58
1
| Date post: | 22-Dec-2015 |
| Category: |
Documents |
| Upload: | gerald-knight |
| View: | 216 times |
| Download: | 1 times |

1

Acute RhinosinusitesSAYED MOSTAFA HASHEMI MD
FEBRUARY 2015

3ANATOMY AND PHYSIOLOGY
— Humans have four pairs of sinuses named for the bones of the skull that they pneumatize The maxillary, ethmoid (divided into anterior and posterior cells), frontal, and sphenoid sinuses are air-containing spaces that are lined by pseudostratified, columnar epithelium bearing cilia. The sinus mucosa contains goblet cells, which secrete mucus that aids in trapping inhaled particles and debris.

Anatomy

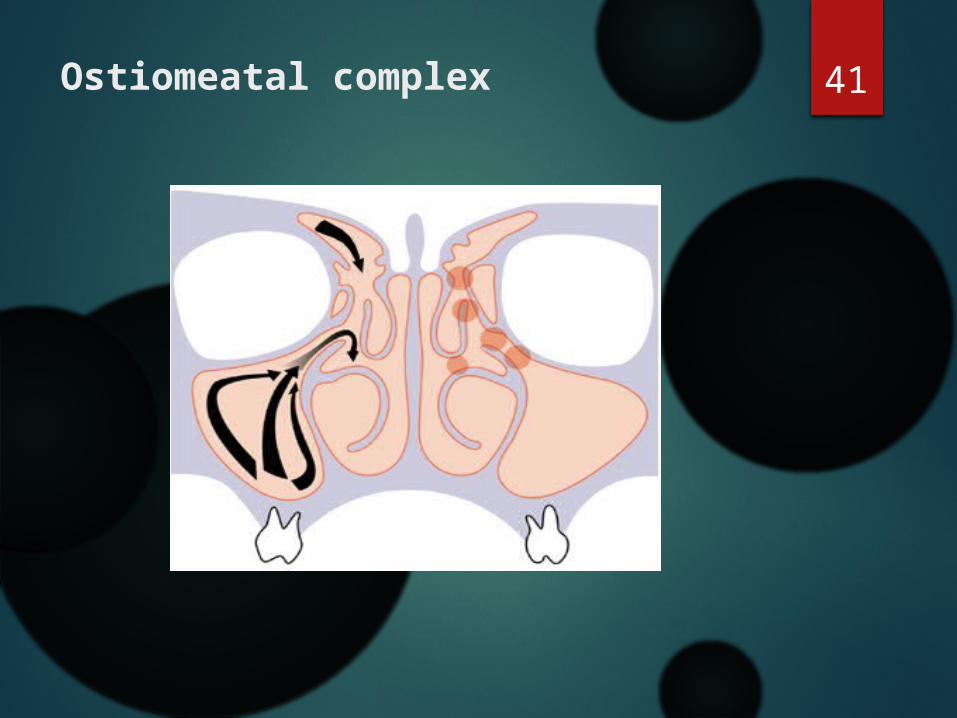
5Ostiomeatal complex
6INTRODUCTION —
Rhinosinusitis is defined as symptomatic inflammation of the nasal cavity and paranasal sinuse
The term "rhinosinusitis" is preferred to "sinusitis" since inflammation of the sinuses rarely occurs without concurrent inflammation of the nasal mucosa [1].

7

8

9Recurrent acute rhinosinusitis
- four or more episodes of ARS per year, with temporary symptom resolution [2].

10
plain sinus radiography
The sensitivity and specificity of plain sinus radiography is poor for detecting mucosal thickening of the paranasal sinuses (76 and 79 percent, respectively)
The high false negative rate is attributable to poor visualization of the ethmoid sinuses in plain films,
The high false positive rate to artifact and the inability to distinguish polyps and nasal masses from fluid or mucosal edema.

