145
1 FDA Advisory Committee March 6, 2003 Dennis M. Erb, PhD Regulatory Affairs Merck Research Laboratories EMEND ® (aprepitant)
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | julia-cobb |
| View: | 216 times |
| Download: | 0 times |

1
FDA Advisory CommitteeMarch 6, 2003
Dennis M. Erb, PhDRegulatory Affairs
Merck Research Laboratories
EMEND® (aprepitant)

2
An Unmet Medical Need
Prevention of Chemotherapy-InducedNausea and Vomiting
Over one million cancer patients receive chemotherapy each year– 20% highly emetogenic chemotherapy (HEC)
Chemotherapy-induced nausea and vomiting (CINV)– Among the most distressing side effects of chemotherapy– Disrupt patients’ daily lives – Patients may even delay scheduled chemotherapy
J Clin Oncol 1997;15(1):103-9American Cancer Society. Cancer Facts & Figures 2001

3
J Clin Oncol 1997;15(1):103-9
Prevention of Chemotherapy-Induced Nausea and Vomiting
No single class of drugs is fully effective
Current therapy guideline: 5-HT3 receptor antagonist plus corticosteroid– Greater than 50% of patients still experience nausea and vomiting– Delayed emesis (>24 hours) remains a serious problem
• Symptoms often occur for several days
Prevention of CINV is an important goal of healthcare providersand their patients
Need for new therapies– More effective prevention with multiple day protection
An Unmet Medical Need

4
EMEND® (aprepitant): Addressing the Need
First new approach to CINV prevention in over a decade
Novel mechanism of action– Blocks substance P at the Neurokinin-1 receptor in the brain
Distinct efficacy profile against CINV – Acts throughout the period when symptoms may occur
• Acute (0-24 hr) and delayed (>24 hr) phases– Improves the effectiveness of current regimens
• Fewer patients experience acute or delayed CINV
May alter an enduring perception of cancer chemotherapy– Nausea and vomiting need not be inevitable

5
Development Program: Results
Prevented nausea and vomiting due to highly emetogenic chemotherapy
– Superior to Standard Therapy alone– Significant benefit in acute and delayed phases– Advantage maintained in subsequent cycles
Improved patients’ daily lives
Demonstrated a favorable safety profile– Similar to Standard Therapy alone– Well-characterized drug interaction profile
EMEND plus Standard Therapy:

6
Proposed Indication
EMEND, in combination with other antiemetic agents, is indicated for the prevention of acute and delayed nausea and vomiting associated with initial and repeat courses of highly emetogenic cancer chemotherapy, including high-dose cisplatin.

7
Consultants
Pharmacology
Dr. Paul AndrewsProfessor of Comparative PhysiologySt. George’s Hospital Medical School, London, UK
Dr. Merrill J. EgorinProfessor of Medicine and PharmacologyUniversity of Pittsburgh Cancer Institute, Pittsburgh, Pennsylvania
Dr. Malcolm RowlandResearch Professor, School of Pharmacy & Pharmaceutical SciencesUniversity of Manchester, Manchester, UK
Statistics
Dr. Janet WittesPresidentStatistics Collaborative, Inc., Washington, DC

8
Consultants
Clinical Research
Dr. Ronald De WitAssociate ProfessorRotterdam Cancer Institute and Erasmus University HospitalRotterdam, The Netherlands
Dr. Steven GrunbergProfessor of MedicineUniversity of Vermont, Burlington, Vermont
Dr. Paul HeskethProfessor of MedicineTufts University School of Medicine, Boston, Massachusetts
Dr. Loren LaineProfessor of MedicineUniversity of Southern California, Los Angeles, California

9
Agenda
Dr. Kevin Petty, Clinical Pharmacology– Background and Rationale– Clinical Pharmacology
Dr. Kevin Horgan, Clinical Research– Clinical Efficacy
Dr. Scott Reines, Clinical Research– Clinical Safety – Summation and Conclusions

10
Background and Rationale
&
Clinical Pharmacology
EMEND® (aprepitant)
Kevin J. Petty, MD, PhDClinical Pharmacology
Merck Research Laboratories

11
Aprepitant Pharmacology: Summary
Novel antiemetic mechanism of action– Blockade of (substance P) NK1 receptors in CNS– Effective against both acute and delayed emesis in ferrets
Favorable pharmacokinetics/pharmacodynamics– Once daily oral dosing– No dose adjustment in special populations
Well characterized drug interaction potential– Generally modest effects with regimen for CINV– Low potential for interaction with chemotherapy

12
Aprepitant Pharmacology: Overview
Pathophysiology of chemotherapy-inducednausea and vomiting
Nonclinical pharmacology– Properties of aprepitant– Efficacy in nonclinical models
Clinical pharmacology– Pharmacokinetics– Drug interaction

13
Mechanisms of Chemotherapy-Induced Nausea and Vomiting
Chemotherapy
Central
Peripheral

14
Mechanisms of Chemotherapy-Induced Nausea and Vomiting
Enterochromaffin cell
Serotonin release
Chemotherapy
Peripheral

15
Mechanisms of Chemotherapy-Induced Nausea and Vomiting
Enterochromaffin cell
Serotonin release
Vagal afferent5-HT3 receptors
Chemotherapy
Peripheral

16
Chemotherapy
Mechanisms of Chemotherapy-Induced Nausea and Vomiting
Dorsal vagal complex
Area postrema
Enterochromaffin cell
Serotonin release
Vagal afferent5-HT3 receptors
Peripheral
Central

17
Chemotherapy
Mechanisms of Chemotherapy-Induced Nausea and Vomiting
BrainstemNK1 receptorsSubstance P
Dorsal vagal complex
Area postrema
Enterochromaffin cell
Serotonin release
Vagal afferent5-HT3 receptors
Peripheral
Central

18
Pharmacological Properties of Aprepitant
Antagonist for NK1 (substance P) receptor
Specific, high affinity human NK1 receptor binding (IC50 = 0.12 nM)– >8000 fold selective for NK1 receptors over known receptors
mediating antiemetic activity• Dopamine D2, serotonin 5-HT3, corticosteroid, and opiate
receptors
No findings in nonclinical toxicology studies that preclude use of aprepitant in humans

19
Aprepitant Pharmacology:Novel Antiemetic Mechanism of Action
Nonclinical pharmacology
– Antiemetic efficacy in nonclinical models
• Chemotherapy-induced emesis in ferrets
– Pathophysiology similar to humans
– Used in discovery of 5-HT3 receptor antagonists

20
NK1 Antagonists Have a Broad Preclinical Antiemetic Profile
Site of Action
Central
Peripheral
Central/peripheral
Emetogen
ApomorphineMorphineNicotineLoperamide
RadiationCyclophosphamideIpecacuanhaCopper sulfate
Cisplatin
NK1
++++
++++
+
5-HT3
––––
++++
+
Antagonist

21
Aprepitant Protects Against Chemotherapy-Induced Emesis in Ferrets
Profile similar to humans(acute + delayed phases)
0
60
120
180
240
300
Ret
ches
and
Vom
its
Acute Delayed
Vehicle
0 24 48 72
Cisplatin

22
Aprepitant Protects Against Chemotherapy-Induced Emesis in Ferrets
Profile similar to humans(acute + delayed phases)
0
60
120
180
240
300
Ret
ches
and
Vom
its
Acute + delayed effects blocked by aprepitant
VehicleAprepitant
(1 mg/kg/day)
0 24 48 72
Cisplatin
0 24 48 72
Cisplatin
Acute Delayed

