56
1 Replace Heparin and Improve Outcomes New Antithrombotic Strategies in ACS Patients Undergoing PCI ANG-PSL-XXX-XXX
| Date post: | 02-Jan-2016 |
| Category: |
Documents |
| Upload: | erica-mclaughlin |
| View: | 224 times |
| Download: | 10 times |
1
Replace Heparin and Improve OutcomesNew Antithrombotic Strategies in ACS Patients Undergoing PCI
ANG-PSL-XXX-XXX

2
Overview
• Thrombin’s critical role
• Clot burden in the ACS patient
• Mechanistic rationale for switching patients to ANGIOMAX®
(bivalirudin) for PCI
• Why is there concern about switching anticoagulants in ACS treatment?– Lessons from SYNERGY
• Clinical evidence in support of switching to ANGIOMAX
• ACUITY PCI Subgroup Analysis: 1-Year Mortality Results
ACS=acute coronary syndromes; ACUITY=Acute Catheterization and Urgent Intervention Triage strategY; AT=antithrombin; PCI=percutaneous coronary intervention; SYNERGY=Superior Yield of the New Strategy of Enoxaparin, Revascularization, and Glycoprotein IIb/IIIa Inhibitors.

3
Why ANGIOMAX® (bivalirudin)?The Critical Role of Thrombin• Thrombin is the link between vessel injury, coagulation,
and platelet response
Vessel Injury
Platelet activation
Platelet aggregation
Fibrinogen
Fibrin
Thrombin
Plasma clotting factors
Prothrombin
Tissue factor
Collagen
ADPplatelet
activation
ADP TXA2=adenosine diphosphate/thromboxane A2.
Coughlin SR. Nature. 2000;407:258-264; Monroe DM et al. Arterioscler Thromb Vasc Biol. 2002;22:1381-1389.

4
Thrombin Promotes Platelet Activation and Clotting
• Thrombin is the link between tissue injury, coagulation, and platelet response
Coughlin SR. Nature. 2000;407:258-264; Monroe DM et al. Arterioscler Thromb Vasc Biol. 2002;22:1381-1389.
Platelet activation
Platelet Aggregation
Fibrinogen
Fibrin
Thrombin is a critical mediator in hemostasis and thrombosis
Thrombinbegetsthrombin
Thrombin is a platelet agonist;
elicits multiple responses in
plateletsThrombin
Plasma clotting factors
Prothrombin

5
Indirect inhibition by heparin requires the presence of AT, the actual inhibitor.
Indirect Versus Direct Thrombin Inhibition
ANGIOMAX® (bivalirudin) inhibits thrombin directly with high affinity and specificity.
ANGIOMAX provides rapid, effective thrombin inhibition to prevent thrombosis and thrombin-mediated platelet effects.
AT=antithrombin.Hirsh J et al. Chest. 2001;119(1 suppl):64S-94S.Weitz JI et al. Thromb Res. 2002;106:V275-V284.
6
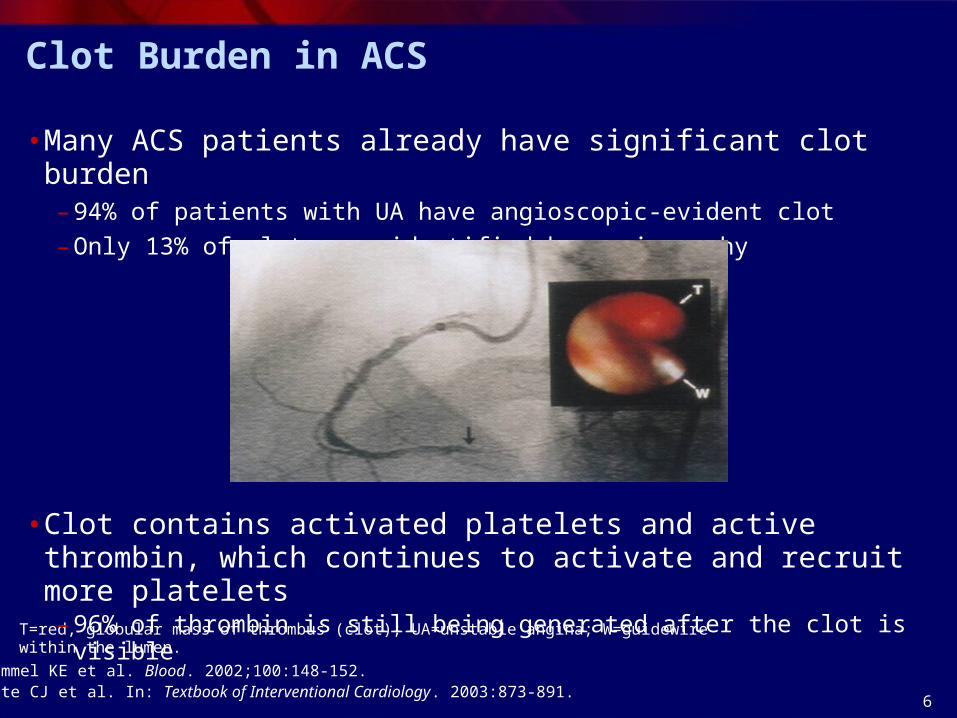
Clot Burden in ACS
• Many ACS patients already have significant clot burden– 94% of patients with UA have angioscopic-evident clot
– Only 13% of clots are identified by angiography
Brummel KE et al. Blood. 2002;100:148-152.White CJ et al. In: Textbook of Interventional Cardiology. 2003:873-891.
T=red, globular mass of thrombus (clot); UA=unstable angina; W=guidewire within the lumen.
• Clot contains activated platelets and active thrombin, which continues to activate and recruit more platelets – 96% of thrombin is still being generated after the clot is visible
7
0
50
100
0.1 0.2 0.4 1.0 2.0 3.0 4.0
Soluble thrombin Clot-bound thrombin
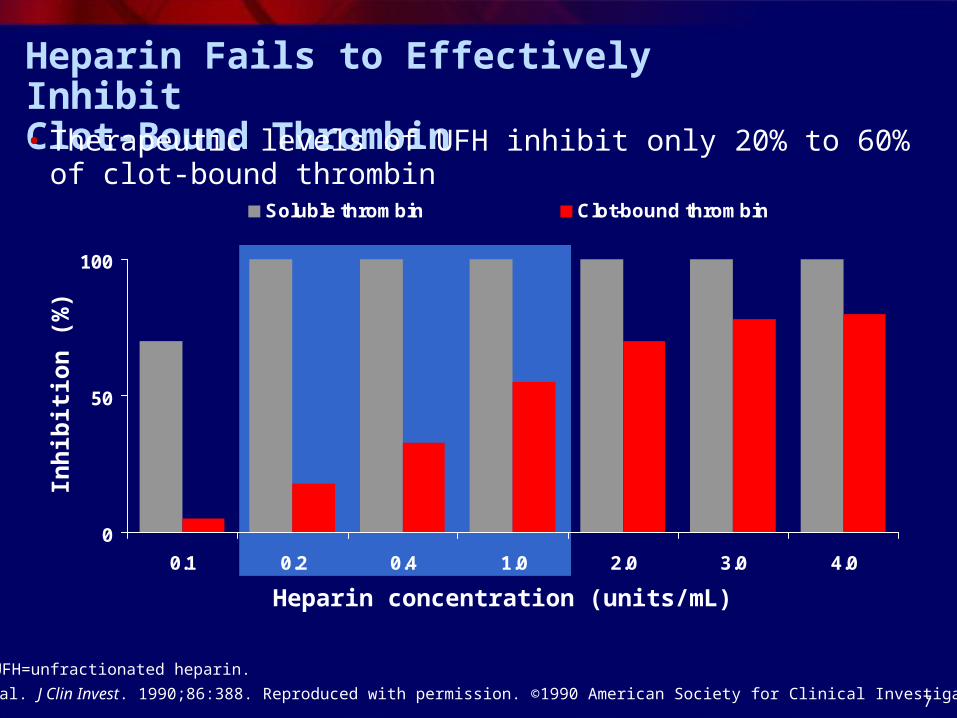
Heparin Fails to Effectively Inhibit Clot-Bound Thrombin• Therapeutic levels of UFH inhibit only 20% to 60% of clot-bound
thrombin
Heparin concentration (units/mL)
Inh
ibit
ion
(%
)
Weitz JI et al. J Clin Invest. 1990;86:388. Reproduced with permission. ©1990 American Society for Clinical Investigation.
UFH=unfractionated heparin.

8
87
10096 100
0
20
40
60
80
100
Solublethrombin
Clot-boundthrombin
0.5 M ANGIOMAX
1.0 M ANGIOMAX
Mean inhibition of fibrinopeptide A production by ANGIOMAX
Data on file. The Medicines Company, Parsippany, NJ.
ANGIOMAX® (bivalirudin) Inhibits Clot-Bound and Circulating Thrombin
Inh
ibit
ion
(%
)
• ANGIOMAX is 100% effective against clot-bound thrombin
9
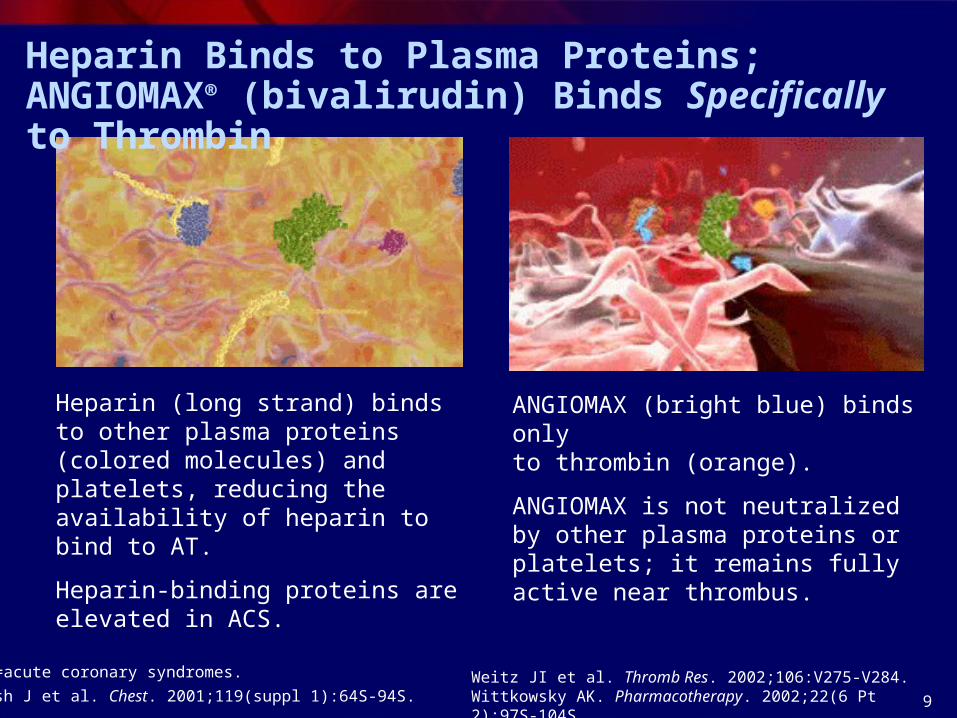
Heparin (long strand) binds to other plasma proteins (colored molecules) and platelets, reducing the availability of heparin to bind to AT.
Heparin-binding proteins are elevated in ACS.
Heparin Binds to Plasma Proteins; ANGIOMAX® (bivalirudin) Binds Specifically to Thrombin
ANGIOMAX (bright blue) binds onlyto thrombin (orange).
ANGIOMAX is not neutralized by other plasma proteins or platelets; it remains fully active near thrombus.
ACS=acute coronary syndromes.
Hirsh J et al. Chest. 2001;119(suppl 1):64S-94S.Weitz JI et al. Thromb Res. 2002;106:V275-V284.Wittkowsky AK. Pharmacotherapy. 2002;22(6 Pt 2):97S-104S.

