28
MUSCLES
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | felicity-gordon |
| View: | 232 times |
| Download: | 1 times |
MUSCLES

Types of Muscle
Skeletal Most common Attached to bone (via tendons) Voluntary Striated

Cardiac Muscle In the heart only Involuntary Striated
Smooth Muscle Surrounds organs Slow, long contractions Involuntary Non-striated; forms dense sheets

The Neuromuscular System
Complex linking of the muscular and neurological systems
Constant use and practice improves the quality, efficiency and ability of these systems to work together E.g. agility training
The Motor Unit Nerves transmit impulses in waves- the resulting
contraction is called a muscle twitch 1 nerve + the muscle fibers it innervates = motor unit 1 nerve stimulates many muscle fibers, thereby producing
muscle movements. 1 nerve + a few muscle fibers =fine movements (eg
blinking) 1 nerve + lots of fibers = gross/big movements (eg
contraction of the quadriceps) All-or-None Principle
When a motor unit is stimulated to contract, either ALL of the muscle fibers will contract, or none will

Types of Muscle Contraction
Concentric Muscle fibers shorten E.g. bicep flexion
Eccentric Muscle fibers lengthen Eg bicep extension
Isometric Contraction without change in length of muscle; no
motion; decreased risk of injury E.g. pushing against a wall; doing a abdominal plank.

http://www.youtube.com/watch?v=A1haS8hR1lE

Muscle Origin vs Insertion
Origin where the muscle attaches to more stationary
of the bones of skeleton. Usually more superior
Insertion Where the muscle attaches to the bone that
moves most Usually more inferior

Antagonistic Pairs
Skeletal muscles are arranged as opposing pairs
Agonist Prime mover of the body part Eg. During knee extension, quadriceps are the
agonist Antagonist
Counter-acts the agonist Eg. During knee extension, hamstrings are the
antagonist

Label the following muscles of the lower limb:
Flexor hallicus longus Anterior tibialis Soleus Gastrocnemius Patella Quadriceps Hamstrings Gluteus medius, minimus, maximus Abductor muscles Adductor muscles Peroneals




Can you label these muscles??

Muscles of the Leg and their Functions
Leg- refers to lower limb below the knee Thigh = hip to knee

Muscle/Muscle Group
Origin Insertion Action
Toe/foot extensors
Anterior tibia/fibula
Distal phalanges (toes)
Extend the toes
Tibialis Anterior
Ant. Tibia Top of foot Dorsiflexion of ankle; foot inversion
Gastrocnemius
Lateral and medial heads both originate on femur
Achilles tendon, which inserts on the heel (calcaneus)
Plantar flexes ankle; flexes knee
Soleus Upper fibula Tendon combines with gastroc to form achilles heel.
Plantar flexes ankle
Flexor hallicus longus
Posterior fibula End of big toe (ie the distal aspect)
Flexes big toe
Peroneals Fibula 1st and 5th metatarsals
Plantar flexion; eversion

Muscles of the Thigh and HipMuscle/ Muscle Group
Origin Insertion Action Location
Quadriceps femoris
Iliac spine (pelvis) & proximal femur
Come together as patellar tendon, insert on tibia
Knee extension and hip flexion
Hamstrings Pelvis Head of fibula and tibia
Hip extension; knee flexion; internal knee rotation
Gluteus maximus
Pelvis and lower spine (iliac crest, sacrum, coccyx)
Proximal femur (greater trochanter) and iliotibial tract ( IT band)
Hip extension, external rotation
Gluteus medius & minimus
Lateral pelvis Greater trochanter/ femur
Abduction; internal hip rotation
Hip adductors Distal pelvis Along the femur
Hip/ thigh adduction

Groups: Figure out where each muscle is located- ie anterior, posterior, medial,
lateral
Questions:
While out trail running, Marie steps on a root and experiences an eversion of her ankle. a) What is this injury? (what happens to the sole of the foot) b) Which muscles will be injured? c) Which muscles would have contracted to aid ankle eversion?
Many athletes, especially women, have muscular imbalances between their quadriceps and hamstring muscle groups(quads are often stronger). a) Why are these athletes at a higher risk for injury? b) What joint is most likely to be injured? c) What type of injury might result at this joint?
The gluteus maximus is one of the strongest muscles in the body. a) What would happen to hip/thigh rotation if other muscles do not
compensate for this strength? b) Which muscles are the antagonists to hip extension by the glutius
maximus?

The TrunkMuscle/Group Origin Insertion Action Location
Rectus Abdominus Pubic crest Xyphoid process and inferior ribs
Flex trunk; expiration; “bearing down”
External ObliquesANDTransverse abdominis
Lower 8 ribs Pelvis Flex and rotate vertebrae; compress abdomen during expiration
Quadratus Lumborum
Pelvis and lumbar vert.
Lower rib and upper lumbar vert.
Extends and bends vert. column; helps with breathing
Erector Spinae
Diaphragm Sternum, ribs, lumbar vert.
Central tendon Respiration; anatomical border, separating thoracic and abdominal cavities
Intercostals Inferior of each rib
Superior of each rib
respiration Layers of muscle b/w each rib

Jeff sustained a serious injury to the left side of his trunk. What muscle group(s) are affected? What movements will be compromised?
What could happen if the diaphragm was punctured or torn in half?
A pregnant woman is in a car accident and sustains an injury to her rectus abdominus (baby is fine). What might be the consequences?

