 to
STEPS 1- 3; and
completed a demand and capacity review and used it to develop strategic resource
plans (workforce and fleet) and, where possible, accelerated implementation.
These priorities translate into 4 key Change Programmes. Our transformation agenda is
underpinned by a robust programme management and delivery mechanism that offers the right
level of rigour and scrutiny to assure the Board and partners that change is being delivered
effectively.
Running through all of this are our refreshed shared behaviours. These too have been developed
over the last 12 months with widespread engagement and will provide a compass to guide cultural
change across the organisation. By making these changes, we will retain and attract the calibre of
staff we need to deliver high quality care to our patients.
Our strategy map that articulates this approach can be seen in section 3.4.
During years two and three of the plan, we will aim for a further acceleration in our journey of
transformation and will:
demonstrate a step change in demand, evidencing a reduction on current levels and
managing the demand which remains more effectively. This will require us to work with the
public and our partners across NHS Wales to influence and demonstrate this shift. We will
also help more callers with telephone advice and support more patients locally either by
referring them to a local health service or by providing all of the care they need at the scene;
re-shape, support and develop our workforce to reflect an increase in capacity across
STEPS 1, 2 and 3 of the New Clinical Response Model, and capability across STEPS 4 and
5, building on the analytical and engagement work we intend to undertake in year one;
implement changes required to our fleet based on our analytical and engagement work in
year one;

11
implement changes required to our estate based on our analytical and engagement work in
year one; and
agree and implement an optimum configuration for our Clinical Contact Centres in line with a
revised Estates Strategy (configuration agreed in year 1 with implementation taking place
across years 2, 3 and beyond). Clinical Contact Centres are important as they are the first
point of contact for all of our callers and patients.
This plan will explore the specific and tangible actions being taken within these areas and the
quantifiable impact we aspire to make, which you will see clearly articulated throughout this
document. For further information on all of our actions you can refer to Appendix 6. The majority of
our improvements will be made visible through our performance against the Ambulance Quality
Indicators.
Our Resources
As we move towards 2020, there are a number of risks and opportunities facing the Trust and the
health economy in general that have shaped the development of our People Strategy, and our
thinking and planning around the future shape of our workforce.
Our People Strategy enables us to align our resources and focus our actions over the next three
years towards delivery of our organisational vision, strategic priorities and New Clinical Response
Model. It builds on the positive progress made in 2015/16, particularly improvements to
establishment control, workforce planning, recruitment, PADR and sickness absence rates. It seeks
to address current and future risks and challenges, including improving the working lives of our staff,
and addressing variability in workforce performance.
Delivery of the strategy will be effected through four key workforce and OD enabling plans including a workforce plan, recruitment plan, training and education plan and a ‘Be our Best’ OD plan. More detail of the people strategy model and enabling plans can be found at section 6.1.
We recognise that the New Clinical Response Model will require the development and re-profiling of our current workforce to take account of the drive to increase capacity to “Hear and Treat”, and strengthen our capability through the development of the higher level of skills needed to ‘see and treat’ patients who are increasingly frail with complex and chronic conditions.
We expect to see an increase in the numbers of specialist paramedics with the skills to better manage patients with long-term chronic conditions at home and in the community, and confidently access alternative pathways to care as appropriate. We will explore and test the impact of creating new roles such as community-based paramedics supporting GP practices and patients within rural areas of Wales, and take steps to maximise the use of our volunteer workforce, including growing our Community First Responder (CFR) workforce and Co-Responder capacity. Our plans also take account of several significant change/transformation programmes, including preparation for the introduction and roll-out of the 111 Pathfinder project and implementation of our Non-Emergency Patient Transport Business Case.
We describe this journey in more detail in our workforce plan at section 6.1. This links clearly to our training and education plan at section 6.1 in which we aim to ensure our people are sufficiently trained and skilled to work to the full scope of their practice, and trained to better clinically manage increasing frailty, mental ill health and complexity within the population.
Clarity on the exact number of each grade and type of staff needed in the future will be achieved
with the support of expert analysts, working with us to undertake a full review of capacity and
demand in the first quarter of 2016. In the meantime, we will continue to focus our actions on
ensuring timely recruitment, effective rostering and training of all staff to ensure momentum is not
lost and our performance and delivery is not adversely affected.

12
Underpinning this IMTP is a three-year balanced financial plan. To achieve this, the Trust will further
improve and deliver on operational efficiencies, meet challenging and ambitious savings plans and
further identify opportunities over the planning period to reduce cost. This balanced financial plan is
not risk free and is presented on the basis of the key financial planning, resource envelope and
funding assumptions fully described in the finance section of this document.
Clearly, years 2 and 3 (2017/18 and 2018/19) of this plan will need further refinement once key
financial variables are known, including the detailed cost pressures for these financial years, impact
of savings delivery between now and then and the opportunities for further efficiencies, but also the
outcomes of key pieces of work being described throughout this document, including the demand
and capacity review and the outcome of the evaluation of the New Clinical Response Model pilot. In
addition, of significance will be the impact of other developments being progressed, including the
expected roll- out of 111, investment in “Hear and Treat” services and expected efficiencies to be
garnered from the new CAD and other technology developments. The impact all these have on both
the staffing and fleet resource requirements of the Trust going forward will see the financial plan
further refined.
In terms of 2016/17, the balanced financial plan is underpinned by some key planning and resource
assumptions, all of which have been shared with the CASC and his team over recent months as this
plan has been developed, and all of which have received broad support. These include the resource
envelope assumptions, the key ones which are as follows:
the baseline level of funding via EASC in 2016/17 for EMS services (at 2015/16 prices) will
be consistent with that provided in 2015/16, PLUS a net small increase of c£0.8m, being the
elements of the additional planned spend incurred in 2015/16 that are currently expected to
continue into 2016/17 (£2m), netted off in part by elements of the core spend and funding in
2015/16 that is non-recurring (a net £1.2m);
what is considered to be a reasonable “fair share” of the additional £200m “general” growth
funding being made available in 2016/17 to the NHS in Wales by Welsh Government to
cover pay awards and other inflationary and other cost pressures – this is estimated at £5m
for WAST;
the resources in relation to NEPTS are consistent with that included within the recently
approved business case for the future delivery of this service;
other key specific service developments, in particular 111 and the support required for the
demand and capacity review, are fully funded;
the delivery of a challenging and ambitious savings plan for 2016/17 of £6.2m, the full details
of which are included within the finance section of this document;
resources have been modelled on the basis of current performance targets; and
where Local Health Boards make major service changes, the impact on our services
(emergency or non emergency) will be fully resourced via their business case mechanisms
and routed through the commissioning arrangements.
The finance section (part 6.2) also summarises the current capital programme over the next few
years, which has been developed in parallel with our service, estate and fleet plans.

13
PART 1: PROGRESS IN DELIVERING OUR 2015/16 PLAN This section provides an update on progress in implementing the Trust’s one-year plan, both in terms of achievements and challenges.
2015/16 was a pivotal year in the transformation of WAST as the new commissioning arrangements came into force and the new National Collaborative Commissioning and Quality Framework was implemented. For this reason, the Welsh Government recognised that an approvable three-year IMTP for the organisation was unrealistic for 2015/16. Consequently, the organisation was asked to focus on producing a one-year plan. A one-year plan was produced, approved by Trust Board, endorsed by the Chief Ambulance Services Commissioner (CASC), the Chair of the Emergency Ambulance Services Committee (EASC) and the lead NHS Wales Chief Executive. We continue to make solid and steady progress in delivering this one-year plan. Key headlines of our successes are:
The launch of a pilot of the New Clinical Response Model on 1 October 2015 (see below);
The full roll-out of digital pen technology (Digi-pens), EMS paramedics and ambulance crews in the organisation- the first ambulance service to use such technology;
Being awarded the ‘hosting’ rights for the 111 Pathfinder project in Abertawe Bro Morgannwg University Health Board;
NHS Wales agreement on a new service model for Non-Emergency Patient Transport Services (NEPTS), the implementation of which will form a major component of the organisation’s activities in year one of this plan;
At the time of writing, the Ambulance Resource Centre (ARC) Wrexham remained on schedule to open in March 2016; and
Improvements in delivery against the time-based targets. Whist challenges remain, we will continue to build on our achievements and celebrate successes.
1.1 The New Clinical Response Model In October 2015, WAST launched a one-year pilot of a New Clinical Response Model (CRM). The
previous CRM (introduced in December 2011) measured the effectiveness of the ambulance service
by time-based measures around how long an ambulance took to reach a call. It was well
recognised by the organisation itself, and from a number of previous reviews (most recently the
McClelland review), that time-based targets are not in themselves a meaningful measure of
performance of a clinical service and that, in some circumstances, they may even be detrimental to
clinical care, particularly because of the practice of sending multiple resources or the deployment of
a less appropriate resource to calls to “stop the clock”, with the intention of meeting a time-based
target rather than satisfying a clinical need.
The major changes in the 2015 CRM pilot were to:
categorise emergency calls based on the clinical need of the patient;
remove time-based targets for all calls except highest priority ‘RED’ calls;
measure clinical achievement using clinical indicator data (measuring the quality of the care
the patient received) rather than time-based data alone; and

14
introduce a new concept of ‘dispatch on code’ for emergency calls other than the highest
priority RED calls. Allowing the ambulance service to decide exactly what help is required
rather than just dispatching an ambulance to the address.
The ‘RED’ code set was examined in detail by a team of senior clinicians. All codes previously in
the 2011 CRM ‘RED-1’ (highest priority) code set remained in the new RED codes; in addition to
this, a number of other codes previously assigned lower priorities were re-categorised as red. This
was based on anticipated clinical need, focusing on those calls where an immediate threat to life
was likely to be present, and the nearest possible emergency response should be sent to maximise
the chance of survival. Learning from adverse incidents across the UK and the views of the other
UK ambulance services were also considered. Such codes include cardiac arrest patients, those not
breathing, unconscious or with other very serious conditions.
Other calls were then prioritised as AMBER or GREEN depending on clinical urgency. Performance
for these calls is measured exclusively using a suite of clinical indicators that have been developed
to measure compliance with key aspects of care, identified as those interventions that improve
outcomes.
Figure 2: Pilot Clinical Response Model
RED – BLUE LIGHTS
Immediately life-threatening
calls
Multiple dispatch Blue light emergency response
AMBER – BLUE LIGHTS
Life-threatening / Serious
calls
Blue light emergency response
GREEN 2 and 3– NORMAL
ROAD SPEED
All other calls
Face to face response Clinical telephone assessment
WAST uses the Medical Priority Dispatch System (MPDS) to prioritise 999 calls. All calls received
are accorded a code that shows the main clinical condition of the patient and the urgency of their
condition. For each individual MPDS code, the ‘ideal’ response has been identified based upon
clinical urgency, anticipated skill mix required at scene, conveyance rates and other historical data.
The new CRM trial suggests that, for AMBER and GREEN calls, no ambulance is dispatched until
the ‘full MPDS code’ is known (i.e. all clinical information has been obtained to allow a detailed
understanding of the presenting problem). This then allows the nearest ‘ideal’ response to be sent,
which should be able both to attend in a timely manner, and deal with the patient’s care
requirements, including conveyance to hospital where needed. For example, this will ensure that an
ambulance is sent to heart attack and stroke patients rather than a paramedic in a response car
who cannot get the patient to hospital.
The aim of this is to reduce multiple unit dispatch (where a rapid response vehicle is sent to ‘stop the clock’ followed by an emergency ambulance to convey to hospital, for example) in favour of dispatching one resource to provide everything the patient needs. The Trust is clear that the new model of care will deliver the following benefits:
the sickest patient will always be treated first;

15
the centrality of patient and public safety will maintained at all times;
patients will receive care which meets their clinical needs rather than wants;
delivery of the best clinical outcome for each and every patient on every occasion and
optimal patient experience; and
a reduction in overall clinical risk within the ambulance service model by offering a range of
treatment options, once the patient’s need has been identified.
EASC is currently undertaking an independent evaluation of the model which we are proactively
engaged with and which will be invaluable in testing the extent to which these benefits have been
realised.
1.2 Quality and Operational Performance Trajectories Operational Performance We recognise that it has been a mixed year for us in terms of operational performance; we have had some achievements and, equally, some areas where we know we need to do more to improve things. Below are just a few of the highlights to represent some of our challenges and successes.
RED Calls Improving the operational performance of the organisation was a priority in 2015/16. Figure 3 below shows that, for the final quarter of 2014/15 and the first quarter of 2015/16, there was a month-on -month improvement in performance rising from 43% of category A calls being responded to within eight minutes in December 2014 to 62% in July 2015, when performance peaked. July and August 2015 saw unfortunate slips in performance: summer months are traditionally challenging when Wales sees an influx of tourists and visitors to the country. A pilot testing the New Clinical Response Model commenced on 1 October that which included:
additional capacity – putting more ambulances on duty;
the introduction of robust performance reviews with Heads of Operations; and
working with Health Boards to reduce handover delays. Figure 3

16
Figure 4
The New Clinical Response Model pilot reduced the number of RED calls received per day from
around 500 under the 2011 model to around 70 per day.
This reduced number of RED calls means that we can focus dispatch processes on immediate
dispatch of multiple resources to RED calls. The challenge associated with this is that, in some rural
and smaller Health Board areas, the daily number of RED calls is small. Our performance
improvement against the 65% national target for RED call attendance in eight minutes is a result of
the focus applied to these most serious calls.
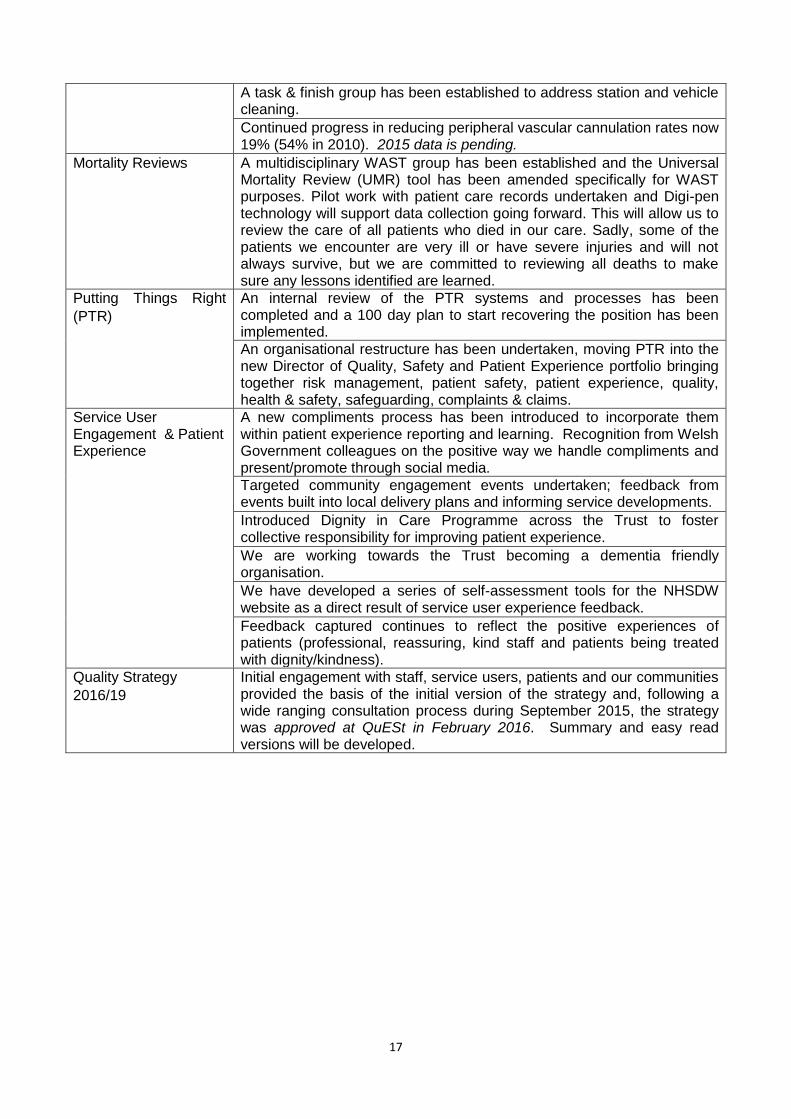
Quality In our 2015/16 plan we challenged ourselves to become a quality-focussed, clinically-led and clinically-driven ambulance service covering emergency medical services, non-urgent patient care services and our 24-hour health care and advice service. In pursuit of this ambition, our 2015/16 plan made a number of commitments regarding quality and much has been achieved over the last 12 months as can be seen in the table below. Figure 5: Quality Improvements 2015/16
Safeguarding Safeguarding changes as a result of the new legislation from the Social Services and Well Being Act 2014.
Education & development is on-going; training packages are being updated to reflect the new legislation and guidance. Educational programmes have been delivered using risk-based methodology and the training strategy is currently under review.
Plans are in place for practitioner educators to undertake a certified Home Office PREVENT Tutor course and a strategy to deliver the required level of training is being considered.
The safeguarding structure review is completed. A new named professional / Head of Safeguarding commenced in post November 2015 with additional supportive posts to be recruited in the 2016/17 financial year.
Infection, Prevention &
Control (IPC)
The IPC Code of Practice has been developed and approved with a supporting operational plan, linking into Health Board areas’ local delivery plans.
17
A task & finish group has been established to address station and vehicle cleaning.
Continued progress in reducing peripheral vascular cannulation rates now 19% (54% in 2010). 2015 data is pending.
Mortality Reviews A multidisciplinary WAST group has been established and the Universal Mortality Review (UMR) tool has been amended specifically for WAST purposes. Pilot work with patient care records undertaken and Digi-pen technology will support data collection going forward. This will allow us to review the care of all patients who died in our care. Sadly, some of the patients we encounter are very ill or have severe injuries and will not always survive, but we are committed to reviewing all deaths to make sure any lessons identified are learned.
Putting Things Right
(PTR)
An internal review of the PTR systems and processes has been completed and a 100 day plan to start recovering the position has been implemented.
An organisational restructure has been undertaken, moving PTR into the new Director of Quality, Safety and Patient Experience portfolio bringing together risk management, patient safety, patient experience, quality, health & safety, safeguarding, complaints & claims.
Service User Engagement & Patient Experience
A new compliments process has been introduced to incorporate them within patient experience reporting and learning. Recognition from Welsh Government colleagues on the positive way we handle compliments and present/promote through social media.
Targeted community engagement events undertaken; feedback from events built into local delivery plans and informing service developments.
Introduced Dignity in Care Programme across the Trust to foster collective responsibility for improving patient experience.
We are working towards the Trust becoming a dementia friendly organisation.
We have developed a series of self-assessment tools for the NHSDW website as a direct result of service user experience feedback.
Feedback captured continues to reflect the positive experiences of patients (professional, reassuring, kind staff and patients being treated with dignity/kindness).
Quality Strategy
2016/19
Initial engagement with staff, service users, patients and our communities provided the basis of the initial version of the strategy and, following a wide ranging consultation process during September 2015, the strategy was approved at QuESt in February 2016. Summary and easy read versions will be developed.

18
1.3 2015/16 Strategic Change Portfolio Our 2015/16 plan outlined a portfolio of strategic change which the organisation committed to deliver. The portfolio brought together five strategic change programmes. The following table outlines the status of each programme.
Non-
Emergency Patient
Transport Programme
(NEPTS)
What did the programmes set out to deliver?
Analysis of three prescribed NEPTS delivery models. Production of business case that identifies a recommended way forward for NEPTS in Wales. Share the findings with the Minister for Health and Social Care by September 2016.
What has been delivered?
Business Case produced that contains the preferred model of service delivery, this being WAST managing and co-ordinating all NEPTS in Wales using a mixed economy of providers. The main benefit is that this provides the new organisational arrangements with time (potentially five years rolling agreement) and investment required to truly modernise and improve the quality and performance of NEPTS in Wales.
A recommendation in terms of how NEPTS are to be commissioned in the future, this being through the Emergency Ambulance Services Committee (EASC). The main benefit of this development is a reduction from nine commissioning processes to one, significantly reducing organisational time, allowing this capacity to focus on and deliver the modernisation agenda. In addition, having a single Commissioner assists in the standardisation of NEPTS in Wales, whilst also ensuring any strategies are developed in such a way that they reflect local and national strategies.
A new Service Level Agreement (SLA) that contains generic service standards and requirements for Wales has been produced and agreed, thus ensuring NEPTS provision is delivered equitably across Wales.
Approval from the Minister of Health and Social Care to proceed and deliver with pace the recommendations contained within the business case.
What is outstanding?
Nothing- full delivery of programme against plan
What are the next steps / phases of work?
Delivery of the implementation plan – this is explored in Part 5

19
Clinical Modernisation
Programme
The Clinical Modernisation Programme Board (CMPB) was established with a primary objective in 15/16 to deliver the New
Clinical Response Model and ensure any changes were clinically-led and managed in a systematic way, starting with the
identification of core clinical activity which could be standardised across Wales with appropriate supporting performance and
clinical indicator information.
The Programme was divided in to five key development project areas using the Five-step New Clinical Response Model, plus an
identified Human Resource project to support these developments, each with underpinning workstreams.
Significant change has been achieved in a short time, the most significant being:
realisation of a New Clinical Response Model which was approved by the Health Minister on 29 July with implementation on 1 October 2015 for a one year pilot; and
the implementation of Digital pen technology across Wales in September 2015 - a first for ambulance services in the UK.
Both changes continue to embed in the organisation and work is ongoing to better understand performance and monitor the impact, including the impact on staff and the public; full benefits, therefore, are still to be realised.
Workforce and Organisational Development Improvement
(WODI) Programme
The People Programme set out to deliver an ambitious programme of workforce, organisational design and improvement activity, aligned to existing strategy, to support the Welsh Ambulance Service Trust to achieve its aspiration of becoming a high performing organisation and continuing its journey from ‘good’ to ‘great’. The programme set out to deliver the following outcomes:
rosters that are safe, sustainable and aligned to demand, and also ensure staff can utilise their full CPD hours to ensure they are appropriately skilled and able to deliver the highest quality patient care;
a 2% point reduction of the cumulative rate of sickness absence across the Trust by 31 March 2016 and consequent reduction in variable pay expenditure;
a streamlined recruitment process, reduced time to hire and plan that ensures all vacancies are filled in a safe and timely manner and staffing levels are safe and sustainable;
achievement of the Gold Corporate Health Standard; and WAST as the Employer of Choice and ‘a great place to work’.
Capacity to deliver this programme was assessed to be the greatest risk to delivery within the required timescales. Resource was over-stretched and reactive (as a consequence), and the WOD Directorate was struggling to deliver the agenda with any

20
pace and impact. As a result, additional HR and OD resource was secured part way through 2015 to support the delivery agenda.
The People Programme made significant progress over the year, and delivered the following headlines:
an operational workforce plan with agreed establishments and identified vacancies, and aligned recruitment and training plans;
successful recruitment to paramedic vacancies resulting in an estimate 6 – 10 vacancies remaining depending on turnover at the start of 2016/17; more paramedic resource available to be deployed as a result and a consequent reduction in demand for variable pay (overtime);
a significant reduction in the time taken to hire staff with an average reduction by 60 days when comparing recruitment timescales in December 2015 / January 2016 with 12 months earlier;
a refreshed annual sickness action plan which reflects learning and best practice from other organisations and ambulance services;
a sustained reduction in the cumulative rate of sickness absence from 8.17% (March 2015) to 6.87% (January 2016); a set of shared organisational behaviours, approved by the Board, and developed from listening to more than 800 staff,
that will assist colleagues to do the right thing in the right way; establishment of staff long service awards & recognition events; improved partnership working relationships with staff representatives, including manager and staff representative
development sessions #GoTogetherGoFar, lead representative development session, regular meetings with the Chief Executive and Director of Workforce & OD, and engagement in key strategic developments such as the People Programme, Clinical Modernisation Programme, NEPTS;
significant improvement in PADR rates from 10% to 60% during 2015/16; review of the Clinical Team Leader role and proposed development programme to support CTLs to be the best they can
be; an Executive Team development programme and development of Executive Team Charter; and a review of the Advanced Paramedic Practitioner role and proposed progression framework.
Following changes to the assessment criteria of the Corporate Health Standard (CHS), it was recommended that the Trust allow more time to develop and embed its well-being framework and activities before seeking to be assessed for the Gold CHS. As a result, we will now seek to achieve Gold status by the end of 2016.
Strategic Efficiency
Programme
The Strategic Efficiency Programme constituted a number of workstreams which collectively laid the foundations for work in future years in terms of realising efficiencies and supporting the organisation to become more efficient. Delivery of this programme included workstreams set out below.

21
Points of Presence: A baseline review of the organisation’s current estate (excluding ambulance stations). This work
identified a number of opportunities to progress and these are now woven into this plan.
Administration Review: A baseline review was successfully completed regarding the organisation’s administrative function. Proposals to carry out a full review of administrative and corporate functions will be developed through 2016/17 and will form part of our plans for year 2.
CCC re-configuration: During 15/16, this workstream was disaggregated from the strategic efficiency programme. This was done in light of the in-year decision regarding the 111 Pathfinder project WAST will now host and the added complexity this now adds to the CCC re-configuration agenda.
Community Engagement
This project set out to develop a Community Engagement Strategy and implementation plan that was citizen-centred, to enable the Trust to interact with all stakeholders and promote community ownership of the service. The project has delivered a full scale engagement scoping exercise that has mapped the levels of reported engagement activities across the Trust and the regions. A ‘living’ database showing levels of community engagement/activity is also ‘live’. The community engagement database has the potential to evolve further and its use broadened. The specification outlined for the database will provide evidence of engagement undertaken and for what purpose. With further development it would be able to highlight where engagement activities will need to be strengthened in order to make certain that engagement activities are representative of all. The system has the potential to be advocated as a pan Wales system to ensure that learning is shared across other health organisations. This will support the principles of prudent healthcare and co-production.

22
1.4 Maturing Commissioning Arrangements and Increased Focus on Financial Strategy
The National Collaborative Commissioning: Quality & Delivery Framework Agreement is a critical
driver of our services (more detail in Part 2). Much progress has been made throughout 2015/16 in
terms of strengthening the collaborative approach to commissioning. Some headline achievements
are outlined below.
Support for 14 Service Change initiatives through the CAREMORE approach.
Publication of the Ambulance Quality Indicators (data and supporting narrative) in January
2016.
From a financial perspective, 2015/16 has seen a significant increased focus on the development of
our financial strategy and financial planning and integrating this with strategic workforce planning
and focussing on the medium as well as short term. Working closely with the commissioning team,
this has also seen significant additional detail provided to the Emergency Ambulance Services
Committee (EASC) in order to clarify critical areas of spend, including those that linked to past
investment in the Trust.
Two specific amounts within the financial value for 2015/16 agreed at the outset of the
financial year, namely:
o £7.5m first provided in 2014/15 predominantly for workforce pressures and
recruitment, and the development of the clinical desk within the CCC; and
o £8m provided at the end of 2014/15 for service change developments to specifically
allow for improvements in operational performance and, in 2015/16, the move
towards the New Clinical Response Model.
The level of additional planned spend in 2015/16, agreed by both the Commissioners and
WG, in order to maintain and improve performance delivery, initially estimated to be c£4.4m,
this is now forecast to be £3.5m. This further stabilisation of the levels of additional spend
required by the Trust to continue its operational performance improvement, whilst delivering
within a resource envelope agreed much earlier in the financial year, is key to the confidence
the Trust now has, assuming the recovery of fair shares of additional monies being available
across NHS Wales, in being able to present, implement and deliver a balanced financial plan
and position over the medium term.
The delivery of significant levels of savings in 2015/16 to achieve financial balance, or even
a small surplus, by year end.
The level of additional detail routinely provided by the Trust to the CASC Team in relation to
detailed spend across the Five-Step Ambulance Care Pathway, and in accordance with the
National Collaborative Commissioning: Quality & Delivery Framework Agreement (CQDF).
Detailed information was provided to the EASC Joint Committee meetings in September 2015,
November 2015 and January 2016 and a summary paper, consolidating these pieces of work, was
provided to the office of the Chief Ambulance Services Commissioner in February 2016.
The maturing relationship between the Trust and the Commissioning Team has also seen an
agreed approach to the basis of the key financial planning assumptions which underpin the three-
year financial plan within this IMTP, including the shift of focus away from pockets of previous

23
investment to concentrate on the efficient use of the total resource, especially in relation to EMS,
and focus on the overall quantum of spend. The agreed approach has been to set out in detail for
the CASC the current expected levels of total spend (including inflationary and other cost
pressures) by the Trust, in order for the operational performance improvement trajectory to be
maintained and the performance ambitions detailed within this IMTP to be delivered, over the next
three years. This includes challenging, ambitious, but deliverable cost improvement, efficiencies and
savings targets, and partly driven by reasonable estimates of fair shares of expected additional NHS
Wales wide funding over this period; these detailed assumptions have been shared with, and
received support from, the CASC, on behalf of the EASC.
Further supplementary detail to support this projected level of EMS spend over the medium term,
based on the detailed financial planning assumptions within this plan, and the financial modelling
that underpins this, have also been provided to the CASC office, including:
a projected pay spend analysis between core and variable pay over the three years;
total forecast spend over the five-steps of the Ambulance Care Pathway; plus
further detail regarding the Trust’s Cost Improvement Programme / efficiency plan for the
coming three years.
24
PART 2: ORGANISATIONAL AND STRATEGIC CONTEXT This section outlines the context within which the Trust operates. It covers:
- the profile of the Trust, including our people;
- demand, activity and population changes;
- the National Collaborative Commissioning Quality & Delivery Framework;
- national policy context;
- major conditions, older people and frailty;
- learning from previous events;
- NHS Wales strategic change agenda;
- blue light partners;
- Prudent Healthcare;
- Treating People Fairly – equality and diversity; and
- Welsh language.
2.1 Profile of the Trust
We, the Welsh Ambulance Services NHS Trust (WAST), provide ambulance services for people in
Wales, delivering high quality and patient-led clinical care – emergency, urgent, scheduled –
wherever and whenever needed.
We are changing the focus of our service to establish ourselves as a clinically-led, quality-driven
emergency medical service, non-urgent patient care service and a 24-hour health care and advice
service that focuses on delivering the best clinical outcomes for patients. We want to (and should)
be seen as an integral part of the ‘frontline’ of the integrated healthcare system in Wales, with
emergency and urgent care services a fundamental part of the national unscheduled care system.
We also work closely with Public Health Wales in our public health messaging and in understanding
the changing health demographics that impact on the unscheduled care system.
Operations Directorate
The Operations Directorate is responsible for all of the ambulance resources provided by the Trust
including Emergency Medical Services (EMS), Urgent Care Services (UCS) and Community First
Responders (CFRs).
Through our EMS workforce, we provide a 999 service responding to emergency calls to the most
vulnerable people in Wales. Our paramedics and ambulance crews are trained to manage a wide
range of presenting complaints and to administer drugs in line with the UK national ambulance
clinical JRCALC Guidelines (Joint Royal Colleges Ambulance Liaison Committee).
Our UCS workforce provides a fundamental back up to our EMS function. Their main objective is to
support inter-hospital transfers and respond to a code set of low acuity presentations aligned to their
training. These are usually patients who have already been assessed by a doctor, nurse or a
paramedic as being suitable to be looked after by a UCS crew.
Both our EMS and UCS services are configured to align with our Health Board partners’ physical
boundaries. Each Health Board area has a clinical structure that consists of a cadre of Advanced
Practitioners (APs) educated to Master’s level, Clinical Team Leaders (CTLs), Paramedics,
Advanced Emergency Medical Technicians (AEMTs), Emergency Medical Technicians (EMTs) and

25
Urgent Care Services (UCS). There exists a Head of Operations (HoO) who oversees operations in
each Health Board area.
Figure 6: Map of our EMS Resource (Funded Establishment)
1. BCU Population – 694,038 Paramedics – 200.8 Clinical Team Leaders – 33 Advanced Practitioners – 5 EMT / AEMTs – 98/7 Urgent Care Staff - 48
2. Powys Population – 132,675 Paramedics – 55 Clinical Team Leaders – 11 Advanced Practitioners – 3 EMT / AEMTs – 42/6 Urgent Care Staff - 14
6. Cwm Taf Population – 295,953 Paramedics – 65 Clinical Team Leaders – 11 Advanced Practitioners – 2 EMT / AEMTs – 22/4 Urgent Care Staff - 26
7. Aneurin Bevan Population – 580,401 Paramedics – 118 Clinical Team Leaders – 19 Advanced Practitioners – 1 EMT / AEMTs – 63/4 Urgent Care Staff - 31
5. Cardiff & Vale Population – 481,979 Paramedics – 80.5 Clinical Team Leaders – 15 Advanced Practitioners – 4 EMT / AEMTs – 41.9/4 Urgent Care Staff – 18.9
4. ABMU Population – 523,001 Paramedics – 124.3 Clinical Team Leaders – 19 Advanced Practitioners – 4 EMT / AEMTs – 44/7 Urgent Care Staff – 33
3. Hywel Dda Population – 383,989 Paramedics – 138 Clinical Team Leaders – 21 Advanced Practitioners – 6 EMT / AEMTs – 52/7 Urgent Care Staff - 23

26
Our Community First Responders (CFRs) are also a highly valued part of the emergency response
team and provide a resource to us to support the provision of our EMS. CFRs also have an
important role in developing community resilience and public awareness. CFRs provide pre-hospital
emergency care within a defined set of protocols before the arrival of an ambulance resource.
There are currently more than 200 Community First Responder schemes across Wales comprising
of approximately 2,200 volunteer members. These responders save lives every year across Wales.
There are several different types of Community Response that are set out below.
Community First Responder schemes - consist of individual volunteers within the community
who must be trained to the basic level of a volunteer responder.
Partner Co-Responding Schemes - across the Central and West areas, they provide an
emergency service based response provided by appropriately trained Fire and Rescue
Service staff. We are also currently supporting a Fire Service National Joint Council Co-
Responder pilot in the North and South East areas until end June 2016.
Medical First Responders - registered Healthcare Professionals who respond to emergency
incidents. These responders have the added benefit of providing additional treatment options
over and above those provided by CFR schemes.
Established Based Responders (EBRs) - static sites e.g. leisure centres, supermarkets
equipped with an automated external defibrillator (AED) which a group of people at the site
have been trained to use in order to provide basic life support.
Community Public Access Defibs- automated external defibrillators stored securely in public
locations. CPADs can be accessed by members of the public who call 999 in close proximity
to the defibrillator and follow the instructions given to them over the phone by an Emergency
Medical Dispatcher.
Within the Operations Directorate there are several key support teams.
Fleet Department
A reliable fleet is a pivotal part of providing ambulance services. We have, through the NHS Wales
Capital Programme, invested heavily in a modern fleet of ambulances and Rapid Response
Vehicles. The national fleet manager and his team are responsible for ensuring that there are
sufficient numbers of vehicles available in each operational area of the Trust to match the demand.
Employing 38 staff spread across the entirety of Wales, the Administration Department is mainly
based at Wrexham and shares the same site as one of the four in-house workshops. The other
three in-house workshops are located in Cardiff, Blackwood and Bangor. There is also a
management team based at Vantage Point House, Cwmbran.
The Fleet Department manages and maintains the vehicles through a rigorous and robust Planned
Preventive Maintenance (PPM) schedule. Maintenance is primarily undertaken at the four in-house
workshops in the North and South East areas.
Resources Department
Ensuring we have sufficient operational staff in the Clinical Contact Centres and out on field-based
operations crewing ambulances and Rapid Response Vehicles is key to providing a safe service.

27
Operational staff are co-ordinated by four resource centres. Resource managers and their teams
ensure that staffing is managed in line with rota patterns. Staffing increases required by special
events are co-ordinated by the resource centres.
NHS Direct Wales Services
NHS Direct Wales provides a one-stop-shop for healthcare information, offering advice and support
over the telephone and online, which includes triage from both nurses and dental health advisors.
The service presently employs approximately 177 staff (136.51 WTE) including call handlers, nurse
advisors, dental advisors and management and administrative support.
Visits to the website continue to rise with users looking for information on particular health
conditions or support services, including use of the online symptom checkers.
In 2014/15
301,739 telephone contacts were received, a 5% decrease on the previous 12 months, of
which 55.3% were directed away from unscheduled care
4,545,133 website visits were received, a 29.29% increase on the previous 12 months
42,481 low acuity ambulance calls were transferred for clinical nurse triage, of which 51%
were directed away from requiring an ambulance response
HART (Hazardous Area Response Team)
The Trust also provides and supports a specialist service known as HART (Hazardous Area
Response Team). The HART team forms the central plank of what would be the organisation’s
response to any major incident, physical incident or weather-related event (including, in the current
political climate, the organisation’s response to any acts of terrorism) and employs 28 paramedics
and 14 EMTs, supported by 2.8 WTE management and administration staff.
The HART team ensures the statutory obligations and duties of the Trust are met in relation to its
role as a Category One Responder under the Civil Contingencies Act 2004 (CCA), the UK
Government’s Counter Terrorism Strategy (CONTEST), and the Security and Counterterrorism Act
(2015). Other legislative and guidance documents relating to security and emergency
preparedness from both UK and Welsh Government are addressed as part of Trust core business,
with the support of the HART team.
The Resilience and Specialist Operations department comprises Resilience Managers responsible for specific Health Board areas across Wales, as well as the Hazardous Area Response Team (HART), the Special Operations Response Team (SORT) and an Event Planning Manager. The Resilience Managers work closely with key partners in delivering against statutory (Civil
Contingencies Act 2004) and non-statutory guidance in relation to emergency preparedness,
resilience and response (EPRR). Resilience Managers engage through the Local Resilience
Forums (LRF) which are coterminous with the four Welsh police forces. The department is also
engaged in national fora to support the area of operations from Resilience / EPRR, HART and
SORT. We are also engaged in the UK Contest Board, the UK counter terrorism strategy.
Under the Civil Contingencies Act 2004 (CCA), Category One responders are subject to the
following full set of legal civil protection duties:

28
risk assessment;
emergency planning;
business continuity planning;
warning and informing;
information sharing; and
co-operation.
In ensuring the organisation is fully discharging its legal obligations and ensuring that it is in a
suitable state of readiness to react to any situation, a number of actions are being progressed by
the organisation and lead by the HART team. These are listed in the governance section of our
plan (section 6).
All of these operational resources, ambulances, HART, rapid response cars and UCS crews are co-
ordinated via three Clinical Contact Centres (CCC). Within the Cwmbran CCC is a team of 18
Secondary Triage Clinicians who provide support to the allocators and call takers who receive and
dispatch the calls.
Our CCC teams answer, prioritise and assess every call that we receive. Most importantly, they give
advice to callers on life-saving first aid that can be given in the minutes while the ambulance is
travelling to the call. They are an often forgotten vital part of every life we save.
Patient Care Services (PCS) – non emergency/ elective patient transport
Non-Emergency Patient Transport (NEPTS) is delivered by the organisation through the Patient
Care Service (PCS) section of the organisation. We employ approximately 590 staff on PCS, with
480 operational, 28 working in ambulance liaison at hospitals and 70 in PCS Control.
The PCS service provides non-emergency transport to the residents of Wales who, for medical reasons, are unable to make their own way to hospital locations and treatment centres. Such journeys include:
outpatient appointments; patients for dialysis and cancer treatments; day centre and psycho-geriatric clinics; admissions and discharges, including inter-hospital transfers; and end of life care pathways.
The service acts as a vital link between communities and is an integral part of the overall package of healthcare that the Welsh Ambulance Service provides in Wales.
There are various aspects involved in the service delivery of the PCS.
Non-Emergency Patient Transport (NEPT) contact centres - where healthcare professionals and/or patients contact the ambulance service to book non-emergency transport
Planning and Day Control teams - who are responsible for the co-ordination of available resources
Operational ambulance staff Ambulance liaison staff – based at many of the hospital sites Customer Services Managers
PCS operational staff are trained in the particular needs of the patients we convey, including first aid, oxygen therapy, specialist driving skills, patient moving and handling techniques, basic life support (including automated external defibrillation) and general patient care skills.

29
The PCS uses specially designed vehicles to provide appropriate levels of clinical care, comfort and safety for patients.
Delivery of these frontline, patient-facing services is supported by a number of corporate
directorates employing approximately 9% of our overall workforce. These include:
Directorate Headcount WTE
Quality & Patient Experience 39 35.04
Workforce & OD (inc NATC and Occupational Health) 79 73.68
Finance & ICT (inc Health Informatics) 71 67.73
Strategy, Planning & Performance 18* 16.01
Clinical Directorate 53 50.93
Chief Executive & Corporate Secretary 7 6.24
Engagement & Partnerships (including Communications) 6 5.56
Total 273 255.19
*This figure includes staff working in Capital Planning- a function currently being managed by the Director of Finance and ICT
Further details of the Directorate portfolios are described below.
Quality, Safety & Patient Experience Directorate
The Quality and Patient Experience Directorate has three core aims:
To support front line teams and managers to deliver quality-led services;
Provide the right quality assured information, in a timely manner that allows the Executive Management Team and Trust Board to make informed decisions regarding the quality of care we provide; and
Provide assurances to the Executive Management Team, Board sub-committees and Trust Board in matters relating to quality, safety and experience.
The core functions of the Directorate include the following.
Patient Experience – Partners in Healthcare
Putting Things Right – complaints, patient safety incidents, claims, inquests
Safeguarding adults and children
Professional standards and practice education
Nursing revalidation
Risk management
Health and safety
Quality assurance
Quality improvement
The Directorate leads the Quality Strategy for the Trust. This embraces the NHS Wales Health and Care Standards (2015) and the All Wales Standards for Accessible Communication and Information for People with Sensory Loss. The Directorate also works in partnership with Health Inspectorate Wales, the Community Health Councils, Commissioner for Older People and Childrens Commissioner.
30
Workforce and Organisational Development Directorate
As a strategic corporate directorate, the Workforce and Organisational Development Team supports
the business of the Trust, and are ambassadors for our shared behaviours, health improvement,
well-being, equality and diversity encouraging these across the organisation.
The Workforce and OD Directorate comprises the following main portfolios.
Operational Human Resources, including workforce governance and information
Organisational Design & Development
Training, Education & Development
Employee Well-being and Occupational Health Services
Engagement & Partnerships (including Communications) Directorate
The Directorate of Partnership and Engagement is a newly created directorate, the purpose of
which is to bring coherence and strategic insight to the Trust’s engagement and partnership
agenda, as well as protecting and enhancing the reputation of the Welsh Ambulance Service among
its many stakeholders. The Directorate, which is led by the Director of Partnership and Engagement,
currently comprises the Office of the Chief Executive and the Communications Team.
Finance (revenue and capital), ICT, Health Informatics and Estate Directorate
The Trust’s Finance Department forms part of the Finance and ICT Directorate and provides
strategic and operational finance leadership and support to the organisation, acts as a key link
between the organisation and a range of external stakeholders, including the Welsh Government,
the Commissioner of EMS through EASC, LHBs and other Trusts in Wales, NWSSP, internal and
external audit.
Based across a number of key Trust sites, the finance teams provide specialist input across all
finance functions, including financial management and management accounting, financial
accounting, financial planning, costing, project accounting and capital support, counter fraud and
lease cars.
The Trust ICT Department forms part of the Finance Directorate and, along with Health Informatics
(HI), provides all information systems and services for the Trust. The ICT Department is made up of
a number of specialist teams based at five key Trust sites. These teams provide day-to-day support
to existing ICT services but also work to support the strategic aims of the Trust.
The Health Informatics functions include information governance, records management, information
analysis, business intelligence development and official statistics reporting. The department
provides services to all facets of the organisation and has developed an excellent reputation, both
internally and externally, for providing a high quality informatics service to its client base.
The Estates and Capital Teams work closely together to provide new capital developments and also
maintain the existing estate infrastructure to ensure suitability for operational staff, Clinical Contact
Centres, training, resource centres to enable stocking and washing facilities for our fleet, fleet
maintenance workshops, as well as providing administration office bases across Wales. The
Capital Team ensures that the Trust adheres to the Welsh Government NHS Wales Infrastructure
Guidance for all major capital developments and also monitors the progress of the internal capital
schemes that are funded via the Trust’s Discretionary Capital Process.

31
Medical Directorate
The Medical and Clinical Services Directorate has responsibility for securing sustainable, consistent, safe and clinically effective care through leading improvements to services and patient care and, in so doing, supporting the Trust in achieving the transformational change necessary. Under the leadership of the Executive Medical Director, the Directorate works collaboratively as a team and with other directorates to ensure that quality and clinical leadership provide the foundations for everything we do. Leading a professional, high-performing team, the Executive Medical Director ensures the identification, maintenance and assurance of agreed clinical standards. He provides the strategic clinical expertise and develops clinical standards that are patient-focused and cost-efficient whilst working together with the Chief Executive and his fellow Directors to shape the future clinical architecture and direction of the Trust.
The remit of the Directorate includes the areas outlined below.
Research and Innovation
Service Improvement
Clinical Audit
Clinical Equipment and Medical Devices
Professional Standards
Planning and Performance Directorate
The Planning and Performance Team has responsibility for leading the strategic planning of the
organisation and the planning cycle that the organisation has adopted. The Directorate also
interfaces with the wider strategic planning community of NHS Wales in order to have visibility of
(and influence over) service reconfigurations that may materially impact the organisation.
The Directorate retains a specialised project and programme management role and oversees the
highly complex programmes of change that the organisation is delivering.
The performance arm of the Directorate manages the performance management framework of the
organisation and the key relationship with the Chief Ambulance Services Commissioner in regard to
ensure delivery of the National Collaborative Commissioning: Quality and Delivery Framework
Agreement.
Corporate Governance Directorate
The role of the team is crucial to the ongoing development and maintenance of a strong governance
framework within the Trust. It is a key source of advice and support to the Trust Chair and other
Board members and is led by the Corporate Secretary. The team acts as the guardian of good
governance within the Trust by:
providing advice to the Board as a whole and to individual Board members on all aspects of governance;
facilitating the effective conduct of Trust business through meetings of the Board and its Committees;
ensuring that Board members have the right information to enable them to make informed decisions and fulfil their responsibilities;
ensuring that in all its dealings, the Board acts fairly, with integrity, and without prejudice or discrimination;
contributing to the development of an organisational culture that embodies NHS values and standards of behaviour;
monitoring the Trust’s compliance with the law, Standing Orders and the governance and accountability framework set by Ministers; and
providing advice to the Board on implementation of the Trust’s Welsh Language Scheme.

32
2.2 Our Demand & Activity
Long Term Trends
Over the last thirty years or so the population of Wales has grown from 2.73 million in 1971 to 2.99 million in 2008, most noticeably in recent years due to net inward migration from the rest of the UK (source PHW). There is considerable variation, however, as some local authorities in Wales have declining populations due to low birth rates and the outward migration of young people.
As our planning function further develops we want to ensure that we start to consider even more
robustly the clinical, operational and quality impacts of changing population trends by working more
closely with Public Health Wales and actively engaging in the Well-Being of Future Generations
(Wales) Act 2015, in particular, the Future Trends report and Public Service Boards.
Action 1: Actively work with Public Health Wales and engage with the Well-Being of Future
Generations (Wales) Act 2015 agenda in order to better develop the Trust’s strategic
responses to predicted changes in our population.
Local Authority Local Development Plans
The Local Delivery Plans developed by each Head of Operations for the seven LHB areas have
identified many major business and large housing developments that will impact in future years on
the Trust.
Under the Town & Country Act (1990), the Trust can make applications for Section 106
contributions towards the costs of healthcare relating to major developments. WAST has recently
been successful in making an application for such a contribution.
What WAST requires is a comprehensive picture of these planned major developments and a
systematic approach to making applications for S106 contributions and modelling and planning the
impact of these major developments on response times and the required resource to respond
appropriately.
Action 2: Engage with local authorities to develop a comprehensive schedule of major
development schemes, so that the Trust can apply for S106 contributions, including
modelling and planning for the required resource to respond appropriately to these
new developments.
Health Economy Changes
Another key aspect of demand and capacity planning is the portfolio of changes within the health
economy. These changes are detailed in 2.13 NHS Wales Strategic Change Agenda. During
2015/16, the Trust procured Optima: software that can simulate the impact of changes in the health
economy and assist the Trust with improved planning for performance.
Patient Flow
The flow of patients through the Trust’s part of the unscheduled care system is shown in Figure 7
below.

33
Figure 7: EMS Patient Flow (December 2015)
N.B. We will receive multiple calls about the same incident hence the reduction in the number of responses (box 5)
compared to the number of calls taken through MPDS (box 4).
The recent publication of the Ambulance Quality Indicators, as part of the CQDF, has provided more
detailed information on patient flow across the Five-Step Ambulance Care Pathway which will be
built on through 2016/17 and will further aid the Trust in developing its approach to effective
management of patient flow.
The Annual Cycle
Patient flow will vary during the year, as a result of seasonal fluctuations in demand, with spikes in
demand during the summer holiday period and during the winter. Whilst the basic EMS demand
cycle is known, predicting demand with more certainty is much more complicated because of the
number of changeable variables. For example, increasingly variable weather patterns and the exact
timing of a flu outbreak, which place a greater emphasis on the organisations ability to flex capacity
in response to changes in demand.
Similarly there are also periods of lower activity for PCS journeys associated with holiday periods,
with the reduction in journeys being attributed to stronger application of the eligibility criteria.
Demand & Capacity Modelling
In recognising the complexity of understanding demand later in our plan (Section Five, STEP 2) we
outline a piece of work to undertake a demand and capacity review of our EMS activity. We are
pursuing this collaboratively with the office of the Chief Ambulance Services Commissioner.
This is a really important piece of work not only because of what is described above but because,
coupled with this, the New Clinical Response Model is currently based on the ideal response to a
999 call. The model makes this ‘decision’ by having a predetermined ideal response to each of the
1800 MPDS codes used to prioritise incoming 999 calls. In addition to the ideal response, a
suitable response has also been identified for all codes to inform allocators’ decision-making where
there is no ideal response available.
We recognise that the model was introduced using our old rosters and staffing grades and thus
currently we not as well informed as we could be regarding what resources we need at our disposal
to make this new CRM as effective as it possible can be.
2.3 The Five-Step Ambulance Care Pathway, Commissioning Quality & Delivery
framework
The Commissioning: Quality and Delivery Framework (CQDF) went live in April 2015. The Chief
Ambulance Service Commissioner (CASC) has identified the “positive work” that has been
undertaken in the first half of 2015/2016 on developing the CQDF.