11
Sinus aspiration
cultures are rarely performed unless there has been a failure of treatment
sinus aspiration is indicated in severe toxic illness, acute illness not responsive to antibiotics within 72 hours, immunocompromised patients, supportive complications
endoscopically guided middle meatus swab correlates fairly well with sinus aspirate

12

13

14
ACUTE RHINOSINUSITIS:
acute rhinosinusitis lasts for up to 4 weeks1 and results from
interactions between a predisposing condition such as allergic
rhinitis, immune deficiency, or inflammatory response from a
viral infection.
The inflammation then leads to edema and obstruction of the
sinus ostium, the normal ventilation and drainage of the sinus is
then impaired, and a secondary bacterial infection ensues (Fig.
46-1).

15
Pathophysiology
Purulent sinusitis can occur when ciliary clearance of sinus secretions decreases or when the sinus ostium becomes obstructed, which leads to retention of secretions, negative sinus pressure, and reduction of oxygen partial pressure.

16
Pathophysiology
This environment is then suitable for growth of pathogenic organisms.
Factors that predispose the sinuses to obstruction and decreased ciliary function are allergic, nonallergic, or viral insults, which produce inflammation of the nasal and sinus mucosa and result in ciliary dysmotility and sinus obstruction.
17
PATHOGENESIS of ABRS
With colds and influenza-like illnesses, viscous fluid frequently accumulates in the sinuses from exocytosis of mucus from goblet cells in the sinus mucosa [6] and possibly as the result of nose blowing.
ABRS occurs when bacteria secondarily infect the inflamed sinus cavity. Though usually occurring as a complication of viral infection

18

19
Conversion of AVRS to ABRS
it is generally not possible to distinguish AVRS from ABRS in the first 10 days of illness based upon history, examination, or radiologic study.
The diagnosis of ABRS is usually clinical, since sinus aspirates for culture are not readily obtainable.

Conversion of AVRS to ABRS Persistent symptoms or signs of ARS lasting 10 or more
days with no clinical improvement
Onset with severe symptoms (fever >39°C or 102°F and purulent nasal discharge or facial pain) lasting at least three following days at the beginning of illness
Onset with worsening symptoms following a viral upper respiratory infection that lasted five to six days and was initially Improving
immunocompromised patients

21
Only a small percentage (approximately two percent) of viral rhinosinusitis is complicated by acute bacterial sinusitis. Uncomplicated viral rhinosinusitis usually resolves in seven to ten days.

22
EPIDEMIOLOGY
— The average adult has from two to three colds and influenza-like illnesses per year and the average child six to 10
Approximately 0.5 to 2 percent of colds and influenza-like in adults and 6-13% in children
complicated by acute bacterial sinusitis in adults

23
Microbiology
24

25
.
TREATMENT:

26
Diagnosis and antibiotic treatment base on the IDSA guidelines
“onset with ‘persistent’ symptoms or signs compatible with acute rhinosinusitis lasting for 10 days or longer without any evidence of clinical improvement;
onset with ‘severe’ symptoms or signs of high fever 39°C or higher and purulent nasal discharge or facial pain lasting for at least 3 to 4 days at the beginning of illness; onset with ‘worsening’ symptoms or signs such as new onset of fever, headache, or increase in nasal discharge following typical viral [upper respiratory infection] symptoms that lasted 5 to 6 days and were improving (i.e., ‘double sickening’).” The IDSA also suggests that antibiotics should be begun once these criteria are met.

27
The recent IDSA recommendations now state that amoxicillin-clavulanate, rather than amoxicillin alone, is recommended as empiric antimicrobial therapy for ABRS in both adults and children and that “high-dose” amoxicillin-clavulanate is recommended for children and adults with ABRS who :1) are from geographic regions with high endemic rates
of penicillin nonsusceptible Streptococcus pneumoniae,
2) have severe infection, 3) were recently hospitalized or used antibiotics within
the past month, or 4) are immunocompromised.
28
Macrolides (clarithromycin and azithromycin) are not recommended for empiric therapy because of high rates of resistance with S. pneumoniae (~30%), and trimethoprim-sulfamethoxazole is not recommended for empiric therapy because of high rates of resistance among both S. pneumoniae and H. influenzae (~30% to 40%).
A good alternative regimen to amoxicillin-clavulanate for initial empiric antimicrobial therapy of ABRS is doxycycline in adults (not recommended in children) because it remains highly active against respiratory pathogens and has excellent pharmacokinetic and pharmacodynamic properties.
Because rates of resistance with S. pneumoniae vary, second- and third-generation oral cephalosporins are not currently recommended for empiric monotherapy of ABRS; however, for patients from geographic regions with high endemic rates of penicillin-nonsusceptible S. pneumoniae, combination therapy that includes clindamycin and a third-generation cephalosporin (cefixime or cefpodoxime) is recommended.

