44
1 Roadmap for Management of Patients with Chronic Hepatitis B (CHB) Prof. Xinxin Zhang Rui Jin Hospital Jiao Tong University
| Date post: | 27-Dec-2015 |
| Category: |
Documents |
| Upload: | elaine-sanders |
| View: | 216 times |
| Download: | 0 times |

1
Roadmap for Management of Patients with
Chronic Hepatitis B (CHB)
Prof. Xinxin ZhangRui Jin Hospital
Jiao Tong University
2
Introduction
Presentation Objectives
Data Review: Associations of HBV DNA with Outcomesi. Natural history studiesii. Impact of treatment
Key role of HBV DNA in On-Treatment Managementi. Timing and magnitude of HBV DNA suppression
On-Treatment Roadmap Concept
Summary and Conclusions
Contents
3
IntroductionTreatment challenges highlight need for new management approach
Treating hepatitis B virus (HBV) infection continues to be a challenge for physicians due to
– Complications arising from chronic HBV (CHB)– The increasing number of available therapeutic options
Treatment guidelines recognize the importance of monitoring and evaluation of treatment response; however, a standard on-treatment management approach does not exist
To establish a new treatment paradigm, we should ask– Does long-term suppression of HBV replication achieve the goals of
treatment in CHB?– Can the degree of on-treatment viral suppression predict outcomes?– Does profound, early viral suppression at week 24 predict clinical
