40
MUSCULOSKELETAL AND SPINAL TRAUMA
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | betty-newton |
| View: | 220 times |
| Download: | 0 times |
MUSCULOSKELETAL AND SPINAL TRAUMA
Objectives
Explain common complications associated with orthopaedic emergencies.
Discuss fracture types, shock classifications, and hemorrhage control devices.
Identify compartment syndrome, rhabdomyolysis, and associated treatments.
Differentiate Neurogenic and Spinal shock and associated treatment modalities.
State the proper principles of the initial assessment and management of musculoskeletal injuries.
Epidemology
More than half of all hospital trauma admissions are a result of a fracture
32 million musculoskeletal injuries annually
Most common causes: MVC, falls, assaults, sports injuries.
Musculoskeletal trauma costs $850 billion annually
Annual lost work days totaling 440 million
Powerpoint statement
Musculoskeletal trauma, as a result of blunt force injury, often presents on a spectrum, it may be relatively benign or life/limb threatening. These injuries, though often dramatic and grotesque, are rarely life threatening. However, pelvic and long bone fractures are often an important source of unrecognized hemorrhagic shock.
Primary vs Secondary Management.
Musculoskeletal trauma does not require a reordering of the priorities of the Primary Survey (ABCDE).
Musculoskeletal trauma is predominantly managed in the Secondary Survey
Musculoskeletal trauma is managed in the Primary Survey when hemorrhage control measures are required.
Primary Survey Priorities
Prevent hemorrhagic shock related to Musculosketetal trauma:
Recognize S/S of hemorrhagic Shock (LOC, skin, pulses)
