25
COUGH COMPONENTS Inspiratory Phase Compressive Phase Glottis closing Building of pressure Expiratory Phase (glottis opening)
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | ariel-bennett |
| View: | 222 times |
| Download: | 0 times |

COUGH COMPONENTS Inspiratory Phase
Compressive Phase Glottis closingBuilding of pressure
Expiratory Phase (glottis opening)

HUFF Not the same components of a cough
Can be more effective in clearing secretions
To train patients, DEMONSTRATION.
FET – active cycle of breathing

ASSISTED COUGH TECHNIQUES Splinting
CABG, thoracotomy, belly surgeries, incision in “pop can”.
Quad CoughingWho?: ALS, SCI
Variety of different ways to increase expulsion force through positioning and careful manual pressure through CHEST WALL and ABDOMEN. (Interconnection)


COUGH ASSIST MACHINE AKA – Coughalator,
Mechanical In-Exsufflator, “The Cougher”
Non-invasive way to clear secretions. (alternative to suctioning)
Two Way Vaccuum
WHO?
Indications for Use:
Any patient unable to cough or clear secretions effectively due to reduced peak cough expiratory flow (less than 3 liters per second), resulting from: High spinal cord injuries Neuromuscular deficits or Severe weakness
associated with intrinsic lung disease, is a candidate for the CoughAssist.
OUR Indications for Use?
Ineffective Cough Unable to clear secretions Diagnoses:
SCI ALS MD Trached patients Pneumonia Atelectasis Bronchiectasis: chronic
secretions. Scarring and damage of lungs.

CONTRAINDICATIONS Bullous Emphysema: airways collapse Known susceptibility to pneumothorax Recent Barotrauma: trauma deep in lungs related
to pressure
EVIDENCE BASED PRACTICE Massery et al. 2003, Cardiopulmonary PT Journal. Showed that
cough assist was just as effective as suctioning. Marchant and Fox 2002, Br J Anaesthesia. Case study preventing
tracheostomy. Kan and Bach 2000, Chest. Deep insufflations improved ability to
air stack; and cough effectiveness. John R. Bach – multiple studies on progressive neuromuscular
diseases. Show cough assist machine even more effective with manual assist (peak cough flows).
Chatwin et al. 2003, Sivasothy et al. 2001. Showing cough assist machine effective with cough augmentation
PROCESS
Set up: Filter is hooked to the port of machine, then
connected to blue tubing (RT) Green plastic connector, then smaller blue tubing Mouth piece, face mask, trach adaptor Throw out small blue tubing at end of session.
Cost – approximately $3,500-5,000
SUCTIONING Sterile Technique
Don sterile glovesKeep one hand sterile and always on the
suction tubeThe other hand touches the valve and
other equipment Ballard
Closed systemUse clean gloves

SUCTIONING Get equipment ready
Suction deviceGlovesAmbu bag
Suction pressure 60-120 mmHg Ventilate, especially if removing vent–
bag 3-5 times Insert to level of carina, no suction
going in Remove and twist, suction on way out

SUCTIONING 10 sec duration in body 20-30 in between suction technique 3-4 times max Clean suction in between contact with
body with sterile saline
Some PTs do use sterile saline or hypertonic saline

SUCTIONING
Indications Pt is unable to clear
secretions independently.
Pt is having difficulties breathing due to secretions/obstruction.
Unable to clear secretions by any other method.
Types Tracheal (only within the
trach.) Deep (further than trach
and into lung tissue). Procedure:
Sterile vs Clean Suction set 120-140
mmHg 10-12 seconds

SUCTIONING
Enter catheter: cautiously but quickly, until you feel resistance (carina)
Apply suction and slowly pull catheter out.
Twist catheter as you pull out catheter.
Monitor saturations, and assist with ambu bag prior/following.
SUCTIONING
What vitals do you want to monitor??Heart Rate Blood PressureSPO2Respiratory Rate

SUCTIONING
Complications Desaturation/hypoxia Cardiac arrhythmias, Tachy cardia and Hypertension Pulmonary hemorrage/bleeding Bronchospasm Elevated ICP
Is one of the most invasive techniques we do as physical therapists.

