21
© 2011 McGraw-Hill Higher Education. All rights reserved. Chapter 13: Off-the- Field Injury Evaluation
| Date post: | 26-Dec-2015 |
| Category: |
Documents |
| Upload: | tyler-howard |
| View: | 215 times |
| Download: | 2 times |
© 2011 McGraw-Hill Higher Education. All rights reserved.
Chapter 13: Off-the-Field Injury Evaluation
© 2011 McGraw-Hill Higher Education. All rights reserved.
Evaluation of Injuries
• Essential skill for athletic trainers
• Four distinct evaluations– Pre-participation (prior to start of season)– On-the-field assessment– Off-the-field evaluation (performed in the
clinic/training room…etc)– Progress evaluation

© 2011 McGraw-Hill Higher Education. All rights reserved.
Clinical Evaluation & Diagnosis
• Diagnosis– Use of clinical or scientific methods to establish
cause and nature of patient’s illness or injury and subsequent functional impairment due to pathology
– Forms basis for patient care
• Physicians make medical diagnosis– Ultimate determination of patient’s physical
condition
© 2011 McGraw-Hill Higher Education. All rights reserved.
• Athletic trainers and other health care professionals use evaluation skills to make clinical diagnoses– Clinical diagnosis identifies pathology and
limitations/disabilities associated with pathology
• Athletic trainers have academically-based credential and in many states some form of regulation which recognizes ability and empowers clinician to make accurate clinical diagnosis
© 2011 McGraw-Hill Higher Education. All rights reserved.
Basic Knowledge Requirements
• Athletic trainer must have general knowledge of anatomy and biomechanics as well as hazards associated with particular sport
• Anatomy– Surface anatomy
• Topographical anatomy is essential
• Key surface landmarks provide examiner with indications of normal or injured structures
– Body planes and anatomical directions• Points of reference (midsagittal, transverse, and frontal (coronal)
planes)

© 2011 McGraw-Hill Higher Education. All rights reserved.
– Abdominopelvic Quadrants• Four corresponding regions of the abdomen• Divided for evaluative and diagnostic purposes• A second division system involves the
abdomen being divided into 9 regions

© 2011 McGraw-Hill Higher Education. All rights reserved.
– Musculoskeletal Anatomy• Structural and functional anatomy• Encompasses bony and skeletal musculature• Neural anatomy useful relative to motion,
sensation, and pain– Standard Terminology
• Used to describe precise location of structures and orientation
• Biomechanics (foundation for assessment)– Application of mechanical forces which may
stem from within or outside the body to living organisms
– Pathomechanics - mechanical forces applied to the body due to structural deviation - leading to faulty alignment (resulting in overuse injuries)
© 2011 McGraw-Hill Higher Education. All rights reserved.
• Understanding the Activity– More knowledge of activity allows for more
inherent knowledge of injuries associated with activity resulting in more accurate clinical diagnosis and rehab design with appropriate functional aspects incorporated for return to activity
– Must be aware of proper biomechanical and kinesiological principles to be applied in activity
– Violation of principles can lead to repetitive overuse trauma
– Increased understanding = better assessment and care

© 2011 McGraw-Hill Higher Education. All rights reserved.
• Descriptive Assessment Terms– Etiology - cause of injury or disease– Mechanism – mechanical description of
cause– Pathology - structural and functional
changes associated with injury process– Symptoms- perceptible changes in body or
function that indicate injury or illness (subjective)
– Sign - objective, definitive and obvious indicator for specific condition
– Degree- grading for injury/condition– Diagnosis- denotes name of specific
condition

© 2011 McGraw-Hill Higher Education. All rights reserved.
– Prognosis- prediction of the course of the condition
– Sequela - condition following and resulting from disease or injury (pneumonia resulting from flu)
– Syndrome - group of symptoms and signs that together indicate a particular injury or disease
– Differential diagnosis – systematic method of diagnosing a disorder
• Refers to a list of possible causes• Prioritizing of possibilities• Also referred to as hypothesis or working diagnosis• Utilize skills to make decision regarding condition
© 2011 McGraw-Hill Higher Education. All rights reserved.
Off-the-field Injury Evaluation
• Detailed evaluation on sideline or in clinic setting
• May be the evaluation of an acute injury or one several days later following acute injury
• Divided into 4 components– History, observation, palpation and special
tests– HOPS