23
Aprepitant Protects Against Chemotherapy-Induced Emesis in Ferrets
Profile similar to humans(acute + delayed phases)
0
60
120
180
240
300
Ret
ches
and
Vom
its
Acute + delayed effects blocked by aprepitant
VehicleAprepitant
(1 mg/kg/day)Aprepitant
(2 mg/kg/day)
0 24 48 72
Cisplatin
0 24 48 72
Cisplatin
0 24 48 72
Cisplatin
Acute Delayed

24
Preclinical Assessment of Aprepitant Antiemetic Activity
Prevents cisplatin-induced emesis in the well established ferret model– Requirement for central NK1 receptor antagonism
Additive with established antiemetic agents (dexamethasone, 5-HT3 receptor antagonists)
Active against both acute and delayed phases– Distinct and novel profile– Efficacy with once-daily dosing

25
Aprepitant Pharmacology: Overview
Clinical pharmacology
– Pharmacokinetics
• Once-daily oral dosing
• No dose adjustment needed:
– Age, gender, race, body weight
– Renal or hepatic insufficiency
• Brain penetrant

26
Regimen for Chemotherapy-Induced Nausea and Vomiting Provides Consistent Daily Plasma Exposure
125 mg
Time Postdose (hr)N=12
Apr
epita
nt P
lasm
a C
once
ntra
tion
(ng/
mL)

27
Regimen for Chemotherapy-Induced Nausea and Vomiting Provides Consistent Daily Plasma Exposure
125 mg 80 mg
N=12 Time Postdose (hr)
Apr
epita
nt P
lasm
a C
once
ntra
tion
(ng/
mL)

28
Regimen for Chemotherapy-Induced Nausea and Vomiting Provides Consistent Daily Plasma Exposure
125 mg 80 mg 80 mg
Time Postdose (hr)N=12
Apr
epita
nt P
lasm
a C
once
ntra
tion
(ng/
mL)

29
Aprepitant Blocks Brain NK1 Receptorsin Humans
Binding of PET tracer to NK1 receptors prior to aprepitant dosing
Low High
Tracer Binding

30
Aprepitant Blocks Brain NK1 Receptorsin Humans
Binding of PET tracer to NK1 receptors prior to aprepitant dosing
Blockade of NK1 receptorsafter aprepitant dosing
Low High
Tracer Binding

31
Aprepitant Blocks Brain NK1 Receptorsin Humans
Binding of PET tracer to NK1 receptors prior to aprepitant dosing
Blockade of NK1 receptorsafter aprepitant dosing
Aprepitant Plasma Trough Concentration (ng/mL)
Bra
in N
K1
Rec
epto
r O
ccu
pan
cy (
%)
0102030405060708090
100
0 1 10 100 1000 10000
Low High
Tracer Binding

32
Aprepitant Blocks Brain NK1 Receptorsin Humans
Binding of PET tracer to NK1 receptors prior to aprepitant dosing
Blockade of NK1 receptorsafter aprepitant dosing
Aprepitant Plasma Trough Concentration (ng/mL)
Bra
in N
K1
Rec
epto
r O
ccu
pan
cy (
%)
0102030405060708090
100
0 1 10 100 1000 10000
Mean (± SD) Plasma Trough Concentrations of the Aprepitant 3-Day
Regimen
Low High
Tracer Binding

33
Aprepitant Pharmacology: Overview
Clinical pharmacology
– Well characterized drug interaction potential
• Generally modest effects with regimen for chemotherapy-induced nausea and vomiting
• Low potential for interaction with chemotherapy
– Supported by Phase III safety data

34
Aprepitant Is a Moderate CYP3A4 Inhibitor
2-fold 5-fold 16-fold
StrongModerateWeak
KetoconazoleItraconazoleClarithromycin
Inhibition of CYP3A4 Ranked According toFold Increase in Oral Midazolam AUC

35
Aprepitant Is a Moderate CYP3A4 InhibitorInhibition of CYP3A4 Ranked According to
Fold Increase in Oral Midazolam AUC
StrongModerateWeak
KetoconazoleItraconazoleClarithromycinErythromycin
DiltiazemVerapamil
Grapefruit juice

36
Aprepitant Is a Moderate CYP3A4 Inhibitor
Aprepitant regimen for CINV produces CYP3A4 inhibition comparable to grapefruit juice and widely used drugs (e.g., diltiazem, verapamil).
Inhibition of CYP3A4 Ranked According toFold Increase in Oral Midazolam AUC
StrongModerateWeak
KetoconazoleItraconazoleClarithromycinErythromycin
DiltiazemVerapamil
Grapefruit juice
Aprepitant (125 mg Day 1; 80 mg/d Days 2 to 5)
Day: 1 5

37
Effects of Aprepitant on Other Drugs
Evaluation of Potential Drug Interactions with Aprepitant Regimen
Coadministered antiemetics– Dexamethasone– Methylprednisolone– Ondansetron– Granisetron
Narrow therapeutic index drugs– Chemotherapy
• Docetaxel (CYP3A4)– Digoxin (P-glycoprotein)– Warfarin

38
Aprepitant Increases Plasma Concentration of Dexamethasone
Dexamethasone: 20 mg P.O. Day 1, 8 mg/d P.O. Days 2-5Aprepitant: 125 mg Day 1, 80 mg/d Days 2-5 N=12 per treatment
0 6 12 18 24
Time (hr)
0
50
100
150
200
250
Dex
amet
haso
ne
Day 1
Con
cent
ratio
n (n
g/m
L)
869-41 Dexa D1 Feb. 19, 2003
with Aprepitantwithout Aprepitant
Dex
amet
haso
ne P
lasm
a C
once
ntra
tion
(ng/
mL)

39
Aprepitant Increases Plasma Concentration of Dexamethasone
Dexamethasone Dose Adjustment in Phase III Studies Ensured Efficacy Not Confounded by Variable Steroid Exposure
N=12 per treatmentDexamethasone: 20 mg P.O. Day 1, 8 mg/d P.O. Days 2-5Aprepitant: 125 mg Day 1, 80 mg/d Days 2-5
0 6 12 18 24
Time (hr)
0
50
100
150
200
250
Dex
amet
haso
ne
Day 1
Con
cent
ratio
n (n
g/m
L)
0 6 12 18 240
50
100
150
200
250
869-41 Dexa D1&D5 Feb. 19, 2003
Day 5
with Aprepitantwithout Aprepitant
Dex
amet
haso
ne P
lasm
a C
once
ntra
tion
(ng/
mL)

40
Aprepitant Has a Small Effect on I.V. Methylprednisolone
N=8Aprepitant: 125 mg P.O.Methylprednisolone: 125 mg I.V.
0 4 8 12 16 20 24
Time (hr)
0
2000
4000
6000
8000M
ethy
lpre
dnis
olon
e P
lasm
a
Con
cent
ratio
n (n
g/m
L)
I.V.
with Aprepitantwithout Aprepitant
869-acm 67 Meth_(Slide3) IV.axg Feb. 24, 2003