outcomes?– Can a Roadmap concept help achieve the goals of treatment in CHB?

4
Presentation Objectives
To explore the association between persistent viraemia and hepatitis disease progression
To assess the relationship between the degree of viral suppression and clinical outcome
To assess the role of early and effective viral load reduction and the association with clinical outcomes*
To review an on-treatment management strategy – the roadmap concept – that may offer a valuable opportunity for enhanced treatment response
* For safety information on the products referred to, please refer to the Product Information.
5
Data Review: Associations of HBV DNA with Outcomes
i. Natural history studies
6
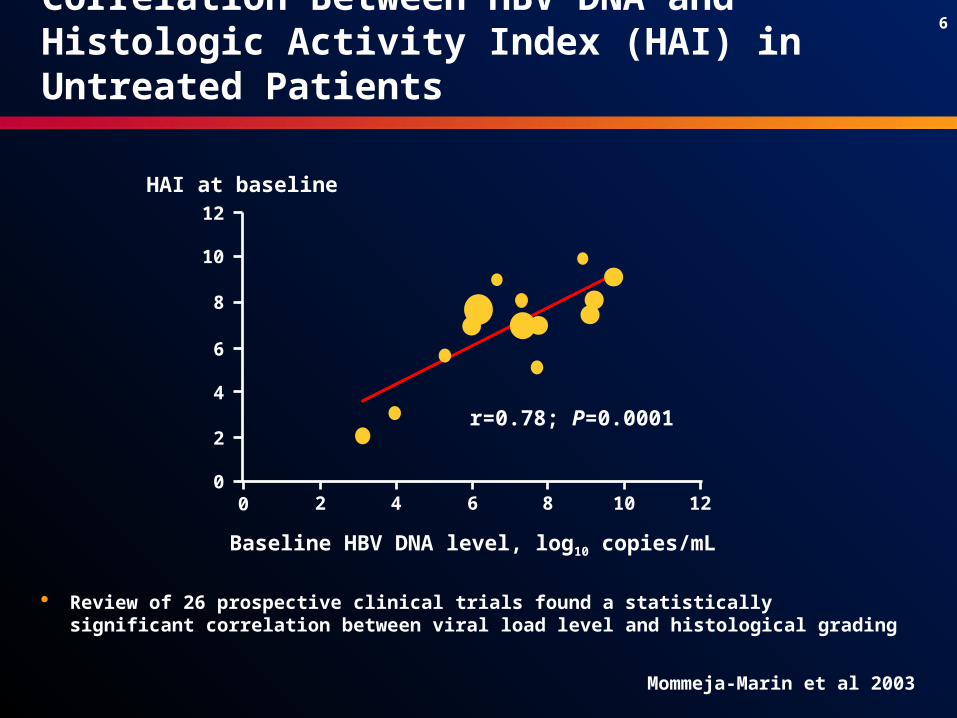
Correlation Between HBV DNA and Histologic Activity Index (HAI) in Untreated Patients
Review of 26 prospective clinical trials found a statistically significant correlation between viral load level and histological grading
2 4 6 8 10 1200
2
4
6
8
10
12
Baseline HBV DNA level, log10 copies/mL
r=0.78; P=0.0001
HAI at baseline
Mommeja-Marin et al 2003
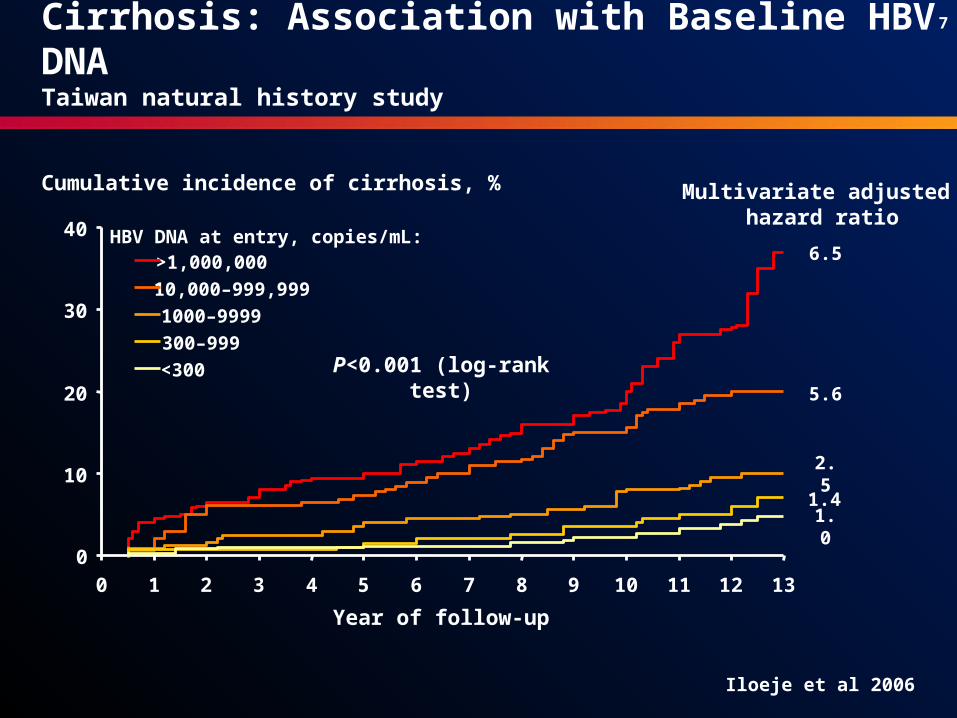
7
2.51.4
1.0
5.6
6.5
P<0.001 (log-rank test)
Multivariate adjusted hazard ratio
0
10
20
30
40
0 1 2 3 4 5 6 7 8 9 10 11 12 13
Year of follow-up
Cumulative incidence of cirrhosis, %
>1,000,000
10,000–999,999
1000–9999
300–999
<300
HBV DNA at entry, copies/mL:
Cirrhosis: Association with Baseline HBV DNA Taiwan natural history study