34
The Five-Step Ambulance Care Pathway
The Ambulance Care Pathway is the five step process for the delivery of emergency ambulance
services within NHS Wales. The Ambulance Care Pathway encourages the Trust to focus on the
patient journey i.e. patient flow, and a whole systems approach, rather than on functional lines. It
acts as a lens for framing all discussions on EMS, is consistent with the Trust’s New Clinical
Response Model and has been widely adopted within the Trust.
Figure 8: Five-Step Ambulance Care Pathway
STEP 1 (‘Help Me to Choose’) – This step focuses on public education regarding the services
provided by WAST and how/when to access them appropriately. This step will include the
development of appropriate linkages between WAST and the future 111 service, building on the
success of NHSDW and its website as well as the secondary triage clinical desk.
STEP 2 (‘Answer my Call’) – This step focuses on the response to 999 and Health Care
Professional (HCP) calls by WAST’s Clinical Contact Centres (CCCs). This step incorporates the
provision of adequate time to assess a call and the use of the Medical Priority Dispatch System
(MPDS) to identify the priority of the call before offering / sending the most appropriate response.
STEP 3 (‘Come to See Me’) – This step focuses on how WAST makes decisions about what
resources to dispatch to assessed/prioritised calls. Broadly, three response options are available:
Emergency Ambulances (EAs) and solo crewed Rapid Response Vehicles (RRV) and
Community First Responders (CFR) will be allocated to RED calls, e.g. cardiac arrest or
choking;
Emergency Ambulances (EAs) will be deployed to AMBER calls where the patient requires
transfer to hospital (e.g. heart attack or stroke);
solo crewed Rapid Response Vehicles (RRV) will be sent to AMBER calls where the
likelihood is that, after assessment, the patient will be referred to another service e.g. GP
Out of Hours. (see, treat and refer);
Clinical Telephone Assessment (CTA - ‘hear & treat’) will be offered to all other low acuity
AMBER and GREEN calls; and
Urgent Care Service crews (UCS) will be dispatched for low acuity GREEN patients who are
assessed by HCPs as requiring admission to hospital.
STEP 4 (‘Give Me Treatment’) – This step focuses on the development and delivery of a range of
clinical care services able to offer a variety of treatment options. The selection of the most
appropriate treatment will be supported by decision support tools e.g. Paramedic Pathfinder for ‘see
& treat’; the Manchester Triage System and the Clinical Assessment System (for ‘hear & treat’).
Treatment options will include the use of Alternative Care Pathways or ACPs (set out in a Directory

35
of Services) allowing patients to be referred to primary and community care. WAST will develop a
Clinical Hub to coordinate the delivery of care to patients (‘sign – posting’ for clinical advice,
managing referrals to alternative care pathways, and arranging non-emergency transportation i.e.
managing any element of WAST’s services that is not time critical or an emergency transport to
ED).
STEP 5 (‘Take Me To Hospital’) – Patients who require ongoing care and treatment will be
transported to hospital or to alternative care settings (e.g. Minor Injury Unit or a primary/community
care facility). The clinical acuity of the patient will dictate the level of transport. For critical care
patients or patients requiring ongoing treatment, EAs will be utilised. All other patients will be
transported by a combination of Urgent Care Services (UCS) and non-emergency patient transport
services (NEPTS) or in some cases the use of a taxi. Patients will also in safe circumstances be
encouraged to make their own way for treatment. This will usually be after secondary telephone
assessment.
Core Requirements
The Ambulance Care Pathway is then underpinned by six enablers, which are referred to as Core
Requirements (CR).
A self-assessment against the Core Requirements was undertaken in December 2015 and reported
to the Quality Assurance Improvement Panel (a sub-committee of EASC). It highlighted a number
of areas where further focus is required:
CR1 Governance
The self-assessment outlined areas for further improvement. Significant progress has been made in
2015/16, for example, the commissioning framework and risk management, but much more remains
to be done in 2016/17 to develop these arrangements before they can be established. Our plan
sets out how we are going to address this.
CR2 Patient Experience & Satisfaction
The self-assessment identified a well-established “Partners in Healthcare” Team which has fully
implemented the National User Service Framework and a range of changes e.g. new compliments
process, Dignity in Care Programme etc. The “Putting Things Right” (PTR) systems and processes
completed a 100 day improvement plan to improve performance, and this remains an area of focus
as this moves into the next phase of work.
An organisational restructure has moved PTR into the new Directorate of Quality, Safety and
Patient Experience portfolio, bringing together risk management, patient safety, patient experience,
quality, health and safety, safeguarding, complaints and claims, as well as a new Director having
started in February 2016. Updating our datix system will also make a significant impact on the PTR
agenda. From April 2016 a quarterly quality assurance report triangulating information will be
reported.
CR3 Equity
There is variation in RED performance between localities with a variation between the best and
worst performers of 32.4% (October 2015). The Trust has developed Strategic Equality Objectives
and a Strategic Equality Action Plan; however, there are different levels of maturity of arrangements
across Wales which WAST can engage with and it remains an area of focus. Managing variation
and addressing inequalities has been identified as a strategic aim of ours and we will use the EASC
commissioning NHS Benchmarking toolkit to shine a light on areas where inequity is most severe.
36
CR4 Clinical Care
A twelve-month pilot of the New Clinical Response Model commenced on 1 October 2015. This has
shifted the focus from the previous time based targets to a clinical focus on the right clinical care
and patient flow, supported by the AQIs (including new clinical indicators). The pilot will be
externally evaluated for Welsh Government and the evaluation procured by EASC. The New Clinical
Response Model is a clear priority throughout this plan.
CR5 Staffing
The self-assessment identified progress with an emphasis on recruitment, reduced sickness, a
review of rosters, an increase in productivity (unit hour production (UHP)) and an increase in
PADRs. The key focus for 2016/17 is the implementation of our People Strategy and workforce
plan, linked to changes in incidents within the New Clinical Response Model. In our plan we clearly
set out our ambition for improving these indicators
CR6 Safety
The self-assessment identified a range of safety issues that needed addressing including:
safeguarding reporting arrangements and the outcomes of Serious Adverse Incidents. A new
professional lead is in place for Safeguarding.
QAIP have also been provided with an action plan in support of the issues identified in the self-
assessment. A key development in 2016/17 will be the development of a set of core requirement
indicators in a similar style to the AQIs. The Trust already reports on a range of enabling activity
indicators; however, it recognises that the current approach needs to be improved and is currently
actively working with the CASC’s team on developing these.
Ambulance Quality Indicators
A key part of the developing CQDF is a set of Ambulance Quality Indicators (AQIs) that provide
information on patient flow, performance and clinical indicators across the Five-Step Ambulance
Care Pathway. The AQIs were published for the first time on 27 January 2016 by EASC (in
collaboration with the Trust) and will be published every quarter thereafter with LHB level
information from July 2016 onwards.
A summary of some of the emerging performance issues arising from the first publication is set out
in appendix 1.
Service Change Ideas
A key part of the CQDF is the identification of service change ideas or the “big ticket items” that the
Trust is working on to deliver the shift towards STEPS 1-3. The CQDF requires these service
change ideas to be framed using a CAREMORE® template. The CAREMORE® template is a form
of project initiation document that helps scope out an idea, its potential impact on the Five-Steps and
how we intend to evaluate it. Some 14 service change ideas have been agreed with EASC and
these, along with a summary of each, can be found in appendix 2.
Each service change idea has key milestones, including an evaluation phase. During 2016/17, the
Trust will work with the CASC’s team to ensure the evaluations are discussed with the QAIP i.e.
whether there is proof of concept and whether the approach should be embedded and/or expanded.
The Chair of QAIP, Professor Siobhan McClelland, has requested a timetable for the 15/16
CAREMORE service change ideas, in particular, when they will return to QAIP for the evaluation
phase. This timetable is currently being finalised.

37
As part of our planning for 2016/17, further service change ideas using the CAREMORE® template
will be discussed with QAIP. The Trust has traditionally suffered from initiative overload, so whilst
2016/17 service change ideas will be forthcoming, a balance needs to be struck between
completing and evaluating the 2015/16 ones and proposing new ones. Both the 2015/16 service
change ideas and emerging 2016/17 service change ideas are covered in Section 5: Our Service
Change Plans and denoted by CAREMORE®.
2.4 National Policy Context
Together for Health
The Welsh Government has set out the national strategic direction for the NHS in Wales through the
overarching “Programme for Government” and the NHS Wales strategy “Together for Health”. This
umbrella strategy has been complemented by a suite of additional policy documents or
supplementary plans, including:
The Primary Care Plan (2014);
Condition-based national delivery plans; and
Informed Health and Care: A Digital Strategy for Wales (2015).
We recognise that, as an organisation, we are not as effectively plugged into the national delivery
or policy groups for all of the delivery plans and the Primary Care plan where we clearly have a role
to play. We will work with Welsh Government colleagues and LHBs to ensure that we have access
opportunities for joint planning and any ring fenced monies associated with these programmes.
The National Unscheduled Care Programme
The National Unscheduled Care Programme gets its mandate following the oral statement of the
Minister for Health and Social Services in 2013. It describes how a ‘Framework for Unscheduled
Health and Care Services for Wales’ will be established to add value and focus to the quality and
efficiency of local unscheduled care delivery. It has recently been re-established and re-framed,
following the methodology and systemised approach of the five-step ambulance model.
We in WAST welcome this approach and the adoption of a whole system model for the
management of unscheduled care. The figure below outlines steps 0 – 10 of the model and is
intended to reflect the non-linear nature of the unscheduled care pathway.

38
Figure 9: 10 Step Unscheduled Care Model
We will use the opportunities that the framework presents to ensure joint approaches and
collaborative working on the improvement required to the unscheduled care system.
NHS Planning Framework
Welsh Government sets out the strategic context and formulates health and social care policy to be
implemented by NHS Wales and its partners. The diagram below presents the Framework of
National Planning Requirements and identifies the key drivers for change.

39
Figure 10: National Framework of National Planning Requirements
CENTRAL ORGANISING PRINCIPLES
Golden threads running through the entire
planning process. They are values and
principles that must underpin plans in the
Welsh NHS.
SYSTEM SHIFTS
Relate to the development in new ways of doing things rather than doing things better within existing models. They should be evident through all aspects of the plan.
PATHWAYS
Whilst there are many, often designed to
respond to local circumstances, the advent
of national programmes for unscheduled
and planned care have and continue to set
common requirements that must be evident
in an organisation.
SPECIFIC NEEDS
The diagnostic stage will identify particular
populations with higher levels of, or
different, needs from services. Meeting
those needs will be common to all services
across the NHS and therefore reflected in
national plans.
Prudent Healthcare
Quality and Safety
Health Inequalities
Prevention and Health Improvement
Primary and Community Care
Integration
Urgent and Emergency Care
Planned Care
Maternal and Child Health
Delivery Plans
Mental Health
Older People
Welsh Language
ENABLERS
The key resources and assets that will allow a plan to be delivered.
Workforce &
OD
Infrastructure Governance Research &
Development
Service
Change
Innovation Finance Digital
Health
NH
S O
UT
CO
ME
S A
ND
DE
LIV
ER
Y F
RA
ME
WO
RK
As well as setting out the key planning requirements, the national planning framework sets out:
Roles and responsibilities of NHS organisations within the planning system;
Clarity on benefits of having an approved IMTP;
Planning cycle timetable; and
The monitoring arrangements for delivery of IMTPs.

40
We will use the planning framework to help develop our local planning model and assure ourselves
we are delivering national policy priorities.
The Social Services and Well Being (Wales) Act 2014
The Act simplifies the web of legislation that previously regulated social care in Wales and is
designed to make access to services easier and more understandable to those who need them. The
Act focuses on:
People – putting an individual and their needs at the centre of their care, giving them a voice
and control over reaching outcomes that help them achieve well-being;
Well-being – supporting people to achieve their own well-being, building on their own
circumstances and capabilities, with better access to information and community support;
Earlier intervention – increasing preventative services within the community to minimise the
escalation of critical need;
Collaboration – strengthening duties of collaboration between social services and the NHS
as well as strong partnership working with other agencies including Third Sector;
Integration – more effective and better integrated models of care and support which provide
a more responsive range of services; and
Workforce – a better qualified workforce with skills that enable people to work across
organisational boundaries.
Welsh Health Circular (2015) 045 sets out the implications of the Act for Health Boards and Trusts.
The direction within the Act is congruent with many of our strategic intentions including, working
across the health sector and with blue light partners (collaboration and integration), focusing on
working up stream of our five-step pathway (earlier intervention) and many of our existing and
emerging workforce models embrace team working. In addition, our strengthened safeguarding
teams will ensure that we discharge our renewed accountabilities with respect to safeguarding.
The Well Being of Future Generations (Wales) Act 2015
The Act places a statutory duty on Public Service Boards and certain named public bodies to
improve the social, economic, environmental and cultural well-being of Wales in accordance with
the sustainable development principles. Whilst we are not a “named organisation” who are
subjected to the new duties, we will work within the spirit of the legislation and will work with our
partners across the public sector in Wales to support delivery of the Well Being Goals as we
recognise the contribution we have to make to many of them. We will do this through our
membership (where invited) of a number of Public Service Boards bodies in the legislation.
The seven well-being goals as well as the five sustainable development principles – long term,
prevention, integration, collaboration and involvement – are consistent with the approach of the
Ambulance Care Pathway and the New Clinical Response Model which promotes need-led
demand. They are also part of the approach we have taken and will continue to take so that we
develop our culture.
Welsh Language
As a result of the Welsh Language Measure 2011, the organisation’s Welsh Language Scheme was
replaced in 2015/16 with the new Welsh Language Standards. The Welsh Language Commissioner
will expect the Trust to comply with these standards, which cover all aspects of healthcare and
public services provided. They will also expect the organisation to increase the opportunities for
staff to use the language internally.
The Trust is committed to ensuring the services patients receive, policies and initiatives are consistent with the Welsh Language Scheme and, to support this, the Equality Impact Assessment

41
process includes a section to identify how service changes impact on Welsh speakers. The Trust is committed to the Welsh Government More Than Just Words Strategy and will put in place action plans to meet the requirements of the strategy and improve bilingual patient information, recruitment of Welsh speaking staff, and education, awareness and training.
We recognise the need to grow our capacity and ability to provide our health services bilingually. A
language skills audit is currently underway and will identify any shortfalls that will be met through a
combination of recruitment, training and partnership arrangements and is fundamental to delivery of
the “Active Offer”.
The Trust has a Welsh Language Skills Strategy. The aim of this Strategy is to identify and develop
the Trust’s bilingual and skills resources. The following actions have been identified as necessary to
achieve this aim:
An audit of existing bilingual skills
This has been successfully delivered. Based on data taken from ESR on 30 June 2015: 97% (3095) of Trust staff have recorded their Welsh Language Skills. In addition, a mapping exercise has been undertaken to identify the current situation of Welsh speakers across the Trust involved in service delivery.
An audit of workplaces and posts
In order to determine the Trust’s bilingual skills requirements, each directorate – with the advice and assistance of the Welsh Language Officer – will need to conduct an audit of all workplaces and posts within their service areas. By examining the nature of the service, each post and workplace provides to the public, the audit will establish a set of criteria against which the linguistic requirements of individual posts (the minimum level of bilingual skills needed to ensure the availability of services in both Welsh and English) can be determined. A Draft Recruitment Guidance to Determine Welsh Language Skills for Vacant Posts has been developed and will need to be approved as part of the Trust’s Recruitment and Selection Policy.
Training – upskill staff who currently have Welsh language skills and those who do not
New members of staff who deal with the public will be encouraged to demonstrate Welsh language skills to Level 1 (basic linguistic courtesy) within their first year of service. Managers will encourage newly appointed staff via local induction/ PADR meetings to achieve Level 1 with the aid of an ‘An Introduction to Welsh – Level 1 CD’ that will be developed by the Trust. Digital Health and Care Strategy In developing our Technology and Information Management capability, we are ensuring alignment
with both our business aims and priorities and the principles of the Welsh Government Digital Health
and Care Strategy.
The four principles of the strategy are listed below with links to key deliveries within this IMTP.
Information for you
We are committed to developing and delivering digital services and alternative access methods for
patients. We are hosts of the 111 Pathfinder that will build on the digital services already in place
within NHDSW. We will also look at developing patient self-service where practicable, especially in
non-emergency situations such as self-service kiosks for NEPTS services, and will look to further
enhance services through tele-health initiatives where practicable.

42
Supporting professionals
We will develop electronic capability to support operational staff and in doing so will look to utilise
greater use of mobile and remote working technologies to enable staff to securely access relevant
information at the point of care and away from their base. In carrying out this work we will work with
partners across NHS Wales not only to consume information from them but to also provide them
with accurate and timely information. The introduction of modern up to date operational system such
as the new CAD will only enhance the opportunities for staff yet further.
Improvement and innovation
We have already put improvement and innovation at the heart of our change agenda and are
committed to continuing with this approach. The availability of high quality and timely information will
be key for the future planning of service re-design. We are implementing modelling tools to assist
with future development. In addition to introducing new information systems the capability to
connect its medical devices to transfer real-time information will prove invaluable in improving
patient care.
A planned future
We are already working with organisations across Health, Emergency Services and wider public
sector and will look for further opportunities to exploit information management and technology to
transform services through providing staff with electronic patient-centred view of information in order
to support high quality care.
2.5 Major Conditions, Older People and Frailty
We recognise that we have a role to play in supporting those with major conditions and those who
are older and/or frail. We are working towards being a Dementia Friendly organisation (Action 16)
and we will work with the Older People’s Commissioner and Ageing Well in Wales National
Programme to ensure we deliver quality care to older people and those with a specific need
including dementia, sensory loss, falls, continence care and learning disabilities.
Major Conditions
In January 2015, the Minister for Health and Social Services announced an extra £70 million for
NHS Wales. Of this, £10 million was invested to support the implementation of a set of delivery
plans focusing on a range of major conditions.
In 2015/16 we were successful in securing £60,000 from the stroke fund for online stroke training for
our EMS staff. This has been fully paid for in 15/16, with training being rolled out over 16/17 (action
39, STEP 4; give me treatment).
Welsh Government has confirmed that it will be extending the lifecycle of Together for Health
Delivery Plans through to March 2020. As a result, we recognise that we need to be looking to take
full use of these funds to supplement our other funding streams.
As part of our approach to collaborative commissioning we produce CAREMORE® templates.
These help us identify and share what we believe to be some of our ‘big ticket’ service change
ideas. The CAREMORE® template helps us fully scope out these ideas and gain a greater
understanding of what the outcomes and benefits potentially are and also the resources required to
progress this work.
In the latest round of templates being produced, we have identified opportunities that may potentially
fit a delivery plan fund criteria. These include:

43
End of life care pathway– End of life delivery plan (currently identified within action 46, STEP
5);
Community paramedic pilot – Primary Care (currently identified within action 38, STEP 3);
and
GP Cluster work – Primary Care (currently identified within action 37, service improvement).
We will work with our Commissioner to gain support for these service changes ideas before then
collaboratively agreeing which is the most appropriate funding stream to access.
Older People and Frailty
Wales has an ageing population. As a service we are cognisant of the fact that a disproportionate
amount of our calls relate to elderly fallers. Consequently, we are looking to implement a range of
alternative care pathways so that these patients are not necessarily taken straight to A&E. Actions
45 & 46, STEP 5 outline alternative pathways for fractured neck of femur and end of life care that we
are looking to put in place with Health Boards. These will be supported by developments in our
training and education for our staff, described in Section 6, to equip them with the skills and
knowledge to care for patients with complex, chronic conditions.
Our data shows that we also receive a high number of calls from nursing / care homes. Action 19 in
STEP 1 commits us to working with this frequent caller category, with the aim of reducing the
number of conveyances to hospital. This is not only a positive step for the performance of the
organisation but, more importantly, will prove better for the patient as they will be able to remain in
their place of residence as opposed to being conveyed to hospital.
In addition, as part of developing the Non-Emergency Patient Transport Business Case, we
engaged with both the Older People’s Commissioner and patients. These discussions highlighted
the following areas where improvements could be made for older people.
Easier access to book transport. Consequently NEPTS will develop a single access number for all transport requests.
Reassurance and confirmation that transport is booked and on its way. Consequently NEPTS will provide a text alert service and a call-ahead service for patients that will provide a more accurate pick up time.
Reduced waiting time at hospital to go home. Consequently NEPTS will be making our liaison areas at key hospitals more patient-facing with a focus on ensuring delays are minimised.
Improved signposting to social and public transport if not eligible for hospital transport. As a result NEPTS will have a single access number for all transport requests with direct links to Traveline Cymru for elderly patients who are not eligible for NEPTS.
Public transport routes to help support visits to hospital. Consequently NEPTS will
progress a working group that is developing an integrated transport hub within North Wales
to bring together different providers to improve access to health.
2.6 Becoming a listening and learning organisation
We recognise that there are events that we need to learn from. We are committed to doing this and
making learning from experience a continual way of moving the organisation forward. An example is
learning from serious adverse incidents and the Putting Things Right agenda. In one particular
case, the Coroner made some recommendations and these are picked up explicitly in this plan.
The demand and capacity review (Section 5, STEP 3) will identify if we have the right levels
of resources to respond appropriately to the level of demand we experience.

44
We have done work on rosters and this will continue when the demand and capacity review
is complete.
We are developing the CFR role and looking to increase the contribution it can make to the organisation (Section 5, STEP 3)
2.7 NHS Wales Strategic Change Agenda
The Ambulance Service operates as part of a complex health and social care system. It is widely
recognised that no organisation can plan or deliver services in isolation due to the critical
interdependencies, the joint challenges in terms of workforce, aging population and the shared
objectives of improving outcomes and ensuring sustainability. Increasingly, collaborative planning
arrangements across regions, or nationally, are developing with each arrangement taking a different
form and reflecting different partnerships. It is key that we are engaged appropriately in these
change programmes and that we are able to model, and influence, the impact of options or
decisions. The capacity to field people to the multitude of service change programmes is
challenging but a revised approach will be led by the Planning Directorate. The proposed Business
Intelligence Hub will also be key in facilitating better understanding of the impact of proposed
changes, specifically the new Optima software. Conversations with the Chief Ambulance Services
Commissioner are ongoing to agree how these reconfigurations impact on our services so that any
resource implications are understood in a timely way. Below is an overview of those that impact
most on our services. Appendix 3 goes into more detail as to the milestones associated with these
changes.
South Wales Programme
The South Wales Programme was formed by the Health Boards of Cwm Taf, Aneurin Bevan, Cardiff
and Vale and Abertawe Bro Morgannwg to explore options for sustainable models of service for
consultant-led maternity care, paediatrics and emergency medicine. WAST was a partner in the
programme arrangements. The decision to consolidate these services on 5 sites (from 8) is being
implemented through the three Acute Care Alliances.
There will be an impact on our services; these were first mapped out by the WAST led Clinical
Conveyance group. As component parts of the South Wales Plan are implemented this impact will
need to be reviewed and the impact on WAST services taken into account as LHBs reconfigure their
services. This IMPT recommends the establishment of a Business Intelligence Hub and it is
anticipated that this group will review this work, using the Optima modelling tool.
All Wales Collaborative
Following the South Wales programme, the NHS Collaborative was formed and a number of change
programmes initiated following the same collaborative model, these include:
Major Trauma Network;
Neonatal services;
redesign of Vascular Services in Southeast Wales;
redesign of Pathology services;
Sexual Assault referral services;
Emergency Surgery redesign; and
Acute Medicine redesign.
This work is driven forward through the Director of the NHS Collaborative and a Collaborative Board
comprising the Chief Executive of each NHS organisation. Some of the workstreams have specific
project structures.

45
For WAST the most significant of these changes are outlined below
I. Major Trauma Network Development
This workstream explores the establishment of a major trauma network (MTN) in South Wales
(North Wales are part of a neighbouring MTN). Under the leadership of the NHS Collaborative, a
programme of work underway across South Wales to develop a major trauma network. The model
will have a single Trauma Centre at UHW, Cardiff or Morriston, Swansea supported by a [yet
defined] number of Trauma Units and underpinned by a clear rehabilitation model.
A series of work streams have been established to support the decision making process around this:
baseline assessment of current service provision, to be considered by the Clinical Reference
Group;
information - which will consider further information requirements to support the impact
assessment of a major trauma centre at either Cardiff or Swansea;
finance and commissioning – which will be asked to estimate the revenue and capital
implications of the development of a major trauma centre at either Cardiff or Swansea;
engagement – which will prepare an engagement and communications strategy which will
underpin the development work, and which will ensure that stakeholder views are taken into
consideration in the decision making process;
workforce - which will confirm the workforce implications of the development of a major
trauma centre at either Cardiff or Swansea; and
rehabilitation - A series of three workshops is being planned to take place in November,
December and January to confirm the service model.
We are well represented across the various workstreams and have recently initiated some work to
quantify the impact from an activity and job cycle perspective. As well as impacting on journey
times and numbers of transfers, there are likely to be implications for our workforce, namely our
EMS crews caring for major trauma patients for potentially longer periods of time as they travel to
the Major Trauma Centre. Once implications are known, these will have to be fed into our training
requirements.
II. Neonatal Services
Neonatal intensive care is currently provided from three hospitals in South Wales: University Hospital of Wales, Cardiff; Royal Gwent Hospital, Newport; and Singleton Hospital, Swansea. The clinical workforce at each neonatal intensive care unit (NICU) includes doctors training in neonatal medicine and the allocation and placement of trainees is managed by the Wales Deanery. A phased reduction in trainee numbers is planned and, as a consequence, training will be concentrated in two units from September 2016. The Neonatal Clinical Reference Group and the Collaborative Board have considered the implications and it has been confirmed that the intention would be to maintain three neonatal intensive care units (NICUs), one of which would become a non-training site. A process to determine the location of the non-training unit is being developed and will be a joint approach through the Welsh Health Specialised Services Committee, which is responsible for the commissioning of neonatal intensive care, the Wales Neonatal Network, the Clinical Reference Group and the Wales Deanery. We continue to be interested and engaged in the outcome of this work as there is a clear impact on our services. The Planning Directorate will lead on this work and engage clinical and medical representatives as appropriate. The Business Intelligence Hub will support the modelling of the options.

46
III. Acute Medicine and Surgical Services
As part of the legacy from the South Wales Programme, work has been ongoing to further progress
the development of service models and recommendations for acute medicine and surgical services
across South Wales.
The service model for acute medicine and the range of service models for the surgical specialities have identified levels of care across the patient pathway that indicate that care can be differentiated across hospitals, and outline the supporting services required to ensure a safe and sustainable service. The work on acute medicine and surgery will be further considered to set it within a strategy for the region. We continue to be partners in these change programmes and will analyse via the Business Intelligence Hub the impact of options, as any changes to these services will clearly impact on our emergency services. Mid Wales Collaborative In January 2014, the Welsh Government commissioned the Welsh Institute for Health and Social Care (WIHSC) to explore the options for the provision of high quality and sustainable healthcare services in Mid Wales. The Mid Wales Healthcare Study, published in October 2014, highlighted a number of issues and made twelve recommendations to ensure healthcare services in Mid Wales are effective for the population. The first recommendation was that a joint governance mechanism, ‘The Mid Wales Healthcare Collaborative’, should be established in order to implement many of the other recommendations made in the Study. The Mid Wales Healthcare Collaborative (MWHC) which comprises the four healthcare organisations that cover Mid Wales – Betsi Cadwaladr University Health Board (BCUHB), Hywel Dda University Health Board (HDUHB), Powys Teaching Health Board (PTHB) and the Welsh Ambulance Services NHS Trust (WAST), was formally launched on 12th March 2015 by the Minister for Health and Social Services at the Rural Healthcare Conference. The objectives of the MWHC is to implement the recommendations of the Mid Wales Healthcare Study in order to:
deliver a single integrated change programme, with full public and professional participation, which addresses the delivery of social care, primary care and specialist care as an integrated continuum, provided as close to home as possible;
address prevention as well as treatment, and promote prudent healthcare; and
deliver a regional plan for Mid Wales. The Collaborative’s governance arrangements together with a dedicated Project team have now been fully established. Appendix 4 details the actions that are being progressed by each of the Innovation sub-groups in order to ensure delivery of the Study’s recommendations with key priority areas of work identified below.
Centre for Excellence in Rural Healthcare: The establishment of a Centre for Excellence in Rural Healthcare with a particular focus on research, development and dissemination of evidence in health service research which addresses the particular challenges of Mid Wales.
Virtual Ward: Roll out the concept of the ‘virtual ward’ to all parts of the Mid Wales area through the establishment of integrated health and social care community teams supporting primary care. This work is being led by the Primary care and Community Services sub-group who will agree the core principles of the ‘virtual ward’ and then allowing for local variation and reflecting local circumstances, ensure the core principles are in place across all parts of the Mid Wales area. The funding requirement is to be identified by Primary Care and Community services sub-group.

47
Telehealth: Ensure that there are accessible and appropriate telehealth services available across Mid Wales. The Welsh Government have awarded £250k funding of which £25k has been used to undertake a scoping exercise of telehealth provision across Wales. The report was published in January 2016 and the balance will be used to fund the implementation of the recommendations.
Mental Health: Ensure that out of hours crisis support is available across Mid Wales.
Access and Transport: Ensure better alignment between clinic times/Day Surgery and patient transport.
Engagement and Involvement: Ensure effective communications, engagement and involvement with the public, staff and stakeholders. This work is being led by the Mid Wales Healthcare Collaborative team and includes a series of engagement events and the establishment of a Stakeholder Reference Group. The first round of engagement events involved 4 events Machynlleth, Aberystwyth, Blaenau Ffestiniog and Welshpool. During these events the public were asked for their ideas and comments regarding the Innovation sub-group actions and this feedback will be used to further inform and enhance the work of the Innovation sub-groups. Also the Stakeholder Reference Group (to be established) will provide a pool of interested and motivated individuals on whose expertise and experience the Innovation Sub Groups could draw upon.
Other change programmes
I A Regional Collaboration for Health (ARCH) The ARCH Programme sets out a vision for an integrated and collaborative medical and life sciences regional economy delivering high quality patient care, developing doctors, healthcare professionals and life scientists to drive excellence for the sustainable benefit of the health, well-being and wealth creation in South West Wales. Key partners are Abertawe Bro Morgannwg UHB, Hywel Dda UHB and Swansea University. The programme sets out to deliver a regional, holistic model of healthcare aimed at transforming healthcare services providing:
a step change in the care delivered closer to home;
drastic improvements in the wellness of the region and health outcomes for citizens with long term condition;
specialist centres providing excellence in care; and
exemplary patient experience. This programme represents a system approach to health and well-being and whilst it is still in its formative stages, WAST, will engage to explore opportunities for collaboration as part of that system.
II Aneurin Bevan – Clinical Futures – Taking Better Care The Clinical Futures – Taking Better Care Programme sets an ambitious vision for increased and
better services involving a rebalancing of primary and community care led services across the
Gwent health economy. Key areas of working include:
Community Resource Teams and the Gwent Frailty Programme;
local General Hospitals;
developing Mental Health and Learning Disability Services through partnership; and
Specialist and Critical Care Centre.

48
The full business case for the Specialist Critical Care Centre is awaiting Welsh Government
approval. Our services will be impacted on and we continue to work within WAST and with the
Health Board to quantify and model this impact. We will take the outcome of this work back through
the EASC commissioning arrangements.
III Change for our Powys patients The NHS Future Fit Programme focuses on the hospital services provided by Shrewsbury and Telford Hospital NHS trust and Shropshire Community Health NHS Trust. Powys Teaching Local Health Board and WAST are partners in this programme. The decision, including a preferred model for clinical services (that was deferred in October 2015), is now due in mid-2016. WAST is a partner in the Programme Board and will step up its senior visibility and engagement in this programme during 2016/17. During 2014 Wye Valley NHS Trust was placed in special measures following an inspection by the
Care Quality Commission. Powys Health Board is working closely with both the English Trust and
the Hereford Clinical Commissioning Group (CCG) to monitor progress against the patient care
improvement plan and ensure that Powys patients access safe and effective high quality care.
Whilst Powys LHB are involved in taking their transformation programme led by Hereford CCG,
further work is required to ensure any implication on WAST are fully understood and modelled.
2.8 Service Change with Blue Light Partners We are cognisant of the Fire and Rescue National Framework that was published by Welsh Government in November 2015. We are very supportive of this document and recognise that whilst it is not a mandatory function of Fire and Rescue Authorities (FRAs) to provide certain forms of emergency medical response and/or support, nonetheless FRAs should continue to work with WAST and other NHS bodies to develop and implement such initiatives. Co-responding schemes already operate in South, Mid and West Wales. Most recently a pilot has been launched in North Wales that now see the Fire and Rescue Service working with WAST to respond to some emergency calls. Fire and rescue vehicles have been kitted out with life-saving equipment such as defibrillators, with staff receiving extra training in CPR and other medical skills. In addition, the Betsi Cadwaladr area of the Trust has embarked on an interesting joint venture with our blue light emergency service partners to develop even closer collaboration and explore new ways of working. In June 2015, the North Wales Emergency Collaboration Board was formulated. This new Board is made up of the three blue light 999 services with a programme of work formally instigated in July 2015.
This programme of work is designed to progress and expand the collaborative working arrangements across the three blue light services. However, this does not preclude other agencies from joining the programme. As the work develops and cross organisational benefits are identified, Betsi Cadwalader University Health Board, local authority professionals or any other professional body as agreed by the Chair of the Board may and should participate. The programme consists of three workstreams each led by one of the 999 services and are:
Integrated Service Delivery Prevent and Respond;
Multi-Organisational Control Room; and
Integrated Service Delivery Support Services.

49
In January 2016 we looked to internally second, for a period of six to twelve months, a member of staff to work with colleagues from the police and fire services in developing opportunities identified in the programme above. Finally, the construction of our new Ambulance and Fire Services Resource Centre (AFSRC) in Wrexham is now complete. The Welsh Ambulance Service and North Wales Fire and Rescue Service (NWFRS) have jointly invested in this purpose-built facility, which will include staff welfare facilities together with meeting and training facilities. The facility becomes operational in the early spring of 2016. We are working together with Mid and West Wales Fire and Rescue Services, Hywel Dda University Health Board and Dyfed Powys Police on a joint project which is aimed at making homes safer for citizens by reducing the risk from slips, trips and falls. It will also include a security assessment service to cascade crime prevention advice to support the Police Service’s aim of crime reduction and reducing the fear of crime. Each home will be assessed individually to ensure that the most appropriate safety and security device is in place to help elderly, disabled or vulnerable people ensure their property is secure. Further information regarding how we plan to work even more closely with our blue light partners
can be found throughout this plan at section 5 (STEP 2), section 5 (STEP 3), section 6.3 and
section 6.10.
2.9 Ensuring Integration with Our Partners’ Three Year Plans
In developing our three year plan and learning from feedback on the plan that was submitted last year, we have been mindful of ensuring effective integration with the strategic plans of our partners. This has been progressed on a number of fronts. At a local level, WAST Heads of Operations have close working relationships with LHB operational and managerial staff. In the local delivery plans of Heads of Operations, there are joint priorities in terms of patient and system flow, pathway development and, in some cases, collaborative workforce approaches WAST has been interfacing with the strategic planning agenda in NHS Wales during the development of this plan.
Revisiting the South Wales Programme plans and timescales
Planning review sessions with Aneurin Bevan UHB to understand more fully the impact of the recently submitted Full Business Case for the Specialist and Critical Care Centre
Engagement with the next stage of the maternity consultation in North Wales
Ongoing and proactive involvement in the Mid Wales Health Collaborative
Engagement in the Future Fit redesign in Shrewsbury and Telford (our Powys patients) In addition to these activities, discussions were held with all LHBs about alignment of plans, with most opting to use the framing of the five-step model where appropriate.
Appendix 4 provides a summary of all the work which both Health Board partners and Trusts are documenting in their IMTPs which we believe will impact on our service, in addition to a summary of all the service developments we are planning which will impact on our partners. These will be agreed with LHBs between January and March 2016 and the document shared with Directors of Planning.

50
2.10 The Organisation and Prudent Healthcare
WAST is committed to the four principles of prudent healthcare. As an organisation that is making great strides in its ambition to move from a transport-based to a clinically-led, quality-driven service, the principles of prudent health reflect the journey on which we have embarked. They are also reflected in our shared behaviours. The Trust Board is resolute in its determination to ensure that the organisation delivers a suite of high quality services that are underpinned by a prudent approach to delivery. Prudent principles also underpin our planning process and are reflected throughout this plan including the three key areas of action within the Securing Health and Well-being for Future Generations document. This aligns to the work already being undertaken in relation to the prevention and management of patients who fall, providing appropriate treatment and care and supporting people to be independent in their homes, avoiding hospital admission wherever possible. Examples are provided in the case studies below. In working to make a prudent approach to healthcare a standard feature of our operating model and our culture, we are cognisant of the need to ensure our enabling strategies, for example our finance, IT, research, estates and workforce plans, facilitate the change and are informed by what we are learning from the implementation of our New Clinical Response Model during the pilot. Working prudently is at the heart of our future workforce training and modernisation agendas, particularly the application of the principle: “only do what only you can do.” As we develop our ambitious plans for service change, we will consider how roles work together to ensure rigid demarcation is avoided and that patients receive their care from teams that work well together across clinical pathways. We are reviewing the development needs of our staff to enable them to work flexibly and to operate at the top of their competence to be able to meet the needs of patients today, but also anticipating changes to demography and population needs.
Improving the evidence base for our decisions is fundamental to embedding a prudent culture. We are investing in technology like digi-pens to record episodes of care in real time and Optima Predict, an interactive strategic planning solution for emergency services that provides a platform to enable effective planning and the simulation of resource requirements, to ensure we are learning from our experiences and using that intelligence to inform future developments. Similarly, we are growing our research and development expertise, and working collaboratively with the higher education and commercial sectors, as well as with health partners, to facilitate an environment where the expansion of knowledge in pursuit of better patient care can flourish. Prudent Healthcare Action Plan In producing this plan, we have been cognisant of the prudent healthcare action plan and the need to ensure alignment and integration with its actions.
Action Number WAST response Cited in IMTP
Action 1: Appropriate tests, treatments, and medications
Heart Attack – taking patients
direct from the scene to a
cardiac catheterisation
laboratory for immediate
interventional cardiology
treatment. This service is
available in all HB areas and
Section 5 - STEP 5

51
delivers better outcomes and
shorter lengths of hospital stay.
Stroke – taking stroke patients
to a hospital where a CT scan
and specialist stroke care is
available leading to better
clinical outcomes and shorter
hospital stays.
Action 2: Changing the model of outpatients
Non-Emergency Patient Transport
Section 5 - NEPTS
Action 3: Working together to improve healthcare
Falls prevention & hospital avoidance – New Clinical Response Model & alternative care pathways Frequent caller management. Putting in place multidisciplinary team plans involving primary and secondary care for frequent callers. This leads to better outcomes and fewer ambulance calls and ED visits. Equity: to support people with learning disabilities access healthcare Welsh Language Standards Inequalities (sensory loss, learning disabilities)
Section 5 - STEP 1, 2 & 5 Section 5 - Action 19
Section 6.9 - Action 138 and the work of Partners in Healthcare Section 2.4 Section 6.9 - Action 138
2.11 Treating People Fairly – Equality, Diversity & Human Rights
Our Equality and Human Rights Strategy (2016-20) is called Treating People Fairly. It explains what
we intend to do to build upon the progress we have made over the last four years. Our aim is that
we create an environment where regardless of background or circumstances, each patient is
provided with a high quality service to meet their needs and every colleague achieves their full
potential.
Our aim, at the heart of all of our plans, is to shift from “treating people how we want to treat them”
to “treating people how they want to be treated”. Treating People Fairly is significant as it links how
we will play our part in delivering the Equality, Welsh Language, Well-being of Future Generations
and Social Services and Well-being Acts. The most important part of delivering Treating People
Fairly is helping every colleague to recognise, understand, and value difference in everyone by
ensuring that no-one is excluded.

52
Our Progress and Learning
The Trust has made significant progress since the launch of Treating People Fairly, as described
below:
2012-16 Strategic Equality
Objectives
What has gone well Areas for development in 2016-20
1
Increase the number of people
choosing healthy lifestyles and
accessing preventative health
care services
Events across Wales with stakeholders
leading to improved understanding;
increased links between Heads of Ops
and LHBs
Further focus on appropriateness of
general public choices when
accessing healthcare
2
Improve the care of: Older
People, Disabled people,
Lesbian, Gay, Bisexual,
Transsexual & Transgender
people by ensuring that they are
treated with dignity and respect
Engagement with specific communities;
greater understanding of local
community needs
Increased linkages across WAST
and partners; more localised
planning
3
Increasing the overall diversity of
WAST workforce-removing any
barriers relating to recruitment of
Staff and Volunteers from
protected characteristic groups
Development and implementation of
modern apprenticeships; building of
relationships with specific groups (e.g.
through Stonewall)
Maintain focus on developing local
and Trust-wide approaches
4
Reduce gender pay differences
through further exploration of
data
Continued research and benchmarking;
some focus on specific identified issues
Further detailed research with
specific data (e.g. training)
5
Improve staff awareness,
understanding and ownership of
equality and human rights issues
through “Treating People Fairly‟
agenda
Launch of Treat Me Fairly e-learning
package; delivery of From Dignity to
Engagement; start of Hear to Be Our
Best; development & launch of shared
behaviours
Ensure Treat Me Fairly and other
learning opportunities are available
and are promoted.
6
Increase staff awareness of hate
crime, harassment and domestic
abuse
Public services partnerships promoting
understanding
Target specific areas and support
colleague awareness
7
Improve engagement with people
from all protected groups in the
review and redesign of services
Feedback through PIH networks on the
development of WAST services; use of
patient stories
More engagement at local level with
service plans
8
Improve outcomes for people
from protected groups by
improving access to services
Improved understanding of access
issues; information supported services
to develop
Increased local engagement to
understand local access issues
Our Strategic Equality Objectives 2016 - 2020
We have reviewed our 2012-16 Strategic Equality Objectives, as required by law, and considered
the lessons we learnt, described above in developing draft objectives for 2016-20. We consulted on
these during December 2015 and January 2016. From what our patients, service users, partners
and colleagues said, we developed objectives as our focus for 2016-20. As our key learning was
that Wales is a series of communities, we have developed broad Strategic Equality Objectives that
have been refined and defined locally. Specific local actions have been locally developed and
owned and will be delivered to meet the needs of each community in Wales

53
What are we trying to achieve 2016-20?
We better understand our local communities by listening to them and finding out what they want
Everyone gets the right service for their needs by providing different things for different people (this may mean taking positive action)
We have a diverse and representative workforce by helping every applicant and colleague feel valued for who they are and what they bring
We tackle unlawful discrimination
We build better relationships between different people and groups
Below are our Strategic Equality Objectives for the next four years.
Our Objectives To Cover
1. Dignity and Respect
Ensure both the people we serve and our staff are treated fairly and with dignity and respect by improving staff awareness, understanding and ownership of what this means.
Local priorities for protected groups by linking with local partners. Awareness raising and training.
2. Involvement and Engagement
Engage with people in the review and redesign of services,
and improve access to services to enhance people’s
experience and care.
Stepping into communities, engaging with protected groups. Asking. Listening. Feeding back.
3. Working for Us
Improve employment practices and have our staff better
reflect the diverse population in Wales.
Recruitment practices, local recruitment initiatives.
4. Being Safe
Raise awareness of all forms of harassment and abuse for staff and public including (but not limited to) domestic abuse, abuse of vulnerable individuals and hate crime.
All colleagues. People in Wales.
5. Being Healthy and Choosing Well
Improve information and awareness about healthy lifestyles and accessing appropriate services.
Including Alcohol, Obesity, Smoking, Mental Health Issues.
Our Board will ensure that Treating People Fairly, and our Strategic Equality Objectives are
delivered by supporting teams to understand the importance of the plan, and to develop and deliver
against their objectives. They will also ensure a prominence in their discussions by receiving and
publishing regular reports on our progress (including publishing an Annual Report).
Our Executive Management Team will ensure that Treating People Fairly is delivered by also
receiving regular updates, and monitoring delivery against objectives through the executive
performance review process.
Our Equality Group is a cross section of colleagues with responsibility, passion and interest and will
provide specific focus, energy and leadership to help us deliver Treating People Fairly. Our aim is to
support all colleagues to acknowledge and understand their own and others’ beliefs and to
recognise the impact of their behaviours so that they can provide the best services. Our Equality

54
Group will help to support local teams to embed local equality objectives (in line with the Strategic
Equality Objectives) and deliver their local equality actions (as an integral part of their Local Delivery
Plans).
Action 3: Use every opportunity to promote understanding and valuing of difference such as
highlighting and marketing specific Wales and UK campaigns (e.g. events, weeks,
days).
Action 4: Develop and implement proactive positive action campaigns across the next three
years to ensure that our workforce is more diverse and representative of each local
community
Action 5: To establish a performance framework that enable us to monitor and review the
impact of the approaches we have taken and work we have done.
2.12 Other Strategic Workforce and OD Drivers
There are a number of key strategic drivers that influence the development of our People Strategy,
and our enabling frameworks and plans. More detail of these can be found at section 6.1.
Working Differently, Working Together
Within NHS Wales, we have described a set of workforce objectives through the Working
Differently, Working Together Framework.
Objective 1 - An engaged workforce aligned and committed to the delivery of the vision for NHS
Wales.
Objective 2 - A sustainable and skilled workforce focussed on helping the people of Wales to
improve their health as well as treating sickness.
Objective 3 - A redesigned workforce, working together to deliver healthcare for the 21st Century.
Objective 4 - A workforce that aims at excellence everywhere within available resources.
These objectives, along with the NHS Wales Workforce and OD Directors National Work
Programme, national projects, and the challenges posed by the wider health context, provide a
reference point and link to the development and implementation our own People Strategy and
enabling action plans.
Implications of the Francis and Trusted to Care Reports
During 2013 and 2014, an additional understanding of the impact of negative culture and
behaviours has emerged in the United Kingdom and more locally in Wales. These reports are still
of relevance and importance, and must be taken into account when considering the strategic
context of any workforce development objectives. They both highlight the impact of culture linked to
behaviours and performance and the importance of having in place robust plans for the ongoing
development of the workforce. We will ensure that our OD enabling plans make very clear links to
the recommendations of Francis and Trusted to Care.
The Leadership Challenge
The 2014 report, Williams Commission on Public Services, Commission and Delivery by Welsh
Government, noted the future requirement for ‘leaders who can deal with uncertainty and ambiguity
and who are able to tackle issues where there is often no simple management solution.’ The

55
Commission also set out the characteristics of high performing organisations and highlighted the
importance of having ‘both effective and progressive leadership and technical excellence in
management [are essential] for the provision of high achieving public services.’ Management can be
seen as ‘doing things right’ whilst leadership is about ‘doing the right thing’. Leadership
development and succession planning is a key strategic priority for the Trust and forms a key part of
our OD framework and enabling plans.
Prudent Workforce
The Minister for Health and Social Services, Mark Drakeford, said: “Our destiny really does lie in the
skill, the experience, and the commitment of staff at all levels in the NHS”. Key for the Trust will be
the application of the Prudent Healthcare principle “only do what only you can do” as it considers
future workforce requirements to deliver new ways of working. We describe our commitment to
prudent principles in the design of services and our future workforce earlier in this plan.
A Planned Primary Care Workforce for Wales
In November 2014 the Welsh Government launched its national plan for a primary care service for
Wales up to March 2018. The plan described a set of principles that will underpin the changes
required in primary care as:
prevention, early intervention and improving health, not just treatment;
coordinated care where generalists work closely with specialists and wider support in the community to prevent ill health, reduce dependency and effectively treat illness;
active involvement of the public, patients and their carers in decisions about their care and well-being;
planning services at a community level of 25,000-100,000 people; and
the prudent healthcare principles. Over the four years of the plan, Welsh Government has articulated the need to see a change in the
way services work together, with Health Boards moving their resources towards primary care,
supported by hospitals and other services, where needed, rather than continuing the traditional
model where hospital-based care has attracted the lion’s share of resources and attention. The
drive to provide more care at, or closer to, home requires a system-wide view of health and social
care services and a team based approach, which makes the most of the skills of this wide range of
professionals.
In our IMTP, you will see the ideas we have about the role that our paramedics can play within the
primary care team to help tackle demand and provide a potential alternative to traditional roles.
These include development of a community based paramedic role, our work with Health Boards to
rotate Advanced Paramedic Practitioner staff across GP Out of Hours and the expansion of the
variety of roles for paramedics within the Trust such as “Hear and Treat”, paramedics supporting GP
home visits and developing research and clinical lead portfolios.
Preparing for the Move to Degree-based Paramedicine
A change to the educational requirements for paramedics is proposed, with the introduction of a
degree level qualification requirement to become a qualified paramedic. This change has potential
to impact on the supply of qualified paramedic staff, existing succession planning routes for staff,
and the banding of newly qualified paramedics from 2019 onwards. It also presents several
practical challenges to be addressed, including the need to identify sufficient hospital and other
clinical placements for students and the university and internal resources required to support
training additional numbers. Conversations continue with Education Commissioners to inform
education provision going forward as part of our workforce planning. This includes preparation for