41
Aprepitant Does Not Affect 5-HT3 AntagonistsOndansetron 32 mg I.V. +Aprepitant 375 mg (N=15)
0 4 8 12 16 18 24
Time (hr)
0
100
200
300
400
500
600
Ond
anse
tron
Con
c. (
ng/m
L) I.V.
869-41&50 Anta_(Slide4) a1 Feb. 19, 2003
with Aprepitantwithout Aprepitant
No dose adjustment of ondansetron or granisetron required
Ond
anse
tron
Pla
sma
Con
cent
ratio
n (n
g/m
L)

42
No dose adjustment of ondansetron or granisetron required
Aprepitant Does Not Affect 5-HT3 AntagonistsOndansetron 32 mg I.V. +Aprepitant 375 mg (N=15)
Granisetron 2 mg P.O. +Aprepitant 125 mg (N=18)
0 4 8 12 16 18 24
Time (hr)
0
100
200
300
400
500
600
Ond
anse
tron
Con
c. (
ng/m
L) I.V.
with Aprepitantwithout Aprepitant
0 12 24 36 48 60 720
2
4
6
8
10
869-41&50 Anta_(Slide4) Feb. 25, 2003
PO
Gra
nise
tron
Con
c. (
ng/m
L)
with Aprepitantwithout Aprepitant
P.O.
Gra
nise
tron
Pla
sma
Con
cent
ratio
n (n
g/m
L)
Ond
anse
tron
Pla
sma
Con
cent
ratio
n (n
g/m
L)

43
Effects of Aprepitant on Other Drugs
Evaluation of Potential Drug Interactions with Aprepitant Regimen
Coadministered antiemetics– Dexamethasone– Methylprednisolone– Ondansetron– Granisetron
Narrow therapeutic index drugs– Chemotherapy
• Docetaxel (CYP3A4)– Digoxin (P-glycoprotein)– Warfarin

44
Aprepitant Does Not Affect Docetaxel Pharmacokinetics
(Ongoing Trial, N=5)
Plasma ConcentrationProfiles of Docetaxel
Docetaxel AUC of individual patients
Without WithAprepitant Aprepitant
0
1
2
3
4
5
869-51 Doce 2 Feb. 25, 2003
Doc
etax
el A
UC
0-
0 4 8 12Time (hr)
0.01
0.1
1
10
Doc
etax
el C
onc.
(m
cg/m
L)
with Aprepitantwithout Aprepitant
Doc
etax
el P
lasm
a C
once
ntra
tion
(mcg
/mL)

45
0 4 8 12 16 20 24
Time (hr)
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
Mea
n D
igox
in P
lasm
a
Con
cent
ratio
n (n
g/m
L)
With APRWithout APR
869-47 Digox 1 Feb. 11, 2003
Day 1 (N=11)
Aprepitant Does Not Affect Steady State Pharmacokinetics of the P-glycoprotein Substrate Digoxin
No dose adjustment of digoxin requiredN=11
AprepitantAprepitant
Dig
oxin
Pla
sma
Con
cent
ratio
n (n
g/m
L)

46
Aprepitant Has Low Potential to Affect I.V. Chemotherapeutic Agents
Pharmacokinetics of chemotherapeutic agents frequently modulated by CYP3A4 and/or P-glycoprotein
– Aprepitant has• Weak to no effect on I.V. CYP3A4 substrates
– Methylprednisolone– Ondansetron– Docetaxel
• No effect on a P-glycoprotein substrate (digoxin)
Low potential to interact with chemotherapy as supported by Phase III safety data

47
Aprepitant Slightly InducesWarfarin Metabolism
Small inductive effect on warfarin warrants closer monitoring of INR
N=11-12
1 2 3 4 5 6 7 8
Day
0.0
0.2
0.4
0.6
0.8
1.0
1.2R
atio
of f
old
chan
ge fr
om b
asel
ine
(AP
R/p
lace
bo)
869-67 INR-R-S GM Ratio a1 Feb. 19, 2003
R(+) Warfarin
S(-) Warfarin
869-67 INR-R-S GM Ratio a1.axg Feb. 19, 2003
APR or PlaceboWarfarin

48
Aprepitant Slightly InducesWarfarin Metabolism
Small inductive effect on warfarin warrants closer monitoring of INR
N=11-12
1 2 3 4 5 6 7 8
Day
0.0
0.2
0.4
0.6
0.8
1.0
1.2R
atio
of f
old
chan
ge fr
om b
asel
ine
(AP
R/p
lace
bo)
869-67 INR-R-S GM Ratio Feb. 19, 2003
R(+) Warfarin
S(-) Warfarin
INR
WarfarinAPR or Placebo

49
Aprepitant Pharmacology: Summary
Novel antiemetic mechanism of action– Blockade of (substance P) NK1 receptors in CNS– Effective against both acute and delayed emesis in ferrets
Favorable pharmacokinetics/pharmacodynamics– Once-daily oral dosing– No dose adjustment in special populations
Well characterized drug interaction potential– Generally modest effects with regimen for chemotherapy-
induced nausea and vomiting– Low potential for interaction with chemotherapy

50
Conclusions
The pharmacokinetics of aprepitant and the potential for clinically meaningful drug interactions with aprepitant have been well characterized
Appropriate guidance can be provided for safe and effective use in the intended patient population

51
Clinical Efficacy
Kevin J. Horgan, MDClinical Research
Merck Research Laboratories
EMEND® (aprepitant)

52
An unmet medical need
J Clin Oncol ;17(9):2971-94, 1999
Prevention of Nausea and Vomiting withHighly Emetogenic Chemotherapy
Highly emetogenic chemotherapy evokes nausea and vomiting in the vast majority of patients in the absence of preventive therapy
Current therapy consists of a 5-HT3 receptor antagonist and a corticosteroid
Despite current therapy many (>50%) patients still have symptoms following highly emetogenic chemotherapy

53
24
1 2 3 4 5
Acute Delayed
Overall
120
Administration ofChemotherapy
Day
Hours 0
Time Course of Nausea and Vomiting Following Chemotherapy

54
Current Standard Therapy
Corticosteroid Therapy+5-HT3 Receptor Antagonist
Augments efficacy of 5-HT3 receptor antagonist in preventing acute symptoms
Some efficacy as monotherapy in preventing delayed symptoms
Not approved as antiemetic
Prevents acute symptoms in ~50% of patients
Equivocal efficacy preventing delayed symptoms
Approved only for acute symptoms
Highly Emetogenic Chemotherapy

55
Aprepitant Program Objective
To define the potential role of aprepitant in theprevention of nausea and vomiting associated
with highly emetogenic chemotherapy

56
Aprepitant Program Overview
Does aprepitant work alone as an antiemetic?

57
Aprepitant Program Overview
Does aprepitant work alone as an antiemetic?
Is a regimen including aprepitant more effective than current standard therapy?

58
Aprepitant Program Overview
Does aprepitant work alone as an antiemetic?
Is a regimen including aprepitant more effective than current standard therapy?
What is the optimum aprepitant dose?

59
Aprepitant Program Overview
Does aprepitant work alone as an antiemetic?
Is a regimen including aprepitant more effective than current standard therapy?
What is the optimum aprepitant dose?
Confirm that the Phase III aprepitant regimen is safe and effective.