10
Heparin is neutralized by PF4, which is present in high concentrations near vascular injury.
Thrombin continues activating platelets.
PF4/heparin complex antibodies activate platelets, causing thrombocytopenia as well as HIT/TS.
ANGIOMAX® (bivalirudin) does not bind to PF4, and remains fully active.
There is no risk of HIT/TS or other thrombotic events associated with PF4/heparin antibodies.
Consequences of Nonspecific Binding
HIT/TS=heparin-induced thrombocytopenia thrombosis syndrome; PF4=platelet factor 4.Weitz JI et al. Thromb Res. 2002;106:V275-V284.Williams RT et al. Circulation. 2003;107:2307-2312.
11
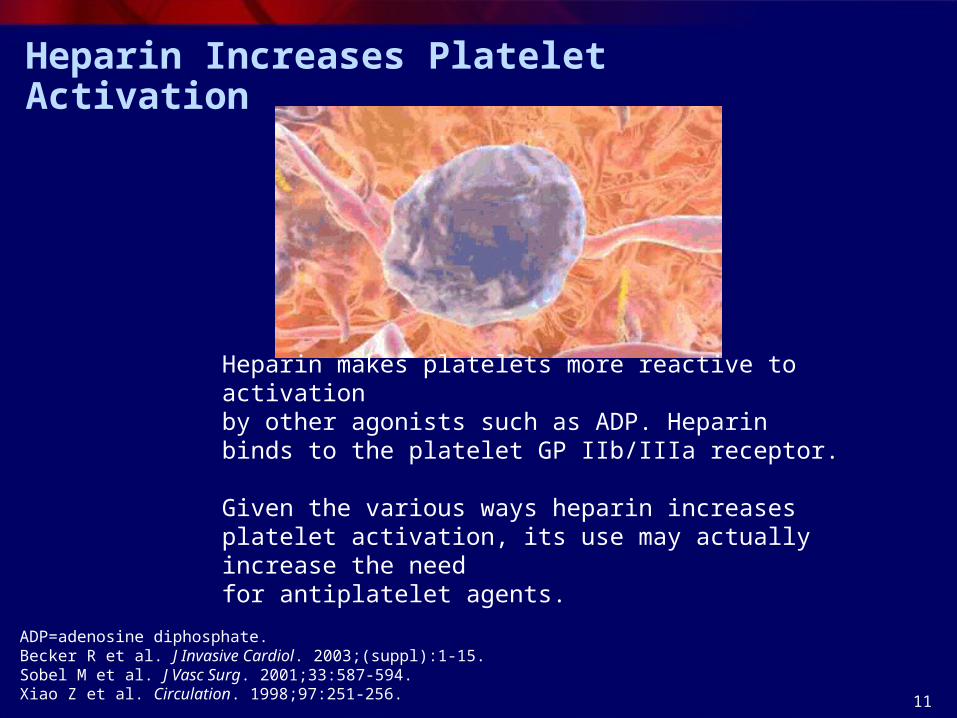
Heparin Increases Platelet Activation
Heparin makes platelets more reactive to activation by other agonists such as ADP. Heparin binds to the platelet GP IIb/IIIa receptor.
Given the various ways heparin increases platelet activation, its use may actually increase the need for antiplatelet agents.
ADP=adenosine diphosphate.Becker R et al. J Invasive Cardiol. 2003;(suppl):1-15. Sobel M et al. J Vasc Surg. 2001;33:587-594.Xiao Z et al. Circulation. 1998;97:251-256.
12
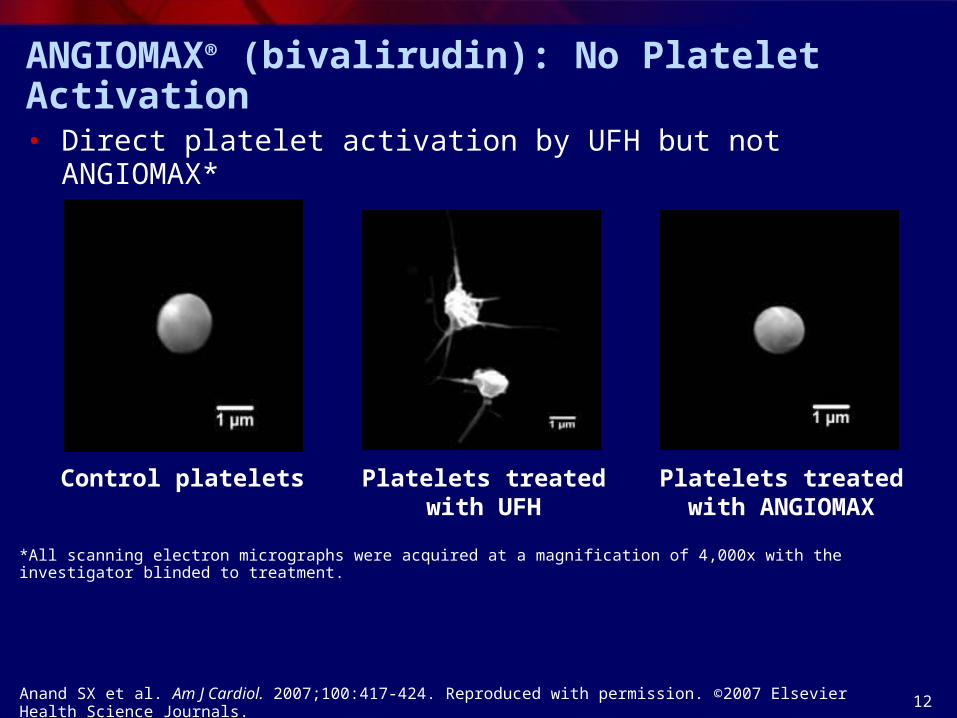
ANGIOMAX® (bivalirudin): No Platelet Activation
*All scanning electron micrographs were acquired at a magnification of 4,000x with the investigator blinded to treatment.
Control platelets
• Direct platelet activation by UFH but not ANGIOMAX*
Anand SX et al. Am J Cardiol. 2007;100:417-424. Reproduced with permission. ©2007 Elsevier Health Science Journals.
Platelets treated with UFH
Platelets treated with ANGIOMAX
13
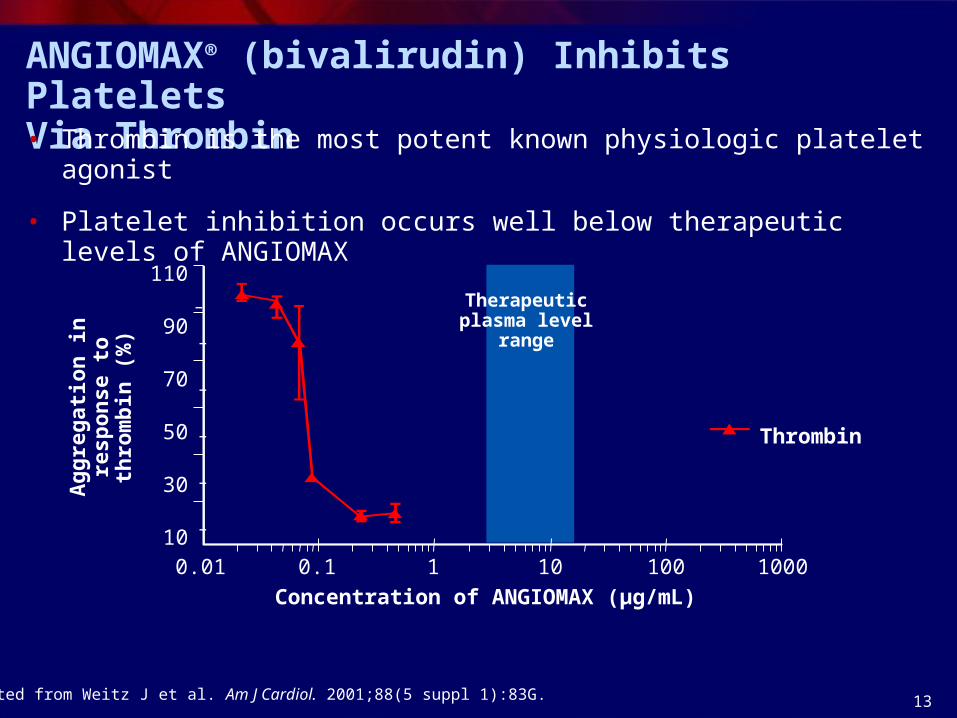
ANGIOMAX® (bivalirudin) Inhibits Platelets Via Thrombin• Thrombin is the most potent known physiologic platelet agonist
• Platelet inhibition occurs well below therapeutic levels of ANGIOMAX
Adapted from Weitz J et al. Am J Cardiol. 2001;88(5 suppl 1):83G.
110
90
70
50
30
100.01 0.1 1 10 100 1000
Concentration of ANGIOMAX (μg/mL)
Thrombin
Therapeutic plasma level range
Ag
gre
gat
ion
in
resp
on
se t
o t
hro
mb
in
(%)

