1 EPI235: Epi Methods in HSR April 24, 2007 L7 Program Evaluation with Longitudinal Data 3: Two case studies (Dr. Schneeweiss) Dr. Schneeweiss will illustrate a time series approach to evaluate health care cost-containment programs with longitudinal claims databases using the example of a Reference Drug Program in British Columbia. Using a formulary restriction for respiratory drugs he will illustrate the design and analytic issues of a randomized versus an observational analysis based on longitudinal data. Background reading: •Schneeweiss S, Walker AM, Glynn RJ, Maclure M, Dormuth C, Soumerai SB: Outcomes of reference drug pricing for angiotensin-converting enzyme inhibitors in British Columbia, Canada. N Engl J Med, 2002; 346:822- 829. •Schneeweiss S, Maclure M, Carleton BC, Glynn RJ, Avorn J. Clinical and
Transcript
1
EPI235: Epi Methods in HSR
April 24, 2007 L7
Program Evaluation with Longitudinal Data 3: Two case studies (Dr. Schneeweiss)
Dr. Schneeweiss will illustrate a time series approach to evaluate health care cost-containment programs with longitudinal claims databases using the example of a Reference Drug Program in British Columbia. Using a formulary restriction for respiratory drugs he will illustrate the design and analytic issues of a randomized versus an observational analysis based on longitudinal data.