Iloeje et al 2006
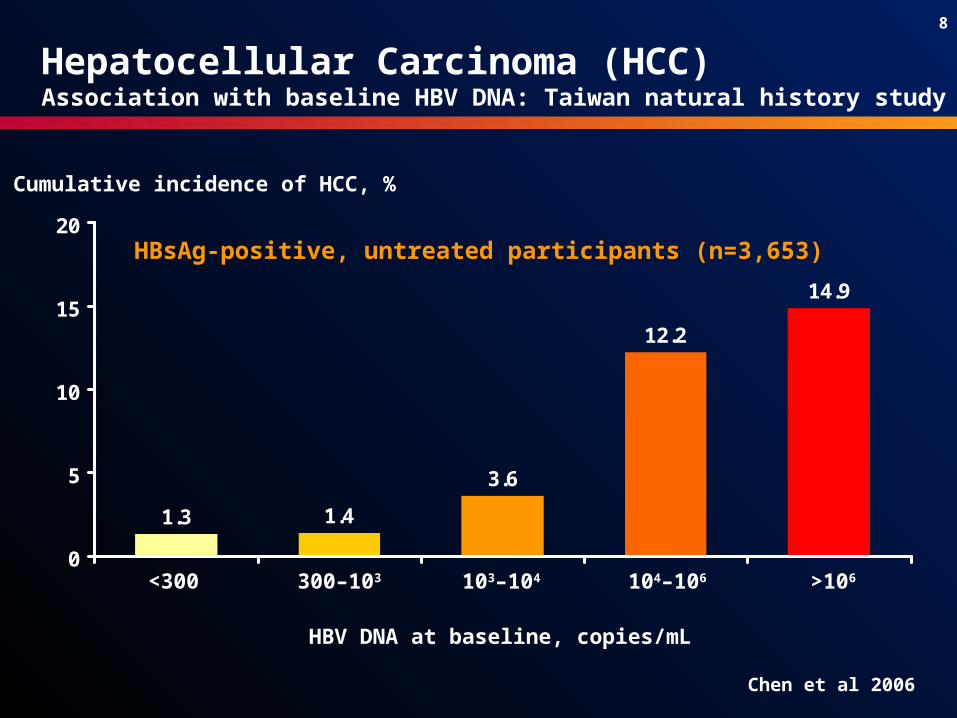
8
1.3 1.4
3.6
12.2
14.9
0
5
10
15
20
Hepatocellular Carcinoma (HCC)Association with baseline HBV DNA: Taiwan natural history study
Cumulative incidence of HCC, %
HBV DNA at baseline, copies/mL
HBsAg-positive, untreated participants (n=3,653)
Chen et al 2006
<300 300–103 103–104 104–106 >106
9
Evidence for Association Between HBV DNA and Clinical Outcomes
Natural history studies demonstrate– Lower HBV DNA levels are associated with better underlying
histology
– High HBV DNA may be an independent predictor for cirrhosis and HCC
– Sustained suppression of HBV may reduce long-term risk of cirrhosis and HCC
Hypothesis needs to be proven prospectively
10
Data Review: Associations of HBV DNA with Outcomes
ii. Impact of treatment
11
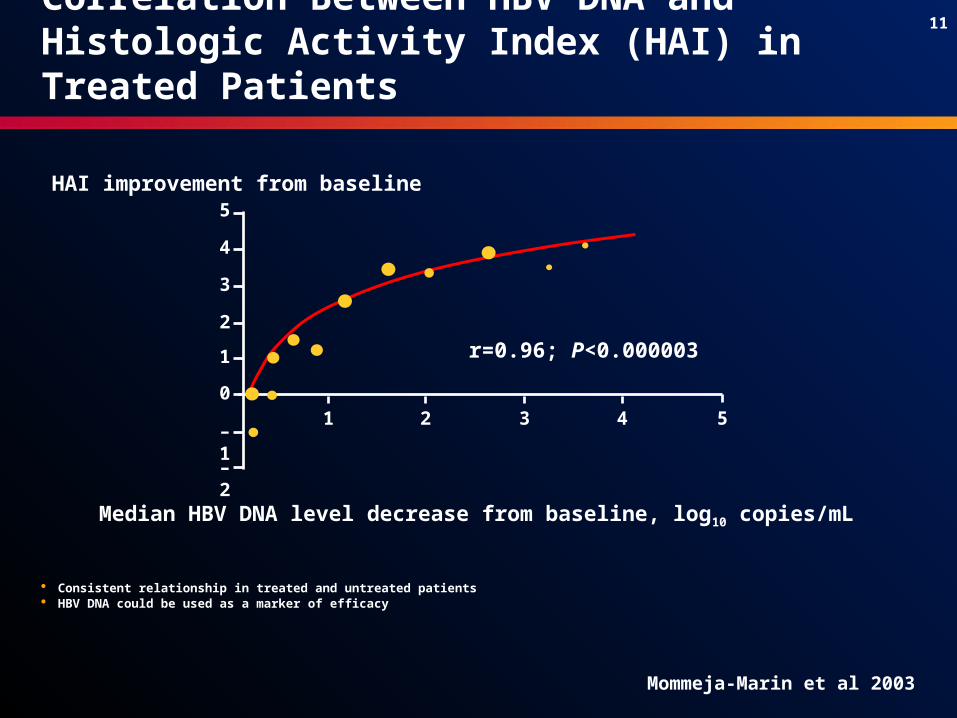
Consistent relationship in treated and untreated patients HBV DNA could be used as a marker of efficacy
Median HBV DNA level decrease from baseline, log10 copies/mL
HAI improvement from baseline
r=0.96; P<0.000003
1 2 3 4 5
–2
–1
0
1
2
3
4
5
Mommeja-Marin et al 2003
Correlation Between HBV DNA and Histologic Activity Index (HAI) in Treated Patients
12
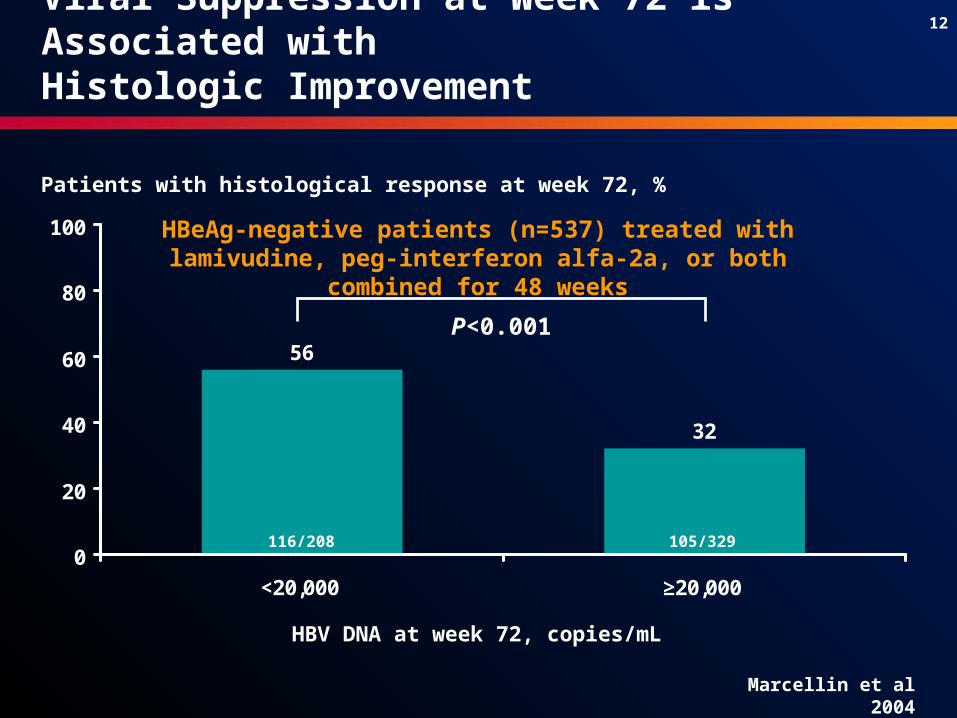
56
32
0
20
40
60
80
100
<20,000 ≥20,000
P<0.001
HBV DNA at week 72, copies/mL
HBeAg-negative patients (n=537) treated with lamivudine, peg-interferon alfa-2a, or both combined for 48 weeks