56
the three-year degree programme expected to commence in September 2017 and a plan to ensure
that there is no fallow year in the move from Diploma to Degree.
Apprenticeships
Developing links with schools, colleges and communities generally, along with offering apprenticeships, is a key part of our IMTP as a whole but particularly linking with Treating People Fairly as it ensures we are reaching ‘harder to get to’ communities. In April 2017 the UK Government is introducing an Apprenticeship Levy, a result of which we will be required to pay 0.5% of our pay bill. This change presents a future cost pressure for the Trust. Depending on the apprenticeship schemes we operate, and the number and quality of our apprenticeships, we may be able to claim this back if we are providing sufficient suitable apprenticeships. However, we prefer to see this as a catalyst to improve our career options for our communities as well as our colleagues. We will develop a co-ordinated approach to Work Experience, Apprenticeships and accessing Accredited Learning Funding across the Trust. We plan to develop our approach to work experience, apprenticeships and accredited learning,
ensuring that we have co-ordination between our workforce planning and learning and development
approaches.
Further information can be found at: https://www.gov.uk/government/consultations/apprenticeships-levy-employer-owned-apprenticeships-training

57
PART 3: CREATING OUR STRATEGIC FRAMEWORK In this section we present the work we have developed on our Strategy Map, outline our performance ambitions and articulate our Strategic Statement of Intent on how we envisage our services developing over the next 5 - 10 years.
As part of the initiation of our planning cycle for 2016/17, we reviewed our purpose, vision, behaviours, strategic aims and priorities. This framing was critical as it provided the clarity and steer required for our operational and corporate services teams to plan against. In future years we would envisage periodic re-visits to our purpose, vision, behaviours and strategic aims to ensure they remain relevant, but we anticipate that these will remain largely static. Future planning cycles would instead focus on recalibrating the priorities of the organisation as work completes and outcomes are realised in order to continually drive forward the organisation.
3.1 Our Vision, Purpose and Behaviours
In order to model and demonstrate our commitment to collaborative approaches, all colleagues were encouraged to be involved in developing our shared vision, purpose and behaviours. This has been done in conjunction with the development of Public Services Values and NHS Wales Core Principles. In order to help all colleagues understand and own these, we have created a visual image of our vision, purpose and behaviours which is striking for both our staff, stakeholders and pateints who access our services. Figure 11: Visions, Purpose and Behaviours
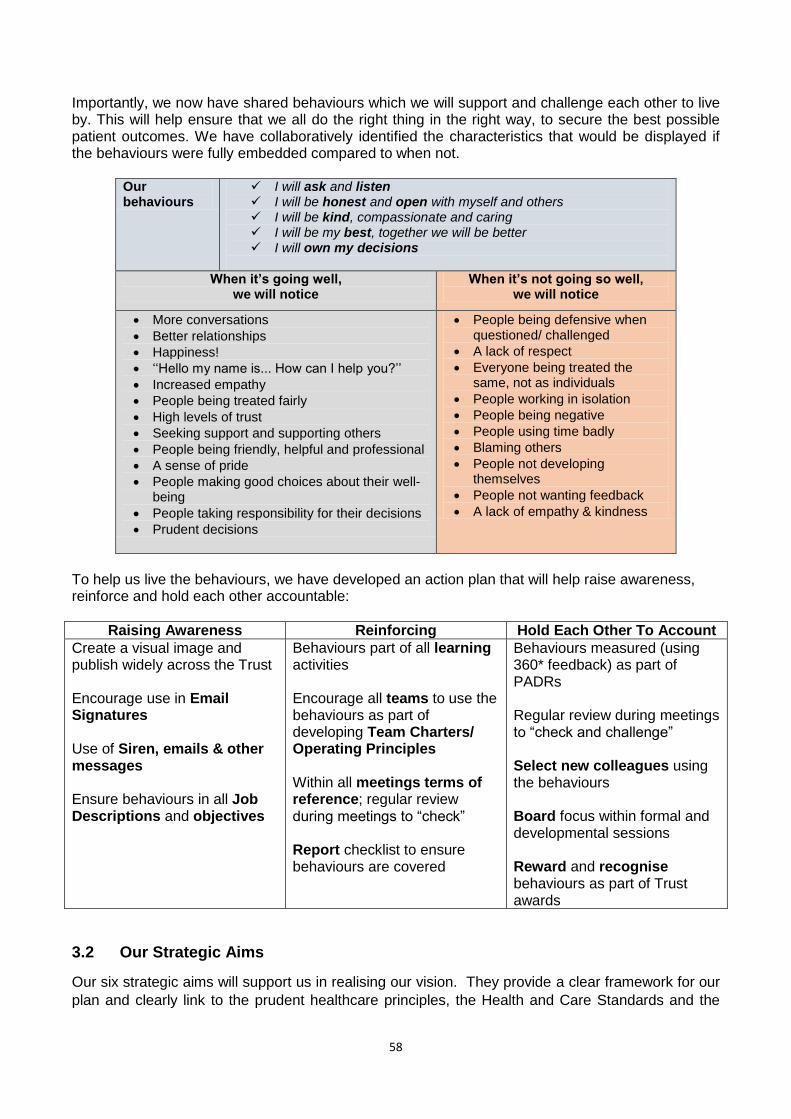
58
Importantly, we now have shared behaviours which we will support and challenge each other to live by. This will help ensure that we all do the right thing in the right way, to secure the best possible patient outcomes. We have collaboratively identified the characteristics that would be displayed if the behaviours were fully embedded compared to when not.
Our behaviours
I will ask and listen I will be honest and open with myself and others I will be kind, compassionate and caring I will be my best, together we will be better I will own my decisions
When it’s going well, we will notice
When it’s not going so well, we will notice
More conversations
Better relationships
Happiness!
‘‘Hello my name is... How can I help you?’’
Increased empathy
People being treated fairly
High levels of trust
Seeking support and supporting others
People being friendly, helpful and professional
A sense of pride
People making good choices about their well-being
People taking responsibility for their decisions
Prudent decisions
People being defensive when questioned/ challenged
A lack of respect
Everyone being treated the same, not as individuals
People working in isolation
People being negative
People using time badly
Blaming others
People not developing themselves
People not wanting feedback
A lack of empathy & kindness
To help us live the behaviours, we have developed an action plan that will help raise awareness, reinforce and hold each other accountable:
Raising Awareness Reinforcing Hold Each Other To Account
Create a visual image and publish widely across the Trust Encourage use in Email Signatures Use of Siren, emails & other messages Ensure behaviours in all Job Descriptions and objectives
Behaviours part of all learning activities Encourage all teams to use the behaviours as part of developing Team Charters/ Operating Principles Within all meetings terms of reference; regular review during meetings to “check” Report checklist to ensure behaviours are covered
Behaviours measured (using 360* feedback) as part of PADRs Regular review during meetings to “check and challenge” Select new colleagues using the behaviours Board focus within formal and developmental sessions Reward and recognise behaviours as part of Trust awards
3.2 Our Strategic Aims
Our six strategic aims will support us in realising our vision. They provide a clear framework for our
plan and clearly link to the prudent healthcare principles, the Health and Care Standards and the

59
Commissioning Quality and Delivery Framework. They are applicable to all of our clinical service
areas, across all five-steps of the Ambulance Care Pathway and to our corporate and support
services. The strategic aims will guide the organisation over the next 3 – 5 years, being used to aid
prioritisation, decision-making and in the framing of PADRs
1. To deliver the best possible patient outcomes and experience through transforming
our models of care across all of our services, using technology, innovation and research and becoming truly clinically-led and quality-driven
2. To have an engaged and skilled workforce operating within an organisational culture
and framework that enables them to work to the top of their skill set to deliver high quality care
3. To effectively manage capacity to meet demand, through aligning resources more
effectively, taking more care to the patients and accessing alterative care pathways
4. To reduce unnecessary variation in our services and processes and tackle inequalities
5. To have strong partnerships with our patients, staff, NHS Wales organisations and public
sector partners, where their voice is heard and together we improve and shape our services, and
6. To be a highly effective organisation with effective leadership embedded across all
levels, robust governance arrangements, financial sustainability and a value for money provider.
In section 3.5, we translate these aims into quantifiable performance ambitions so that we can
articulate what successful will look like against each of these aims.
3.3 Our Priorities
Our priorities represent the key deliverables that we will realise in the life of this plan. Whilst we anticipate our purpose, vision and strategic aims, remaining constant over the life of this plan, it is conceivable that priorities may change, reflecting any progress made within the course of the planning period and delivery against the priorities demonstrated. Each of the six strategic aims is relevant and applicable to each priority, for example reducing variation applies to ongoing improvements in our New Clinical Response Model as it is in improving management of our fleet. The five-step ambulance pathway is a key driver for much of our work and so, where relevant, we have also mapped our priorities to the relevant step(s) of the pathway. Against each priority we have also mapped the sections within the plan where more detail can be found regarding the specific actions that we will take to deliver these priorities. Our approach to documenting our strategic objectives and priorities, mapped in this way, ensures
the organisation is not only being fully transparent in regard to where it is investing its time, resource
and focus, but also ensures the organisation is addressing and responding to the Chief Ambulance
Service Commissioner’s (CASC) commissioning intentions. Principally:
To use the M1 Schedule: High Level Description for Model of Care – Five-Step Ambulance
Care Pathway –in order to promote and assist in the understanding of the emergency
ambulance as a clinical service within the integrated Welsh healthcare system;

60
Consider, develop and, where appropriate, deliver service change proposals for more
efficient and/or effective healthcare services by shifting the delivery emphasis on earlier
steps of the ambulance care pathway without disruption to service capability across all five
steps; and
Demonstrating plans that – when clinically safe and appropriate – reduce: o conveyances; o attendances at scene; o calls.
The table below gives an overview of our priorities, how they relate to the Collaborative
Commissioning Framework and where they are addressed in the plan.

61
Priority Description Step on pathway which priority
supports
Page Reference in
document
Clinical Response Model
supporting the strategic aim of best possible patient outcomes
and experience / manage capacity to meet demand / reduce
unnecessary variation
The 12 month pilot runs until September 2016 and will continue to be a priority for the organisation throughout 2016/17. The focus will be on specific cycles of improvement of our performance against RED calls, the clinical indicators associated with AMBER calls and on effective management of GREEN calls. The five-step ambulance care model will be a key part in framing the actions associated with this priority. Engagement in, and learning from, the evaluation of the pilot will be a critical activity for WAST in partnership with the Emergency Ambulance Services Committee. We will also use the outputs of the NHS Benchmarking Toolkit to help focus areas of activity. Developing a clear understanding of capacity required to deliver the model is key.
1 – 5
95 - 107
Modernisation of our clinical contact centres supporting the strategic aim of best possible
patient outcomes and experience / manage capacity to meet
demand / reduce unnecessary variation
Our clinical contact centres (ccc) are a key part of our service model for emergency, non-emergency and telephone assessment services (EMS, NEPTS and NHSDW/111). Key parts of this work programme are: Procure and implement a new Computer Aided Dispatch system – more than just an IT system replacement project, this represents significant workforce and businesses change for our control centres 111 Pathfinder – working with the all Wales NHS Project, the 111 Project team and ABMU, deliver successful implementation of the pathfinder
2
96 - 99
Non-Emergency Patient
Transport (NEPTs) supporting all of the organisation’s strategic
aims
Implementation of the outcome of the Non-Emergency Patient Transport (NEPTs) business case – an NHS wide project, led by WAST and aimed at delivering the disaggregation of NEPTS services from emergency medical services representing a major change programme for these services, systems and our workforce.
NEPTS
commissioning framework to be
developed
108 - 110

62
Collaborating in the development of a commissioning framework for NEPTS will also form a key part of our business in year one.
Plans for workforce, fleet and
estate supporting all of the organisation’s strategic aims
Develop robust enabling strategies and plans for workforce, fleet and estate based on the learning from the New Clinical Response Model and a comprehensive and thorough demand and capacity review.
1 - 5
111 – 146
& 163 - 167
Organisational development and becoming a highly effective organisation
supporting strategic aims of engaged and skilled workforce /
strong partnerships / highly effective organisation
Much progress has been made in establishing stable and visible leadership at Board and Executive Director level, developing clinical leadership through the organisation is now beginning to crystallise through the APP and CTL workstreams, which will continue into 2016/17. All of our strategic aims will be delivered only through an active and maturing partnership relationship with our staff and our staff representatives and robust corporate governance arrangements. Our People Strategy and enabling frameworks will support this work going forward.
1 - 5
111 - 146

63
3.4 Our Strategy Map
These interdependent elements of purpose, vision, behaviours, strategic aims, and priorities have subsequently all been drawn into a single strategy map to share with staff and stakeholders. This strategy map is shown below in Figure 12.

64
Figure 12: Our Strategy Map

65
3.5 Our Performance Ambitions
In order to translate our Strategic Aims into quantifiable ambition, we have set out the levels of performance to which we will aspire over the life of this plan. These can be found in Figure 13 below. In stating these aspirations, it should be recognised that these represent our ambitions; they are demanding ambitions but ones which remain realistic. They are complementary to the detail in the wider plan and again represent an indicative list of our more quantitative ambitions. These should not be taken in totality or in isolation from the rest of the plan. This table continues to be tested within the organisation, with our commissioners and, critically, as part of the impending demand and capacity work. As the organisation evolves and new pieces of evidence or benchmarking emerge, it may be necessary to recalibrate these ambitions.

66
Figure 13: Performance Ambitions Indicator Type Reference Measure Performance Improvement Ambition Comment
Baseline Year 1 Year 2 Year 3 Beyond
Strategic aims 1: The Best Possible Patient Outcomes and Experience
Implementing our Quality Improvement Strategy: Quality Indicators
STEPS 1-5 Core Requirements: CR2 Health & Care Standards: Individual Care
Patient engagement & experience: Satisfaction with the service
90%
91% 92% 93% 95% Baseline based on 2015 National Survey results. In addition a qualitative report on patient engagement and experience is produced on a quarterly basis for Trust Board.
Dementia Friendly Organisations – accreditation. (Ageing Well in Wales (AWW)
30 Dignity champions Trust wide Pledged
Approved implementation plan by
AWW
Implementation of plan
with quarterly
reporting to AWW
Accreditation by AWW
Maintain accreditation
status
Compliance with the accreditation process is monitored by Ageing Well in Wales, therefore providing some degree of external assurance
Bevan Innovators One project Bevan Advocate
Status
Embedding Advocate
Status
Exemplar Status
Bevan Commission Framework implementation – influencing Trust & Health Board services and plans. Independent assessment process.
STEPS 1-5 Core Requirements CR1 CR2 Health & Care Standards Governance, Accountability & Leadership Individual Care
Concerns: Response times improvement enabling timely identification of quality issues and implementation of improvements / triangulation of intelligence.
38% 50% 55% 60% Meet Tier 1 targets
Baseline based on Jan 2016. 100 day turnaround plan saw compliance increase from 6% to 38% in 2015/16.Phase 2 sustainability plan which will consider leadership & education training plan by April 2016. Note: Concerns process is under national review currently therefore these measures will undergo further review.

67
Indicator Type Reference Measure Performance Improvement Ambition Comment
Baseline Year 1 Year 2 Year 3 Beyond
STEPS 1-5 Core Requirements CR1 CR6 Health & Care Standards Safe Care
Patient Safety Increase in clinical incident reporting with an incremental decrease in the severity of incidents across all grades. *Coding sets require development
2014/15 All clinical
incidents
Baseline data
Approx. 1600
incidents per annum
Source Datix*
3% ↑ 3% ↑ 3% ↑ 20%↑ It is recognised that a healthy reporting and safety culture indicator is a high reporting organisation, with incremental reduction in the severity of incidents. Required investment & resources to enable Datix to be a fit for purpose system enabling triangulation of information and analysis of data is currently under review. External benchmarking & baseline internal data is required to determine severity reduction as coding systems within Datix are very limited currently. A safety culture assessment is planned for 2016/17.
STEPS 1-5 Core Requirements CR5&6 Health & Care Standards Safe Care
Infection , Prevention & Control: Flu vaccinations
26% 48% 52% 57% Sustained Key prevention measure however noted that ultimately employee decision.

68
Indicator Type Reference Measure Performance Improvement Ambition Comment
Baseline Year 1 Year 2 Year 3 Beyond
STEPS 1-5 Core Requirements CR6 Health & Care Standards Safe Care
Safeguarding Adults & Children Appropriate attendance at Adult & Safeguarding Boards pan Wales. (Currently 11 Boards)
One Board
80% 90% 100% 100% Sustained
Statutory requirement that WAST engage and attend with Adult & Child Safeguarding Boards pan Wales. Senior member of the safeguarding team and clinical representation from Operations to be in attendance. Configuration of the Boards is currently under review and the ambitions will be reviewed in accordance with this once finalised.
Safeguarding Quality Outcomes Framework
Amber Amber with
Incremental improvement
Amber with
Incremental improvement
Green Green Pan Wales internal assessment process. Rated Red, Amber or Green.
Implementing the Non-Emergency Patient Transport service Business Case: Performance Indicators Indicators being developed -Section to be confirmed
NEPTS
Quality
Indicators
(NEPTSQIs)
are currently
under
development.
Baseline performance is currently being established for the developed indicators, yet to be agreed. Performance
indicators are in the initial draft stage and are subject to discussions internally, externally and with the Commissioner.
Included below are the ones identified as most important in year one; identified as having the biggest impact in driving
down activity and freeing up the resources required to deliver the NEPTS modernisation agenda.
NEPTSQI9 Number of
bookings received
on- line
30% 40% 50% 60% 70% Increasing on-line booking
will free up call taking
capacity
NEPTSQI19 % of Enhanced
Service patients
arriving less than
30 min before
their appt.
55% 85%
(TBC)
TBC TBC TBC Business Case Deliverable
(Sept 2016)

69
Indicator Type Reference Measure Performance Improvement Ambition Comment
Baseline Year 1 Year 2 Year 3 Beyond
NEPTSQI20 % of Enhanced
Service patients
picked up within
30 min of time
notified as ready
72% 85%
(TBC)
TBC TBC TBC Business Case Deliverable
(Sept 2016)
NEPTSQI21 % of renal
patients travelling
more than 30
minutes
35% 30%
(TBC)
TBC TBC TBC Business Case Deliverable
(Sept 2016)
Strategic Aim 2: Engaged and Skilled Workforce
Workforce Indicators.
WG Scorecard Core Requirements
PADR 60% 85% 90% 95% Sustained We will aim for 100% of the addressable workforce.
Sickness 6.87% 5.87% 5.37% 4.87% Sustained Baseline will be based on end of year position.
CPD attendance compliance
68% 100% 100% 100% 100% Baseline based on compliance at end of Jan 16.
Staff Engagement; Index Score
43% 48%
55%
65% 65%+ Baseline based on the last
staff survey.
Percentage of EMS staff who have been offered their rest breaks on time
TBD TBD
TBD TBD TBD The importance of staff receiving rest breaks on time and a reduction in overruns is recognised. Work to be undertaken to agree meaningful measures for the organisation and staff. Overruns may have to be expressed in monetary terms to start with as this is the easiest currency to measure.
Overruns TBD TBD TBD TBD TBD

70
Indicator Type Reference Measure Performance Improvement Ambition Comment
Baseline Year 1 Year 2 Year 3 Beyond
Strategic Aim 3: Manage Capacity to Meet Demand
Resource Indicators
Core Requirements CR5
Unit Hours Production (UHP)
>90% 95% TBD TBD TBD Discrete project within resources programme proposed to make improvements to resource measures e.g. development of Unit Hours Utilisation, developing an aggregate reporting mechanism to include hours, at Health Board level, broken down by EMS, UCS and RRV to provide more detailed assessment. This will be further informed by the planned capacity and demand review.
Fleet and Estate Indicators
Fully kitted and functional ambulance that is ready to respond
75% 80% 85% 90% 90% The baseline is based on an estimate of the current situation and total vehicle stock, including spare vehicles that may not be fully kitted. All new vehicles come fully kitted. This indicator captures where a piece of equipment fails and is awaiting replacement. The model of make ready depots will, when rolled out across the organisation, significantly reduce the number of hours lost awaiting ordering of specific parts as will be centrally stocked
Vehicle Cleaning <20% >30% 40% 50% >50% We will develop a system for deep cleaning

71
Indicator Type Reference Measure Performance Improvement Ambition Comment
Baseline Year 1 Year 2 Year 3 Beyond
ambulances in line with the servicing programme. The ambition will be that there is 100% compliance with an ambulance being deep cleaned (cab and saloon) as part of the servicing programme.
NHS National Cleaning Standards Audit Assessment Toolkit
Building Cleaning Not recorded
50%
75% 95% 100% High Risk Areas: Sterile Storage, Linen Store, Sluice rooms, Medical equipment Store. Significant Risk Areas: include all other areas in an Ambulance Station Low Risk Areas: non-clinical buildings such as admin office and Control Centres. Cleaning contract for the estate to be let 15/16
Performance of Trust’s Estate is measured by NWSSP
Planned Maintenance of Estates:
NWSSP publish an annual
report NHS Estate In Wales
– Estate Condition and
Performance Report for all
Trusts in Wales.
Improvements to the
physical condition and
suitability will be
determined by levels of
investment in the estate as
well partnering
opportunities.
ISO 14001, 30% of the
estate has been accredited
(northern region complete)
Physical Condition
35% 37% 40% 43% 50%
Statutory and Safety Compliance
75% 80% 85% 90% 100%
Fire and Safety Compliance
40% 60% 80% 100% Maintain
Functional Suitability
35% 37% 40% 43% 50%
Space Utilisation
95% 95% 95% 95% Maintain
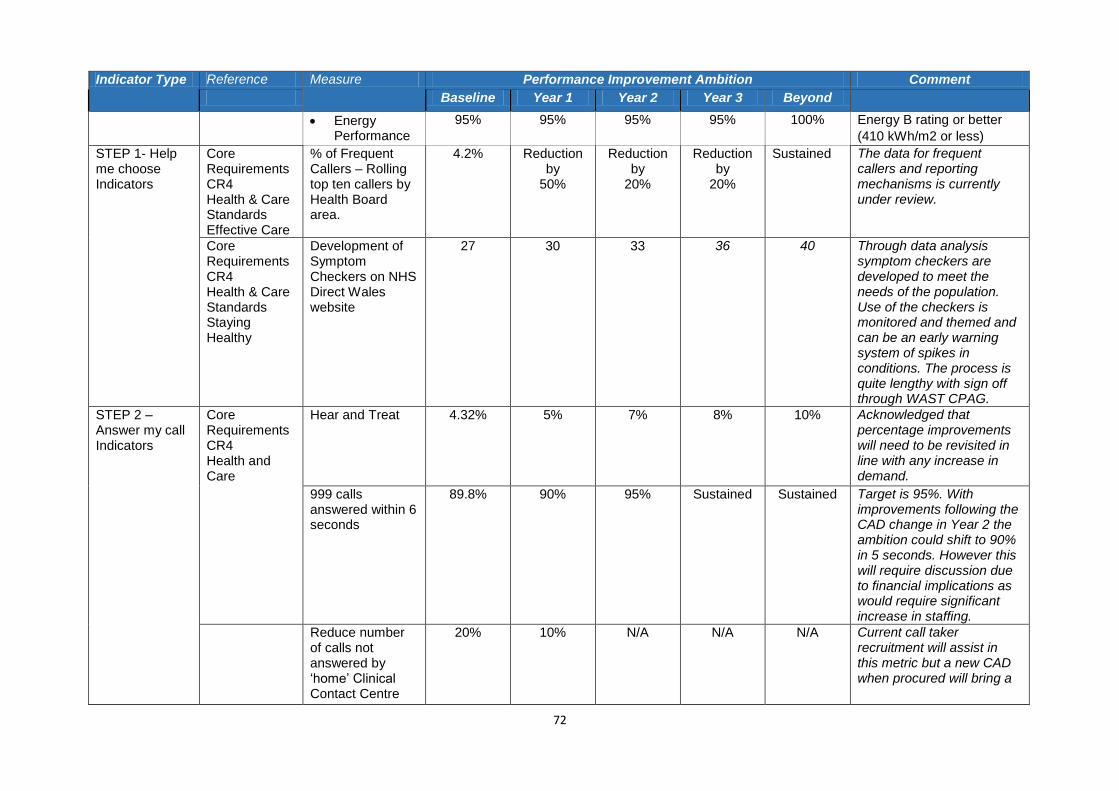
72
Indicator Type Reference Measure Performance Improvement Ambition Comment
Baseline Year 1 Year 2 Year 3 Beyond
Energy Performance
95% 95%
95% 95% 100% Energy B rating or better
(410 kWh/m2 or less)
STEP 1- Help me choose Indicators
Core Requirements CR4 Health & Care Standards Effective Care
% of Frequent Callers – Rolling top ten callers by Health Board area.
4.2% Reduction by
50%
Reduction by
20%
Reduction by
20%
Sustained The data for frequent callers and reporting mechanisms is currently under review.
Core Requirements CR4 Health & Care Standards Staying Healthy
Development of Symptom Checkers on NHS Direct Wales website
27 30 33 36 40 Through data analysis symptom checkers are developed to meet the needs of the population. Use of the checkers is monitored and themed and can be an early warning system of spikes in conditions. The process is quite lengthy with sign off through WAST CPAG.
STEP 2 – Answer my call Indicators
Core Requirements CR4 Health and Care Standards
Hear and Treat 4.32% 5% 7% 8% 10% Acknowledged that percentage improvements will need to be revisited in line with any increase in demand.
999 calls answered within 6 seconds
89.8%
90%
95%
Sustained Sustained Target is 95%. With improvements following the CAD change in Year 2 the ambition could shift to 90% in 5 seconds. However this will require discussion due to financial implications as would require significant increase in staffing.
Reduce number of calls not answered by ‘home’ Clinical Contact Centre
20%
10%
N/A N/A N/A Current call taker recruitment will assist in this metric but a new CAD when procured will bring a

73
Indicator Type Reference Measure Performance Improvement Ambition Comment
Baseline Year 1 Year 2 Year 3 Beyond
technological change in performance
Increased cardiac arrest recognition, improving allocation times <45sec
TBC 60% 65% Sustained Sustained This will be included in the CCC Modernisation work stream.
STEP 3 – Come to see me Indicators
Core Requirements CR4 Health and Care Standards
Red 8 minute performance
70.6% 65% -70%
65% -70% 65% -70% 65% -70% Baseline based on Oct 15- Jan 16 performance, post implementation of New Clinical Response model. Target is a minimum of 65% Need to recognise the whole system and the opportunities and challenges within the system that will impact upon the ambitions. There is a need to stabilise and standardise performance across Wales. This ambition will be continually reviewed and developed in light of the demand and capacity review.
CFR Contribution
2.3% 4% 5% 6% 7.5% Overall CFR contribution. Current target is 5%.
STEP 4 – Give me treatment Indicators
Core Requirements CR4 Health and Care Standards
Cardiac arrest with a return of spontaneous circulation (ROSC) on arrival at hospital.
14.6% 14.6% 15.0% 15.5% 20% New indicator. Baseline based on December 2015 performance only.
Stroke patients documented as receiving appropriate
96.2% 99% 100% Sustained Sustained Baseline based on Oct – Dec 15. Target is 100%

74
Indicator Type Reference Measure Performance Improvement Ambition Comment
Baseline Year 1 Year 2 Year 3 Beyond
stroke bundle of care
Fracture hip/femur who are documented as receiving analgesia
83.1% 95% 100% Sustained Sustained Baseline based on Oct – Dec 15. Target is 100%
Acute coronary syndrome patients who are documented as receiving appropriate STEMI care bundle
68.5% 95% 100% Sustained Sustained Baseline based on Oct – Dec 15. Target is 100%
STEP 5– Take me to a place of care Indicators
Core Requirements CR4 Health and Care Standards
Conveyance rate following face to face assessment
70.5% 70% 68% 65% 60% Baseline based on Oct – Dec 15 performance
Conveyance rate not to a major A&E
8% 10% 15% >15% TBD Baseline based on Dec 15. To develop further to Include information on referrals to other pathways.
Handover to clear-
81.8% 90% 100% Sustained Sustained Trust to have discussions with Welsh Government regarding the practicality of ever achieving a target of 100%.
Strategic Aim 4: Reduce Unnecessary Variation.
Operational and Clinical Indicators
STEPS 1-5 Core Requirements: CR3 Equity
RED performance by LHB and localities
57.1%-87.5%
65% -70%
Increasing but dependent on demand
and capacity modelling work.
Trust maintains an ambition to get to as many patients as quickly as it can.
RED performance within 8 minutes 95th percentile
00:16:44 00:15:00 00:10:00 Sustained Sustained Baseline based on Dec 15 AQI
AMBER 95th percentile
00:48:50 00:40:00 00:35:00 00:30:00 00:20:00 Baseline based on Dec15 performance, post the New

75
Indicator Type Reference Measure Performance Improvement Ambition Comment
Baseline Year 1 Year 2 Year 3 Beyond
response Clinical Response Model implementation.
Conveyance rate following face to face assessment by LHBs
TBD TBD TBD TBD TBD Measure to be developed as part of development of AQIs by Health Board. This expands on the previous conveyance measure reviewing by Health Board area.
Strategic Aim 5: Strong Partnerships
Partnership Indicators To be confirmed
STEP 1, AQI3
Number of attendances at key stakeholder events
TBD To show a year on year increase in the amount of appropriate events attended.
This AQI under development.
STEPS 1-5 Core Requirements CR1 CR2 Health & Care Standards Governance, Accountability & Leadership Individual Care
Time taken to respond to concerns
Please see above.
Strategic Aim 6: Highly Effective Organisation
Financial and Governance Indicators
Statutory Financial Duty
Breakeven Duty Breakeven Breakeven over rolling three-year accounting period
To ensure that revenue is not less than sufficient to meet outgoings properly chargeable to revenue account in respect of each rolling three-year accounting period

76
Indicator Type Reference Measure Performance Improvement Ambition Comment
Baseline Year 1 Year 2 Year 3 Beyond
Creditor Payments: Welsh Government Target
Creditor
Payments to non
NHS creditors
based on the
number of bills
within 30 days of
delivery or receipt
of a valid invoice
whichever is
sooner
98% At least 95%
Of non-NHS bills
paid within 30 days
At least 95%
Of non-NHS bills
paid within 30 days
At least 95%
Of non-NHS bills
paid within 30 days
Target 95%
Administrative Financial Duties
To remain within
External
Financing Limit
(EFL) for the
Trust
Within EFL Within EFL
Within EFL
Within EFL
STEPS: STEP 1-5 Core Requirements: CR1 Health & Care Standards: Governance, Accountability & Leadership
Risk Management Strategy & Framework Movement along the risk maturity pathway.
Risk Aware 2015/16
Risk Defined 16/17
Risk Managed
17/18
Risk Enabled
18/19
External Audit rates: Substantial Assurance External
Audit rates: Substantial Assurance
Definitions: Risk aware: Scattered silo based approach to risk management. Risk defined: Strategy and policies in place and communicated. Risk managed: Trust-wide approach to risk management developed and communicated .Risk enabled: Risk management and internal control fully embedded Trust wide The Wales Audit Office Structured Assessment of WAST (December 2013) concurred with the findings of the internal review and included the 7 key recommendations as part

77
Indicator Type Reference Measure Performance Improvement Ambition Comment
Baseline Year 1 Year 2 Year 3 Beyond
of the assurances that the Trust was moving forward in terms of governance & risk management. The Strategy is the output of the review.

78
3.6 Developing a Frontline-Led Approach to Planning
As an organisation, we recognised that our approach to planning needed to be stronger. This focus on a more rigorous approach to planning saw the appointment of a new Director of Planning and Performance and the subsequent strengthening of Planning Directorate capacity. A further facet of taking a more robust approach to planning within the organisation has been the introduction of local planning across the organisation. The requirement is for all aspects of the organisation to develop local delivery plans (LDPs) which clearly articulate what that part of the business will deliver in the coming period and how those key deliverables contribute to the corporate aims and priorities. An overview of the key deliverables (KD) in each of the service LDPs are shown below in Figure 14. There is variation in these key deliverables to reflect local (e.g. LHB footprint) context, pressures and opportunities. Delivery will largely be tracked through Performance Reviews with organisational delivery units.

79
FIGURE 14: Operational LHB-WAST Area Key Deliverables Strategic Aims
Best Possible Patient
Outcomes And
Experience
Engaged And Skilled Workforce
Manage Capacity To
Meet Demand
Reduce Unnecessary
Variation
Strong Partnerships
Highly Effective
Organisation
Abertawe Bro Morgannwg WAST operational area
KD01 Develop alternative care pathways x x
KD02 Improve job cycle efficiencies x x x x x x
KD03 Develop staff/community engagement x x x
KD04 Patient Care Services (NEPTS project) x x
KD05 Develop our teams and staff x x x
KD06 Support the wider health community on service reconfiguration
x x x x
KD07 Ensuring a focus on quality of care x x x x
KD08 Workforce planning and capacity x x x
KD09 Resilience/business continuity planning x x x
Aneurin Bevan WAST operational area
KD01 Strengthen approach to communication and engagement
x x x
KD02 Performance management across and down our structures
x x x x
KD03 Develop alternative care pathways x x x x
KD04 Improve working with Trust support services x x
KD05 Ensure effective rosters and workforce capacity x x
KD06 Support the wider health community on service re-configuration
x x x x
KD07 Ensuring a focus on quality of care / demand management
x x x x
KD08 Resilience/business continuity planning x x x
KD09 Develop our teams and staff
x x x

80
FIGURE 14: Operational LHB-WAST Area Key Deliverables Strategic Aims
Best Possible Patient
Outcomes And
Experience
Engaged And Skilled Workforce
Manage Capacity To
Meet Demand
Reduce Unnecessary
Variation
Strong Partnerships
Highly Effective
Organisation
Betsi Cadwaladr WAST operational area
KD01 Increase the availability of alternative care pathways
x x x x x
KD02 Ensuring a focus on quality of care x x x x x x
KD03 Improve the delivery of Patient Care Services x x x
KD04 Workforce planning and development x x x x
KD05 Improve job cycle efficiencies x X x x x x
KD06 Further develop Community First Responders and Public Access De-Fibs
x X x x x
KD07 Supporting sustainable change x x
KD08 Staff/staff side and public and community engagement
x X x
KD09 Resilience and Special Operations X x x
KD10 Infrastructure development x X x x x
Cardiff & Vale WAST operational area
KD01 Clinical Priorities as agreed with the LHB x X x x x x
KD02 Workforce planning/HR/Health & Well-being in partnership
x X x x x x
KD03 Performance management across and down our structures
x X x x x x
KD04 Financial budgeting/savings x X x x x x
KD05 Partnership working/co-production x X x x x
KD06 Resilience/business continuity planning x X x x x x
KD07 PCS/NEPTS x X x x x x
Cwm Taf WAST operational area
KD01 Maintain & transition the “Explorer project” pending outcome from UHB/WAST Exec Team
x X x x x

81
FIGURE 14: Operational LHB-WAST Area Key Deliverables Strategic Aims
Best Possible Patient
Outcomes And
Experience
Engaged And Skilled Workforce
Manage Capacity To
Meet Demand
Reduce Unnecessary
Variation
Strong Partnerships
Highly Effective
Organisation
KD02 Developing our workforce x X x
KD03 Agree medium term solutions to Cwm Taf infrastructure needs
x X x
KD04 Clinical governance and quality x X x x x x
KD05 Develop, refine & re-launch alternative care pathways
x X x x x
KD06 Communication & engagement x X x
KD06 Performance management across and down our structures
x X x x
Hywel Dda WAST operational area
KD01 Improve job cycle efficiencies x X x X x x
KD02 Workforce (planning & development) X x x
KD03 Infrastructure (Fleet & Estates) x x
KD04 CFR & PADS x x x
KD05 Engagement (in partnership with staff / public / Health Board)
x x x
KD06 Improving the quality of care x x X x x
KD07 Business planning x x x x
KD08 Patient Care Services x x x
KD09 Equality x X x
Powys WAST operational area
KD01 Reduce lost hours (job cycle efficiencies) x x x X x x
KD02 Patient disposition – develop alternative care pathways
x x x
KD03 Effective utilisation of resources x x x x
KD04 Workforce plan x x x x
KD05 Community and public engagement x

82
FIGURE 14: Operational LHB-WAST Area Key Deliverables Strategic Aims
Best Possible Patient
Outcomes And
Experience
Engaged And Skilled Workforce
Manage Capacity To
Meet Demand
Reduce Unnecessary
Variation
Strong Partnerships
Highly Effective
Organisation
KD06 Operational management capacity x x
KD07 NEPTS x x x
KD08 Estates x x
KD09 Business continuity x x x
KD10 Equality x x x
Resilience
KD01 PREVENT training (counter terrorism) x
KD02 Tier one multi-agency exercise x
KD03 Commander competency training and roll out of national occupational standards
x
KD04 Reconfigure equipment on national resilience vehicles
x
KD05 Staff engagement, introduction of TRiM, continuation of PDR and 1:1 processes and ongoing development of HART 2/ICs
x
KD06 Complete re-write of the Trust’s major incident plan to meet best practice
x
KD07 Second stage of rolling out the LiD system for operational debriefing across the Trust
x x
KD08 Substantive resilience manager for South Wales and Gwent LRF areas
x
Patient Care Services (Non-Emergency Patient Transport)
KD01 Full implementation of PCS management structure x x x X x
KD02 Workforce development x
KD03 Increased flexibility of service x x
KD04 Engagement and effective communication x x
KD05 Implement enhanced service x x x

83
FIGURE 14: Operational LHB-WAST Area Key Deliverables Strategic Aims
Best Possible Patient
Outcomes And
Experience
Engaged And Skilled Workforce
Manage Capacity To
Meet Demand
Reduce Unnecessary
Variation
Strong Partnerships
Highly Effective
Organisation
KD06 Maximise the utilisation of the CLERIC system x
KD07 Reduce abortive journeys X x x
KD08 Fleet x x x
KD09 Resilience planning x
KD10 Governance and audit x x These Key Deliverables are complemented by and align to our “Treating People Fairly – Strategic Equality Plan” and the area-specific priorities. They will be tracked as a package of activities through the Performance Management Framework arrangements.

84
3.7 Becoming a Leading Ambulance Organisation: Where Do We Want to be in 5 – 10 years?
Our work on revisiting our purpose and vision exposed a strong appetite for more ambitious and
strategic visioning and planning for our services. The discussion has commenced in earnest with
the Executive and Non-Executive members of our Board.
The culmination of this is anticipated to be a new strategy for ambulance services in Wales that will
be developed during the lifetime of this plan.
Action 6: The Development of a long-term strategy for ambulance services in Wales
Our statement of intent:
A “strategic statement of intent” is emerging. The thinking is congruent with the strategic report
developed by the Association of Ambulance Chief Executives (AACE) “A Vision for the Ambulance
Service 2020 and Beyond”, and further work will be done to explore and test some critical lines of
enquiry and a route map, agreed with partners, to develop a new strategy agreed.
Our strategic narrative will be further informed by the new NHS Wales strategic publication,
expected in the wake of a new Government post May 2016.
Notwithstanding the further work required, there are a number of strategic themes where there is
emerging consensus and a clear view. We are describing this via our “Strategic Statement of Intent”
and a series of statements describing our future state.
Our Strategic Statement of Intent: In 5 – 10 years, WAST will have successfully:
moved away from a response and treatment provider towards an urgent and emergency
mobile healthcare service offering a wide range of skills and expertise for clinical decision-
making, supported by a range of options and alternatives for referral and/or advice;
proven ourselves to be an ambulance service employer of choice, with established and
respected credentials in our clinical outcomes for patients, our patient experience markers,
our responsiveness and our high levels of staff satisfaction. We will be able to recruit, retain
and develop our staff, and will have in place a structured career pathway which will include
apprenticeships. We will have a flexible workforce that is more representative of the
communities we serve;
proven ourselves to be a great place to work and to belong, with each colleague
understanding what they are trying to achieve and able to be themselves as much as
possible to achieve their goals; we will have high levels of trust, respect, participation and
ownership and will be a role model for public service organisations in Wales and the UK;
become a technology-enabled workforce and service, expanding the interfaces through
which the public can access our services and similarly maximise the benefits of technology
in communication with our staff and equipping them in the field (for example apps for training
through to diagnostic and care support);
made progress towards our vision for Clinical Contact Centres delivering an integrated
health model (across 111, EMS, non-emergency patient transport and other NHS services)
and taken the opportunity to improve and realise benefits from collaboration with our blue
light partners in control centres;

85
recalibrated and strengthened our offer to the primary care system, working effectively with
primary care clusters for both in-hours and the out-of-hours service;
set and delivered our agenda for collaboration with our blue light partners when it has
delivered benefits for patients and the public purse;
developed a fleet that is responsive and agile to demand, taking more care to patients with
vehicles that act as diagnostic hubs, providing a wider range of imaging and testing, either
for interpreting locally by paramedic or to enable results to be electronically sent to
alternative clinicians;
created an environment where patients and staff will see themselves as partners, working
within Prudent Healthcare principles;
established effective collaborative relationships with NHS Wales teams, with opportunities
for cross-boundary working; and
have established ourselves as a provider of high quality teaching, research and innovation.
We will have strengthened strategic partnerships with academic and teaching institutions
and become a Trust with University status.
Where we are less clear on our direction of travel, we will explore the opportunities and benefits,
through engagement and a review of the evidence of the following lines of enquiry. These are not
exhaustive:
re-positioned ourselves into a more central role in the urgent and emergency care system,
confirmed our “offer” to the management and running of Minor Injuries Units for example –
clarified what it means to be system leaders;
explored our role as the navigation route/gateway for urgent and emergency care (in terms
of referral to anticipatory or definitive care);
clarity on our role and offer in the prevention agenda;
defined our model for community resilience; and
challenged our thinking and approach to plan for our workforce in its widest sense – our
staff, our volunteers, and even the public as co-producers of their care.
Whilst this is exciting and inspiring work, we will not allow it to distract us from our commitment to
sustain our current performance and establish some foundations in terms of corporate
infrastructure. Through discussion with our staff, our Board, our Commissioners, our partners in
the blue light, public and voluntary sector and Welsh Government, we will develop a timeline for
unpacking these lines of enquiry. Where this is a clear direction of travel and vision, we will not use
the absence of a fully worked up strategy to delay progress. We will work agilely to test, develop
and implement improvements to the system.

86
PART 4: QUALITY AND PRUDENT HEALTHCARE This section sets out our ambition to put quality at the heart of our plans. It sets out the practical steps we are taking to move towards our vision and covers:
Listening to our patients and the public
Quality themes and improvements for 2016/17 and beyond
Quality improvement, measures and assurance system
Quality governance
Quality underpins all elements of our plan. Providing good quality clinical services is paramount but
applying the quality and prudent lens to all of our service, including non-clinical services, is critical.
For example, delivering a quality fleet service or ICT provision is essential to the overall delivery of
our ambitions. Additionally, we recognise the value to patients and to the healthcare system of
adopting a prudent approach to the delivery of our services. By placing better outcomes for patients
at the heart of our operating model, the Trust is embedding the principles of prudent healthcare at
the very centre of the organisation and is building firm foundations for the future. Our commitment to
quality is also central to Treating People Fairly.
We are committed to putting patients, service users and carers at the centre of everything we do,
engaging and listening to those who use our services to inform quality improvement. The Health
and Care Standards (2015) set the framework of our Quality Strategy 2016/19 and focus on the
delivery of safe and effective care, achieving excellent patient/user/carer and staff experience and
supporting the implementation of this Plan.
The Quality Strategy 2016/19 was approved at the Trust Board meeting in March 2016 (a priority
from our 2015/16 plan). It was developed during 2015/16 from triangulation of local and national
data and patient/user/staff feedback and aligns with the requirements set out in Achieving
Excellence - Quality Delivery Plan for the NHS in Wales 2012-2016 and Safe Care, Compassionate
Care, the National Governance Framework to enable high quality care in NHS Wales (2013).
Following the consultation period during September 2015, the Strategy was revised to reflect
feedback themes and was approved at the Quality, Experience and Safety (QuESt) Committee in
February 2016. The Strategy incorporates the learning from internal assessments and
local/national reports including the Abertawe Bro Morgannwg University Health Board “Trusted to
Care” report and the Francis Report (2013) reviewing the care delivered at Mid Staffordshire NHS
Foundation Trust. The Francis Report identified five key themes, underpinned by the requirement
of a fundamental quality improvement culture and the adoption of common values across
organisations focusing on:
fundamental standards;
openness, transparency and candor;
compassionate, caring and committed staff;
strong, patient-centered healthcare leadership; and
accurate, useful and relevant information.

87
4.1 Moving Forward 2016/19
Developing through engagement and improving through continuous feedback.
Feedback from staff, service users, patients, stakeholder and communities has been taken into
consideration and helped shape our areas for improvement across all of our services for 2016/19
and these will be reviewed and refreshed on at least an annual basis. We are fortunate that,
through the work of our Partners in Healthcare Team, we have a significant amount of rich
information from service users, patients and communities.
Our patients and service users have defined ‘quality’ as:
“Confidence to receive a prompt response”
“Providing a prompt response appropriate to the needs of the patient”
“Being able to get medical help as soon as possible and not wait”
“To arrive in good time, administer appropriate treatment”
“Being informed every step of the way, treated with courtesy and professional expertise”
“Help when you need it and the ability to make a patient feel safe when they are at their most
vulnerable i.e. when they are ill”
“Meeting the patient’s needs”
“Assurance that treatment/help will not be compromised”
“Good communication with patient/family”
They have told us that, for when they receive good care it can be characterised as:
Professionalism and caring staff
Excellent service
Kindness of staff
Treated with respect and politeness
Knowledgeable staff
Helpful and reassuring
They have told us they would like improvement in the following areas:
X Hospital handover delays X Longer than expected wait for an ambulance X Waiting times to be picked up for appointments X Long journeys for appointments X Too many asked/repetitive questions on phone X Long wait for a call back
Feedback from staff walkabouts/workshops, staff surveys, engagement events and other
discussions identified the following areas on which to focus our quality improvement work:
handover delays at Emergency Departments and the impact on the quality of care patients receive including delays in treatment, pain relief, continence needs, pressure area care, hydration and warmth and comfort;
Infection Prevention and Control practices with pressures to turn vehicles around quickly;
involvement in shaping the clinical audit programme locally;
time for training and continued professional development including clinical notices, alerts, and new guidance;

88
improving organisational learning and sharing improvements;
reducing waiting times in Patient Care Services and improving patient experience;
improving and simplifying the complaints process;
our clinical team leaders who need time to undertake appraisals and support their staff ;
focusing more on the outcomes of the care they deliver, not just time related measures; and
fleet issues.
4.2 Quality Themes and Improvements
The Trust has adopted the Health and Care Standards (2015) Quality Themes and the NHS Wales
Outcomes Framework to form the basis of our Strategy, whilst considering the principles of Prudent
Healthcare. Following public and staff consultation, the Trust’s first Quality Strategy 2016/19 was
approved by the Trust Board in March 2016 and supports the implementation of the IMTP. The
strategy is a detailed document breaking down our aspirations over 2016/19 across the Quality
Themes. This document is publicly available on the Trust’s internet site.
Quality and quality improvement is embedded throughout the whole of our plan across all services
including the implementation of the new Clinical Response Five-Step Model and Non-Emergency
Patient Transport. In addition to the actions included in other elements of this IMTP supporting
quality improvement, we have identified the following key areas of action:
Infection, Prevention & Control (IPC):
Action 7 Strategic oversight of the implementation of the Infection Prevention and Control
(IPC) two year operational plan; this will include monitoring of staff immunisation
rates with Occupational Health.
Action 8 Auditing of peripheral vascular cannulation rates.
Action 9 Implement a task & finish group to address vehicle cleaning Trust-wide.
Developing quality measures & a quarterly quality assurance report:
Action 10 To commence from April 2016, a quarterly quality assurance report triangulating
intelligence (qualitative and quantitative) to make sustainable improvements at
corporate level 2016/17 including our own locally determined quality measures
aligned to the Core Requirements and national mandatory targets and measures.
Action 11 Review the capability and development requirements of the Trust’s risk management
information system, Datix, to support the development of our monthly and quarterly
reporting, heat mapping and early warning systems.
Action 12 Undertake an internal assessment against progress with the Health & Care
Standards (2015) for 2016/17.
Safeguarding adults, children, domestic abuse & PREVENT
Action 13 Development of a training strategy to meet legislative requirements including
PREVENT.
Action 14 Implementation of the safeguarding review outputs.
Board to Floor to Board
Action 15 Develop programme for walkarounds and feedback mechanisms.

