28
Preoperative patient survey Aspirin?
| Date post: | 06-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | shen-chih-wang |
| View: | 164 times |
| Download: | 0 times |
Preoperative patient survey
Aspirin?

Nightmare
Can Aspirin improve mortality
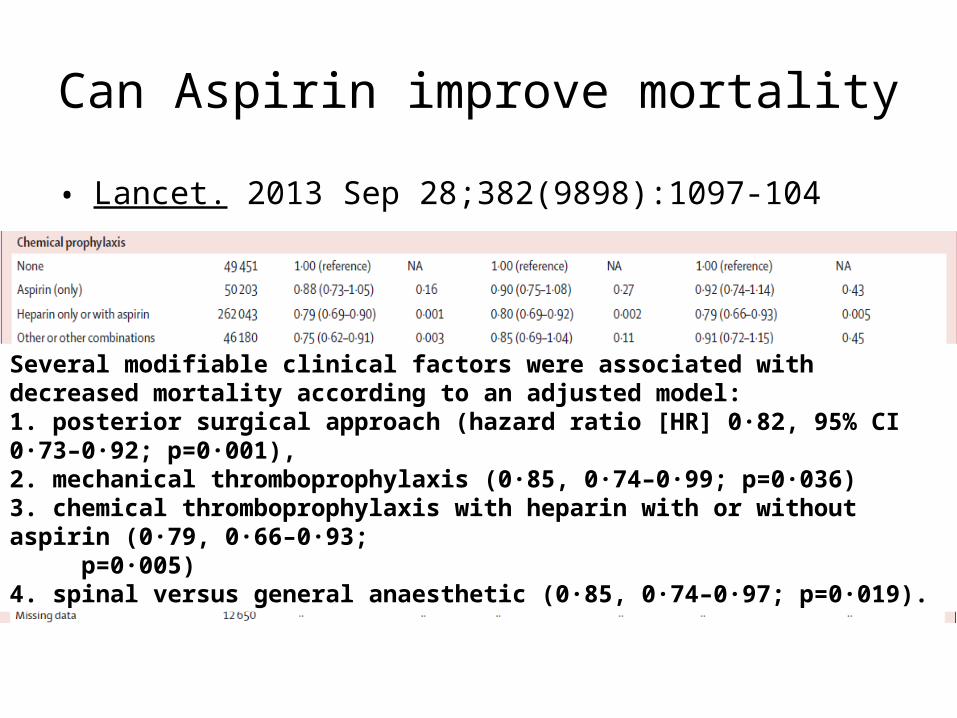
• Lancet. 2013 Sep 28;382(9898):1097-104
Several modifiable clinical factors were associated with decreased mortality according to an adjusted model: 1. posterior surgical approach (hazard ratio [HR] 0·82, 95% CI 0·73–0·92; p=0·001),2. mechanical thromboprophylaxis (0·85, 0·74–0·99; p=0·036)3. chemical thromboprophylaxis with heparin with or without aspirin (0·79, 0·66–0·93; p=0·005)4. spinal versus general anaesthetic (0·85, 0·74–0·97; p=0·019).

Guidelines from neurology
• Clinicians managing antithrombotic medications periprocedurally must weigh bleeding risks from drug continuation against thromboembolic risks from discontinuation. – Stroke patients undergoing dental procedures should routinely
continue aspirin (Level A). – Stroke patients undergoing invasive ocular anesthesia, cataract
surgery, spinal/epidural procedures, and carpal tunnel surgery should probably continue aspirin (Level B).
• Neurology. 2013 May 28;80(22):2065-9.

Choice of intraoperative lab test
INR, plt count or TEG

Thromboelastography

Thromboelastogram

Thrombelastography (TEG) or thromboelastometry(ROTEM) to monitor haemotherapy versus usual care in patients with massive
transfusion
Cochrane Database Syst Rev. 2011 Mar 16;(3):CD007871