Patients with histological response at week 72, %
Marcellin et al 2004
Viral Suppression at Week 72 is Associated with Histologic Improvement
105/329116/208

13
Months
0
5
10
15
20
25
0 6 12 18 24 30 36
13%
21%
5%
Liaw 2005
Patients with disease progression, %
Viral Suppression Significantly Impacts Disease Progression
Lamivudine – Wild typeLamivudine – YMDDmPlacebo
HBeAg-positive patients (n=651) treated with lamivudine or placebo
14
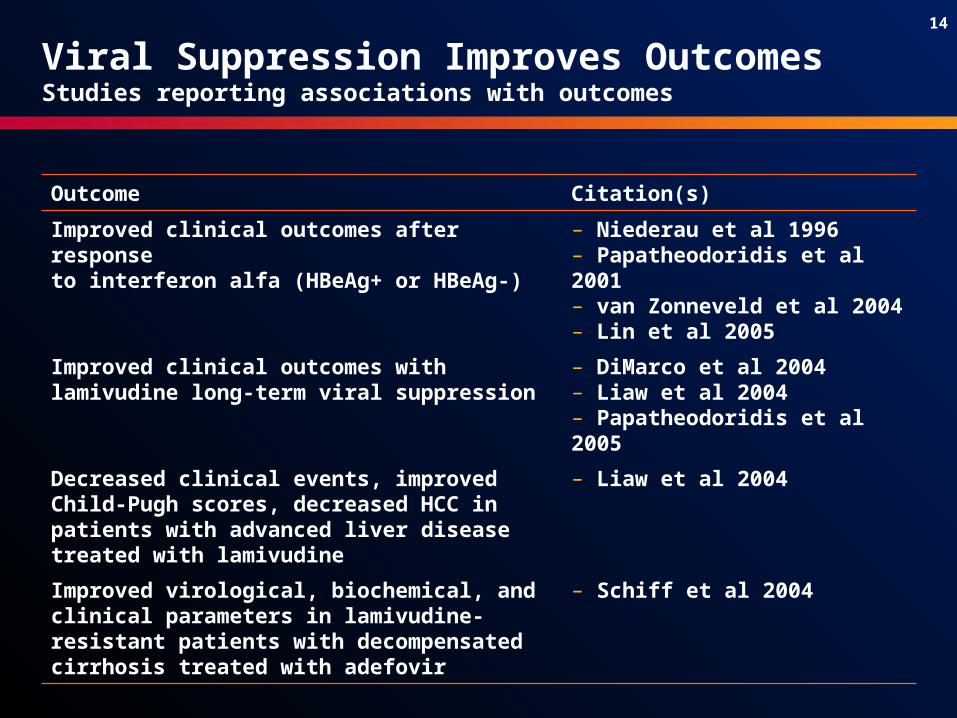
Viral Suppression Improves Outcomes Studies reporting associations with outcomes
Outcome Citation(s)
Improved clinical outcomes after response to interferon alfa (HBeAg+ or HBeAg-)
– Niederau et al 1996– Papatheodoridis et al 2001– van Zonneveld et al 2004– Lin et al 2005
Improved clinical outcomes with lamivudine long-term viral suppression
– DiMarco et al 2004– Liaw et al 2004 – Papatheodoridis et al 2005
Decreased clinical events, improved Child-Pugh scores, decreased HCC in patients with advanced liver disease treated with lamivudine
– Liaw et al 2004
Improved virological, biochemical, and clinical parameters in lamivudine-resistant patients with decompensated cirrhosis treated with adefovir
– Schiff et al 2004
15
Key Role of HBV DNA in On-Treatment Management
i. Timing and magnitude of HBV DNA suppression
16
Rapid and Profound HBV Suppression: a Critical Goal of Therapy
Outcomes
Primary goal of treatment