Identify the source of the ongoing hemorrhage (chest, abdomen, pelvis, extremities, external)
Intervene appropriately
Primary Survey Interventions
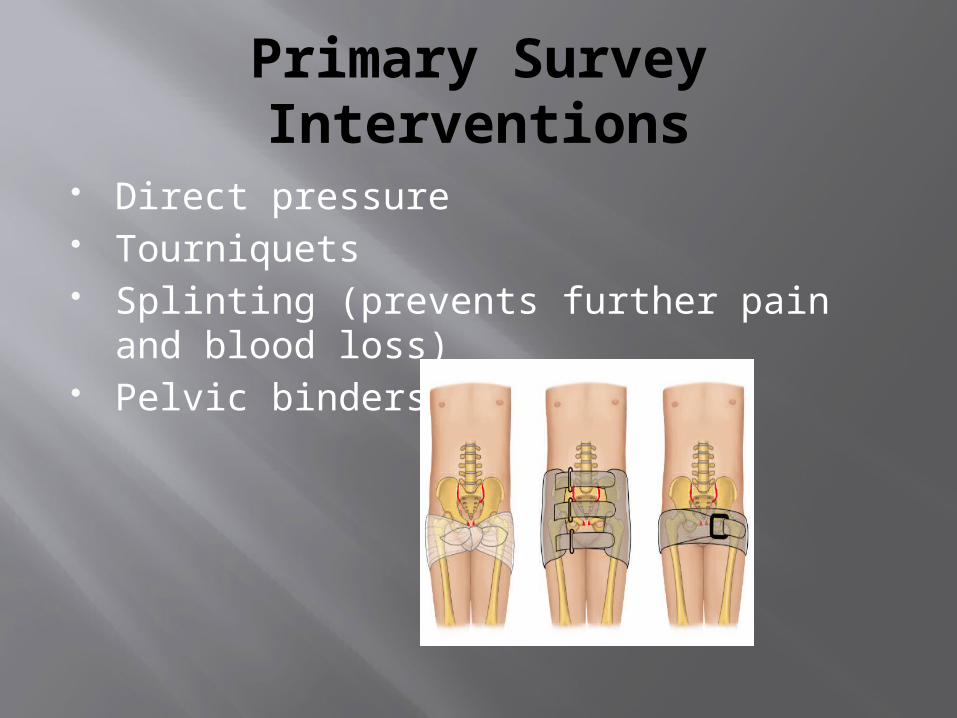
Direct pressure Tourniquets Splinting (prevents further pain and blood
loss) Pelvic binders
Secondary Survey Priorities
History to include MOI SAMPLE Physical examination (Head-to-toe exam) Look, listen, & feel Assess for pain/paresthesias Radiological studies
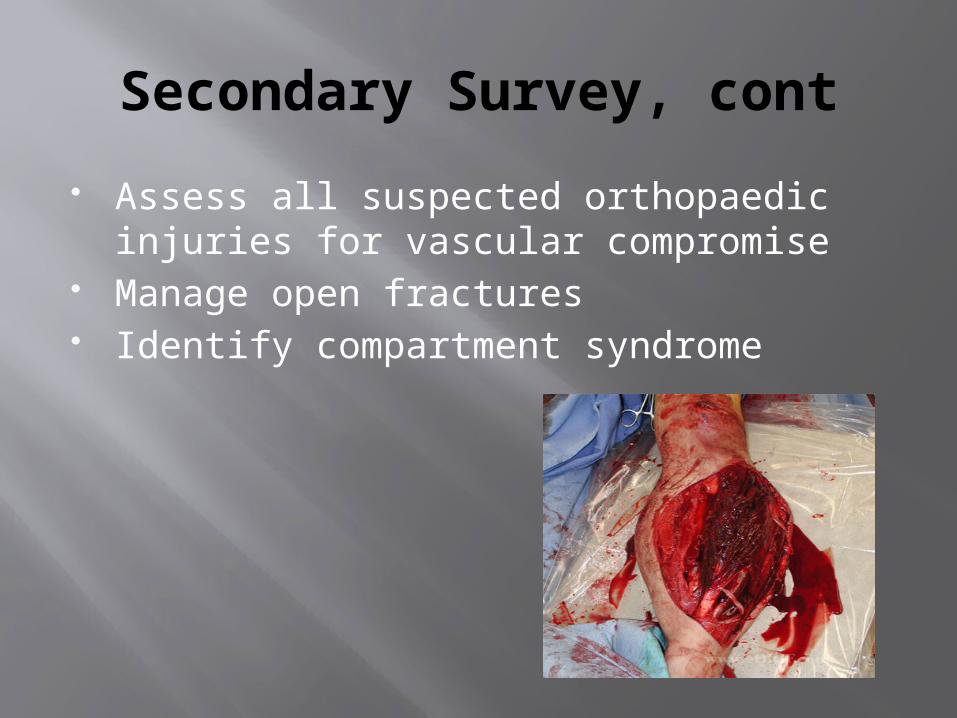
Secondary Survey, cont
Assess all suspected orthopaedic injuries for vascular compromise
Manage open fractures Identify compartment syndrome
Secondary Survey, cont.
Appropriately reduce and splint fractures Irrigate, cleanse, and dress all wounds Ensure appropriate antibiotic therapy Tetanus toxoid prophylaxis Radiologic studies (for hemodynamically
normal patients) Orthopaedic consult early Do not delay transfer
TIME IS
CRITICAL
Case Study
28 y/o male “tree surgeon”. Fell approximately 20 feet while performing his job duties. Fall onto grassy surface with a subsequent “entrapment” by the severed 1000 lb tree limb.
No loss of consciousness. Pt reportedly trapped, by tree limb, for > 2 hours.
Pt reportedly pale, cool, diaphoretic. Enroute via HEMS with full spinal
immobilization.
Case Study, cont.
A: Patent airway. Speech clear and comprehensible. No blood, vomitus, teeth, etc
B: Tachypnea noted. No accessory muscle use. LCTAB. No chest crepitus. Equal chest rise and fall.
C: No obvious external hemorrhage. Two large bore IV’s infusing with isotonic crystalloid. Skin pale, cool, and diaphoretic with weak central pulses. Labs obtained. Pt is confused and lethargic.

Case Study, cont.
