1 JF Geschwind, MD Professor Radiology, Surgery, and Oncology Director, Vascular and Interventional Radiology Johns Hopkins University School of Medicine Baltimore, Maryland Drug-Eluting Beads Chemoembolization (DEBDOX) for Hepatocellular Carcinoma in 2011: The Case for a Treatment Standard
Transcript
1
JF Geschwind, MDProfessor Radiology, Surgery, and Oncology
Director, Vascular and Interventional Radiology
Johns Hopkins University School of Medicine
Baltimore, Maryland
Drug-Eluting Beads Chemoembolization (DEBDOX) for Hepatocellular Carcinoma in
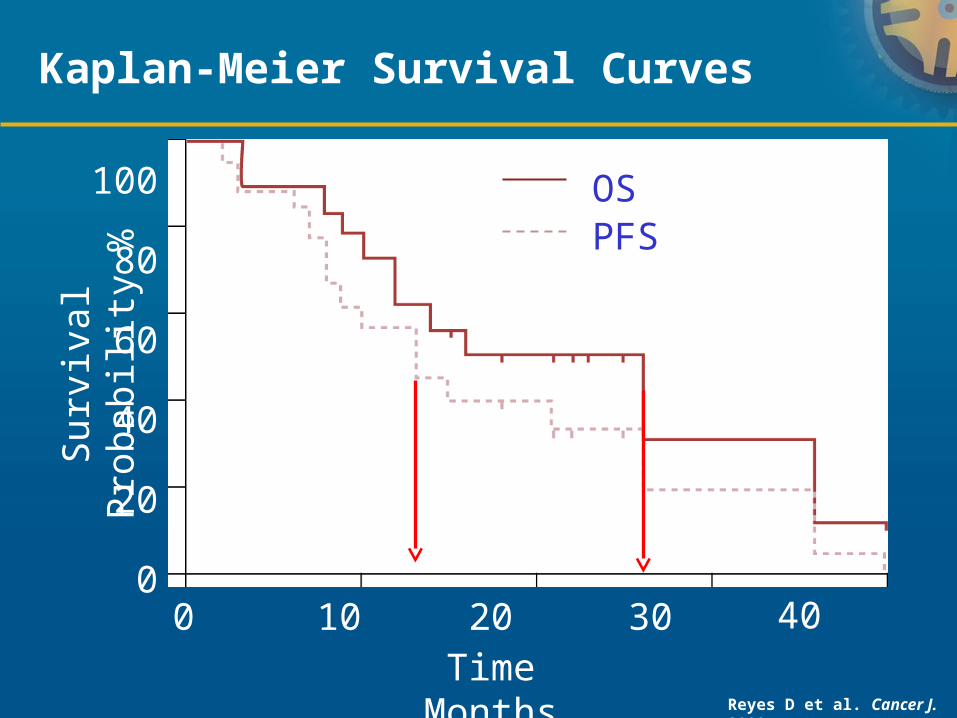
*p=0.0001 for analysis with assumption of independence of events