Delay in progression to cirrhosis and HCC
Improved survival Reduced resistance Increased seroconversion Improved liver histology Normalised alanine
aminotransferase (ALT) levels
Sustained suppression of HBV replication to the lowest possible level
Fontana 2003; Gauthier et al 1999; Keeffe et al 2006; Liaw et al 2004; Liaw et al 2005; Mommeja-Marin et al 2003; Niederau et al 1996; Yuen et al
2001
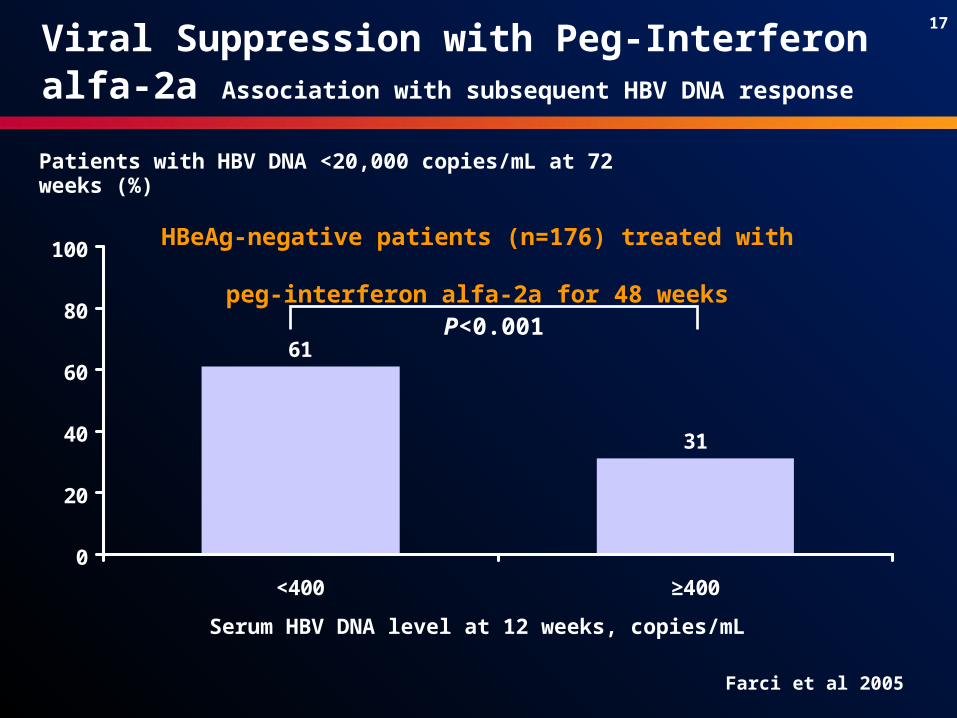
17
Patients with HBV DNA <20,000 copies/mL at 72 weeks (%)
31
61
0
20
40
60
80
100
<400 ≥400
Serum HBV DNA level at 12 weeks, copies/mL
HBeAg-negative patients (n=176) treated with peg-interferon alfa-2a for 48 weeks
P<0.001
Farci et al 2005
Viral Suppression with Peg-Interferon alfa-2a Association with subsequent HBV DNA response
18
73
60
28
7
82
61
40
20
0
20
40
60
80
100
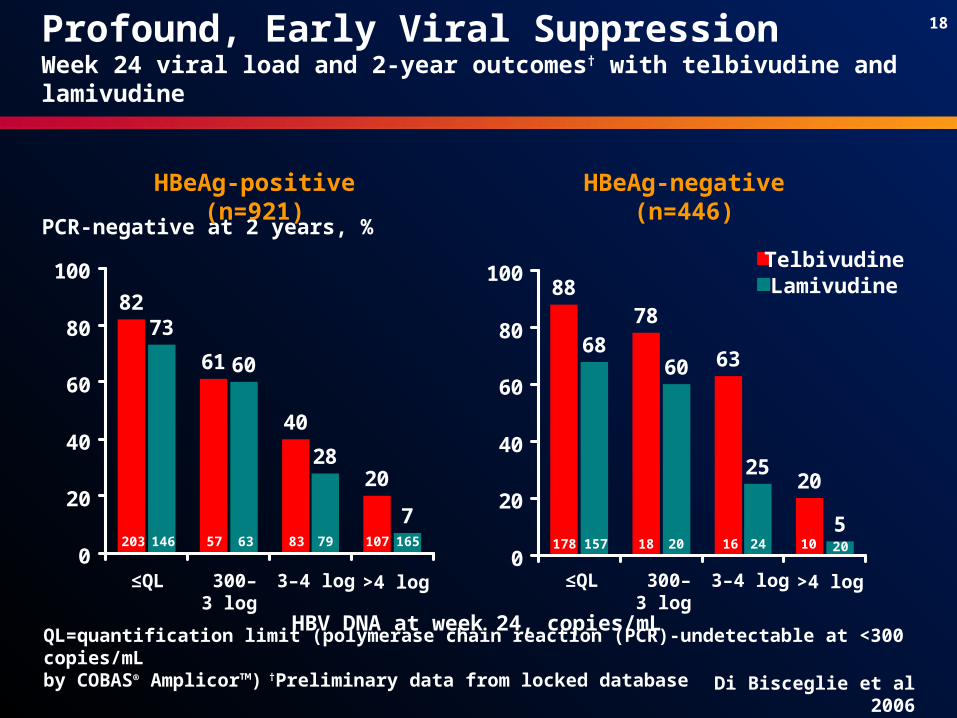
Profound, Early Viral Suppression Week 24 viral load and 2-year outcomes† with telbivudine and lamivudine
QL=quantification limit (polymerase chain reaction (PCR)-undetectable at <300 copies/mL by COBAS® Amplicor™) †Preliminary data from locked database Di Bisceglie et al 2006
HBV DNA at week 24, copies/mL
PCR-negative at 2 years, %
HBeAg-positive (n=921) HBeAg-negative (n=446)
≤QL 300–3 log
3–4 log >4 log ≤QL 300–3 log
3–4 log >4 log
TelbivudineLamivudine
203 146 57 63 83 79 107 165
6860
25
5
8878
63
20
0
20
40
60
80
100
178 157 18 20 16 24 10 20