C: Skin remains pale, cool, diaphoretic despite 4L of warmed isotonic crystalloid. O+ PRBCs administered. Source of hemorrhage identified: Unstable pelvis and bilateral angulated, deformed femurs. Pelvic binder placed. Interventions improve perfusion.
D: GCS 13. Confusion noted. PERRL. E: Pt exposed and warmed blankets
placed.
Case Study, cont.
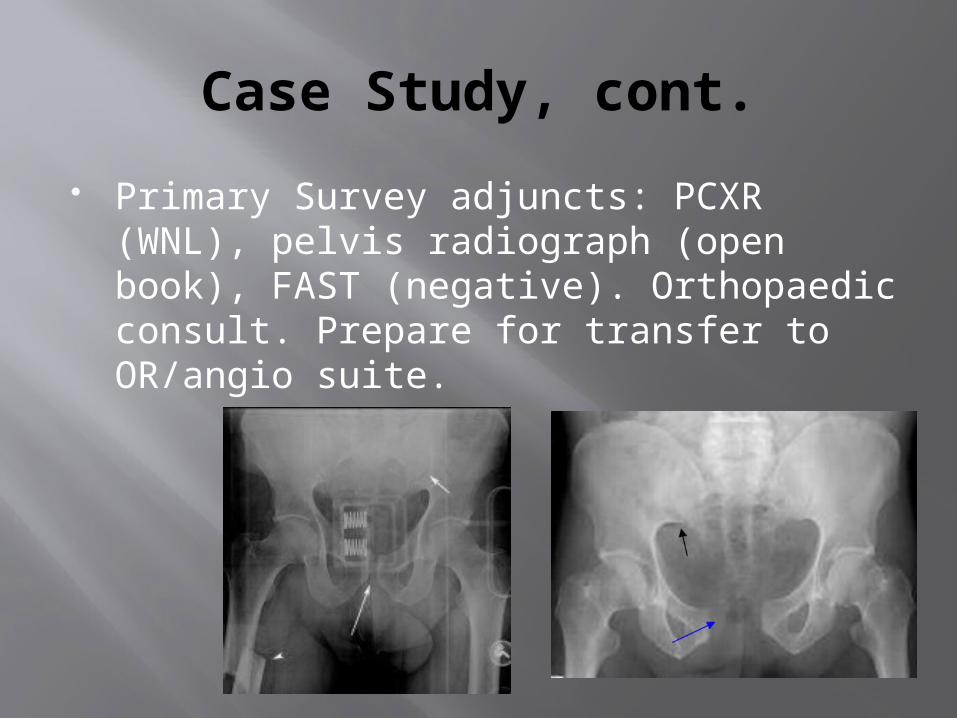
Primary Survey adjuncts: PCXR (WNL), pelvis radiograph (open book), FAST (negative). Orthopaedic consult. Prepare for transfer to OR/angio suite.
Case Study, cont.
SAMPLE history (NKA, No PMH). Pain control measures Head, face, neck, chest, abdomen all
atraumatic, non-tender, and non-deformed. Pelvic binder in place. Urinary catheter
contraindicated due to blood at the urethral meatus.