DEAN’S HIERARCHY FOR TREATMENT WITH IMPAIRED OXYGEN TRANSPORT
1. Mobilization and Exercise2. Body Positioning3. Breathing Control Maneuvers4. Coughing Maneuvers5. Relaxation and Energy Conservation
Interventions6. ROM exercises7. Postural Drainage Positioning8. Manual Techniques9. Suctioning
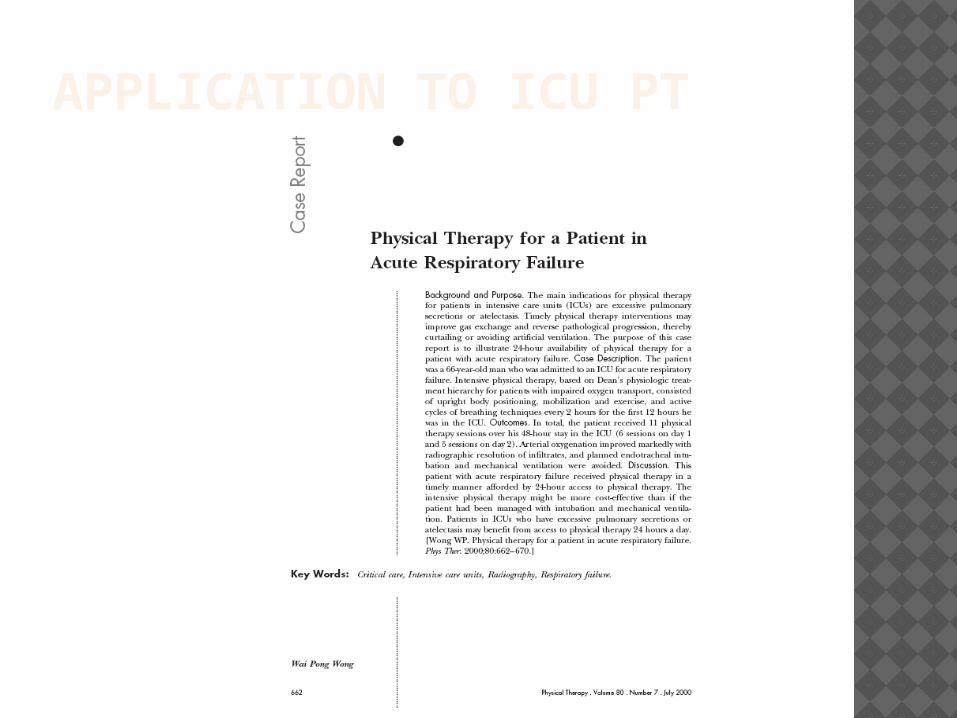
APPLICATION TO ICU PT