DC Bead® is approved in 40 countries worldwide, including the
USA (as LC Bead™) and Europe2
10
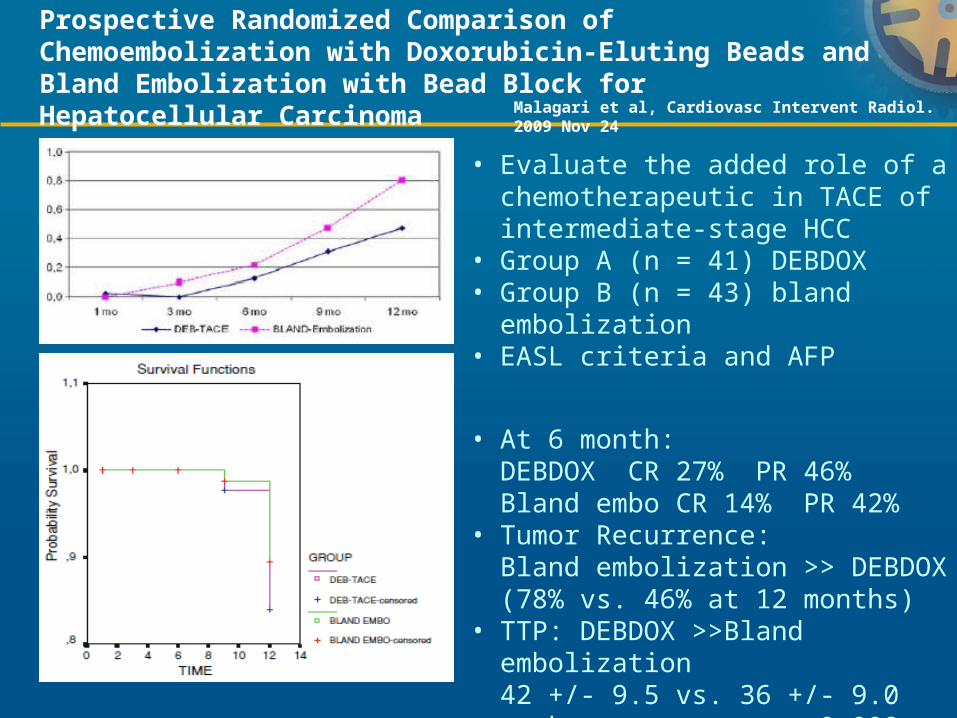
Prospective Randomized Comparison of Chemoembolization with Doxorubicin-Eluting Beads and Bland Embolization with Bead Block for Hepatocellular Carcinoma
• Evaluate the added role of a chemotherapeutic in TACE of intermediate-stage HCC
• Group A (n = 41) DEBDOX• Group B (n = 43) bland embolization• EASL criteria and AFP
Lammer (2008) 3iiDiii 30 A (26)/B (4) 40% (RECIST)
44% (EASL)
N/A
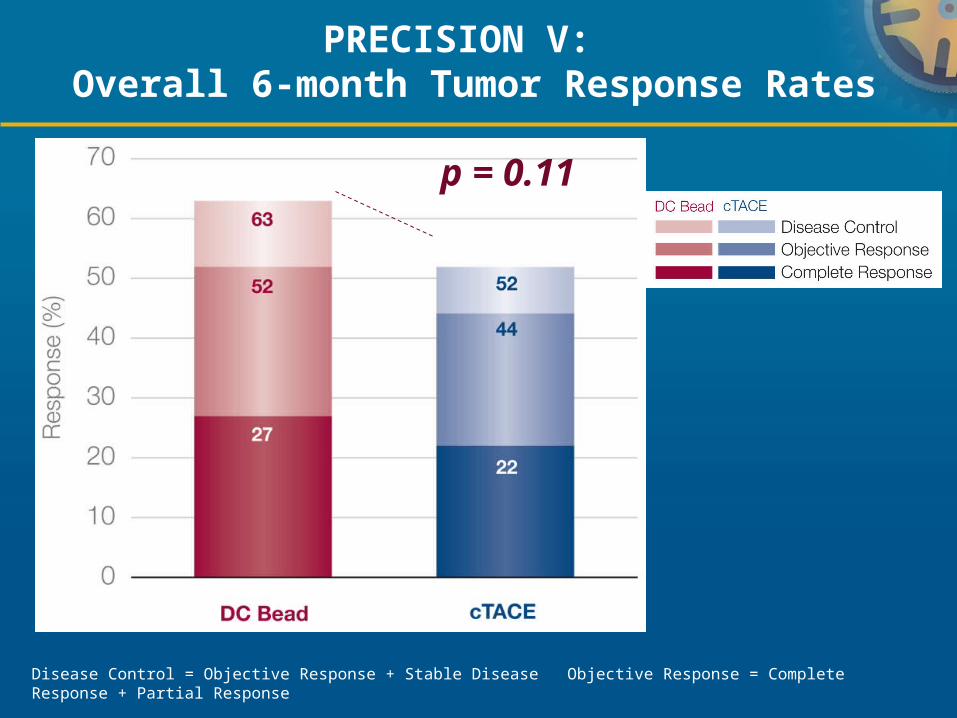
Lencioni-PRECISION V (2010)