BLE closed angulated, deformed femoral areas
Posterior surfaces with superficial abrasions
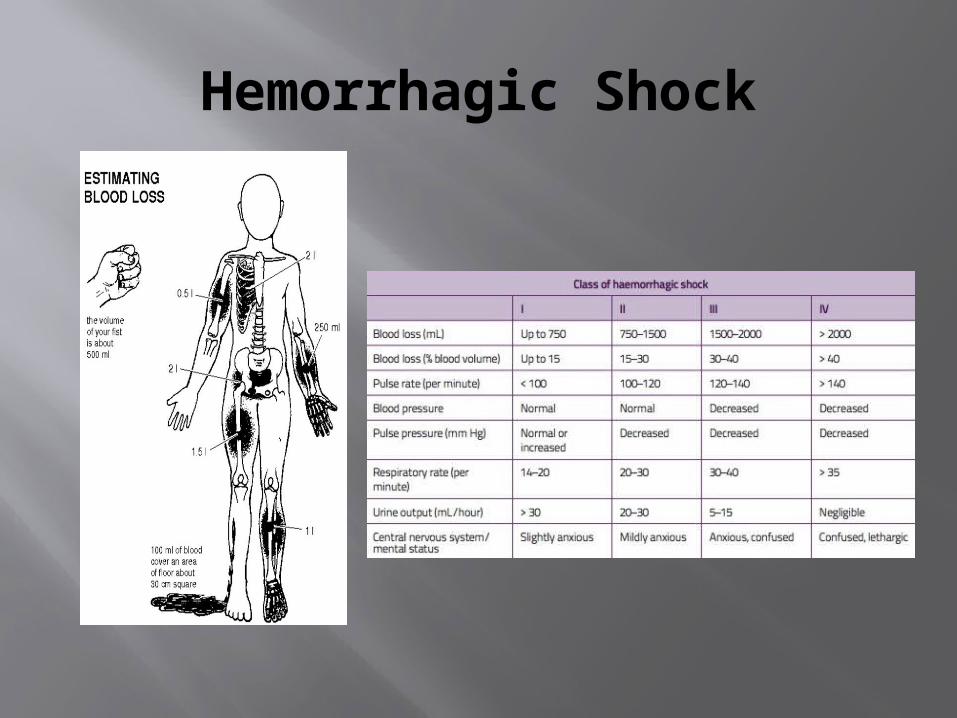
Hemorrhagic Shock
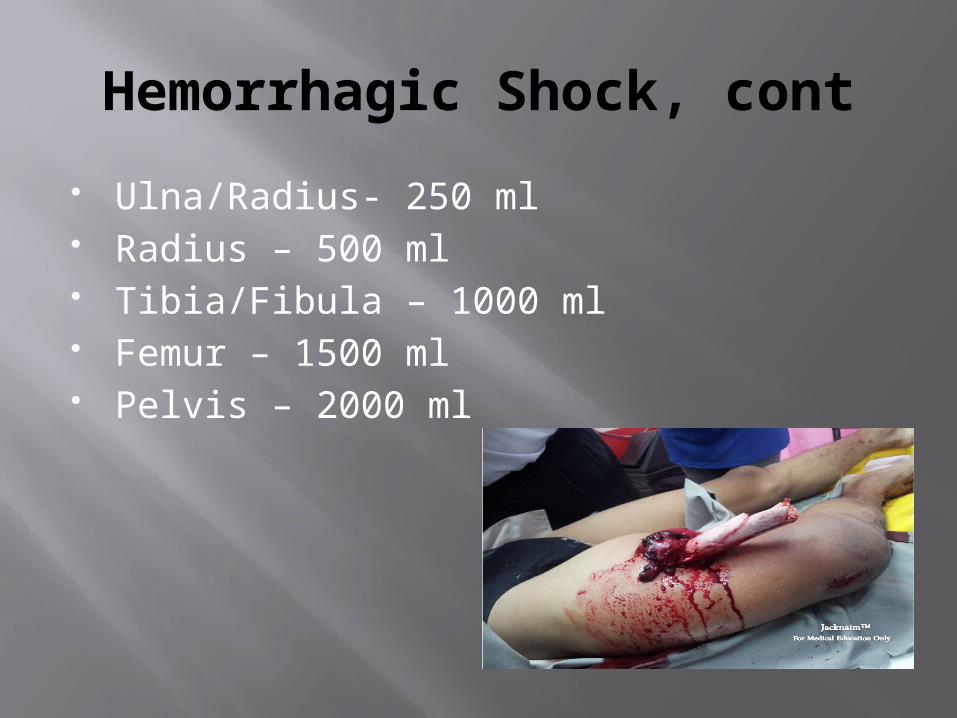
Hemorrhagic Shock, cont
Ulna/Radius- 250 ml Radius – 500 ml Tibia/Fibula – 1000 ml Femur – 1500 ml Pelvis – 2000 ml