14
Return to Hemostasis—Safety Advantage
ANGIOMAX® (bivalirudin) is cleaved by thrombin, allowing thrombin to quickly recover hemostatic activity upon discontinuation of ANGIOMAX.2
The natural reversibility and the short, 25-minute half-life may explain the significantly lower bleeding rates seen in clinical trials.3
When heparin dissociates from cells/proteins, there can be an anticoagulant effect even when it's not needed. This may explain the prolonged bleeding risk after discontinuation of heparin.1
1. Hirsh J et al. Chest. 2001;119(suppl 1):64S-94S.2. Weitz JI et al. Thromb Res. 2002;106:V275-V284.3. ANGIOMAX (bivalirudin) [prescribing information]; December 6, 2005.
15
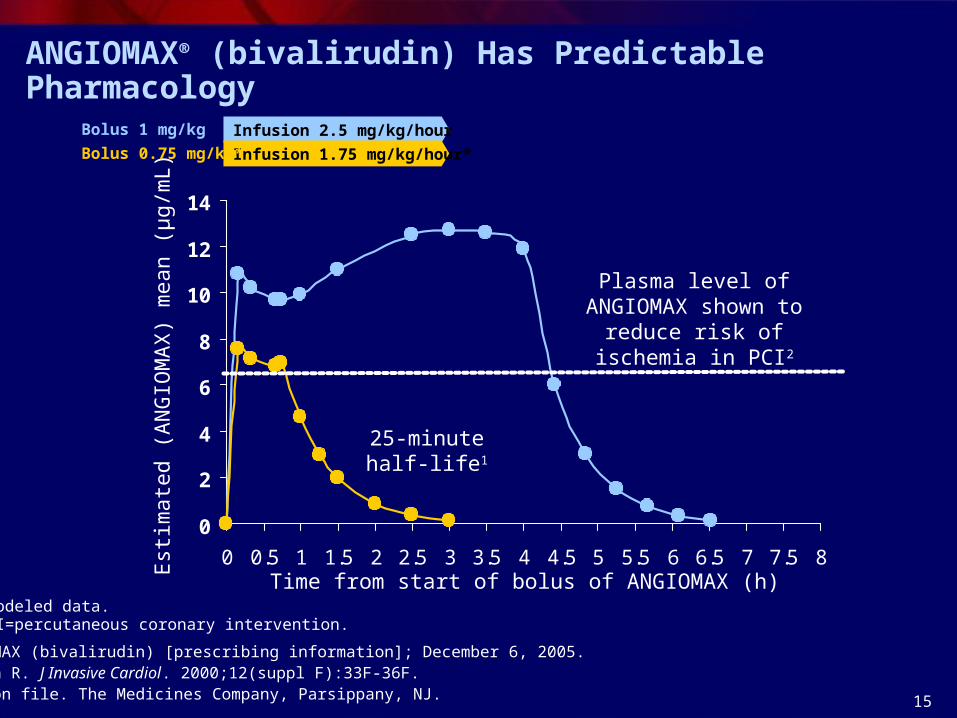
ANGIOMAX® (bivalirudin) Has Predictable Pharmacology
ANGIOMAX (bivalirudin) [prescribing information]; December 6, 2005.Robson R. J Invasive Cardiol. 2000;12(suppl F):33F-36F. Data on file. The Medicines Company, Parsippany, NJ.
*Modeled data. PCI=percutaneous coronary intervention.
0
2
4
6
8
10
12
14
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 5.5 6 6.5 7 7.5 8
Infusion 2.5 mg/kg/hour
Est
imat
ed (
AN
GIO
MA
X)
mea
n (μ
g/m
L)
Time from start of bolus of ANGIOMAX (h)
Infusion 1.75 mg/kg/hour*
Bolus 1 mg/kg
Bolus 0.75 mg/kg*
25-minutehalf-life1
Plasma level of ANGIOMAX shown to
reduce risk of ischemia in PCI2
16
ANGIOMAX® (bivalirudin)—Unique Mechanism of Action Overcomes the Limitations of Heparin
• Direct thrombin inhibitor that is reversible via thrombin yielding a 25-minute half-life– Heparin requires antithrombin to be able to deactivate thrombin
• Inhibits clot-bound and circulating thrombin– Heparin fails to effectively inhibit clot-bound thrombin
• Inhibits thrombin-mediated platelet aggregation and does not activate platelets– Heparin activates platelets
• Provides predictable pharmacology and linear pharmacokinetics– Heparin is unpredictable and has nonlinear pharmacokinetics

17
Switching to ANGIOMAX® (bivalirudin) for PCI Delivers Improved Outcomes
ANG-PSL-484-XXX
18
SYNERGY: Switching Between Heparins
• SYNERGY overall primary end point results– No difference in the composite of death/MI with enoxaparin
compared with UFH
– Significant increase in bleeding (TIMI major) with enoxaparin compared with UFH
• Patients who crossed over after randomization from UFH to enoxaparin or vice versa had– Increased rates of death/MI at 30 days compared with those who
did not cross over
– More bleeding complications (transfusions)
Ferguson JJ et al. JAMA. 2004;292:45-54.
MI=myocardial infarction; TIMI=Thrombosis in Myocardial Infarction.

19
SYNERGY: 30-Day Death/MI
• Patients who crossed over from UFH to enoxaparin or vice versa had increased rates of death/MI within 30 days compared with those on consistent therapy*
14.2 13.5
22.0
17.4
0
10
20
30
40
UFH Enoxaparin
Consistent Crossover
Dea
th/M
I a
t 30
day
s (%
)
n=677 n=45 n=593 n=103
*Postrandomization crossovers.
Ferguson JJ et al. JAMA. 2004;292:45-54.

20
SYNERGY: 30-Day Transfusions
• The rate of transfusion doubled in patients who crossed over from UFH to enoxaparin or vice versa within 30 days compared with those on consistent therapy*
15.1 15.3
35.1
30.2
0
10
20
30
40
UFH Enoxaparin
Consistent Crossover
Tra
nsf
usi
on
s at
30
day
s (%
)
n=724 n=72 n=671 n=179
*Postrandomization crossovers.
Ferguson JJ et al. JAMA. 2004;292:45-54.

21
SYNERGY: Switching Between Heparins
• The SYNERGY trial suggested that changing therapies between UFH and enoxaparin (or vice versa) resulted in an increased risk of bleeding
• Do these findings apply to ANGIOMAX® (bivalirudin)? Is it better to switch to ANGIOMAX or stay on consistent heparin therapy?

22
Evidence to Support Switching to ANGIOMAX® (bivalirudin)• BAT analysis (Bittl)
– Evaluate switching in era of conservative management
– Switching to ANGIOMAX improved ischemic and bleeding outcomes
– Improvements more profound in higher risk strata
• SWITCH study (Waksman)– Impact (safety) of switching, relative to last enoxaparin dose
– Switching outcomes consistent with other ANGIOMAX trials
• REPLACE-2 analysis (Gibson)– Data in patients undergoing PCI
– Switching to ANGIOMAX associated with improved bleeding outcomes
• ACUITY analysis (White)– Data in ACS patients undergoing PCI
– Switching to ANGIOMAX yielded improved bleeding outcomes
23
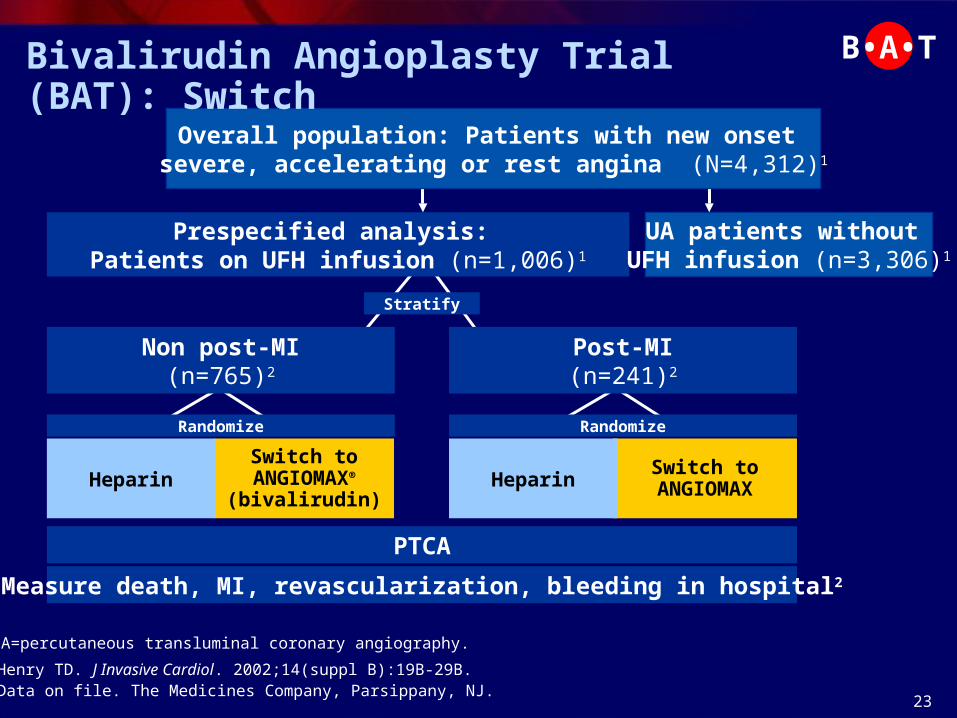
PTCA
Stratify
Randomize Randomize
Measure death, MI, revascularization, bleeding in hospital2
Prespecified analysis: Patients on UFH infusion (n=1,006)1
Non post-MI(n=765)2
Post-MI(n=241)2
Switch toANGIOMAX®
(bivalirudin)Heparin
Switch toANGIOMAXHeparin
UA patients without UFH infusion (n=3,306)1
1. Henry TD. J Invasive Cardiol. 2002;14(suppl B):19B-29B.2. Data on file. The Medicines Company, Parsippany, NJ.
Overall population: Patients with new onset severe, accelerating or rest angina (N=4,312)1
PTCA=percutaneous transluminal coronary angiography.
Bivalirudin Angioplasty Trial (BAT): Switch B•A•T