89
Other key areas
We will work with the Older People’s Commissioner and Ageing Well in Wales National Programme
to ensure we deliver quality care to older patients and those with a specific need including
dementia, sensory loss, falls, continence care and learning disabilities. Partnership working to
establish good practice on learning disability care bundles, learning and appropriate
training/education of staff across the Trust will also be undertaken. This links with Section 5, STEP 5
of the plan regarding our further development of alternative care pathways.
Action 16 Implementation of our accreditation plan to be a Dementia Friendly organisation.
Action 17 Work to achieve Bevan Advocate status by August 2016 and Bevan Exemplar status
by August 2018.
4.3 Quality Improvement, Measures and Assurance System
Quality assurance is provided through our improving compliance with the Health and Care
Standards (2015), which have informed our Quality Strategy and key improvement priorities. We
will develop our key quality indicators and measures to complement national mandatory targets and
these will be at Trust level initially, then Health Board level with the aim of then developing locality /
station level measures with staff relevant to the communities they serve across the life of this plan.
These will then provide a framework for continuous monitoring and measurement. The image below
provides an overview of our whole systems approach to quality, improvement and assurance.
The development of our quality measures will consider the balance of the data to include the
structure of key services (number of people accessing our services), how key processes are
working (how many people received all of the care they should have received) and the key
outcomes that signal safe, effective and efficient services. Data collection at the Trust will be further
enabled through the use of Digi-pen technology with the Partners in Healthcare team engaging with
patients, service users and communities to obtain feedback on all of our services.

90
Currently the Trust uses some quality triggers including concerns, patient/service user/staff
feedback, clinical audit data and performance and clinical indicators. However, we recognise the
need to develop quality measures as detailed above and to use our information more intelligently
through triangulation, heat mapping and early warning systems developing this over the life of this
plan.
Key questions are applied when triangulating the information from a variety of sources to consider
the dimensions of quality to demonstrate that we are actively listening and learning.
Are we providing safe care?
Are we meeting required standards of effective care?
Are we improving user experience?
Are we providing efficient services within our resources?
Are we engaging with the workforce?
Are we providing accessible and equitable services?
Are we improving population health?
4.4 Quality Improvement and 1000 Lives Improvement
The 1000 Lives Improvement Service and Health Board/Trusts across Wales have built national
improvement priorities into their three year integrated plans. The 1000 Lives Improvement Service

91
(part of Public Health Wales), Health Boards and NHS Trusts in Wales have agreed a set of national
priorities for improvement in their integrated plans:
improving patient flow;
reducing inequalities (long-term condition management and end-of-life care); and
Improving Quality Together – Model for Improvement.
The Trust is fully engaged with the 1000 Lives Improvement Service and recognises quality
improvement draws on a number of approaches and tools and fundamentally means reducing or
removing waste and variation in the system. This includes reducing delays and waiting times and
ensuring care is equitable across Wales.
The Trust has adopted the Model for Improvement and is working with colleagues in 1000 Lives
Improvement Service to implement a senior quality improvement team with Silver Improving Quality
Together accreditation.
The Trust recognises that, in order to implement sustainable quality improvements, firm foundations
must be in place including good governance with robust reporting systems and a culture of
openness and transparency.
4.5 Quality Governance
Quality governance is the combination of structures and processes at and below Board level to
identify and act upon Trust-wide quality performance which includes:
Ensuring required standards are achieved;
Investigating and taking action on sub-standard performance;
Planning and driving continuous improvement;
Identifying, sharing and ensuring delivery of best practice; and
Identifying and managing risks to quality of care.
The Board has overall accountability for the quality of services provided by the organisation. The
Quality, Experience and Safety Committee (QuESt), as a sub-committee of the Trust Board, has
delegated responsibility for all matters relating to the quality of care we provide. QuESt has a
number of sub groups supporting our quality agenda and these are detailed in our quality
governance committee structure.
Providing assurances to the public and Trust Board is a fundamental element of this Plan and, to
deliver this, we have developed supporting local delivery plans for 2016/17 and an assurance
framework which will be monitored at the Quality, Experience and Safety Committee (QuESt) on a
quarterly basis. Following each meeting of QuESt, an update will be provided by the chair to the
Trust Board through the Trust’s reporting and escalation routes.

92
What will success look like?
1 We will be a clinically led, quality driven organisation adopting the principles of Prudent
Healthcare.
2 We will have effective leaders and our staff will be developed and supported to deliver
high quality care, in a high performing organisation that staff are proud to be part of and
feel valued.
3 We will have made demonstrable improvements for our service users across all of our
services, with sustainable quality improvements aligned to key performance indicators,
measures and targets supported by our research & innovation work.
4 There will be clear lines of reporting and escalation routes with the Board receiving the
right quality assured information, in a timely manner in a format that allows the Board and
Executive Team to make informed decisions about the quality of the services we provide.
5 We will have good governance and risk management foundations in place that provide
confidence in our systems to support decision-making, planning and quality delivery.
6 Staff will be engaged and will shape our priorities and know why they are important. We
will continue to work in partnership, fostering productive relationships.
7 Quality indicators at station, contact centre and Health Board level will be developed by
staff locally, relevant to the local population / service needs.
8 Service users, our communities, partners and stakeholders will be engaged in shaping our
goals and priorities on a continual basis.
Risk Management Strategy and
framework 2016/19 focuses on managing
the risk associated with providing our
services.
Quality Strategy sets out our quality objectives and commitment to quality improvement.
Assurance providing confidence the
organisation is delivering the objectives.
Quality led organisation with foundations for delivering quality Together they put quality at the heart of the Board’s work

93
9 Our commissioners and other stakeholders will have confidence in our services and we
will be striving to drive quality improvement through the commissioning process.
10 We will be a credible ‘go to’ organisation.

94
PART 5: OUR SERVICE CHANGE PLANS This section, along with Part 6: Our Enablers, represents the heart of our plan. Taking our strategic aims, and subsequently our priorities for this plan, we are now able to focus on the key service areas in which we will be investing our change capacity and resources, along with the specific actions that we intend to deliver upon over the next three years. Further details regarding each action documented can be found in Appendix 6
The organisation is taking forward four major ‘flagship’ service changes as part of transforming the
organisation. These can be clearly linked back to our overarching strategic aims.
Embedding and sustaining the New Clinical Response Model
Transforming and modernising our Clinical Contact Centres (CCCs)
Implementing the agreed new model for Non-Emergency Patient Transport
Supporting the implementation of the 111 Pathfinder Project with NHS Wales partner
organisations.
Delivering on our priorities and realising our proposed service changes identified above will require
the successful execution of a number of related actions and activities.
The impact of these actions will be measured through the Ambulance Quality Indicators and show
incremental improvement towards our stated performance ambitions as per Figure 13 in Part 3.
The remaining section of this plan describes those activities and places them in the context of the
five step model. Some of the actions documented have been agreed with (or are being proposed
to) our Commissioner to receive specific funding. Where this is the case, a CAREMORE® template
has had to be produced and submitted to the CASC’s office as part of the agreed commissioning
process. In order to easily identify these actions, they are labelled with the “CAREMORE®” symbol.
When settling upon the appropriate actions, consideration was given to the fact that the CRM pilot
only runs until September 2016, at which point there will need to be an evaluation. Coupled with the
further work required on a demand and capacity model, these two key activities will help to shape
the focus and priorities for years two and three. The organisation was cognisant of the fact
therefore that it has 6-9 months to provide assurance that this model is working and should
continue. Consequently, whilst this is a three-year plan, many actions have a real focus on year 1
to ensure the model’s operational life is extended but also recognising that it is problematic to plan
for years two and three with uncertainty surrounding the continuation of the model beyond
September 2016.

95
To deliver the five-step New Clinical Response Model, there will need to a cultural shift in the way
that the public access our services, which will require a change in service user behaviour.
This step is where we address our contribution to the public health agenda, recognising that whilst
we have a positive contribution to make, we will need to work across NHS Wales and with partners
to deliver a step change. Engineering this shift in behaviour will require a strategy. We intend to
engage with Public Health Wales on the development of this strategy. We are not starting from a
zero base, we already have work underway that will roll up into this strategy. For example it will
reflect the work we are doing to:
further develop the NHS Direct Wales website in response to feedback form our
communities;
closer working with partners organisations to support the Choose Well message and using
WAST wisely;
continued development of information through media mediums; and
providing additional symptom checkers to enable people to manage their health and be well
informed to choose appropriate services.
In support of this strategy, our Partners In Healthcare team will identify whether service users are
accessing any alternative services and pathways before calling 999 and, if not, the reasons why.
Through this work, we will take every opportunity to influence the work of and get support from any
national work underway or initiated as part of the “Prudent Patient” response to the Prudent
Healthcare Action Plan.
Action 18 Develop a longer term ‘Help Me Choose’ strategy.
Improving our response to frequent callers (FC) has demonstrated a reduction in the number of calls
received and ambulances dispatched. It is also managing individual patient need better through the
partnership work we have undertaken with GPs, specialist services, police and local authority
partners. This multidisciplinary approach has, however, identified unmet healthcare needs and
patient behaviour via the 999 system, which the wider NHS system was unaware of. Through this
work, we are continuing to use our unique position as the only 24-hour national provider of
emergency care in Wales, to benefit patients and NHS Wales.
Applying the National Frequent Caller definition, this work will continue to apply to all individuals
who regularly call 999 but extending the scope to include callers from:
residential homes and nursing homes – this work will include working with LHBs to address
known problems such as non-injury fallers; and
the Police Service.
Action 19 Demonstrate effective management of Frequent Callers (FC), who impact upon the 999 demand, in each Health Board Area. A 2015/16 CAREMORE® action.
STEP 1: Help me choose
This step focuses on public education regarding the services provided by
WAST and how/when to access them appropriately.

96
This step also has implications for our workforce planning and development. Achieving a step
change in behaviours will require staff to have the necessary skills to be able to educate and inform
the public at every appropriate contact. There will be an opportunity to strengthen the management
of local Community First Responders so they become the local community experts, particularly in
rural areas. It will be important that our staff understand the needs of their communities so that they
are able to help people in Wales make the best possible choices. This is likely to mean proactive
positive action with some communities to ensure that our workforce is more diverse and
representative. In planning for our future workforce, we anticipate opportunities for our more
experienced staff to undertake educational roles on a more frequent basis.
Clinical Contact Centres (CCCs)
CCCs are the centre of the entire WAST operation, making it one of the highest priority areas for
improvement, with some of the biggest returns to be made in regard to efficiency and effectiveness
of EMS. Performance is dependent on the front end (CCCs) getting it right, and this requires
appropriate systems to support staff to deliver the best outcomes for patients.
The long-term success of the new CRM is also in part dependent upon the transformation of the
organisation’s CCCs.
This means that there are significant implications and opportunities for our CCC workforce in the
future, particularly as we seek to re-profile the workforce to increase our capacity and capability to
help respond to a growing demand in activity resulting from the increasing frail and elderly
population in Wales.
CCCs deliver a call answering, assessment and triage service and a dispatch of vehicle service to a
population of 3.3 million making 1200 “999” calls every day. Two elements of clinical assessment,
information and advice services are hosted within CCCs: NHS Direct Wales and Clinical Support
Desk (CSD). The CSD reviews more than 2000 patients each month to ensure appropriate
utilisation of emergency response vehicles.
CCC staff also work closely with operational colleagues to develop and implement systems-based
processes, providing and delivering new guidelines, procedures and policies associated with remote
telephone assessment practice. This work is currently prioritised alongside the 111 pathfinder
project, for which the team is leading on the clinical development of an updated Clinical Assessment
System (CAS).
The Emergency Medical Services element of call taking is completed on the MIS Alert 2000
Computer Aided Dispatch system (CAD). Most ambulance services in the UK have moved on from
this system and therefore we are not realising the operational effectiveness and productivity benefits
STEP 2: Answer my call This step focuses on the response to 999 and Health Care Professional
(HCP) calls by WAST’s Clinical Contact Centres (CCCs). This step
incorporates the provision of adequate time to assess a call and the use of
the Medical Priority Dispatch System (MPDS) to identify the priority of the
call before offering / sending the most appropriate response.

97
that we could. The key determinants of CCC performance are infrastructure (telephone, CAD etc),
capacity, management processes and culture. The plan for our CCCs reflects all of these
components, more detail can be found in the CCC Local Delivery plan.
Performance management processes are being tested and realigned to the New Clinical Response
Model, utilising “signals from noise” software from Lightfoot, a commercial company.
The demands on the service exceed the available capacity at certain times of the day because of
historical working patterns which do not necessarily support the varied, unscheduled nature of the
activity presenting to the service i.e. CCCs rely on overtime to bolster up our peaks in demand
which is not always possible; the highest risk is currently in Call Taking.
The Clinical Support Desk’s (CSD) function has changed on a number of occasions since inception
in December 2014. Since the New Clinical Response Model, the benefits of enhanced triage and
Hear and Treat have meant that there is a requirement to review the current system and ensure that
governance-led triage processes support staff, along with regular clinical supervision.
CCC is a high risk area in terms of business continuity and resilience. There is a requirement to
further train and update all teams on business continuity, whilst maintaining day-to-day operations
and continuing to test existing plans.
Risks with the current approach have been identified and the successful mitigation of these risks
has, and continues to, allow the EMS element of CCC to operate with minimal operational risk whilst
a new CAD is procured and implemented. Changing the culture of EMS to one that is performance
and patient-focused has enabled some performance improvement and this journey of development
will continue.
Much of the mitigation has focused on increasing the establishment of the CCC workforce. For
example, in the clinical desk, the organisation is currently unable to maximise its “Hear and Treat”
because of three potential clinical queues and a difficult manual process to accept calls for a
clinician. Recruiting an allocator on the clinical desk will allow work flows to be more effectively
managed whilst also providing a point of contact for the coordination of inter-CAD incident transfers.
The actions detailed below demonstrate a coherent and phased approach to strengthening our CCC
function.
2016/17 (Year 1)
With the two major change projects for the organisation completing in year one of this plan (the end
of the CRM pilot and the procurement and potential full implementation of a CAD) there will be a
major impact on the EMS CCC.
There will be the need to deliver considerable training to all EMS staff and, therefore, abstraction
rates will be high.
Any new structure is also highly likely to require changes in rotas for all EMS staff, as well as
training with potential role movement with some staff groups.
Consequently, the main drivers and areas of focus for the CCC in year one of this plan will be:
supporting the procurement and implementation of a new CAD;
restructure of all staff group rotas and roles (in line with organisational change policies);

98
embedding the New Clinical Response Model pilot following completion of the pilot;
embedding the national systems delivered into normal practice with a new staff structure fit
for purpose;
supporting staff through the journey of change, ensuring frequent communication and
support to individuals who need it; and
ensuring a robust framework of engagement of staff representatives within the
transformation project.
Action 20: Continue to mitigate current risks associated with CCC service provision. Action 21: Clinical and functional development of Clinical Assessment Software and supporting
processes Action 22: Undertake a review of the Practice Coach title, role and banding Action 23: Procurement and Implementation of a new Computer Aided Dispatch (CAD) System
Recognising limitations of the current CAD identified but also the importance of improving our “Hear
and Treat” rates means that we plan to recruit an allocator to the clinical desk, who will develop and
manage a clinical queue for appropriate “Hear and Treat” calls, to include non-injury falls. The
potential for expansion of the Clinical Desk, including the clinical support to non-clinical staff in the
CCC, will also be reviewed and scoped.
Action 24: Increased Hear and Treat services through the Clinical Desk.
A 2016/17 CAREMORE® action.
We want to ensure we allocate an appropriate response for non-injury falls through clinical
telephone assessment with appropriate referral and dispatch of ideal ‘Face to Face’ resource, if
required. We will link this work to the Aneurin Bevan Health Board and WAST Falls response project
Frequent Caller work.
Action 25: Implement appropriate service provision for non-injury falls.
Action 26: Implement the findings of Consultancy “Lightfoot” baseline review of the Clinical Contact Centres patient call cycle
2017/18 (Year 2)
Following the introduction of new CAD and staff structures, year 2 of this plan will entail embedding
a performance management framework into the new staff teams to deliver performance
improvements.
We recognise that status planning processes in WAST are not yet best practice and that the new
CAD will likely go live on the existing methodology but with better technology. Following introduction
of the new CAD, we will need to complete a review of all dispatch points, engaging with the
operational areas and reviewing zones and priorities. We may also take the opportunity to move to
a more appropriate planning system that meets the outcomes of the New Clinical Response Model.
Quality of call handling will be addressed through achieving accreditation to Priority Dispatch ‘ACE’
qualifications. This is an aspiration for the Trust: we will not be able to deliver it until we have
completed the main CAD project with its associated training plan.
Main targets and plans for year 2 will thus be:
99
performance management embedded in staff structures and aligned to organisational shared
behaviours;
status planning; and
ACE accreditation.
We anticipate the plans outlined above will increase our workforce numbers by approximately 23.5
WTE, factored into our financial plan for 2016/17. Any additional resource required will need to be
assessed as part of the developing CAD business plan. Our financial plans and templates will
reflect year 1 numbers, but not year 2 and 3 at this stage pending further analysis and completion of
the demand and capacity work.
Our vision for our service model for CCCs influences our estate plans. We want to create an
integrated health model. This will include EMS and NEPTS control, Clinicians, NHSDW (111) and
GPOOH services. We will also explore the opportunity to work with Health Boards around the
potential to include other jointly beneficial roles within the environment of the CCC, for example
specialist mental health practitioners and bed management operations.
Alongside this is the very important aspect of tri-service control rooms across Wales. We remain
committed to working with fellow emergency services partners and firmly believes the integrated
health model and tri-service are not mutually exclusive; we can achieve both. More information
regarding potential CCC estate reconfiguration and how we will deliver this can be found in our
estate section, part 6.3 of this plan.
111 Service
It is generally recognised that the unscheduled cares system is difficult to navigate and often results in patients taking the easiest and most easily accessible route into our health services. Welsh Government policy over the last few years has reaffirmed the importance of helping people navigate what is often seen as a complex health system.
A Welsh 111 Service has the potential to be a vital service to help people with urgent care needs get the right advice in the right place, first time.
The Welsh Government’s Manifesto Commitments (2011) were clear that an introduction of a 111 system should:
build on the success of NHS Direct and offer a single number for accessing out of hours health care in Wales; and
ensure all out of hours services are provided by the local NHS.
The intent is to collectively deliver functionally-integrated urgent care that is the ‘front door’ of the NHS and provides the public with access to urgent care advice, support and treatment.
We were selected as the organisation to host the initial 111 Pathfinder which will incorporate ABMU Health Board and the Carmarthenshire area. The Pathfinder will be evaluated before a decision on further roll out is considered by Welsh Government. An evaluation partner has recently been appointed to support this review and it is anticipated that an interim report will be provided at the mid way point (around October 2016) with a final report due in March 2017.
The 111 Service model has been built up through extensive discussion with key stakeholders. The Welsh model is distinctly different from the model developed in England. In Wales, we want to develop a system that is aligned with prudent health care principles, but also one that can manage complex patients.

100
The design principles underpinning the model are that:
all call taking is provided within the NHS and patients access a service through a single, free-to-call 111 telephone number;
the service is delivered by both non clinical call takers and registered professionals, working in a multi-disciplinary team in line with the principles of prudent health care;
GPs are an integral part of the system and in line with prudent health care, maximising their role and utilising their skills and those of other professionals such as Extended Scope Practitioners to manage complex care; and
the model should proactively support the wider urgent care system.
The service model for the pathfinder has 3 key elements:
call taking – calls will be taken by non-clinical call takers who will be employed within the service. Call takers will use existing call streaming and prioritisation software (called CSPT). Call takers will take initial demographic details and a brief summary of the issue. Call takers will be able to close calls where there is a clear governance framework in place to support this;
clinical telephone assessment – this will be carried out by registered professionals and could include nurses, paramedics, pharmacists, therapists and other staff groups such as dental health advisors. Calls that are assessed as ‘urgent’ during the GPOOH period will continue to be routed for GP triage by the ABMU OOH service. The data demonstrates that up to 2/3rds of calls are classed as ‘less urgent’ and these are the calls where we anticipate other professionals will support these calls in line with prudent health care principles; and
Clinical Support Hub – the clinical support hub will supplement the core clinical telephone service by providing expertise in the management of patients with complex issues. The hub will be staffed by experienced decision makers using their expertise and professional judgement.
Demand and capacity modelling has been undertaken as part of the planning for the pathfinder. The implications from a workforce perspective (i.e. numbers of additional WTE required are outlined below:
Staff Group ABMU Pathfinder
Carmarthenshire Total
Call Handlers 13.24 4.33 17.57
Nurse Advisors
15.07 4.93 20.00
These calculations were based on:
current activity within GPOOH services plus a growth factor of 20% (based on 2014 data);
average call length times : o For call taking 480 seconds (plus 60 seconds hold time for initial six months of
pathfinder); and o Nurse call lengths of 900 seconds per call for normal activity and 1500 seconds for
GREEN 3 (calls transferred from ambulance service);
priority 1 calls routed to GP OOH service (equating to a third of total call volume) and all other calls progressing through nurse triage or via Clinical Support Hub; and
planned shrinkage levels set at 35.10% for nurse advisors and 32.85% for call takers.
Recruitment to these posts for the initial phase of the pathfinder (ABMU) has been successful.

101
Demand and Capacity – All Wales
An initial assessment of the likely demand if the service were to roll out nationally has also been undertaken.
If the pathfinder demonstrates an increase in call volumes as a result of the free telephone number being widely available, the All-Wales service may need to have capacity to handle up to 1m calls when fully rolled out. This would require a significant increase in call centre capacity over and above the current service, which is currently handling circa 250k calls per annum. Given constraints on the physical infrastructure this will require more innovative options to be considered which could include:
a ‘hub and spoke’ model whereby a central service is supported by regional spokes at a Health Board level. This would offer advantages given that the call profile is distributed unevenly across the 24 hour period, with significant surges in call volume during the early evening period and at the weekend;
further discussion on the New Clinical Response Model and call flow options between 111 and GP OOH services, aligned with the above, where calls are routed to the most appropriate professional (the pathfinder will test elements of this);
remote working to facilitate surge capacity at peak times; and
options that align call flow with other similar services e.g. ambulance delivery – create flexible workforce opportunities.
It is important that this work programme is aligned with the wider strategic modernisation plans that we are considering in regards to our Clinical Contact Centres and their configuration.
The following table provides an indicative assessment of the anticipated workforce requirements using the same methodology as set out above.
Staff
Group NHSDW (core 0845 service)
Funded Establishment
WTE
ABMU WTE
Carmarthenshire
WTE
Pembs/ Ceredigion
WTE
CTU HB
WTE
ABHB WTE
BCU HB
WTE
CVU HB
WTE
Powys WTE
Total WTE
Call Takers
31.78 13.24 4.33 4.89 6.95 11.63 18.89 12.27 5.21 109.19
Nurse Advisors
68.70 15.07 4.93 5.56 7.91 13.24 21.50 13.96 5.39 156.26
As part of the continued development of the pathfinder the service model will evolve, in particular to reflect the delivery of new models in line with prudent healthcare principles:
different skill mix and the introduction of new roles including rotational or joint posts with Health Board (e.g. Band 5 roles and Advanced Practitioners);
stretching the role of call takers to ensure that professionals are being used to their maximum potential;
utilising roles of other professionals such as physiotherapists and pharmacists; and
specialist roles that will help to ensure the delivery of 24/7 service models – some of these will only be possible at scale (e.g. specialist nursing roles, midwives, mental health professionals etc.) which could be delivered through remote working or other innovative options
These opportunities will be enhanced through a new IT system to be procured and available towards the end of 2017/18 which will facilitate improved information sharing across 111 service

102
and other services but also will help to facilitate new working models by offering multi-channel access and facilitating remote working options.
Action 27: Work with the 111 Project Board and team to ensure the successful implementation
of the 111 Pathfinder project in association with ABMU and subsequently the Carmarthen locality. A 2015/16 CAREMORE® action.
Part of the modernisation of our Clinical Contact Centres described in STEP 2 above also spans STEP 3. Focused effort on improving this step will ensure that we provide a timely response to immediately
life-threatening calls (RED calls in 8 minutes), AND an appropriate response to AMBER calls. The
actions below highlight some of the key ways we will improve the system. These actions must be
considered alongside the relentless and daily focus our operational staff have, both in CCCs and in
our geographical teams to improve performance, system flow and efficiencies. The Local Delivery
Plans include some detail of EACH area’s specific initiatives.
The demand and capacity review and the NHS Benchmarking toolkit may point to further actions we
can take to improve performance against the AQIs within this step and we will remain open to trying
and testing new approaches.
Healthcare professional calls are our second highest demand category of call. Following 1 April
2016, and the implementation and embedding of the EASC-funded HCP desk model across all
three CCCs, we will work towards rolling this out across Wales so all HCP calls are now captured.
Action 28: Implement HCP desk implementation plan to ensure efficient management of HCP calls at a local and regional level.
It is referenced throughout this plan that the New Clinical Response Model may change the type
and level of capacity required. There is also a need to reduce variation (and increase equity) in the
five-step model. In recognising this, we have recently produced a 2016/17 CAREMORE® Service
Change Idea for sharing with our Commissioner. The aim of the review would be to improve the
management of capacity to deliver a sustained level of performance (this level to be agreed) across
all LHBs and also help inform our organisational workforce and fleet strategies. This approach of
external capacity reviews has been adopted in many ambulance services throughout the UK.
This capacity review would be undertaken in phases and phase 1 of the review would be to
establish:
if we are going to send the ideal response to each incoming 999 call, how many of each type of resource do we need by hour of the day and by location? (This will tell us where we need, who, at what time);
STEP 3: Come to see me This step focuses on how WAST makes decisions about what resources to dispatch to assessed/prioritised calls and the timeliness and appropriateness of our response

103
given our current WTE by skill grade, what this means for numbers of paramedics, EMTs, UCS staff and CCC clinicians; and
the amount of cover we need per day to meet our A8 target and provide a safe service.
A full specification of this, and future phases of the review, is being drafted.
Action 29: To agree a full specification for, and subsequently undertake, a demand and capacity review.
The Demand and Capacity review must deliver an analysis of:
1. Call volumes – current and future.
2. Demographics.
3. The current operational context including handover delays at hospital.
4. Seasonal and special event demand patterns.
5. The ambition to increase the Trust’s A8 performance target to 70% and then 75%.
6. The requirement to release Clinical Team Leader staff from core operational rotas for 20, 50
or 100% of the time.
The Trust requires modelling in relation to the type and optimum location of its resources required in
light of the findings of 1-6 above. This modelling must advise the Trust on:
1. Optimum dispatch locations - fixed and standby.
2. Optimum crew configuration against the New Clinical Response Model.
3. Staffing numbers for “Hear and Treat” services, solo-crewed rapid response and conveying
ambulance resources.
4. Future staffing requirements.
5. The opportunity for use of taxi and non-emergency transport to support EMS.
6. Numbers and locations of Community First Responders.
7. A number of known possible NHS Wales reorganisation scenarios.
In section 2 of this plan, we described the important contribution volunteers make to the organisation and, in particular, the types of Community First Responder (CFR) schemes that the organisation utilises. We recognise that CFRs form a very important component of the resources at our disposal and, whilst they make a very valuable contribution to our performance levels, we want this contribution to be even greater. Our work plan on CFRs links directly to recent Coroner reports recommendations, and whilst we encourage CFRs across all of our communities, their role in rural areas is particularly critical. Reviewing the scope of practice for our healthcare professional CFRs will also be looks at.
To help support CFRs to make an even greater contribution we will, in year one of this plan, finalise
our CFR strategy.
Action 30: To finalise and gain Trust Board sign off of a CFR Strategy Within the strategy, a number of explicit objectives are emerging; these will be progressed over the
life of this plan;
Action 31: Explore and expand where possible the provision of co-responding groups across
Wales (Fire and Rescue Services, Police Services, RNLI, RLSS etc.)
Action 32: Introduce WAST Medical First Responders and ensure appropriate utilisation and
allocation of available equipment

104
Action 33: Introduce explicitly clear and unambiguous formal arrangements in the forms of
Memoranda of Understanding and Service Level Agreements with all parties
responding on behalf of WAST with recruitment, training and clinical governance
embedded within the new proposed structure
Action 34: Introduce a standardised support and accredited training package that is delivered to
all volunteer groups responding on behalf of WAST
Action 35: Introduce standardised equipment for all groups dependent on skill levels
Action 36: Review CFR dispatch/activation protocols for more effective distribution of resources
Many of the above actions represent 2015/16 CAREMORE® actions. We recognise the importance of taking learning from other ambulance services around the UK and, where appropriate, further afield. South East Coast Ambulance Service have successfully deployed a community paramedic model which has resulted in a 15% reduction in conveyance to hospital - 35 fewer patients every day; we are committed to more fully exploring this as a potential model of service provision. Examining this model will allow the Trust to build on the successes of the Cwm Taf Explorer pilot. In Wales, with an integrated health system, this model should work well, further aligning emergency and unscheduled care with secondary care only when required. Action 37: Establish a working relationship with ‘General Practice Clusters’ to ensure that the
Trust develops its future services in line with the needs of primary care.
Action 38: To explore the potential of a community paramedic model in urban and rural area.
STEP 4 (and 5) requires that the most appropriate clinician attend each incident, whether to deal with a life threatening issue requiring urgent transport to hospital or to treat at home (or in the community) and make decisions on the appropriate alternative pathway to care for their patient. There is an increasing demand for our paramedic workforce to be able to see and treat the growing number of frail, elderly patients with chronic conditions and / or mental health issues. This requires an overall up-skilling of our staff to be trained in chronic conditions management, and will be addressed through our training and education plans (further described in section 6.1). At page 43, we noted the Trust had received £60,000 from the Stroke Delivery Plan flexible funds money in 2015/16. This was awarded for delivery of standardised stroke-focused online training to all WAST EMS staff in 2016/17.
Action 39: Delivery of standardised stroke focused online training to all WAST emergency medical services (EMS) staff.
This demand driver may also see an increase in the numbers of staff qualified at a higher clinical level as advanced paramedic practitioners, and band 6 “specialist” practitioners. The demand and capacity work described above will assist us in gaining clarity on the actual impact of this on the
STEP 4: Give me treatment This step focuses on the development and delivery of a range of clinical care services able to offer a variety of treatment options.

105
numbers of Band 5, 6 and 7 staff needed to deliver the New Clinical Response Model, and any consequent opportunities to re-profile the overall skill mix in response to any change. During the life of this plan we will ensure further development of clinical indicators. An improvement plan, aligned with commissioning requirements, will also be developed following each Ambulance Quality Indicator monthly (and quarterly) report.
Action 40: To ensure roll out and development of clinical indicators.
In recognising this step in the New Clinical Response Model, we have also recently approved an
internal clinical equipment business case to ensure our members of staff have the most up-to-date
kit necessary to deliver the care and treatment which that patients need.
Action 41: Implement Digi-pen phase 2
This is key in ensuring we transform from being perceived as simply a transport-based organisation
into being a high quality provider of clinical services, as it enables the development of a suite of
clinical indicators which in turn allow WAST to increase its focus on clinical outcomes and be
clinically-led. This will also include the digitisation of safeguarding referral forms and the creation of
docking facilities at hospitals.
Action 42: Develop and modernise the Trust’s existing medicines management arrangements, by supporting the introduction of the Omnicell automated medicines management system.
At section 6.1 of this plan we describe the importance we place on clinical leadership and the work we want to undertake during this plan to drive forward clinical leadership across the Trust. This work is critical in our reorientation towards being clinically-led and, quality focused and in particular is relevant to this step. Indeed the work we want to progress around end of life care demonstrates what can be achieved when dedicated leads exist for specific clinical areas. We have recently produced a CAREMORE® service change idea for our Commissioner for eight dedicated clinical leads for the following portfolios: trauma/PHEM, cardiac arrest, stroke/TIA, clinical modernisation, mental health, end of life care, sepsis and elderly people who have fallen. The introduction of paramedic leads to cover these eight specialist areas would support our transformation to a clinically-focused service, in particular staff training and development on key clinical developments (cardiac arrest/stroke) and the development of pathways. In addition, the continued development of alternative care pathways will reduce current pressure on emergency departments.
Action 43: Introduce eight dedicated clinical leads for trauma/PHEM, cardiac arrest, stroke/TIA clinical modernisation, mental health, end of life care, sepsis and elderly people who have fallen.
We have also created tools for our paramedic workforce, to support robust clinical decision- making and safe patient care. Paramedic Pathfinder (PPF) has been in clinical practice within the Trust for
STEP 5: Take me to hospital This step refers to patients who require ongoing care and treatment and will be transported to hospital or to alternative care settings (e.g. Minor Injury Unit or a primary/community care facility).

106
12 months. Notable achievements have been made to train all Trust paramedics, implement reporting tools and develop a series of clinical monitoring indicators. All Health Boards were fully engaged during 2014 on the basis that the Trust was moving to this model of face-to-face paramedic triage. Whilst there has been sporadic interest from some unscheduled care partners and stakeholders across health and social provision, there is no national engagement framework in place to support the necessary progress in order to achieve the full benefits of the PPF model. Strong clinical leadership at the patient interface, robust clinical audit and meaningful feedback are imperative to the safe and effective application of PPF in ambulance clinical practice.
Action 44: Embed and sustain Paramedic Pathfinder as a face-to-face triage tool for paramedics
(Paramedic Pathfinder 2)
Pressures on the unscheduled care system are huge and, whilst we are working (and continue to work) closely with Health Board partners, handover delays do exist. Consequently, it is vital that all partners look to reduce the pressure on emergency departments and the wider system..
In response to this, a number of alterative care pathways are proposed during the life of this plan. Their successful implementation is dependent on the continued commitment of all partners.
A ‘Pathway Development’ workstream within the Clinical Modernisation programme is to be
established. This will map pathways currently in place across Health Board areas and use data
from Paramedic Pathfinder to identify gaps and develop priority pathways for implementing across
Wales. Developed pathways will be presented to the Clinical Pathways Advisory and Approval
Group (CPAAG) prior to roll out. This workstream includes roll out of the Mental Health pathway and
development and roll out of the End of Life care pathway, across Wales. Local Delivery Plans show
a focus of joint working on the following areas.
Action 45 - Implement a range of alternative care pathways
Pathway / Health Board Powys ABMU ABHB CTUHB C&VUHB BCUHB HDHB
Mental Health √ √ √ √
Early Adopters (111) √
Acute GP √
Falls / falls vehicle √ √ √
Alcohol treatment centre / city
help point initiatives
√ √
Fractured neck of femur √ √
General hospital admission √ √
Obs & Gynae √ √
Ambulatory Emergency Care √
Community Integrated
Assessment service
√
MIU √ √ √

107
Chronic obstruction
pulmonary disease
√
Stroke √ √
Primary Care Hub √
*Mental health pathways and CCPAG represent 2015/16 CAREMORE® actions.
The choice of proposed pathways to implement has been based on the top reasons for 999 calls
and the groups of patients that were identified as regularly being discharged from ED after tests with
no treatment.
Decisions will also be based on an assessment of local Health Board area need via the close
working relationship of our Heads of Operations and their Health Board counterparts.
Further details regarding the expected timescale of the implementation of these pathways can be found in appendix 5. A high volume of End of Life Care (EoLC) patients are conveyed to emergency departments inappropriately. Some 32,000 people die in Wales each year and it is estimated that 75% of those have some form of palliative care need. Data also shows that 56% of the 32,000 will die in a hospital and that there are 65,000 hospital admissions in Wales for people in their last year of life. On average each person will be admitted to hospital 2.16 times in their last year of life. In 2014, emergency admissions in the last year of life accounted for almost 842,000 bed days. Consequently, we have recently submitted a CAREMORE® service change for 16/17 idea proposal
to our Commissioner for EoLC pathway funding. This would allow us to introduce:
mandatory EoLC training for all WAST Paramedics which includes the recognition of end
stages of life and symptom management;
the use of anticipatory medicines;
24 hour access to palliative specialist advice for the paramedic on scene; and
read only access to CaNISC (national electronic palliative patient database) by CCC
Clinicians.
We would expect the combined benefits of this to be a reduction in inappropriate ED admissions of EoLC patients with patients being able to stay at home or conveyed to a hospice if appropriate. The pathway would help achieve a patient’s wishes for their preferred place of death. This All Wales EoLC pathway would also facilitate a reduced demand on EAs, reduced lost hours at
EDs, reduced demand on EDs and a reduced total amount of EoLC patient bed days.
Action 46: Introduction of an All Wales End of Life Care Pathway
Paramedics and Emergency Medical Technicians were trained in 2015 in the use of the Paramedic Pathfinder (PPF) reductive triage system. PPF allows staff to determine safely the needs of their patients. We will develop a decision support “APP” for our clinical staff to use. This APP will link to the 111 Directory of Service and allow ambulance staff to determine the nearest appropriate service for their patient. The development of the APP will be linked to the roll-out of a portable communication device for
operational staff (more details regarding this initiative can be found in part 6.9 of this plan).
Action 47: Development of a decision support “APP” for our clinical staff to use
108
Our Patient Care Services (PCS) division generates income in excess of £21m and employs
approximately 485 staff across Wales. PCS transports patients who would not normally be able to
access the care planned for them, some of which can be life determining, if it were not for this
support. Unlike EMS, many of the patients who travel with PCS do so a regular basis. This provides
frontline crews and volunteers with the opportunity to build rapport with patients that helps to
understand and support their care needs whilst also improving overall experience.
PCS operates a seven day service (currently limited on weekends) transporting patients to and from
outpatient clinics, day centres, renal dialysis units, cancer care or to transfer between, or discharge
from, hospital wards. In the 12 months from October 2014 until September 2015, PCS undertook
827,000 patient journeys.
Since the McClelland Review of 2013, the future of Non-Emergency Patient Transport Services
within WAST has been uncertain. However, this uncertainty has now been addressed since
Ministerial approval was received to progress all recommendations contained within a NEPTS
business case that was produced in 2015/16. One of these recommendations was that WAST
should manage and coordinate NEPTS on behalf of NHS Wales.
In Part 1 of this plan, the success of the original NEPTS project (which was the vehicle for producing
the business case described above) is highlighted.
Representatives from WAST, Welsh Government and the Chief Ambulance Services Commissioner (CASC) have agreed the Emergency Ambulance Services Committee (EASC) will progress the commissioning key deliverables, whilst WAST will focus purely on the service delivery elements of the business case and the establishment of the new NEPTS model. The key deliverables for the CASC on behalf of EASC are:
establishing EASC as commissioning body in Wales for NEPTS;
establishing commissioning arrangements;
a national set of NEPTS service standards and requirements; and
creation of a new expert commissioning group to agree KPIs and monitor the same.
The key deliverables for WAST in implementing the recommendations of the business case are
summarised in the actions below which will form the core of the NEPTs agenda over years 1 and 2
of this plan.
Action 48: Agree and establish a dedicated NEPTS management team within WAST.
This will include establishing the NEPTS principles, vision and purpose
Action 49: Establish a single point of contact
Action 50: Improve discharge and transfer service for all scheduled care
Action 51: Extend operating hours of the service.
Action 52: Develop an enhanced service for renal, oncology and end of life care.
Non-Emergency Patient
Transport Services

109
Action 53: Engage a range of third party transport providers to help support the delivery
of NEPTS
Action 54: Creation of a new NEPTS brand.
Action 55: Explore how health and social care might work together on transport issues.
As an organisation, we have agreed with the CASC that NEPTS will adopt a similar approach to that
of our EMS services. A stepped model of service is to be developed that will support and drive the
service.
In addition to the above implementation programme, there are a number of additional actions that
are picked up by other directorates that will support the delivery of NEPTS as part of ‘business as
usual’ over the next three years. These include:
changes to the current configuration of the operational estate. i.e. Cardiff ARC (identified
within Section 6.2 Our Estate) and the potential implications for NEPTS;
any changes to the current CCC configuration (identified within Section 6.2 Our Estate), and
again the implication for NEPTS; and
the closure of Cefn Coed Divisional Headquarters which would require the relocation of the
NEPTS Call Centre (identified within Section 6.2 Our Estate).
It is important to note that the operational estate requirements for NEPTS may not always dovetail
with the operational requirements of the EMS. This will be reviewed as part of the development of
the estates strategy, in particular:
the use of discretionary capital to support NEPTS Development (identified within the capital
part of section 6); and
the procurement of a new NEPTS Planning CAD System (identified within the ICT part of
section 6).
As the new NEPTS model is implemented during year one, we will require an increase in the use of
alternative providers from the voluntary, local authority and community sector. These organisations
will focus on the transportation of patients with low-level mobility issues. The more complex mobility
patients will continue to be conveyed by ambulance.
From a workforce perspective it is likely that, in areas where alternative providers have good
geographical coverage, we will not need to recruit to certain positions. We will instead look to
allocate regular work to these providers as and when needed. This will add to the flexibility of the
NEPTS service: this is likely to commence from year two onwards. In the meantime, we will
continue to review and maintain a focus on timely recruitment when required, and to reviewing the
employment status of the existing workforce to ensure they are supported and retained as
appropriate.
When we do recruit to replace existing positions, we will be recruiting more part-time positions to
cover peak periods and early or late periods in the day. In year two or three, we will look to develop
apprenticeships into the service, and potentially through to other roles within the Trust.
As described in the approved NEPTS Business Case, the new model will require the existing WAST
PCS service to be internally disaggregated from the WAST EMS service. Fundamentally, this is
about creating a new management structure to take forward the service. This will be completed
during year one and will enable us to build a robust workforce plan to take us towards 2020. The
requirements of the new management structure have been built into the Trust’s workforce and
financial plans for 2016/17.

110
This structure will introduce PCS Team Leaders who will develop a team approach and ensure each
member of the team is supported and undertakes effective PADR. In addition, the PCS Team
Leaders will work alongside their team members and undertake observed practice and provide
remedial support as necessary.
In addition, developmental opportunities will be provided through the PADR process that will provide
the PCS workforce with the necessary skills to undertake their role to a high standard and also help
them develop skills for the next stage of their career for those who wish to. We will develop a
leadership and management plan aimed at identifying, training and developing managers and
leaders at all levels to take a proactive role in driving quality and safety, and encouraging innovation
throughout the service.

111
PART 6: OUR ENABLERS This section, along with Part 5: Our service change plans, represents the heart of our plan. It describes how a suite of enablers with a suite of actions relating to each enabler will help support us in delivering our ambitions. Further details regarding each action documented can be found in Appendix 6
The transformation we seek in our service and patient-facing areas can be achieved only through
the effective delivery of our enabling plans. Without a doubt, our most important enabler is our staff,
but ensuring we have appropriate estate and fleet is also critical alongside a timely, sophisticated
and relevant businesses intelligence function (health informatics), an appetite for learning and
improvement (service improvement, innovation and R&D) and robust and clear governance
arrangements.
This section covers the plan for our “building blocks for change”; more detail on some of the
technical elements are found in the appendices:
Our People
Our Finances (revenue and capital)
Our Estate
Our Fleet
Our Partners, Patients and Stakeholders - engagement
Service Improvement and Innovation
Health Informatics/Business Intelligence
Information Management and Technology
Research and Development
Our Governance
For each of these areas, we have also continued to be explicit in the actions that we will take.
6.1 Our People
Our people are our biggest asset and it is vital that we use the talents and experience of our whole
workforce to provide high quality, safe services to the individuals, families and communities we
serve. Changes to our New Clinical Response Model mean the make-up of our existing workforce
may need to change.
However, effective workforce planning is more than getting the numbers right. It is about getting the
staff with the right skills to meet our future demands, performing within the right culture, built with the
right staffing model, with the right skills, supported by effective management and clinical leadership
that will successfully transform the way we provide care and services to the patients and
communities we serve.
In this section of our IMTP, we share with you details of our current workforce profile, our People
Strategy and enabling frameworks and plans w will support us to deliver against our strategic
priorities. More specifically we will:

112
take a closer look at our workforce plan, and how we intend to tackle some of the challenges
facing us, including supply of qualified paramedics;
share our thinking on how we will drive up clinical skills and excellence across the Trust, and
how changes to the education and training of paramedic and other staff will support that
drive ; and
outline our OD plans to transform the way we do things and culture of the organisation, and
actions we will take to improve the working lives of our staff and their well-being.
Our Workforce Profile
The Trust employs approximately 3,030 members of staff (December 2015). The majority of these
people are employed within our Operations Directorate, which includes our Clinical Contact Centres,
Emergency Medical Service (EMS), Urgent Care Staff (UCS) and Non-Emergency Patient Care
Services (PCS) staff.
Our frontline teams are supported by colleagues working within our Corporate / Executive functions
and teams. Detailed breakdown of staffing numbers by headcount and whole time equivalent by
service / directorate can be found in section 2.1.
Below are some facts about our workforce
Working Longer
Our current workforce profile presents a number of challenges and opportunities. Almost 35% of
our workforce is over 50 years of age. There are profession specific challenges and also
organisation wide challenges that come from an ageing workforce. It is perhaps helpful to note that,
within our front line EMS service, only 29% of our workforce is aged over 50.
Changes to retirement provisions mean that predicting potential retirements is harder, with a
prospect of staff working beyond a traditional retirement age. As such, it is predicted that the Trust
will continue to have an older workforce profile. Retaining our older workforce is multifaceted and
involves balancing a number of competing factors, such as awareness of health issues and
113
managing absence whilst also managing the changing capabilities of the older workforce. These
changes could be a result of a decrease in confidence, the need to work with greater speed and
dexterity and the capacity to engage with transformational change.
Given the nature of the service changes planned, how we enable this workforce to work differently
will also require a specific focus. In addition, an older workforce is likely to have increased family
responsibilities and also health concerns and a different perspective on work life balance. This
means different strategies will be required to ensure the Trust benefits from their extensive
knowledge and experience. This group also has potential to create significant turnover and
succession planning will need to be carefully managed to ensure service provision is not
jeopardised.
The Trust is part of an all-Wales project group looking at the implications of working longer, and
opportunities to support staff to remain in work. As a service, we foresee that the shift in workforce
capacity to the first three steps of the New Clinical Response Model may provide future
opportunities for our older workforce in roles educating the public and school children of the
importance of choosing well, and basic life support skills. Opportunities to work within our clinical
contact centre and NHSDW / 111 service may also provide an alternative for many paramedic staff
nearing the limits of their physical capability to deal with the demands of responding to 999 calls.
A more diverse workforce
Presently less than 1% of our people identify themselves as from Black & Minority Ethnic (BME)
origin. There is some further work to do to ensure our records are as up to date as possible, but we
recognise that our workforce is not as diverse as it needs to be. For example, our local community
in Cardiff is approximately 10% BME communities; our workforce isn’t. This potentially creates a
barrier to providing great care. In our Strategic Equality Plan and Objectives, we state our intention
to proactively work with partners to help our BME communities to be want and be able to work in the
Trust. This will include encouraging people to become volunteers, working with schools and
Swansea University to encourage applications for paramedic training from minority groups, and in
developing apprenticeships. Details of our Strategic Equality Plan and Objectives, ‘Treating People
Fairly’ are outlined in section 2 of this plan.
Our Volunteers
We recognise the important role which volunteering plays in complementing the work of our staff. We support and encourage the efforts of individual volunteers and voluntary organisations for the benefit of patients and their relatives.
Community First Responders
Our Community First Responders (CFRs) are a valued part of the emergency response team and
provide a resource to us to support the provision of our EMS. CFRs also have an important role in
developing community resilience and public awareness. CFRs provide pre-hospital emergency care
within a defined set of protocols before the arrival of an ambulance resource.
There are currently more than 200 Community First Responder schemes across Wales comprising
approximately 2,200 volunteer members and these schemes contribute more than 3% to RED
performance pan Wales. Part 5 of this plan (Our Service Change Plans) explores in more detail the
emphasis we will be placing on developing the CFR role over the life of this plan.

114
Voluntary Car Drivers
The Ambulance Car Service is a vital component of the Patient Care Service and consists of a team of dedicated volunteer drivers who use their own cars and give their time freely to assist in transporting patients to various hospitals and clinics throughout Wales and England. As at January 2016, the Trust had 235 ambulance volunteer car drivers. Each year, the Ambulance Car Service drivers cover eight million miles providing transport to patients with limited mobility who are able to travel by car. The Trust’s strategy is to use the Ambulance Car Service volunteers as the service of choice for those patients who fit the criteria. The volunteer drivers transport regular patients and develop strong bonds with them.
Workforce Key Performance Indicators (KPIs)
Below in Figure 15 are some of our workforce and OD KPIs that we currently monitor on a monthly basis within the Trust:
Figure 15
Figures are correct as at 31 January 2016 with exception of staff engagement, which is taken from most
recent NHS Wales Staff Survey in 2013. A new survey will be run later in 2016.
Note that Statutory and Mandatory Training figures are not currently available as the ESR report and data is currently under review. However, this will be reported and monitored across the Trust as soon as available.
Monitoring of these key performance indicators takes place on a monthly basis through Executive Performance Review meetings with each Head of Operations, and also through production of the Trust’s monthly IPR, which is received at Executive Management Team, Finance & Resource Committee and also Trust Board.
Our People Strategy ‘Being our Best’
One of our key strategic priorities as a Trust is the need to have an engaged and skilled workforce
operating within an organisational culture and framework that enables them to work to the top of
their skill set to deliver high quality care.
Our People Strategy is designed to enable us to build on the positives of the last 12 months and
respond to the challenges ahead by providing focus and opportunity to align our resources
accordingly. Below in Figure 16 is a simple SWOT analysis that has assisted in developing our
strategy and action plans.

