62
Director of Clinical and Business Development Wedgwood Christian Services Anthony Muller MA, LPC, CAADC
| Date post: | 28-Dec-2015 |
| Category: |
Documents |
| Upload: | jemimah-marshall |
| View: | 217 times |
| Download: | 0 times |
Director of Clinical and Business Development
Wedgwood Christian Services
Anthony Muller MA, LPC, CAADC
Change What Creates It
Response to treatment in the first few sessions is highly predictive of the eventual outcome.
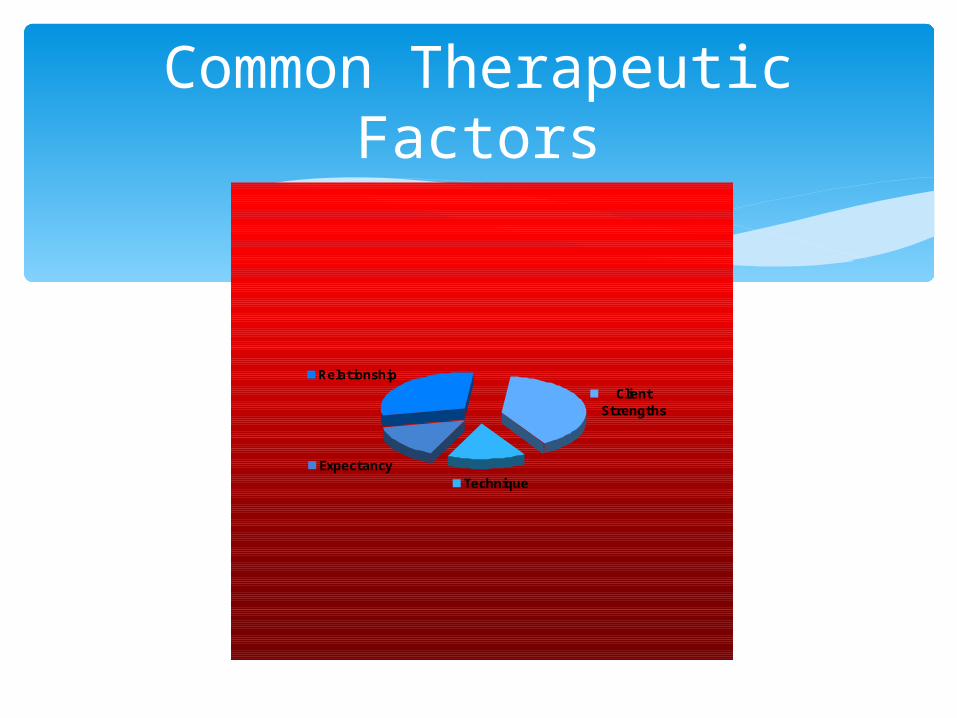
Common Therapeutic Factors
TechniqueExpectancy
Relationship
Client Strengths
Motivational Readiness Therapeutic Alliance
Relationship Factors
Affective Relationship Clients’ Capacity to Work in Counseling
Purposefully Therapist’s Empathetic Understanding and
Involvement Client-Therapist Agreement in the Goals and
Tasks True Change Partnership
Therapeutic Alliance
“Within the client is a theory of change waiting for discovery, a framework for intervention to be unfolded and accommodated for a successful outcome”.
Hubble, Duncan, Miller, 1999
Hope and Expectancy
Possibility Focus
Therapist Expectancy
Know Your Role
Stages of Substance Use
Developmental Psychology
The study of how things change and stay the same over time.
Macro Theories of Major Struggles, Events, Cognitions and Developments applicable to almost all adolescents.
Adolescence: Biosocial Development
•Puberty
Length of time for average adult to become physically dependent on alcohol 7-14 years
Length of time for average adolescent to become physically dependent on drugs or alcohol
9-18 months
Adolescence: Cognitive Development
Adolescent Egocentrism Characteristic of adolescent thinking that
sometimes leads young people to focus on themselves to the exclusion of others and to believe that their thoughts feelings and experiences are unique
Invincibility fable Adolescents feel they are immune to the laws of
mortality and probability (and nature) Take all kinds of risks
Personal fable Adolescents imagine their own lives as mythical or
heroic See themselves destined for fame or fortune
Imaginary audience Adolescents fantasize about how others will react
(opinions of onlookers) Assume everyone else judges appearance(s) Not at ease with social world
Adolescence is a time for personal decisions and independent choices with far-reaching consequences
Because adolescents think about possibilities, not practicalities, few adolescents decide important matters rationally
Egocentrism and intuitive thinking makes it hard to analyze and plan ahead
Adolescent Decision Making
Identity Status
Erikson’s Developmental Stages – Review of Past Stages
Adolescent stage struggle is identity versus role confusion
Identity achievement = attainment of identity: self-understanding in accord with past experiences and future plans Willing to reconsider values and goals of parents
and culture, accepting some, rejecting others.
Adolescent Development
Cognitive Problem Solving Hypothesize Inspect Data
Identity & Personality Many Theories Erickson’s
Developmental Theory Identify vs Confusion
Emotional Tasks Needed For “Recovery” Self Manage Stress Identification of Feelings Sort Current Feelings Expressing & Managing Feelings Delayed Gratification Impulse Control
Emotional Intelligence Pt -1
•Integrated From Daniel Goleman’s Emotional Intelligence
Most Substance Abusing or Dependent Adolescents are Behind in Emotional Development.
For Treatment to be Successful we Must Address and Build Skills to Complete the Emotional Tasks
Emotional Intelligence Pt -2
Heart Attacks Follow Doctors Orders? 40% Diabetes Follow Doctors Orders? 35% Drug and Alcohol Abuse/Dependent Who
Make Significant Change? 35%
Why Focus On Change
Change Model Trans Theoretical Model Focuses on Internal Motivation Provides a Treatment “Compass” Concept of “Sequencing Treatment”
Why Stages of Change
Pre-ContemplationNot Ready To Change
Description May see behavior as
posing some problems but not as a problem.
No serious consideration of or desire to change.
Not aware or denying consequences associated with the behavior
Reason For Contact - Mindset
Pressure From Others Proving to others he/she does not have a
problem Court or Legal Referral
Pre-ContemplationNot Ready To Change
ContemplationThinking About Change
Description Serious consideration
to modify behavior Mostly considers
behavior to be a problem
Trying to understand problem
Not yet decided to change