24
BAT: Switch Analysis
• Among 4,312 patients, there were1,2
– 1,006 patients who had a UFH infusion during the hour prior to randomization and were switched to ANGIOMAX® (bivalirudin) or continued on UFH
– 241 in the post-MI patient group (<2 weeks) who received UFH during the hour prior to randomization and were switched to ANGIOMAX or continued on UFH
• In patients receiving UFH prior to PTCA, infusion was discontinued at least 30 minutes prior to switching
1. Bittl J. Circulation. 2000;102(suppl 2):813. Abstract 3927.2. Henry TD. J Invasive Cardiol. 2002;14(suppl B):19B-29B.
B•A•T
25
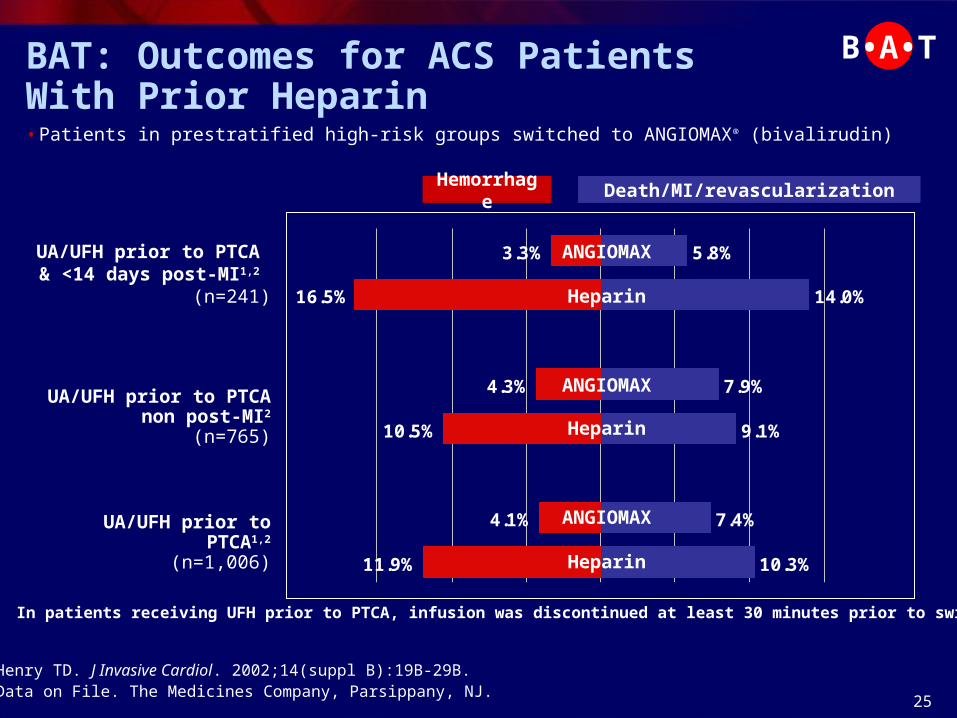
10.3%
7.4%
9.1%
7.9%
14.0%
5.8%3.3%
16.5%
4.3%
10.5%
4.1%
11.9%
Death/MI/revascularization
Heparin
ANGIOMAX
Heparin
Heparin
ANGIOMAX
ANGIOMAX
UA/UFH prior to PTCA & <14 days post-MI1,2
(n=241)
In patients receiving UFH prior to PTCA, infusion was discontinued at least 30 minutes prior to switching.
Hemorrhage
BAT: Outcomes for ACS Patients With Prior Heparin• Patients in prestratified high-risk groups switched to ANGIOMAX® (bivalirudin)
1. Henry TD. J Invasive Cardiol. 2002;14(suppl B):19B-29B.2. Data on File. The Medicines Company, Parsippany, NJ.
UA/UFH prior to PTCA1,2
(n=1,006)
UA/UFH prior to PTCA non post-MI2
(n=765)
B•A•T
26
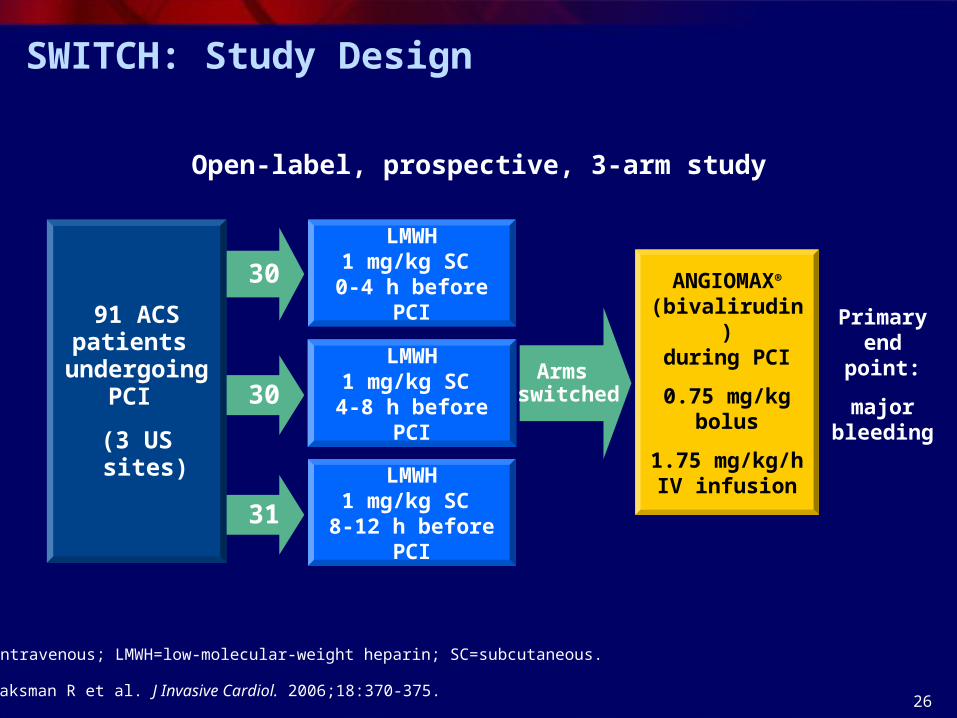
31
30
30
Primary end point:
major bleeding
91 ACSpatients
undergoing PCI
(3 US sites)
Open-label, prospective, 3-arm study
LMWH1 mg/kg SC
0-4 h before PCI
LMWH1 mg/kg SC
4-8 h before PCI
LMWH1 mg/kg SC
8-12 h before PCI
ANGIOMAX® (bivalirudin)during PCI
0.75 mg/kg bolus
1.75 mg/kg/h IV infusion
Arms switched
SWITCH: Study Design
Waksman R et al. J Invasive Cardiol. 2006;18:370-375.
IV=intravenous; LMWH=low-molecular-weight heparin; SC=subcutaneous.

27
EVENT All
(N=91)
SWITCH0-4 h
(n=30)
SWITCH4-8 h
(n=30)
SWITCH8-12 h(n=31)
P value
All major bleeding 8% (7) 13% (4)* 3% (1) 7% (2)* .39
Transfusion ≥2 units 4% (4) 3% (1) 3%(1) 7% (2) 1.00
Intracranial bleed 0 0 0 0 --
Retroperitoneal bleed 0 0 0 0 --
Drop in Hg >4 g/dL, no site 2% (2) 7% (2) 0 0 .21
All transfusions 4% (4) 7% (2) 0% (0) 7% (2) 1.00
Minor bleeding 4% (4) 7% (2) 7% (2) 0 (0) .39
*One patient received postprocedural enoxaparin and/or heparin.Hg=hemoglobin.
SWITCH: Bleeding Outcomes in Patients Switched to ANGIOMAX® (bivalirudin)
Reproduced with permission. Waksman R et al. J Invasive Cardiol. 2006;18:370-375. ©2006 The Journal of Invasive Cardiology.

28
SWITCH: Conclusions
• There were no significant differences in major bleeding between the various enoxaparin pretreatment groups when switched over to ANGIOMAX® (bivalirudin) for PCI
• For patients on LMWH, ANGIOMAX can be started 8 hours after the last LMWH dose
Waksman R et al. J Invasive Cardiol. 2006;18:370-375.
29
REPLACE-2: SWITCH Analysis
• The goal of this analysis was to evaluate whether a hazard existed when UFH or LMWH was administered prior to ANGIOMAX® (bivalirudin)
• This analysis compared bleeding among patients treated with or without UFH or LMWH in the 48 hours before study treatment
Gibson CM et al. Am J Cardiol. 2007;99:1687-1690.