1iiDiii 212 (102 DEB)
A (77)/B (16) 52% (RECIST) 63% (EASL)
N/A
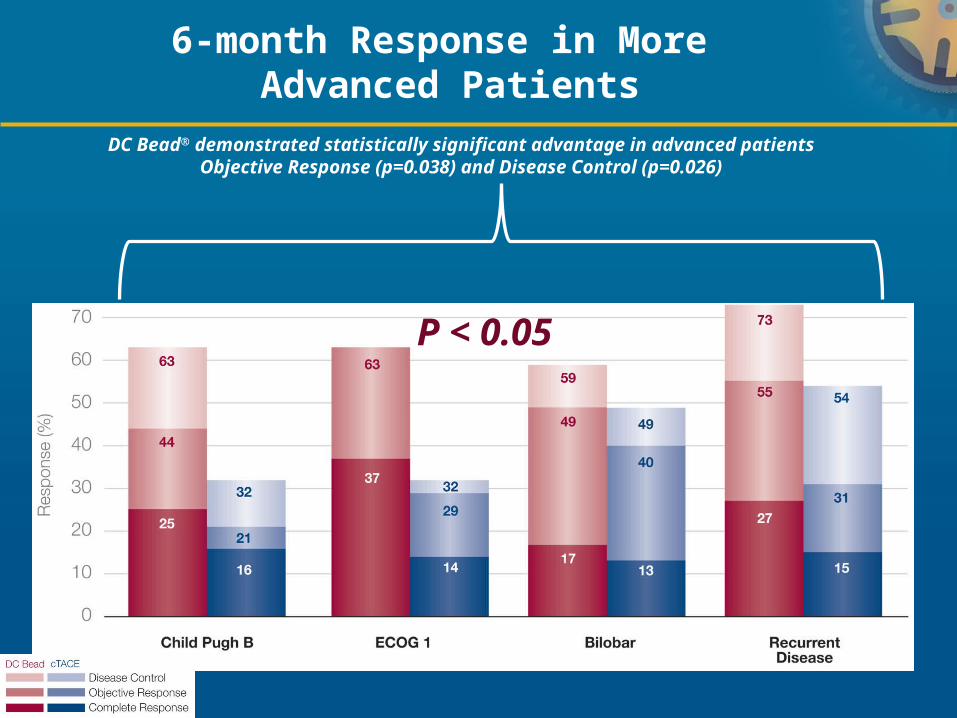
*Survival data on DEBDOX are restricted to less than 4 years and longer term follow-up results will be published soon.**DEB vs TACE: p=0.11. DEB advantage for CP B/ECOG 1/bilobar or recurrence: p= 0.038. Fewer dox side effects: p=0.0001
2. How? Technical Considerations: Towards a Standardized Protocol
Drug delivery not embolotherapy!Drug delivery not embolotherapy!
1. Choice of particle size2. Choice of drug: doxorubicin vs. irinotecan3. Catheter placement4. Actual delivery (how? Contrast or not?)5. End point (?)
14
1.