Reason For Contact - Mindset
To Understand Problem or Get Information To Manage Family Problems To Manage Associated Problems
ContemplationThinking About Change
PreparationGetting Ready To Make A Change
Description Has Decided to commit to
Change Willing to make efforts/pay
the price Ready to Take
Responsibility For Change in Behavior
Not Yet Fully Implemented Plan to Change
ActionReady To Make A Change
Description Taking Significant Action
on Own or with Professional Help to Modify Problem
Implement Plan As Long As Active
Attempts With Some Success Are Being Made With Some Success
MaintenanceContinuing To Support Behavior
Change
Description After Some Period of
Active Change, the Individual has Demonstrated Some Ability to Cease or Control the problem
For Research Purposes Generally 6 Months
Pre-ContemplationNot Ready To Change
Tasks Consciousness
Raising- Education and Feedback
Environmental Reevaluation
Reinforcement Management
Social Liberation
In English Intervention-provide
info and personalized feedback, increase perception of risks and problems, discuss possibility of change.
Contemplation Thinking About Change
Tasks Self-Reevaluation Environmental
Reevaluation Consciousness
Raising Helping Relationship Dramatic Relief
In English Intervention - tip
balance in favor of change, elicit reasons for change and risks of not changing, increase confidence
PreparationGetting Ready To Make A Change
Tasks Self Liberation Self Reevaluation Helping Relationship Social Liberation Environmental
Reevaluation Dramatic Relief
In English Intervention -
Strengthen commitment, find a change strategy that is acceptable, accessible and effective
ActionReady To Make A Change
Tasks Counter-Conditioning Stimulus Control Helping Relationships Self Liberation Reinforcement
Management
In English Intervention - Affirm
commitment, identify steps, identify resources, check adequacy of plan, skills and preparation
MaintenanceContinuing To Support Behavior
Change
Tasks Counter-
Conditioning Stimulus Control Reinforcement
Management Self-Liberation
In English Intervention - affirm
commitment, focus on positive benefits noticed, identifying tempting situations, develop relapse prevention plans

Most Utilized Approach In AOD Treatment. Oldest Of All Major Treatment Approaches Focus of Support and Self Reflection With Recent Professionalism Of Field Many See
As A Valuable Support But Not As “A” Or “The” Only Primary Approach To Treatment.
Self Help - 12 Step Approach
Self Help - 12 Step ApproachFor Adolescent Treatment
PRO’S
Easy Model to Follow Broad Reaching
Support Focus on Immediate Positive Culture
CON’S
Developmental Challenges
Motivation Levels Immediate Strain on
Relationship Not Person Centered
or Holistic
Crux of a Medical Model approach 1956 AMA - “The Disease” Most commonly generalized to all
“addictions” Focus - It’s not your fault, It is your
responsibility
Disease Concept
Disease ConceptFor Adolescent Treatment
PRO’S
Medically Endorsed Use Has Serious
Effects PPCF Three - Interrelated
Factors
CON’S
If You Are In Treatment You Have The Disease
Genetic Link Only Established For Alcohol
Forever Focus
Six Stage Objective Process of “Recovery” Comprehensive Linear Model Holistic Life Change Not Just Behavioral
Marker of Non-Use Core Concept Of Process Focus - Progressive Life Style Change Moving
From Using Lifestyle To Sobriety
Developmental Model of Recovery
Developmental Model Recovery
For Adolescent Treatment PRO’S
Progressive Objective Markers More Than One
Behavior Answers Tough Topic
Of Glamorization and Euphoric Recall
CON’S
Behavioral Markers - Where To Go, Not How To Get There
“Dependent” Focus
Stages of Substance Use Holistic Assessment - (Functional) Family Assessment Focus - Altogether a complete treatment
model. Sees adolescent treatment as different. Thorough assessment, LOC recommendation, strength based treatment plan, holistic treatment12 step oriented.
Nowinski’s Model
Functional Assessment
Education Life Skills LEISURE COPING Emotions Self Esteem Spirituality
Cognitive, Literacy, Grade + Future
Communication + Assertiveness Meaningful Fun, Peer Group Stress,Anger, Loss,
Disappointment Pendulum of Happiness to Anger Self Perception, Future Options Personal Values and Ethics
Nowinski’s ModelAdolescent Considerations
PRO’S
Stages of Substance Use
Functional Assessment Strengths Based Adolescent Counselor
Mindset
CON’S
Treats All as Addicts LOC Tied With Stages Focus on Denial not
Person