Background reading: •Schneeweiss S, Walker AM, Glynn RJ, Maclure M, Dormuth C, Soumerai SB: Outcomes of reference drug pricing for angiotensin-converting enzyme inhibitors in British Columbia, Canada. N Engl J Med, 2002; 346:822-829.•Schneeweiss S, Maclure M, Carleton BC, Glynn RJ, Avorn J. Clinical and economic consequences of a reimbursement restriction of nebulised respiratory therapy in adults: direct comparison of randomised and observational evaluations. Br Med J 2004;328:560-4.
2
Case Study 1
Evaluating a Reference Drug Program
3
Reference Drug Pricing in British Columbia
Reference price
(dhp CCBs: $31 per 30 days supply)
Paid by drug benefits program
Out-of-pocket contribution
Total drug price
Better name: Therapeutic MAC (maximum allowable cost)
$0
$31
$50
RP is not a pricing policy but a
reimbursement policy
4
Reference Pricing in British Columbia
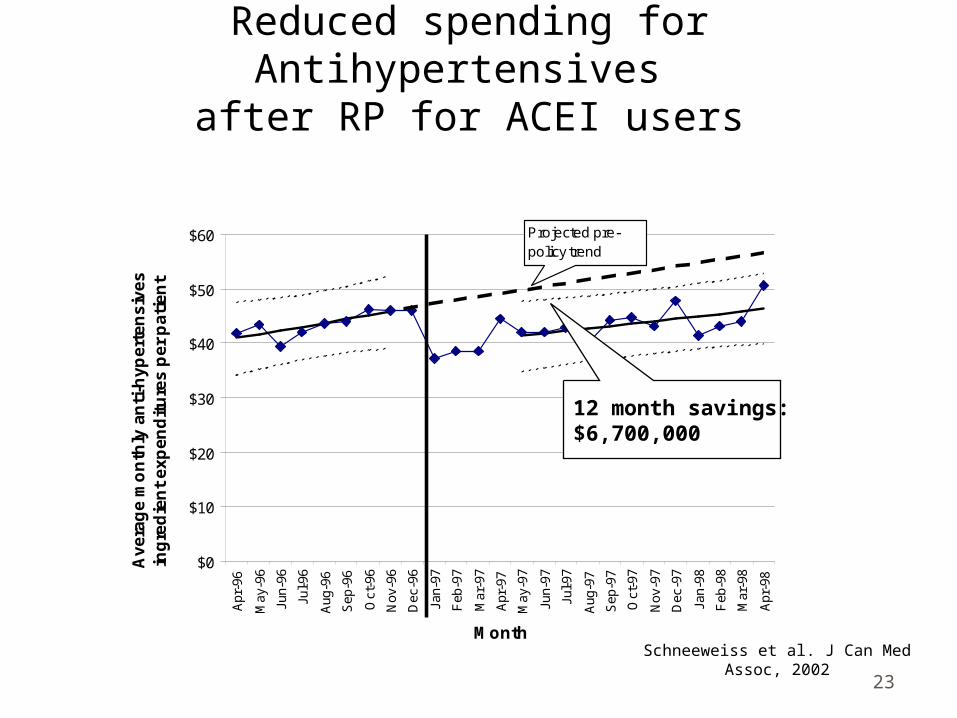
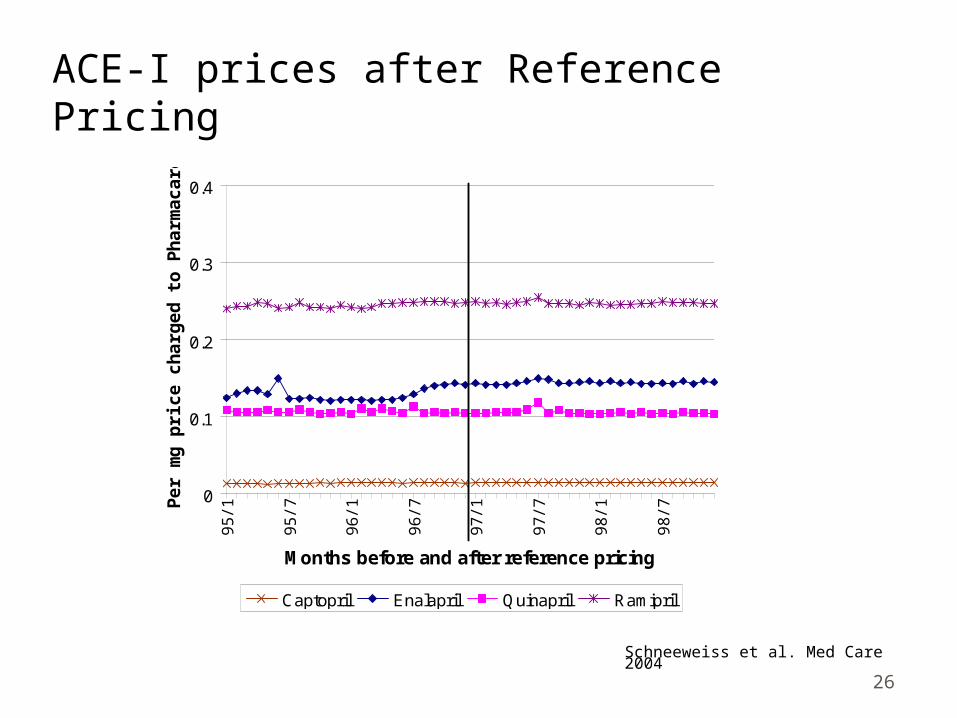
RP for ACEI also in 1997 Captopril, Quinapril, and Ramipril fully covered Enalapril required cost-sharing by patients
RP for dhp-CCBs in 1997 Felodipine fully covered Nifedipine, amlodipine, nicardipine required cost-
sharing by patients
5
RP in BC and other jurisdictions?
Reference Pricing was suggested to contain cost for a Medicare drug benefits program.Huskamp HA, Rosenthal MB, Frank RG, Newhouse JP. Health Affairs 2000;19:8-23.
Kanavos P, Reinhardt U. Health Affairs 2003;22(3).
Germany was the first jurisdiction with RP. However, there were no evaluations of clinical consequences and net savings.Schneeweiss S, Schoffski O, Selke GW. Health Policy 1998;44(3):253-60.