Optimizing Drug Delivery: Importance of Particle Size
15
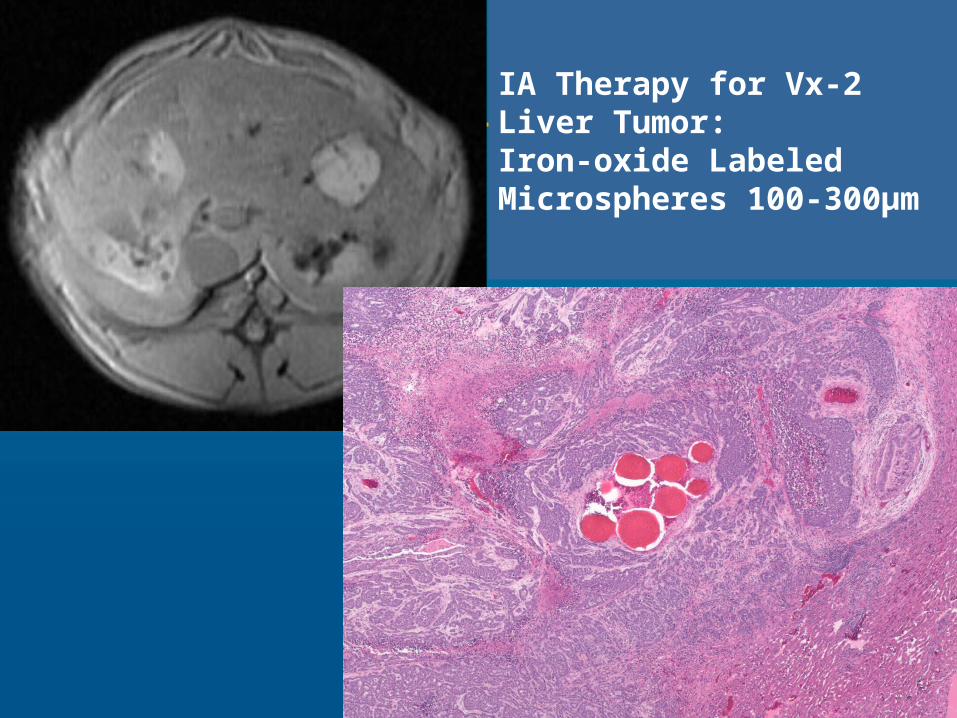
Distribution of iron oxide-containing Embosphere particles after transcatheter arterial embolization in an animal model of liver cancer: evaluation with MR imaging and implication for therapy.Lee KH, Liapi E, Vossen JA, Buijs M, Ventura VP, Georgiades C, Hong K, Kamel I, Torbenson MS, Geschwind JF. J Vasc Interv Radiol. 2008 Oct;19(10):1490-6.
IA Therapy for Vx-2 Liver Tumor:Iron-oxide Labeled Microspheres 300-500µm
16
IA Therapy for Vx-2 Liver Tumor:Iron-oxide Labeled Microspheres 100-300µm
17
Drug-Eluting Beads for liver embolization: Concentration of doxorubicin in tissue and in beads in a pig model
100-300μm or 700-900μm loaded with 37.5 mg dox/mL Livers analyzed 28 or 90 days after embolization DEBs eluted 43% of their initial drug load after 28 days and
89% after 90 days Drug detected at distances as far as 600μm from bead
edge 100-300μm induced more necrosis than 700-900μm
beads (p= .0036)
MicroCT analysis: Small beads distal arteries + homogeneous distribution
Doxorubicin concentration declines with increasing distances from the bead edge (still enough to be cytotoxic in vitro)
Namur J et al. J Vasc Interv Radiol. 2010 Feb;21(2):259-67Dreher M et al. GEST 2010
18
1.