Method: monitoring frequency
Surgery Baseline
CPB Re-warm After Protamine
ICU 6hr after CPB
24hr after CPB
Ak 2009
Elective CABG
● ● ● ● ● ●
Avidan 2004 ● ● ● ● (if bleeding >100ml/hr)
Girdauskas 2010
Aortic surgery with circulatory arrest
● (at 32 )℃Transfused with protamine
● ( If abnormal bleeding, 15min after transfusion)
● (if bleeding > 200ml in the 1st hour and >100ml/hr thereafter)
Nuttal 2001Elective cardiac surgery
● (repeat test if bleeding persisted)
Royston 2001 Cardiac
surgery ● ● ● ( 35 )≧ ℃ ●
Shore-Lesserson
1999Valve or aortic replacement
● ● ● (Transfusion was prescribed only in the presence of bleeding)
Westbrook 2009 Cardiac
surgery ● ●( 36.5 )≧ ℃ ● (Repeat tests in 3 hourly cycles if bleeding
> 60ml/0.5hr)

Avidan 2004
• Comparison of structured use of routine laboratory tests or nearpatient assessment with clinical judgement in the management of bleeding after cardiac surgery.– If there was excessive bleeding: Fresh frozen plasma (4 units) was
given when thromboelastography suggested clotting factor deficiencies (tissue factor R clotting time >10 min) or INR or APTT ratio were more than 1.5 times the control value .
– If there was excessive bleeding: A platelet pool was transfused when a prolonged PFA-100 channel closure time (ADP channel >120s, epinephrine channel > 170s) or the platelet count was less than 50x109/l.
• British Journal of Anaesthesia 92 (2): 178-86 (2004)

Shore-Lesserson 1999
• All intraoperative results of the TEG and laboratory coagulation tests were interpreted by an anesthesiologist investigator not directly involved with the patient’s care. The recommended therapy according to the patient’s group assignment was communicated to the anesthesiologist and surgeon by this investigator, as appropriate.
• Celite-activated TEG– Celite and kaolin produce differing activated clotting times during CPB
under aprotinin therapy.• Anesth Analg 1999;88:312–9
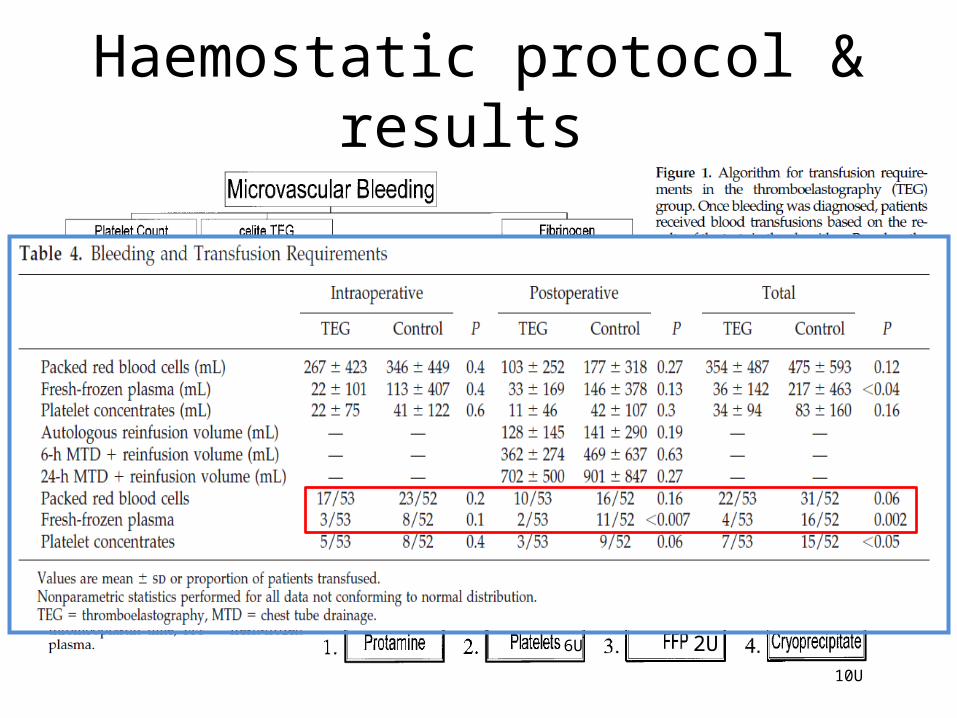
Haemostatic protocol & results
2U6U
10U
2U6U10U

Results Surgery Results
Ak 2009
Elective CABGLess FFP, platelet and total allogenic units transfused.
Avidan 2004 No difference in PRBCs and blood components use between the two algorithm-guided groups.
Girdauskas 2010Aortic surgery with circulatory arrest
Transfusion of allogeneic blood was significantly reduced in the thromboelastometry group. Postoperative blood loss and re-exploration rate were similar.
Nuttal 2001 Elective cardiac surgery Less FFP use, chest tube drainage and reoperation rate
Shore-Lesserson 1999 Valve or aortic
replacementIntraoperation: Less FFP use and fewer platelet transfusion. Postoperation: less transfusionNo difference in chest tube drainage
Westbrook 2009Cardiac surgery
TEG-based management reduced total product usage by 58.8% in the study group but this was not statisticallysignificant. This was associated with a statistically insignificant trend towards better short-term outcomes.