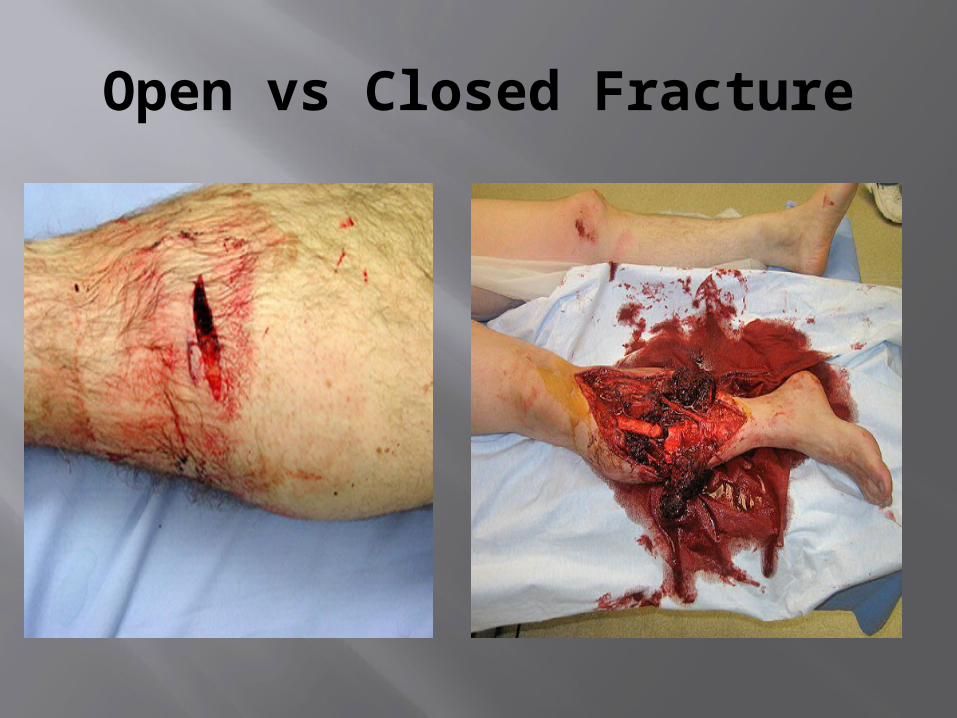
Open vs Closed Fracture
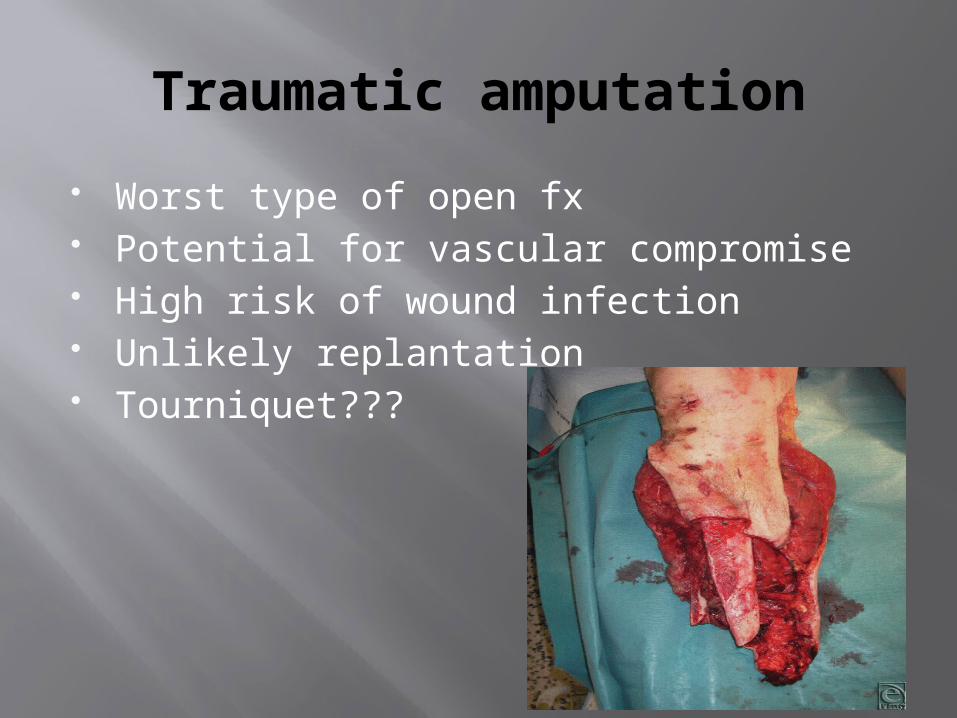
Traumatic amputation
Worst type of open fx Potential for vascular compromise High risk of wound infection Unlikely replantation Tourniquet???