Optimizing Drug Delivery: Importance of Particle Size
SMALL
19
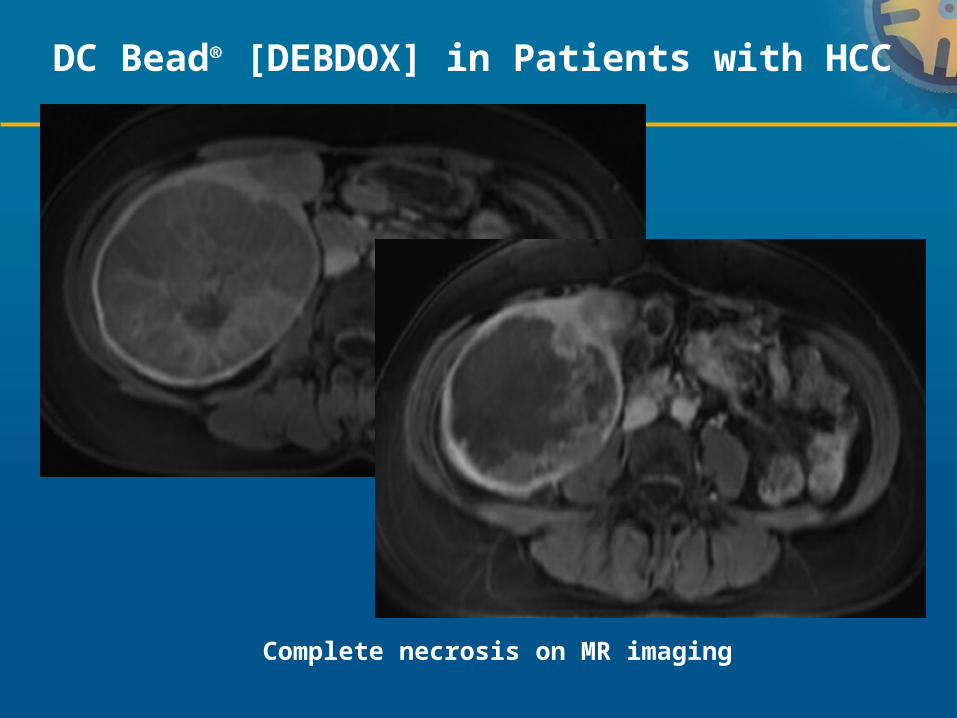
Complete necrosis on MR imaging
DC Bead® [DEBDOX] in Patients with HCC
20
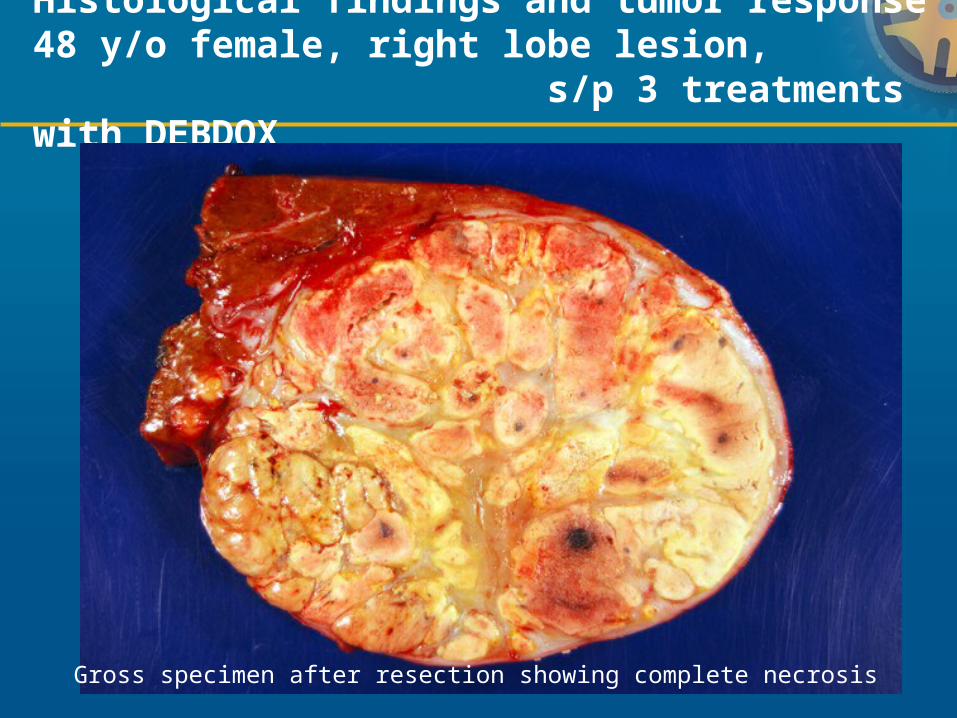
Histological findings and tumor response 48 y/o female, right lobe lesion, s/p 3 treatments with DEBDOX
Gross specimen after resection showing complete necrosis
21
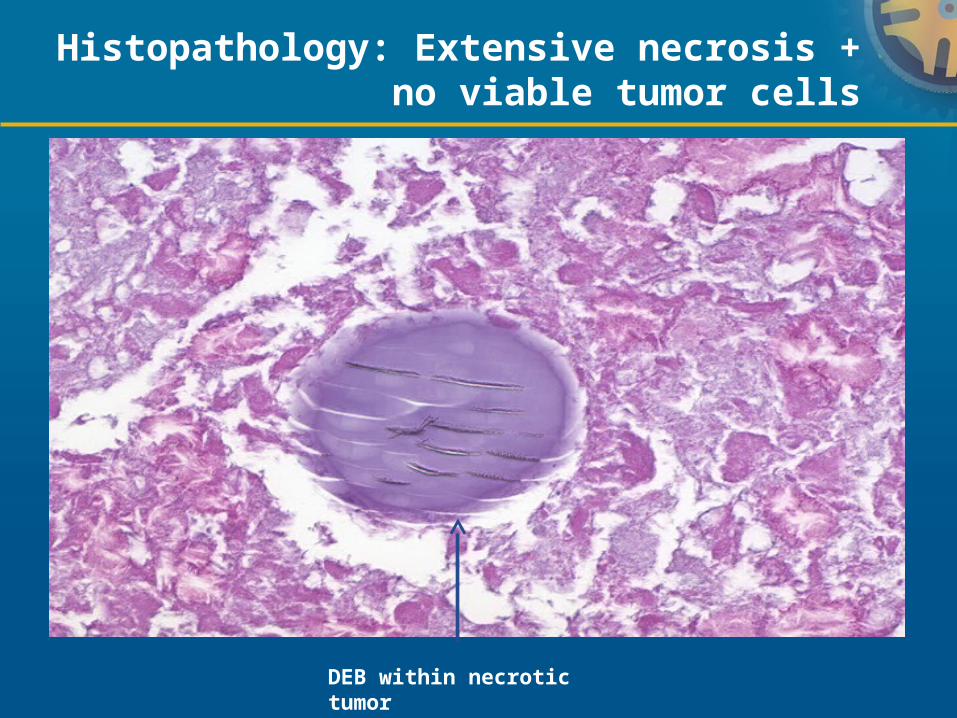
Histopathology: Extensive necrosis + no viable tumor cells
DEB within necrotic tumor
22
2.
Optimizing Drug Delivery: What drug?
Doxorubicin: HCC, NET
Irinotecan: CRC (?), No data
23
3.
Catheter Placement
Selective?
YES
1.Better control