Shoulder and BackMuscle/group
Origin Insertion Action Location
Latissimus dorsi
Sacrum, lumbar, thoracic vert
Humerus Adduction, extension, interior rotation of arm
Pectoralis major
Clavicle, sternum, external obliques
Humerus Adduction, flexion, internal rotation of arm
Rotator Cuff (4 muscles)
Scapula Humerus Shoulder stabilization and rotation
Trapezius Base of occipital bone (head); cervical and thoracic vert.
Scapula and shoulder bone bones (acromion, clavicle)
Moves the scapula; extends the neck
Deltoids (anterior, lateral, posterior)
Clavicle, acromion, scapula
Humerus Flexion, extension, abduction and rotation of arm
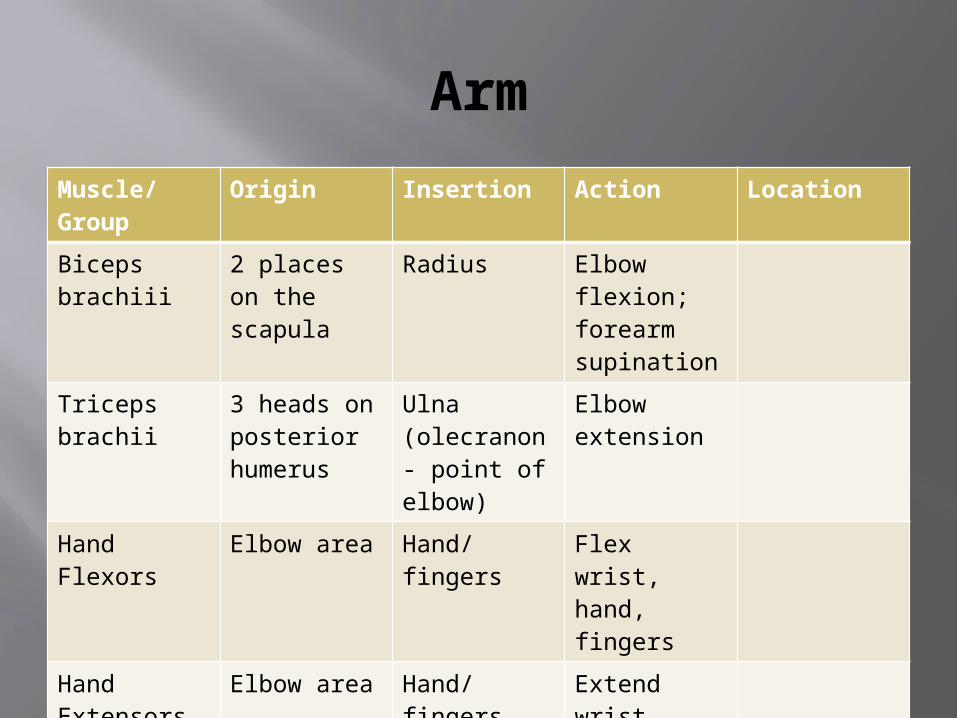
Arm
Muscle/Group
Origin Insertion Action Location
Biceps brachiii
2 places on the scapula
Radius Elbow flexion; forearm supination
Triceps brachii
3 heads on posterior humerus
Ulna (olecranon- point of elbow)
Elbow extension
Hand Flexors
Elbow area Hand/fingers
Flex wrist, hand, fingers
Hand Extensors
Elbow area Hand/fingers
Extend wrist, hand, fingers

Joints
Types: Fibrous joints – no movement- eg sutures of the
skull Cartilaginous joints- some movement- eg between
the vertebrae Synovial joints- lots of movement
6 common types: Ball and socket (eg the hip, shoulder) Gliding (eg foot) Hinge (elbow, knee) Pivot (neck) Saddle (thumb) Ellipsoid (wrist)

Synovial Joints
Separated by a lubricating fluid and cartilage
Joined by ligaments that also help form the joint capsule (surrounds and protects joint)

Joint Injuries http://www.youtube.com/watch?v=9QTCBrefXso
Tendinitis Inflammation of a tendon via irritation due to
overuse/abnormal use Tx- rest, cold, heat therapy, anti-inflammatories
Tears, Sprains, Pulls Tear/pull= injury to muscle Sprain = injury to ligaments and tendons 3 levels of severity: 1st degree injury is mild; 2nd is moderate;
3rd is severe Dislocations
When bone displaced from original position Symptoms:
Joint looks awkward/deformed Painful to touch/move Inability to use joint

Injury Treatment
Recognizing an Injury SHARP
Swelling Heat Altered function Red Pain
Treating RICE
Rest Ice Compression Elevation
NEVER use heat to initially treat an injury Why?

How Can We Protect Our Joints?
strengthen surrounding muscles Stretch muscles Proper conditioning Warm up before exercising Proprioceptive training

Muscles Causing Movement at the Hip Joint Iliopsoas Adductor Muscles Gluteus Maximus Gluteus Medius
Muscles Causing Movement at the Knee Joint Sartorius Quadriceps Group
Rectus Femoris Vastus Muscles
Hamstring Group Biceps Femoris Semimembranosus
Semitendinosus Muscles Causing Movement at the Ankle and Foot Tibialis Anterior Peroneus Muscles Gastrocnemius

