60
Cisplatin Is PrototypicHighly Emetogenic Chemotherapy
Cornerstone of therapy for common cancers (e.g., lung, ovarian)
Most emetogenic chemotherapy 50 mg/m2 infused over 3 hours is highly emetogenic
Predictable and well characterized pattern of emesis
Benchmark for evaluation and approval of novel antiemetic therapies– 5-HT3 receptor antagonists: Ondansetron, granisetron, dolasetron– Dopamine D2 receptor antagonist: Metoclopramide
Antiemetic efficacy with cisplatin predictive of antiemetic efficacy with other agents (e.g., carboplatin, doxorubicin, cyclophosphamide)

61
Key Elements of the Clinical Trials
All studies double-blind versus appropriate control
All patients cisplatin näive
All patients to receive high dose cisplatin– 70 mg/m2 infused over 3 hours on Day 1– Additional emetogenic chemotherapy permitted on Day 1
Randomization stratified– Gender– Additional emetogenic chemotherapy
“Rescue” therapy allowed for established nausea or vomiting

62
Key Elements of the Clinical Trials
Daily patient diary – All emetic events– All use of rescue therapy– Nausea assessments
Primary efficacy assessments– Initial cycle of cisplatin chemotherapy– Modified intention-to-treat population

63
Efficacy Endpoints
Primary endpoint – Complete Response: No emesis and no rescue
• Reflects control of both emesis and nausea• Primary endpoint in ondansetron and
dolasetron development programs
Other key endpoints– Frequency of emetic events – Use of rescue therapy– Nausea– Impact of nausea and vomiting on daily life

64
Aprepitant Program Overview
Does aprepitant work alone as an antiemetic?
Is a regimen including aprepitant more effective than current standard therapy?
What is the optimum aprepitant dose?
Confirm that the Phase III aprepitant regimen is safe and effective.

65
Eur J Cancer 37:835-842, 2001
Aprepitant as Monotherapy
Day 1
Aprepitant I.V. prodrug60 or 100 mg
Ondansetron I.V.32 mg
Protocol 004

66
0
20
40
60
80
100
Per
cent
of P
atie
nts
Acute Delayed
AprepitantOndansetron
869 acm 4 ComplResp Feb. 14, 2003
Complete Response: Acute and Delayed PhasesAprepitant as Monotherapy
Protocol 004
37%
48% 48%
17%
p<0.05
N= 30 23 29 23

67
0
20
40
60
80
100
Per
cent
of P
atie
nts
Acute Delayed
AprepitantOndansetron
869 acm 4 ComplResp Feb. 14, 2003
Aprepitant as Monotherapy
†Cancer 78:2193-2198, 1996
HistoricalData†
(Untreated)
p<0.05
Complete Response: Acute and Delayed PhasesProtocol 004
37%
48% 48%
17%
N= 30 23 29 23

68
Protocol 004
ConclusionsAprepitant as Monotherapy
Aprepitant is an effective antiemetic– In both acute and delayed phases
Distinctive efficacy profile relative to 5-HT3 receptor antagonists– Significantly superior efficacy in delayed phase
Distinctive efficacy profile implied potential for better efficacy by combining with a 5-HT3 receptor antagonist

69
Aprepitant Program Overview
Does aprepitant work alone as an antiemetic?
Is a regimen including aprepitant more effective than current standard therapy?
What is the optimum aprepitant dose?
Confirm that the Phase III aprepitant regimen is safe and effective.

70
Aprepitant Regimen Study
Aprepitant loading dose strategy– Day 1: 400 mg P.O.– Days 2-5: 300 mg P.O.
Control regimen contains “Standard Therapy”– Day 1 only: Granisetron 10 µg/kg I.V.
Dexamethasone 20 mg P.O.
Protocol 007
Design Features

71
P
Aprepitant Regimen Study
Day 1 Days 2 to 5
Primary Treatment GroupsProtocol 007
G DControl
Group
G=granisetron; D=dexamethasone; A=aprepitant; P=placebo
P

72
Aprepitant Regimen Study
Group
Control
Day 1 Days 2 to 5
G D A A
G=granisetron; D=dexamethasone; A=aprepitant; P=placebo
P P
PAprepitant 1-Day
Aprepitant 5-Day
400
400 300
Primary Treatment GroupsProtocol 007

73
0
20
40
60
80
100
Per
cent
of P
atie
nts
Acute Delayed
869-7 Acute-Del 1A Feb. 14, 2003
Aprepitant Regimen Study
N Engl J Med 340: 190-5: 1999
Complete Response: Acute and Delayed Phases
Aprepitant 5-Day
Aprepitant 1-Day
Control
77%
57%52%
16%
p<0.05
p<0.01
N= 53 50 54 5154 51
83%
43%
p<0.01
p<0.01
Protocol 007

74
Aprepitant Regimen Study
Aprepitant enhances the efficacy of a “Standard Therapy” regimen– Acute and delayed nausea and vomiting
Aprepitant is more effective when administered for multiple days– Delayed nausea and vomiting
• Even when a very high dose is administered on Day 1
ConclusionsProtocol 007

75
Aprepitant Program Overview
Does aprepitant work alone as an antiemetic?
Is a regimen including aprepitant more effective than current standard therapy?
What is the optimum aprepitant dose?
Confirm that the Phase III aprepitant regimen is safe and effective.

76
Dose Finding Study
Primary Endpoint: Complete Response– Overall (Days 1 to 5) = Acute + Delayed
Evolution of “Standard Therapy” – Day 1: Ondansetron + dexamethasone– Days 2 to 5: Dexamethasone
Transition from tablet to capsule formulation– Formulation for all subsequent studies and for market
Protocol 040/042
Design Features

77
Dose Finding Study
Initiated with two aprepitant dose regimens– Day 1: 375 mg Days 2 to 5: 250 mg– Day 1: 125 mg Days 2 to 5: 80 mg
Capsule formulation had better than anticipated bioavailability– Both 375/250 mg and 125/80 mg regimens were predicted
to have similar clinical efficacy
In order to explore the dose response adequately – 375/250 mg regimen discontinued after 35 patients– 40/25 mg regimen added
Protocol 040/042
Design Features

78
Dose Finding Study
Day 1 Days 2 to 5
O D D
Protocol 040/042
Primary Treatment Groups
O=ondansetron; D=dexamethasone; A=aprepitant; P=placebo
Group
Control P P

79
Dose Finding Study
Day 1 Days 2 to 5
O D A AD
Protocol 040/042
Primary Treatment Groups
O=ondansetron; D=dexamethasone; A=aprepitant; P=placebo
Group
Aprepitant 40/25
Control P P
40 25

80
Dose Finding Study
Group
Control
Day 1
125
40
Days 2 to 5
80
25
O=ondansetron; D=dexamethasone; A=aprepitant; P=placebo
O D A AD
P P
Aprepitant 40/25
Aprepitant 125/80
Protocol 040/042
Primary Treatment Groups

81
Dose Finding StudyOverall Complete Response
0
20
40
60
80
100
Per
cent
of P
atie
nts
869 40-42 Compl Resp 1A Feb. 14, 2003
Aprepitant 125/80
Aprepitant 40/25
Control
N= 131 126119
59%
44%
71%p<0.05
p<0.01
Protocol 040/042

82
Dose Finding StudyOverall Complete Response
0
20
40
60
80
100
Per
cent
of P
atie
nts
869 40-42 Compl Resp 1A Feb. 14, 2003
Aprepitant 125/80
Aprepitant 40/25
Control
N= 131 126119
59%
44%
71%
Protocol 040/042
p<0.05