2.Minimize reflux
3.Better visualization of beads
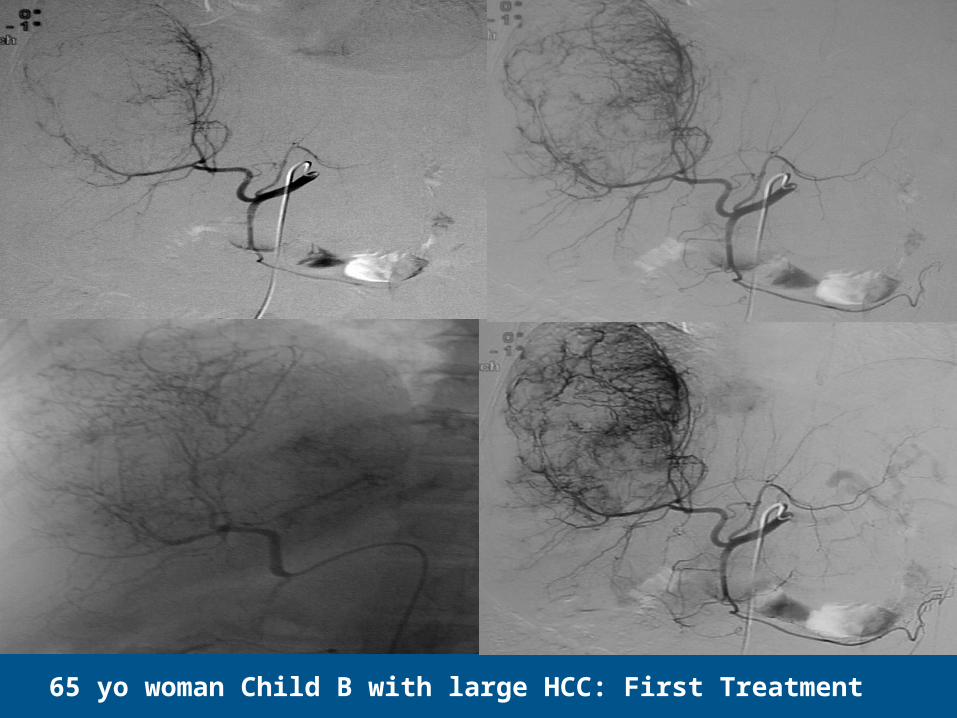
2465 yo woman Child B with large HCC: First Treatment
25Post-treatment #1: Residual viable tumor
Pre-treatment
26
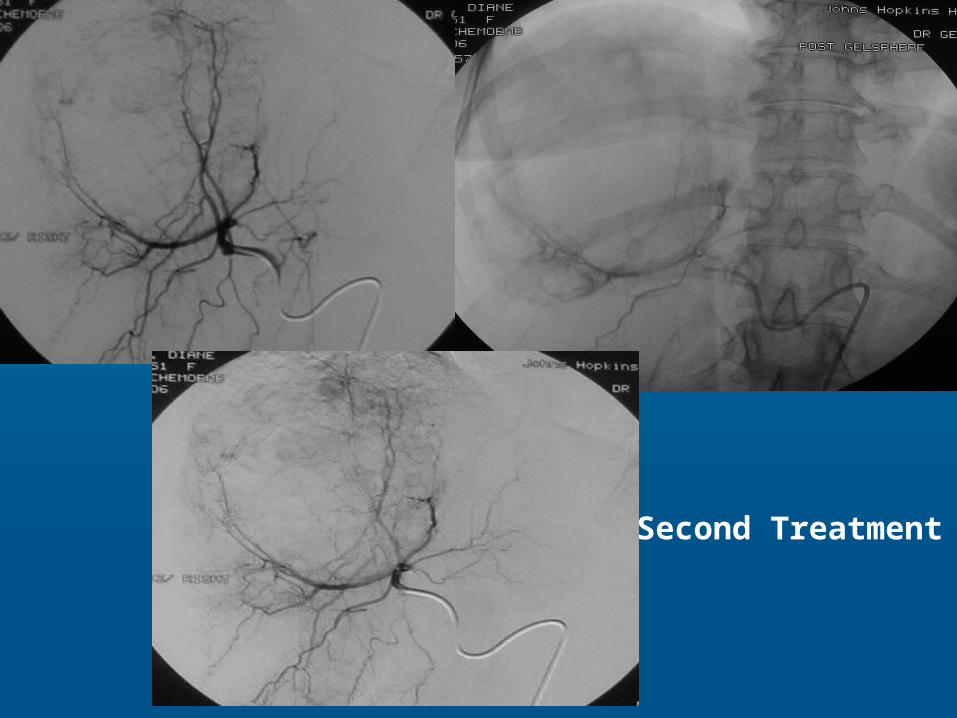
Second Treatment
27
MRI Post-treatment #2No recurrence 29 months post initial treatment
28
4.Actual Delivery
1. Must use microcatheter2. Use cone beam CT for targeting3. Visibility of beads critical4. Mix with contrast (4:1)5. Inject slowly (1 ml/min)
29
Usefulness of Cone Beam CT
Imaging: Research and Clinical Use
1. Visualize the tumor2. Target the tumor (drug delivery)3. Proof of success = predicting response:
Tumor perfusionTumor segmentation
30
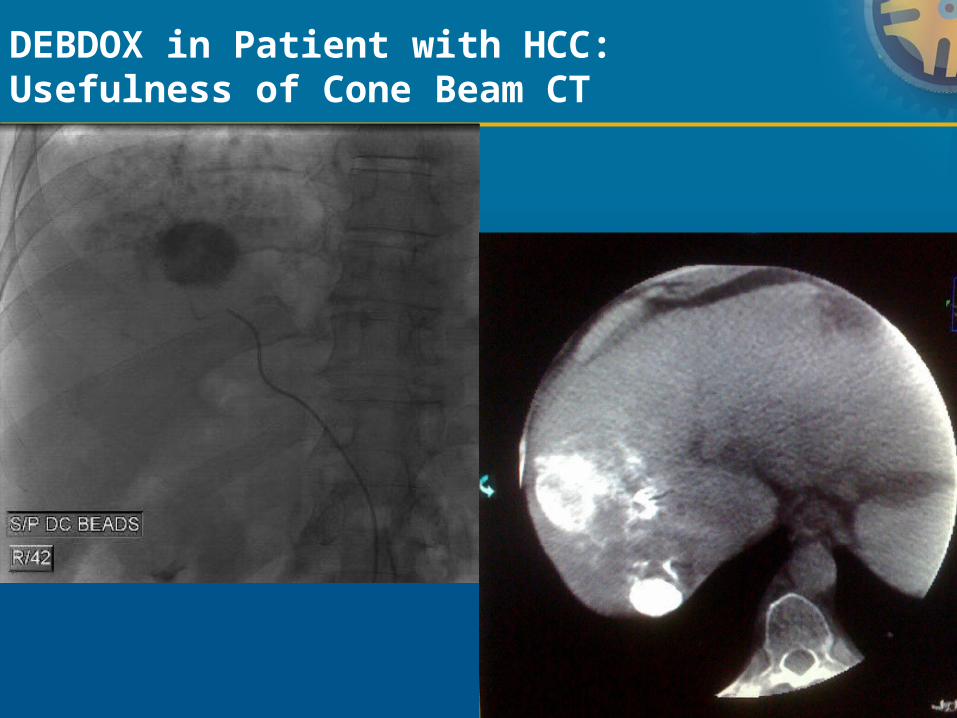
DEBDOX in Patient with HCC: Usefulness of Cone Beam CT
31
5.
End Points
1. Entire planned dose administered
2. Stop before stasis!!
3. No need for further bland embolization
32
ConclusionsDrug-Eluting Beads in 2011: Why, how and when?
WHY? Rationale ESTABLISHED HOW? Technical considerations NEARING CONSENSUS
(panel of experts) Bead size: Nearly there! SMALL >>large Drug: Doxorubicin (YES) vs. irinotecan (NO) Catheter position: SELECTIVE End point: FULL DOSE (no stasis) Unknown: Frequency treatment/dosing
WHEN? HCC: Good data
NET: On-going studies, CRC: On-going studies
33
DISCLOSURES
Grant support:
Genentech, Bayer Healthcare, Nordion, Biocompatibles, Abdulmalik Research Fund, Alice Pratt Liver Cancer Fund, NIH/NCI, DOD, RSNA, SIR
Consultant:
Philips Medical System, Bayer Healthcare, Nordion, Biocompatibles, Guerbet, PreScience
Patent:
Use of 3-BrPA as an anti-cancer agent Founder: PreScience Pharma








![750824 Nepalese 1NedM...BROTHER / bfHobbffHHoobfHo\ \\\ jf jjff jf EffO{ SISTER / lbbL jf alxgL GRANDFATHER / afh] afh] GRANDMOTHER/ aHo}aHo} CHILDREN / afnaflnsfafnaflnsfafnaflnsf](https://static.documents.pub/doc/80x56/60a55d6948a28404f924d965/750824-nepalese-brother-bfhobbffhhoobfho-jf-jjff-jf-effo-sister-lbbl.jpg)