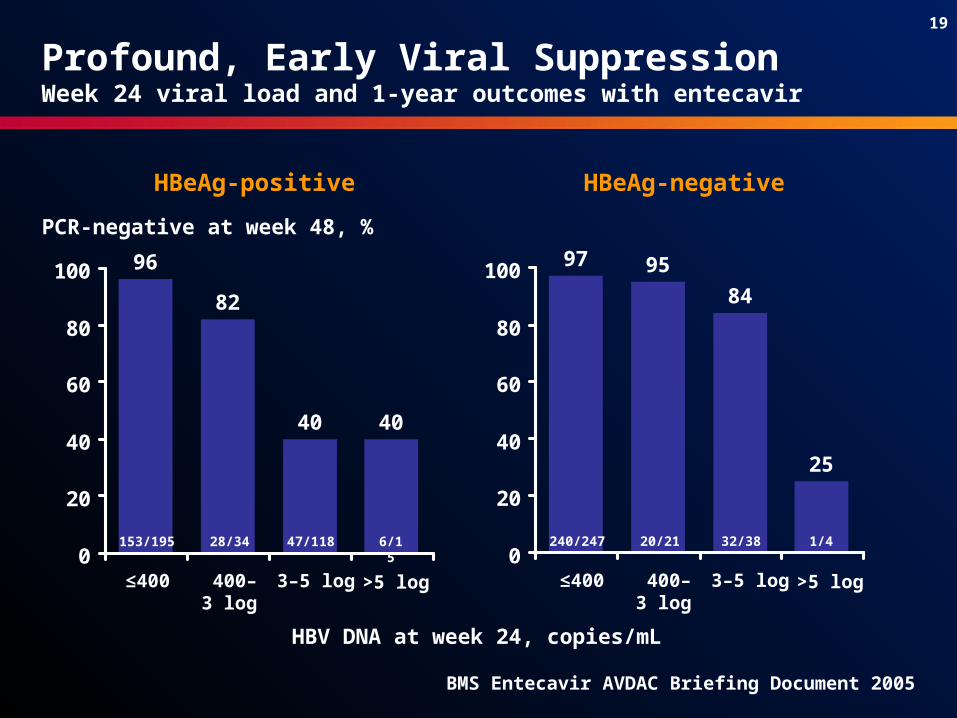
19
97 95
84
25
0
20
40
60
80
10096
82
40 40
0
20
40
60
80
100
Profound, Early Viral Suppression Week 24 viral load and 1-year outcomes with entecavir
HBV DNA at week 24, copies/mL
PCR-negative at week 48, %
HBeAg-positive HBeAg-negative
≤400 400–3 log
3–5 log >5 log ≤400 400–3 log
3–5 log >5 log
153/195 28/34 47/118 6/15 240/247 20/21 32/38 1/4
BMS Entecavir AVDAC Briefing Document 2005
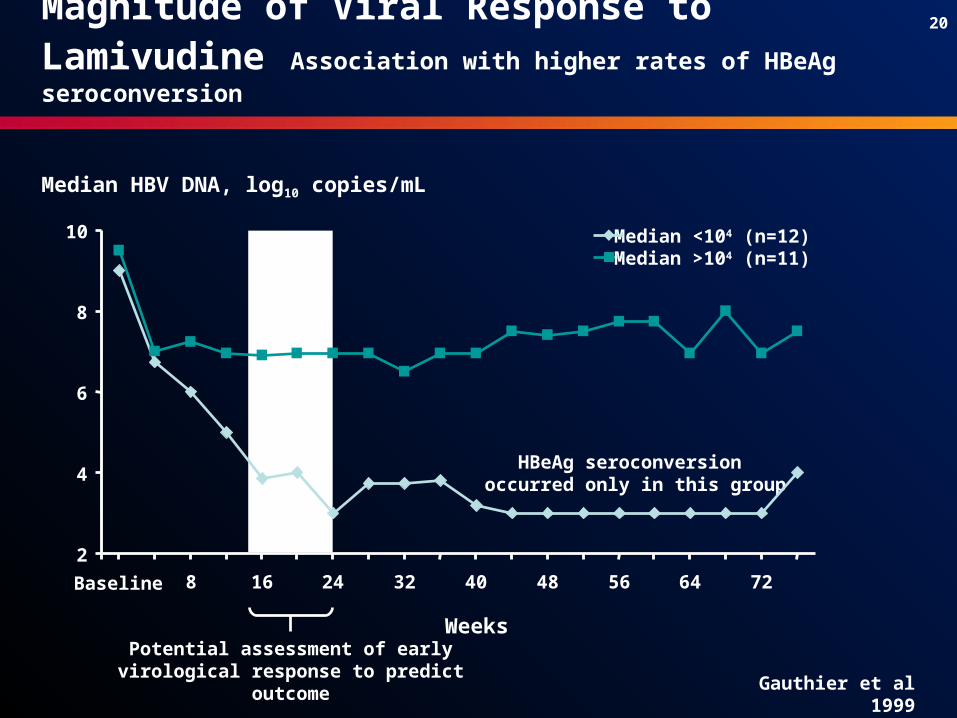
20
HBeAg seroconversion occurred only in this group4
6
8
10
2
Baseline 8 16 24 32 40 48 56 64 72
Weeks
Median HBV DNA, log10 copies/mL
Median >104 (n=11)Median <104 (n=12)
Potential assessment of early virological response to predict outcome Gauthier et al 1999
Magnitude of Viral Response to Lamivudine Association with higher rates of HBeAg seroconversion
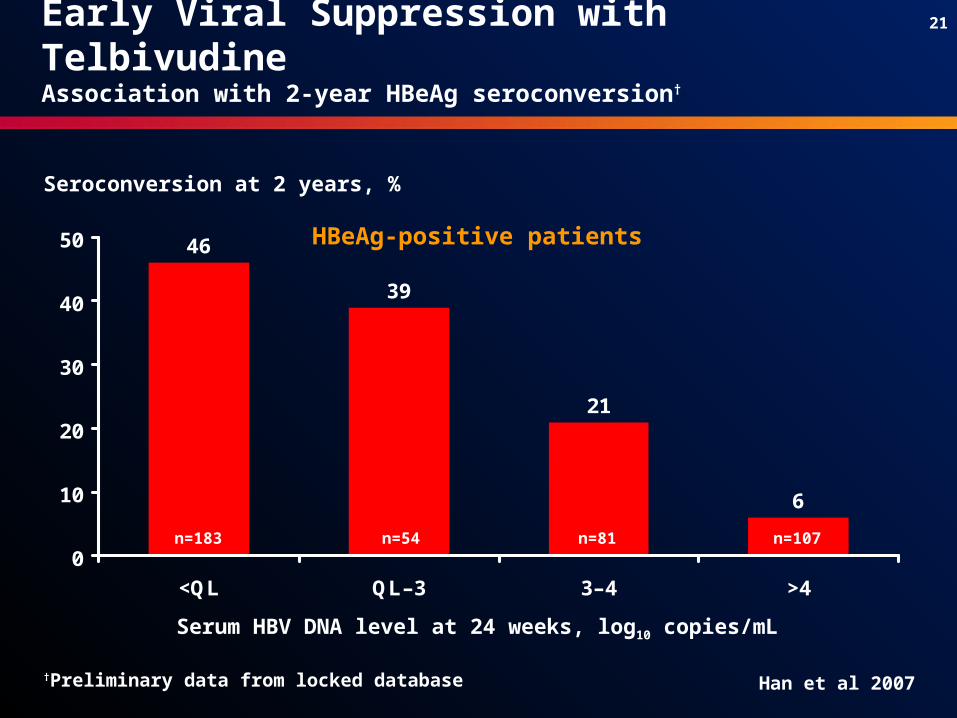
21
6
21
39
46
0
10
20
30
40
50
<QL QL–3 3–4 >4
n=183 n=54 n=81 n=107
Seroconversion at 2 years, %
Serum HBV DNA level at 24 weeks, log10 copies/mL
Early Viral Suppression with Telbivudine Association with 2-year HBeAg seroconversion†
HBeAg-positive patients
Han et al 2007†Preliminary data from locked database
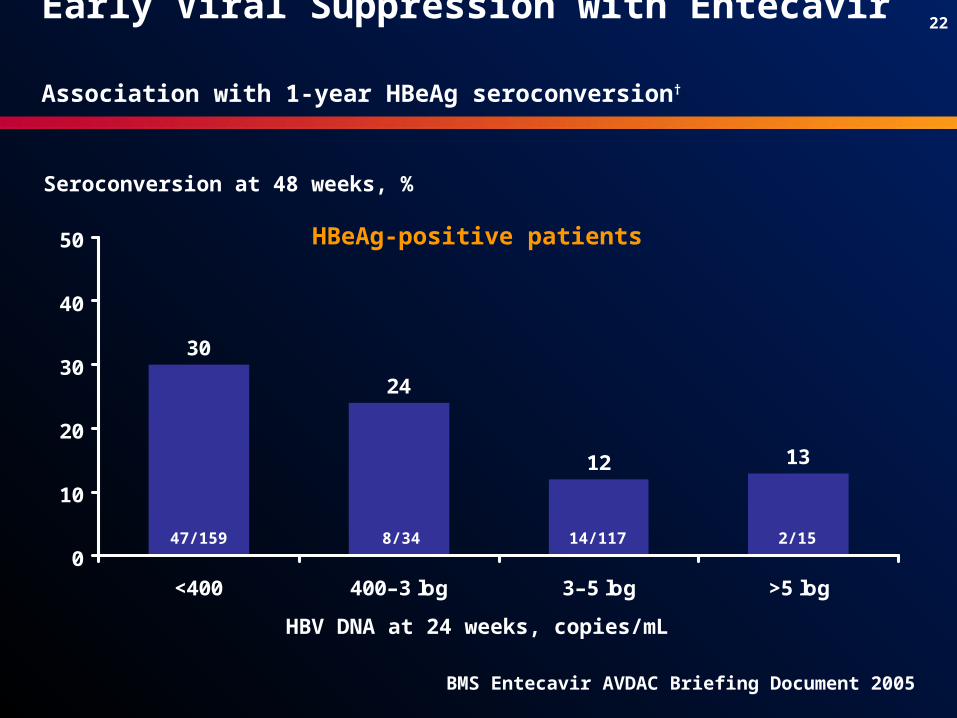
22
1312
24
30
0
10
20
30
40
50
<400 400–3 log 3–5 log >5 log
47/159 8/34 14/117 2/15
Seroconversion at 48 weeks, %
HBV DNA at 24 weeks, copies/mL
HBeAg-positive patients
BMS Entecavir AVDAC Briefing Document 2005