83
Dose Finding StudyComplete Response: Acute and Delayed Phases
0
20
40
60
80
100P
erce
nt o
f Pat
ient
s
869-acm 40-42 S8A Feb. 14, 2003
Acute DelayedPhase
Aprepitant 125/80
Aprepitant 40/25
Control
N= 131 126119 132 126119
64%
76%83%
71% 73%
45%
p<0.05
p<0.01
p<0.01
Protocol 040/042

84
Dose Finding StudyTime to First Emesis or Rescue
0 24 48 72 96 120
Hours
040
60
80
100
Per
cent
of P
atie
nts
869-acm 40-42 Time Cr3 Feb. 15, 2003
with
Com
plet
e R
espo
nse
Control
Protocol 040/042

85
Dose Finding StudyTime to First Emesis or Rescue
0 24 48 72 96 120
Hours
040
60
80
100
Per
cent
of P
atie
nts
869-acm 40-42 Time Cr3 Feb. 15, 2003
with
Com
plet
e R
espo
nse
Control
APR 125/80
APR 40/25
Protocol 040/042

86
Dose Finding StudyTime to First Emesis or Rescue
0 24 48 72 96 120
Hours
040
60
80
100
Per
cent
of P
atie
nts
869-acm 40-42 Time Cr3 Feb. 15, 2003
with
Com
plet
e R
espo
nse
Control
APR 125/80
APR 40/25
APR 375/250
Protocol 040/042

87
Dose Finding Study
Aprepitant 125/80 mg regimen is effective – 40/25 mg less effective– 375/250 mg adds no apparent benefit
Almost all initial therapy failures occur within 72 hours – 3-day dosing likely to provide full benefit
Phase III aprepitant regimen:125 mg on Day 1 followed by 80 mg on Days 2 and 3
ConclusionsProtocol 040/042

88
Two large multinational studies, both with multiple cycle extensions,in patients receiving high-dose cisplatin chemotherapy
Phase III Primary Hypothesis: Cycle 1
Compared to Standard Therapy:
– The aprepitant regimen will provide superior control of nausea and vomiting as measured by the proportion of patients with an Overall Complete Response
• No emesis and no rescue
• In the 120 hours following the initiation of cisplatin

89
Phase III Studies
Aprepitant regimen refinements
– 3-day aprepitant dosing
– Dexamethasone dose reduced to provide plasma exposure similar to control
Protocols 052 and 054
Design Features

90
Phase III Studies
Aprepitant
Control
Group Day 4
16
8
Day 1
12
20
Days 2-3
8
16
O D A DD A
O=ondansetron; D=dexamethasone; A=aprepitant; P=placebo
P P
Protocols 052 and 054
Primary Treatment Groups

91
Phase III Studies
Inclusion Criteria– Cisplatin dose 70 mg/m2
Exclusion Criteria– Laboratory value parameters
• AST or ALT 2.5 x upper limit of normal (ULN)• Neutrophil count <1500/mm3 and WBC <3000/mm3
• Bilirubin >1.5 x ULN; Creatinine >1.5 x ULN– Concomitant or very recent use of
• Strong CYP3A4 inhibitors• CYP3A4 inducers
Design FeaturesProtocols 052 and 054

92
Phase III Studies
Protocols 052 and 054 Combined
Patient Demographics
(N=549)
(N=554)
Aprepitant
Control
0 20 40 60 80 100
Percent of Patients
869-acm 52-54 S8B Feb. 28, 2003
Male
<65
Gender
Age
Additionalemetogenicchemotherapy

93
Phase III Studies
0 20 40 60 80 100
Percent of Patients
Lung
Ovarian
Head and Neck
Esophageal
Gastric
869-acm 52-54 S10 B Feb. 14, 2003
Aprepitant (N=549)
Control (N=554)
Protocols 052 and 054 Combined
Primary Cancer Diagnoses

94
Phase III Studies
Protocols 052 and 054 Combined
Concomitant Chemotherapy
Aprepitant (N=549)
Control (N=554)
0 20 40 60 80 100
Percent of Patients
EtoposideFluorouracilGemcitabineVinorelbinePaclitaxelCyclophosphamideDoxorubicinDocetaxelCisplatin (only)
869-acm 52-54 S11 A Feb. 28, 2003

95
Phase III Studies: Cycle 1
0
20
40
60
80
100
Per
cent
of P
atie
nts
052
869-acm 52-54 S12A1-A2 Sep1 Feb. 13, 2003
AprepitantControl
p<0.001
52%
N= 260 260
73%
Primary Endpoint: Overall Complete Response
Protocol 052

96
Phase III Studies: Cycle 1
0
20
40
60
80
100
Per
cent
of P
atie
nts
052
869-acm 52-54 S12A1-A2 Sep1 Feb. 13, 2003
AprepitantControl
p<0.001
N= 260 260
0
20
40
60
80
100
869-acm 52-54 S12A1-A2 Sep2 Feb. 13, 2003
054
63%
43%
p<0.001
263260
Protocol 054Protocol 052
Primary Endpoint: Overall Complete Response
52%
73%

97
Phase III Studies: Cycle 1
0
20
40
60
80
100
Per
cent
of P
atie
nts
Acute Delayed
052
869-acm 52-54 S12 H1-A Feb. 13, 2003
AprepitantControl
89%
78% 75%
56%
N= 259 260 260 260
p<0.001p<0.001
0
20
40
60
80
100
869-acm 52-54 S12 H1-B Feb. 13, 2003
Acute Delayed
054
83%
68%
47%
68%
260263261 263
p<0.001
p<0.001
Protocol 052
Complete Response: Acute and Delayed Phases
Protocol 054

98
Phase III Studies: Cycle 1
0 24 48 72 96 120Hours
040
60
80
100
Per
cent
of P
atie
nts
Protocol 052
0 24 48 72 96 120Hours
040
60
80
100
869-52-54 Time_1st_Cr Feb. 14, 2003
Protocol 054
ControlAprepitant
Time to First Emesis or Rescue
APR N=260 Control N=260 APR N=260 Control N=263

99
0
20
40
60
80
100
Per
cent
of P
atie
nts
No Emesis No Rescue
052052
0
20
40
60
80
100
No Emesis No Rescue
054054
869-acm 52-54 S14 A3 Feb. 13, 2003
AprepitantControl
Phase III Studies: Cycle 1
N= 260 260 260263260 260 260 263
78%
55%
81%
71%66%
45%
82%
73%
p<0.01 p<0.01
p<0.01
p<0.01
Components of Primary Endpoint: Overall
Protocol 052 Protocol 054

100
Nausea is a particularly important symptom for patients
A validated 100 mm visual analog scale (VAS) was used
Patient places a vertical mark corresponding to level of nausea
Prespecified endpoints (Days 1 to 5)– No Nausea: Maximum VAS <5 mm– No Significant Nausea: Maximum VAS <25 mm
How much nausea have you had over the past 24 hours?
Nonause
a
Nausea as bad as it could be
Phase III Studies: Cycle 1
0 mm 100 mm
Nausea Assessment

101
Phase III Studies: Cycle 1
0
20
40
60
80
100
Per
cent
of P
atie
nts
VAS <5 mm VAS <25 mm
052
0
20
40
60
80
100
869-acm 52-54 S14 B3 Feb. 14, 2003
VAS <5 mm VAS <25 mm
054
AprepitantControl
48% 44%
73%66%
49%
39%
71%64%
N= 257 260 260263257 259 260 263
p<0.05
No Nausea and No Significant Nausea: Overall
Protocol 052 Protocol 054