115
Figure 16: SWOT Analysis
From this we have developed a simple four-step model (Figure 17) with key activity areas which will
be our focus for the next three years and from which our enabling frameworks flow. The model also
identifies the core ‘golden threads’ that run through the whole strategy and everything we do as a
Workforce & OD Directorate and organisation.
Strengths More robust operational workforce planning capacity and clarity of vacant posts Improved establishment control and monitoring of recruitment activity Aligned recruitment and training plans More frontline EMS staff in post, and increased UHP available Improved sickness absence rates, plus lower number of vacant posts and less requirement for overtime Pilot New Clinical Response Model and positive impact on outcomes (AQI) and performance Improved partnership working with Trade Unions Significant increase in number of PADRs for staff
Introduction of CPD hours into rosters New Executive leadership team, clear strategic direction Agreed shared behaviours and vision – built from bottom up
Weaknesses ESR system set up requires further work and data cleanse to ensure workforce and financial data is aligned Limitations of an ‘out of date’ CAD system Low levels of engagement of staff and morale High expectations of change and improvements brought about by New Clinical response Model Resourcing levels at peak times and in rural areas Absence of a clear clinical leadership strategy and limited effective use of the paramedic pathfinder Limited access to alternative pathways and GPs / Third Sector services to support patients at home Need for changes in behaviours Limited availability / access to workforce benchmarking information for ambulance services
Threats / Risks ….. Financial risk posed by introduction of Band 6 for paramedics in some English Ambulance Services and discussions of grading reviews of paramedics nationally Service developments within Health Boards and Trusts attracting Advanced Paramedic Practitioners into GP Out of Hours and multi-disciplinary teams within the hospital and community setting. Impact of continuing pressures across USC system, and impact on patients and also staff working lives through overruns and inability to take timely meal breaks High levels of abstractions / variation across CCCs and Health Board teams Overall affordability of potential developments Capacity and/ or capability in management and supervisory infrastructures, inc. corporate teams
Opportunities Potential benefits offered by new models such as the ‘community based paramedic’ in rural areas and critical care paramedic Development of a modular approach to disease specific training to increase clinical skills and decision making Increase use of the clinical desk to assess non injury falls, option to employ specialist mental health nurses and midwives on the desk Volunteer car drivers instead of taxis or one step further and employ staff similar to the those in local authorities 'man (person) in a van' who does this. Expanded use of the CFRs and Co-responder models Review of the staffing model (crews) of EMS Vehicles Development of the CTL role and APP role

116
Figure 17: Four-Step Model
Key Enabling Frameworks
There are four key enabling frameworks of activity linked to the model. They are:
Workforce Planning (Plan)
We know that robust and effective workforce and resource planning is key to our future success and to ensuring a resilient, safe and sustainable future workforce. We will know we have been successfully in our workforce and resource planning when we have
a resilient, flexible and sustainable workforce with low turnover and low sickness;
increased paramedic hours available to be rostered and a consequent reduction in our reliance on overtime and private ambulance usage;
the most appropriate response clinical staff attending calls that make best use of their skill sets, and the lowest acuity healthcare professional (HCP) calls are being managed by the Urgent Care Service rather than paramedic staff;
improved performance and, most importantly; and
improved quality of care and positive patient experiences.
Recruitment (Recruit)
The opportunity for paramedic staff to move into roles in the ambulance and wider NHS setting, including GP OOHs, is growing and, like many other ambulance services in the United Kingdom, we are experiencing difficulties in attracting qualified paramedics to our vacancies. We want to be seen as the employer of choice among ambulance services. We will know that we have successfully achieved our recruitment plan objectives when:
we have recruited to all our vacancies in a timely manner;
the time taken to hire new staff and the process is as efficient as possible and candidates have a positive experience;
WAST is seen as the employer of choice, and Wales as the place to live and work;
117
our workforce profile better reflects the communities we serve, and our patients (continue to) receive care and support in their preferred language of Welsh or English.
Training and Education (Train)
Our people have a fantastic appetite for personal and professional development. Ambulance training and education is evolving in terms of developments to degree level education, driver training and our staff need the skills and confidence to deliver high quality care adapting to increasing pressure of demographic changes and an ageing population (and an ageing workforce). Strong clinical leadership and direction in this area will help make our plans to deliver the highest standards of training and education for staff a reality. We will know that we have successfully achieved our training and education plan objectives when:
we can show evidence of improved clinical decision-making across the Trust and lower conveyance rates;
we see improved clinical outcomes for patients and receive stories of positive patient and staff experience;
we experience a reduction in complaints and concerns related to treatment and care;
our workforce is well trained and keeping up with the latest clinical and technological advances;
we meet our CPD and mandatory training target; and
we have transformed our National Training Centre into a flagship training facility, recognised as a centre of excellence with state of the art training facilities
Organisational Development (OD) (Retain)
We have a dedicated and skilled workforce, committed to delivering the highest quality of patient care for the people of Wales. We are on a journey of transformation over the next three years – transforming our services, culture and workforce. The OD framework and plans will help underpin this transformation by focusing on leadership and management capacity and capability, health and well-being, engagement and appreciation of staff, and creating personal responsibility and accountability, and ultimately ensuring we retain a skilled, dedicated and motivated workforce. We will know that we have successfully achieved our OD plans when:
our people are more resilient and better able to deal with the day to day emotional challenges of the job, and stress-related absence falls;
we have achieved Gold Corporate Health Standard (2016) and then Platinum (2019);
all staff receive regular, high quality feedback on performance and care & undertake a quality PADR with their line manager;
levels of colleague participation and ownership will be much higher, reflected in an improved employee engagement score from staff surveys;
we have in place a sustainable model of clinical supervision and appraisal, with a network of skilled clinical mentors to support staff and students;
levels of turnover will be low; and
diversity and inclusivity among our workforce improves and we are recognised as a Stonewall Top 100 Employer.
A number of core ‘golden threads’ run through our strategy and are integral to what we do and the outcomes we seek. They are:
leadership (including clinical leadership);
behaviours;

118
quality; and
staff well-being.
The development of our new set of organisational shared behaviours and plans to embed these are outlined in section 3 of this IMTP. Similarly, details of our Quality Strategy and commitment to being a quality driven, clinically-led organisation are described in Section 5 of this document.
Leadership
We define leadership as “the ability to positively impact and influence others”. Therefore, vibrant,
empowering and effective leadership is a key enabler for us to deliver our strategic priorities and
plans described further on in this section. Good leadership is also key to enabling our staff to be
their best.
To help us develop and grow our leaders, we have developed principles of effective leadership in the Trust. These are outlined below:
to create high levels of humility and self-inquiry, and listening/ questioning and trust
towards others;
all development needs to be chosen by the learner and not forced: we always work with
the willing and want leaders to be the best they can be in their own way;
each leader is unique and will have unique needs: we try to avoid set programmes for
any group unless it is absolutely required;
we are part of Public Services Wales; we take every opportunity to develop leadership
with partners;
we focus on transformation rather than transaction; our activities are facilitated and not
“trained”; and
leadership can be shown by anyone; all our opportunities are available to all of our
colleagues.
Leadership development is a cornerstone of our OD plan, further details of which can be found later
in this section.
Clinical Leadership
Driving forward clinical leadership across the Trust is a vital part of our overall leadership and
management development plan. It is a key part of a developing, integrated agenda, working closely
with Heads of Operations, Workforce Development and the Medical and Clinical Services
Directorate.
Rising unscheduled care demand for individuals with long-term conditions is a major challenge for
the NHS in Wales. This has resulted in a call for more care to be delivered closer to home in the
community setting and the modernisation of NHS clinical roles and delivery systems. Similarly, the
concept of prudent healthcare strongly promotes clinical role substitution and adaptation in order to
achieve similar or, better outcomes for patients, albeit using less expensive human and technical
resources. In this IMTP, we outline a significant programme of clinical change to modernise
ambulance practice and clinical service delivery. Ensuring the quality and consistency of
ambulance clinical practice during this period of change is a challenge. Effective high quality clinical
leadership is, therefore, pivotal to achieving any benefits predicated by this change and remains a
key priority.
Our clinical leadership development plans will ensure an appropriate structure is in place to
encourage clinical leadership throughout the Trust, made more important because of increasing

119
levels of clinical decision-making at the patient interface. We aim to further support and challenge all
clinicians to understand and develop their own and others’ clinical practice. This will be based on a
range of indicators, evidence and feedback across multi-professional teams and groups.
We have already made progress towards improving clinical leadership within the Trust by:
reviewing the Advanced Paramedic Practitioner (APP) role;
exploring options to improve access to clinical supervision for frontline staff;
strengthening links between training and education, with operations and clinical and medical
directorate;
reviewing of the role of the Clinical Team Leader (CTL) and the development and support
required to be able to deliver their role effectively;
development of the Organisational Learning Group; and
developing clinical pathways and clinical lead roles (described earlier in this plan).
As part of our plans, existing and future clinical team leaders will be developed in the underpinning
theories of leadership and management of change within a clinical setting. We will do this through
the development and implementation of a structured development programme and action learning
workshops across the Trust. We expect this to result in a greater understanding of clinical
leadership across a wider range of clinical disciplines, grades and groups in the Trust.
We will also review our existing Clinical Services Strategy, which is nearing the end of its term, with
a view to developing and consulting upon a refreshed strategy linked to a Clinical Leadership Plan.
Having a clear clinical leadership and supervision infrastructure across the Trust will help serve as a
quality assurance function and work closely with Research and Clinical Audit departments to
provide the ability and systems to identify best practice. This will have a key impact on both
individual and organisational learning and performance improvement.
As part of this developing infrastructure, the Trust will consider the role and benefit of introducing
consultant paramedics in the future. There is a clear need to ‘do things differently’ to provide safe,
high quality care to patients, relieve pressures on the clinical workforce and ensure prudent use of
NHS Wales resources and finance. The key benefits of introducing a consultant paramedic role
include ensuring contribution to the wider NHS health economy by improving patient safety and
clinical quality at both ‘advanced’ and ‘core’ levels of paramedic practice within the Hear & Treat
and “See & Treat” domains; assistance in the implementation and monitoring of organisational
learning into clinical practice though expert clinical supervision and mentorship; and support of the
development and delivery of national clinical strategy through system thinking, developing shared
visions and supporting the internal/external clinical education and research agenda.
Well-being
The health and well-being of our staff will remain a core focus for us in terms of the realisation of our
vision of valuing staff. Continuing development of our in-house Occupational Health and Well-being
Service to ensure a range of services, advice and guidance to promote and improve the well-being
of staff is a key objective for us.
In 2015/16 we developed the following services for our staff to help promote their health and well-
being:
immediate access to telephone counselling for all staff, with opportunity for face to face
counselling if required;

120
display of posters and leaflets with technology enabled QR codes with direct links to
dedicated support services to signpost staff to resources for advice; and
launch of two occupational health and well-being vehicles across Wales. This provides local
services that are tailored to WAST needs. They have been used for flu awareness campaign
including vaccinations and health screenings.
The Trust’s Health and Well-being Steering Group will continue to develop and promote initiatives within the Trust which support and encourage improved health and well-being through engagement with staff and in line with the NHS Wales Health and Well-being Charter.
Through the development of a network of well-being advocates, health promotion activities can be targeted to local need and demand and facilitate support local to where staff live and work.
We will continue to work with our partners in charities like The Ambulance Services Charity (TASC), MIND and Time To Change Wales to ensure that staff can access specialist support services and treatment if appropriate.
Recently, the Trust has launched a new employee assistance programme which includes many
interactive and online tools to help inform and influence individuals to take positive steps towards
improving their lifestyle; diet and exercise, sleep and debt management for example. These tools
will continue to be promoted and encouraged.
Our People Strategy map (Figure 18 below) provides an overview of the strategy, the context and challenges, enabling frameworks and plans with key dependencies and outcomes.

121
Our People Strategy 2016/17 – 2018/19
Our Vision A leading ambulance service providing the best possible care through a skilled, professional and healthy workforce
Our Strategic
Priorities
Strategy will underpin delivery of all Trust strategic priorities but particularly aligned to priorities 2, 5 and 6
National Policy
& Strategy
(Workforce &
OD)
The Social Services and Well Being (Wales) Act 2014 – a better qualified workforce with skills that enable people to work across organisational boundaries
Prudent Healthcare – working prudently to ensure you do only what only you can do.
NHS Wales Working Differently, Working Together Framework – engaged workforce, a sustainable and skilled workforce, a redesigned workforce, a workforce that aims at
excellence within available resources
Implications of Francis and Trusted to Care Reports - impact of culture and behaviours upon performance and care
2014 Williams Commission on Public Services – articulates the leadership challenge, importance of leadership development and succession planning
Primary Care Workforce Plan
Equality Act (2010), Welsh Language Measure (Wales) 2011 and standards
Enabling
Frameworks
WORKFORCE PLANNING (PLAN) RECRUITMENT (RECRUIT) TRAINING & EDUCATION (TRAIN) ORGANISATION DEVELOPMENT
(RETAIN)
What
opportunities
and challenges
face us in the
next three to
five years?
National move towards a degree based
paramedic profession
Potential for a ‘fallow’ year on move to
degree
Impact of degree requirement on internal
succession routes
Financial affordability of re-banding of
paramedic staff to B6
Increased demand for Advanced
Paramedics to work within HBs and
Primary Care
Competition for qualified paramedics in
face of national shortages and differences
in terms and conditions to English
Ambulance Services
Long lead in times for recruitment
Challenge to attract and recruit to rural
areas and retain staff there
Lack of diversity and poor representation
from visible BME groups among the
workforce at all levels (including Board)
Launch of Trust refreshed shared
behaviours and need to embed into
Changes to Clinical Response Model
Ageing population and increase in need
for skills to manage chronic conditions
and support patients to remain at home
(so that they can be treated on an
individual basis for their needs)
Opportunity to positively contribute to
flow across the system through increased
clinical decision making to support
patients at home or access alternative
pathways
Changes to the Driving Qualifications /
Increasing numbers of volunteers
including CFRs to support, engage and
retain
Challenge to engage staff and improve
against 2013 NHS Staff Survey response
rate (30%) and engagement score (43%)
which benchmarked significantly lower
than the average for NHS Wales (55%)
Turnover rates of 11% in 2015
Need to develop vibrant, authentic and
empowering leaders at all levels
Improving management capability and
Figure 18: Our People Strategy

122
Delivery of New Clinical response Model
and changes to demand / ideal response
Opportunity to develop community
paramedic role in rural areas, Specialist
Paramedic and APP roles
Review of Clinical Team Leaders role &
rosters
Implementation of NEPTS and 111
Pathfinder
Increasingly ageing workforce – a third of
EMS workforce over the age of 50
Potential to integrate and participate in
multi-disciplinary teams within primary
care
Delays to hospital handovers and high
levels of abstractions
2015/16 a 1.5 percentage point reduction
(approx) in sickness absence, with a further
one percentage point reduction would
place WAST among majority of Ambulance
Services
Resourcing levels and policy, particularly at
peak demand times (e.g. Christmas) and in
rural areas at night
selection processes to ensure right person,
right place and right time
Increasing role for Community First
Responders and Co-Responders with Fire
Service
Minimum levels of bilingual skills to ensure
services can be delivered to patients in
both Welsh and English as part of
recruitment plans
Standards
Strengthening of infrastructure to deliver
clinical leadership and supervision across
clinical staff to support PADR and
reflective practice
Poor physical infrastructure within NATC
and need to maximise use of technology
to deliver training
Expectations of staff /graduates /
millennials
Up-skilling and maintenance of trainer
competences
Challenge to ‘professionalise’ the
paramedic workforce
Ability to transfer skills such as nursing
qualifications within paramedic training
capacity at scale, across Wales
History of bullying and harassment,
learning from experience of others such
as London Ambulance Service
Lack of structured succession planning to
middle and senior management roles
Improving TU relationships but challenge
to embed strong partnership working
with Trade Unions at middle
management level
Staff experiencing long shifts due to
lengthy overruns and delays at hospital
Low compliance with meal break
requirements
National statistics of 1 in 4 people suffer
with mental health problems – increasing
prevalence of stress, anxiety and
depression as a reason for absence
Flu vaccinations for front line staff a
Ministerial priority
Enabling Plans Workforce Plan Recruitment Steering Group Action Plan Workforce Education Development
Group Action Plan
Being Our Best – OD Plan
Inter-
dependencies /
linked action
plans
Demand & Capacity Review
Workforce Education Development Group
Sickness Action Plan
Local Delivery Plans
Strategic Equality Plan
CFR and Co-Responder Strategy
Communication & Engagement Plan
NHS Wales Workforce & OD Directors
Work Programme
Clinical Leadership Task & Finish Group
Action Plan
NATC Training & CPD Plan
Quality Improvement Strategy
Clinical Strategy (Development)
Strategic Equality Plan
Health & Well-being Steering Group
Corporate Health Standard Action Plan
Improving our Staff Working Lives –
problem solving test beds

123
Education Commissioning
WiFIS
Communication & Engagement Plan
Quality Improvement Strategy
Staff Recognition and Appreciation Plan
How will we
know we have
been
successful?
Resilient and sustainable workforce – low
vacancies, low sickness, increased UHP and
improved quality and performance
Decreased cost of overtime and private
ambulance usage
Positive patient experience
Workforce profile will better reflect the
communities we serve
No / minimal vacancies in EMS
Trust is seen as Employer of Choice
Less disciplinary cases
Reduced time to hire
Patients will (continue to) receive care and
support in their preferred language of
Welsh or English
Positive patient and staff experience
Reduction in complaints and concerns
Strengthened clinical leadership and
improved clinical decision making across
the Trust
Lower conveyance rates
Improved clinical outcomes for patients
Sickness absence targets will be met
We will have achieved Gold Corporate
Health Standard and then Platinum
We will be a Stonewall Top 100 Employer
All staff will receive regular, high quality
feedback on performance and care &
PADR
Levels of colleague participation and
ownership will be much higher
Workforce profile will better reflect the
communities we serve

124
Workforce Plan
In 2015/16, we took action to build a solid foundation for future workforce planning by improving establishment control, confirming budgeted and actual establishments (particularly for Emergency Medical Service- EMS- staff), and aligning recruitment and training plans.
Developing the skills, capacity and capability to workforce plan continues to be a priority. Working closely with finance and operations colleagues, we
have also taken action to improve data quality with the ESR system and align this with our financial data. We have trained a number of HR staff in workforce planning, and begun to develop closer links between our workforce and resource planning teams.
Our ability to workforce plan depends upon an understanding of current and future demand for 999
and other services and what that means for the workforce, and of the supply chain of paramedics
and other staff. Our EMS workforce is our biggest resource and, therefore, remains a focus for our
workforce planning.
As a result of our planning work:
we have been able to demonstrate an increase in the number of staff and production hours available to our Health Board operational teams and a consequent reduction in the need for overtime during 2015/16;
we know how many paramedic staff we currently need up to 2019 based on existing
requirements if there is no change to our current skill mix or establishments, and how many
we students are currently in the supply chain. We know that if we do nothing to change our
existing skill mix, there is sufficient supply to meet demand based on average turnover
among the workforce but this may be significantly impacted by our ability to recruit from
among the student workforce;
we have taken action in our education commissioning of paramedic students to avoid the
potential for a fallow year as a result of the potential introduction of a degree requirement for
all paramedic students. This is described in further detail below;
we expect that demand for 999 services will continue to grow, and is linked to an increase in
the frail elderly population of Wales. The graph below demonstrates that an increasing
number of our patients are now over 65. This change in demographic will also result in a
change of case mix. Our staff will require an increasing focus on health issues associated
with frailty and chronic illness as well as injury patterns associated with old age;
we recognise the need to plan for increasing competition for paramedic staff to other
ambulance services, but also to new roles in the wider NHS unscheduled care system and
also outside the NHS;
future demand and workforce requirements will be driven by the ideal response under the
New Clinical Response Model; and
we expect to drive a re-profiling of our workforce over the next three years to increase
capacity and capability across STEP 2 (Answer my call) and STEP 4 (Give me Treatment) of
the New Clinical Response Model.

125
Figure 19: Ambulance Demand (999 + Verified Incidents)
The Supply Chain – Paramedic Education Commissioning
Paramedic education has gone through significant change since 2008 with the introduction of the Diploma in Paramedic Science at Swansea University. Given the evolving nature of the service and the preparation required to equip paramedics with the knowledge and skills necessary, further change will be required. Paramedics have traditionally been trained to deal with life-threatening conditions; however, this forms only a small part of their work and they are increasingly being called upon to deal with non-life threatening conditions and complete an episode of care or refer on to other staff rather than transport everyone to the local Emergency Department.
It is proposed that paramedic education in Wales be extended to a three-year undergraduate degree programme. Although Welsh Government has given no official confirmation, it is expected that this will be supported and confirmed at some point in 2016/17. It is likely that, in the other parts of the UK, this will be introduced at a later date.
With a change from a two-year programme to a three-year programme, there is the risk of a fallow year. To mitigate this risk, the Trust is taking forward discussions with Swansea University, with the support of the Welsh Education Development Service (WEDS) on the following recommendations:
a. the one year EMT conversion programme is continued for the next 5 years (2015-2020) at diploma level. This will enable current EMTs to work within that timescale to progress to a paramedic role; and
b. the diploma and degree programmes are run simultaneously for one year (the year the degree is introduced). This would have the effect of ensuring an output of Paramedics each year from the EMT conversion programme and the diploma/degree programme. Critically, there would be no fallow year.
The following tables in Figure 20 demonstrate the required number of paramedics over the five-year period (depending upon when the degree requirement is introduced). Note that current education commissioning numbers have been increased in 2017 to mitigate against the potential for a ‘fallow year’ if degree requirement is introduced in 2017.

126
Figure 20: Paramedic Recruitment Plan
Original Plan (Introduction of Degree in
2016)
Start Output
Diploma Degree Diploma Degree
2014 17
2015 64
2016 32 32 17
2017 32 64
2018 39 32
2019 32
2020 39
Total output over 5 years = 184
Amended Plan (Degree in 2017)
Start Output
Diploma Degree Diploma Degree
2014 17
2015 64
2016 32 17
2017 32 32 64
2018 39 32
2019 32
2020 39
Total output over 5 years = 184
In addition to Diploma / Degree candidates, WAST will also be provided with 30 places in
September each year on the EMT Conversion Programme, which is an 18 month process - 6 month
bridging module and 1 year academic programme, with a March outturn of paramedics.
Our assessment indicates that our basic paramedic replacements required to 2019 based on no
change to our future skill mix will be just about met based on:
Current paramedic workforce 765.04 WTE;
Average paramedic turnover circa 48 WTE per annum;
Estimated number of newly trained paramedics required simply to replace average staff turnover (inc Turnover and Internal Promotion) c.186 WTE;
Estimated number of new paramedics coming out of training (including EMT) to 2019 = c205; and
This will result in a narrow surplus by 2019.
It should be noted however that this surplus provides a very narrow buffer in terms of supply given potential increases in turnover that could result from increased competition for paramedic and APP staff, and recruitment rates of the student workforce into posts with WAST. In the 2015/16 WAST secured only c.50% of the student outturn, which if repeated would result in a deficit of newly qualified paramedics. This highlights the importance of our recruitment plans, details of which follow further on in this section.
Demand and Current / Future Capacity
Our demand will be driven by the New Clinical Response Model, which was launched as a 12 month pilot in October 2015. This pilot will be evaluated later in 2016. However, in order to understand what the new response model means for our current configuration of workforce, a detailed analysis of demand and capacity is planned for the first quarter of 2016/17.
This exercise will assist us to understand the picture of demand by hour, by day in each area and the ideal response under the new model. It will tell us how many of each type of resource we need by hour and by location if we are going to send the ideal response, and what this means for the number of paramedics, EMTs and UCS staff and CCC clinicians in order to meet our A8 target and provide a safe service.
This work will also enable us to model and understand the impact of different scenarios and growth drivers, including demographic changes and changes to Health Board service models. We will be able to model the impact of crewing ambulances with a UCS member or staff and a paramedic, the impact of releasing all Clinical Team Leaders from rosters (whether for 20, 50 or 100% of the time),
127
and how many WTE we would need if we were to introduce new roles such as community-based paramedics, critical care paramedics and specialist paramedics.
This work is too complex for the analysis tools and skills currently available to us, and we will work with an expert provider (yet to be agreed) to develop our capacity demand and workforce model through April, May and June 2016. As a result, we have not reflected any change to our workforce numbers and skills mix for years two and three at this stage of planning, but expect the detail to be available to us for August / September 2016.
We know that, in addition to the implications of the capacity and demand work, there will be other
developments over the planning period that are likely to impact on workforce numbers and the cost
base of the Trust, for example, linked to the replacement of the Trust’s CAD. The impact of these
will need to be modelled and assessed, including consideration and identification of funding sources
to support any developments.
The numbers in our workforce and finance plans do, however, take account of the following
developments described in Section 5:
development of the 111 Pathfinder in 2016/17 and estimated numbers if rolled out pan Wales in 2017/18 and 2018/19;
development of the NEPTS service, and specifically the need for a more resilient management infrastructure in 2016/17; and
known developments with the CCC as part of its Transformation programme.
Future Workforce Modernisation Opportunities
We have referenced at different points in this plan a number of potential future roles and opportunities that the Trust plans to develop and progress over the next three years. These include:
opportunities to collaborate on expanded roles for paramedics across NHS Wales unscheduled care services, GP Out of Hours services and the potential for paramedics to undertake GP home visits and also with education providers;
development of specialist roles such as community-based paramedics in rural areas and critical care paramedics;
reviewing the evidence base and potential benefits of the specialist paramedic role within the Trust;
expanding the expert knowledge base of staff working on the CCC clinical desk by collaborating with Health Boards to extend opportunities to midwives and mental health nurses; and
introduction of consultant paramedic roles into the Trust. We will be exploring these opportunities in year one of our plan.
We will also seek to develop the career pathways for staff using, where appropriate, the College of Paramedics career framework in Figure 21 pictured below.

128
Figure 21
We will be exploring the following :
The potential to create ‘ambulance paramedic’ roles suitable for newly qualified staff in the first 5 years of their career;
progression routes for band 5 paramedics into a band 6 role through competency based assessment supported by modular training on, for example, chronic conditions management;
Progression into roles such as specialist and advanced paramedics providing supervision or advanced care; and
Apprentice opportunities for PCS staff and UCS through to paramedic.
Workforce Efficiency and Productivity
As we plan and develop our future workforce, we recognise the need to ensure we do not lose focus on opportunities to increase workforce efficiency and productivity. Our main areas of opportunity to reduce variable pay spend and spend on private ambulance providers are:
Resource Planning – Efficient Rostering
Over the past 24 months, we have been reviewing existing EMS operational rosters with colleagues
and staff side representatives, the purpose being to accommodate changes and developments to
staffing levels, growth in demand, changes to the job cycle and re-configuration of hospital services
over recent years. The project team worked in partnership to realign rosters to the funded
establishment and to predicted demand in order to achieve the best possible fit. The opportunity
was also taken to incorporate a set number of training hours and to determine the existing level of
variable capacity.
This process highlighted a number of issues, which are yet to be addressed:
some areas are under resourced and have insufficient variable capacity;
unfunded local initiatives which have been introduced over time have resulted in a reduction of planned unit hours; and
Effective resource planning and efficient rostering of resources, with a drive to tackle
variability in abstractions and performance
Improving attendance at work, reducing cumulative sickness absence rates by a further
2% over the next three years
Improving the working lives of staff by reducing overruns and improving meal break
compliance
Maximising the benefits of a technology enabled workforce
Streamlining recruitment and reducing time to hire

129
approach being taken regarding the allocation and management of Clinical Team Leader "protected" time is inconsistent.
These are significant contributing factors to our high reliance on overtime during the 2015/16 period
despite a reduction in absence and a general increase in the EMS funded establishment.
Our existing rosters provide circa 20% variable cover capacity that varies from 7% to circa 30%. This is low in comparison to the generally accepted best practice for ambulance services, where the benchmark is 34%. Our current abstraction rate is approximately 35 – 40% which excludes hours uncovered because of vacancies or the 3% reduction in available hours as a result of introducing the Learning and Development hours. The deficit in variable cover capacity therefore results in our heavy reliance on overtime to produce a robust level of resourcing and must be addressed as part of our demand and capacity planning exercise.
Action 56: Address the variable relief capacity as part of the capacity and demand work and workforce planning exercise
Going forward, the Roster Review project in its current form will be closed and the Demand and
Capacity work will commence.
Through this work we will review current working practices to identify opportunities that allow us to
increase productivity. These include:
learning and development hours (CPD) – a review of the current allocation of hours, how these are utilised, what % is currently being utilised, how the unused hours are being recouped by the Trust. We are discussing with our trade union colleagues a proposal to realign a % of existing CPD hours to enable a working shift where ‘on the job’ development and reflective practice with either a CTL or APP can take place. It is important to create opportunity for all clinical staff to reflect on the care they provide to patients. As registrants, it is a requirement under the HCPC fitness to practice guidance that reflection is a facility that all registrants should embrace. There are a number of benefits to being able to critically and clinically evaluate practice for both the practitioner and the patient;
review of CTL position/management time – work is on-going to review the role and management time, recommendations should be available by the end of May 2016;
skill mix of Emergency Ambulance – Review of crew skill mix to identify where we can do more within the same resource envelope;
abstractions – a performance framework will be developed to demonstrate the flow of recruitment into operational hours. This will allow us to understand the implications of high abstraction rates on the workforce and manage them more effectively;
variable relief capacity within rosters where appropriate to further reduce reliance on overtime, and ensuring appropriate control of overtime usage. (flexibility); and
the potential positive benefits of ‘over-recruitment’, and appointment of staff on a more flexible basis on a Health Board or regional pool basis.
The financial impact of some of these proposals has been modelled and is described at section 6.2 of this plan.
Improving Attendance at Work
WAST considers reducing sickness absence the number one priority and in 2015/16 we developed
a comprehensive Sickness Action Plan to deliver the 1% point target reduction set by Welsh
Government and the 2% point stretch target we set ourselves. This internal stretch target was an
ambitious target and we have made good progress in reducing absence across the Trust.

130
Trust Absence Rates - Effective Date: 31/01/16
We believe there is still more we can do to further reduce sickness absence and we have set
ourselves a target of 1% point reduction of the cumulative sickness rate by the 31 March 2017, with
a further reduction of 0.5% point to be delivered in 2017/18 and again in 2018/19.
A holistic approach to our employee health and well-being is instrumental in being able to deliver
against our target reduction and we have described the importance of this agenda earlier. There are
further details of some of our wider health and well-being planned actions later in this section.
We already have a sickness action plan in place that will be refreshed and rolled over into 2016/17.
This plan reflects learning from our own success and that of other organisations including West
Midlands Ambulance Service. There are 6 key things that we believe we need to maintain a focus
on in 2016/17:
ensuring Return to Work interviews are completed in a timely manner;
ensuring Executive and Board level focus on sickness absence, and robust monitoring
continues;
access to counselling and stress management support to protect staff mental well-being;
consistent application of the revised Sickness Policy and Industrial Injury Process;
continued training programme on sickness management for managers and supervisors; and
improving support and guidance for dealing with musculoskeletal problems and access to ‘fast track’ physiotherapy.
In order to deliver a 1% point reduction in our sickness levels, we have modelled the minimum rates
of sickness that each LHB area needs to achieve by the end of 2016/17. Progress against the
target will be discussed at our monthly Executive Performance Review meetings. Areas that had
already reached their target are assumed to remain at the current level and we have reduced other
areas based on the percentage required against the current rates to achieve the reduction
Action 57: Develop action plan to reduce sickness absence by 1% point by 31st March 2017, and
a further 0.5% point in 2017/18 and in 2018/19.
Further detail of the financial impact of reducing sickness is described later in this plan.

131
Improving the working lives of our staff
In 2016/17 the Operations Directorate’s key objectives are designed to start the process of ensuring
staff are supported to begin working in new ways to deliver the benefits the New Clinical Response
Model offers. These changes will increase the efficiency of the EMS as well as improving the
working lives of staff.
Reducing shift overruns is one of these key priorities.
There are a number of actions to consider, but among the main ones are:
maximising the contribution of the clinical desk;
increasing the use of HCP referrals by EMS staff. This will reduce overruns caused by conveyance to hospital;
maximising the use of safe, alternative transport solutions by the EMS staff;
developing agreement with Health Board colleagues about the release of crews delayed awaiting handover at shift end; and
tackling variation in conveyance rates.
This will be supported and enabled by:
using clinical information via the digipen system to allow CTL staff to discuss alternatives to conveyance with colleagues;
our training and education plans to improve access to educational modules which staff can take using their KSF hours which will increase staff confidence in using alternative pathways;
the development of a decision making support app which staff can use to support their clinical decision making; and
ensuring staff feel supported when cases go wrong providing there are good records of decisions made and the rationale behind them.
In addition to these priorities it is vital that staff are given opportunity to take rest breaks during their shifts. In Q1 of 2016/17 we will develop a series of test bed projects with staff and staff representatives to provide local solutions to this issue.
Workforce Enabled Technology
We aim to standardise and streamline workforce processes, maximise the potential benefits of the
whole ESR system and enhance the quality of workforce information available to managers. ESR is
a programme providing a dual payroll and HR package that works together and is integrated as a
national system used in the NHS throughout Wales and most of England. The roll out of ESR
Manager Self Service is enabling us to ensure that managers are taking the necessary
accountability and responsibility for the staff they manage.
In order to realise the full benefits of ESR, we will encourage all staff and managers to use ESR.
We believe that in doing so, there is the potential to lead to a more engaged, skilled, competent and
safe workforce with improved efficiencies, processes and productivity. It is difficult to quantify the
financial impact of this at present. However, it will also assist us to be compliant with safety
standards, and maintain up-to-date records of appraisal/ PADR, registrations, CRB/DBS, etc.
Moving to a fully electronic solution in the future will result in a reduction in waste as we remove
paper and duplication. The system also offers the functionality to support talent management
processes.

132
We will continue our roll out programme throughout 2016/17, with a particular focus on raising
awareness and the use of the business intelligence elements of ESR to enable line managers to
access comparative management data and reports from their desktops. We have refreshed our
project arrangements for the roll out of ESR and associated systems to accelerate implementation.
With the recruitment of a dedicated WFIS team, this work will be progressed during 2016/17. This
will significantly enhance individuals’ and line managers’ ability to ‘live report’ and provide intelligent
data to drive managerial decisions.
This work will be monitored by our local WFIS Programme Board. In the near future, we expect the introduction of ESR Enhance, which is being developed to meet
improvements requirements as determined with user groups and through communications to HR
Directors. There are 16 areas for improvement. The first release will introduce a new more intuitive
and engaging homepage that provides key information for Self-Service users regarding their
compliance with mandatory training and appraisals and their absence record. It will provide far
greater accessibility as it will be available through the internet, on mobile devices and via Apps,
giving both online and offline capability. Employees will have full or view-only self-service access
which includes access to national e-learning, easy access to their payslips and information on
training and professional registration.
Future developments will cover payroll admin improvements, data management, expenses
management, reporting, workforce data, finance, data validation and medical revalidation.
Our ability to maximise the true benefits of this depends on accessibility for our staff, particularly
those based across Wales in the many ambulance stations we have with limited numbers of
computers.
Recruitment Plan
We recognise our employees are fundamental to our success. The main aim of the recruitment plan is therefore to ensure we have timely and safe recruitment processes that ensure the right calibre of staff with the appropriate qualifications, skills, experience, competencies and personal qualities to meet both present and future requirements of the Trust.
Promoting the Trust as an employer of choice is also a key objective of this plan, with an emphasis placed on the kind of employment experience the Trust can offer potential candidates and a clear understanding of why people stay within the organisation and are prepared to go the extra mile. This will be our ‘employee value proposition,’ and will be developed over the next few months. As part of our recruitment campaigns, we want to show potential candidates just how much Wales has to offer as a place to work and live and the benefits of working with us at WAST. We will ensure we link our work to that being undertaking on an all-Wales basis, led by the NHS Wales Directors of Workforce and OD, specifically in relation to developing an ‘NHS Wales Recruitment Brand’. Action 58: To progress the Trust’s corporate recruitment branding and development of new
promotional boards and materials.
Action 59: To develop targeted recruitment events and a positive action recruitment plan to
increase applications from members of ethnic groups currently under-represented in
the workforce.

133
In 2015/16, we set ourselves a clear ambition to ensure we have no EMS vacancies by April 2016. Good progress has been made towards this; however, challenges continue to face our EMS workforce and current vacancy projections for April 2016 estimate we will have:
approximately 7 WTE paramedic vacancies;
an over-establishment of approximately 2 WTE Advanced / Emergency Medical Technicians;
approximately 4 WTE Urgent Care staff vacancies; and
approximately 9 WTE Advanced Paramedic Practitioner vacancies. Recruitment of Qualified Paramedics
Our workforce plan illustrates that, over the course of the three years, we have commissioned sufficient student placements to meet demand for paramedic staff within our current staffing model. However, on an annual basis, demand is likely to exceed supply at different points of the year because of natural turnover. This is at least until October each year when we will see the paramedic degree course student outturn. One of our key aims is to retain the majority (if not all) of those students who train and qualify in Wales, and take swift action to employ them.
Recruitment to paramedic posts continues to be a challenge nationally, and action is needed to get us to full establishment and ensure we stay ahead of the recruitment curve. Changes to terms and conditions and changes to paramedic banding in some ambulance services in England also present a recruitment and retention challenge to us. Over the next three years, we aim to ensure we are able to move to a place where we can
confidently make a contingent offer of employment to all HEI students on commencement of their
diploma or degree subject to successful completion of their studies and practice placement training.
Our ability to do this is dependent upon robust workforce planning.
We will work closely with our colleagues in Swansea University over the HEI intake and ensure we maintain close contact and communication with the student cohort at regular points in the year, taking the opportunity to promote the Trust as a great place to work, including our preceptorship programme and clinical support mechanisms. In the future, we hope to create opportunity for our Practice Placement Manager to sit on student course interviews, which in effect becomes a WAST job interview too. Action 60: Ensure focus on ongoing recruitment activity to fill vacant posts whilst work in
progress to complete the demand / capacity work and future workforce requirements.
Action 61: Continue to develop links with the military careers services and other potential
partners.
Advanced Paramedic Practitioners
Our workforce planning has also highlighted a growing problem with the retention of Advanced Paramedic Practitioners (APPs), as a result of them leaving to take up posts in Health Boards and universities in 2015/16. Filling the APP vacancies from our existing staff will place an additional drain on our paramedic workforce. Our current APP educational programmes will deliver the following qualified staff over the next three years: July 2016 – 7 WTE; July 2017 – 13 WTE; July 2018 – 15 WTE. We have commenced work with our APPs and staff representatives to review the APP role and remit as senior clinical leaders, the reporting arrangements and explored how we can systematically support them to meet the four pillars of advanced practice.

134
We will take a proactive stance with Health Board colleagues in a prudent approach to identify opportunities to place our APPs, and paramedics at the very heart of the urgent unscheduled care system. This could provide a sustainable solution to some of the challenges facing Health Boards, and an important opportunity for APPs to diversify in their practice by rotating across EMS, primary and other community-based areas of care, thereby supporting CPD and potentially addressing retention issues. Action 62: Review the number of APPs in training for future years, scope proposal to develop
workforce modelling tool with WEDS to facilitate this action.
Action 63: Progress proposal for the development of a structured approach for newly qualified APP’s to make the transition from novice to expert.
At present, we do not experience or foresee any future difficulties in recruiting to our Advanced / Emergency Medical Technician, Urgent Care, Call Taker, Patient Care Services or nursing workforce. Recent recruitment of call takers and nurses to NHS Direct Wales in advance of the 111 Pathfinder was successful. However, this does have a potentially negative impact on Health Boards losing qualified nursing staff to WAST. As the Pathfinder progresses, we will need to consider the broader impact of 111 recruitment activities.
Reducing Time to Hire
In 2015/16 our recruitment task and finish group was tasked to identify opportunities to streamline recruitment processes, reduce time to hire and ensuring safe hire of new staff.
The group has supported the work to confirm vacancy requirements and successfully developed a recruitment plan aligned to a training plan. This group also facilitated a process mapping workshop to identify opportunities to streamline recruitment processes, organised targeted recruitment training sessions (supported by NWSSP), introduced a recruitment link advisor role into the WOD structure and piloted a new approach to bulk recruitment, a “One Stop Shop” approach for Paramedic, EMT and UCS. As a result there has been a significant improvement on the average time to recruit – and an improving downward trend shown in the table below, which compares performance in December 2014 and then 2015, and January 2015 and then 2016.
Average time to recruit (in days)
Date All Wales average WAST
December 2014 69.9 119.4
December 2015 65.2 90
Date All Wales average WAST
January 2015 83.2 169
January 2016 70.5 82.8
However, we believe there is more we can do to further reduce time to hire, particularly by reviewing the process map and targeting constraints experienced within our Occupational Health service.

135
Action 64: To work in partnership with NWSSP and Occupational Health to review the recruitment process map to identify opportunities to further reduce time to hire to achieve the average all Wales target.
There are a number of risks and sensitivities within the Trust’s workforce plan which we continue to work to mitigate. These are described further in section 7.3.
Education, Training and Development of Our People
Rising unscheduled care demand for individuals with long term conditions has
been identified as a major challenge for the NHS in Wales, resulting in a call
for more care to be delivered closer to home in an out-of-hospital community
setting. Redesigning new clinical roles and patient pathways, driving up the
quality of clinical care and decision-making is taking on an increasing
importance and presents a challenge and opportunity for the Trust.
Ambulance education is also evolving in terms of developments to degree level education
(registrant – Paramedic) and a change to the accrediting body (pre-registrant education - EMT).
Additionally, there are imminent legislative and accrediting body changes in relation to driver
education.
The importance of ensuring effective high quality clinical leadership, education and development
therefore cannot be understated and remains a key priority for us in 2016/17 and beyond.
We recognise that, to safely and effectively clinically modernise service delivery and implement
programmes of change, we need to ensure any improvements predicted by these initiatives are fully
supported by an informed, innovative and professional clinical workforce. Clinical leadership in this
context is best facilitated by those clinicians who deliver patient care so they can positively support
and influence others to change whilst continually improving the quality of care delivered.
National Ambulance Training College (NATC)
Training and education for the bulk of our staff is delivered through our National Ambulance Training College (NATC). To support the education and development of our staff, it is imperative that we work with our partners such as Swansea University to ensure we have an education function that is ‘future-proof’ and clinically excellent, through which we can deliver the range of education and learning interventions required in light of the changing educational models and increasing clinical standards.
We are considering the potential for a consultant paramedic post within our Training and Education team to lead development of a training and education strategy, in response to the changing educational requirements of the New Clinical Response Model and demographic drivers. This would also support us to ensure we create a fit for purpose collaborative HEI curriculum and readiness for introduction of a Paramedic Science degree programme requirements for all new paramedics.
Action 65: Scope the proposal to create a consultant paramedic role with a lead for clinical training and education
The NATC provides leadership to all educational programmes to equip Ambulance Service
personnel with the essential knowledge, skills and behaviours to allow them to respond safely and
deliver evidence-based high quality, safe care to our patients. With growing expectation placed
upon the delivery of pre-hospital care, there has been a commitment to develop and deliver
expanding educational and training programmes to meet the continued education and development
needs of the Trust and its staff. NATC also provides induction and CPD for all clinical and non-

136
clinical staff in-house, through our National Ambulance Training College facilities in Swansea and
associated regional training centres, which are IHCD and Future Quals accredited.
At present, the NATC Team consists of 11 Learning & Development Managers, who cater for the
educational needs of circa 2,500 members of staff. A benchmarking exercise against other UK
ambulance trusts has identified a deficit in terms of existing tutor: student ratio, and goes some way
to understanding some of the constraints in capacity to deliver training courses to meet ad hoc
demand experience. This exercise points to a requirement for an additional circa 13 Learning &
Development Managers to match national ratios.
Over the next three years, we will be working with colleagues in the Clinical Directorate and National
Ambulance Training Centre to address capacity constraints and ensure our education, training and
development facilities and programmes are fit for future purpose.
Future estates changes also indicate that Central and West Headquarters at our Cefn Coed site
(National Ambulance Training College) will be required to relocate by 2018.
Our ambition is to develop our National Ambulance Training College into a flagship training facility,
recognised as a centre of excellence with state of the art training facilities by 2019. During 2016/17,
we will scope and develop a business case and plan that will seek to address the capacity
constraints, estate challenge and opportunities presented by technology, ensuring we also seek
collaborative solutions with partners such as Swansea University.
Action 66: Develop the business case and plan for the transformation of the NATC
The NATC continues to progress its proposals for the provision of a Virtual Learning Environment
for staff and a fully functional and effective e-learning platform that will provide students and tutors
with state of the art, innovative learning and reference materials and tools. A business case for the
purchase of tablet devices has been approved for 2016/17, which will not only improve the learning
experience for students and lead the way in terms of ambulance education, but will also reduce
costs associated with purchase and issue of key reading materials for WAST education
programmes. These technological advances will ensure WAST is equipped to embed the principles
of the NHS Wales Technology Enabled Learning (TEL) strategy.
Action 67: Develop eLearning portfolio for all WAST staff
Action 68: Introduce bespoke eLearning platform for Driver Education
Action 69: Expand and develop bespoke eLearning platform to include clinical education
The NHS Direct Wales Practice and Service Development Team also works independently to
provide education, training and professional development for all disciplines of NHSDW Clinical
Contact Centre staff, as well as in collaboration with the NATC to schedule programmes of
mandatory and statutory training through the Team’s annual CPD plan.
Continuing Professional Development
We have already touched on the opportunity for the Trust to make a significant contribution to patient flow across the unscheduled care system, and that demand for ambulance clinicians and managers to take highly complex decisions on patient care and management is increasing. It is therefore imperative that any future CPD programmes address the professional, legal and ethical dimensions of decision-making, including duty of care, to ensure the Trust delivers safe and effective patient-centred clinical services.
Embracing the notion of a shared ‘decision making framework’ for both clinicians and operational
managers, the Trust’s CPD programmes must be aimed at increasing clinician confidence in

137
professional reasoning, increasing their influencing and negotiating skills and foster individual and
team understanding of collaborative practice and how clinical decisions are effectively
communicated. Central to this approach will be to enable clinicians and managers to reflect ‘in’ and
‘on’ both clinical and managerial practice using a recognised model to achieve safe and effective
care. The subject matter of CPD will be informed by lessons learnt from SAIs, research and audit,
changes to clinical practice guidelines and will be informed by trends and themes recorded in staff
PADRs, for all staff groups.
Our workforce has a fantastic appetite for learning. The Workforce Development Team has recently
devised a ‘Voluntary CPD Programme’ that will be rolled out from 1 April 2016. These sessions will
be delivered by our operational tutors across the country and will cover a range of topics.
It is also planned to introduce a modular approach to training and education for the development of
the existing paramedic workforce. This requires consideration of available HEI modules pan Wales
and identification of supporting funding streams (WEDS). It is anticipated that this will enhance skills
such as chronic disease management and clinical decision-making.
We have revised our Study Leave Policy to ensure managers can provide equitable support to all
staff groups who wish to undertake formalised education and development. In addition to this, there
are various funding streams available to our staff to support specific career development e.g.
Bespoke EMT to Paramedic Conversion programme, MSc in Advanced Practice (for both
paramedic and nurse registrants), NVQ and vocational funding for all staff groups e.g. ILM, NVQs.
In 2016, we will also launch a new Staff Bursary Scheme to create opportunity for staff to apply for
financial support for their professional research and / or development. However, there is a need to
consider a centralised training budget within the Trust to further support all staff development
opportunities, and this will be considered as part of our budget setting discussions.
Based upon internal evaluation and external quality assurance mechanisms, the NHSDW Team
delivers high quality education in the classroom setting, as well as developing excellence in the
clinical practice environment, through coaching and performance support activities. Induction
courses for all disciplines of call-taking staff are academically accredited. Additionally, the Team
developed an accredited mentorship course for HCSW level staff, which has now been rolled out
across other areas of the Trust by the NATC. Currently, the Team is working alongside external
experts to develop a series of e-learning modules to support mental health learning for all CCC staff
on the Learning@NHSWales platform.
The Team’s approach to NHSDW induction and CPD activities strives to equip staff with excellence
in their practical skills, with an underpinning emphasis upon compassion, respect and dignity for
patients and callers and a sound understanding of prudent healthcare principles. These elements of
clinical practice are run as themes through all learning.
The Team works closely with operational colleagues to ensure that NHSDW appropriately invests in
workplace and HEI education and training. Our strategy provides staff with an opportunity to
constantly evaluate their practice against evidence based healthcare guidelines and research. This
approach evolves alongside developments in the sphere of adult education by identifying
opportunities to innovatively embed supported, self-directed learning for our staff. By taking this
approach, we aim to teach our staff how to learn independently, as well as providing them with new
skills and knowledge.
Action 70: Compilation of an extensive CPD directory for all staff groups with regard to learning
and funding opportunities and a CPD Programme that reflects current and future

138
changes to clinical practice, learning from adverse incidents and development needs
identified through the PADR process
Action 71: Benchmark skills development for existing, vocationally trained paramedic staff e.g.
commissioning of HEI educational modules
We currently receive funding from the Workforce, Education & Development Services (WEDS) on
an annual basis, for the release and backfill (single time) of Paramedic staff to attend annual CPD
refresher training. This funding is accounted for by the Trust’s Finance Department as income for
the year and as such, there are significant financial, as well as patient safety and legislative
implications if the Trust does not ensure that every paramedic attends the annual refresher
programme.
Action 72: Seek support to create an appropriate education and development budget to support
staff in achieving their professional development needs.
The following chart (Figure 22) illustrates Trust-wide CPD Compliance by directorate and discipline
as at 31st January 2016:
Figure 22: Trust Wide CPD Compliance
Attendance at CPD sessions is reported on a monthly basis and shared with relevant managers,
with a regular review by the Senior Management Team (SMT) and Executive Management Team
(EMT).
Statutory and Mandatory Training
Completion of statutory and mandatory training is a legal requirement of every member of staff and
the importance of this cannot be overstated. Failure to comply with Statutory& Mandatory training
requirements could pose a significant risk to the Trust with regard to patient safety, litigation,
legislative requirements, staff competence and confidence. We have identified a number of
constraints affecting compliance rates, including reluctance of staff and managers to adhere to the
agreed KSF Hours CPD allocation process and restrictions on staff release because of operational
demands.
The statutory and mandatory training programme for corporate areas has been rolled out via
eLearning across the Trust for the last two years. Significant focus is being paid to improving
compliance rates for this group of staff, with key performance figures shared with managers on a
regular basis.

