27
Incision and Closure Youmans Chapter 29
| Date post: | 22-Jan-2018 |
| Category: |
Health & Medicine |
| Upload: | neurosurgery-vajira |
| View: | 251 times |
| Download: | 0 times |

Incision and Closure
Youmans Chapter 29
Outline
• Wound healing
• Indication for antibiotics
• Incision
• Surgical anatomy
• Clinical consideration
• Closure

Wound healing
• Inflammatory phase
• Proliferative phase
• Maturation phase

Inflammatory phaseDay 1-3
• Incision initiate the inflammatory phase
• Factors released from activated platelets, complement components, and prostaglandins induce vasoconstrict hemostasis vasodilatation with increase permeability influx of leukocyte
• PMN are the first cell to migrate into the wound followed by macrophage and mononuclear(Day 2-3)
• Monocytes are essential for normal wound healing by triggering invasion of fibroblasts into the wound and initiating the proliferative or fibroblastic phase of wound healing

Proliferative phaseDay 4-21
• Fibroblasts migrate into the wound at approximately day 4 after injury and deposit disorganized collagen, which produces a scar
• Fibroplasia : restructor tissue– lysis of fibrin platelet– Macrophage,ECM secret growth factor induce fibroblast – Fibroblast create collagen
• Granulation : red from vascular, macrophage, fibroblast• Contraction : rim of wound contracture to center

Maturation phase 21 day – 1-2 Yrs
• ECM remodeling

Indication for antibiotics
• Contaminate wound : 3 hr from time to injury to the time of ATB administration
• Traumatic wound : jet lavage or 35 ml syringe c gauge 18 needle and debridement
• Anatomic location : head and scalp lowest, foot highest rate of infection
• Crush injury have higher rate than linear injury• Preoperative hair removal and its impact on
reducing surgical site infection have controversal

Incision
• Perpendicular to the direction of underlying musculature contracture

Incision
• Perpendicular to the skin and avoid scything or undetermining the adjacent epidermis
• Unequal bite inversion of wound edge inverted scar

Surgical anatomy

Scalp
• Scalp is composd of five layer • outer three layer – skin, subcutaneous fat, galea as a unit

Scalp
• Scalp skin(epidermis and dermis) : 3 mm at vertex to 8 mm at occiput
• Subcutaneous tissue : hair follicle, sweat gland, rich vascular(dense fibrous : manual compression more effective to control bleeding)
• Galea : aponeurotic layer that connect the frontalis to the occipitalis muscle and is contiguous with the temporoparietal fascia laterally

Scalp
• temporoparietal fascia, epicranial aponeurosis, superficial muscular aponeurotic system(SMAS), galeal extension : superficial temporal a. and vein
Flap
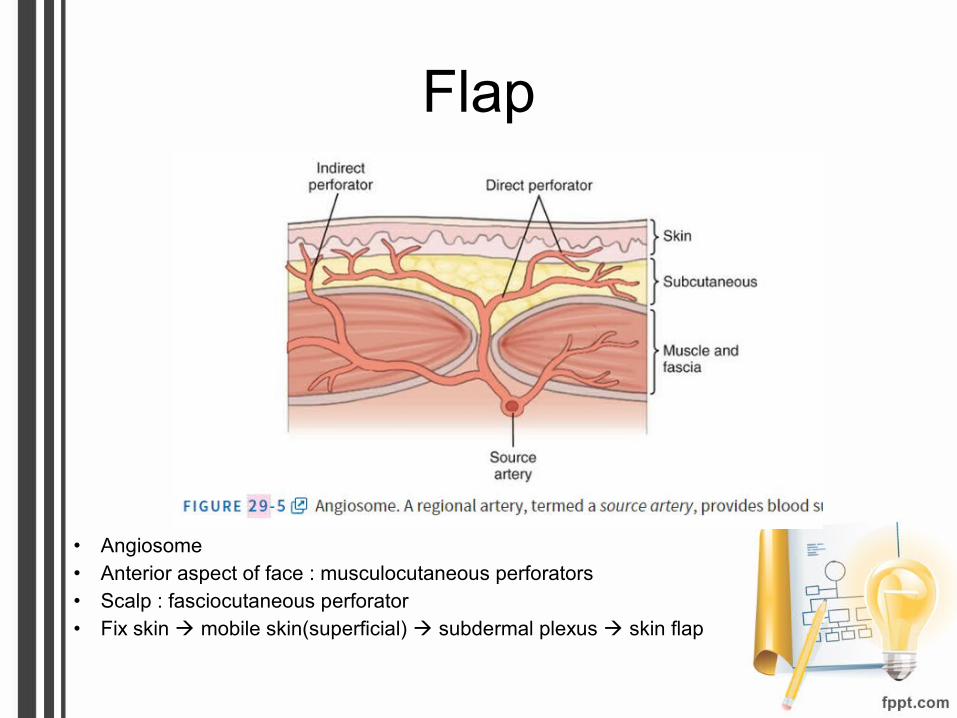
• Angiosome• Anterior aspect of face : musculocutaneous perforators• Scalp : fasciocutaneous perforator• Fix skin mobile skin(superficial) subdermal plexus skin flap