102
0
20
40
60
80
100
Per
cent
VAS <5 mmVAS <5 mm0
20
40
60
80
100
869-acm 52-54 S14 C Feb. 14, 2003
VAS <25 mmVAS <25 mm
AprepitantControl
Phase III Studies: Cycle 1
48%42%
72%65%
N = 517 523 522517
p<0.05
p<0.05
No Nausea and No Significant Nausea: OverallProtocols 052 and 054 Combined

103
Phase III Studies: Cycle 1
Complete Protection = Complete Response + No Significant Nausea– Aprepitant statistically superior in both protocols 052 and 054
Total Control = Complete Response + No Nausea – Aprepitant statistically superior in protocol 054
No Impact on Daily Life– Validated nausea- and vomiting-specific questionnaire– Aprepitant statistically superior in both protocols 052 and 054
Other Prespecified Endpoints

104
Phase III Studies: Cycle 1
Protocols 052 and 054 Combined: Overall(Post-hoc Analysis)
0
20
40
60
80
100
Per
cent
of P
atie
nts
869-acm 52-54 S14 D Feb. 14, 2003
with
Com
plet
e R
espo
nse
Aprepitant (N=70)
Control (N=72)
p<0.001
59%
26%
Concomitant Emetogenic Chemotherapy (Cyclophosphamide and/or Doxorubicin)

105
Phase III Studies: Cycle 1 Conclusions Aprepitant highly effective in two replicate clinical trials
– Overall 20% fewer patients vomited or required rescue medications for established nausea or emesis (p<0.001)
Superiority of aprepitant evident
– In both acute and delayed phases
– For both components of primary endpoint: Emesis and use of rescue medications
– In patients taking cisplatin plus other emetogenic chemotherapy (post-hoc analysis)
Consistent advantage for aprepitant regimen on nausea endpoints
– More rescue medications used in control group

106
Phase III Studies: Multiple Cycles
Up to 5 additional cycles of blinded treatment – 68 out of 71 sites participated
Multiple cycle efficacy data collection– Two questions at Day 6 to 8 clinic visit in cycles 2 to 6
• Did you have 1) Emesis? 2) Significant nausea interfering with daily life?
Protocols 052 and 054

107
Protocols 052 and 054 Combined
2 3 4 5 6
Chemotherapy Cycle
20
40
60
80
100
Per
cent
of P
atie
nts
869-acm 5254 Cycle 11 Feb. 14, 2003
Aprepitant
Control
N= 349 270 184 117 83N= 393 278 180 111 72
Observed Proportion of Patients without Emesis and without Significant Nausea
Phase III Studies: Multiple Cycles

108
Proportion of Patients Symptom Free by Cycle Phase III Studies: Multiple Cycles
Protocols 052 and 054 Combined
1 2 3 4 5 60
20
40
60
80
100
Per
cent
of P
atie
nts
Aprepitant
Control
Time to First Emesis
1 2 3 4 5 6Cycles
0
20
40
60
80
100
869-acm 5254 1Em-1Frzn Feb. 24, 2003
Aprepitant
Control
Time to First Significant Nausea
N=520 256 185 119 70 51 N=523 201 131 80 46 29
N=517 264 183 115 67 46N=522 259 165 108 56 34
Chemotherapy Cycle

109
Aprepitant Efficacy Conclusions
Addition of aprepitant to a regimen of a 5-HT3 receptor antagonist and a corticosteroid is beneficial in the prevention of nausea and vomiting due to highly emetogenic chemotherapy
The benefit is– Clinically important– Evident during both the acute and delayed phases– Sustained during multiple cycles of chemotherapy

110
Clinical Safety
Scott A. Reines, MD, PhDClinical Research
Merck Research Laboratories
EMEND® (aprepitant)

111
Number of Patients Receiving Aprepitant
Phase I clinical pharmacology studies
Studies in non-cancer patients
Studies in patients receiving cancer chemotherapy
Phase II 915Phase III 544
711
1172
1459
Total 3342
Clinical Development Program

112
APR 125/80(N=544)
%
69.1
17.1
13.4
7.7
3.7
Control (N=550)
%
67.6
12.7
13.6
5.8
3.8
Adverse experiences (AEs)
Drug-related AEs
Serious AEs
Discontinuations due to AEs
Deaths
Percent of Patients with:
Phase III: Cycle 1
Clinical Adverse Experience Summary

113
Most Common Serious Clinical AEs
Control(N=550)
%
13.61.10.91.30.20.50.20.50.70.7
Percent of Patients with:
Serious adverse experiences Neutropenia Dehydration Febrile neutropenia Respiratory insufficiency Pulmonary embolism Thrombocytopenia Pneumonia Cardiac arrest Leukopenia
Phase III: Cycle 1 APR 125/80(N=544)
%
13.42.21.81.30.90.70.70.70.40.2
(Incidence 0.7%)

114
Control(N=543)
%
19.5
2.6
0.2
0.7
APR 125/80(N=539)
%
22.3
4.1
0.2
0.4
Laboratory adverse experiences
Drug-related laboratory AEs
Serious laboratory AEs
Discontinuations due to lab AEs
Percent of Patients with:
Phase III: Cycle 1
Laboratory Adverse Experience Summary

115
Evaluation of Toxicity Due toConcomitant Therapies
Cisplatin-induced toxicity– Serum creatinine– Neurotoxicity, ototoxicity
Other chemotherapy-induced toxicity– Neutropenia categorized using NCI Common Toxicity Criteria– Hematologic adverse experiences– Fever, infection, febrile neutropenia, dehydration
Glucocorticoid-induced toxicity– Hypertension, hyperglycemia, hypokalemia
Chemotherapy metabolized by CYP3A4

116
Day 6 to 8
APR 125/80(N=501)
%
14.4
11.0
3.2
0.2
0.0
Control(N=507)
%
16.2
12.6
3.2
0.4
0.0
Day 19 to 29
APR 125/80(N=482)
%
7.4
6.8
0.6
0.0
0.0
Control(N=495)
%
7.7
6.3
1.2
0.2
0.0
> Upper Limit of Normal (ULN)
> ULN to 1.5 x ULN
> 1.5 to 3.0 x ULN
> 3.0 to 6.0 x ULN
> 6.0 x ULN
Serum Creatinine(NCI Criteria)
Phase III: Cycle 1
Serum Creatinine by NCI CriteriaCisplatin-Induced Toxicity

117
Cisplatin-Induced ToxicitySerum Creatinine by NCI Criteria
No differences in nephrotoxicity as indicated by serum creatinine
Day 6 to 8
APR 125/80(N=501)
%
14.4
11.0
3.2
0.2
0.0
Control(N=507)
%
16.2
12.6
3.2
0.4
0.0
Day 19 to 29
APR 125/80(N=482)
%
7.4
6.8
0.6
0.0
0.0
Control(N=495)
%
7.7
6.3
1.2
0.2
0.0
> Upper Limit of Normal (ULN)
> ULN to 1.5 x ULN
> 1.5 to 3.0 x ULN
> 3.0 to 6.0 x ULN
> 6.0 x ULN
Serum Creatinine(NCI Criteria)
Phase III: Cycle 1