© 2011 McGraw-Hill Higher Education. All rights reserved.
• History– Obtain subjective information relative to
how injury occurred, extent of injury, MOI– Inquire about previous injuries/illnesses
that may be involved as well as past treatments
– Ask the following questions• What is the problem?• How and when did it occur?• Did you hear or feel something?• Which direction did the joint move?• Characterize the pain
© 2011 McGraw-Hill Higher Education. All rights reserved.
• Observations– Asymmetries, postural mal-alignments or
deformities?– How does the athlete move? Is there a
limp?– Are movements abnormal?– What is the body position?– Facial expressions?– Abnormal sounds?– Swelling, heat, redness, inflammation,
swelling or discoloration?

© 2011 McGraw-Hill Higher Education. All rights reserved.
• Palpation– Bony & soft tissue
• Special Tests– Used to detect specific pathologies– Compare inert and contractile tissues and their
integrity– Assessment should be made bilaterally
• Range of Motion Assessment– Active– Passive
• Normal vs. Abnormal end points• Manual muscle tests• Goniometric measures vs. Digital inclinometers

© 2011 McGraw-Hill Higher Education. All rights reserved.
Figure 13-4 A & B
© 2011 McGraw-Hill Higher Education. All rights reserved.
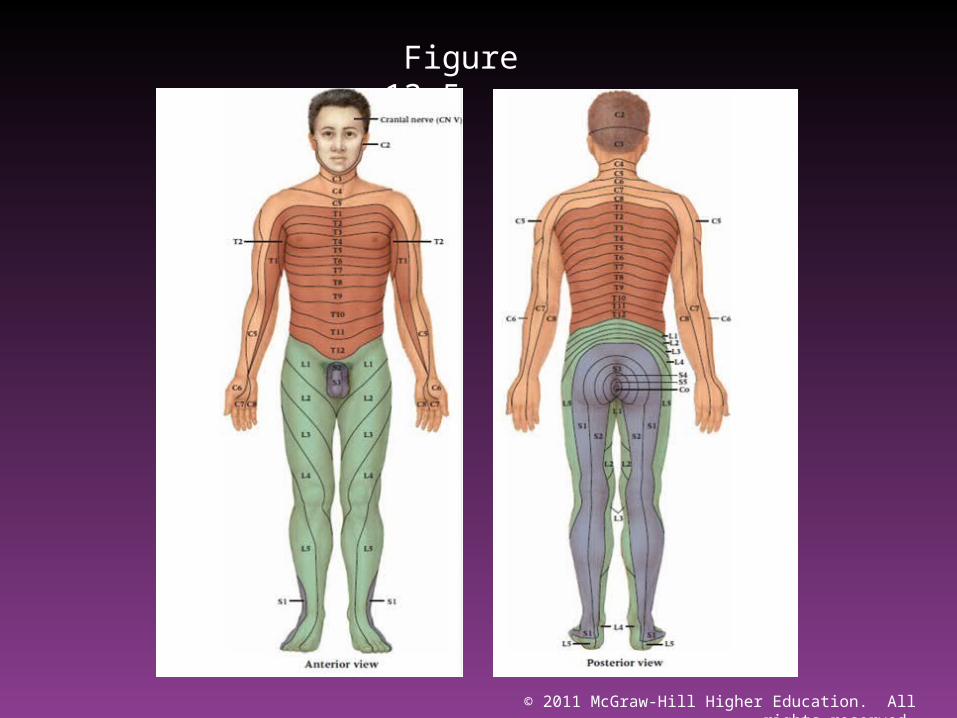
• Neurologic and circulation assessments– Brain
• Cerebral, cranial nerve function, cerebellar function– Sensory & motor function
• Dermatome– Area of skin innervated by a single nerve
• Myotome– Muscle or group of muscles innervated by a specific
motor nerve
– Reflex testing• Involuntary response to a stimulus
– Deep tendon – caused by stimulation of stretch reflex– Superficial – stimulation of skin which causes reflexive
muscle contraction– Pathological – superficial reflex indicative of upper motor