Flap
• Converse scalp flap : capture two territories(superficial temporal a., supra orbital)• McGrejor flap : capture four territories which often result in tip necrosis
Flap
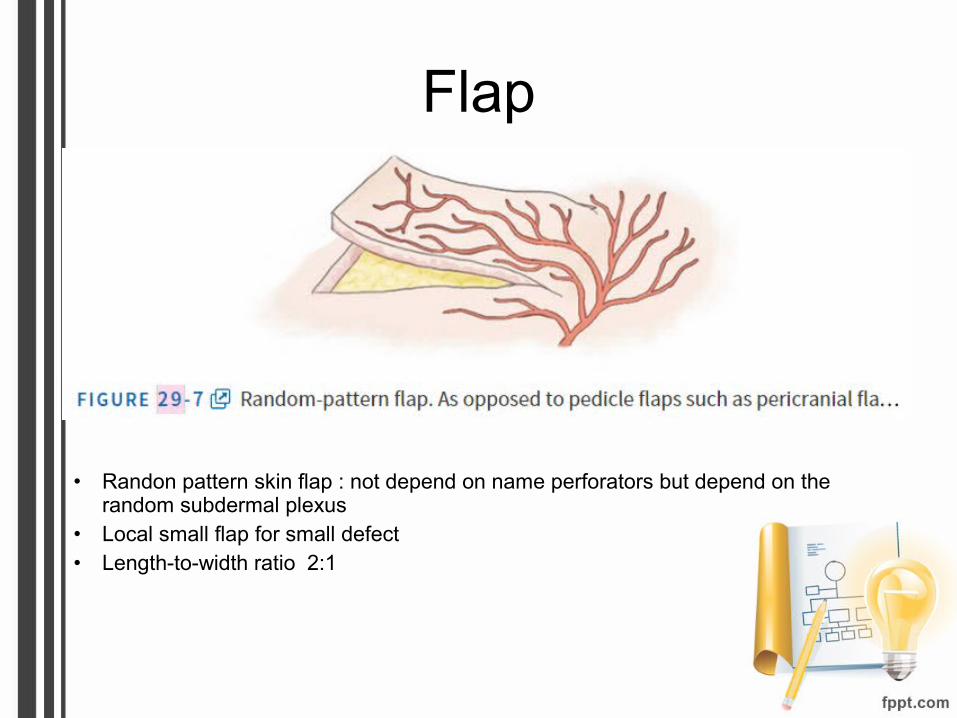
• Randon pattern skin flap : not depend on name perforators but depend on the random subdermal plexus
• Local small flap for small defect• Length-to-width ratio 2:1
Blood supply of scalp
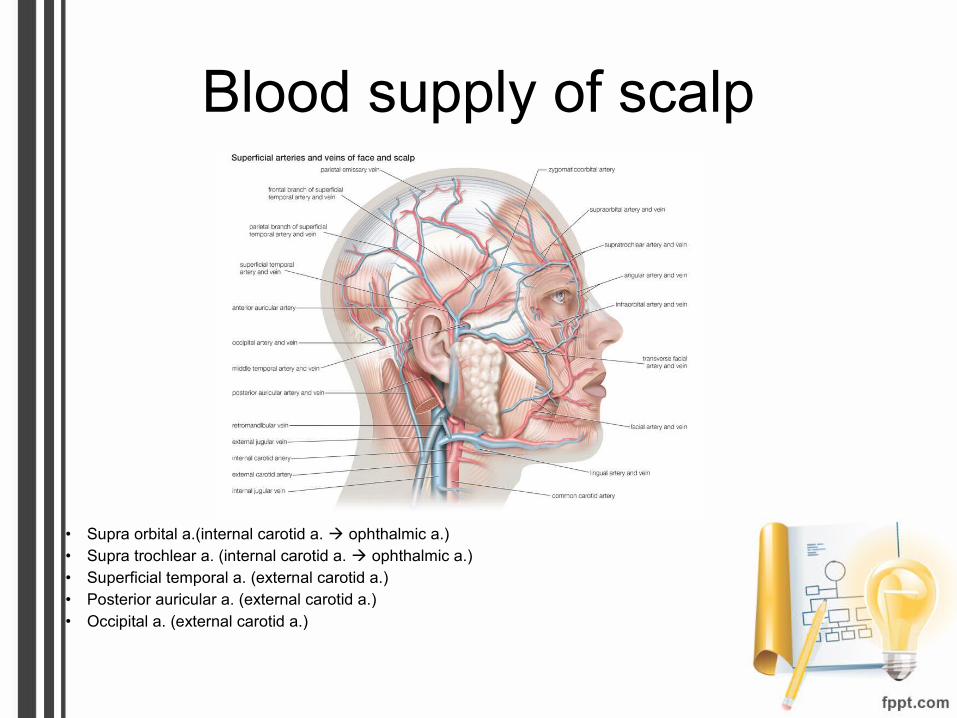
• Supra orbital a.(internal carotid a. ophthalmic a.)• Supra trochlear a. (internal carotid a. ophthalmic a.)• Superficial temporal a. (external carotid a.)• Posterior auricular a. (external carotid a.)• Occipital a. (external carotid a.)