Early Viral Suppression with Entecavir Association with 1-year HBeAg seroconversion†
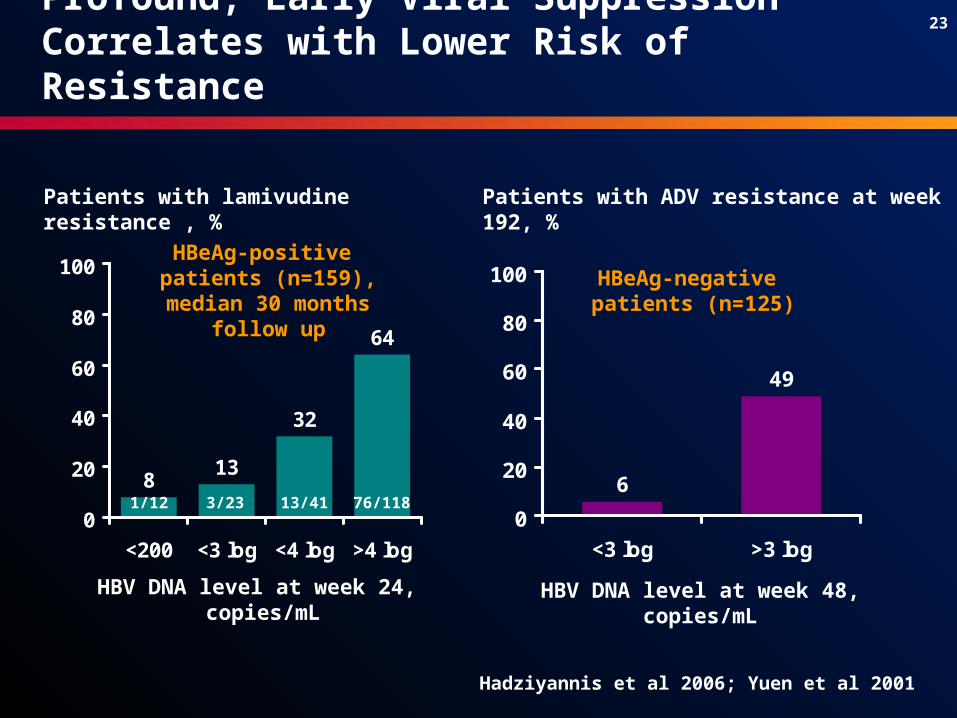
23
64
32
138
0
20
40
60
80
100
<200 <3 log <4 log >4 log
Profound, Early Viral Suppression Correlates with Lower Risk of Resistance
Hadziyannis et al 2006; Yuen et al 2001
Patients with lamivudine resistance , %
HBeAg-positive patients (n=159), median
30 months follow up
HBV DNA level at week 24, copies/mL
1/12 3/23 13/41 76/118
49
6
0
20
40
60
80
100
<3 log >3 log
Patients with ADV resistance at week 192, %
HBeAg-negative patients (n=125)
HBV DNA level at week 48, copies/mL
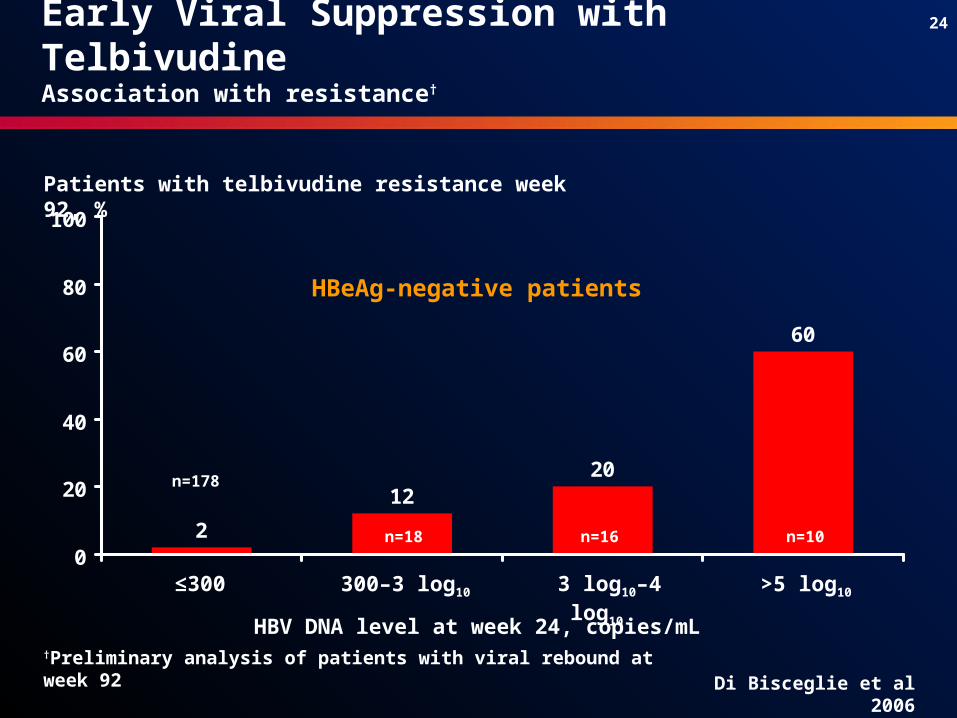
24
2
1220
60
0
20
40
60
80
100
HBeAg-negative patients
Patients with telbivudine resistance week 92, %
n=178
n=16n=18 n=10
Di Bisceglie et al 2006
Early Viral Suppression with TelbivudineAssociation with resistance†
†Preliminary analysis of patients with viral rebound at week 92
HBV DNA level at week 24, copies/mL
≤300 300–3 log10 3 log10–4 log10 >5 log10

25
HBeAg loss
Liver inflammation and fibrosis
HBeAg-positive
HBeAg-negative
Reduce serum HBV DNA
Normal ALT PCR negative
Anti-HBeAg sero-conversion
HBsAg loss
Reduce serum HBV DNA
Normal ALTPCR negative
HBsAg loss
Goals of HBV therapya) Prevent cirrhosis,
liver failure and HCCb) Improve survival
Signpost
Signpost
Early Viral Suppression Can Be a Signpost for Future Therapeutic Response
StartRx.