30
Randomize
Protocol major/minor bleeding, TIMI bleeding, transfusion, mortality
ANGIOMAX® (bivalirudin)0.75 mg/kg bolus/1.75 mg/kg/h infusion with
“provisional” GP IIb/IIIa (n=2,994)1
Prior UFH (n=287)2
Naïve – no prior AT
(n=2,345)2
Overall population: Urgent or elective PCI patients (N=6,002)1
UFH 65 U/kg with planned GP IIb/IIIa
(n=3,008)1
Prior LMWH
(n=258)2
Naïve – no prior AT
(n=2,325)2
Prior UFH (n=349)2
Prior LMWH
(n=313)2
REPLACE-2: SWITCH Analysis
AT=antithrombin.1. Lincoff ML et al. JAMA. 2004;292:696-703.2. Gibson CM et al. Am J Cardiol. 2007;99:1687-1690.
31
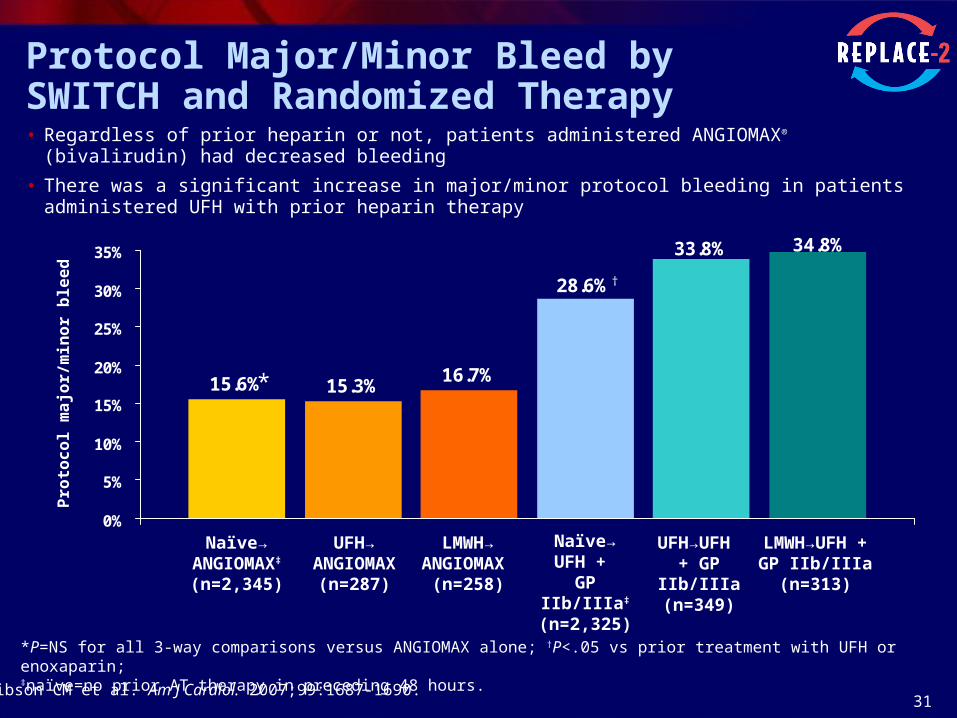
Protocol Major/Minor Bleed by SWITCH and Randomized Therapy• Regardless of prior heparin or not, patients administered ANGIOMAX® (bivalirudin) had decreased bleeding
• There was a significant increase in major/minor protocol bleeding in patients administered UFH with prior heparin therapy
*P=NS for all 3-way comparisons versus ANGIOMAX alone; †P<.05 vs prior treatment with UFH or enoxaparin; ‡naïve=no prior AT therapy in preceding 48 hours.
Pro
toc
ol
ma
jor/
min
or
ble
ed
15.6% 15.3%16.7%
28.6%
33.8% 34.8%
0%
5%
10%
15%
20%
25%
30%
35%
Naïve→ANGIOMAX‡
(n=2,345)
LMWH→ANGIOMAX
(n=258)
UFH→ANGIOMAX
(n=287)
LMWH→UFH + GP IIb/IIIa
(n=313)
Naïve→ UFH +
GP IIb/IIIa‡
(n=2,325)
UFH→UFH + GP IIb/IIIa
(n=349)
*
†
Gibson CM et al. Am J Cardiol. 2007;99:1687-1690.
32
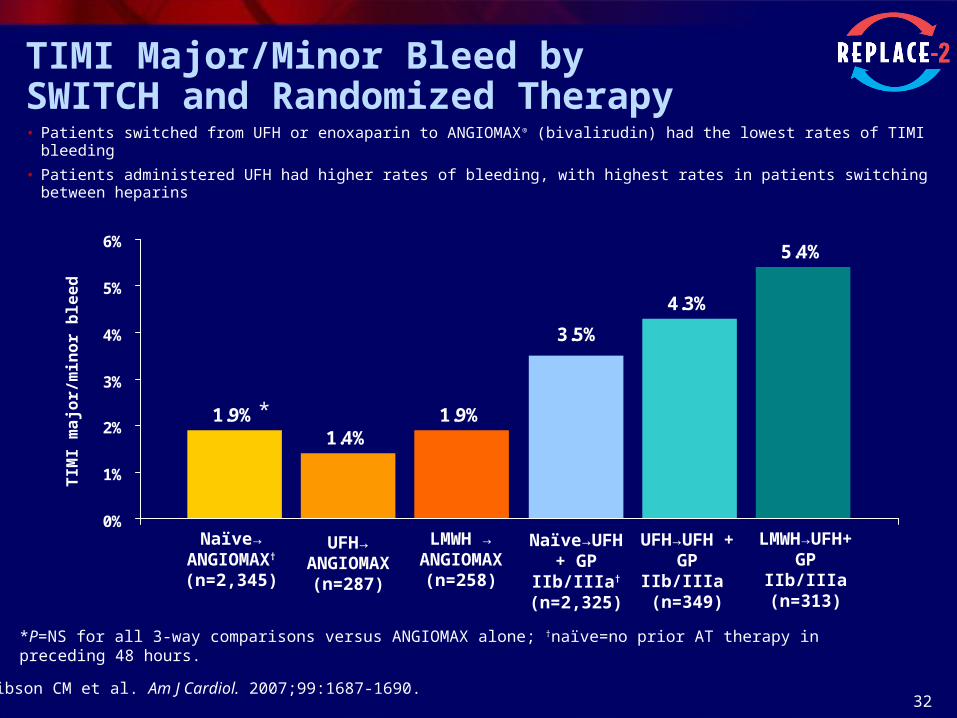
TIMI Major/Minor Bleed bySWITCH and Randomized Therapy• Patients switched from UFH or enoxaparin to ANGIOMAX® (bivalirudin) had the lowest rates of TIMI bleeding
• Patients administered UFH had higher rates of bleeding, with highest rates in patients switching between heparins
TIM
I m
ajo
r/m
ino
r b
lee
d
1.9%1.4%
4.3%
5.4%
1.9%
3.5%
0%
1%
2%
3%
4%
5%
6%
Naïve→ANGIOMAX†
(n=2,345)
LMWH → ANGIOMAX
(n=258)
UFH→ANGIOMAX
(n=287)
LMWH→UFH+ GP IIb/IIIa
(n=313)
Naïve→UFH + GP IIb/IIIa†
(n=2,325)
UFH→UFH + GP IIb/IIIa
(n=349)
*
*P=NS for all 3-way comparisons versus ANGIOMAX alone; †naïve=no prior AT therapy in preceding 48 hours.
Gibson CM et al. Am J Cardiol. 2007;99:1687-1690.
33
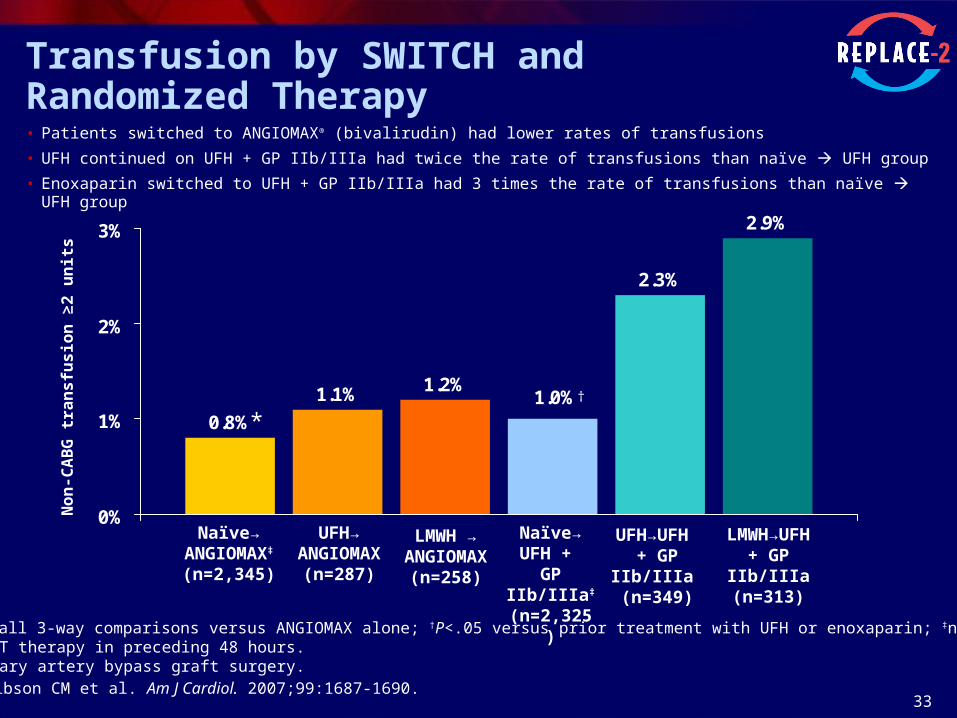
Transfusion by SWITCH and Randomized Therapy• Patients switched to ANGIOMAX® (bivalirudin) had lower rates of transfusions
• UFH continued on UFH + GP IIb/IIIa had twice the rate of transfusions than naïve UFH group
• Enoxaparin switched to UFH + GP IIb/IIIa had 3 times the rate of transfusions than naïve UFH group
0.8%
1.1%
2.3%
2.9%
1.2%1.0%
0%
1%
2%
3%
No
n-C
AB
G t
ran
sfu
sio
n ≥
2 u
nit
s
Naïve→ANGIOMAX‡
(n=2,345)
UFH→ ANGIOMAX
(n=287)
UFH→UFH + GP IIb/IIIa
(n=349)
LMWH→UFH+ GP IIb/IIIa
(n=313)
Naïve→ UFH +
GP IIb/IIIa‡
(n=2,325)
LMWH → ANGIOMAX
(n=258)
*†
*P=NS for all 3-way comparisons versus ANGIOMAX alone; †P<.05 versus prior treatment with UFH or enoxaparin; ‡naïve=no prior AT therapy in preceding 48 hours.CABG=coronary artery bypass graft surgery.Gibson CM et al. Am J Cardiol. 2007;99:1687-1690.

34
2.1%2.2% 2.1%
3.8%
4.9%
3.3%
0%
1%
2%
3%
4%
5%
UFH pretreatment*(n=685)
LMWH pretreatment*(n=591)
Any heparinpretreatment* (n=1,228)
ANGIOMAX with "provisional" GP IIb/IIIa Heparin + GP IIb/IIIa
1-Year Mortality: Prior UFH or LMWH
• Patients switched to ANGIOMAX® (bivalirudin) with “provisional” GP IIb/IIIa experienced a 33%-57% relative risk reduction in mortality at 1 year
Lincoff AM et al. JAMA 2004;292:696-703.Data on file. The Medicines Company, Parsippany, NJ.
Cu
mu
lati
ve d
eath
s at
12
mo
nth
s
*Pretreatment within prior 48 hours.
P=.38 P=.07 P=.07
33% 57% 45%

35
• Moderate- and high-risk UA or NSTEMI patients undergoing an earlyinvasive strategy
• Prospective, randomized, active-controlled trial
ACUITY Study Design
*Stratified by preangiography thienopyridine use or administration. †UFH or enoxaparin. ‡ ANGIOMAX alone = ANGIOMAX monotherapy with GP IIb/IIIa reserved for severe breakthrough ischemia and procedural complications during PCI. NSTEMI=non-ST–segment elevation myocardial infarction; R=randomized.The safety and effectiveness of ANGIOMAX have not been established in patients with ACS who are not undergoing PCI.
CABG
Moderate-and high-risk ACS
(N=13,819)
An
gio
gra
ph
y w
ith
in 7
2 h
Aspirin in all;clopidogrel
dosing and timingper local practice
Heparin(s)† + GP IIb/IIIa(n=4,603)
ANGIOMAX®
(bivalirudin)+ GP IIb/IIIa(n=4,604)
ANGIOMAXalone‡
(n=4,612)
R*
Medicalmanagement
PCI
Stone GW et al. N Engl J Med. 2006;355:2203-2216.