139
The WD Team plans and delivers all statutory and mandatory training requirements for NHSDW and
CCC staff, in conjunction with the Quality and Nursing Directorate. The remit for systems and
clinical updates for this group of staff remain with the respective Heads of Operations.
At present, we are unable to report against our statutory and mandatory training compliance targets
because of system difficulties in the set-up of ESR and OLM. This is currently under review to re-
establish the link and ensure we can implement reporting and monitoring arrangements.
Action 73: Work with the operations teams to improve CPD and Statutory Mandatory Training
Compliance to ensure targets are met
Action 74: Strengthen the link role of Learning & Development Managers with
Operational teams to discuss compliance at locality level during briefings
Action 75: Maximise use of the business intelligence reporting mechanism of OLM.
HCSW Framework & Development Needs
The Trust has appointed a project lead and small team, sponsored by WEDS, to fully implement
and integrate the Framework and its associated agenda in WAST. This is being driven through
WEDG and consists of three phases delivered over three years, to ensure compliance by the
mandated deadline of 2018. Post year one, consideration will need to be given to acquisition of
funding for the continuation of this team.
Action 76: Progress the WEDG HCSW Development Agenda workstream.
Action 77: Develop apprenticeship opportunities within WAST in line with Government mandate
and to mirror best practice in other UK ambulance Trusts
Organisational Development Plan
We are part way into a longer term OD plan that started several years ago to transform the Trust. So far we have redesigned the structure of the Trust, developed overarching principles/approaches and focused on leadership behaviours to help the transformation.
In this time, we have seen a change to the Executive Team and Board members, and many new faces join the Trust. This has brought fresh
thinking, new ideas and a new drive for culture change across the organisation.
Our Approach to OD
The underpinning principles are based on the very best practices and NHS Wales policies (e.g. Prudent Healthcare). They are:
use evidence-based approaches: e.g. neuro-science, psychology, team-based working etc.;
“power is where decisions are made”; the safest and highest quality decisions are made by those close to the issues; limited number of core parameters with as much choice for individuals/teams as possible;
the Trust needs to rebalance quantity and quality so overt focus on behaviours;
transformation requires disruption by breaking the norm; and
continuously reinforce.
The Francis Report (2013) highlighted the importance of setting and embedding a culture of
openness, candour and good care as fundamental to the delivery of high quality safe services to our

140
population. For WAST, this is set out in Being Our Best, which clearly articulates the actions we
believe are needed to achieve the transformational change required to deliver both the outcomes of
the Francis report and the Trusted to Care report to support the step change in culture, systems and
leadership we need.
There is an increasing knowledge base about effective OD, with NHS Employers suggesting that
there are High Impact Changes that organisations need to focus on to deliver great services. These
are intertwined throughout Being Our Best as they focus on: developing local evidence-based
solutions; trusting and empowering visible leadership at all levels; sufficient management capacity
and capability; excellent health and well-being support services; colleagues having as much
personal responsibility as possible.
Our Approach to Colleague Participation, Engagement & Empowerment
Why this is essential for WAST:
patient safety is determined by how engaged people are in their work (West); clinician behaviour determines quality of care; this is underpinned by how they feel about
work; community/primary care is the unknown: clinicians can only give their best healthcare if they
are trusted to do their best within as loose parameters as possible; and high levels of participation and engagement lead to less conflict and, therefore, a more
productive workplace.
Our Evidence-Based Principles:
“power is where decisions are made”: the best decisions are made closest to the issue; we each need as much as choice as possible about what we do and how we do it; we each need to be very clear and know what we’re trying to achieve and how we need to
do it; listening is the single most dignified thing that someone can do; dignity builds respect with
respect building trust; many colleagues work remotely and have little contact with each other; human relationships
and interactions create warmth and belonging, so every opportunity needs to be taken to get people together and build relationships to strengthen belonging;
strong employee engagement is a positive indicator for employee well-being and will have a positive impact on our sickness absence rates.
The OD challenge and opportunity for leadership is to lead, model and support a move from processes to people. This will be done through:
taking every opportunity to have clear parameters (outcomes and rules) and encouraging colleagues to be themselves so that they fully participate and own their actions and behaviours;
taking every opportunity to support every individual and team to develop their OD capacity so that they can do the right things in the right way; and
creating Trust-wide systems, processes and approaches to help individuals and teams to perform to their best.
During 2016-17, we will implement our action plan to assist colleagues to understand and live the
shared behaviours, vision and purpose including selection processes, PADRs, team meetings,
performance frameworks, award systems and Board focus. This action plan is described in Section
3 of this document.

141
During 2017-18, we will take the opportunity to review the impact of our approaches as well as
reviewing the shared behaviours. We will collaboratively update the behaviours and approaches as
appropriate.
Action 78: To develop an appropriate evaluation framework and mechanism to enable
assessment of the impact of communicating shared behaviours and culture change
How we help people to be involved, participate and take real ownership
Welcoming New Colleagues All colleagues should expect to be warmly welcomed into the Trust both corporately and locally with their team. Both welcomes should emphasise the importance of each individual being their unique best within the Trust/local parameters. In 2015/16, 71% of new starters were released to attend our colleague welcome days. We aim to ensure 100% of all new starters receive an induction to the Trust. We will support all teams and managers to understand the importance of welcoming new colleagues and the focus on recognising their unique individuality.
Action 79: Review local induction arrangements to ensure the Trust’s expectations of shared
behaviours are reinforced and 100% of new starters receive induction.
Personal Appraisal and Development Reviews
Every member of staff has a right to receive an annual appraisal, and we have been working hard to
ensure robust measures are in place to monitor and report Personnel Annual Development Review
(PADR) compliance on a monthly basis. In 2015/16, we set a challenging target of 85% compliance
by 31st March 2016. Significant improvement has been made since early 2015 when reported rate
on ESR was less than 10%. As at 1st March 2016, we are reporting a completion rate of nearly
60%.
Our focus during 2015/16 has been to ensure that not only do we achieve our compliance target,
but that the quality of the PADR is also improved. There has been significant focus on supporting
colleagues with both the quality and quantity of PADRs as ‘career conversations’ and this work will
continue in 2016/17. The work to continue improvement in this area includes:
supporting Team Leaders and Middle Managers with understanding their role and developing their skills and behaviours. This has included listening skills and using appreciative inquiry;
supporting colleagues to want to participate and take ownership of their PADR. This has included a “marketing” plan; and
using pulse surveys to review the quality of PADRs and testing “user-friendly” ways of inputting PADR information onto ESR, including the production of a video for managers. The feedback from many colleagues is that currently PADRs have not been of sufficiently high quality to be beneficial, as the balance has been on managing performance rather than being supportive.

142
Therefore, the Trust will focus its actions on developing improved qualitative approaches during the course of the IMTP.
As a result of both improved quantity and quality of relationship and focus, individuals will become more engaged, increasingly effective in delivering appropriate patient care and will experience and encourage high levels of trust with patients and colleagues. These will be measured through a range of measures including quantitative and qualitative patient and colleague experience measures (e.g. pulse surveys, patient outcomes, patient stories, accolades/complaints). Further evaluation of this will be undertaken following the staff survey in 2016. Action 80: Achieve a PADR target of 85% by 31st March 2017 through vigorous focus on the
importance, quality and quantity of PADRs with managers and their team members.
Pulse/Staff Surveys
Giving and receiving feedback provides a common theme throughout our IMTP. In order to improve,
it is essential to know how we are doing. The knowledge gained from the feedback helps us make
better decisions. The act of taking part in surveys, receiving and using immediate feedback and
being part of making decisions about improvements are known to be an excellent way of improving
participation and ownership. Importantly, the evidence-based actions will become integral to each
team’s Local Delivery Plans and not stand-alone actions.
To help improve our knowledge of colleagues’ experiences of the workplace, we have used a series
of pulse surveys so that the information can be used to inform groups, teams and individuals to
make decisions with a better understanding of their colleagues’ perspectives. Additionally, we have
actively encouraged groups and teams to run their own surveys. Preparations are being made for
the roll-out of the next NHS Wales Staff Survey in June 2016. We will work in partnership with TU
colleagues to help raise participation and engagement levels through supporting colleagues to
actively take part. We aim to improve on the participation rates from the baseline of 30% in 2013 to
50% in 2016.
During 2016-17, we will:
Action 81: Work in partnership with TU colleagues to use the data from the survey to help support
development of local and organisational action plans as part of each team’s LDP.
Action 82: Implement a monthly pulse survey using the engagement index to provide ongoing
assessment
During 2017-19, we will:
Action 83: Implement a system to provide real time feedback on colleagues’ experiences of work;
this will provide information to enable proactive decisions to be made to improve day to
day experiences of the workplace, linked to annual PADR
Team and Identity
We recognise how important it is for our staff to know and feel connected to their closest work
colleagues. For most of us, this takes place within a team setting. We will continue to ensure that
every team has sufficient time to understand, plan and deliver its requirements, including making
sure that the team focuses on its own development.
Action 84: Support leaders and develop systems to value team meetings, and apply principles
of team development to achieve improved team performance and success.
Staff Appreciation and Recognition

143
We have collaboratively developed a shared vision, purpose and set of behaviours. Along with the
annual priorities, these will be widely publicised to support colleagues. In particular, the Trust will
reward and award colleagues who live the behaviours as these will be accessible and within the
circle of control for every colleague.
Highlighting and rewarding excellence is an important way of reinforcing the actions and behaviours
we expect from colleagues. As we have collaboratively developed a shared vision, purpose and set
of behaviours and these are a crucial focus for us because they are measurable, they will be the
focus for our Staff Appreciation Awards.
Other actions that we will actively model and encourage are:
always find a positive first; smile (it’s contagious); say “thank you”; give someone a thank
you note;
use Twitter and Siren to publish a “kudos” or ‘thank you’ column;
recognise people who show initiative by creating opportunities for them to get involved
with or lead specific projects or pieces of work as part of development;
arrange for teams or individuals to present their ideas or the results of their efforts to others
at learning events, team meetings and the Executive Team and create colleague story
boards;
senior leaders (Heads of Operations, Execs etc) to meet colleagues in person to thank
individuals and teams;
write a letter of praise recognising specific contributions and achievements; send a copy
to senior management and the employee’s personnel file;
share positive feedback with an individual when you hear something positive about them
as soon as possible (face-to-face is best); create and share your own positives about
someone with others;
create a ‘hall of fame’ wall with photos of outstanding employees in reception at VPH but
also at stations;
develop a colleague of the month scheme in directorates (e.g. Health Board level) based
on feedback from colleagues and the public; and
create an employee recognition event to publically celebrate success and achievements.
Therefore, our key action for 2016-17 is to:
Action 85: Review and expand our opportunities to recognise staff for their broader contribution,
celebrate success and recognise excellence through development of our
‘Appreciating our People’ Awards Ceremony
Mentors and Coaches
Helping each colleague understand the choices that they have in their work can be a vital role for a
coach or mentor. We will continue to actively support all colleagues to access a coach or mentor
(either from within WAST or from the broader public services). Colleagues can also expect to
access internal or external mentoring support via their manager or teams to help coach them but
also provide appropriate advice.
Action 86: Build links with partners across the public sector with a renewed focus on supporting
colleagues to “ask and listen” including refreshing the coaching and mentoring plan to
ensure everyone can access coaching and mentoring and there is sufficient capacity.

144
Personal Development
Research-based evidence of levels of engagement within UK healthcare highlights the importance
of developmental development – i.e. development that is over and above the requirements to meet
the job. This is highlighted as the second most important factor in determining engagement and
participation levels. Therefore, the Trust corporately, and each manager, should always support
individuals to develop to know and achieve their ambition so that they achieve their full potential.
Action 87: Develop the Trust’s approach to succession planning, career planning and career
pathways from April 2016 with an ongoing focus of supporting individuals to fulfil their
potential.
Management and Leadership Development
The relationship each of us has with our manager is the single biggest determinant as to how we
feel about work and, therefore, our levels of engagement and participation. Many of the approaches
identified in this IMTP rest on good leadership and management practices. In particular, the ability
to ‘actively listen’ has not been a visible part of the management culture. Therefore, a key part of
our approach to supporting colleagues to be involved and participate is developing managers and
leaders with their knowledge, skills, behaviours and, above all, beliefs.
Action 88: Create and market leadership development opportunities through the
development of a prospectus for all staff
Action 89: Develop and implement a management passport to support managers to have
appropriate capability and confidence to manage their teams and services.
Action 90: Undertake a review of where decisions are made across the Trust and the impact of
these; highlight adverse consequences and implement system changes to improve
its organisational effectiveness
Driving Forward Clinical Leadership
Driving forward clinical leadership across the Trust is a vital part of our overall leadership development plan. Traditionally, within the ambulance service, clinical leadership has been seen to come from senior clinicians with management responsibility i.e. Medical, Paramedic and Nursing Directors. More recently, however, the increasing levels of clinical decision-making responsibility that ambulance clinicians are asked to take when assessing and managing patients at home, suggests there is a far greater need for clinical leadership through all levels of the service.
Our Clinical Leadership Development Plan will ensure an appropriate structure is in place to
encourage clinical leadership throughout WAST, made more important because of increasing levels
of clinical decision-making at the patient interface. We have already made progress towards
improving clinical leadership within the Trust – reviewing the importance of the Advanced
Paramedic Practitioner role, proposing a clinical leadership structure and also taking steps to
improve access to clinical supervision.
We aim to further support and challenge all clinicians to understand and develop their own and
others’ clinical practice. This will be based on a range of indicators, evidence and feedback across
multi-professional teams and groups. Additionally, existing and potential clinical team leaders will
also need to be developed in the underpinning theories of leadership and management of change
within the clinical practice setting. We will do this through the development and implementation of

145
action learning workshops across the Trust, to facilitate a greater understanding of clinical
leadership across a wider range of clinical disciplines, grades and groups in the Trust.
Executive and Board Development A programme of development for the Executive Team has been established to explore and develop how this new team is going to provide leadership for the Trust. The sessions have included the opportunity to explore what type of Director is required and to open up discussions regarding Director portfolios. A team profile has been produced using Myers Briggs Type Inventory (MBTI) and Thomas – Kilmann Conflict Mode Tool (TK); although neither of these tools was new to the Executive Team, the production of the team profile has proved helpful to explore in the context of:
MBTI: the impact preferences and behaviours can have on team effectiveness.
TK: an indication of individual’s preferences for dealing with conflict and the effectiveness and appropriateness of the use of each.
Further development sessions, including some joint sessions with the Heads of Operations, on a quarterly basis are scheduled for the next 18 months. This will further strengthen the team to provide effective leadership for the Trust. An integral part of the Executive Team development to date has been the development of an Executive Team Charter as a statement of intent and commitment to a set of behaviours and operating principles in their interactions as a team, and also their leadership and management of the Trust. A Board Development Programme has also been established, to support the Board in understanding its accountabilities, and also to develop as a team together. A series of ‘two at the top’ development sessions have been run for the Chair and Chief Executive, and will now be run for individual pairings of Director and Non-Executive Directors with common portfolios.
Effective Partnerships
Working collaboratively for the greater good is at the heart of the Trust’s redesign. The evidence of the “wisdom of crowds”, “nothing about me without me” and that “two heads are better than one” underpin the Prudent Healthcare principles. Involving everyone in developing the future and making decisions about how to get there not only prevents avoidable conflict but it promotes ownership. Where people own things, they are significantly more likely to happen. Our external partnerships have flourished through realigning our management structures with partner organisations (particularly Health Boards). This has enabled collaborative teams to identify local issues and create local solutions to meet local needs. These partnerships need further support and development as together teams understand the needs of local communities and plan and deliver services to meet these. Internally, we will continue to support colleagues to understand the importance of trusting each other, collaboration and working together. This is at all levels of the Trust and includes the relationship between managers and their teams, within teams and across teams (both internal and external). We have seen significant improvements with our partnership working between trade union representatives and managers through our Go Together Go Far programme. During 2016-19, the ongoing actions we will take are: Action 91: Develop planned activities that support individuals and teams to understand the
benefits of trusting each other and working together; support individuals to develop
their partnership capabilities including skills and approaches through our leadership
development plans

146
Action 92: Support and encourage individuals and local teams to develop relationships across the
Public Services in Wales
Health and Well-being
Our continuing commitment to improving the health and well-being of all our staff has been described earlier in this section. In terms of our plans for this, in 2016/17 we will continue our efforts to embed employee health and well-being into the culture of the organisation by ensuring a robust action plan and that appropriate systems and processes are in place to encourage and enable staff to be responsible for their own well-being. Our overall aim is to achieve Gold Corporate Health Standard status by the end of 2016, and
Platinum by 2018. An action plan is in place to support the ambition to achieve Gold status.
The Trust has refreshed and re-launched its Health and Well-being Steering Group, chaired by the Director of Workforce and OD, and a full range of actions are planned to develop our services to staff. We will also ensure we make links to work ongoing at an all Wales level, led by the NHS Wales Directors of Workforce and OD. In 2016/17, our primary focus will be on supporting good mental health and the management of pressure.
We will work with partners to seek ways to reduce mental health stigma in the workplace,
building a proposal to introduce a system of psychological assessment of risk
programme (TRiM), roll out of Mental Health First Aid training and developing a focused
stress recognition and awareness training programme. We will also roll out across the
Trust o the ‘Looking after your Well-being and Managing Stress’ leaflets.
We will champion lifestyle improvements through the promotion of workplace challenges and team events and promotion of healthy options i.e. mindfulness, standing desks, take the stairs campaign etc.
We plan to further develop our in-house health-screening services to incorporate night workers screening, bi-annual health screening and voluntary health checks.
Our flu vaccination programme failed to deliver the expected levels of frontline staff vaccinations to meet the Welsh Government target in 2015/16. We therefore plan to review our delivery plan and capacity, with a view to commencing our planning at a much earlier stage of the year in 2016.
We will continue to develop proposals for staff benefits which include the launch of car lease and computer salary sacrifice schemes alongside, cycle scheme, and childcare vouchers.
Action 93: We will sign the Welsh Government ‘Time to Change Wales’ campaign pledge in
April/ May 2016
Action 94: Pending successful achievement of Gold status, prepare action plan to help us gain
the Corporate Health Standard Platinum accreditation

147
6.2 Our Finances Overview
WAST has recently implemented a number of service developments that are focused on delivering
the best outcomes for patients and improving performance. At this stage, some of these
developments have been introduced on a pilot basis. The full service, activity, performance and
subsequent financial impact of these significant developments will continue to be assessed and
refined in line with emerging evidence and evaluation and, where appropriate, factored into the
financial plan.
The implementation of the New Clinical Response Model is very likely to have a significant impact
on the resources required to deliver the service. There will be a fundamental review of the skill mix
of staff required to maximise the benefit of the new model along with the potential change in fleet
requirements. Similarly, there are further key service developments planned for implementation over
the immediate and medium term that will increase productivity and efficiency and enhance services.
On top of this, WAST has been selected as the host provider for the 111 pathfinder project.
A strategic approach has been taken to the development of a Medium Term Financial Plan that will
address both immediate financial requirements, but will also need to remain flexible to adapt to
service change. As part of this approach it is vital that the effects of service change and the
resultant financial impacts are considered at a system wide level and that resource and investment
plans reflect the principles that underpin prudent healthcare. This includes working in conjunction
with the Trust’s commissioners. Similarly, there is a drive to further increase efficiency, to ensure
value for money and to maximise the benefits of the resources available. This will be a key focus in
the IMTP, with the scrutiny of costs and financial governance central to the delivery of our vision for
a caring and responsive ambulance service for people in Wales.
To achieve this, we will work both internally within the organisation to ensure that there is cohesion
between financial, workforce and service planning to support decision making and to optimise
service delivery and also with our partners, including the Chief Ambulance Services Commissioner
(CASC) and the Emergency Ambulance Services Committee (EASC). This will include exploring
opportunities for further collaborative working, such as estates, but also the potential to establish
joint posts that could provide both financial and service benefits across health and emergency
service partners.
Whilst the Integrated Medium Term Plan looks forward over the next three years, it is evident that,
for WAST, there are a number of significant service changes which will impact during this period.
This financial plan is being developed based on a number of current assumptions, but also
recognises the need for a level of agility to be able to respond to service change.
The finance resources have been modelled on the basis of current performance targets, no change
to the targets have been accounted for. The sensitivity of our plan to any changes will be scenario
tested via the demand and capacity work.
Similarly, we have assumed that where Local Health Boards make major service changes, the
impact on our services (emergency or non emergency) will be fully resourced via their business
case mechanisms and routed through the commissioning arrangements
The current revenue financial position – 2015/16
At the end of February (month 11), the Trust continues to forecast a small surplus (£0.150m) for the
financial year 2015/16. This position is inclusive of additional planned costs associated with specific
actions agreed to increase operational capacity, which have delivered performance improvements

148
in 2015/16, and have enabled schemes such as the Cwm Taf Explorer pilot. Additional non-
recurring income of £3.5m has been provided by Welsh Government to offset these costs. On this
basis, the Trust is on target to meet each of the statutory financial duties in 2015/16.
Figure 23 below presents a summary of the Trust’s financial position for the year to date at 29
February and the forecast year end outturn for 2015/16.
Figure 23: Financial Position at 29th February 2016
It is anticipated that to maintain capacity and performance improvement, elements of the planned
additional costs in relation to EMS will continue into 2016/17. This is an assumption that has been
fully recognised by the commissioners.
Future year revenue financial planning assumptions
WAST receives the vast majority (more than 80%) of its income through a commissioning arrangement, led by the Chief Ambulance Services Commissioner, who acts on behalf of all Welsh Health Boards on the commissioning of Emergency Ambulance Services. This arrangement is conducted through the Emergency Ambulance Services Committee (EASC), which is responsible
Financial position at 29 February 2016
Plan Actual Variance Annual Annual Annual
YTD YTD YTD Plan Forecast Variance
£000s £000s £000s £000s £000s £000s
INCOME
Welsh NHS Local Health Boards 16,273 16,317 44 17,756 19,161 1,405
Welsh NHS Trusts 728 729 1 794 811 17
WHSSC 116,987 117,037 50 128,066 129,384 1,318
Welsh Government 787 4,019 3,232 4,281 4,281 0
English NHS Organisations 174 199 25 190 217 27
Other Operating income 2,666 2,775 109 2,905 3,027 122
Other Income 6,200 6,950 750 3,046 4,624 1,578
Total Income 143,815 148,026 4,211 157,038 161,505 4,467
EXPENDITURE
Pay - Sub Total 102,615 104,877 2,262 111,806 114,449 2,643
Non Pay - sub total 29,624 31,310 1,686 32,535 34,181 1,646
Total Expenditure 132,239 136,187 3,948 144,341 148,630 4,289
Non allocated contingency 118 0 -118 283 0 -283
Unidentified Savings target -131 0 131 -173 0 173
Profit / Loss on asset disposal -217 -87 130 -237 -87 150
DEL - Depreciation, Accelerated Depreciation & Impairments 11,008 11,008 0 12,009 12,009 0
AME - Depreciation & Impairments 606 606 0 606 606 0
Total Interest Receivable -29 -35 -6 -32 -37 -5
Total Interest Payable 221 214 -7 241 234 -7
Net Surplus / (Deficit) 0 133 133 0 150 150

149
for developing collective commissioning intentions and plans. Welsh Government incorporates funding for ambulance services as part of the allocations made to NHS organisations. It is expected that national, NHS-wide, planning assumptions, including funding uplifts, will be equally relevant to commissioning agreements and financial plans for WAST have been developed on this basis.
The key financial assumptions within the Trust’s three-year financial plan are:
National position
The UK Government spending review announced an increase in NHS revenue expenditure over the next five years. The Welsh Government draft budget similarly provided for an increase in 2016/17. The headline figures indicate plans for an additional £293.5m for the NHS in Wales.
This increase is against the 2015/16 baseline and consists of £260m revenue to support:
core NHS delivery £200m;
intermediate Care Fund £30m;
older people and mental health services £30m; plus
an additional £33.5m capital.
Of the additional £260m revenue funding, £60m is targeted to specific programme areas. The increase of £200m to core NHS delivery represents an increase of 3.2% on health budgets.
WHC (2015) 059 provides detail in relation to the initial 2016/17 Health Board Revenue Allocations and whist the allocations at this stage are incomplete in that they do not include the £200m additional funding, it is indicated that for planning purposes that this funding will be available to support the costs of inflation and other cost pressures, by way of the following paragraph:
“For planning purposes Health Boards can plan on the basis that the £200 million funding will be allocated to NHS organisations to meet these pressures, including the costs of 2016/17 pay awards, and will be distributed primarily using population shares.”
It is assumed that once this uplift is reflected in LHB Allocations, there will be a corresponding increase to the commissioning agreements with WAST. For 2016/17, a “fair share” of this £200m has been estimated at £5m within the Trust’s financial plan, and this IMTP therefore.
Similarly assumptions have been made in relation to the levels of uplift to be applied for 2017/18 and 2018/19 and that these will be applied on a fair shares basis across all NHS organisations in Wales.
On this basis the expected share for the Trust has been estimated based on a 3.2% uplift in
2016/17 providing for a fair share of the £200m additional NHS core funding of £5.0m, and for
the years 2017/18 and 2018/19 uplifts of £4.0m and £4.5m respectively.
Inflation and unavoidable costs
Figure 24 below presents the costs that have been calculated demonstrating how inflation is likely to
impact on the current cost base and which have been provided by WAST as part of national
modelling work.

150
Figure 24: Inflationary Pressures
Inflationary Pressures 2016/17 2017/18 2018/19
£m £m £m
Pay
1% Pay award 1.16 1.17 1.18
Cost of increments 1.25 1.41 1.27
National Insurance and Pensions – Impact of contracting out arrangements (2016/17 only) and auto enrolment (2017/18 and 2018/19)
2.00 0.27 0.27
Total Pay 4.41 2.85 2.72
Other statutory compliance issues 0.40 0.40 0.40
Non-pay inflation 0.70 0.70 0.70
Total 5.51 3.95 3.82
Apprenticeship levy
During 2015, the UK Government consulted on the intention to apply an Apprenticeship Levy from
2017/18. NHS Employers responded to the consultation, indicating the NHS would be the major
contributor but would not benefit significantly.
The UK Government Spending Review and Autumn Statement 2015 confirmed the apprenticeship
levy will come into effect in April 2017 which will require employers to make a payment of 0.5% of
their pay costs. The Apprenticeship Levy will be collected by HMRC from employers via PAYE;
however, skills policy and arrangements, including apprenticeships, are devolved matters. The level
to which WAST, as an employer, might receive financial benefits from the scheme are as yet
unquantified.
On this basis our plans have assumed the costs associated with the payment of the apprenticeship
levy as c£0.4m for each of the years 2017/18 and 2018/19.
The net financial impact of expected uplifts, inflation and unavoidable costs (including
apprenticeship levy) are summarised in the figure 25 below.
Figure 25
Summary of Financial Implications 2016/17 2017/18 2018/19
£m £m £m
Assumed fair share of additional funding 5.00 4.00 4.25
Less:
Inflation and unavoidable costs 5.51 3.95 3.82
Apprenticeship Levy 0 0.40 0.43
Estimated Financial Impact Shortfall
£0.51m
Shortfall
£0.35m
Balance
Inflationary increases and unavoidable costs exceed the expected share of additional
funding, presenting a cost pressure to the Trust of £0.51m in 2016/17 and £0.35m in 2017/18.

151
2016/17 baseline position
In developing our financial plans, the following assumptions have been made to provide a planning
baseline for income for 2016/17, and future years.
Emergency Medical Services (EMS)
Additional funding has been made available through EASC during each of the last two financial
years totalling £15.5m (£7.5m + £8m). Based on the agreed approach with the CASC to determine
the reasonable resource envelope for EMS over the next three years which will underpin this
financial plan, it has been agreed to look to move away from pockets of previous incremental
investment in the Trust to much more focus on the increasingly efficient use of the whole quantum
of spend. This has seen significant additional detail provided to the CASC office by the Trust over
recent months, to fully support the previous recurring investments in the Trust, and with which to
agree this expected reasonable level of spend and resulting resource envelope, against which the
Trust has developed its financial plans.
Through this process, it has been assumed that £14.3m of the above £15.5m funding will be
recurrent within the baseline for future years. It has been recognised that £1.2m of the original
£15.5m supported elements of variable pay spend in 2015/16.
In addition, during 2015/16, further non-recurring funding of £3.5m was provided by Welsh
Government to support the planned costs of increased capacity. Figure 26 below summarises this.
Figure 26
During 2015/16 there have been a number of initiatives that have been implemented which will
require recurrent funding. Many of these have system-wide benefits and their continuation is
contingent upon the availability of continuing financial resource and funding. This includes
increasing operational capacity and providing additional resources to include support for the
Explorer Project in Cwm Taf. The associated costs within the Trust’s financial plan for all this have
been estimated as a minimum of £2m in 2016/17, for which it is assumed that this will now be
funded via its commissioning agreement with EASC, and which has also been included as such in
the above process to determine the reasonable resource envelope on which this Trust is building its
financial plan.
Other examples of local initiatives which will need to be considered for funding in 2016/17, including
the Alcohol Treatment Centre in Cardiff (for which the current funding stream is due to cease in
2016/17) and establishment of similar centres elsewhere in Wales, will require further discussion
with commissioners to determine their financial sustainability.
On this basis, the Trust’s financial plans have, therefore, included the following income assumptions
in relation to baseline EMS funding:
Funded Additional EMS Capacity 2015/16
Planned Costs Funding
£m £m Source
Variable Pay 1.7
3.5 Additional Non-
Recurring WG funding Use of other providers
1.8
Variable costs to support additional capacity included within EASC agreement
1.2 1.2 Within EASC
baseline
Total 4.7 4.7

152
Baseline EMS funding at 2015/16 funding levels:
Estimated spend on EMS 2016/17 - @ 2015/16 prices £m
Current forecast of EMS spend 2015/16:-
Baseline spend 129.8
Additional planned spend 2015/16 3.5
Total forecast spend 2015/16 133.3
Less net non-recurring spend 2015/16 within above baseline spend -1.2
Less additional planned spend 2015/16 (initially planned to be non-recurring)
-3.5
Plus capacity and performance enhancing schemes 2016/17 2.0
Total estimated spend on EMS 2016/17 - @ 2015/16 prices 130.6
This baseline position results in a real terms reduction of income of £2.7m against current
levels.
Impact of assumed share of additional £200m funding:
The apportionment of the fair share of additional funding (£5m) could be disaggregated on the basis
of income distribution that would result in a split of around £4.1m attributed to EMS with the balance
attributed to other activity, e.g. PCS. However, for consistency, it has been assumed the full value,
£5m, will be facilitated in total through the EMS element of the EASC agreement (on a similar basis
to the 2015/16 pay award).
On the basis that the additional funding is fully facilitated through EASC the baseline
funding expected for EMS from EASC for 2016/17 is £135.6m
Transitional cost pressures linked to EMS performance:
Versatility and responsiveness of services has been a critical feature of the improvement in
performance and at times this has required a premium in terms of the costs incurred. Consistent
with the further development of the Trust’s financial strategy and fully integrating this with the
strategic workforce plan and People Strategy, the further continuation of such variable costs is
currently under review, both to establish how greater efficiency can be achieved, yet still maintain a
level of agility that would allow the flexibility that is required to respond most effectively to demand.
Whilst some of the costs incurred to increase capacity in 2015/16 (£4.7m) are expected to
immediately reduce, by up to £1.5m, there will continue to be a reliance on elements of variable pay
and alternative providers to maintain performance levels.
Our plan has assumed an initial cost pressure associated with maintaining levels of EMS
capacity for 2016/17 in the region of £3.2m, for which savings and other efficiencies will be
required to offset such costs, should they continue, and based on the funding assumptions
previously described, in the context of a balanced financial plan

153
Renal Transport Funded Through WHSSC
It is assumed that income for renal services will remain, as a minimum, constant in real terms with
2015/16 levels. On this basis, at least £1.1m will continued to be funded, separate to EMS, through
WHSSC.
Patient Transport Services
The Deputy Minister for Health announced the implementation of the Non-Emergency Patient
Transport Services (NEPTS) business case on 22 January 2016. The financial case included a
commitment to fund service developments through increasing efficiency in this service and is
predicated on an assumption that future funding streams will reflect current levels. This is in line with
the assumptions included as part of the business case developed in partnership with all Health
Boards and Trusts. Following this recent announcement a detailed implementation plan is being
developed which will include refining the profile of the financial plan.
It is assumed that income for PCS for 2016/17 will, as a minimum, remain constant in real
terms with 2015/16 levels.
111
The direct financial impact of the 111 pathfinder is assumed to be cost neutral, with corresponding
income (initially via ABMU) and expenditure assumptions of £1.775m for 2016/17, made up as
follows:
It is also assumed within this IMTP and financial plan that the implementation of 111 will not lead to
a direct increase in 999 calls, and it is on this basis that both the operational and financial plans for
the Trust have been constructed within this IMTP.
ESMCP
It is also assumed within this financial plan that any additional revenue costs falling to the Trust as a
result of the ESMCP (Emergency Services Mobile Communications Programme) and associated
business cases will be financially neutral, i.e. funding will be made available to offset any additional
costs.
Demand / capacity review
Finally, as detailed elsewhere within this IMTP, the Trust is looking to complete a comprehensive
demand and capacity analysis in early part of 2016/17, linked to the ongoing evaluation of the New
Clinical Response Model. It is assumed that any additional costs incurred in delivering this
(expected to be c£100k) will be funded.
Additional Costs for 111 Service Delivery 2016/17
£000
Core staffing costs 1,461
Telephony Costs 62
IT costs 150
Subtotal 111 service delivery 1,673
Plus Project costs via WAST 102
Total expected income and expenditure 2016/17 1,775

154
2017/18 and 2018/19
Funding uplifts
Whilst the Welsh Government draft budget provides only for 2016/17, the UK spending review
provided indicative budgets for the next four financial years. These figures present plans for further
increases for the NHS in England, and, consistent with other NHS Wales health organisations, it is
on this basis that WAST financial plans have been developed, which assume that additional funding
will be provided for each of these years resulting in further uplifts of a minimum of £4.0m and
£4.25m respectively.
111
The financial implications of an extended roll-out of the 111 pathfinder have also been considered
and estimated within years two and three of the financial plan, building on those expected above in
year one (2016/17). Initial estimates suggest this could potentially increase our workforce over the
following two years by a further 59.84 WTE call takers, and 67.56 WTE Nurse Advisors. However, it
must be noted that these figures are subject to change and would require further investment. Again,
the working assumption within the Trust is that any additional cost impacts of the implementation of
111 throughout this planning period will be financially neutral to the Trust, i.e. will be externally
funded. Assuming full roll-out of 111 by the beginning of year three of this planning period (2018/19)
would see a further increase in the Trust’s costs of c£5.8m (including estimated telephony and IT
costs); the planning assumption within this plan for year two (2017/18) is a half roll-out of this over
and above that already committed for 2016/17. In each year, additional funding via ABMU has also
been assumed to offset these additional costs.
Other developments
There is a significant range of further developments over the planning period that are likely to be
implemented leading to changes in the cost base and profile of the Trust, in terms of type of spend
across the Five-Step Ambulance Care Pathway. Work continues to assess the impact of such
changes, many of which will be clearer following the outcomes of the demand and capacity review
and the implications of other developments, e.g. the replacement of the Trust’s CAD. Whilst the
detailed impact on service, workforce and finance of these developments cannot yet be fully
quantified and included within this three-year financial plan, it expected that the impact will
commence through years two and three (2017/18 and 2018/19) with the planning work being
completed through 2016/17. It is also assumed within this financial plan that the costs of any such
developments will either be separately funded, release spend elsewhere within the Trust to offset
such costs (including across other steps of the pathway) or will only be implemented when further
additional savings and efficiencies have been identified. Examples of these include:
further developments in CCCs, in addition to 111. This includes the further investment in staff and the clinical desk resource to increase “Hear and Treat” rates in line with other ambulance services across the UK. The implementation of a new CAD system will also see operational efficiencies within CCCs, as will the further review of the configuration of CCCs as part of the wider estates review and rationalisation. This may see the number of dispatch desks required reduce because of greater automation, especially during the night, alongside reviewing shift patterns;
furthering the ICT strategy of the Trust to develop a technically enabled workforce, especially in relation to front line operational staff, which will provide for even more treatment at scene and resulting impact on hospital conveyances; and

155
working with Health Board colleagues and others to further develop the availability of alternative care pathways, ability to access direct to speciality, etc, releasing resources and further enabling the proportion of the Trust’s spend to move towards STEPS 1 and 2 of the ACP.
As part of the financial modelling that underpins this IMTP, some initial preliminary analysis has
been conducted which starts to consider how EMS costs can be attributed across each of the five
steps of the ACP over the planning period being considered. The table below presents the initial
results of this and provides indicative detail of how costs might shift between steps during the next
three years. This information includes the assumed full roll-out of the 111 pathfinder.
Further future refinements of this analysis will need to reflect the outcomes of the demand and
capacity review, the evaluation of the New Clinical Response Model and the future resources
(staffing, fleet, etc) required to deliver this, and take account of the implications of developments
above (as appropriate). Therefore, at this stage, this information must be viewed purely as an early
indication that will be developed throughout 2016/17 in conjunction with the Commissioner.
Estimated costs across STEPS
Year Estimated
split
between
STEPS
Steps
STEP 1
Help me
choose
STEP 2
Answer
my call
STEP 3
Come
and see
me
STEPS 2 & 3
Answer my call
& Come and
see me
STEPS 4 & 5
Give me
treatment &
Take me to...
Total
2015/
16
£ £0.7m £7.0m £13.3m £1.6m £110.7m £133.3m
% 0.52% 5.27% 9.92% 1.23% 83.07% 100.0%
2016/
17
£ £0.7m £9.1m £13.8m £1.7m £112.0m £137.4m
% 0.52% 6.65% 10.0% 1.24% 81.5% 100.0%
2017/
18
£ £0.7m £11.4m £14.2m £1.8m £115.3m £143.4m
% 0.52% 7.92% 9.92% 1.23% 80.4% 100.0%
2018/
19
£ £0.8m £13.7 £14.7m £1.8m £118.8 £149.8m
% 0.52% 9.14% 9.79% 1.23% 79.4% 100.0%
Other initial supporting analyses to further describe other shifts in spend within the planned EMS
resource envelope over the next three years have also been initially estimated and shared with the
CASC and his team. A key example is the level of pay costs over this period and, in turn, how this is
expected to break down into core costs and variable pay. Clearly, this is a key area that will need
some significant further refinement once the current key outstanding pieces of work previously
described have been concluded. Based on the known plans being progressed by the Trust,
including recruitment, workforce efficiencies, and savings plans (see below), this suggests a
reduction in the levels of variable pay by 2018/19 of in the region of £4m pa (a drop from c9% of
total pay spend to just over 4%, or a nearly 50% reduction in the levels of variable pay itself) when
compared with current levels.
Summary of financial changes
Figure 27 below sets out a summary of the assumed in year, material revenue cost changes
described for each of the years 2016/17 to 2018/19.
Figure 27

156
R NR Total R NR Total R NR Total
£m £m £m £m £m £m £m £m £m
Brought forward recurring deficit/-surplus 0.00 0.00 0.0 0.0 0.0 0.0
Income changes
Share of £200m -5.0 -5.0 0.0 0.0
Future years inflation 0.0 -4.0 -4.0 -4.3 -4.3
Additional Funding 2015-16 3.5 3.5 0.0 0.0
Variable element of EASC 1.2 1.2 0.0 0.0
Assumed funding for continuuation of capacity -2.0 -2.0 0.0 0.0
Assumed funding for 111 (via ABUHB) -1.8 -1.8 -2.0 -2.0 -2.1 -2.1
Total income changes -4.1 0.0 -4.1 -6.0 0.0 -6.0 -6.4 0.0 -6.4
Expenditure changes
Unavoidable costs - Inflation, pension, statutory
compliance etc 5.5 5.5 4.0 4.0 3.8 3.8
Apprenticeship levy 0.0 0.4 0.4 0.0 0.0
Continued capacity 2.0 2.0 0.0 0.0 0.0 0.0
Reduction of non recurring costs -1.5 -1.5 0.0 0.0 0.0 0.0
Non-recurring savings delivery / gains 2.5 2.5 1.4 1.4 0.5 0.5
Assumed 111 costs 1.8 1.8 2.0 2.0 2.1 2.1
Total expenditure changes 10.3 0.0 10.3 7.7 0.0 7.7 6.4 0.0 6.4
Sub total deficit / -surplus (inc bfwd) 6.2 0.0 6.2 1.7 0.0 1.7 0.1 0.0 0.1
Efficiencies / service re-design / gains
Planned accountancy gains (profit on disposal) -1.0 -1.0
Potential savings -4.9 -4.9 -1.2 -1.2 -0.1 -0.1
Non recurring savings -0.4 -0.4 -0.5 -0.5 0.0 0.0
Total efficiencies / service re-design / gain -4.9 -1.4 -6.2 -1.2 -0.5 -1.7 -0.1 0.0 -0.1
Total deficit / -surplus 0.0 0.0 0.0
Recurring deficit/-surplus carried forward 0.0 0.0 0.0
2016-17 2017-18 2018-19
Summary of assumed financial changes
Savings and efficiency
The scale of the financial challenge for future years is significant. Whilst it is expected that a fair
share of additional funding will be provided to support the majority of the forecast inflationary and
unavoidable costs, it is clear that the achievement of financial balance will require further
efficiencies and the financial plan has been developed on this basis.
The Trust’s financial position for 2015/16 includes a savings target of £4.5m (3%). Of this, a number
of the schemes implemented are non-recurring and will require additional savings of £2.5m to be re-
provided in future years.
This adds to the potential shortfall against inflation and unavoidable costs of £0.5m (in 2016/17) and
initial cost pressures of £3.2m associated with continuing current levels of capacity to maintain
performance.
The financial plan therefore presents a savings requirement for 2016/17 of £6.2m increasing,
to cover the costs of the apprenticeship levy, to £6.5m in 2017/18.
Significant progress has been made to establish a range of cost reduction, cost avoidance and
savings schemes to deliver financial balance both for 2016/17 and in the longer term, which
includes a reduction of costs through a range of initiatives set out below.

157
Further reducing sickness rates – significant financial savings have been delivered in 2015/16, as a result of a reduction in sickness rates during the year. Our plans are to reduce sickness rates further, by 1% point in 2016/17 and 0.5% point in each of the following two years which will provide additional savings over the next three financial years, increasing from £0.6m in 2016/17 to £0.8m in 2018/19.
Other variable pay initiatives – this includes a range of schemes which will improve
efficiency, benefit staff and reduce spend, such as increasing job cycle efficiencies
(including reducing the time from handover to clear), reductions in overruns, reviewing
meal breaks, a proposed re-alignment of some operational CPD and further reducing the
time to recruit operational staff. These will all reduce the variable costs associated with
overtime hours. Together with service modernisation, it is anticipated that further variable
costs (overtime) of over £1m can be saved.
Management of (non-operational) vacancies – is expected to save a minimum of £0.2m.
Through reducing reliance on other providers – such as St John and other private
providers will plan to reduce costs over this planning period by up to £1.3m.
Fleet maintenance and fuel - the review and rationalisation of these costs is planned to
save up to £1m. This will include a detailed review of current contracts for maintenance
and repairs, assessing the potential threshold for such repairs in the future, looking at
innovative ways in which some elements of routine maintenance can be provided, and a
prudent assumption in relation to the potential continuation of current low fuel prices.
Consumables, Drugs and Medical Gases – through a combination of Trust-wide and local
schemes we will reduce costs by up £0.5m.
Procurement – Our continued drive towards cost effective procurement, and working to
maximise this with colleagues in NWSSP, will result in additional savings being delivered
in 2016/17.
Reviewing and minimising expenses – will provide a source of additional savings both in
the immediate and medium term. This will include further exploring the pool car policy
within the Trust with a view to creating a number of points around Wales where staff can
access pool cars, thus reducing travelling expenses costs. Other areas of spend also
being further reviewed and considered for savings opportunities include:
o further exploring salary sacrifice schemes, including those in relation to vehicle
purchases and the impact on cost per mile expenses paid;
o using the introduction of telemetry to facilitate the ability to better challenge certain
claims against the Trust, potentially reducing losses and compensation costs as well
as further protecting our staff;
o assessing the cost / fuel impact of reducing conveyance rates in some areas;
o review of use of taxi policies, especially for EMS, and the potential use of voluntary
car users;
o reviewing future uniform replacement polices; and
o reviewing other local practices.
Further financial benefits are anticipated including through estates realisation, which will provide
non-recurring gains of more than £1.0m in 2016/17.