118
No differences in nephrotoxicity as indicated by serum creatinine
Cisplatin-Induced Toxicity
No differences in neurotoxicity or ototoxicity between groups
Serum Creatinine by NCI Criteria
Day 6 to 8
APR 125/80(N=501)
%
14.4
11.0
3.2
0.2
0.0
Control(N=507)
%
16.2
12.6
3.2
0.4
0.0
Day 19 to 29
APR 125/80(N=482)
%
7.4
6.8
0.6
0.0
0.0
Control(N=495)
%
7.7
6.3
1.2
0.2
0.0
> Upper Limit of Normal (ULN)
> ULN to 1.5 x ULN
> 1.5 to 3.0 x ULN
> 3.0 to 6.0 x ULN
> 6.0 x ULN
Serum Creatinine(NCI Criteria)
Phase III: Cycle 1

119
Neutropenia Severity by NCI CriteriaChemotherapy-Induced Toxicity
Any neutropenia < 2000/mm3
1500 < 2000/mm3
1000 < 1500/mm3
500 < 1000/mm3
< 500/mm3
Neutropenia Severity(NCI Criteria)
Day 6 to 8
APR 125/80(N=481)
%
6.6
3.1
2.3
1.0
0.2
Control(N=489)
%
4.9
2.5
1.4
0.4
0.6
Day 19 to 29
APR 125/80(N=462)
%
24.2
10.8
6.3
5.6
1.5
Control(N=477)
%
28.3
13.4
7.5
5.9
1.5
Phase III: Cycle 1

120
No evidence of differences in hematological toxicity
Chemotherapy-Induced ToxicityNeutropenia Severity by NCI Criteria
Any neutropenia < 2000/mm3
1500 < 2000/mm3
1000 < 1500/mm3
500 < 1000/mm3
< 500/mm3
Neutropenia Severity(NCI Criteria)
Day 6 to 8
APR 125/80(N=481)
%
6.6
3.1
2.3
1.0
0.2
Control(N=489)
%
4.9
2.5
1.4
0.4
0.6
Day 19 to 29
APR 125/80(N=462)
%
24.2
10.8
6.3
5.6
1.5
Control(N=477)
%
28.3
13.4
7.5
5.9
1.5
Phase III: Cycle 1

121
APR 125/80(N=544)
%12.5
5.95.04.03.12.92.21.7
2.61.81.7
Control(N=550)
%10.5
5.15.83.52.53.52.41.3
2.71.31.8
Percent of Patients with:
InfectionsDehydrationNeutropeniaThrombocytopeniaAnemiaFeverLeukopeniaFebrile neutropenia
HypokalemiaHypertensionHyperglycemia
Phase III: Cycle 1
Prespecified Adverse Experiences
Chemotherapy-induced
Glucocorticoid-induced
Chemotherapy or Glucocorticoid-Induced Toxicity

122
(Etoposide, Vinca Alkaloids, Taxanes, Irinotecan, Ifosfamide)
Safety of Aprepitant in Patients Receiving Chemotherapy Metabolized by CYP3A4
Overall summary of adverse events– Clinical– Laboratory
Hematological toxicity– All chemotherapy metabolized by CYP3A4– Individual chemotherapies
• Etoposide, vinorelbine, paclitaxel

123
APR 125/80(N=266)
%
74.1
30.1
15.0
0
Control(N=251)
%
74.5
28.3
13.5
0
Percent of Patients with:
Clinical adverse experiences
Prespecified AEs
Serious clinical AEs
Serious laboratory AEs
Phase III: Cycle 1
(Etoposide, Vinca Alkaloids, Taxanes, Irinotecan, Ifosfamide)
AE Summary in Patients Receiving Concomitant Chemotherapy Metabolized by CYP3A4
124
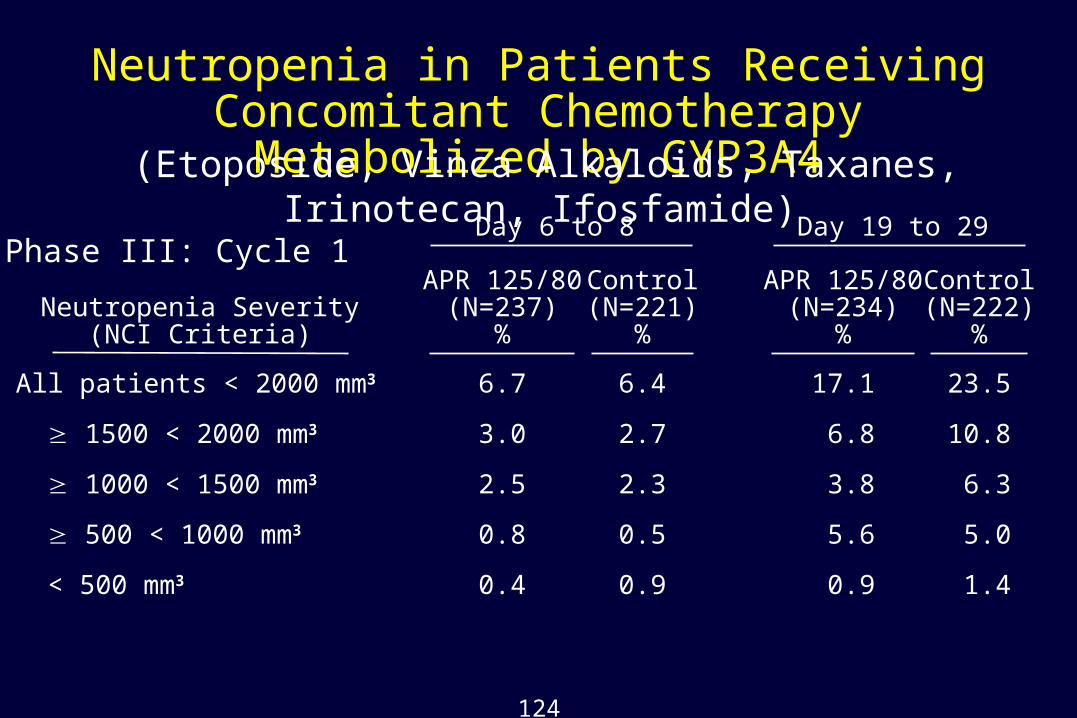
Neutropenia in Patients Receiving Concomitant Chemotherapy Metabolized by CYP3A4
(Etoposide, Vinca Alkaloids, Taxanes, Irinotecan, Ifosfamide)
All patients < 2000 mm3
1500 < 2000 mm3
1000 < 1500 mm3
500 < 1000 mm3
< 500 mm3
Neutropenia Severity(NCI Criteria)
Phase III: Cycle 1Day 6 to 8
APR 125/80(N=237)
%
6.7
3.0
2.5
0.8
0.4
Control(N=221)
%
6.4
2.7
2.3
0.5
0.9
Day 19 to 29
APR 125/80(N=234)
%
17.1
6.8
3.8
5.6
0.9
Control(N=222)
%
23.5
10.8
6.3
5.0
1.4

125
Day 6 to 8
APR 125/80(N=237)
%
6.7
3.0
2.5
0.8
0.4
Control(N=221)
%
6.4
2.7
2.3
0.5
0.9
Day 19 to 29
APR 125/80(N=234)
%
17.1
6.8
3.8
5.6
0.9
Control(N=222)
%
23.5
10.8
6.3
5.0
1.4
Neutropenia in Patients Receiving Concomitant Chemotherapy Metabolized by CYP3A4
All patients < 2000 mm3
1500 < 2000 mm3
1000 < 1500 mm3
500 < 1000 mm3
< 500 mm3
Neutropenia Severity(NCI Criteria)
Phase III: Cycle 1
No change in hematological toxicity of chemotherapy metabolized by CYP3A4
(Etoposide, Vinca Alkaloids, Taxanes, Irinotecan, Ifosfamide)