Authors’ conclusion
• There is weak to moderate evidence to support the use of TEG or ROTEM in the cardiac surgery.
• Despite signs of reduced bleeding, we did not find a statistically significant effect of TEG and ROTEM on mortality or other clinically relevant outcomes.

Confounding factors
• Time point– Regular vs. Bleeding
• Transfusion trigger– Prophylaxis vs. Bleeding– Indication for transfusion– Units use to correct coagulopathy
• What is your ideal protocol for monitoring and transfusion therapy?
Transfusion of red blood cell (RBC)
RBC use increase mortality
• Retrospective studies– Red blood cell transfusion in patients having cardiac surgery is strongly
associated with both infection and ischemic postoperative morbidity, hospital stay, increased early and late mortality, and hospital costs.
• Circulation.2007;116:2544-2552.
– There is a dose-dependent adverse effect of intraoperative blood transfusion. Caution should be used with intra-operative transfusions for mildly hypovolemic or anemic patients.• transfusion of seemingly small and possibly discretionary amounts of intraoperative
PRBCs is associated with adverse surgical outcomes.• Patients who received more than 4 units of PRBCs within 48 hours before the
operation were excluded• Arch Surg. 2012;147(1):49-55

Normovolemic hemodilution

Protocol
• 17% ± 2% of the circulating volume was removed– by gravity through a large-bore catheter (8.5F) placed into the internal
jugular vein and was collected into sterile bags containing citrate phosphate dextrose (Fenwal; Baxter Healthcare Corp., Irvine, CA) by using a blood mixer and balance system (Easy-mix V3; Baxter).
– During blood withdrawal, 4% succinylated gelatin in 0.9% NaCl (Eufusin; Fresenius Kabi Potenza S.r.l., Tito Scalo, Italy) was infused at a 1:1 ratio.
• Tranexamic acid as an IV bolus of 1 g 20 min before sternotomy, followed by a continuous infusion of 400 mg/h until the end of surgery.
• Anesthesia & analgesia 2004;98(5): 1217-1223
National Blood Authority recommendations (II)
• RBC transfusion should not be dictated by a haemoglobin ‘trigger’ alone, but should be based on assessment of the patient’s clinical status. In the absence of acute myocardial or cerebrovascular ischaemia, postoperative transfusion may be inappropriate for patients with a haemoglobin level of >8
g/dL.
Monitoring for perfusion of vital organs
Insufficient literature to evaluate efficacy.

Our daily practice
• Brain: cerebral oximetry– Self-pay, doubtful clinical value.
• Heart: 5 lead ECG, TEE– TEE category 1 indication: hemodynamic unstable
• Lung: PaO2/FiO2
– Injury or distress
• Kidney: urine output– Kidney injury biomarkers: Beta-N-acetyl-beta-D-glucosaminidase
(NAG), neutrophil gelatinase-associated lipocalin (NGAL) and alpha-1 microglobulin.
• ScvO2: ?

Massive transfusion
Blood loss Blood product use in certain periodVital sign unstable


Borgman et al. J Trauma 2007
• a retrospective chart review of massive transfusion at a US Army combat support hospital.– Massive transfusion was defined as >10 RBC units in 24 h.
• From this nonrandomized, retrospective analysis, the authors concluded that a higher ratio of plasma to erythrocytes contributed to a better outcome.

Survivor bias
• Survivor bias is associated with having survived long enough to receive a particular therapy.

Conclusions
• The immediate benefits of plasma transfusion only outweigh the risks when a coagulopathy is severe.
• However, overall risks increase with escalating plasma exposure, thus affecting patient safety.
• Point-of-care coagulation monitoring can be used to avoid excessive allogeneic blood transfusions including plasma and its associated complications.
• British Journal of Anaesthesia 113 (S2): ii3–ii8 (2014)
不要猶豫喊急找

Thanks for your attention