neuron lesion» Babinski’s sign, Chaddock’s, Oppenheim’s Gordon’s
– Referred pain
© 2011 McGraw-Hill Higher Education. All rights reserved.
Figure 13-5
© 2011 McGraw-Hill Higher Education. All rights reserved.
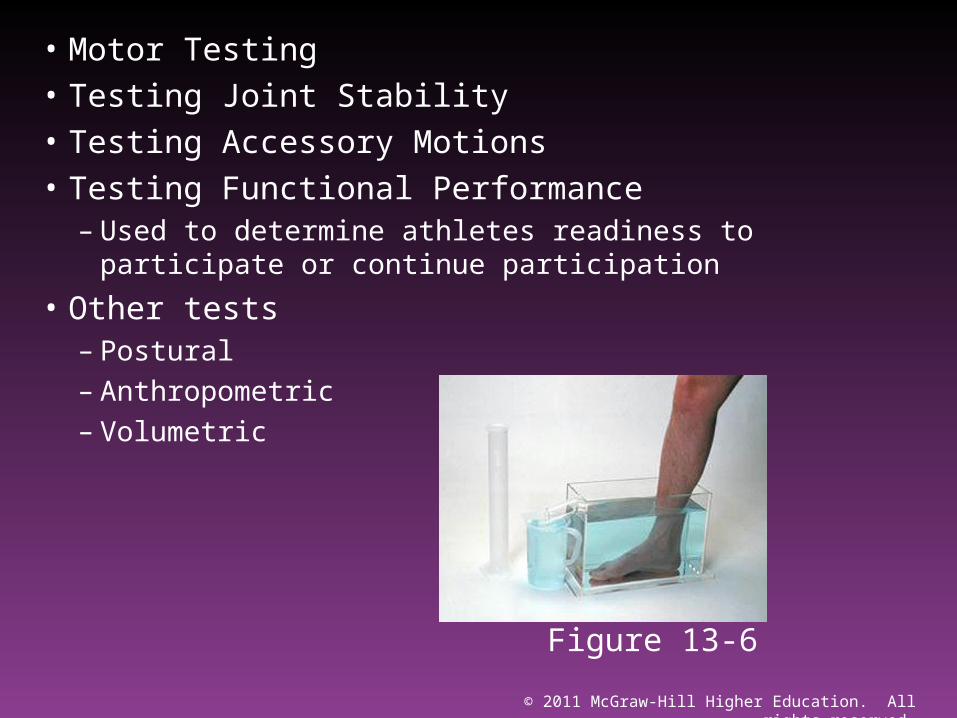
• Motor Testing• Testing Joint Stability• Testing Accessory Motions• Testing Functional Performance
– Used to determine athletes readiness to participate or continue participation
• Other tests– Postural– Anthropometric– Volumetric
Figure 13-6
© 2011 McGraw-Hill Higher Education. All rights reserved.
Documenting Injury Evaluation Information
• Complete and accurate documentation is critical
• Clear, concise, accurate records is necessary for third party billing
• While cumbersome and time consuming, athletic trainer must be proficient and be able to generate accurate records based on the evaluation performed
© 2011 McGraw-Hill Higher Education. All rights reserved.
• SOAP Notes– Record keeping can be performed systematically
which outlines subjective & objective findings as well as immediate and future plans
– SOAP notes allow for subjective & objective information, the assessment and a plan to be implemented
– S (subjective)• Statements made by patient - primarily history information
and patient’s perceptions including severity, pain, MOI
© 2011 McGraw-Hill Higher Education. All rights reserved.
– O (Objective)• Findings based on athletic trainer’s evaluation
– A (Assessment)• Athletic trainer's professional opinion regarding
impression of injury• May include suspected site of injury and structures
involved along with rating of severity
– P (Plan)• Includes first aid treatment, referral information, goals
(short and long term) and examiner’s plan for treatment

















