1 QF-PCR stand-alone prenatal QF-PCR stand-alone prenatal diagnosis: the initial London diagnosis: the initial London experience. experience. Caroline Mackie Ogilvie Cytogenetics Department Guy’s Hospital London
Transcript
1
QF-PCR stand-alone prenatal diagnosis: QF-PCR stand-alone prenatal diagnosis: the initial London experience.the initial London experience.
Caroline Mackie Ogilvie
Cytogenetics Department
Guy’s Hospital
London
2
Guy’s QF-PCR dataGuy’s QF-PCR data
2000 - 2007
Total samples tested: 23,311
CVS 6729 (28.9%)
AF 16582 (71.1%)
97% of samples receive a result within one working day
3
Should we karyotype pregnancies at Should we karyotype pregnancies at risk of Down syndrome?risk of Down syndrome?
• 32,674 pregnant women having invasive PND in London/South East
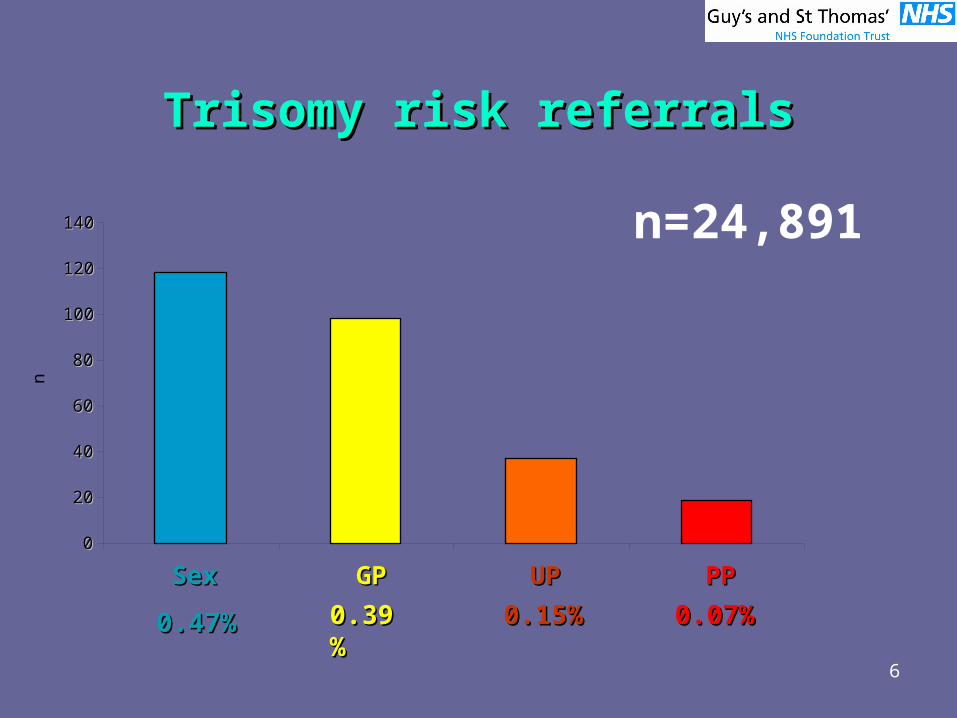
• 24,891 (76.2%) were referred for exclusion of Down syndrome
• others at risk of single gene disorders or complex chromosome abnormalities
4
• 24,891 pregnancies referred for exclusion of T21
• 118 sex chromosome abnormalities
• 153 other abnormalities
5
Good prognosisGood prognosis::
– balanced rearrangementsbalanced rearrangements– variant regionsvariant regions
Uncertain prognosisUncertain prognosis::
– small marker chromosomessmall marker chromosomes– mosaic anomaliesmosaic anomalies
1 liveborn (10q del) minor facial dysmorphism but normal development at 20 months
2 miscarried
4 outcome unknown, of which 1 = T16, 2 = 46,XX,del(18), 1=46,XX,add(9)
11 TOP (61%)
8
9
Advantages of QF-PCR stand-alone Advantages of QF-PCR stand-alone testingtesting
• uncertain or harmless karyotypes not detected, reducing anxiety and follow-up studies
• no residual anxiety while waiting for karyotype results
• better use of resources
10
New service May 2007New service May 2007
All abnormal QF-PCR results followed up by karyotype analysis
11
Criteria for karyotypingCriteria for karyotyping
Clinical indication, viz:
• structural abnormality on U/S