6
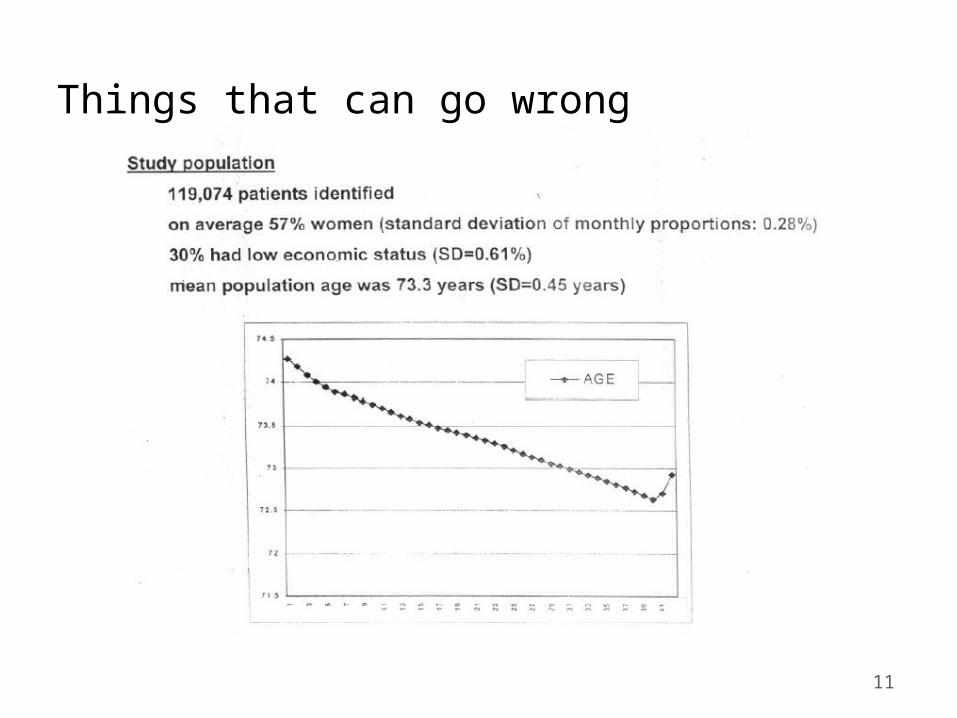
Study PopulationAll residents of British Columbia >65 covered by
Pharmacare plan A, the state wide pharmaceutical benefits program (1/2 million).
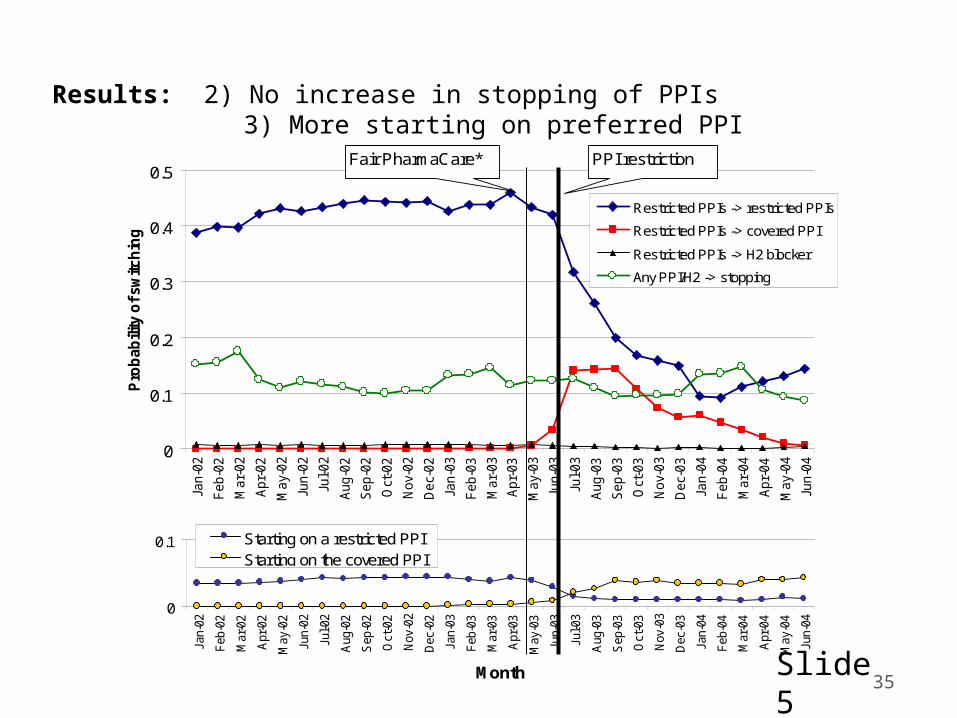
Results: 6) At least $2.9 million net savings in the first 6 months
-3
-2
-1
0
1
2
Jan
-03
Fe
b-0
3
Ma
r-0
3
Ap
r-0
3
Ma
y-0
3
Jun
-03
Jul-
03
Au
g-0
3
Se
p-0
3
Oct
-03
No
v-0
3
De
c-0
3
Month
Sa
vin
gs
/ex
ce
ss
sp
en
din
g (
$)
pe
r s
en
ior
. PharmaCare spending ($)
Patient spending ($)Total drug spending ($)
B
D
PPI restrictionFair PharmaCare†
C
A
Slide 8
39
Methods: PPI utilization data
Individual level data from all British Columbia seniors
LinkingAll pharmacy dispensings
(PharmaNet)Medical services, hospitalizations, and
vital statsMain outcome variable:
GI complications (power to show +-24 cases/m)
Drug spending (plan and patients)Time trend analyses are least prone to biasSlide 9
40
Background: Therapeutic substitution
Logic extension of generic substitution Is based on therapeutic equivalence of drugs
in groupPPIs ideal examples because very
homogeneous group of drugsSimilar policies: Reference Drug Programs
RDP for ACE, CCB, nitrates, and NSAIDs in British Columbia
Slide 10
41
Background: Implementation IssuesNeed to be careful establishing therapeutic
equivalenceWorks only if several alternatives are
availableWorks best if preferred drug is a lot less
costlySingle drug markets:
Combine with PA programs Aim to ensure that patients with specific indications
receive drugs
Slide 11
42
Summary & Questions
Substantial and rapid change in utilizationNo increase in discontinuationsNo increase in adverse GI outcomesSubstantial savingsHomogeneous groups like PPI are idealCareful expansion to more groups
Slide 12
43
Case Study 3
Randomized policy trial vs. quasi-experimental time trend analyses
44
… or randomization?
