69
+ Impact of New Anticoagulants on the Blood Bank January 24 th , 2012 Transfusion Medicine Resident Teaching Session Dr. Sudeep Shivakumar, Hematology
| Date post: | 22-Dec-2015 |
| Category: |
Documents |
| Upload: | ashlie-hensley |
| View: | 213 times |
| Download: | 0 times |

+
Impact of New Anticoagulants on the Blood Bank
January 24th, 2012Transfusion Medicine Resident Teaching Session
Dr. Sudeep Shivakumar, Hematology

+Objectives
To briefly review the concepts of hemostasis and thrombosis
To provide an overview of anticoagulants currently in use
To discuss the new anticoagulant agents and their mechanism of action
To review the evidence for the new anticoagulants in DVT/PE and atrial fibrillation
To discuss implications of these medications for the blood bank

+Overview
Anticoagulants are widely used
Vitamin K antagonists used to be the only oral option
Times are changing…

+
+

+Overview
Big advantage: No lab monitoring
Big disadvantage: No lab monitoring
Unpredictability of coagulation tests No reversal agents Variety of different agents with different characteristics

+Background
What are anticoagulants? Substances that prevent blood from clotting
“Blood thinners”
How do they do this? Interfering with coagulation mechanisms

+Hemostasis
Complex process which causes bleeding to stop:
Formation of blood clot formation at the site of vessel injury
Carefully regulated system Involves platelets and coagulation factors
Lack of coagulation factors bleeding
Overactive coagulation cascade thrombosis
+Thrombosis
The formation of a blood clot within a blood vessel
Can occur in the arterial or venous systems
Leads to obstruction of a blood vessel in the circulatory system
Can lead to ischemia and infarction, and even death
Can also lead to embolism Clot within a vessel breaks free and travels through body
(“embolizes”) Thromboembolism is combination of a thrombosis and embolus

+Atrial fibrillation
Most common cardiac rhythm disorder Affects >10% in those > 80 years old
Krahn et al, Am J Med, 1995
Incidence of atrial fibrillation in 4000 male air crew recruits

+Atrial fibrillation
Lifetime risk for a 40 year old is ~25% (Framingham1)
Independent risk factor for ischemic stroke Rate of stroke in those not on antithrombotic therapy is ~4.5%/year Increases the risk of stroke 5x across all age groups Incidence of stroke increases with age2
1.3% per year for those aged 50-59 5.1% per year for those aged 80-89
2Frost, Am J Med, 2000
1Wolf, Stroke, 1991

+Anticoagulants in atrial fibrillation
Goal is to prevent stroke
Reduces risk to ~1% per year
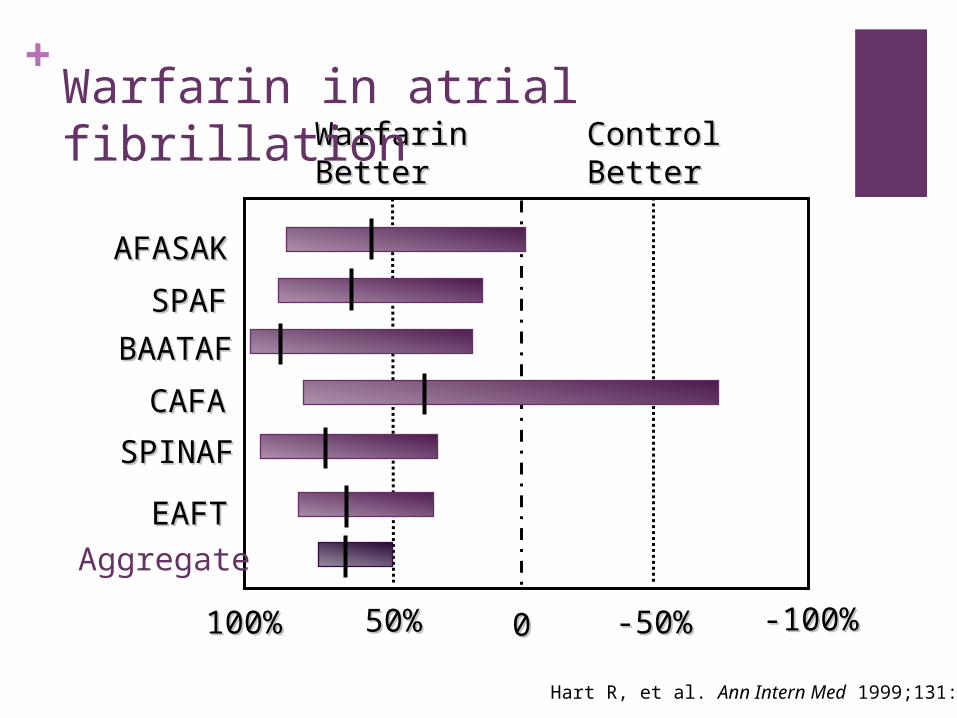
Warfarin shown to be more effective than aspirin
+
Hart R, et al. Ann Intern Med 1999;131:492
WarfarinWarfarinBetterBetter
ControlControlBetterBetter
AFASAKAFASAK
SPAFSPAF
BAATAFBAATAF
CAFACAFA
SPINAFSPINAF
EAFTEAFT
100%100% 50%50% 00 -50%-50% -100%-100%
Aggregate
Warfarin in atrial fibrillation