WONG 2000
Patient in respiratory distress.
PT performed multiple treatments. STG to improve V/Q, decrease WOB, and airway clearance
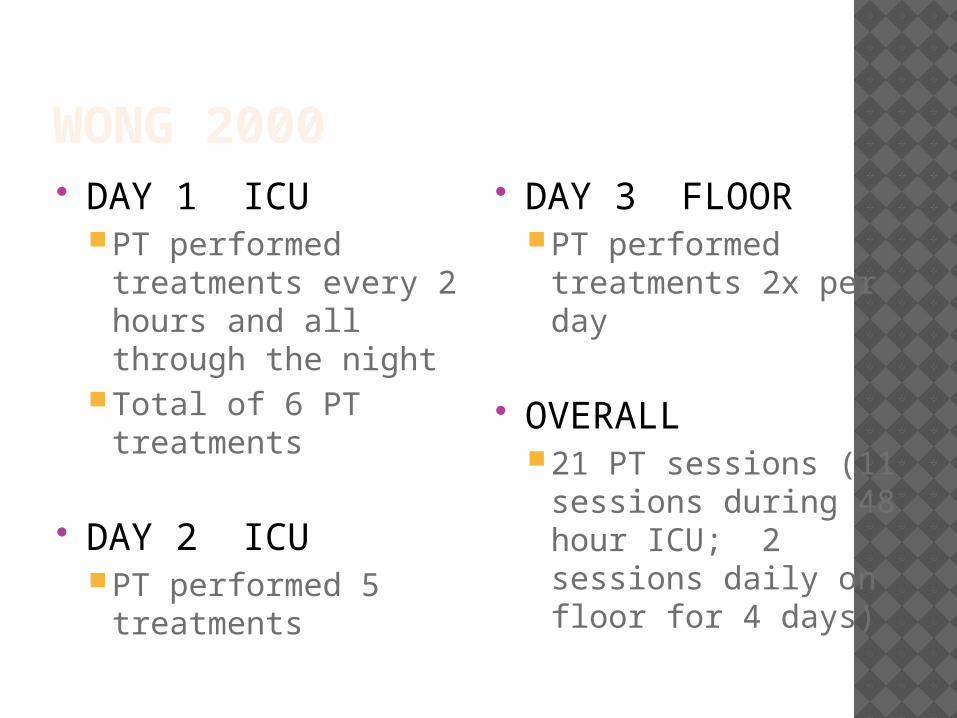
WONG 2000 DAY 1 ICU
PT performed treatments every 2 hours and all through the night
Total of 6 PT treatments
DAY 2 ICUPT performed 5
treatments
DAY 3 FLOORPT performed
treatments 2x per day
OVERALL21 PT sessions (11
sessions during 48 hour ICU; 2 sessions daily on floor for 4 days)
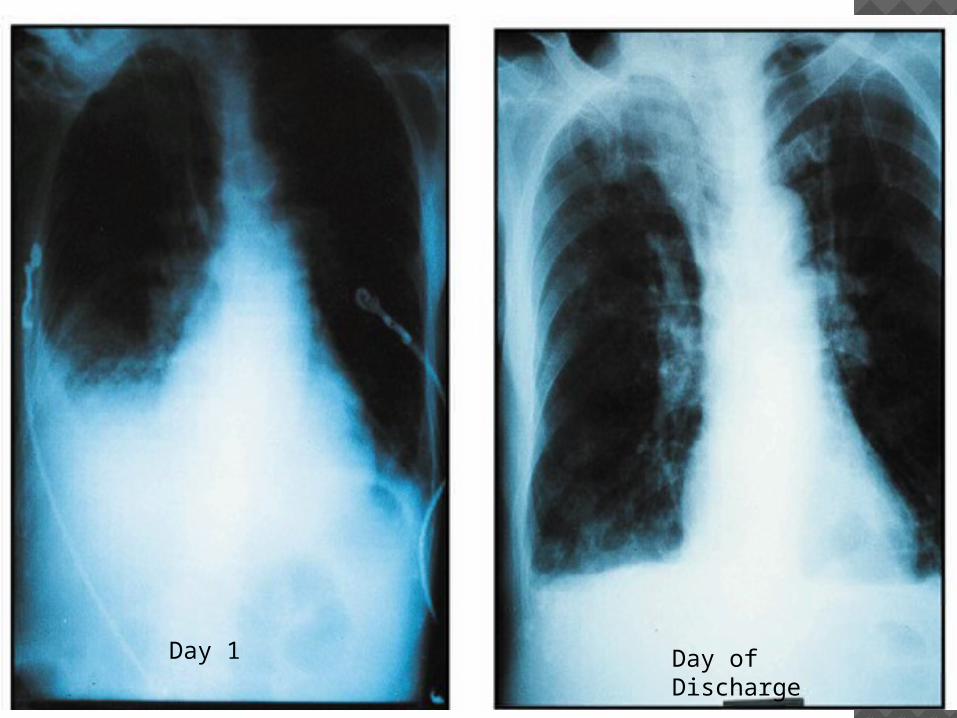
Day 1 Day of Discharge
SUMMARY OF CURRENT EVIDENCE Airway Clearance techniques assist in
short term for secretion removal but currently there is no evidence supporting long term benefit above cough alone.
All techniques show improvement in secretion removal though no one technique has been proven better than the others and different patients will show different benefits from each technique.

SUMMARY OF CURRENT EVIDENCE Method of airway clearance for any
particular patient needs to be tailored to that patient’s needs to assure effective therapy with the greatest independence.
What works for any particular patient now may not work in the future with that patient, and what does not currently work for any particular patient now may become more helpful in the future.
SUMMARY OF CURRENT EVIDENCE Position change is the only consistently
demonstrated method of changing ventilation to any particular part of the lung
ULTIMATELY – use of ANY technique is better than nothing.
EX: if had pneumonia in left, then best on right, which is nice for moblization.

