Blood supply of scalp
• Anterior : supraorbital and supratrochlear a. – Supraorbital a. exit through supraorbital
notch,superficial to orbital rim 1.5 cm and lateral to midline 3 cm
– supratrochlear a.,1 cm superior to medial palpebral ligament, 1.5 cm lateral to midline
• Posterior territory : medial and two lateral occipital a.,5 cm lateral to occipital protuberance

Blood supply of scalp
• Posterolateral territory : posterior auricular a.,2 cm inferior to the auditory canal
• Lateral scalp territory : frontal and parietal branch of the superficial temporal a.(superficial temporal a. give branch to middle temporal a.the blood supply to the temporalris muscle and deep temporal fascia)

Facial nerve
• Facial n. lies within a small fat pad between the layers of the deep temporal fascia,posterior to the superficial temporal a. and vein,at level of zygomatic arche
• 2.5 cm anterior to the tragus• 1.5 cm lateral to the orbital rim• Lie within deep temporalis fascia• Should be preserve when elevating a pericarnial flap
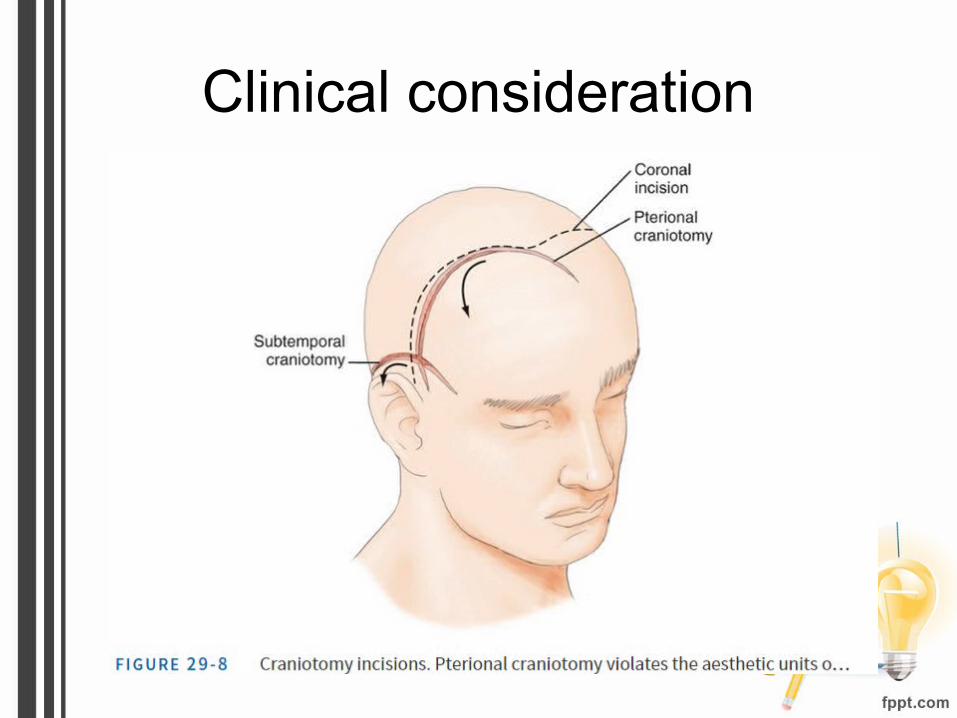
Clinical consideration

Frontosphenotemporal or pterional craniotomy
• anterior aneurysms and parasellar, sphenoid and anterior skull base tumour
• Incision from the roof of zygoma to the linea temporalis and anteriorly to the center of forhead
• Five aesthetic part unit : two temporal, two brow and one central component

Frontosphenotemporal or pterional craniotomy
• Coronal incision,providing better exposure and cosmetic result because it preservs all the aesthetic units of the head.
• Longer incision, necessitate operative time
• Should be preserve frontal branch of the facial nerve
• Detach of the muscle from it superior insertion result in retracton of m. inferiorly and muscle wasting
• Leaving a cuff of temporalis m. superiorly attached to skull to provide, reapproximating m. fiber and resultant in muscle wasting
Subtemporal craniotomy
• Hoarseshoe-shape flap• Tentorial, clivus and basilar a lesion• Becareful, superficial temporal a. and posterior
auricle a.
Midline suboccipital craniotomy
• Inconspicious scar, advantage of vascular between two bellies
• Reliable closure is complicated by many factor – Radiation
– Embolization
– Previous scalp surgery
– > 60 Years

Closure
• Primary closure : simple, atraumatic, noncontaminated wound
• Goal– Obliterate dead space
– Distribute tension along deep suture line
– Maintain suture strength until tissue tension strength adequate
• Interrupted stitch,it avoid compromising the vessel within the galea suppling the scalp but longer operative time
• Metallic staples may used in region of compromised vascularity to improve potential
Closure
Monofilament Multifilament
Infection less more
Tension Less tension More tension
Galea,scalp Nylon

