29
In cases of type I hypersensitivity allergy to penicillin or suspected allergy, doxycycline or a respiratory fluoroquinolone(levofloxacin or moxifloxacin) may be recommended as alternative agents for empiric initial antimicrobial therapy in adults. In children, levofloxacin is recommended when there is a history of type I hypersensitivity to penicillin.
. Treatment should be for 5 to 7 days in adults and for 10 to 14 days in children based on current literature.

Treatment failure
— Treatment failure is defined as progression or worsen after 72 or failure to improve after 3-5 days of therapy.
Patients who fail first-line therapy require alternative antibiotic selection. Ideally, an endoscopically-guided culture could be performed to redirect antibiotic therapy. If no material is available on endoscopy for culture, a broader antibiotic choice can be empirically started and monitored for improvement. high-dose amoxicillin-clavulanate (4 grams/250 milligrams per day) have been recommended
A CT scan of the sinuses may be performed if symptoms worsen or fail to improve, to verify that symptoms are in fact due to acute sinusitis, and not to concomitant allergy or other noninfectious etiologies.
30

31
Saline irrigation
— Mechanical irrigation with buffered, physiologic, or hypertonic saline may reduce the need for pain medication and improve overall patient comfort, particularly in patients with frequent sinus infections.
It is important that irrigants be prepared from sterile or bottled water, as there have been reports of amebic encephalitis due to tap water rinses [13]. Instructions for preparing a rinse solution are shown in a table (tabl

32
Topical glucocorticoids
— The theoretic mechanism of action for intranasal glucocorticoids (corticosteroids) is a decrease in mucosal inflammation that allows improved sinus drainage
intranasal glucocorticoids are likely to be most beneficial for patients with underlying allergic rhinitis

33
Topical decongestants
— The use of topical decongestants, such as oxymetazoline, may provide a subjective sense of improved nasal patency. If used, topical decongestants should be used sparingly (no more than three consecutive days) to avoid rebound congestion
Topical decongestants are suggested for symptomatic relief in the treatment of AVRS and 2012 guidelines advise that they are not helpful in patients with ABRs
oral decongestants are not helpful in patients with ABRS

34
oral decongestants
oral decongestants are not helpful in patients with ABRS
When eustachian tube dysfunction is a significant confounding factor in AVRS, a short course (three to five days) of oral decongestants may be warranted.
Oral decongestants should be used with caution in patients with cardiovascular disease, hypertension, or benign prostate hypertrophy due to systemic adverse effects with oral alpha adrenergic preparation

35
Antihistamines
— Antihistamines are frequently prescribed for symptom relief due to their drying effects; however, there are no studies investigating their efficacy for this indication
Additionally, over-drying of the mucosa may lead to further discomfort. Antihistamines have side effects (drowsiness, xerostomia),
Their use for the treatment of acute sinusitis is not recommended
36
Indications for urgent referral
— Patients with high fever, acute facial pain, swelling, and erythema should be treated for acute bacterial rhinosinusitis, even if symptoms have not been present for seven days.
Patients with high fevers and severe headache warrant immediate evaluation and probable imaging.

37

38
•Chronic Rhinosinusitis

39

40
Chronic rhinosinusitis
Chronic rhinosinusitis is a group of disorders characterized by inflammation of the mucosa of the nose and paranasal sinuses of at least 12 consecutive weeks’ duration.
Patients with CRS may have intermittent acute flare-ups; in such cases, the disorder is called acute exacerbation of chronic rhinosinusitis(AECRS)
41
Ostiomeatal complex

EPOS Management Algorithm: Adult Chronic Rhinosinusitis*Primary Care




46
Pathogenesis
Ostia obstruction creates increasingly hypoxic environment within sinus
Retention of secretion results in inflammation and bacterial infection
Secretion stagnate, obstruction increases, cilia and epithelial damage become more pronounced

47
COMPLICATIONS:
Most episodes of ABRS respond to appropriate medical treatment. However, ARS can become complicated by extension to an adjacent structure. These infections can have devastating outcomes, including blindness, neurologic morbidity, and death. These complications are rare and are estimated to occur once in every 95,000 pediatric hospital admissions.