Medical Marijuana
Tweeners
SYNTHETIC MARIJUANA
WHAT IS IT?
Commonly referred to as K2 or SPICE. It is a dried blend of herbs and spices that is
sprayed with a synthetic chemical. When consumed, K2 or Spice mimics the effects
of Marijuana.
SYNTHETIC MARIJUANA
K2 is sold as incense or potpourri and is commonly purchased in tobacco shops, head shops, gas stations, convenience stores and over the Internet.
It is often marketed as incense or “fake weed.”
It is important for parents to realize that K2 is not illegal in every state so it is easily accessible for purchase over the Internet.

Synthetic marijuana

SYNTHETIC MARIJUANA
Common street names:
Spice Spice Gold Spice Silver Spice Diamond Fire & Ice Demon Genie
SYNTHETIC MARIJUANA
IT IS OFTEN LABELED AS “POTPOURRII”
AND “NOT FOR HUMAN CONSUMPTION”
Synthetic marijuana
PUBLIC HEALTH OFFICIALS ACROSS THE COUNTRY HAVE NOTED THE INTENSE EFFECTS OF SYNTHETIC MARIJUANA.
SOME HAVE FOUND THAT THE CHEMICALS USED IN THE MANUFACTURING OF SYNTHETIC MARIJUANA CAN CAUSE IT’S EFFECTS TO BE 10 TIMES MORE POTENT THAN MARIJUANA.
IN LARGE DOSES, SYNTHETIC MARIJUANA CAN CAUSE SEVERE HALLUCINATIONS AND DISORIENTATION THAT CAN LAST FOR DAYS.
SYNTHETIC MARIJUANA
WHY IS IT SO POPULAR?
IT IS SEEN AS A “SAFE” ALTERNATIVE TO MARIJUANA BY TEEN AGERS
IT IS EASY TO BUY IT IS UNTRACEABLE IN DRUG SCREENS WITH IN
TWO HOURS OF USE.
Synthetic marijuana
REPORTED SIDE EFFECTS: Soaring heart rates Respiratory issues Panic attacks Paranoia, Hallucinations Delusions Vomiting Increased Agitation
Why Kids Use It
1. To Avoid Detection Already have Abuse or Addiction Already have consequences
2. Alcohol and Marijuana Aren’t Enough Tolerance has Developed Tweener Drug
3. Think its Safe and Like Marijuana Curious Misinformed
Managing Resistance
Categories of Resistant Behavior Arguing Interrupting Denying Ignoring
(Miller and Rollnick 1991)
Resistant Behaviors
Arguing: Challenging Discounting Hostility
Interrupting Talking Over Cutting Off(Miller and Rollnick 1991)
Resistant Behaviors (cont)
Denying Blaming Disagreeing Excusing Claiming Impunity Minimizing Pessimism Reluctance Unwillingness to change(Miller and Rollnick 1991)
Resistant Behaviors (cont)
Ignoring Inattention Non-answer No response Side tracking(Miller and Rollnick 1991)
Strategies for Dealing with Resistant Behaviors
Simple Reflection:Respond with “non-resistance” A simple
acknowledgement of the client’s disagreement, emotion, or perception. This can permit further exploration rather than defensiveness.
Amplified Reflection:Reflect back what client has said in an exaggerated
or amplified form. Do not use a sarcastic tone.(Miller and Rollnick 1991)
Strategies for Dealing with Resistant Behaviors, (cont)
Double Sided reflection: Acknowledge what the client has said, and add to it
the other side of the client’s ambivalence. Example: “You can see some real problems, but you are not willing to think about quitting altogether.
Shifting Focus: Shift the client’s attention away from what seems to
be a stumbling block in the way of progress.(Miller and Rollnick 1991)
Strategies for Dealing with Resistant Behaviors, (cont)
Agreement with a twist: Offer initial agreement, but with a slight twist or
change of direction. A reflection followed by a reframe. Example: “You’ve got a good point there, there is a bigger picture, drinking problems like these do involve the whole family.”
Emphasizing personal choice and control: Example: “It really is up to you to decide to change. No one can make this decision for you. No one can
make you change.” Etc. Very important when person feels their freedom has been infringed upon. (Miller and Rollnick 1991)

Real Talk Topics

















