11
1 1 Il trapianto renale a Bergamo Eliana Gotti 23 Dicembre 1954, ore: 8.00 Ospedale Peter Bent Brigham di Boston

1
1
Il trapianto renale a Bergamo
Eliana Gotti
23 Dicembre 1954, ore: 8.00Ospedale Peter Bent Brigham di Boston

2
1.223,624 ORGAN TRANSPLANTS PERFORMED WORLDWIDE UP TO 2009
KidneyLiverHeartLungKidney/pancreasPancreas/IsletHeart/lungIntestine
873,538194,41987,82330,09524,0938,2434,476
937
Transplants n°
Cecka et al., Clinical Transplants, 2010
1
Kidney transplantation
In patients with end stage renal diseasesuccessful renal allotransplantation improves
the quality of life and increases survival ascompared with long-term dialysis treatment
Wolfe et al, N Engl J Med 1999

3
5
THE GAP BETWEEN KIDNEY TRANSPLANT DEMAND AND SUPPLY
US 84,766
Waiting list*
UNOS.org, 2010
Transplant* Death on waiting list °
(n) (n) (n)
16,829 5,251
Italy 6,808 1,651 102
* By December 31, 2009. °During 2009CNT, 2010
CAUSE DI INSUFFICIENZA RENALE CRONICA
• Diabete mellito 24 %
• Glomerulonefriti 11.8 %
• Pielonefriti /reflusso 7.8 %
• Malattia Policistica dell’adulto 7.5 %
• Malattia renovascolare 6.9 %
• Ipertensione 6 %
• Altre cause 15.6 %
• Diagnosi incerta 20.7 %

4
Controindicazioni relative a trapianto
• Età > 65
• Malattie cardiovascolari
• Obesità
• Infezione da HIV
• Pregressa neoplasia
• Epatite cronica B/C
Trapianto renale
- Da donatore: - cadavere- vivente
- Trapianto di rene singolo / doppio
- Trapianto pre-emptive

5
1
Trapianto renale
THE IMMUNOSUPPRESSIVE ARMAMENTARIUM TO CONTROL GRAFT
REJECTION1954
1960
1965
1970
1980
1990
1995-2005
None
Azathioprine
Steroids
Anti-T cell Abs
Cyclosporine
OKT3 mAb
MizoribineDeoxyspergualinTacrolimusMycophenolate mofetil/myforticBasiliximab/DaclizumabSirolimus/everolimusFTY720

6
Gjertson et al., 1992
% 1
-Yea
r Gra
ft S
urvi
val
100
80
60
40
20
075 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91
Year of Transplant (1975-1990)
CsA
55-60
35-40 CsA + ST + AZA ‘83
ST + AZA ‘77
Acute rejection (%)
1
Analysis of UNOS data on patients with functioning kidney 1 year post transplant
Hariharan et al., N Eng J Med, 2000
GRAFT SURVIVAL AFTER RENAL TRANSPLANTATION IN THE PERIOD 1988-2004
OPTN website, 2009
years of transplant
Pro
ject
ed m
edia
n ha
lf-lif
e(y
ears
)
88 89 90 91 92 93 9594
Cadaver donor30
20
10
0
8
11
2004
13.8
1

7
THE MAINTENANCE IMMUNOSUPPRESSION
Maintenance immunosuppression is best achieved using combination of immunosuppressive agents
Combination therapy aims to minimize the side-effects of any single drug whilst targeting multiple steps in T-cell activation
Triple-drug regimen
Corticosteroids Calcineurininhibitor
Antiproliferativeagent
CALCINEURIN INHIBITOR NEPHROTOXICITY IS VIRTUALLY UNIVERSAL BY 10 YEARS AFTER TRANSPLANTATION
Nankivell et al., N Engl J Med, 2003
120 type 1 diabetic patients with kidney-pancreas transplant
961 kidney transplant biopsy: Tx to 10 years thereafterTriple-therapy immunosuppression: CsA or tacrolimus, Aza or MMF, prednisolone
100
60
0
80
40
1 yr
CN
-inhi
bito
r nep
hrot
oxic
ity(%
)
20
5 yrs 10 yrs
76.4
93.596.8
Post-Tx