158
Ambitious plans that will deliver a balanced financial position for each of the next three
financial years are in place.
However, it must be recognised that, whilst efficiencies will in some cases result in cash releasing
savings, other actions will instead enable improvements in productivity and performance. The
balance of efficiency gains between performance and cash releasing savings will be an important
element of the on-going discussions with our commissioners. A key example is the implementation
of the NEPTS business case, where efficiency savings have been reprioritised to fund agreed
service developments. Whilst this is welcomed in terms of the improvement to patient care, it
presents limitations in relation to the potential to provide additional cash releasing savings.
In developing the financial plan for 2016/17 to 2018/19, there is emphasis both on the identification
of immediate efficiencies, either in terms of performance or cost, but also exploring potential longer
term opportunities, which will be further developed and enhanced throughout this planning period.
Part of this approach includes the scrutiny and comparison of costs through internal and external
benchmarking, including working with the Commissioner-led development of a benchmarking toolkit,
in conjunction with the NHS Benchmarking Network.
Whilst our plans for the delivery of savings are at both local and corporate levels, there are clear
lines of accountability and progress of delivery will be closely monitored. Savings plans are being
progressed towards implementation via robust project plans, being very clear in terms of ownership
of the actions required to deliver, key milestones, deadlines, and monitoring arrangements, which
have further informed the current expected profile of such savings delivery over the lifetime of this
financial plan.
Similarly, how we look to describe, quantify and evidence the likely shift in the Trust’s spend on EMS from STEPS 4 and 5 more towards STEPS 1 and 2 of the Ambulance Care Pathway will form an important part of our financial plans for the future. It is recognised that an important part of this will be to develop a fuller understanding of how these shifts influence costs across the whole system and the financial impacts both for the Trust and our partners.
Summary of Financial Risks:
No financial plan is risk free. Financial risk management forms a key element of the project plans
that underpin both our ambitions and savings targets. We have strengthened our financial capacity
and corporate focus on finance and, as an organisation, have structures in place to drive through
the delivery of our financial plan.
A summary of the key risks to the delivery of the Medium Term Financial Plan includes:
funding assumptions in relation to pay and non-pay inflation;
financial impact of New Clinical Response Model and the transition of any changes to workforce and fleet requirements;
implementation of the NEPTS business case, specifically matching the profile of efficiency with service development;
availability of capital funding to support the infrastructure investment required to implement service change;
financial impact of EASC commissioning intentions, and confirmation of the EMS financial resource envelope as assumed within our financial plan;
outcomes of demand and capacity work; and
delivery of cash-releasing savings and efficiencies.
Scenario planning will help to mitigate these risks, highlighting the levels of financial risk but also
indicating the service and performance impact. However, the extent of service change that the Trust

159
is implementing is extensive, with key developments such as the NEPTS business case at an early
stage but with the potential to transform the quality and efficiency of services.
Impact on Workforce
Co-ordination between financial and workforce plans is vital to both financial and service delivery.
This alignment is a critical element of our future plans as WAST implements service developments
and includes both immediate and longer term planning, both in terms of existing workforce and
recruiting and training the workforce required for the future.
As part of this our workforce plans reflect a commitment to:
reduce sickness absence;
streamline recruitment processes to reduce the reliance on more costly forms of cover for operational staff; and
minimise the costs of relief cover, whilst maintaining a level of flexibility that will enable the most efficient use of staff resources.
The current funded establishment is presented within the table below. This represents the
contracted establishment and does not reflect levels of variable resource.
Funded Establishment as at 31st March 2016
CE Office
Board
Secretary Operations
Finance
& ICT Strat Dev
Quality &
Nursing W&OD Clinical Total
Funded Funded Funded Funded Funded Funded Funded Funded Funded
WTE WTE WTE WTE WTE WTE WTE WTE WTE
Chairman & Non Execs 8.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 8.00
Executive Board 7.00 0.00 0.00 0.00 0.00 0.00 0.00 0.40 7.40
Senior Manager 1.00 4.00 60.91 30.30 6.80 8.81 26.80 22.00 160.62
Admin & Clerical 1.00 7.67 186.82 51.60 2.00 17.68 37.18 21.09 325.04
Other Staff 0.00 0.00 131.81 0.00 0.00 16.48 7.60 1.00 156.89
Ambulance Staff 0.00 0.00 2,359.12 0.00 0.00 0.00 0.00 3.00 2,362.12
Total 17.00 11.67 2,738.66 81.90 8.80 42.97 71.58 47.49 3,020.07
Our financial plans are being developed to reflect both the planned workforce investment and the
potential to reduce variable costs. These will also be influenced by the longer term workforce
requirements arising from the New Clinical Response Model and the implementation of NEPTS.
Our workforce plans have identified a number of areas where there is expected to be investment in
contracted workforce during 2016/17, including:
recruitment within our Clinical Contact Centres (CCC);
implementation of the NEPTS business case (i.e. strengthening of the NEPTS management and supervisory structure); and
the implementation of 111 Pathfinder will increase our workforce, with the following additional workforce assumptions included in our current plans for 2016/17.
Increase in WTE
Staff Group ABMU Carmarthenshire Total
Call Handlers 13.24 4.33 17.57
Nurse Advisors 15.07 4.93 20.00

160
The table below indicates how these changes might initially impact on our contracted workforce in
2016/17.
Capital
The capital programme has been developed in parallel with our service, estate and fleet plans. The Trust’s current Capital Plan includes schemes with a gross investment value of more than £226m profiled over the next five years. This includes new estate developments and the replacement of the CAD system, as well as a rolling vehicle replacement programme. We will build on the current organisational processes for the management and prioritisation of
capital planning and, in parallel with our commitment to allocate our revenue expenditure across the
five steps of the ambulance care pathway, we will seek to align our capital planning processes on
the same basis.
There are two elements to our capital plans:
1. Discretionary Capital
2015/16
The Welsh Ambulance Services NHS Trust Discretionary Capital Programme allocation is funded
from the Welsh Government All Wales Capital Programme (AWCP). WAST has been allocated a
total of £3.884m discretionary capital for 2015/16. This is an increase of £0.826m from 2014/15,
where the initial allocation was £3.058m (although an additional £3m was allocated later in the year,
bringing the total allocation to £6.058m for 2014/15).
2015/16 discretionary capital spend included (but was not limited to);
£961,000 on 85 Corpuls Defibrillators;
£29,755 on Advanced life support (ALS) mannequins;
£175,000 on a rolling IT hardware replacement programme; and
£917,000 maintaining and improving estate.
Potential Funded Establishment as at 31st March 2017
CE
Office Board
Secretary Operations Finance
& ICT Strat Dev
Quality &
Nursing W&OD Clinical
Total Funded Funded Funded Funded Funded Funded Funded Funded
Funded
WTE WTE WTE WTE WTE WTE WTE WTE
WTE Chairman & Non Execs 8.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
8.00
Executive Board 7.00 0.00 0.00 0.00 0.00 0.00 0.00 0.40
7.40 Senior Manager 1.00 4.00 60.91 31.30 6.80 8.81 26.80 22.00
161.62
Admin & Clerical 1.00 7.67 228.31 56.10 2.00 17.68 39.18 21.09
373.03 Other Staff 0.00 0.00 151.81 0.00 0.00 16.48 7.60 1.00
176.89
Ambulance Staff 0.00 0.00 2,366.52 0.00 0.00 0.00 0.00 3.00
2,369.52
Total 17.00 11.67 2,807.55 87.40 8.80 42.97 73.58 47.49 3,096.46

161
Recognising that demand for discretionary capital monies always outstrips funds available, the organisation recognises the importance of taking greater advantage of other funding opportunities or routes, such as the Health Technology Fund, ‘Invest to Save’ and Integration Funds.
Future Years
It has been confirmed that WAST has been allocated a total of £5.826m discretionary capital for 2016/17. This is an increase of £1.942m from 2015/16, subject to the approval of this IMTP.
The organisation has an Internal Capital Planning Group that meets monthly and oversees all
aspects of discretionary capital planning. A robust assessment and prioritisation process has been
undertaken to determine how funding will be prioritised and allocated to schemes, with final
approval by the Trust Board, ensuring that the Discretionary Capital allocation is utilised effectively
to support the Trust in achieving its strategic goals which are aligned to this plan.
All of the bids received for funding from the Discretionary Capital allocation for 2016/17 have been
recorded and verified by the Finance Department and the Internal Capital Planning Group (ICPG)
using agreed criteria and scoring matrix that includes the following considerations:
improved quality and safety;
statutory compliance requirements;
affordability in terms of capital and revenue;
transformation aligned to the IMTP; and
invest to save.
The results of this exercise, which form the Trust’s Discretionary Capital Programme for 2016/17, has be to the Trust Board’s Finance and Resources (FRC) Committee, and Trust Board for approval.
On this basis, the draft plan has assumed discretionary capital funding of £5.826m for
2016/17, reflecting a baseline at the 2015/16 level of funding with a non-recurring increase of
£1.942m, subject to the approval of this IMTP.
2. Capital Investment Awarded for Major Capital Schemes Based on the Submission of Five Case Model Business Cases to Welsh Government.
Our capital programme also supports a number of major capital schemes that facilitate the
implementation of our plans, and underpin our strategic aims and priorities. Capital investment will
unlock quality and efficiency improvements/gains through the purchase of the most up-to-date
vehicles, along with clinical equipment. In addition, this investment will provide our staff with the
most appropriate buildings that allow vehicles to be cleaned and stocked, with suitable rest facilities
to ensure they are ready for the next call of the day.
2015/16
For 2015/16, the Trust’s Capital Expenditure Limit is £19.682m, which will fund:
discretionary capital £3.9m (above);
Joint Ambulance/Fire Development ARC Wrexham £4.9m;
vehicle replacement 2015-16: further EMS vehicles £8.3m;
Blackweir business case costs £0.15m;
“Hear and Treat” function - planning & dispatching £0.39m;
Omnicell- £0.42m;
communication devices to more than 400 community first responders £0.47m; and

162
EMS equipment £1.2m.
A high level summary of current progress is indicated in Figure 28 below.
Figure 28
Scheme Status Timescales
Wrexham Ambulance and Fire Service Resource Centre
On target / on budget
Handed over mid February 2016
Cardiff Ambulance Resource Centre Strategic Outline Case approved by Welsh Government; currently undertaking development of the Outline Business Case
OBC under development
Vehicle Replacement 2015/16 On target
Complete end March 2016
Computer Aided Dispatch System Business Case submitted to WG – Planned implementation summer 2016
Currently going through the Tender Process
Non-Emergency Patient Transport Business Case submitted Approved
Relocation of Trust HQ St Asaph Options Appraisal complete, BJC to be developed
Ambition to be completed by April 2017
All Wales Capital: Future Years
A high level overview of our current capital plan includes:
continued investment in vehicle replacement and fleet that will align with the requirements of
changing service delivery models including the New Clinical Response Model and Patient
Transport;
Clinical Contact Centre configuration to support service developments;
Blackweir ARC together with Bangor ARC and Newport MRD;
ICT infrastructure development;
replacement of operational systems including the Control and Despatch and 111;
Community First Responders;
ESMCP & ARP; and
estates review.
The details of the capital programme for 2016/17 are currently under discussion both internally and
externally with officials within Welsh Government. As part of this, consideration is being given to
potential schemes that can be accommodated within year, as well as the progress of existing capital
schemes which currently include a number of strategically important initiatives including vehicle
replacement, Cardiff Ambulance Resource Centre (ARC), Bangor ARC, and Newport Make Ready
Depot (MRD), each of which is vital to increase efficiency.
Our current plans present schemes for additional investment with a total value in the region of
£200m over the next five years, of which £27m relates to 2016/17.

163
The Welsh Government final budget published on 1st March 2016 provided for £10m of
capital funding in 2016/17 to support the replacement of vehicles across Emergency Medical
Services and Non-Emergency Patient Transport Services as well as some Specialist National
Resilience Vehicles.
Costs of Capital
The costs of capital have been included as £12.728m in accordance with the allocation value
presented within WHC (2015) 059. Our initial calculations have indicated that depreciation charges
will increase over the next five years and it is assumed that these costs of capital will be fully funded
by Welsh Government.
6.3 Our Estate
The Estates Department forms part of the Finance, ICT & Estates Directorate and reports directly to
the Director of Finance and ICT.
Our estate currently comprises some 43,548m2 (gross internal) floor area in 110 buildings located
throughout Wales. The revised estates Strategic Outline Programme (SOP), if fully completed, will
eradicate all issues of less than ideal building functionally; it will also address a significant element
of the backlog maintenance which currently stands at c£13.4m. In the interim, this is being
addressed through the internal discretionary programme.
Our Frontline Operational Sites
Our organisation has an Estates Strategy that was written in 2011. It aimed to deliver:
Ambulance Resource Centres to provide office and welfare facilities for staff with workshops
to maintain, wash, clean and restock our fleet vehicles;
Make Ready Depots to provide office and welfare facilities for staff with vehicle washing,
cleaning and restocking; and
Social Standby Points (SDPs): places where staff can rest and recuperate and have access
to office facilities usually through sharing other buildings such as fire stations.
We recognise that lots has happened and that many things have changed since 2011 and that
subsequently this strategy needs updating.
MRD Dobshill was constructed in 2012 and has been operating successfully since then. ARC
Wrexham is in the final stages of being constructed and will be operational in March 2016.
It is envisaged that, moving forward, Ambulance Resource Centres (ARC) and Make Ready Depots
(MRD) will form the core of the Trust’s operational estate as they will be underpinned by an
integrated network of deployment points strategically located in areas of peak patient demand,
ensuring we are best serving people in Wales.
We also recognise, however, that the current Estates SOP now also needs to be reviewed and updated, in line with the proposed ‘direction of travel’ along with any other changes to operational requirements and to ascertain whether there are any estates priorities emerging, which may need to be reprioritised. It is important to ensure that the review of the SOP is operationally led. The SOP review will thus commence with a series of 1:1 meetings between with the Director of Operations and each of the

164
Heads of Operations. Each Health Board area will be reviewed, comparing the original SOP proposals against what may have changed or be deemed to be a more urgent requirement now. Once the meetings are completed, an exercise will be undertaken to map the findings, which will be applied on a national basis across Wales against what was planned initially in the original SOP.
Our Control Centres and Administrative Bases
Our Clinical Contact Centre (CCC) function is currently provided from five separate premises across Wales. This configuration is a legacy from the merger of five former ambulance services into a single Trust for Wales, along with the integration of the NHS Direct Wales service.
The current configuration of CCCs is detailed in Figure 29 below. Figure 29
CCC Region Services No of
Workstations
Llangunnor, Carmarthen Central & West PCS & 999 29
Thanet House, Swansea Central & West NHSDW 44
Bangor North NHSDW 20
Llanfairfechan North PCS & 999 28
VPH, Cwmbran South East NHSDW, PCS & 999 68
In 2014/15, we had an opportunity to join South Wales Police, Mid and West Fire & Rescue Service and South Wales Fire & Rescue Service in the development of a joint control room facility located in Bridgend, South Wales. Although this was presented to the Trust Board in March 2015 as an option, it was felt that there was insufficient information and evidence to support the option at that time. There was an added issue regarding the outstanding decision on the hosting of the 111 service in Wales, as this was recognised as having a significant impact on the capacity required in any CCC configuration.
Whilst the development at the Bridgend facility has progressed with Police and Fire Service, we have committed to a minimum of a single desk, thus making the control centre ‘tri-service’. In North Wales the CCC situation is slightly different. The Trust Board approved the development of a Strategic Outline Case (SOC) in partnership with North Wales Police and North Wales Fire and Rescue Service for a joint emergency control centre based in North Wales. The decision to move towards the development of the SOC for North Wales was predicated on a review of CCCs across Wales that was completed by Consultants ORH and finalised in December 2014. Whilst this report is still considered accurate, it started from the assumption that an integrated health model i.e. EMS, PCS NHSDW (111) and GPOOH, all located in the same CCC, was the preferred service model option. We subsequently recognise that we need to be clear what our preferred service model is before we can progress to considering our optimum and desired configuration of our CCC estate.
Our Research and Development Team have committed to a piece of work to explore and consider the evidence for an integrated health service model, whilst we have also held workshops to begin scoping out what the full range of options (and what they ‘look like’) are. Combined, these two

165
exercises will allow us to agree our preferred service model and subsequently fully initiate any estate reconfiguration work. Sites We Share with Health Board Partners We will work with all LHBs in Wales to ensure our individual plans are dovetailed together. This is
particularly important where this Trust shares LHB sites such as at Cefn Coed, Swansea. ABMU
has plans to redevelop the Cefn Coed site, which will require us to relocate our Regional
Headquarters and Training School (this is likely to be in years 2 or 3 of the plan).
Our model for future service delivery will be considered in the context of the lease opportunities and
options to further rationalise the administrative estate, such as at Vantage Point House, will be
considered during the term of this plan.
Our Estate and Our Blue Light Partners
In addition to the tri-service control centres which are documented above, we are also working with
the Mid and West Fire and Rescue Service (MWFRS) to design and develop a model for a shared
vehicle maintenance facility.
Currently, a fleet of 45 PCS vehicles in the Abertawe Bro Morgannwg (ABM) Health Board area is
repaired and maintained by three local dealers based in Swansea and Llanelli. The vehicles operate
from various stations including Bryncethin, Glynneath, Gorseinon, Neath, Pontardawe, Port Talbot
and Swansea.
A one-year pilot project will provide the opportunity for MWFRS and WAST to work together to
establish if effective and efficient use of publicly funded assets through a joint vehicle maintaince
site can be achieved.
More widely, it is also proposed to engage with other emergency services within Wales to jointly review the estates proposals for all of the emergency services. This will enable strategic estates planning for collaborative working for the future.
Year 1:
Action 95: Commence the process of establishing the organisations next ARC in Cardiff.
Action 96: Review and update the Trust’s National Estate Strategy 2011 to include all Trust
Estate.
Action 97: Review joint WAST / Mid and West Wales Fire and rescue Service (MWFRS) vehicle
maintenance pilot.
Years 2 & 3
Action 98: Relocate the organisation’s Trust HQ from its current site at St Asaph to another site
in North Wales.
Action 99: Relocate the organisation’s regional West Wales HQ from Cefn Coed
Action 100: Progress any CCC estate reconfiguration that may result from earlier work

166
6.4 Our Fleet
We operate 706 vehicles:
273 Accident and Emergency Ambulances (EMS);
143 Rapid Response Vehicles (RRV);
260 Patient Care Services (PCS); and
30 specialist and auxiliary vehicles encompassing the Hazardous Area Response Team
(HART).
Our Fleet covered in excess of 20 million miles in 2015/16, used £5 million of fuel and was serviced
and inspected circa 5,000 times by the Fleet Department.
The accident and emergency ambulance fleet is a modern range of coach built, box body vehicles.
The average age is 3.1 years; rapid response cars have an average age of 2.4 years. The
ambulances are equipped with all the latest clinical technology and labour-saving devices such as
electrically operated tail lifts and stretchers that help to reduce manual effort and improve the patient
experience. The design of all vehicles has been undertaken in partnership to maximise user
contribution.
The Fleet Department employs 38 staff spread across Wales; the Administration Department and
one of the four in-house workshops at Wrexham are in the process of relocating to a new purpose-
built site that will be shared premises with North Wales Fire and Rescue Service. The other three
in-house workshops are located in Cardiff, Blackwood and Bangor. There is also a management
team based at Vantage Point House, Cwmbran.
Ambulance reliability is a key priority for us. The Fleet Department manages and maintains the
vehicles through a rigorous and robust Planned Preventive Maintenance (PPM) schedule. In the
North and South East areas maintenance is undertaken at the four in-house workshops; Central
and West areas are predominantly maintained by third party suppliers.
We are moving from the current PPM system to a time-based service interval system. This will
assist in increasing reliability and the release of vehicles for servicing.
As a result of the New Clinical Response Model the CCC has the opportunity to dispatch the most
appropriate resource to a 999 call rather than simply the closest resource. Each incident outcome
code contains details of the ‘ideal response’; this, by default, will identify the most appropriate
vehicle to send to an incident. This will inevitably lead to a change in the current vehicle mix. This
will be thoroughly tested through the analysis of historical demand as part of the demand and
capacity work described earlier in this plan. The historical activity will be aligned to the New Clinical
Response Model which will provide information on the fleet requirements to deliver the most
appropriate resource. This information will be compared to the current fleet available and a plan
developed to move towards the ‘best fit’ fleet mix.
We are in the process of developing a three- year vehicle Strategic Outline Programme (SOP); this
will include migration to the optimal fleet mix that will be derived from the analysis described above.
The SOP will also smooth out the procurement process by removing some of the peaks and troughs
in the current replacement cycle. The SOP will outline the new/replacement vehicle requirements
over the next three years and, once approved, will enable funding to be allocated by WG on a
systematic basis without the need for lengthy annual Business Justification Cases (BJCs).

167
The Fleet Department currently provides CCC with a schedule of planned maintenance; arrangements are then made for the vehicles to be taken out of service at the appropriate time. This is not a robust process, with many vehicles not being available on the exact day for scheduled service. Localities and CCC are also responsible for arranging repair for unplanned breakdown; this is time consuming and unproductive in terms of use of resources. The solution, in-conjunction with time- based scheduling, is to implement a virtual fleet and logistics help desk in CCC to take much of this work away from CCC staff. Action 101: Implement a Virtual Fleet and Logistics Help Desk in CCC
In 2015, the Trust invested in on-board vehicle telematics, and aims to roll it out to the entire fleet. Before the information can be used to create improvements, an agreed policy must be in place to provide both guidelines to management and assurances to staff that the systems are there only to help protect them and to provide additional information to the fleet department.
During 2015/16, we invested in a replacement computerised fleet management system. This is a state-of-the-art system that will be a keystone for the modernisation of the Fleet Department and further developments of the Make Ready Operation in that it will:
reduce manual effort (less manual inputting of data);
increase efficiencies of both administration and maintenance processes;
improve accountability for vehicle compliance;
improve stock control;
provide greater visibility of vehicles for all key stakeholders (internal and external);
provide greater control of maintenance budgets through uniformity and consistency across all suppliers; and
provide up to the minute status for all vehicles that are off the road and not operational.
Consequently, we want to fully install and embed this system in year one.
Action 102: Install and fully utilise a new computerised Fleet Management System
There is an industry-wide shortage of skilled motor vehicle technicians as there has been a reduction in companies taking on apprentices in recent times. We have a vision to introduce an apprentice training scheme and now need to ensure that there is a return from the time and money invested in the scheme to date.
Last year, we conducted a trial of “vehicle movers” in North Wales using agency personnel. This proved very successful and is now funded annually as part of the fleet core budget. A business case for rolling out vehicle movers in the South and East has been approved and recurring monies made available to fund the employment of a small team of driver/cleaners. The next part of the solution is to employ the North drivers directly on Trust contracts. The fleet age profile is inconsistent owing to large number of vehicles being procured some years and very few in other years. This inconsistency creates challenges with regard to managing maintenance revenue budgets. Challenges also arise when funding is not available to replace large numbers of vehicles in one financial year. We know this age profile needs to be addressed through a smoother and more manageable replacement programme.

168
6.5 Research and Innovation
We have highlighted that one of our six strategic aims is to deliver the best possible patient outcomes and experience through transforming models of care across all of the Trusts services, using technology, innovation, research and best practice to become truly quality driven. We recognise that both research and innovation along with service improvement (Section 6.6
below) are not mutually exclusive. We recognise that these functions support the Trust to develop
an integrated approach towards innovative and sustainable change. We do, however, also
appreciate that innovation and service improvement shouldn’t happen in silos or pockets of the
organisation-owned and driven by the few. Both should be a core principle of the organisation and
fostered within a culture that encourages innovation and continuous improvement. We therefore
want to develop an innovation strategy that clearly outlines what innovation means to WAST and
how we plan to embed it in the organisation.
Action 103: Develop a Research and Innovation Strategy for WAST
Significant innovation is already embedded throughout the organisation through its systems, structures, the nature of the business, and its need to develop strategic partnerships to deliver future sustainable services with partner Health Boards. The implementation of the New Clinical Response Model as a one-year pilot demonstrates the significant innovative change programme underway within the Trust. The New Clinical Response Model is regarded as innovative by other UK ambulance services, and is also attracting interest worldwide. The Clinical Modernisation Programme Board (CMPB), chaired by the Medical Director, oversees its implementation, with work streams based around each step of the model (see Appendix 9: Structure Diagram). This programme is one of four transformational programmes going forward and the Programme Board structure is outlined in Appendix 8. Oversight of the delivery of the programmes is through the Delivery and Assurance Group (DAG). The Programmes have also embraced technological change; e.g. the implementation of digi-pen, the new CAD, embedded within the modernisation of the Clinical Contact Centres. We are proud of the Research and Innovation that we conduct, and recognise the pivotal role that
Research and Innovation (R&I) has to play in the organisation. The R&I functions for the Trust are
delivered by the Pre-Hospital Emergency Research Unit (PERU), which is part of the Health and
Care Research Wales arm of Welsh Government. The Trust is widely recognised as having a
strong research focus and as an attractive place to undertake pre-hospital research, mainly
because of our exemplary track record in delivering on trials, but also in relation to the geography of
Wales, which encompasses both rural and sparsely populated areas. The Trust is, therefore,
strategically well placed to take advantage of this environment to improve health through
developments in the pre-hospital phase of care.
In order to optimise grant capture from research funders, the Trust needs to work with academic,
clinical and industry partners. In 2015-2016, the RS&PD allocation was used to good effect on the
two projects:
Rapid Analgesia for Pre-hospital Hip Disruption (RAPID): a feasibility study for a randomised
controlled trial; and
Transient Ischaemic Attack 999 Emergency Referral (TIER): feasibility trial
Some of our highlights include;

169
Two Clinical Trials of Medicinal Product:
o (CTIMP); RIGHT 2; and
o Paramedic 2. Rapid Intervention with GlycerylTrinitrate in Hypertensive stroke Trial 2
RIGHT-2.
High quality research can be costly and time consuming, which relies on collaborations across many
stakeholders. Consequently, the Trust’s R&I team engages in and contributes to high level fora
such as the:
South West Wales Regional Academic Health Sciences Hub;
South East Wales Academic Health Science Partnership; and
UK National Ambulance Services Research Group.
Planned Research activities for Year One of this plan include:
Action 104: Delivery of RAPID / TIER / PARAMEDIC-2 / RIGHT-2 trials
Action 105: Develop a work plan to support the R&I Strategy
Action 106: Develop Intellectual Property Rights and revenue Sharing Agreements
6.6 Service Improvement
Our Service Improvement (SI) Team has an overall aim of supporting the Trust to spread good practice, and to increase its capacity for sustainable change. The SI Team works alongside Public Health Wales, and in particular, the 1000 Lives Plus
Programme, to improve patient care through the adoption of standardised methodology.
The SI Team has consistently had two primary corporate objectives recurring annually. These are:
to provide direct expert SI support to the organisation to improve certain systems of patient care; and
to establish a learning centre to support all staff in developing their own SI skills / knowledge, which will enable WAST to run numerous programmes of improvement.
The Service Improvement Team provides support within the context of the four underpinning principles of Prudent Healthcare and it supports WAST to change how services are designed and delivered so that patients are always put first. As a result of this ‘patient-centred approach’, the SI Team is part of the Medical and Clinical Services Directorate as outlined above. This enables the team to benefit from the clinical leadership of the Executive Medical Director, and engage in team working with other lead clinicians. The focus for 2015/16 of this specialist resource was to:
design a model for the demand generated by Card 35 processes (STEP 3 deliverable);
prepare CCC staff with the necessary skills and knowledge to adopt the revised response model – ‘go – live’ with the new response model from 01 /10/15 (STEP 3 deliverable);
design and create an ICT framework to enable staff to submit innovative ideas and receive timely feedback;
undertake a monitoring plan to constantly review the testing period of the new response model 01/10/ 15 – ongoing through to 01/10/16 (STEP 3 deliverable);
launch the ‘Sense Maker APP’ to test a method of capturing ideas from staff in real time – testing period until 31/03/16;

170
falls pathway for all paramedics to access community services on behalf of patients who are not injured / ill as a result of a fall;
referral process for all paramedics to inform a patient’s General Practitioner (GP) of resolved epileptic seizures and hypoglycaemia events;
Mental Health Pathway (tested in the Cardiff and Vale Health Board area);
development of a specific dispatch and transport service for the predictable demand of Health Care Professional (HCP) low acuity patient admissions to hospital; and
testing of a dedicated ‘Falls Response Service’ with a joint team of paramedics and community healthcare professionals (e.g. physiotherapists and occupational therapists).
Importantly, all frontline-led developments have been captured through the planning process for the
IMTP with developments throughout local delivery plans for each Health Board area and
directorates.
A governance process for supporting innovation for the Trust’s Five-Step New Clinical Response Model (or Patient Pathway) has been established. A structured approach has been created through the work of the Clinical Prioritisation Advisory Software (CPAS) Group, and the Clinical Pathways Advisory Group (CPAG). Both groups are medically / clinically-led, and are the main fora for considering, supporting and developing new ideas / ways of working in relation to call handling and dispatching to calls (CPAS), and to delivering patient treatment and care (CPAG). The principle objectives for the service improvement team for the period of this plan include:
Action 107: Support the production of an external evaluation report on the new Patient-Centred
Clinical Response Model (PCRM), by being the main point of contact for the
organisation that is awarded the successful tender by EASC. Providing an
independent and objective report that measures key elements of the innovative
PCRM, which is likely to attract both national and international interest.
Action 108: Design a web-based Ideas Portal to enable staff to develop ideas/innovations to improve Trust core business. The system design will ensure that all ideas are aligned to the Trust’s strategic objective of highlighting the importance of innovation across the Trust.
6.7 Health Informatics and Business Intelligence Health Informatics provide information services to all facets of the organisation and are broadly
arranged under the following functions:
1. Information services and business intelligence
2. Information governance & records management
As the Trust has re-orientated itself as a clinically-led quality-driven service, rapid transformation is
reflected in the Trust’s business information assets as there is an increased dependency to
continuously increase the access to, and analysis of, clinical and non-clinical information to improve
and optimize decisions and improve patient care. We are already on a development pathway to
better manage the Trust’s information assets - a best of breed data warehouse (Microsoft and Data
Academy) has been in development over the past 6 years which includes data from mission critical
systems such as CAD, Cleric and Clinical Solutions as well as CCC telephony and elements of
information streams from Datix. A data warehouse-based clinical indicator monitoring system has
been introduced since the digitalisation of the Trust’s patient care record in 2015, which is shown in

171
the literature to have both clinical effectiveness and efficiency benefits as well as improved systems
operating experience.
Building on this work, the department will stabilise the existing information asset management in
year 1 through improved governance structures and procedures, including setting up an information
governance steering group. A key dependency will be on ensuring that data quality is a top priority
for business units as well as clearly linking information outputs with the business processes
underpinning them.
A key work programme this year will be to support the Quality Improvement, Measures and
Assurance system. Improving the organisation’s ability to realise the benefits of its information
assets will include a review and investment in business intelligence tools as legacy information
portals such as Launchpad are outdated and no longer reflect the business requirements. As such a
business intelligence strategy will be developed which includes an immediate requirement to
continue to develop the data warehouse.
In addition to these requirements is the production of our organisation’s commissioning dataset for
unscheduled care and non-emergency patient services to support the new commissioning agenda.
As the roll-out of national and local commissioning arrangements continue, how we share
information with our partners and regulators is rapidly changing. The department will continue to
support internal and external capacity and service reviews such as the outcome of the New Clinical
Response Model evaluation. The implementation of information tools such as Optima, CAD and the
Signalsfornoise pilot will require resourcing from the department, the demand for which is unknown
at this time. An important scheme of work has been to develop an information portal for how we
locally engage with our communities which supports the benefits of prudent healthcare and
coproduction. It is expected that this service will continue to develop over the lifetime of this 3-year
plan.
Building on the foundations of year one, key features of year two and three will be:
to support the clinical leadership structure with new information for clinicians to understand
and develop their own and others’ clinical practice;
to support better management and reduction of demand through new streams for health
information to be delivered to support the self-care agenda in NHS Wales;
to support CCC to embed a performance management framework into the new staff teams
to deliver performance improvements which may require a rework of the existing information
landscape and indicators;
to supply information analyses to review of all dispatch points, engaging with the operational
areas and reviewing zones and priorities will be key to ensuring the Trust is efficient and
effective in its service operations;
continue to support the strategic planning agenda, including modelling of options and
scenarios, and
ongoing support of the performance management framework, the reporting of performance
information in quantitative forms and creating new information lenses through which to view
initiatives such as clinical pathways and public access defibrillator sites.

172
As such, key actions include:
Action 109: Develop a long-term plan for new streams for health information to be delivered to
support the self-care agenda in NHS Wales.
Action 110: Develop a business intelligence strategy and associated programme of work for a
long term roadmap of the management of information assets in the Trust.
Action 111: Document a long-term plan to incorporate additional data streams into the data
warehouse such as clinical data and risk management information.
Action 112: Develop a data quality strategy that will maximise the completeness, accuracy and
timeliness of clinical and non-clinical data within the Trust.
Action 113: Develop a data dictionary coterminous, where relevant, to national data descriptors.
Information Governance and Records Management
We will strengthen the Trust’s Information Governance standards to maintain our clinical and
corporate information’s confidentiality, integrity and availability. On an annual basis, every Health
Board and Trust in Wales must complete the Caldicott Principles Into Practice (C-PIP) assessment
in relation to Information Governance. The organisation is then provided with an outturn report that
highlights areas of improvement for the following year. Whilst it is recognised that the Trust has
increased its performance of this assessment from 34% to 82% over the past seven years, areas for
improvement arising from this assessment and Standards for Health assessments include
information governance management, information governance training and records management. In
response to this, an Information Governance Steering Group has been established to formalise the
management arrangements of information governance. Going forward, there will be a need to
develop an Information Governance strategy and associated policies to ensure the Trust has a long
term plan for delivery. In order to address the information governance training gap, the IG team has
worked with the Trust’s education and training department to strengthen the arrangements for IG
training at induction for clinicians and as part of mandatory ongoing training.
In order to address the records management gap, a records and archives manager has been
employed encapsulating the totality of the Trust’s records management resource. This work area is
historically fragile and the scale of this programme is substantial. Work this year has delivered
against a project to centrally store historical patient care records (PCR’s) of which there are circa 1
million. With minimal investment, the department has resolved a quarter of a million records to date
and is forecast to double this figure during the first half of 2016/17. Building on this will be the need
for a robust records management strategy and associated policies since there has been no
corporate ownership or investment in records management previously. As an immediate priority,
work to develop a Trust wide information classification system for the security marking and handling
of information assets will be complete. A larger programme of work is to develop the Trust’s
information asset register and to identify and take forward information asset owners for all facets of
the organisation where electronic or paper records are stored.
Priorities for this area include:
Action 114: Develop an information classification system for the security marking and handling of
information assets.
Action 115: Develop an Information Governance Strategy and policy directory to strengthen
Information Governance Management.
Action 116: A baseline review of the Trust’s records through inventory and information asset
owner’s directory to create a central register of records.

173
Action 117: Implement at Trust wide Records Management (RM) policy and framework, which
complies with the legislation and regulatory standards (ISO 15489).
6.8 Information Communication & Technology (ICT) Over the life of this plan, the vision of the ICT department will be to support the Trust’s strategic
transformation and modernisation agenda through providing Trust staff with an electronic, patient-
centred view of information in order to support high quality care.
The high level strategic priorities for the ICT department are as follows:
Maintaining and improving the ICT Infrastructure
To support the transformation of the Trust, a robust and resilient ICT infrastructure will be required
as a greater reliance is placed on electronic information and the ability to access such information
by increasing numbers of staff. Future plans must be in place to ensure we have sufficient flexibility
within the ICT Infrastructure to scale up to meet this demand.
Action 118: Improve and enhance the ICT infrastructure to provide a basis to support the implementation of new systems and solutions including the greater use of mobile and remote working technologies which will enable staff to access relevant information at the point of care and away from their ‘base’. (Years 1, 2 & 3).
The Trust’s ambition to ensure all staff have easy access to an electronic device will lead to a
significant improvement in two-way communications. This will enable greater and quicker
compliance with information such as clinical notices, but will also enable provision of support
through, for example, a health and well-being App. Mobile devices will also support clinical
decision-making when caring for patients by providing electronic access to tools like the Paramedic
Pathfinder and alternative care pathways for treatment.
Action 119: As reliance on ICT systems and electronic information increases, there will be a need
to review and revise business continuity and disaster recovery procedures to ensure
robust safeguards are in place (Years 1, 2 & 3).
Working with corporate departments to improve operational information systems
We will work across all areas and programmes within the Trust to improve current operational
information systems while ensuring they meet the needs of the Trust and, as far as possible, comply
with national standards. In conducting this work, we will ensure that data quality is critical as the
information needs to be up-to-date, accurate, and available wherever care is being delivered.
Making this a practical reality is a significant challenge in light of the continued reliance on paper
records, the number and variation in IT systems in use across the Trust and the level of investment
in technology required to enable and sustain change and modernisation
Action 120: Work with colleagues within the Trust on implementation of operational and business solutions and to enhance the capability of current systems.
o implementation of the new CAD (year 1) o Implementation of a NEPTS planning and coordination system to
replace the existing CLERIC system (year 2). Action 121: Delivery of the Emergency Services Mobile Communication Programme (ESMCP)
having started will see a need to mobilise a Trust project to support implementation

174
of the Emergency Services Network (ESN) and associated works for the Trust.(Years 1, 2, 3)
Action 122: We will also look to commence work on a potential replacement roster solution (Year
3)
Improve information sharing and collaboration by working with partners across health and
other sectors
We will work with other Health Boards, Trusts and NWIS to share patient and clinical information. In
the short to medium term, the approach will be to identify opportunities that maximise the benefits of
investment in existing information and technology in order to provide more joined-up clinical
information to Trust staff at the point of service delivery.
Action 123: Work with colleagues in ABM and the wider NHS along with key suppliers to deliver and support the introduction of 111 pathfinder project (Year 1) and to implement a new patient management system to support the national 111 service to replace the existing CAS system (year 2& 3).
Action 124: Work with NWIS to provide access to national information resources, such as the
Master Patient Index (eMPI) and Individual Health Records (IHR) as well as investigating options to provide Trust information into national repositories, such as Welsh Clinical Records Service (WCRS) and national systems such as EDCIMS and CCIS. (Years 1 and 2)
Improve staff access and patient engagement and access
Considerable technological advances and mobile coverage improvements over recent years have
presented an opportunity to promote and develop a greater use of mobile and remote working
technologies which will enable staff to access relevant information at the point of care.
We will need to ensure that systems are capable to supporting mobile and agile working within the Trust and similarly ensure appropriate choice of end user devices to carry out routine tasks. Opportunities will arise to investigate options around ePCR as ESMCP will improve mobile coverage and the initial three-year Digi-Pen contract will be due to expire.
Action 125: As Microsoft support for Office 2007 is due to end we will need to be upgrade Office in order to mitigate any security risks and capitalise on modern functionality which will support the provision of remote and mobile working for operational staff.
Action 126: Review options around ePCR as the initial 3-year Digi-Pen contract will be due to
expire (Year 3)
Similarly, we will also look at leveraging these technological advances to improve patient
accessibility to Trust services through deploying a wider range of services securely via the internet
to better direct patients and the public to the care they need at the right time, thus supporting the
prudent healthcare agenda.
Action 127: We will work with colleagues across the Trust to look for opportunities to maximise the benefits of patient self-service (Years 1, 2, 3).

175
Develop the skills and professionalism of ICT staff
In order to achieve this ambitious programme of work, it will be essential that ICT staff are given the
appropriate skills to ensure they are equipped to play their part in supporting future developments
and technologies.
Action 128: Conduct a baseline of the current skills and abilities of ICT staff and identify any gaps in key technology areas. Develop a structured development programme for each member of staff (Years 1, 2)
6.9 Partnerships and Engagement
Our recently refreshed purpose and vision statements emphasise our values, which involve caring for our patients and staff and securing improved outcomes for those who use our services. Achieving improvement is not just a function of process, organisational or system change. It is predicated as much on working with our employees, our patients, the wider public and our stakeholders to shape change, to help us understand what’s important to our staff, the people we serve and our partners and to develop our services in a way that genuinely reflects the needs of our population. It is only by working in this way that we will begin to move away from a culture predicated on today’s issues, to one where we are focused on tomorrow. We now need to move forward this agenda with pace, discipline and cohesion if we are to realise the substantial organisational gains which effective partnership and collaboration offer.
This means looking at how we work together to build mutual understanding and support to create better, more productive relationships and more resilient communities: ultimately, to, deliver better services for the people we serve.
We have a unique role in the Welsh NHS as a bridge between two significant elements of our public services, the NHS community and the emergency service, blue light family.
We are committed to working with our emergency service partners (and our current activities are
outlined in section 5 (STEP 2), section 5 (STEP 3), section 6.3 and section 6.10.). We want
to do this in an even more collaborative and integrated way, identifying shared opportunities to learn and work together. How we do this in a way that adds value for the people we serve, and for our respective employees, remains an important debate for us that we will need to conclude and deliver on within the lifetime of this IMTP.
Wrapped around this whole agenda is our wish to be a more open, communicative organisation that tells its story better through our employees, our patients, the media and to politicians. We hope that, in so doing, we can develop a shared understanding of the improvement journey we have embarked upon, what it means, why it's important and how everyone can support us to deliver an ambulance service of which everyone in Wales can be proud.
During the last 12 months, we've started to redefine our future, but there's still much work to do.
While our engagement activities straddle a number of Director level functions, for example Quality, Safety and Patient Experience and Workforce and Organisational Development, the Trust has also established a new Directorate of Partnerships and Engagement, the purpose of which is to bring coherence and strategic insight to the Trust’s engagement and partnership agenda, as well as protecting and enhancing the reputation of the Welsh Ambulance Service among its many stakeholders.

176
This agenda, for the first time, now has prominence at Board level through the Director of Partnerships and Engagement and demonstrates the Trust’s commitment to working more effectively and collaboratively with stakeholders to deliver tangible organisational and service benefits.
Analysis
As an organisation, we have recognised that the risks of not engaging better outweigh the risks of
maintaining the status quo, but this does not mean that the engagement journey will be smooth.
Financial pressure across the public services, coupled with increasing demand for healthcare,
including ambulance services, means that, while the need for collaboration has never been greater,
the risk of organisational retrenchment poses a real threat, both by WAST and our partners.
Strong leadership and organisational courage will be needed to ensure that we deliver what is
needed to move us away from an organisation focused on the problems of today, to one which is
redefining its purpose as a clinically-led service on the frontline of emergency, pre-hospital and
scheduled care.
Similarly, the organisation’s tendency towards silo working is a risk in engagement terms, which is
why the development, delivery and evaluation of an engagement strategy which has a broad base
of support across the organisation, and from stakeholders, will be so critical to the success of this
work.
Feedback from patients and the public provides a rich seam of organisational insight that is
currently underutilised in the decision-making process. There is a huge opportunity to triangulate
data from patient experience, including concerns, staff, stakeholders and others to give the
organisation an insight into its strengths and weaknesses and to identify opportunities for further
development and collaboration.
Partnership and Engagement Priorities for 2016/17 – 18/19 Our objectives in delivering a refreshed approach to partnership and engagement are:
To deliver better services to the people we serve
To position the Welsh Ambulance Service at the forefront of public service collaboration
To add operational capacity within the organisation and reduce demand on services through better public engagement and education
To improve our reputation and restore public/political confidence in our ability to deliver Given the all-Wales nature of the organisation, and the elevated temperature that often surrounds the wider unscheduled care system and the performance of the Welsh Ambulance Service particularly, the significance of positive engagement with our staff and partners cannot be overstated. One of our primary goals over the lifetime of this IMTP will be to develop an integrated approach to engagement that allows the organisation to systemise its engagement more effectively, identifying clearly the outcomes it is seeking to achieve through partnership and collaboration. Part of this will be to ensure that the principles of effective partnership and engagement underpin organisational priorities and that the organisation actively seeks opportunities to optimise its delivery through identifying appropriate and realistic opportunities to work collaboratively with partners. Similarly, in galvanizing staff around new ways of working and developing the organisation into one that is genuinely clinically-led, the involvement of colleagues will be key. This must be

177
complemented by a robust and comprehensive approach to listening to our patients and wider stakeholders, providing mechanisms for their experiences and ambitions to be heard and keeping them involved in our improvement journey in order that they understand what needs to change, why and how they can help. Importantly, the Trust will develop mechanisms to source, triangulate and interrogate stakeholder intelligence in order that the organisation has its finger very firmly on the pulse. While the challenges we face are not necessarily easily segmented by stakeholder, they centre on a number of key areas. Detailed below are some indicative actions that we will be taking in the partnership and engagement realm over the life of this plan. Please note that this summary section of our engagement priorities set out below should be read in tandem with the relevant more detail sections, e.g. Workforce (section 6.1) and Quality (section 4). Workforce
Listening to our staff using a variety of face-to-face, digital and other tools and working with them to develop new models of care/ways of working which are supported
Ensuring our people are advocates for the service and feel confident in advising patients and the wider public on lifestyle choices and use of NHS services, using the “Making Every Contact Count” model. This means ensuring colleagues understand the priorities and ambition of the Welsh Ambulance Service as one which is clinically-led and has a public health remit. This approach will support the Service’s demand management activities
Ensuring our staff understand their contribution to delivering our objectives through a robust process of PADR and that they are involved in shaping our services and the way in which they are delivered
Ensuring that staff understand the importance of listening to patients, that it is everyone’s business and that we provide them with the right tools and training to do so
Ensuring the experiences and views of patients are fed back to staff, good and bad, so that staff have an opportunity to reflect on and understand what it feels like to be a Welsh Ambulance Service patient, helping to inform their clinical practice and communication skills
Ensuring our policy development agenda is informed by feedback from staff
Ensuring our relationships with recognised trade unions and professional organisations are predicated on mutual respect and understanding and are underpinned by a culture of partnership
Patients
Listening to the experiences of our patients and learning from them in a way that actively influences service delivery, including those from seldom heard groups. This will include reporting patient experience feedback in the right format and fora to influence decision-making
Ensuring that the tools we use to measure patient feedback are sufficiently robust and diverse and that we analyse feedback data in a systematic way. This will involve a review of how this is currently undertaken and any necessary changes made
Ensuring that we are triangulating all the patient feedback we receive, be that via concerns, compliments, serious incidents, media coverage or other sources to ensure we understand what our patients are telling us and sharing that across and beyond the organisation in a systematic way
Ensuring that the Board and leadership team review patient feedback regularly and that it is reported in an open and transparent way
Ensuring we publicise to patients, staff and the wider public what we have done in response to the feedback we have received. We will undertake a review of current practice to ensure we are doing this well
We will analyse how well our online tools work by reviewing how patients use the NHSDW website and analysing its potential and use as a call attendance/avoidance mechanism (i.e.

178
does it serve a preventive purpose?). We will do this by working in partnership with colleagues across the unscheduled care system to understand the journey of our NHSDW patients across the unscheduled care pathway
Public
Supporting members of the public to understand our ambition and our New Clinical Response Model, as well as the wider unscheduled care system, so that they understand when and how to use the services we provide by reviewing and refreshing our approach to communicating our New Clinical Response Model and ambition
Engaging the public in widespread and varied conversations, embracing the full range of groups, ethnicities, ages and genders, to stimulate debate and mutual understanding on the role of the Welsh Ambulance Service in the wider health system by seeking opportunities to collaborate with partners on appropriate opportunities,
Ensuring our engagement methods are diverse and robust, embracing social media, face-to-face and more traditional methods to seek and provide feedback
Ensuring that our engagement activities are aligned with organisational objective and support the needs of operational staff by regularly reviewing work programmes and sense checking against organisational requirement
Stakeholders
Optimise the use of our resources for the benefit of the people we serve by identifying and exploring opportunities to work more collaboratively with partners to deliver better services for people in Wales
Build trust and confidence in the Welsh Ambulance Service as a respected and dependable partner that is innovative and open to collaborative opportunities. We will do this by delivering on our commitments and being a visible and present partner in key public service arena
We will work with our political and media stakeholders to uphold the reputation of the Trust by celebrating our successes and being open and transparent where improvements are needed, and by responding in a timely fashion to requests for information, data, concerns, media enquiries etc
We will map our engagement activities using an engagement database to ensure we are working in an equitable fashion across Wales and that we are capturing the feedback from stakeholders in a way which informs future interactions
Evaluation
In adopting a revised approach to collaboration and engagement, it is important that the impact of
these changes is understood and kept under regular review.
In this respect, the planned Engagement Strategy will set out how, and at what intervals, work in
this area will be reviewed so that outcomes are evaluated and any issues identified at an emerging,
rather than at a potentially critical, stage.
As the IMTP is a living document, so its various iterations will continue to refine what and how we
“do” engagement, so that it keeps pace with organisational and stakeholder requirements.
Action Plan
Action 129: Agree a definition of engagement internally to avoid ambiguity and to provide
organisational clarity (2016/17)
Action 130: Review engagement activities taking on board the views of stakeholders as to their
effectiveness (2016/17)

179
Action 131: Review organisational structures to ensure that the organisation is set up to deliver
its engagement agenda effectively (2016/17)
Action 132: Agree at Board level its collaborative priorities for the period 2016/17 to 2018/19
(2016/17)
Action 133: Introduce a system of stakeholder account management to ensure consistency of
approach and contact at Director level (2016/17)
Action 134: Develop and deliver an engagement strategy which outlines our partnership and
engagement priorities and identifies a system for collating feedback and feeding this
into the decision-making process at Executive and Board level (2016/17)
Action 135: Agree and deliver one key priority with its top 6-10 stakeholders in 2016/17 and
repeat in 2017/18 and 2018/19
Action 136: Undertake a baseline stakeholder assessment in 2016/17 and subsequently in
2017/18 and 2018/19 to track progress against objectives
Action 137: The Board to agree the introduction of collaboration as a fundamental operating
principle against which organisational developments will be measured (2017/18)
Action 138: Continue the work in progress measuring Patient Experience to inform us what it is
like to be a user of Welsh Ambulance Services (and identifying issues affecting all
communities within Wales)
Action 139: Real time capture of patient experiences
o reporting themes
o working with colleagues to identify and implement learning
o identify services changes/benefits
o feedback to patients/service users of changes
Action 140: Work with other emergency response organisations such as the fire service and
police force to consider how we better interface to streamline response and meet
community needs
Action 141: Collaboration with NHS colleagues and voluntary/3rd sector organisations on shared
capture of patient experience; learning and actions to improve experiences of the
NHS care/treatment pathways
Action 142: Integrated reporting of all methods of patient/service user feedback.
Action 143: Develop a Patient Experience Diagnostic Tool to measure where the Trust is against
best practice in patient experience, engagement and learning.
6.10 Corporate Governance and Risk Management
In simple terms, governance refers to the way in which organisations ensure that they are doing the
right thing, in the right way, for the right people, in a manner that upholds the values set for the
Welsh public sector.
The Board has overall responsibility for ensuring good governance within the Trust. The Board is
responsible for setting strategic direction and satisfying itself that there is a good system of

180
governance and internal control in place, underpinned by an effective risk management system. The
Board will oversee the delivery of the Trust’s Strategic priorities and the non-executive members of
the Board will hold the Executive Team to account for performance and delivery.
We recognise that the effectiveness of our governance arrangements has a significant impact on
how well we meet our aims and objectives.
We also recognise that, as the Trust evolves and grows, so too must our governance systems and
processes. As a consequence, during 2016/17, a great deal of emphasis will be placed on ensuring
that our governance and risk management systems are fit for purpose and have or are adapting to
meet the considerable strategic and operational changes taking place within the Trust. Such
changes include the New Clinical Response Model, the new 111 non-emergency helpline and the
revised management arrangements around the Non-Emergency Patient Transport System
(NEPTS).
Work has already begun to strengthen the governance and risk management frameworks. This
includes the delivery of a Board Assurance Framework, a review of the groups and sub-committee
structures that support the Board and Board Committees, and a review of the risk management
arrangements, including the corporate risk register. The outcome of this work will be seen and
introduced during 2016/17.
Additionally, in October 2015, the Trust Board commissioned an internal review of the governance
processes and in November 2015, agreed seven key areas of improvement. The Board agreed to
implement a revised Board assurance and risk management framework over the lifespan of this
plan aiming to form an integral part of the successful delivery and sustainability of the following set
out below.
Integrated Medium Term Plan (IMTP) & programmes of change
Organisational Development Strategy
Planning & performance management framework
Quality Improvement Strategy 2016-19
Research & Development Strategy 2015-19
Clinical Audit Programme
Meeting Commissioners requirements through the Commissioning Quality & Delivery Framework (CQDF) – CAREMORE® Framework Patient Care Pathways and Core Requirements and
Inform the Annual Governance Statement.
Action 144: Implement and embed the Risk Management Strategy & Framework 2016/19
approved at Trust Board in March 2016 and assess maturity in 2017/18
Action 145: Develop a Board Assurance Framework (BAF) document mapped to the strategic
aims and priorities
Action 146: Development & embedding of the content and breadth of the new Corporate Risk
Register (CRR) and Local Risk Registers (LRR) with central oversight, monitoring
and reporting
Action 147: Review the effectiveness, reporting and monitoring arrangements of groups sitting
below sub-committee level.
Action 148: Implement a document management system with supporting policy and guidance.