48
Complications
Orbital complication:Spread by direct extension via osseous structures or indirectly via valveless venous plexuse
Orbital complications more common in children than adults
Most common is medial subperiosteal abscess
Intracranial: More common in adolescents/adults Include meningitis (most common), epidural abscess,
subdural abscess, intracerebral abscess, cavernous sinus thrombosis

49
Classification
• Group I complications include patients with preseptal cellulitis or inflammatory edema superficial to the tarsal plates and orbital septum.
• Group II patients have orbital or postseptal cellulitis in which there is edema of the orbital contents without a discrete abscess.
• Group III patients have a subperiosteal abscess adjacent to the lamina papyracea and under the periosteum of the medial orbit.
• Group IV patients have an orbital abscess or a discrete collection within the orbital tissue.
• Group V complication is when a patient has a cavernous sinus thrombosis.
50
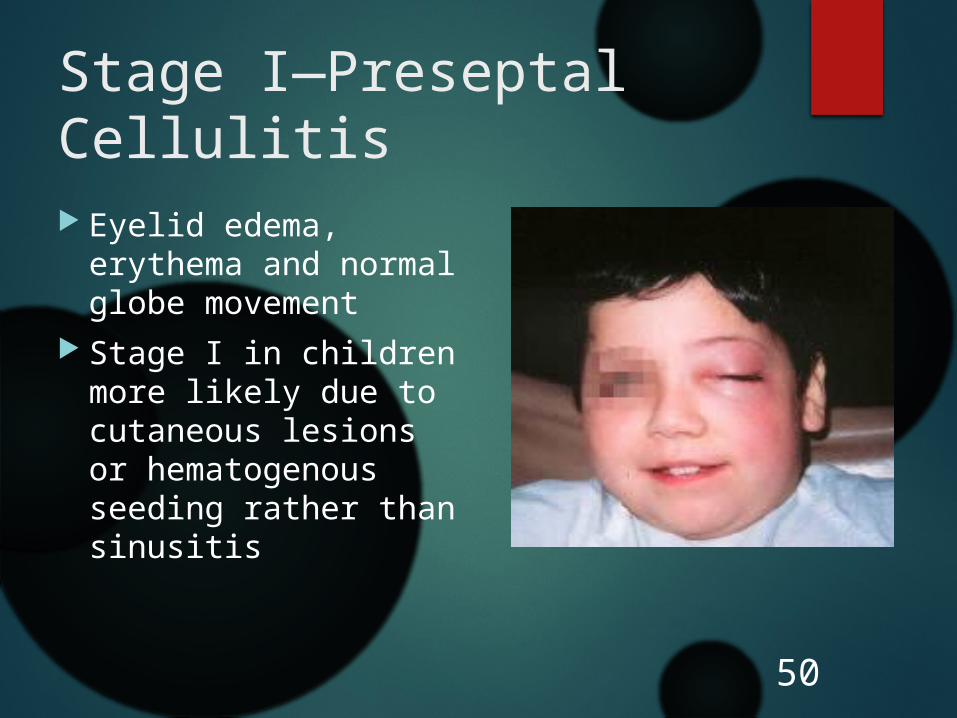
Stage I—Preseptal Cellulitis
Eyelid edema, erythema and normal globe movement
Stage I in children more likely due to cutaneous lesions or hematogenous seeding rather than sinusitis
51
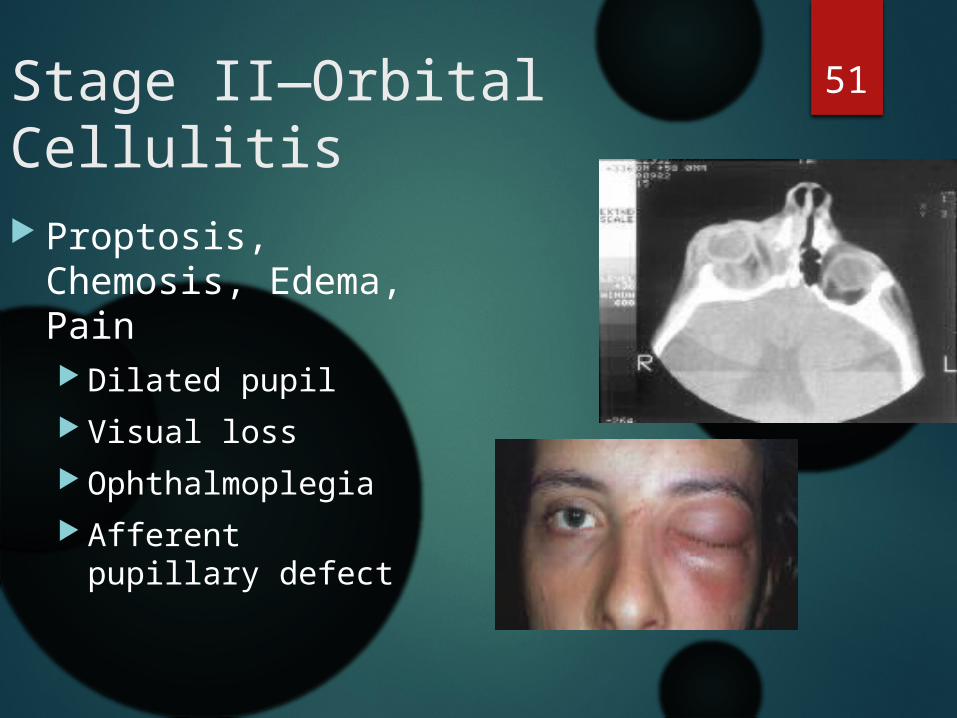
Stage II—Orbital Cellulitis
Proptosis, Chemosis, Edema, Pain Dilated pupil Visual loss Ophthalmoplegia Afferent pupillary
defect
52
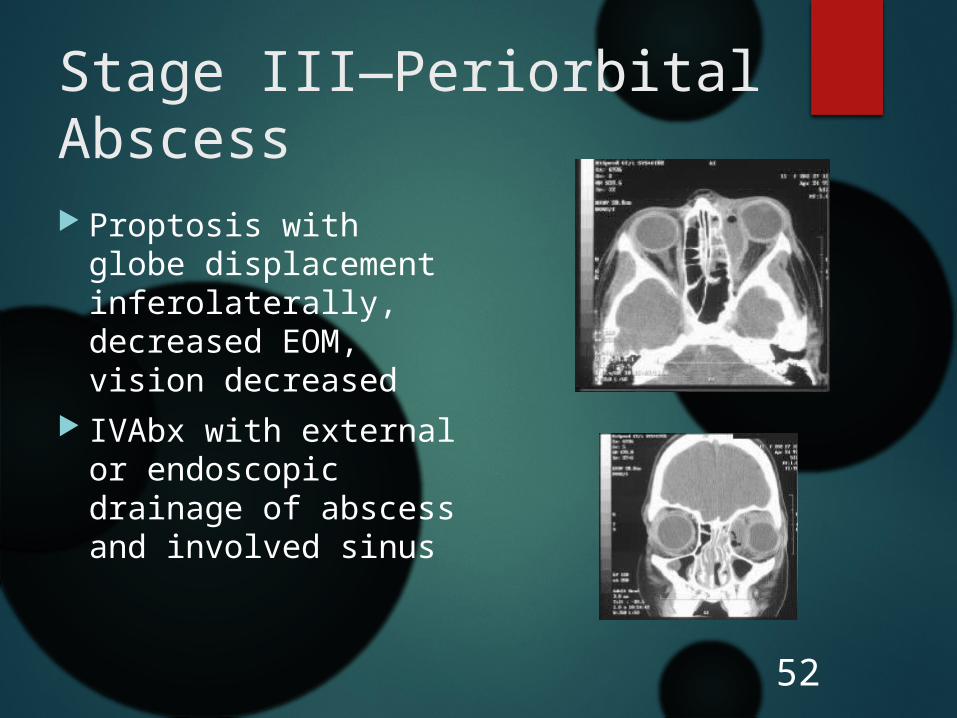
Stage III—Periorbital Abscess
Proptosis with globe displacement inferolaterally, decreased EOM, vision decreased
IVAbx with external or endoscopic drainage of abscess and involved sinus