+Anticoagulants in atrial fibrillation
Most recent Canadian Cardiovascular Society guidelines (2010):
Patients with CHADS2 score of 1 or higher should be on oral anticoagulants

+

+

+Venous thromboembolism
Deep venous thrombosis Pulmonary embolism

+Venous thromboembolism
Incidence estimated at 1-2 in 1000
Known predisposing conditions – Virchow’s triad:
Venous stasis
Hypercoagulability Vessel wall injury

+Venous thromboembolism
Not uncommon Longitudinal investigation of thromboembolism etiology (LITE)
study1
>21 000 participants Cohort study Incidence of 1st time VTE = 1.92 per 1000 person years
Major cause of morbidity and mortality JAMA study2 looking at post-mortems of 3 412 hospitalized patients
between 1966 and 1980 6% of deceased patients had evidence of massive pulmonary
embolism
Most common preventable cause of in-hospital death1Cushman, Am J Med, 2004
2Dismuke, JAMA, 1986

+Pulmonary embolism
Untreated PE Mortality rate of ~30%1
Most die within hours of diagnosis
Treated PE Prospective NEJM study looked at 399 patients with newly
diagnosed PE 94% received anticoagulant treatment Only 2.5% (10 patients) died of PE
Treatment of PE is life-saving!
1Dalen, Prog Cardiovasc Dis, 1975
2Carson,NEJM, 1992

+Anticoagulants in DVT/PE
Goals of treatment:
Short term: Prevent the extension of thrombus and embolization for DVT Reduce mortality for PE by reducing recurrent events Relief of symptoms
Long term: Prevent recurrent events

+Anticoagulants currently used
Unfractionated heparin
Low molecular weight heparin
Vitamin K antagonists Ie. warfarin

+Warfarin
Can be reversed:
Vitamin K Fresh frozen plasma Activated prothrombin complex concentrates

+Warfarin
Dosage varies because of:
Vitamin K status Dietary factors Nausea/vomiting Absorption
Activity level Other medications Genetics
Monitoring by INR necessary!

+Difficulties with warfarin use
Requires monitoring
Numerous drug and diet interactions
Narrow therapeutic range
Difficult to control – takes time to get in or out of the system
Role for new anticoagulants?

+New anticoagulants
Many new targets being explored Eg. thrombin, factor Xa, tissue factor, protein C, factor V and VIII
New agents developed Direct thrombin inhibitors Factor Xa inhibitors Novel anticoagulants
Oral agents increasingly in studies Venous thromboembolism often studied first because of shorter
follow up
Increasing data on dabigatran and rivaroxaban

+New anticoagulants
Ideal anticoagulant: Equally efficacious Equally safe No monitoring Fewer interactions Oral Reversible

+New anticoagulants
Direct thrombin inhibitors Dabigatran
Factor Xa inhibitors Rivaroxaban

+New anticoagulants
Leung, The Hematologist, 2011

+Dabigatran
Ximelagatran studies showed possible use for oral direct thrombin inhibitors in atrial fibrillation
Dabigatran Oral prodrug of dabigatran etixalate Inhibitor of thrombin Predictable anticoagulant response No need for monitoring Excreted by kidneys Less than 1% see a transaminase elevation

+Dabigatran
An ideal anticoagulant:
No monitoring
Fewer interactions
Oral
Reversible
Equally efficacious
Equally safe

+Dabigatran
An ideal anticoagulant:
No monitoring
Fewer interactions
Oral
Reversible
Equally efficacious
Equally safe
✓
✓
✓
✗
?
?

+Dabigatran
Pharmacokinetics
Half life 12-17 hours Time to peak, plasma 1 hour Hepatic metabolism Not recommended for CrCl <30

+Dabigatran
Many studies for VTE prophylaxis: REMODEL – thromboprophylaxis after knee surgery REMOBILIZE – thromboprohylaxis after knee surgery RENOVATE I and II – thromboprophylaxis after hip surgery
Studies for VTE treatment: RECOVER – acute VTE treatment REMEDY – secondary VTE prevention
Studies for atrial fibrillation: PETRO study – phase II RELY study – phase III

+

+Dabigatran for atrial fibrillation
RELY trial
Looked at stroke prevention in patients with atrial fibrillation Compared warfarin to dabigatran >18 000 patients Results:
110 mg BID dose of dabigatran as effective and less bleeding 150 mg BID dose more effective, similar bleeding
Published in NEJM in September 2009 (Connolly et al)

+

+Dabigatran for atrial fibrillation
RELY trial
Note trend towards increased MI rates with dabigatran 150 mg BID Also increased dyspepsia
Consider higher dose if <80 and low risk of bleeding