• 2 or more soft markers for trisomy 21
• nuchal measurement >3mm at below 14 weeks gestation
• nuchals measurement >6mm for gestations >= 14 weeks
• family history of chromosome rearrangement
12
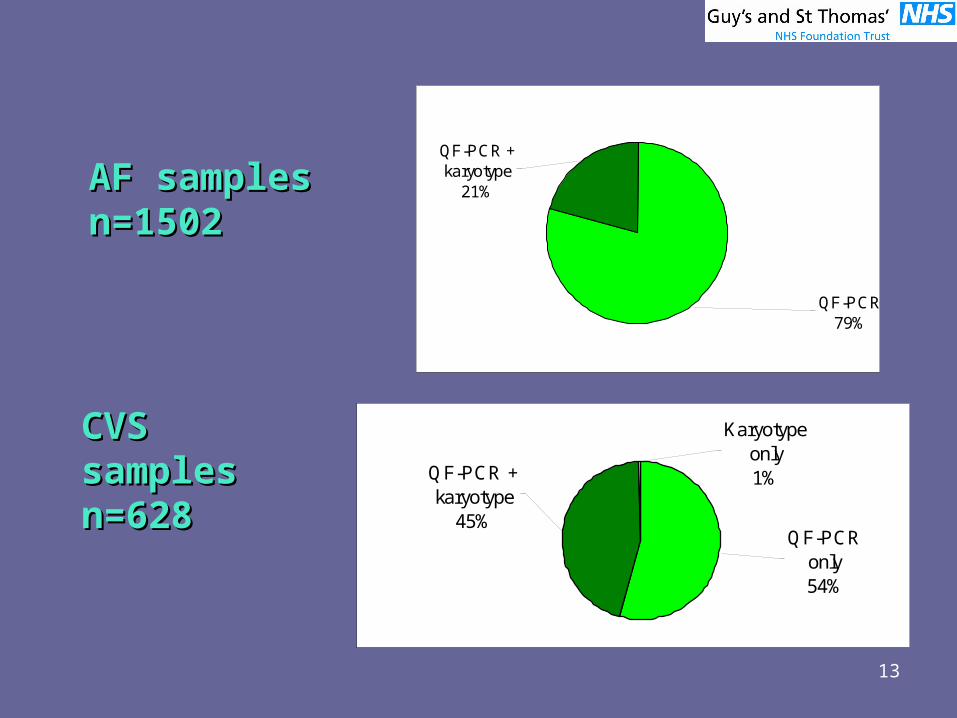
Data from 3 London labsData from 3 London labs
01/05/2007 – 30/11/2007
Consortium samples only
13
QF-PCR + karyotype
21%
QF-PCR79%
AF samples AF samples n=1502n=1502
Karyotype only1%
QF-PCR only54%
QF-PCR + karyotype
45%
CVS samples CVS samples n=628n=628
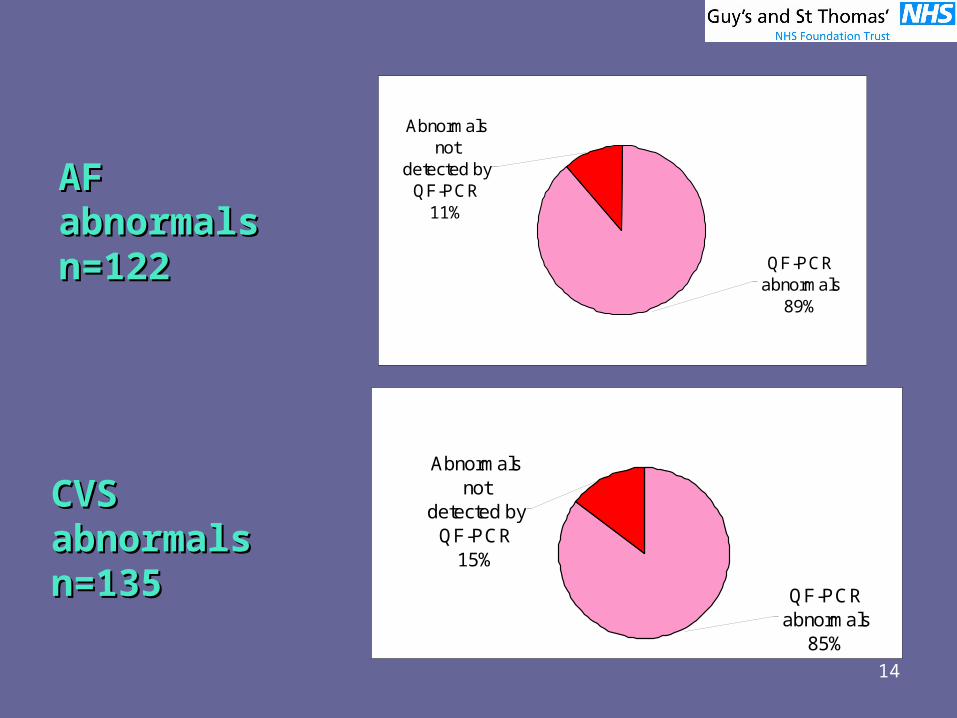
14
Abnormals not
detected by QF-PCR
11%
QF-PCR abnormals
89%
Abnormals not
detected by QF-PCR
15%
QF-PCR abnormals
85%
AF abnormals AF abnormals n=122n=122
CVS abnormals CVS abnormals n=n=135135
15
Abnormalities not detected by Abnormalities not detected by QF-PCRQF-PCR
Detection rate in karyotyped AF 3%
Detection rate in karyotyped CVS 7%
No abnormal babies reported to date.
16
One pregnancy:• QF-PCR only at CVS• ultrasound showed severe IUGR and abnormal placenta
at 26 weeks • follow-up amnio: mos tetraploidy • pregnancy terminated • fetal blood showed normal karyotype
Tetraploid cell line probably confined to placenta leading to placental insufficiency
Abnormalities not detected by Abnormalities not detected by QF-PCRQF-PCR
17
NT >3mm<4mmNT >3mm<4mm
“An alternative strategy whereby qf-PCR is the main method of analysis and full karyotyping is reserved for those cases with a minimum fetal NT thickness of 4 mm would require full karyotyping in 10.1% of the cases, would identify 99.0% of the significant abnormalities, and would cost 60% less than full karyotyping for all.”
Chitty et al. (2006) BMJ 25;332(7539):452-5.
18
NT >3mm<4mmNT >3mm<4mm
normal/trisomy97%
abnormality not detected by QF-
PCR3%
19
NT >3mm<4mmNT >3mm<4mm
2 abnormal karyotypes in this group• 47,XY,+22• 47,XX,+mar[19]/46,XX[28]
– v small non-satellited marker, apparently all heterochromatin
– ?CPM– follow-up amnio and parental bloods requested, but