36
*ANGIOMAX monotherapy with GP IIb/IIIa reserved for severe breakthrough ischemia and procedural complications during PCI.
P=.47 P<.001
48%
Adv
erse
eve
nts
(%)
30-day
9.0%
3.5%
8.2%
6.7%
0
5
10
15
Composite ischemia Non-CABG major bleeding
P=.75
Adv
erse
eve
nts
(%)
1-year
2.7%2.9%
0
1
2
3
4
5
Mortality
Data on file. The Medicines Company, Parsippany, NJ.
Switch to ANGIOMAX* vs consistent heparin + GP IIb/IIIa outcomes
Switching to ANGIOMAX® (bivalirudin) Improves Bleeding Outcomes
• Ischemic suppression was maintained and bleeding significantly reduced at 30 days
• Long-term efficacy in both groups was consistent at 1 year
ANGIOMAX* (n=1,292)switch arm
UFH/enoxaparin + GP IIb/IIIa (n=1,236)consistent arm
PCI Subgroup
37
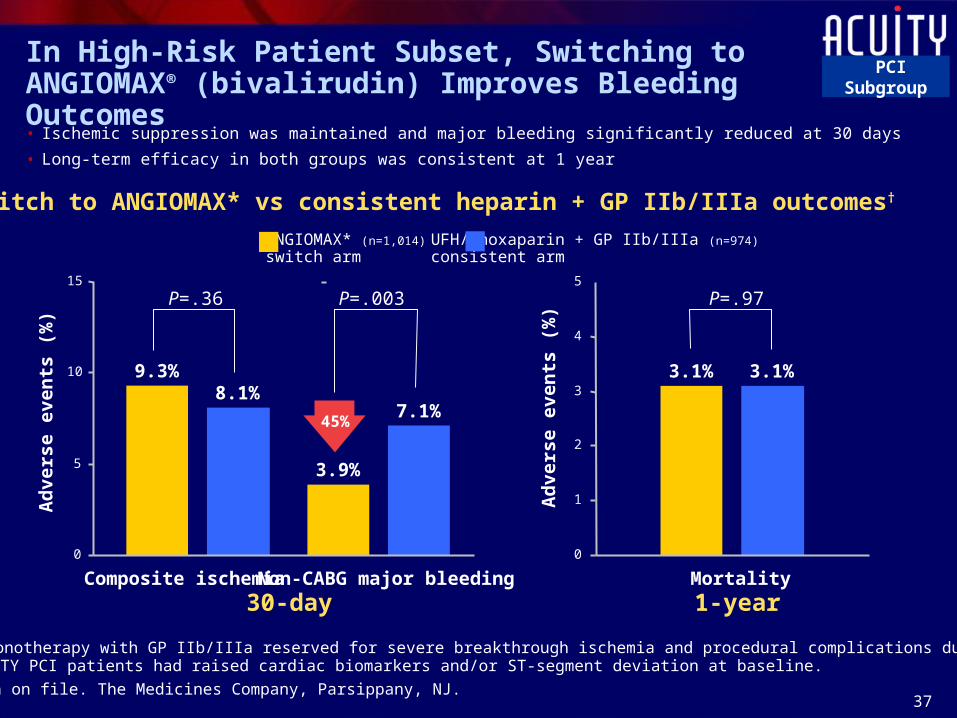
ANGIOMAX* (n=1,014)switch arm
P=.36 P=.003
45%
*ANGIOMAX monotherapy with GP IIb/IIIa reserved for severe breakthrough ischemia and procedural complications during PCI. †76% of ACUITY PCI patients had raised cardiac biomarkers and/or ST-segment deviation at baseline.
9.3%
3.9%
8.1%7.1%
UFH/enoxaparin + GP IIb/IIIa (n=974)consistent arm
0
5
10
15P=.97
3.1% 3.1%
0
1
2
3
4
5
30-dayComposite ischemia Non-CABG major bleeding
1-yearMortality
Adv
erse
eve
nts
(%)
Adv
erse
eve
nts
(%)
Data on file. The Medicines Company, Parsippany, NJ.
In High-Risk Patient Subset, Switching to ANGIOMAX® (bivalirudin) Improves Bleeding Outcomes
• Ischemic suppression was maintained and major bleeding significantly reduced at 30 days
• Long-term efficacy in both groups was consistent at 1 year
Switch to ANGIOMAX* vs consistent heparin + GP IIb/IIIa outcomes†
PCI Subgroup

38
How to Switch from Heparin(s) to ANGIOMAX® (bivalirudin) for PCI
Reed MD et al. Pharmacotherapy. 2002;22(6 pt 2):105S-111S.
UFH
LMWH
From UFH to ANGIOMAX, discontinue UFH for
30 minutes before starting ANGIOMAX for PCI
From LMWH to ANGIOMAX, discontinue LMWH for
8 hours before starting ANGIOMAX for PCI
39
ACUITY PCI Subgroup Analysis: 1-Year Mortality Results
PCI Subgroup

40
56% of Patients in ACUITY Underwent PCI
56.4%
11.1%32.5%CABG (n=1,539) Medical management
(n=4,491)
Heparin(s) + GP IIb/IIIa(n=2,561)
Heparin(s) + GP IIb/IIIa(n=2,561)
ANGIOMAX® (bivalirudin) +
GP IIb/IIIa(n=2,609)
ANGIOMAX® (bivalirudin) +
GP IIb/IIIa(n=2,609)
ANGIOMAX alone(n=2,619)
ANGIOMAX alone(n=2,619)
Stone GW et al. N Engl J Med. 2006;355:2203-2216.
PCI (n=7,789)
41
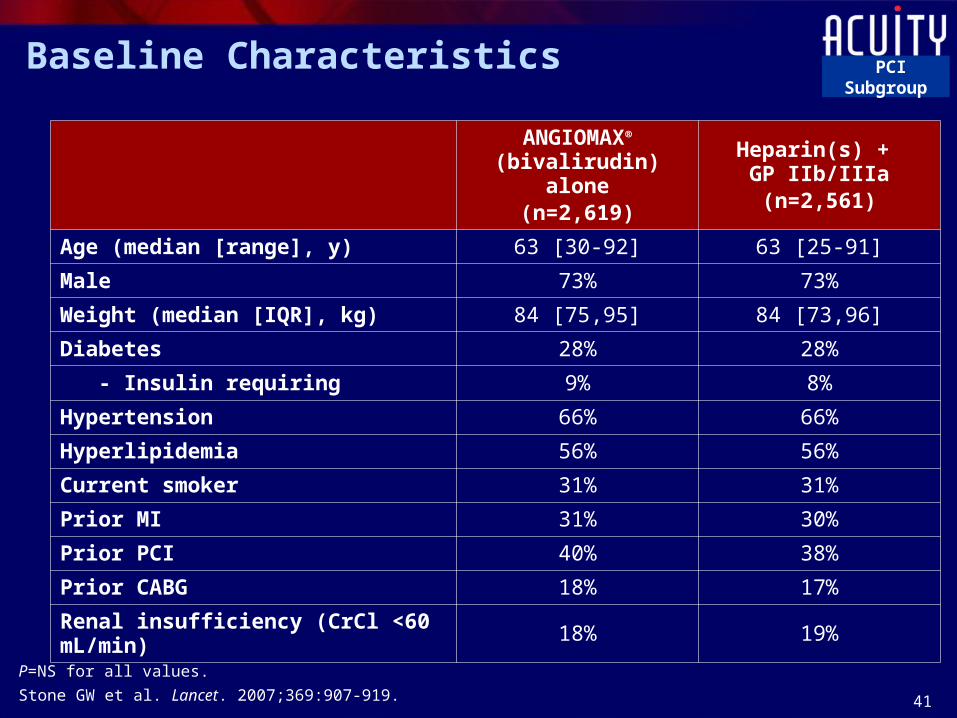
Baseline Characteristics
ANGIOMAX® (bivalirudin) alone
(n=2,619)
Heparin(s) + GP IIb/IIIa(n=2,561)
Age (median [range], y) 63 [30-92] 63 [25-91]
Male 73% 73%
Weight (median [IQR], kg) 84 [75,95] 84 [73,96]
Diabetes 28% 28%
- Insulin requiring 9% 8%
Hypertension 66% 66%
Hyperlipidemia 56% 56%
Current smoker 31% 31%
Prior MI 31% 30%
Prior PCI 40% 38%
Prior CABG 18% 17%
Renal insufficiency (CrCl <60 mL/min) 18% 19%
P=NS for all values.
Stone GW et al. Lancet. 2007;369:907-919.
PCI Subgroup