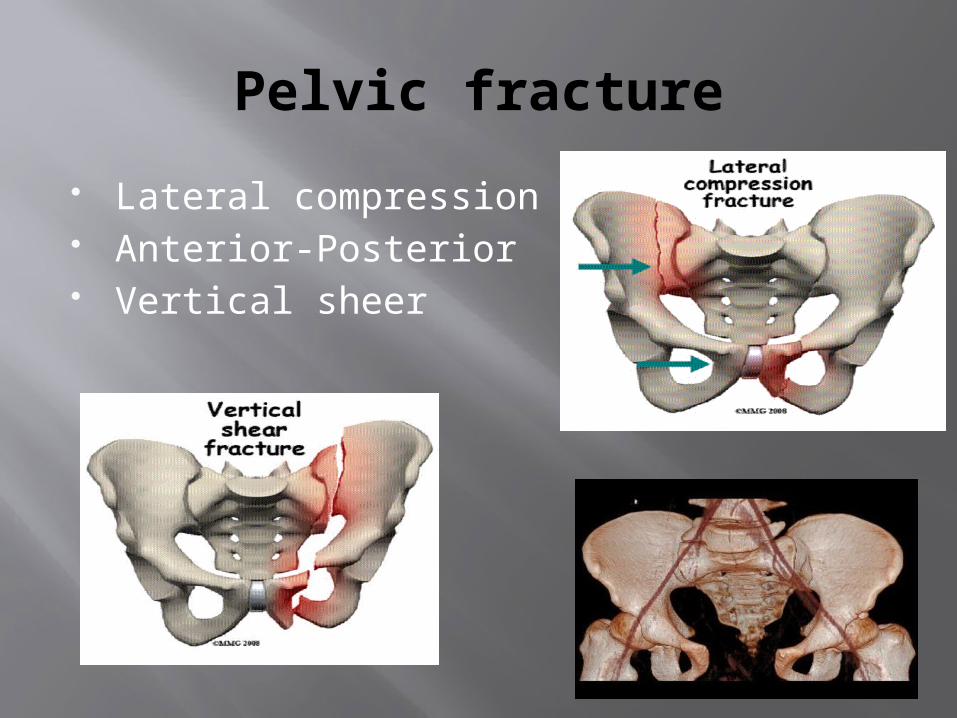
Pelvic fracture
Lateral compression Anterior-Posterior Vertical sheer
Pelvic fractures, cont.
Lateral compression pelvic fractures are often a result of motor vehicle accidents. Involved hemipelvis internally rotates. Pelvic volume decreases. Rarely causes life-threatening hemorrhage.
Anterior-Posterior pelvic fractures are most often caused by pedestrian vs auto injuries, falls >12 feet, MCC, or a direct crush injury. There is pubic diastasis, ligamentous tearing, and hemorrhage likely from the posterior venous complex or iliac arteries.
Vertical Sheer pelvic fractures typically result from a high energy force as falls. This results in major pelvic instability, ligamentous injuries, and potential for life threatening hemorrhaging.
Pelvic fractures, treatment.