181
Action 149: Undertake a Trust-wide safety culture assessment
Action 150: Development of Datix as the supporting infrastructure for the management of risk and
concerns, monitoring of improvement plans and sustainable organisational learning.
Risk Management and Risk Appetite
The Risk Management Strategy & Framework 2016/19 was approved by the Trust Board in March
2016. This document describes the approach the Board will take in developing its risk appetite and
tolerances in relation to the strategic aims and priorities for 2016/17. This will link to the
development of the Board Assurance Framework document.
Whilst risk is inherent in many of our activities, the Trust will not accept risks that materially impair
the ability to deliver services to a high standard of safety and quality. As such, the Trust will not
accept risks that materially impair its reputation or cause any disrepute with stakeholders.
In common with other NHS providers, the Trust is limited in the extent to which it is permitted to use
public funds to reduce/eliminate risks. This is a major influence in determining the risk appetite of
the Trust.
Meeting our Statutory Obligations:
As an organisation we have a rage of statutory obligations many of which are documented in our
standing orders.
Under the Civil Contingencies Act 2004 (CCA) Category One responders (such as WAST) are also subject to the following set of legal civil protection duties:
risk assessment;
emergency planning;
business continuity planning;
warning and informing;
information sharing; and
co-operation.
As part of discharging these duties during the life of this plan we will undertake the following actions;
Action 151: PREVENT training (counter terrorism)
Action 152: Tier One Multi-Agency Exercise
Action 153: Re-write of the Trust’s Major Incident Plan to meet best practice
Action 154: Commander Competency training and roll out of National Occupational Standards

182
PART 7: DELIVERING OUR PLAN
This section describes our localised approach to planning and how we will deliver our plan, including scrutiny and performance management.
7.1 Approach to Planning
The Trust has adopted an integrated planning approach for development of this and future IMTPs.
This approach recognises that the Trust will be able to better develop clear medium and long term
strategic objectives which in turn frame the development of short, medium and long-term service
improvement plans. The trust is fundamentally changing the way in which it has “done planning”
over recent years and is guided by the following key principles:
ensuring a clarity of purpose, vision and priorities to shape the plan and Local Delivery Plan
(LDP) process;
board engagement through all stages of plan development;
prudent healthcare and the new Quality Strategy as a golden thread throughout the plan;
a multi-disciplinary group overseeing the planning cycle;
using a wide stakeholder group to explore action against the five-step model;
early and detailed work on the financial baseline position, exploring opportunities for further
efficiencies, using benchmarking, analysis and peer review to challenge the organisation;
improved alignment across the service, workforce and financial elements of the plan through
the IMTP delivery group and senior planning, workforce and financial input from the outset
and throughout;
built on improved modelling of activity and demand;
informed by and aligned to the strategic planning agenda across wider NHS Wales (for
example the Mid Wales Collaborative, South Wales Programme, joint work with Fire and
Police service);
consolidation of the critical national policy and legislative drivers that will impact on WAST
over the three year period, the impact of the Well Being and Future Generations Act, the
Well Being and Social Services Act and the outcome of the Green paper consultation;
early and ongoing engagement with key partners and stakeholders;
early and ongoing engagement with our Partnership forums;
building on the benefits and credibility of having a clear New Clinical Response Model whilst
demonstrating ambition in terms of future opportunities; and
reflecting the strengthening relationship with and influence of the collaborative Commissioning Quality and Delivery Framework.
This is a maturing approach, an approach that the organisation remains committed to however recognises that it will be a number of “cycles” before the organisation is entirely comfortable with the nuances of this sort of approach. Nevertheless significant strides have been made.
7.2 Plan Delivery
The organisation has developed a very strong delivery focus, which has been developing year on year since the Strategic Transformation Programme in 2014.

183
Over the course of the last two years the organisation has sharpened its focus on a number of key principles:
a programme and project management model that tracks performance/delivery against plans;
a reinforced approach to managing all activities with robust governance and focused performance management; and
an overarching delivery framework that supports delivery by specialist advice and a programme infrastructure and support.
We have identified four strategic change programmes that will support and drive delivery, in a co-
ordinated way, of a number of the actions contained within this plan. These programmes have
previously been identified in section 5 but for clarity are;
Clinical Modernisation
Clinical Contact Centre Modernisation
Non-Emergency Patient Transport
111 Pathfinder Project
We have also created a Planning and Business Intelligence group that is intended to be a
permanent business structure and an Executive Finance Group.
An overview of the structure we are putting in place can be seen in Figure 30 below. A deep dive
into the individual programme structures can then be seen in appendix 8. Finally Figure 31 below
offers a little more detail on each of the programmes and group we have put in place.
This structure does not abandon the delivery mechanism that currently exists, which has been
driving strategic change within the organisation. Rather it has taken lessons and built on the
existing structures to ensure focus is retained, bureaucracy is minimised and the chances of
success are maximised.
We have taken direct scrutiny of change management out of the Executive Team forum. This
scrutiny is now undertaken by a Delivery Assurance Group. We nevertheless recognise the
importance of the Executive Team retaining a line of sight of the holistic delivery of change thus this
assurance group will report on a monthly basis to the Executive Team.
The Trust Board will also receive strategic change updates (and wider IMTP implementation
updates) in line with NHS Wales planning guidance.
The delivery assurance group will be chaired by the Director of Planning and Performance.
Membership will constitute the senior responsible owner (SRO) and programme manager for each
programme of work along with representatives from other key areas across the organisation. The
high level purpose of the group will be to:
Ensure programmes deliver within agreed parameters (time, resource and scope)
Resolves strategic issues between programmes
Makes resource decisions in regards to delivery
Give approval (or not) of key milestone outputs and authorisation to proceed to next phases.
We have been careful to build a delivery structure that offers assurance and rigour to the complex process of change management; however we have balanced this with a structure that is capable of managing and adapting to the dynamic environment within which we, and the wider NHS in Wales, operate within. Consequently this structure might evolve further overtime.

184
Figure 30

185
Clinical Modernisation Programme
Purpose
The purpose of the Clinical Modernisation Programme is to drive and ensure performance of the
New Clinical Response Model during the 12-month pilot, which started on 1 October 2015. The
impact of the New Clinical Response Model will be monitored and managed using a revised set of
performance measures and clinical indicators; this will include the impact on service users to
ensure delivery of high quality care and a positive service user experience. The Clinical
Modernisation Programme Board will oversee implementation of the New Clinical Response
Model, ensuring it is clinically-led and managed in a systematic way, including monitoring
progress against agreed milestones.
The Programme is designed to support the recommendations of the McClelland Strategic Review
of Welsh Ambulance Services (2013) and is aligned to the NHS Wales agenda; Our Plan for a
Primary Care Service for Wales up to March 2018 (2015), Health and Care Standards (2015) and
Prudent Healthcare Principles.
Actions which the programme will own
Actions 18, 19, 24, 25, 28, 30, 31, 32, 33, 34, 35, 36, 37, 38, 40, 44, 45, 47, 62, 126
The programme will be structured to mirror that of the New Clinical Response Model, i.e. STEP 1
help me choose project, STEP 2 answer my call project…..
The programme will own a range of actions across the New Clinical Response Model.
Clinical Contact Centre Modernisation Programme
Purpose
Clinical Contact Centres are at the heart of the organisations operations. This programme has
been designed to oversee the vast transformation and modernisation of processes, infrastructure
and practices that currently exist within the function. There are many inter-dependencies
associated with modernising our CCCs and this programme Board will have a key role to play in
managing both internal programme dependencies and also the dependencies which exist with
other change programme.
Actions which the programme will own
Action 23, 26, 100
Non-Emergency Patient Transport Programme
Purpose
A NEPTS implementation programme board has been created to directly oversee the
recommendations of the NEPTS business case which was approved by the minister in January
2016. It will have direct oversight for a number of work streams that will each individually focus
on a number of the recommendations.
Actions which the programme will own
Action 48, 49, 50, 51, 52, 53, 54, 55
Figure 31

186
111 Pathfinder
Purpose
This programme represents the pre-existing Joint Implementation Group (JIG) which exists
between the Trust and the 111 Pathfinder project team.
Actions which the programme will own
Action 27, 123
Executive Finance Committee
Purpose
To lead and oversee the delivery of the Trust’s financial plan.
Planning and Business Intelligence
Purpose
To ensure all work associated with demand prediction/capacity assessment, strategic
development intelligence etc. is captured by a focal point within the organisation and can be
reviewed, examined, challenged and shared with the result of the organisation in a coordinated
and coherent manner. This group will both;
Act as an enabling function to the four change programmes
Represent a permanent business structure to support management of core business
Those actions we have committed to in this plan that do not map to one of these strategic change
programmes are being managed ‘internally’ by the relevant Directorate as part of their business as
usual activities. Scrutiny of delivery will be managed via renewed Performance Management
arrangements that aim to embed a culture of performance improvement. An overview of the
performance hierarchy and escalation process within which all these actions are to be managed is
shown below in Figure 32.

187
Figure 32
Assurance- Performance and Management
From the 1 April 2016 we will be implementing a set of core performance management principles
that over the course of Q1 and Q2 of year one will be formalised into a fully agreed Planning and
Performance management framework for the organisation.
The purpose of the framework will be to support the delivery of the right clinical care at the right time
through good planning and performance improvement, in particular, improved patient flow and
effective resource utilization.
A good Planning and Performance Improvement Framework should help front line staff do their jobs
and help remove barriers that are preventing them from giving their best.
7.3 Risks and Issues to plan delivery
It is recognised that every action identified in this plan has risks and issues attached to delivery and
these are highlighted at a high level in appendix 5. Action owners will be actively managing these
risks/issues and mitigating them to a tolerable level. The performance management arrangements
identified above will then ensure the appropriate escalation where necessary.
However there are a number of overarching risks and issues that exist in relation to plan delivery.
These are documented below.
Annual Report
6 Month JET Review
Quarterly Assurance Reports
Integrated Performance Report & Programme Reports (monthly)
Directorate Performance Reviews (inc Heads of Operations)
In month reports
1:1s and PADRs

188
Political Landscape. The life of this plan will see both a Welsh Assembly election and a
referendum on the UKs membership of the European Union. Both could have
consequences for the organisation, the targets to which we are expected to perform and our
strategic direction.
The wider unscheduled care system in NHS Wales. We are a vital partner in the
unscheduled care system within Wales and we must work closely with all other stakeholders
to re-engineer the system. The system is under pressure and at periodic points throughout
the year escalation levels are such that delivery of our plan will face some risks, as will
delivery of LHB plans. We are committed to working with our LHB partners and WG to
better plan for these peak times (through the Seasonal planning process). Our plan will be
sensitive to these risks and we will work agilely and proactively to mitigate.
A commissioned service. We recognise that we are a commissioned service and must be
responsive to the collaborative commissioning arrangements, including any decisions
regarding performance and funding levels. We have a good relationship with the
Commissioner and will endeavour to maintain this, however planned delivery is dependent
on being commissioned to the level that we have assumed.
Planning assumptions. In developing our plan we have had to make some explicit
assumptions (section 6.2 details our financial assumption for example). These assumptions
have been in relation to our finances, performance targets, availability of capital, no
significant changes to demand etc. Should these assumptions not prove to be accurate, we
will have to revisit sections of the plan. The sensitivity if each assumption may vary. We
will use the demand and capacity modelling exercise to test the sensitivity of the
assumptions through what if scenarios. Our financial planning assumptions have been
shared with our Commissioner repeatedly and the advice has been that these were
reasonable and in line with what other NHS Wales organisations are assuming.
Many of the risks and sensitivities to our workforce and other plans have been referenced
throughout this plan. These include:
Recruitment of sufficient numbers of EMS staff. We have already described our intent to maintain a focus on the recruitment of qualified paramedic and other frontline staff whilst further work is done to understand the true picture of demand and capacity of our services across Wales. There is a national challenge to the recruitment of qualified paramedic staff, and our education commissioning numbers are just about sufficient to ensure adequate supply of qualified staff provided we are able to secure employment of the graduate paramedics. The move to a degree requirement for future paramedics may also impact on our current career pathways and supply channels of EMTs converting to paramedics. Failure to recruit in sufficient numbers will result in the continued use of overtime and external providers at premium costs to support operational delivery. However, to date we have been successful in our recruitment plans, and we will continue to target our recruitment activities and plan our training courses appropriately. This work is supported by the work of the recruitment task and finish group plans to further streamline the recruitment process reducing time to hire, and to develop a national recruitment/advertising campaign, promoting the advantages of our New Clinical Response Model and of joining #TeamWAST, to ensure sufficient numbers of high quality applicants into the future.

189
Band 6 for paramedics At UK level there is a push by Trade Unions to gain a band 6 grading for qualified paramedic staff. Whilst this may result as an introduction of a degree requirement in the future, we are increasingly seeing different UK ambulance services introducing Band 6 roles and/or career pathways into their existing structures. For some English ambulance services who have Foundation Trust status, this is easier to do as they have increased flexibility to manage and make changes to A4C terms and conditions. In WAST we are committed to working with our trade union colleagues through 2016/17 to explore the possibilities of new roles described in section 6 of our plan, and will be seeking to develop the career pathway and create more opportunities for our paramedic staff to work at a Band 6 level. There is clearly a cost implication to any potential development, and this will need to be modelled and assessed, including consideration and identification of funding sources to support any developments in discussion with our Commissioners and any increased flexibility that may be needed to address constraints offered by existing terms and conditions structures.
Constraints on capacity within the National Ambulance Training Centre (NATC) There is a regular review of training timetables and constraints to delivery within the National Ambulance Training Centre (NATC) as part of the ongoing workforce planning process. This enables us to ensure capacity to deliver training courses can be matched with demand going forward and there is sufficient flexibility within the resource to accelerate timetables where required in the future. However, our current staffing levels do not benchmark favourably against other Ambulance Services, and there is a need to review current staffing ratios and potential alternative models to delivery. This is described further in section 6 of our plan.
Further work to ensure robust vacancy and establishment control at locality level A process of quarterly review and monitoring of establishments takes place through the workforce and finance teams. At present this is still reliant upon manual intervention which increases the risk of error. The data used and ease of process has already been significantly improved upon following commencement of the new Workforce Information Systems Manager. However there is still much work to do to improve the quality of the data within the ESR system and systems of control and reporting of workforce data required for planning and performance management purposes. We expect this work to be completed by September 2016.
Whole System pressures and impact on workforce and workforce target
We are listening to our staff who tell us of the impact that the pressure across the whole USC
system is having upon their work-life balance, morale and heath. As a result, there is a risk that
continued and sustained demand across the system will impact on our ability to recruit and retain
qualified staff, and spikes in demand and increased pressure also impact our ability to meet our
sickness targets.
Our Risk Management Strategy, approved in the Trust Board of March 2016 (a priority from our
2015.16 Plan) will be key in helping us to manage these risks and continuously review their impact.

190
7.4 Engagement and approval arrangements
The Chief Ambulance Services Commissioner was provided with a copy of the first formal IMTP
submission to Welsh Government at the end of January 2016.
Discussions then took place through January and February with both the Chief Ambulance Services
Commissioner (CASC) and the chair of EASC to agree a mechanism by which this plan would gain
both parties support. It was agreed that the final plan would not go before a full EASC committee.
The following roadmap though was agreed so that assurance on the plan would still be achieved:
through February and March regular fortnightly meetings were arranged between the
Director of Planning and Performance, the Assistant Director of Finance and the CASC to
apprise the Commissioner on the development of the plan and to take, and respond to,
feedback;
a further copy of the full plan to be shared with the Commissioner’s office on the 10 March
inviting any further comments; and
subject to the CASCs views a letter of support of the plan to be received from the
Commissioner that can be shared with Trust Board at the open meeting where they will
discuss, and agree, the plan and subsequently Welsh Government as part of final plan
submission.
7.5 Internal Planning model and cycle
Planning the re-fresh of the 2017/18 – 2019/20 IMTP is a critical element of the continued
transformation of WAST and will signal the continued shift towards a front line lead, creative
approach to strategic planning and delivery rather than a “top-down” executive level document.
Recognising that the organisation needs to change its approach to planning; moving from the more
centralised approach in 2015/16 to an approach that fully engages internal and external
stakeholders a planning timetable for 2016/17 has been agreed, this takes learning from the
2016/17 cycle and recognises that WAST still has a maturing approach to planning.
The planning cycle will commence with an Executive Team away day in May and provide the forum
for Executive team to consider:
feedback on the refined purpose, vision, aims & behaviours;
strategic context;
organisational context – financial, workforce; and
the organisation’s eight priorities.
An Integrated Planning team will be re-convened to drive the day to day delivery of a robust and
approvable refreshed IMTP. The team will include representatives from:
Strategy, Planning and Performance;
Quality;
Operations;
Health Informatics;
ICT;
Workforce and OD; and
Finance.

191
The high level milestones for plan development are outlined below and will be underpinned by a
more detailed development plan.
The timetable for developing the 2017/20 IMTP:
Date Forum Purpose
June / July 2016 Executive Team Away Day
Lessons learnt
Review of strategic priorities
Finance
Workforce
Emerging wider NHS Wales / blue light services planning issues
Beginning June/July 2016 Establish IMTP Delivery Group
To lead development of IMTP
August – October 2016 Development of organisation Local Delivery Plans (LDPs) WAST Interdependency workshop
To begin the ‘front line lead’ approach to planning in the organisation which will inform the subsequent re-fresh of the IMTP.
September – October 2016 Initial plan development To begin the re-fresh of the IMTP
October 2016 NHS Wales Peer Review To share, learn, challenge, scrutinise plan development with other Health Boards and Trusts.
October – March 2016/17 Plan refinement to include production of-
1st draft for sharing with Trust Board and Welsh Government.
Final draft for Trust Board and Welsh Government approval.
To progress the development of the IMTP

192
WAST
IMTP 2016/17 – 2018/19
APPENDICIES
Appendix 1: Emerging performance issues arising from the first publication of the AQIs
Appendix 2: CAREMORE® service change ideas currently agreed with EASC
Appendix 3: NHS Wales Strategic Change agenda milestones
Appendix 4: Mid Wales Healthcare Collaborative (MWHC) – Key actions
Appendix 5: Summary of Health Board and Trusts IMTPs integration with
Appendix 6: Supporting information relating to documented actions
Appendix 7: WAST 2016/17 Discretionary Capital Plan
Appendix 8: Strategic Change Programme structures
193
APPENDIX 1 Summary of some of the emerging performance issues arising from the first publication of
the AQIs.
STEP 1 – Help me choose
WAST has a good Partners In Health Team who undertake a good number and range of community
engagement events, but consideration needs to be given to a public education programme
regarding the whole unscheduled care system.
A more systematic approach to STEP 1 must include consideration of how the NHS direct Website
is used for conveying our message – NHSDW has around 300,000 unique hits a month.
The Trust has made good progress in establishing a frequent caller team and actively managing this
cohort of patients, many of who are vulnerable adults. Further work will need to be undertaken in
2016/17 on expanding this approach.
Across NHS Wales our collective aim must be to reduce calls through a clear and effective
education and engagement approach.
STEP 2 – Answer my call
“Hear and Treat” rates (NHSDW and Clinical Desk) are improving, from a low base and are now just
over 5% and expected to hit 5/6% in the first half of 2016/17; however the UK average is circa. 10%,
so there is room for improvement. We should be aiming to increase “Hear and Treat” rates and thus
reduce (unnecessary) attendance at scene.
Future iterations of the AQIs and Benchmarking Toolkit are likely to highlight variation in terms of
time to answer call and call abandonment rates that we will seek to improve.
STEP 3 – Come to see me
In the January AQIs release RED performance for the first three months of the New Clinical
Response Model was 70.6%; however the 95th percentile (for December 2015) was 16.44 minutes,
which is twice the 8 minute target. RED calls are immediately life threatening where every minute
counts, so moving the distribution curve towards a bell shape (and less of a curve) is a key area of
focus, as previously detailed. Similarly, the AMBER 95th percentile (for December 2015) was 48.50
minutes, compared to an internal guidance of 20 minutes.
AQI14: Number of responded incidents that received at least 1 resource allocation, is an important
indicator for the New Clinical Response Model, as the old A8 target encouraged multiple dispatch,
which was inefficient. AQI14 details the percentages for 1 vehicle through to 4 or more vehicles
allocated and will be important to monitor over time.
During 2015/16 the Trust invested in a new structure to support the recruitment, training,
deployment and retention of Community First Responders (CFRs). AQI15 measures the
effectiveness of our CFRs. For the period October 2015 to December 2015, CFRs were the first
response on scene (when deployed) in 79.6% of responses.
STEP 4 – Give me treatment
The AQIs provided information on four clinical indicators, including one new one: the number of
patients suffering cardiac arrest with a return to spontaneous circulation (ROSC). Performance on
these indicators is comparable with other UK ambulance services with the expectation that our
future plans will include improvement trajectories.

194
We would expect AQI17: number of incidents that resulted in non-conveyance to hospital, to
increase overtime as the Trust works on improved clinical leadership and key pathways e.g. mental
health, end of life.
Whilst not published in the January iteration AQI18 will provide information on the dispatch of
ideal/suitable responses, which is a key indicator for the New Clinical Response Model.
STEP 5 – Take me to...
The AQIs in STEP 5 provide information very similar to that detailed in 1.1 Quality and Performance
Trajectories; however, AQI19ii Number of patients conveyed to hospital by type is of particular
interest as it clearly demonstrates the high level of conveyance into Major A&E Units which the “shift
left” is seeking to reduce where it is clinically safe and appropriate to do so:-
Figure 33: Number of Patients Conveyed to Hospital by Type
AQI19ii Number of patients conveyed by hospital
type
Oct 15 Nov 15 Dec 15 Total
Total Number of patients conveyed 23,208 22,551 23,927 69,686
Tier 1 Major A&E Units 21,111 20,645 21,938 63,694
Tier 2 Minor A&E Units 473 455 466 1,394
Tier 3 Medical Admissions Unit 558 532 602 1,692
Other (all other units such as Maternity or
Mental Health)
1,066 919 921 2,906

195
Appendix 2
CAREMORE® service change ideas currently agreed with EASC
Ref. Service Change Idea
Summary
1.
111 Pathfinder
The aim is for the 111 service to become a trusted, easy to use resource for urgent advice and clinical assessment which integrates the current contact services within NHSDW together with GPOOHs call handling and nurse triage services across Wales.
2.
Digi-Pen
Digi-pens to record patient care records. Paper copy is left with the patient and
a digital copy stored in data warehouse (improved data security). The digital
record is then validated and a report can be produced. Enables much greater
focus on reporting and improving clinical outcome, in particular, the reporting
of 10 clinical indicators (with further sub-indicators) compared the previous
four. A key project related to the New Clinical Response Model.
3.
Community First Responders
The effective deployment and utilization of first responders e.g. community first responders or uniformed first responders, through a single management team for Wales.
4.
Mental Health Pathway
To improve the quality and clinical appropriateness of care provided to mental health patients accessing WAST by involving a mental health professional at the earliest opportunity. This is done via a phone call between the Paramedic on scene and a crisis team worker. A decision can then be made as to the most appropriate course of action. The options are; direct admission to a mental health facility. For the patient to stay at home for follow up from G.P or mental health services. For the patient to be taken to the ED
5.
Health Care Professionals (HCP)
- Dedicated desk
- Urgent Care Staff (UCS) provision
A dedicated HCP calls service desk within the CCC function designed to manage the UCS provision and plan admissions with hospitals from HCP non-emergency calls, who are requesting transport for patients within an agreed timeframe of 1 to 4 hours (HCP GREEN 3 calls). Additional dedicated UCS resource to exclusively manage this demand.
6.
Clinical Pathway Appraisal and Approval Group
Ensuring any clinical innovation or alternative pathway of care is based on patient need, has a current or emerging evidence base and has an associated clinical audit and evaluation plan to assess its effects on patients and the overall service delivery in term of patient flow and clinical outcomes.
7.
Paramedic Pathfinder
Training costs associated with the development and roll out of a reductive
triage model for paramedics to better enable them to conduct face to face
triage of patients when they arrive at scene, using a flow chart of presenting
signs and symptoms, to determine the most appropriate clinical pathway for
the patient’s needs e.g. community care, self-care or patient specific pathways
to, which should also help reduce conveyance rates to A&E
8.
Frequent Callers
A pan-Wales manager to ensure a standardised approach to improving clinical outcomes and reducing ambulance activations to 999 calls for frequent callers, working partnership with other health providers, the Police and social care.
9.
Resuscitation
Initiative set up as part of the cardiac arrest survival plan. 3RU team set up to

196
Rapid Response Unit
support and lead resuscitation efforts at cardiac arrest/peri arrest calls. A
dedicated team specialising in managing cardiac arrest patients with skills
including clinical decision-making and crew resource management.
10.
GP/Paramedic Out of Hours
The initiative was to provide the concept (accepted) and potential benefits of Advanced Paramedic Practitioners and Training Advanced Paramedic Practitioners supporting GPOOHs with home visits. Based on best practice and much quoted report from Everden et al in 2003 that Band 5 Paramedics “can handle most of the likely GPOOHs home visits.”
11.
Clinical Response Model
The New Clinical Response Model 1 year pilot was driven by clinicians and the
new 2015 Policy is clinically led. It recognises that getting to patients with life
threatening symptoms requires an 8 minute emergency response (or less) and
the organisation will continue to be performance measured against this. It also
recognises that for the majority of callers, an 8 minute emergency response
will not impact on the patient’s outcome. This model allows call takers up to
two minutes extra time to identify the patient’s need and to send, or refer to, a
clinically appropriate care provider e.g. an APP, refer to Hear & Treat/Direct,
refer to GP, take the patient to the right hospital or facility. This model also
monitors and measures the clinical care provided to the patient on scene.
12.
Transformation of CCC
CCCs are the lynchpin to the EMS service. The effectiveness of them is a key
determinant of the effectiveness of the rest of our service. They are integral to
STEPS 2 and 3, Answer my Call and Come to See Me. The modernisation of
CCCs (including the new Computer Aided Dispatch system) has been
identified as a priority for the 2016/17 IMTP; however, there are a number of
immediate actions that have been undertaken to mitigate identified risks
around the CCC, staffing structure and ICT pending the new CAD and
restructure.
13.
Overtime/Private Providers
The initiative aims to boost WAST’s capacity to respond to demand through increased unit hours production delivered through either incentivized overtime 7days a week or the use of private providers.
14.
Cwm Taf Explorer
To improve the ambulance response times for immediately life threatening
calls for patients in Cwm Taf. The initiative includes: 1) the delivery of a
shared programme of public education to ensure residents of Cwm Taf
understand the full range of services available 2) a communication strategy to
support the work of Explorer 3) the commencement of the development of a
clinical culture that encourages and supports clinicians to operate fully within
their scope of practice 4) the geographic ring fencing of emergency ambulance
resources within the boundaries of Cwm Taf 5) The implementation of a
system to appropriately convey patients where the request originates from our
HealthCare Professional colleagues (HCP) within the appropriate timescale

197
Appendix 3
NHS Wales Strategic Change agenda milestones
This table gives a high level overview of the major service changes planned for NHS Wales and,
where clear, the critical milestones. Only those changes that will impact on WAST services have
been included. For some, for example the Mid Wales Health Collaborative, only as the programme
progresses will milestones for change become clearer. This work will be routed through the
Business intelligence Hub
NHS WALES STRATEGIC SERVICE CHANGE (where impact on WAST)
MILESTONE
CWM TAF (SOUTH WALES PLAN)
Transfer of obstetrics, paediatrics from Royal Glam Hospital
Transfer of ED activity from Royal Glam
Development of Royal Glam as diagnostic hub
ENT service reconfiguration (emergencies to UHW)
Summer 2017
To be determined
?
Qtr 1 2016/17
ANEURIN BEVAN
Specialist and Critical Care Centre (SCCC)
SCCC Full Business Case submitted to WG
SCCC operational
Potential changes to GI bleeds
Potential changes to ENT
Dec 2015
Spring 2019
To be determined
To be determined
CARDIFF AND VALE
ENT service reconfiguration (emergencies to UHW – from RGlam and POW)
Qtr 1 2016/17
ABERTAWE BRO MORGANNWG
ENT service reconfiguration (emergencies to UHW – from RGlam and POW)
A Regional Collaboration for Health (ARCH) Programme
Qtr 1 2016/17
Key milestones TBD
POWYS
Future Fit – Redesign of services across Shrewsbury and Telford
To be determined
MID WALES COLLABORATIVE
As service planning and engagement work development – milestones will emerge
MAJOR TRAUMA NETWORK (South)
Establishment of Major Trauma Network (MTC plus MTUs plus rehab model)
To be determined

198
Appendix 4
Mid Wales Healthcare Collaborative (MWHC) – Key actions
Priority Action Expected outcome Service, workforce and
financial implications Target date
1. MWHC team
Secure required resources for 2016/17 to continue the work of the MWHC.
Secure the required funding and resources. Implementation the recommendations of the Mid Wales Healthcare Study.
Funding requirement is £200k with £50k contribution from WG on the basis that of match funding of £50k from the three HBs. Plus Resources required from collaborative healthcare organisations to support the Innovation sub-groups.
Mar 16
2. Centre for Excellence in Rural Healthcare
Establish a Centre for Excellence in Rural Healthcare, with a particular focus on research, development and dissemination of evidence in health service research which addresses the particular challenges of Mid Wales.
Scope the innovative approaches needed to address education, research and development for healthcare in Mid Wales. Scope appropriate models for the Centre of Excellence in Rural Healthcare. Develop a Business Case for the establishment a Centre for Excellence in Rural Healthcare.
The establishment of critical mass of applied research excellence, conducting new work on the healthcare challenges of Mid Wales, and working closely with local clinicians, managers and others to apply the lessons from experience elsewhere. Generate a new level of credibility in Mid Wales to help to recruit strong candidates for local clinical posts.
Funding requirement is £133,500 per annum for the first 2 years (total £267,000) to be funded equitably by the three collaborative Health Boards and WAST.
Mar 16
2. Primary Care and Community Services
Establish the role of Physician Associates (PA) across Mid Wales.
Introduce a 4-year PA development programme which supports the student PA through training and offers a 2-year fixed term internship following graduation
Up to 6 qualified and experienced PAs working across Mid Wales.
Funding through WG allocation for developing the primary care workforce, with costs to be shared equally between the three HBs. Total costs as follows: Year 1 = £60,000 Year 2 = £60,000 Year 3 = £282,000 Year 4 = £293,000 Total = £695,000
2016 - 2020

199
Priority Action Expected outcome Service, workforce and financial implications
Target date
Up-skill the rural primary care workforce.
Produce a skills and competencies framework for the practice nurses and health care assistants (and other non-GPs involved at primary care level in the delivery of long-term conditions management. Following the delivery of a skills and competencies framework deliver a programme of training and development opportunities for appropriate primary care staff to help each achieve their maximum potential within the framework
Completed skills and competencies framework delivered. Programme of training and development available and offered to all appropriate primary care staff in the MWHC area
Funding requirement to be identified by Primary Care and Community services sub-group. Funding requirement to be identified by Primary Care and Community services sub-group.
2016 2018
Establish an enhanced community-focused service that supports the timely discharge/ transfer of ‘medically fit’ patients from Bronglais Hospital.
Identify current ‘blockages’ and strategies for over-coming them.
All medically fit patients are discharged or transferred from Bronglais Hospital in a timely manner and to safe and appropriate alternative forms of care.
Funding requirement to will be the cost of recruiting a Discharge Liaison post.
2018
Establish an integrated community focused dental service in Mid Wales.
Develop an integrated service that involves the development of an intermediate oral surgery service for complex extractions. Develop an integrated service that involves the development of a joint GA list (involving CDS staff) in Bronglais Hospital using existing facilities not fully utilised due to lack of suitably trained staff. Develop an integrated service that involves the future development of a maxillofacial service which avoids the unnecessary use of secondary care services and patient travel to South Wales.
Regular, readily accessible GA dental sessions operating at Bronglais Hospital. Regular, readily accessible GA dental sessions operating at Bronglais Hospital. Ready access to a clinically appropriate locally based maxillofacial service that avoids unnecessary travel to more distant hospitals outside the Mid Wales area.
Funding requirement to be identified by Primary Care and Community services sub-group. Funding requirement to be identified by Primary Care and Community services sub-group. Funding requirement to be identified by Primary Care and Community services sub-group.
2016 2016 2017
Rolling out the concept of the ‘virtual ward’ to all parts of the MWHC area.
Agree the core principles of the ‘virtual ward’ and then allowing for local variation, reflecting local circumstances, ensure the core principles are in place across all parts of the MWHC area.
Core principles of the ‘virtual ward’ are in place and being worked to in all parts of the MWHC area
Funding requirement to be identified by Primary Care and Community services sub-group.
2016

200
Priority Action Expected outcome Service, workforce and financial implications
Target date
3. Mental Health and Learning Disabilities
Ensuring out of hours crisis support is available when needed.
Alternatives to admission, with in-patient access when needed.
Developing integrated services for people with Dementia.
Extending access to psychological therapies.
Child and adolescent mental health services.
4. Telehealth and Innovation
Re-establish a Tele-Dermatology service for Mid Wales.
Develop a Business Case for the re-establishment of the Tele-Dermatology service for Mid Wales.
Re-establishment of the Tele-Dermatology service for Mid Wales thereby reducing the need for patients to travel to more distant hospitals/clinics outside the Mid Wales area.
Six month pilot to commence April 2016. Cost of approx £25,000 to be funded by HDUHB.
Apr 16
Review telehealth, telemedicine and telecare across Wales to identify activities that present opportunities for adoption or expansion across Mid Wales.
Undertake an All Wales Scoping exercise to establish a baseline of all Tele-health equipment that is currently available or in use within Tele-health, Tele-care and Tele-medicine.
An understanding of the provision of Tele-health equipment that is currently available or in use within Tele-health, Tele-care and Tele-medicine across Wales.
WG have awarded grant funding of £25k to undertake this exercise.
Jan 16
Implement the recommendations of the review of telehealth, telemedicine and telecare across Mid Wales.
Use the final report from the Scoping exercise to draft a specification to determine where equipment is needed. Use the final report from the Scoping exercise to determine where extra support is required (staff, estates and IT infrastructure) to deliver services via tele-health. Use the final report from the Scoping exercise to draft a specification to determine where training is needed.
Accessible and appropriate telehealth services available across Mid Wales. Appropriate infrastructure in place to support the operation of telehealth equipment across Mid Wales. All relevant staff provided with a programme of training in the use of equipment.
WG have awarded grant funding of £225k for equipment and training.
Dec 16
5. Palliative Care and End of Life
Identify and assess the range and scope of end of life and palliative
Carry out a scoping exercise to map the range of services provided.
An understanding of the provision of palliative and end of life care across health, local
WH have awarded the End of Life Board grant funding of
May 16

201
Priority Action Expected outcome Service, workforce and financial implications
Target date
care services in rural mid-Wales.
Identify:
service demand by the take up of services, occupancy levels, effectiveness / outcomes, working hours and waiting times;
geographical location / accessibility of services;
gaps in service provision;
duplication of services;
‘what works well’
authority and third sector provision in rural Mid Wales. Improved ability to develop co-ordinated pathways. Improved ability to ensure any proposed service improvements / new developments reflect identified gaps in current provision and improve the experience and outcomes for patients and their families.
£44k to undertake this exercise.
Understand the public perception for end of life and palliative care services of patients, families and their carers living in rural mid-Wales
Identify ‘key messages’ relating to end of life / palliative care from the public engagement meetings facilitated by the Mid-Wales Healthcare Collaborative.
‘Targeted’ stakeholder engagement with support from members of the Innovation Sub Group / Working Group
Liaison with service providers
Targeted stakeholder engagement included as an integral aspect of the project. Recommendations for service improvements and / or service change informed by stakeholder views and opinions.
Costs of public, staff and stakeholder engagement covered by MWHC budget.
Mar 17
Understand the demographic and health profile of rural mid-Wales
Identify and analyse relevant data sources in order to establish an estimate of the level and location of need.
Recommendations for service improvements and / or service change informed by an enhanced understanding of the characteristics of the local population.
Provide an overview of key messages from research, national guidance and good practice relating to end of life and palliative care services in rural areas.
Research examples of best practice / service models for end of life and palliative care services in rural areas - including legislation, national guidance and local commitments.
Evidence based examples of best practice service models for EoL / palliative care services (cancer and non-cancer). Evidence based examples of new technology (tele-health, tele-rehab, telemedicine) in enhancing EoL / palliative care services in rural settings. Successful EoL / palliative care services in rural areas from the perspective of patients, families and their carers. Successful EoL / palliative care services in rural areas from the perspective of the workforce.
Feb 16

202
Priority Action Expected outcome Service, workforce and financial implications
Target date
Underpinning evidence, policy and national guidance.
Identify service improvements / service change where appropriate with particular emphasis on new technology.
Make recommendations for service improvements / service change with particular emphasis on new technology and Hospice at Home.
Proposals for service improvements / service change with particular emphasis on new technology and Hospice at Home.
Jun 16
6. Bronglais General Hospital
Actively engage clinical staff in all discussions about how services should be developed.
Create/strengthen professional networks to provide a robust support unit and to share good practice.
A robust professional support network to share innovations and good practice.
On-going
Active recruitment to medical and nursing vacancies.
On-going recruitment to vacant posts. Specific Bronglais General Hospital recruitment campaign.
All specialties have a full complement of staff (all clinical staff) in order to provide efficient and effective service to its population. Sufficient nurse complement to reduce the need for agency staff
Funding requirements included in HDUHB IMTP.
On-going Jan 16
Increase bed capacity to restore surgical throughput, reduce waiting lists and avoid accident and emergency delays for medical patients.
Introduce an additional 12 beds at Bronglais General Hospital.
Improve patient flow in and out of Bronglais Hospital.
Funding requirements included in HDUHB IMTP.
Jan 16
Work innovatively to increase surgical capacity.
Develop and agree a surgical service model. To create a safe, sustainable surgical service at Bronglais Hospital for the people of Mid Wales.
Funding requirement to be identified by Bronglais General Hospital sub-group
May 16
Establish a new closed MRI scanner servicing all specialties.
Develop a Business Plan for the proposed acquisition of a new MRI scanner with Anaesthetic Kit that will service all specialities.
A new, fit for purpose MRI scanner, serving all specialties including colorectal and paediatric services thereby reducing the need for patients to travel out of the area.
Funding requirements included in HDUHB IMTP.
Dec 16
7. Access and Transport
Better alignment between clinic times/Day Surgery and public transport.
Undertake pilot on subsection of outpatients in Bronglais to test approach to improved alignment
Reduce “wasted” time for patients Improve patient experience
To be tested as part of pilot July 16
Implementation of mixed service provision to meet new service specification for Non-Emergency Patients Transport Service (NEPTS).
Implementation of the all Wales NEPTS Business Case
Better quality of NETPS service Improved arrangement for renal patients Extended hours of operating
Full detail in the NEPTS business case
April – Dec 2016
Implement the New Clinical Pilot launched 1 Oct 2015. 65% RED performance across all MWHC Delivered through current Pilot to

203
Priority Action Expected outcome Service, workforce and financial implications
Target date
Response Model. Focused action plan for Hywel Dda area Demand and capacity review Evaluation of New Clinical Response Model
areas Improving performance against clinical indicators Reducing variation of performance Improved patient experience
resources Sept 16
Strengthen models of community resilience, including Community First responders, co-responding and alternative models (e.g. Community Paramedics)
CFR action plan Co-responder pilots Explore pilot for community paramedics with MWHC Cluster
65% RED performance across all MWHC areas Improving performance against clinical indicators Reducing variation of performance Improved patient experience
CFR funded through EASC Implications of community paramedic to be developed
Ongoing
8. Communications and Engagement
Ensure effective communications, engagement and involvement.
Develop, implement and evaluate a Mid Wales Healthcare Collaborative Engagement Plan.
Effective engagement with:
Public;
Staff;
Health and social care staff and senior clinicians;
Local Authorities, including officers and elected members;
Third Sector;
Community Health Councils Support for dialogue with the community through a programme of media relations based on the development of good relationships with local media.
Costs of public, staff and stakeholder engagement covered by MWHC budget.
Dec 17

204
Appendix 5
Summary of Health Board and Trust IMTPs integration with WAST
Organisation Joint Priorities Health Board/Trust actively engaged on priority
e.g. WAST’s priorities which require collaborative work with Local Health Boards and
other NHS Wales Trusts Detail degree of engagement, e.g. Health Board aware of
scheme, conversations taken place, etc.
ABMU 1) 111 pathfinder, including Pre-pathfinder initiatives 2) Working together to improve hospital handover (in line with guidance) 3) NEPTS BC implementation Pathways implementation: Mental Health / Early Adopters / Acute GP (Swansea)
/ Falls vehicle (Swansea) / help point plus (Swansea) / end of life (all wales work)
1) 111 ongoing engagement with the HB 2) Handover ongoing engagement 3) NEPTS minimal engagement 4) Pathways ongoing engagement except for End
of Life
Hywel Dda
1) Collaborative AP development pilot with primary care partners and GPOOH services
2) Mid Wales Health Collaborative 3) Joint Performance action plan 4) 111 Pathfinder - Carmarthen 5) NEPTS BC implementation 6) Pathways implementation: Stroke / end of life (all wales work) 7) Retention of dedicated ambulance vehicle (DAV) Withybush
1) Joint interviews with two APs appointed - target date of go live early April 16
2) WAST supporting the collaborative at both public events and through the work streams
3) Action plan agreed, implemented and kept under regular review and refinement.
4) Locality Manager part of implementation group 5) Engagement 6) Stroke pathway agreed 7) Ongoing discussions with HB to make this
service part of core business.
Aneurin Bevan 1) Working together to improve hospital handover (in line with guidance) 2) Development of new model for unplanned care - Code Zero RED AMBER
Release of EA’s to support patients in community when delays impact 3) SCCC Joint partnership project (hyper acute stroke, ENT, etc.) 4) NEPTS BC implementation 5) Pathways implementation: Mental Health / neck of femur / Falls / end of life
(all wales work) / Community Nursing 24 hour project
1) Joint WAST and AB weekly meeting and partnership work with HALO
2) SOP shared with AB and control, request implemented as required with DGH’s.
3) Continued WAST engagement with AB 4) Active engagement – proposed pilot live for AB
early April. 5) Joint Falls service working well with weekly

205
conference with Almanac, Community nurse 24/7 live 29th Feb.
BCU
1) Alcohol treatment centre in Wrexham 2) NEPTS BC implementation 3) Pathways implementation: Mental Health / district nurse / MIU / Falls / end
of life (all wales work) / interface with GPOOH and clinical support CCC (local to BCU area)
4) BCU acute service re-configuration 5) Working together to improve hospital handover and patient experience
through improved performance (in line with guidance)
1) Project completed in partnership with HB and others
2) Engagement 3) Pathways ongoing engagement 4) Actively engaged on project teams/board 5) Actively engaged
Cardiff & Vale
1) Alcohol treatment centre 2) Development of new model for unplanned care - Code Zero RED AMBER
Release of EA’s to support patients in community when delays impact 3) Working together to improve hospital handover (in line with guidance) 4) NEPTS BC implementation also PCS transition from Whitchurch to Lansdowne 5) Pathways implementation: Falls / end of life (all wales work) / emergency obs
and Gynae / Ambulatory care / Barry MIU Pathway / Cardiac stemi 6) Strategic estates Planning pending substantial road network potential
changes at UHW
1) Joint working with external budget removed 2) Joint meetings in process 3) Joint Process Mapping 4) Regular joint meetings ongoing 5) Some pathways already in place or being
developed 6) Joint engagement with ARC development
Cwm Taf
1) Implementation of South Wales plan inc. diagnostic centre, paeds, obs &neo 2) Optimising use of paramedic pathfinder 3) Evaluation of Cwm Taf Explorer 4) NEPTS BC implementation 5) Pathways implementation: Mental Health / MIU / fractured neck of femur /
Falls / end of life (all wales work) / community integrated assessment service 6) Acute medicine model whereby pathways have been developed and agreed
with WAST for patients going to Royal Glamorgan Hospital.
1) WAST attends all meetings 2) MD and P Care lead involved 3) Equal partners 4) Engagement 5) Ongoing work – regular meets to develop and
improve/tweak 6) Ongoing monthly clinical meetings
Powys
1) Meaningful and joint engagement in Future Fit Programme 2) Mid Wales Collaborative – focus on exploring modes for community, new
model for Bronglais 3) NEPTS BC implementation
1) Option appraisal being reconsidered, assistant head of Ops in discussion.
2) Supporting public meetings and work streams 3) Minimal involvement
206
4) MIU acceptance criteria 4) Locality team meeting with Health Board leads March 16 to take this forward.
Public Health
Wales
1) Development of Help me choose strategy
1) Engagement
Velindre NHS
Trust
1) Engaging with the Velindre cancer programme – link with NEPTS 2) NEPTS BC implementation
1) Engagement 2) Engagement

207
Appendix 6
Supporting information relating to documented actions
See separate excel spreadsheet.

208
Appendix 7: WAST 2016/17 Discretionary Capital Plan as at February 2016
Bid Code Title Directorate
Total Capital
Cost (yr1) (inc VAT)
Cumulative Cost
Remaining Discretionary
Capital (£5.826m)
Total Score
Rank Notes
BID1035 Bargoed Enhancement Signal
Ops 18,000 18,000 5,808,000 25 1
The signal strength for hand portable radios is extremely poor at Bargoed, and indeed within some rooms in the station there is no signal at all. Clearly this poses a significant risk to the organisation and patients where crews cannot be contacted to respond to the next emergency call.
BID1004
Replacement of Hazardous Area Response Team (HART) Breathing Apparatus Equipment
Ops 49,161 67,161 5,758,839 24 2
1. Revenue cost already in place for existing equipment 2. price only indicative as tender process next year
BID1002 Training School Tablet Computers
Training 57,311 124,472 5,701,528 21 3 Spend to save modernisation initiative
BID1013 Llanfyllin station – Boiler replacement works
Estates 10,000 134,472 5,691,528 21 3 Essential remedial work
BID1022 Pwllheli AS – Boiler replacement works
Estates 15,000 149,472 5,676,528 21 3 Essential remedial work
BID1023 Rhyl AS – Boiler/Control/Pipework replacement works
Estates 84,810 234,282 5,591,718 21 3
Essential remedial work

209
Bid Code Title Directorate
Total Capital
Cost (yr1) (inc VAT)
Cumulative Cost
Remaining Discretionary
Capital (£5.826m
Total Score
Rank Notes
BID1017 Colwyn Bay AS – replacement roof
Estates 187,000 421,282 5,404,718 20 4 Essential remedial building work, costs may be less (£147,000) if planning permission agreed
BID1019 Holyhead AS – roof covering renewal
Estates 145,920 567,202 5,258,798 20 4 Essential remedial building work
BID1016 Pembroke Dock – roof repairs
Estates 20,000 587,202 5,238,798 19 5 Essential remedial building work
BID1028 Pontypool station – roof covering
Estates 20,000 607,202 5,218,798 19 5 Essential remedial building work
BID1029 Tredegar Ambulance Station – Internal and External refurbishment
Estates 260,000 867,202 4,958,798 19 5
Essential remedial building work, asbestos in structure, building owned and retained as reporting station, price includes temp accommodation
BID1011
Aberystwyth station – structural repairs to concrete frame and masonry
Estates 18,000 885,202 4,940,798 18 6 Essential remedial building work
BID1012 Haverfordwest station – roof covering renewal
Estates 65,000 950,202 4,875,798 18 6 Essential remedial building work, required because of terms of lease
BID1020 Various station – Drainage remedial works
Estates 50,160 1,000,362 4,825,638 16 7 Statutory Requirement
BID1024 Aberdare station – roof light renewal
Estates 25,000 1,025,362 4,800,638 16 7 Essential remedial building work
Bid Code Title Directorate
Total Capital
Cost (yr1) (inc VAT)
Cumulative Cost
Remaining Discretionary
Capital (£5.826m
Total Score
Rank Notes

210
BID1027
Monmouth Ambulance Station – Provisions of alternative accommodation to enable disposal of dilapidated former station
Estates 82,000 1,107,362 4,718,638 16 7
Actual net cost after savings £7K Capital and annual Revenue £4K but only until station sold. DJ to provide a Business Case for the whole project, confirming the approval process and final outcome.
BID1003 SmartBoard ICT requirements for Equitable Staff Education
Training 5,199 1,112,561 4,713,439 15 8
Costs halved (from £10,399). Only need one smartboard – moved one board to Carmarthen. Technology, enabled learning – most out of dolls etc link to these boards £5k
BID1008 Sit-Stand Desk Provision – Get WAST Standing
Workforce and OD
71,471 1,184,032 4,641,968 15 8 To be combined with BID1001 for CCC furniture. It was suggested that this bid would be piloted.
BID1021 Porthmadog-Llandudno-Holyhead Kitchen replacements
Estates 31,680 1,215,712 4,610,288 15 8 H&S/improvement
BID1038 Major Incident Response Equipment
Ops
£53,918
1,269,630
4,556,370 25 1 Specialist Major Incident Equipment

211
Appendix 8: Strategic change programme structures
Clinical Modernisation Programme

212
Clinical Contact Centre Modernisation Programme

213
Non-Emergency Patient Transport

