42
Baseline High-Risk Features
• 77% of the PCI patients had elevated cardiac biomarkers or ST-segment changes
ANGIOMAX® (bivalirudin) alone
(n=2,619)
Heparin(s) + GP IIb/IIIa(n=2,561)
Cardiac biomarker (MB or troponin) 66% 65%
- Troponin 66% 65%
ST-segment ≥1 mm 35% 35%
Cardiac biomarker or ST-segment 77% 77%
Stone GW et al. Lancet. 2007;369:907-919.
PCI Subgroup
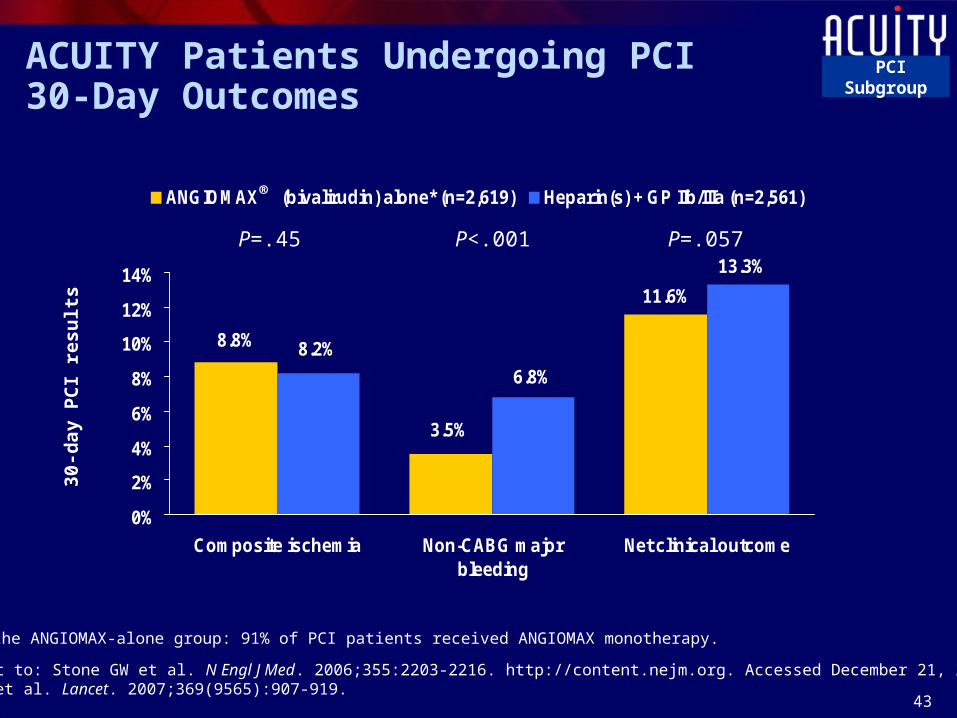
43
ACUITY Patients Undergoing PCI30-Day Outcomes
Supplement to: Stone GW et al. N Engl J Med. 2006;355:2203-2216. http://content.nejm.org. Accessed December 21, 2006.Stone GW et al. Lancet. 2007;369(9565):907-919.
8.8%
3.5%
11.6%
13.3%
6.8%
8.2%
0%
2%
4%
6%
8%
10%
12%
14%
Composite ischemia Non-CABG majorbleeding
Net clinical outcome
ANGIOMAX (bivalirudin) alone* (n=2,619) Heparin(s) + GP IIb/IIIa (n=2,561)
P=.45 P<.001 P=.057
30-d
ay P
CI
resu
lts
*In the ANGIOMAX-alone group: 91% of PCI patients received ANGIOMAX monotherapy.
®
PCI Subgroup
44
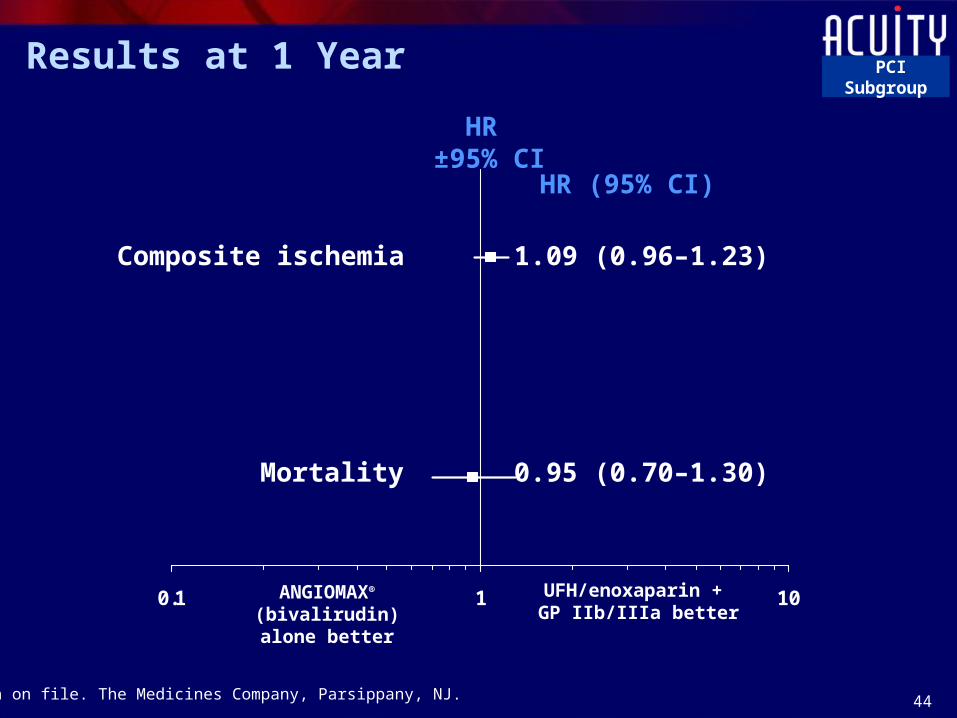
0.1 1 10
Results at 1 Year
HR ±95% CI
HR (95% CI)
ANGIOMAX® (bivalirudin) alone
better
UFH/enoxaparin + GP IIb/IIIa better
Composite ischemia 1.09 (0.96–1.23)
Mortality 0.95 (0.70–1.30)
Data on file. The Medicines Company, Parsippany, NJ.
PCI Subgroup
45
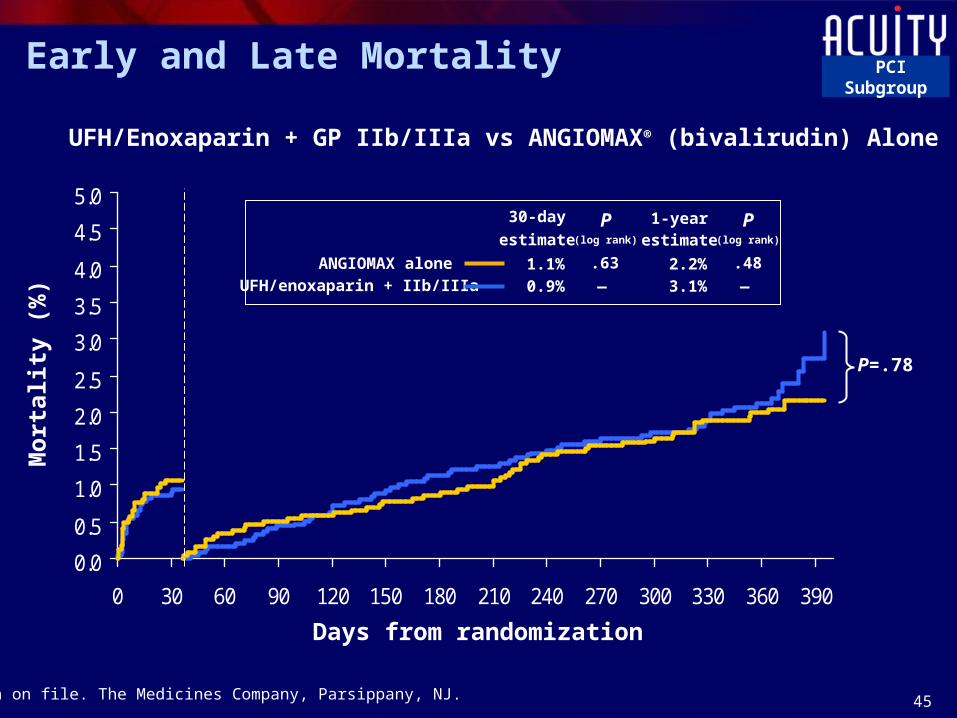
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
0 30 60 90 120 150 180 210 240 270 300 330 360 390
Mo
rtal
ity
(%)
Days from randomization
Early and Late Mortality
UFH/Enoxaparin + GP IIb/IIIa vs ANGIOMAX® (bivalirudin) Alone
30-day
estimateP
(log rank) estimateP
(log rank)
ANGIOMAX alone .631.1% .482.2%
1-year
UFH/enoxaparin + IIb/IIIa 0.9% — 3.1% —
P=.78
Data on file. The Medicines Company, Parsippany, NJ.
PCI Subgroup
46
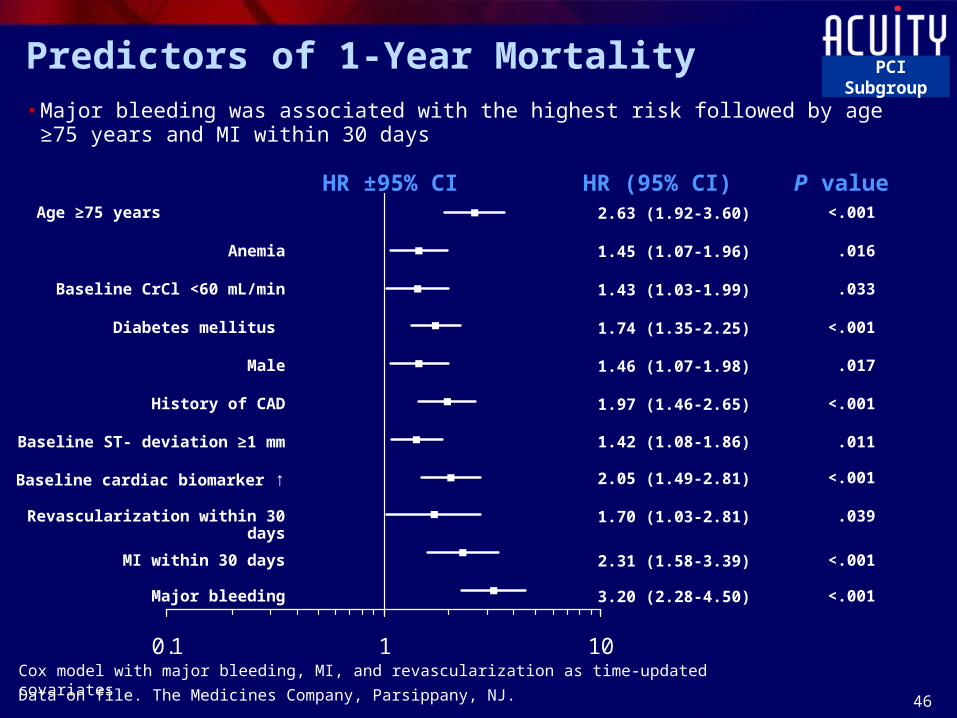
0.1 1 10
Age ≥75 years 2.63 (1.92-3.60) <.001
Anemia 1.45 (1.07-1.96) .016
Baseline CrCl <60 mL/min 1.43 (1.03-1.99) .033
Diabetes mellitus 1.74 (1.35-2.25) <.001
Male 1.46 (1.07-1.98) .017
History of CAD 1.97 (1.46-2.65) <.001
Baseline ST- deviation ≥1 mm 1.42 (1.08-1.86) .011
Baseline cardiac biomarker ↑ 2.05 (1.49-2.81) <.001
Revascularization within 30 days 1.70 (1.03-2.81) .039
MI within 30 days 2.31 (1.58-3.39) <.001
Major bleeding 3.20 (2.28-4.50) <.001
HR ±95% CI P valueHR (95% CI)
Predictors of 1-Year Mortality
• Major bleeding was associated with the highest risk followed by age ≥75 years and MI within 30 days
Cox model with major bleeding, MI, and revascularization as time-updated covariates
Data on file. The Medicines Company, Parsippany, NJ.
PCI Subgroup
47
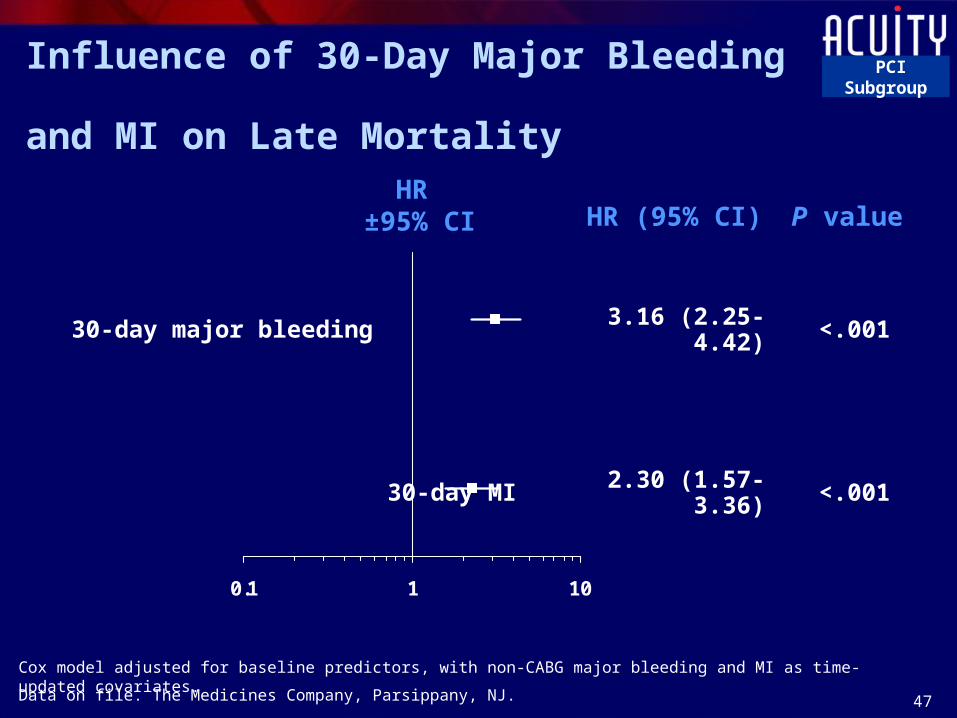
Influence of 30-Day Major Bleeding and MI on Late Mortality
0.1 1 10
HR ±95% CI
30-day major bleeding 3.16 (2.25-4.42) <.001
HR (95% CI)
Cox model adjusted for baseline predictors, with non-CABG major bleeding and MI as time-updated covariates.
30-day MI 2.30 (1.57-3.36) <.001
P value
Data on file. The Medicines Company, Parsippany, NJ.
PCI Subgroup