8
Corticosteroids and calcineurin inhibitors are effective in reducing the incidence of acute rejection, but are a major cause of morbidity and mortality
As a result, a number of clinical trials have examined whether steroids or calcineurin inhibitors can be safely withdrawn after renal transplantation
One of the major questions remaining in clinical transplantation is whether it will be possible to induce states of true tolerance with little or no long-term drug therapy
…ideally one would like to alter the host’s initial contact with the graft to promote a state of donor-specific unresponsiveness
Carpenter, N Engl J Med, 1993
THE TARGET: TRANSPLANTATION TOLERANCE
9
17
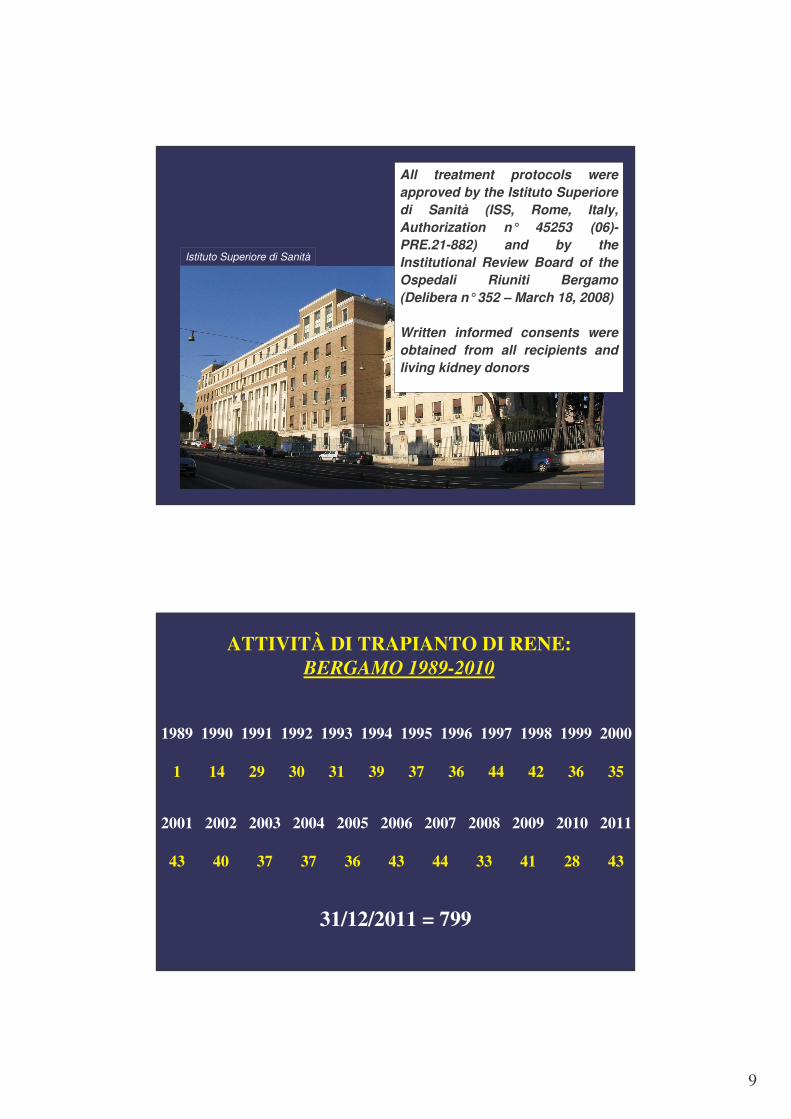
All treatment protocols were approved by the Istituto Superiore di Sanità (ISS, Rome, Italy, Authorization n° 45253 (06)-PRE.21-882) and by the Institutional Review Board of the Ospedali Riuniti Bergamo (Delibera n°352 – March 18, 2008)
Written informed consents were obtained from all recipients and living kidney donors
Istituto Superiore di Sanità
17
ATTIVITÀ DI TRAPIANTO DI RENE:BERGAMO 1989-2010
1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000
1 14 29 30 31 39 37 36 44 42 36 35
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
43 40 37 37 36 43 44 33 41 28 43
31/12/2011 = 799

10
Attività di Trapianto a Bergamo
- Da donatore vivente: 29
- Doppio trapianto: 68
- Trapianto combinato- cuore-rene: 5- fegato-rene: 30- rene-pancreas: 7
20
CURVA DI SOPRAVVIVENZA DEL TRAPIANTO DI RENE (END-POINT: DIALISI)
0
50
100
0 10 20Anni
Sop
ravv
iven
za d
elgr
aft(
cens
urat
a pe
r la
mor
te) %
UNOS registry37 %

11
6 12 18 24 30 360
102030405060708090
100
Sop
ravv
iven
za
dell’
orga
no
trapi
anta
to(%
)
p=0.83
0
Trapianto singolo o doppioBiopsia pre-trapianto: SIDonatore > 60 anni
Trapianto singolo Biopsia pre-trapianto: NODonatore < 60 anni
6 12 18 24 30 360
102030405060708090
100
p=0.02
Trapianto singolo o doppioBiopsia pre-trapianto: SIDonatore > 60 anniTrapianto singolo Biopsia pre-trapianto: NODonatore > 60 anni
Sop
ravv
iven
za
dell’
orga
no
trapi
anta
to (
%)
Mesi dal trapianto0
Remuzzi et al., N Engl J Med, 2006

