Time
Intervention
Intervention group
Control group
R
Assumptions for causal inference:
1. Subjects comply with their assigned ‘treatment’ = policy
45
Research question
Will we observe the same effects of a formulary restriction using A) a randomized trial design vs. B) a state-of-the-art observational design
recommended and used by policy evaluation researchers? Soumerai et al. Milbank, 1993
46
Case study: A Formulary restriction for nebulized respiratory drugs
Nebulized drugs were no longer covered by PharmaCare, B.C., after March 1,1999 but were fully covered before
10% of physicians were randomized to be exempted from the restriction for 6 months
(=randomized controls)10% of physicians who were subject to the
restriction were matched by location and volume (=intervention group)
Schneeweiss, BMJ under review
47
Figure 1: Pairs of smaller more remote communities from which one was randomly selected to be a control
48
Figure 2: A pair of urban physician addresses (marked +) from which one was randomly selected to be a control
49
EvaluationStudy subjects
Patients with at least 2 nebulizer dispensings from same study physician before the formulary restriction
386 control patients; 449 intervention patients
Longitudinal claims data for entire province: Rate of physician visits Rate of ER hospitalizations $$ for nebulized drugs $$ for inhalers
Outcome measures
50
Design
51
Randomized analysis
-$20
$0
$20
$40
$60
$80
$100
Nov-98
Dec-98
Jan-99
Feb-99
Mar-99
Apr-99
May-99
Jun-99
Jul-99
Aug-99
Month
Neb
uli
zer
exp
end
itu
res
in C
an$
per
p
atie
nt
per
mo
nth
Start of ran-domized trial
End of ran-domized trial
Intervention group
Control group
Difference $10
52
Observational analysis:4,625 patients not involved in randomized design
Historical controls
Intervention group
-$40
-$20
$0
$20
$40
$60
$80
$100
Sep Oct
Nov
Dec Ja
n
Feb
Mar
Apr
May Ju
n
Jul
Aug
Months
Neb
uli
zer
dru
g e
xpen
dit
ure
s in
Can
$
per
pat
ien
t p
er m
on
th
Difference $20
53
Randomized analysis: 60% of control patient were non-compliant!
-$20
$0
$20
$40
$60
$80
$100
Nov-98
Dec-98
Jan-99
Feb-99
Mar-99
Apr-99
May-99
Jun-99
Jul-99
Aug-99
Month
Neb
uli
zer
exp
end
itu
res
in C
an$
per
p
atie
nt
per
mo
nth
Start of ran-domized trial
End of ran-domized trial
Intervention group
Control group
54
Physician visit rate
55
ER hospitalization rate
56
Key results
Outcomes per month
Randomized analysis
Observational analysis
Corrected for non-
compliance
$$ for nebulizer -$8.2 -$24 ** -$21 1
$$ for inhaler $1.1 $2.8 **
ER hospitalization
-0.4/100 0.4/100
Visits 6.2/100 2.6/100
** p < 0.0001 (bootstrap estimate) 1 Zelen, Biometrics 1991
57
0
1
2
3
4
5
6
7
CON (n=140) TRT (n=147)
Mea
n M
iniA
QL
Q s
core Before After
Figure 7: Comparison of Treatment and Control Group Quality of Life
58
Weighing the benefits of randomized and non-randomized drug policy research
Randomization Observation
Upfront investment for planning and implementation