48
Impact of Bleeding on Length of Stay
• Patients with a bleeding event had a significant increase of 2 days in their length of stay
Patients with bleeding event
(n=459)
Patients without bleeding event
(n=7,318)
Pvalue
Hospital length of stay, median days
5.0 3.0 <.001
Data on file. The Medicines Company, Parsippany, NJ.
PCI Subgroup

49
In High-risk Patients With Elevated Troponin Levels and/or ST-segment Changes
Risk Ratio±95% CI RR (95% CI)
HR±95% CI HR (95% CI)
UFH/enoxaparin + GP IIb/IIIa
better
0.1 1 10ANGIOMAX® (bivalirudin) alone
better
ANGIOMAX alone better
30-Day Results 1-Year Results
Composite ischemia 1.08 (0.88-1.32)
Major bleeding 0.55 (0.42-0.72)
Mortality 0.94 (0.67-1.31)
UFH/enoxaparin + GP IIb/IIIa
better
Data on file. The Medicines Company, Parsippany, NJ.
PCI Subgroup
50
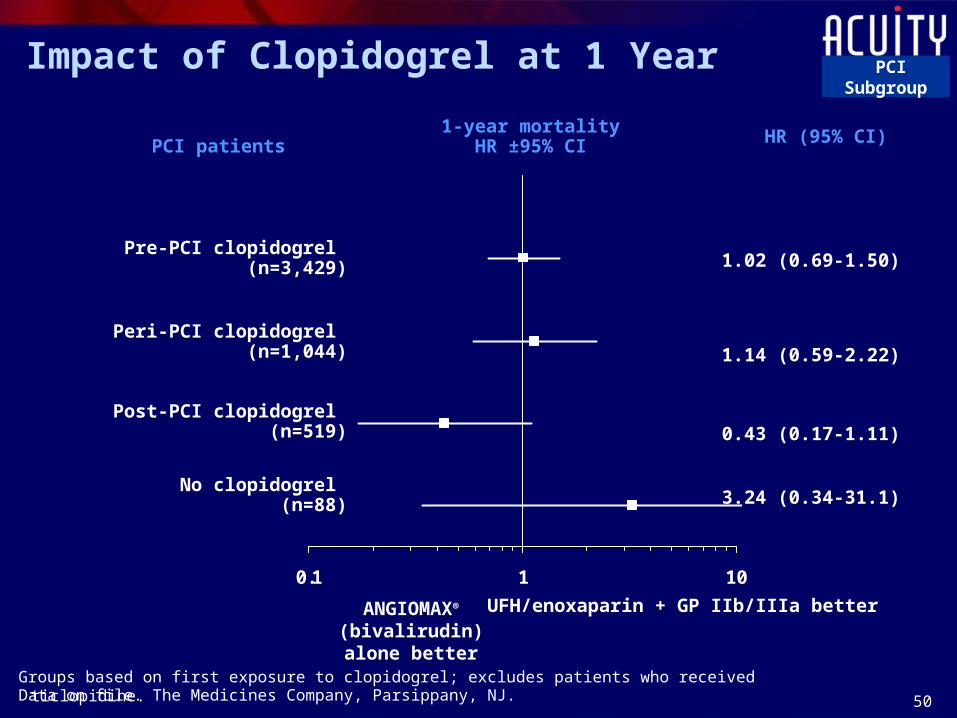
Impact of Clopidogrel at 1 Year
0.1 1 10
PCI patients
1-year mortalityHR ±95% CI HR (95% CI)
ANGIOMAX®
(bivalirudin) alone better
UFH/enoxaparin + GP IIb/IIIa better
Groups based on first exposure to clopidogrel; excludes patients who received ticlopidine.
Pre-PCI clopidogrel (n=3,429) 1.02 (0.69-1.50)
Peri-PCI clopidogrel (n=1,044) 1.14 (0.59-2.22)
Post-PCI clopidogrel (n=519) 0.43 (0.17-1.11)
No clopidogrel (n=88) 3.24 (0.34-31.1)
Data on file. The Medicines Company, Parsippany, NJ.
PCI Subgroup
51
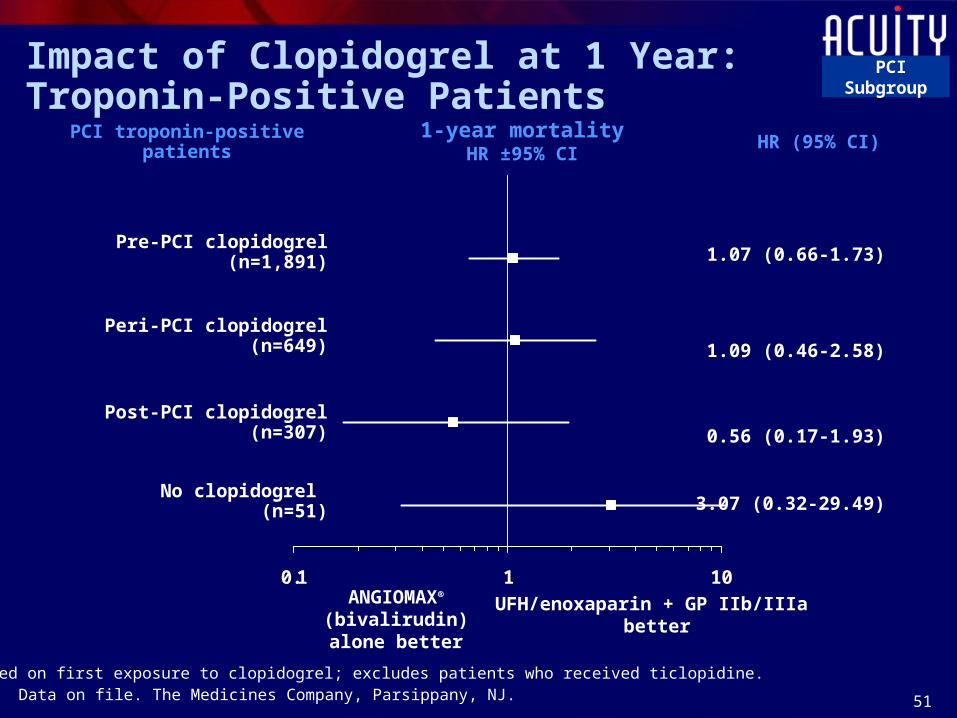
Impact of Clopidogrel at 1 Year:Troponin-Positive Patients
0.1 1 10
PCI troponin-positive patients1-year mortality
HR ±95% CIHR (95% CI)
ANGIOMAX®
(bivalirudin) alone better
UFH/enoxaparin + GP IIb/IIIa better
Groups based on first exposure to clopidogrel; excludes patients who received ticlopidine.
Pre-PCI clopidogrel (n=1,891) 1.07 (0.66-1.73)
Peri-PCI clopidogrel (n=649) 1.09 (0.46-2.58)
Post-PCI clopidogrel (n=307) 0.56 (0.17-1.93)
No clopidogrel (n=51) 3.07 (0.32-29.49)
Data on file. The Medicines Company, Parsippany, NJ.
PCI Subgroup

52
Additional ConsiderationsANGIOMAX® (bivalirudin) Important Safety Information, Dosing and Administration

53
Important Safety Information
• ANGIOMAX® (bivalirudin) with provisional use of GP IIb/IIIa inhibitor is indicated for use as an anticoagulant in patients undergoing percutaneous coronary intervention (PCI), and in patients with or at risk for heparin-induced thrombocytopenia and thrombosis syndrome (HIT/HITTS) undergoing PCI
• ANGIOMAX is intended for use with aspirin and has been studied only in patients receiving concomitant aspirin
• ANGIOMAX is contraindicated in patients with active major bleeding or hypersensitivity to ANGIOMAX or its components
• The most common (≥10%) adverse events for ANGIOMAX were back pain, pain, nausea, headache, and hypotension
• An unexplained fall in blood pressure or hematocrit, or any unexplained symptom, should lead to serious consideration of a hemorrhagic event and cessation of ANGIOMAX administration
ANGIOMAX (bivalirudin) [prescribing information]; December 6, 2005.
54
Dosing and Administration
• The recommended dose for ANGIOMAX® (bivalirudin) is an intravenous (IV) bolus of 0.75 mg/kg
• This should be followed by an infusion of 1.75 mg/kg/hour for the duration of the PCI procedure or up to 4 hours per physician discretion
• After the 4 hours of the initial infusion, an additional infusion may be initiated at a rate of 0.2 mg/kg/hour for up to 20 hours, if needed
• If the low-rate infusion is used after the initial infusion, a lower concentration bag of 0.5 mg/mL should be prepared. See Prescribing information for diluting instructions
• Special precaution: It is important to note that the pre-PCI ANGIOMAX dose for patients with acute coronary syndromes in the ACUITY trial is not an approved dose and is much lower than the approved PCI dose discussed in these instructions
ANGIOMAX (bivalirudin) [prescribing information]; December 6, 2005.
55
Special Population: Patients With Renal Impairment• No reduction in the bolus dose of ANGIOMAX® (bivalirudin) is needed
• The infusion dose may need to be reduced– Severe renal impairment (CrCl <30 mL/minute): reduction in the infusion rate
to 1.0 mg/kg/hour should be considered
– On hemodialysis: infusion should be reduced to 0.25 mg/kg/hour
• Standard infusion dose for patients with normal to moderate renal impairment (CrCl ≥30 mL/minute)
• Anticoagulation status should be monitored in patients with renal impairment
ANGIOMAX (bivalirudin) [prescribing information]; December 6, 2005.
56
ANGIOMAX® (bivalirudin) in PCI
• ANGIOMAX improves bleeding outcomes while preserving ischemic suppression for UA/NSTEMI patients undergoing PCI even if the patients are switched from UFH or enoxaparin to ANGIOMAX
• Consistent results in low-, moderate-, and high-risk patients
For more information about ANGIOMAX, please see the representative for full ANGIOMAX Prescribing Information.

