Primary Survey management of a Pelvic fracture with affiliated s/s of hemorrhagic shock:
Stop the bleeding (compressive hemorrhage control device-Pelvic binder/Sheet)
Assess for need to transfer (facility, OR, angio) Get expert advice (trauma/ortho surgeon,
interventional radiologist) Continue initial resuscitative efforts to achieve
balanced resuscitation (SBP approx 90mmHg).
Crush Syndrome
This term refers to the clinical effects of crush injury, compartment syndrome, rhabdomyolysis, and acute renal failure.
Often described as a localized injury with generalized effects.
Most common injury types are lower extremity injuries ( tibia/fibula are the most common)and upper extremity injuries (ulna/radius are the most common)

Crush Injury
Compartment Syndrome
Pressure within the fascial compartment occludes distal perfusion therefore depriving the muscle of necessary oxygen and nutrients.
Ischemia > 6 hours causes necrosis Devastating effects of muscle necrosis
cause the cellular release of myoglobin and potassium, hyperkalemia, acidosis, coagulopathies, and subsequent acute renal failure.
Compartment Syndrome Causes
Severe crush injuries Burns Fractures or associated vascular injuries Constrictive splints, dressings, casts Tibia and radius fractures the most
common injuries associated with compartment syndrome. Other injury types include foot, hand, gluteal, and thigh injuries.
Recognizing Compartment Syndrome
6 P’s (disproportionate PAIN, PALLOR, PULSELESSNESS (late sign), PARESTHESIA, PARALYSIS, and PRESSURE.
Asymmetrical, firm, swollen extremity Intracompartmental pressure > 35-45
mmHg (delta-P = DBP - compartment pressure) Delta-P of 30 mmHg or less is suggestive of compartment syndrome.
Patient’s with altered sensorium may require more objective assessments (pale, cool, swollen, bruised, or pulseless extremities).
Compartment Syndrome management
Remove all potentially constricitve dressings, casts, and splints.
If no improvement, a fasciotomy is required
Frequent neurovascular assessments OR for fascial decompression and
debridement of necrotic muscle tissue. Prevent the progression to traumatic
rhabdomyolysis.
Rhabdomyolysis
Muscular trauma is the most common cause
Ischemic muscle tissue releases myoglobin, Potassium, and creatine kinase (CK).
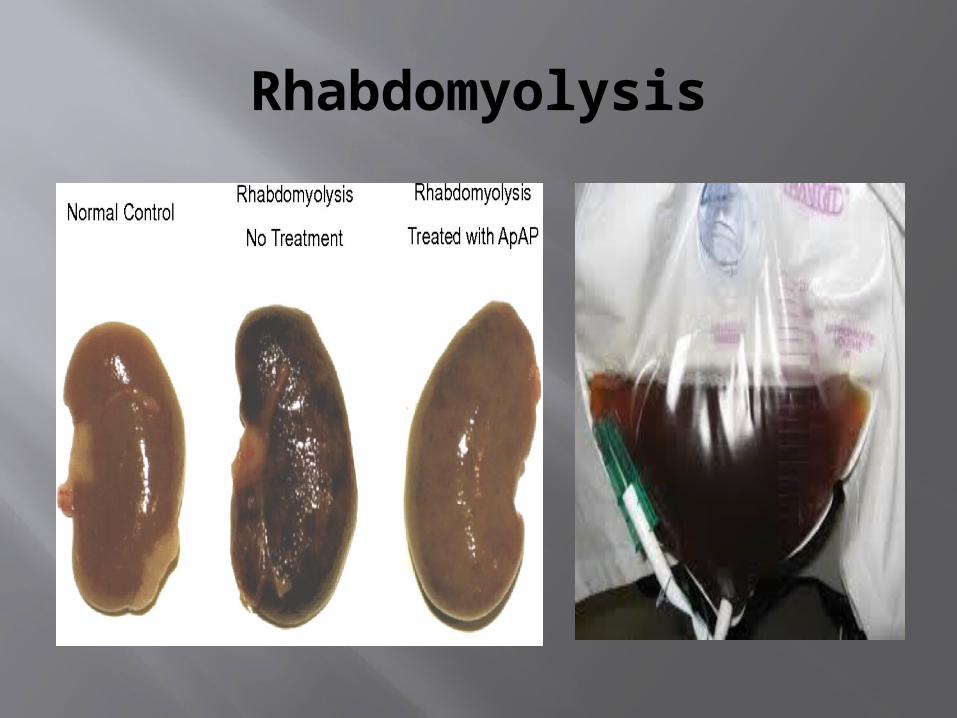
Myoglobin and CK accumulate in the renal tubules producing dark amber urine which tests positive for hemoglobin (myoglobin assay is necessary to confirm the presence of myoglobin).