53
Stage IV—Orbital Abscess
orbital abscess severe proptosis
and chemosis usually no globe
displacement opthalmoplegia
present Impaired visual
acuity

Medical treatment
. Orbital complications are managed according to severity at the time of presentation. group I infections may be successfully treated with a course of oral antibiotics and close monitoring. Broad-spectrum intravenous antimicrobial agents that cover the most likely pathogens should be started at the time of admission for all patients in Chandler groups II through V.

Surgical intervention Surgical intervention is indicated in any patient with decreased visual acuity, an afferent pupillary defect, or failure to improve on medical treatment after 48 hours of antimicrobial treatment. If neurosurgical intervention is planned, unilateral sinus drainage should be coordinated. Surgical drainage is indicated in most cases of abscess formation. However, a small subperiosteal abscess can be treated medically for 48 hours if the patient presents with normal vision. In the treatment of cavernous sinus thrombosis all the involved sinuses must be drained, including the sphenoid sinus.
56
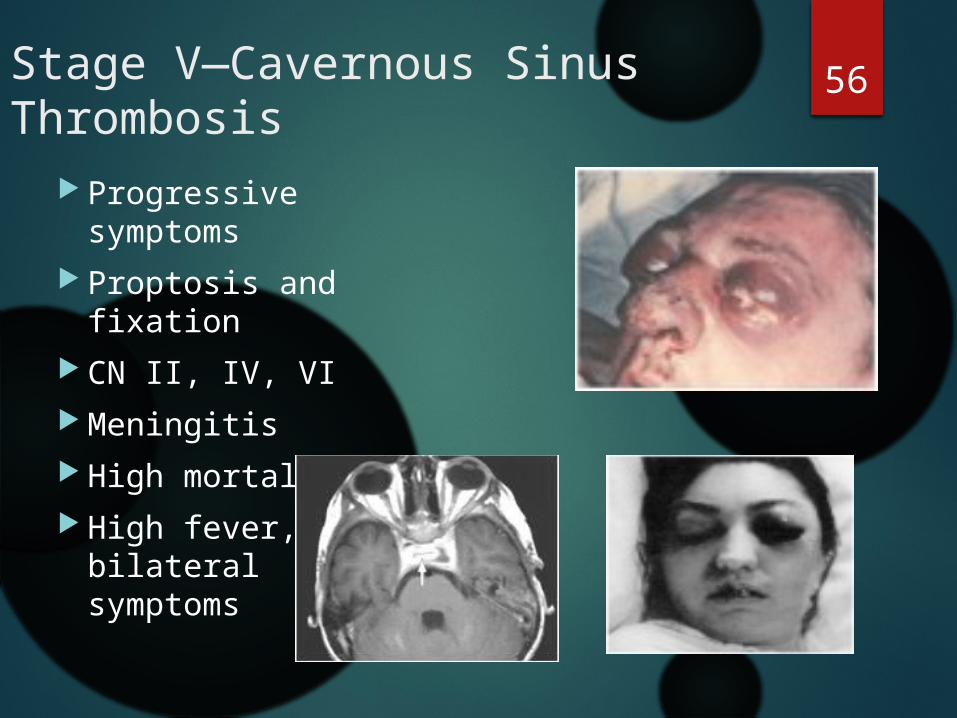
Stage V—Cavernous Sinus Thrombosis
Progressive symptoms
Proptosis and fixation
CN II, IV, VI Meningitis High mortality High fever, bilateral
symptoms

57
Intracranial Complications
Meningitis, Epidural Abscess, Intracerebral Abscess, Pott’s Puffy Tumor
Neurosurgical Consultation, high-dose antimicrobial therapy, drainage of intracranial abscess planned in concert with drainage of affected sinus
Frontal sinus is most implicated sinus: venous drainage of the frontal sinus via small diploic veins extending through sinus wall; these communicate with venous plexi of dura, periorbita and cranial periostuem


