+

+

+Dabigatran for VTE
RECOVER trial
Dabigatran exilate vs warfarin in the treatment of acute thromboembolism
Randomized double blind trial 2539 patients with acute VTE All treated initially with 5 to 11 days of LMWH or UFH Randomized to dabigatran 150 mg BID vs warfarin Primary outcome: objective recurrent VTE, or VTE-related death up
to 6 months of treatment

+Dabigatran for VTE
RECOVER trial Results:
Recurrent VTE: 34 patients (2.7%) in dabigatran group 32 patients (2.5%) in warfarin group (not significant)
Major bleeding: 20 patients (1.6%) in dabigatran group 24 patients (1.9%) in warfarin group (significant)
Deaths similar between groups Conclusions:
Dabigatran as safe and efficacious as warfarin Published in NEJM in December 2009 (Schulman et al)

+

+

+Dabigatran
Approved by Health Canada for atrial fibrillation
Not covered by MSI… yet
Not approved for VTE treatment
Costs $2.30 per day

+Dabigatran and coagulation assays

+Dabigatran and coagulation assays
aPTT affected at peak concentrations aPTT >90 sec suggests over-dosing or accumulation
PT not affected
Fibrinogen testing underestimated results in 2 of 4 reagents
Antithrombin levels varied greatly
Overall, unpredictable results, but elevated aPTT suggested accumulation

+Factor Xa inhibitors
•Lack of direct thrombin inhibition = less bleeding?

+Rivaroxaban
Oral, direct factor Xa inhibitor
Potent (greater selectivity for factor Xa than other drugs)
Fixed, once-daily dosing Predictable pharmacokinetics Half life 7-11 hours
Peak concentration 4hrs after administration
Excreted via biliary and renal routes
Does have interactions CYP3A4 inhibitors Ie. ketoconazole, macrolides

+

+Rivaroxaban
EINSTEIN study NEJM study (Dec 2010) Complicated – 2 studies in one One study compared rivaroxaban to warfarin for DVT/PE
1700 patients Similar outcomes in both arms for bleeding/thrombosis No LMWH briding in rivaroxaban arm
Conclusion: rivaroxaban as safe and effective as warfarin
Not currently approved or covered for DVT/PE

+

+Rivaroxaban
Studied in ROCKET-AF trial Rivaroxaban once daily oral direct factor Xa inhibition compared
with vitamin K antagonism for prevention of stroke and embolism trial in atrial fibrillation
Phase III, non-inferiority, double-blind study of rivaroxaban 20 mg OD vs. warfarin in patients with non-valvular atrial fibrillation and 2 other stroke risk factors
Recently approved by Health Canada for stroke prevention in atrial fibrillation

+Rivaroxaban and coagulation assays

+Rivaroxaban and coagulation assays
aPTT affected at therapeutic doses, but varied greatly Depended on reagents used Unpredictable
PT completely unpredictable
Antithrombin levels depended on reagent used
Fibrinogen not affected
Xa (sensitive to rivaroxaban) only affected slightly
Overall, varied, unpredictable results

+Bleeding
~2% of patients/year on long term anticoagulants will end up with a major bleed requiring medical attention
Holding anticoagulants is the first step, but often other steps are needed
Depends on anticoagulant

+

+Bleeding
Warfarin Give vitamin K 5-10 mg Fresh frozen plasma Octaplex
Prothrombin complex concentrate Works within 1 hour More effective than plasma at reversing INR Small volume 40 ml usually enough for most patients $$$$$

+Reversal of new anticoagulants
Warfarin had several predictable options for reversal:
Vitamin K Fresh frozen plasma Activated prothrombin complex concentrates
No reversal agents for new anticoagulants

+
Circulation, 2011

+Reversal using PCC
Randomized, double-blind, placebo controlled study
12 healthy male volunteers received rivaroxaban 20mg BID or dabigatran 150 mg BID for 2.5 days
Followed by bolus of 50IU/kg PCC (Cofact) or saline
Procedure then repeated with the other anticoagulant treatment

+Reversal using PCC
Rivaroxaban: Prolonged the PT Immediately reversed by PCC completely Endogenous thrombin potential inhibited Also completely normalized with PC
Dabigatran: Affected PTT, ecarin clotting time, and thrombin time Not reversed by PCC

+

+

+Bleeding
Dabigatran, rivaroxaban and other new agents No known antidotes Half-lives roughly 11-14 hours Blood product support Fresh frozen plasma Consider activated factor VIIa if ongoing bleed
Watch for thrombosis

+Reversal of new anticoagulants
Suggested approach:
Transfuse as necessary Packed red blood cells Platelets if less than 50
Consider use of other blood products Fresh frozen plasma Activated factor VII
No good evidence!

+

+Summary
New anticoagulants are coming that may replace warfarin
Dabigatran has been approved for atrial fibrillation, and will likely be approved for DVT/PE
Rivaroxaban has been approved for atrial fibrillation, and will likely be approved for DVT/PE
No antidotes for new agents
Coagulation tests not standardized
Research needed!


