If untreated, this leads to acute renal failure, metabolic acidosis, and coagulopathies.
Rhabdomyolysis Management
EARLY and AGGRESSIVE IV fluid administration.
Prevent hypotension (utilizing IV fluids) Goal is to achieve 100 ml/hr of urinary
output. Consider osmotic diuresis (caution in
trauma patients) to achieve goal urinary output.
Prevent hypothermia
Rhabdomyolysis Managgement, cont.
Rhabdomyolysis associated hyperkalemia treatment:
Sodium Bicarbonate (1mEq/Kg) Calcium chloride IVP Regular Insulin 10 units IVP followed by
25 grams of D50. Kayexalate Hemodialysis or CRRT. Closely monitor EKG and be wary of
cardiac dysrhythmias.
Rhabdomyolysis
New Research in Rhabdomyolysis management
TRADITIONAL thoughts on Rhabdomyolysis: Crush injuries cause skeletal muscle damage Damaged skeletal muscle releases myoglobin Myoglobin lodges in the renal tubules Acute renal failure ensues due to the
accumulation of myoglobin Treatment includes: copious amounts of IVF,
Sodium Bicarbonate, dialysis (HD of CRRT), prevention of hyperkalemia, acidosis, coagulopathies, and hypothermia.
New Research in Rhabdomyolysis management
Vanderbilt study on Rhabdomyolysis: Crush injuries cause skeletal muscle damage Damaged skeletal muscle releases
myoglobin Myoglobin lodges in the renal tubules Myoglobin undergoes “Redox-cycling” Release of oxidative free radicals Acute renal failure caused by oxidative free
radical damage Treatment includes all traditional options
with Acetaminophen
Spinal shock
Signs & Symptoms: Loss of muscle tone Loss of reflexes below the level of the
injury Loss of sensation Treatment: No specific treatment Transient in nature Symptomatology is often self limiting
Neurogenic shock Pathophysiology
Almost always occurs in injuries above T6 Loss of descending sympathetic
pathways Loss of vasomotor tone and sympathetic
innervation to the heart. Loss of vasomotor tone results in
peripheral vasodilation, pooling of blood, and subsequent hypotension.
Loss of sympathetic innervation to the heart results in bradycardia or the loss of the reflexive tachycardia.
Neurogenic Shock Treatment
Customary hypovolemia treatment is often unsuccessful
Judicious IV fluid administration Vasopressors Atropine (for hemodynamically significant
bradycardia) Airway support due to potential for
phrenic nerve paralysis (injuries at or above C5)
Support hemodynamics.
Conclusion
Musculoskeletal trauma does not require a reordering of the priorities of the Primary Survey (ABCDE).
Musculoskeletal trauma is managed in the Primary Survey when hemorrhage control measures are required.
Musculoskeletal trauma is typically managed in the Secondary Survey with splinting, wound care, orthopedic consults, radiological studies, antibiotics, tetanus toxoid, & transfer consideration.
Conclusion
Identify symptomatology related Crush injuries, compartment syndrome, and rhabdomyolysis.
Provide appropriate treatment related to these injuries.
Differentiate Spinal and Neurogenic Shock
Provide appropriate treatment for these injuries.


