126
Percent of Patients with Neutrophil Counts <1500/mm3
(Day 19 to 29)
0
5
10
15
20
25
30
All CYP3A4 Etoposide Vinorelbine Paclitaxel
APR 125/80
Control
Pe
rce
nt o
f Pa
tien
ts
N= 266 251
Individual Chemotherapies Metabolized by CYP3A4
101 96 82 76 52 58
Phase III: Cycle 1

127
0
5
10
15
20
25
30
All CYP3A4 Etoposide Vinorelbine Paclitaxel
APR 125/80
Control
N= 106 91 52 5882 76
Pe
rce
nt o
f Pa
tien
ts
Phase III: Cycle 1
266 251
Percent of Patients with Neutropenia Adverse Experiences
Individual Chemotherapies Metabolized by CYP3A4

128
Conclusions
Safety of Aprepitant in Patients Receiving Chemotherapy Metabolized by CYP3A4
Extensive evaluation of clinical and laboratory safety– Over 250 patients per treatment group
No pattern of clinically important changes – Overall incidences of adverse experiences
• Serious AEs• Prespecified AEs
– Neutropenia • NCI criteria, adverse events

129
Safety of Aprepitant in Patient Subgroups
Demographic variables assessed during Phase III, Cycle 1– Age– Gender – Race– Primary cancer diagnosis
Aprepitant displayed a consistent, favorable safety profile

130
Safety Evaluation DuringMultiple Chemotherapy Cycles
Treatment up to 6 total cycles of chemotherapy
Data collection
– Drug-related AEs
– Serious AEs
– Discontinuations due to AEs
– Laboratory evaluations

131
Cycle 2
Cycle 3
Cycle 4
Cycle 5
Cycle 6
413
337
250
184
148
APR 125/80N
438
347
255
189
152
ControlN
Phase III
Numbers of Patients Entered into Multiple Chemotherapy Cycles

132
Drug-related AEs
Serious Clinical AEs
Discontinuations due to AEs
Serious laboratory AEs
Deaths
Percent of Patients with:
APR 125/80(N=413)
%
5.6
19.1
12.1
0.8
6.8
Control(N=438)
%
4.1
18.3
9.6
0.7
5.3
Phase III: Cycles 2-6
Safety Summary DuringMultiple Chemotherapy Cycles

133
Percent of Patients with Neutrophil Counts <1500/mm3
(Day 19 to 29)
0
5
10
15
20
25
30
1 2 3 4 5 6
APR 125/80
Control
Chemotherapy Cycle
Pe
rce
nt o
f Pa
tien
ts
N= 462 477 366 377 304 303 219 231 169 173 134 143
Chemotherapy-Induced Toxicity: Multiple Cycles

134
Aprepitant Overall Safety Conclusions
Incidences of adverse experiences similar to Standard Therapy
No significant changes in toxicity of concomitant therapies – Cisplatin– Chemotherapy, whether or not metabolized by CYP3A4– Glucocorticoids
No clinically important differences among patient subgroups– Age, gender, race, primary cancer diagnosis
Well tolerated during multiple chemotherapy cycles

135
Summation and Conclusions
EMEND® (aprepitant)

136
A Major Advance in the Supportive Care of Cancer Patients
Aprepitant
A cancer diagnosis has profound implications– Life-threatening disease – Potentially disruptive and debilitating treatment
• Daily function can be compromised by nausea and vomiting

137
A Major Advance in the Supportive Care of Cancer Patients
Aprepitant
A cancer diagnosis has profound implications– Life-threatening disease – Potentially disruptive and debilitating treatment
• Daily function can be compromised by nausea and vomiting
5-HT3 receptor antagonists introduced into clinical practice in 1991– Quickly recognized as a therapeutic advance

138
A Major Advance in the Supportive Care of Cancer Patients
Aprepitant
A cancer diagnosis has profound implications– Life-threatening disease – Potentially disruptive and debilitating treatment
• Daily function can be compromised by nausea and vomiting
5-HT3 receptor antagonists introduced into clinical practice in 1991– Quickly recognized as a therapeutic advance
Many patients still experience nausea and vomiting despite best available therapy
– Ranked among the most distressing symptoms• Delayed symptoms remain difficult to treat

139
Patients treated with best therapy available today
Many Patients Still Experience Nausea andVomiting After Highly Emetogenic Chemotherapy
Protocol 052 Protocol 054100
90
80
70
60
50
400
Per
cent
of P
atie
nts
0 12 24 36 48 60 72 1081209684
100
90
80
70
60
50
400
Per
cent
of P
atie
nts
0 12 24 36 48 60 72 1081209684
Hours Hours
Time to First Emesis or Use of Rescue
ControlControl
N=260 N=263

140
Evaluated in 7-year multinational clinical development program– >3000 patients and subjects in total
• >1400 patients in cancer chemotherapy trials
Unique Attributes for Patients Receiving Highly Emetogenic Chemotherapy
Aprepitant

141
Evaluated in 7-year multinational clinical development program– >3000 patients and subjects in total
• >1400 patients in cancer chemotherapy trials
Developed for use in conjunction with standard agents– Unprecedented efficacy
• Benefit sustained over multiple cycles
Unique Attributes for Patients Receiving Highly Emetogenic Chemotherapy
Aprepitant

142
Evaluated in 7-year multinational clinical development program– >3000 patients and subjects in total
• >1400 patients in cancer chemotherapy trials
Developed for use in conjunction with standard agents– Unprecedented efficacy
• Benefit sustained over multiple cycles
Very well tolerated– Across patient subgroups and concomitant therapies
Unique Attributes for Patients Receiving Highly Emetogenic Chemotherapy
Aprepitant

143
100
90
80
70
60
50
400
Per
cent
of P
atie
nts
0 12 24 36 48 60 72 1081209684
100
90
80
70
60
50
400
Per
cent
of P
atie
nts
0 12 24 36 48 60 72 1081209684
Protocol 052 Protocol 054
Hours Hours
APR 125/80 RegimenAPR 125/80 Regimen
Time to First Emesis or Use of Rescue TherapyMore Patients Benefit with Aprepitant
Control Control
APR N=260 Control N=260 APR N=260 Control N=263

144
Aprepitant: Conclusions
A new class of antiemetic therapy
– First NK1 receptor antagonist introduced into clinical practice
• Novel mechanism with distinct clinical benefits
Marked reduction in emesis and need for rescue medication
– Aprepitant improves the best available antiemetic therapy
May alter an enduring perception of cancer chemotherapy
– Nausea and vomiting need not be inevitable

145
Proposed Indication
EMEND, in combination with other antiemetic agents, is indicated for the prevention of acute and delayed nausea and vomiting associated with initial and repeat courses of highly emetogenic cancer chemotherapy, including high-dose cisplatin.















![[Product Monograph Template - Standard] · 2018-03-06 · PRODUCT MONOGRAPH . EMEND ® aprepitant capsules . 80 and 125 mg . Neurokinin 1 (NK. 1) receptor antagonist . Merck Canada](https://static.documents.pub/doc/80x56/5ea7e50e6fc5d14308453e78/product-monograph-template-standard-2018-03-06-product-monograph-emend-.jpg)