26
On-Treatment Roadmap Concept
27
Potential Foundation for Building a CHB Therapeutic Roadmap
On-treatnent early virological response monitoring Can help to identify suboptimal responders Provides opportunities to modify treatment to
enhance antiviral efficacy Can help support individualised treatment maps Has the potential to improve long-term outcomes
Response markers act as signposts for clinical management
Chosen therapy is effective and well tolerated
Additional interventions
required

28
Unresolved questionsWhat Is the best on-treatment marker?When Is the best timing for decision points?What Cut-off level for on-treatment decisions?Which Type of initial/add-on therapy?
? ?
Expert panel convened to evaluate evidence and develop
treatment recommendations
Report of an International Workshop: Roadmap for Management of Patients Receiving Oral Therapy for Chronic Hepatitis BKeeffe EB et al.Clinical Gastroenterology and Hepatology 2007
Proposed New Treatment Algorithm for CHBRecent expert panel and Roadmap publication
Keeffe et al 2007
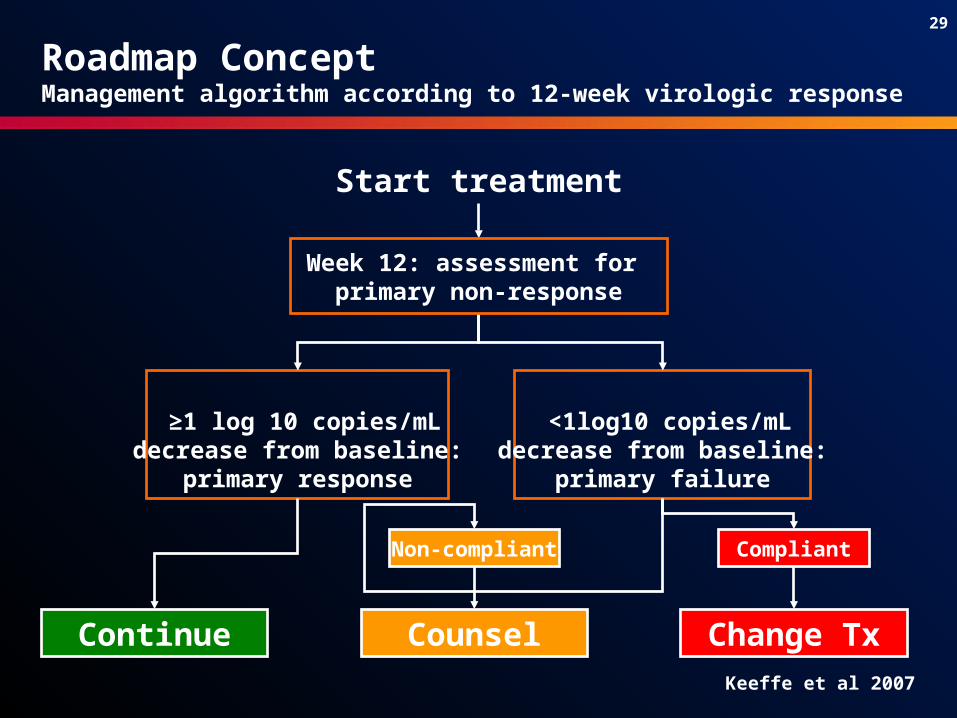
29
Start treatment
≥1 log 10 copies/mLdecrease from baseline:
primary response
Roadmap ConceptManagement algorithm according to 12-week virologic response
Continue
<1log10 copies/mLdecrease from baseline:
primary failure
Non-compliant Compliant
Counsel Change Tx
Week 12: assessment for primary non-response
Keeffe et al 2007
30
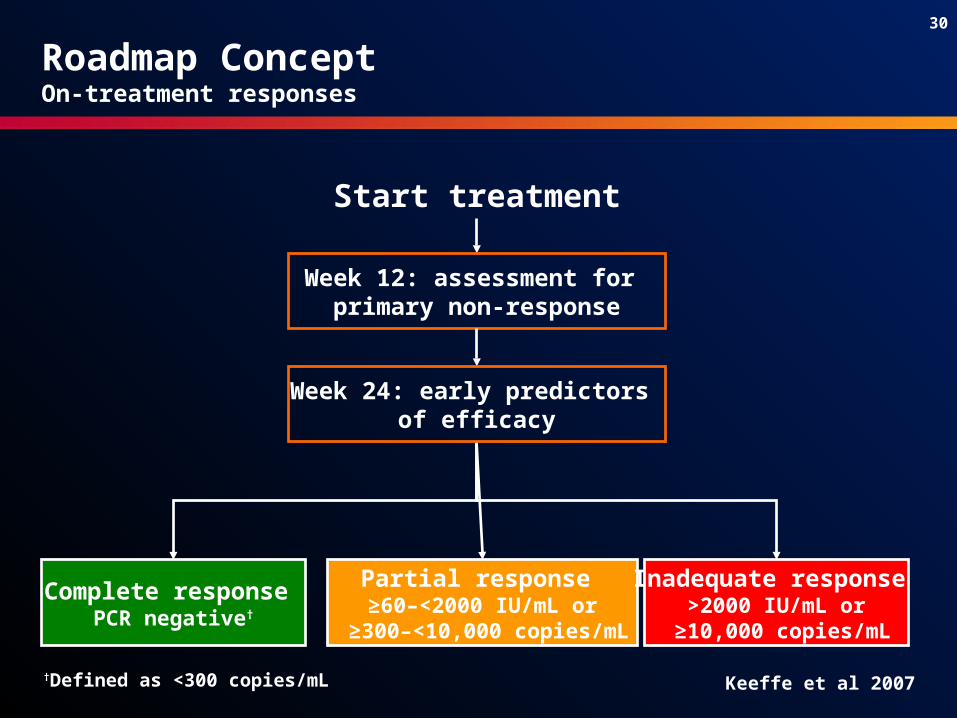
Start treatment
Roadmap ConceptOn-treatment responses
Complete response PCR negative†
Partial response ≥60–<2000 IU/mL or
≥300–<10,000 copies/mL
Inadequate response >2000 IU/mL or
≥10,000 copies/mL
Week 12: assessment for primary non-response
Week 24: early predictors of efficacy
Keeffe et al 2007†Defined as <300 copies/mL
31
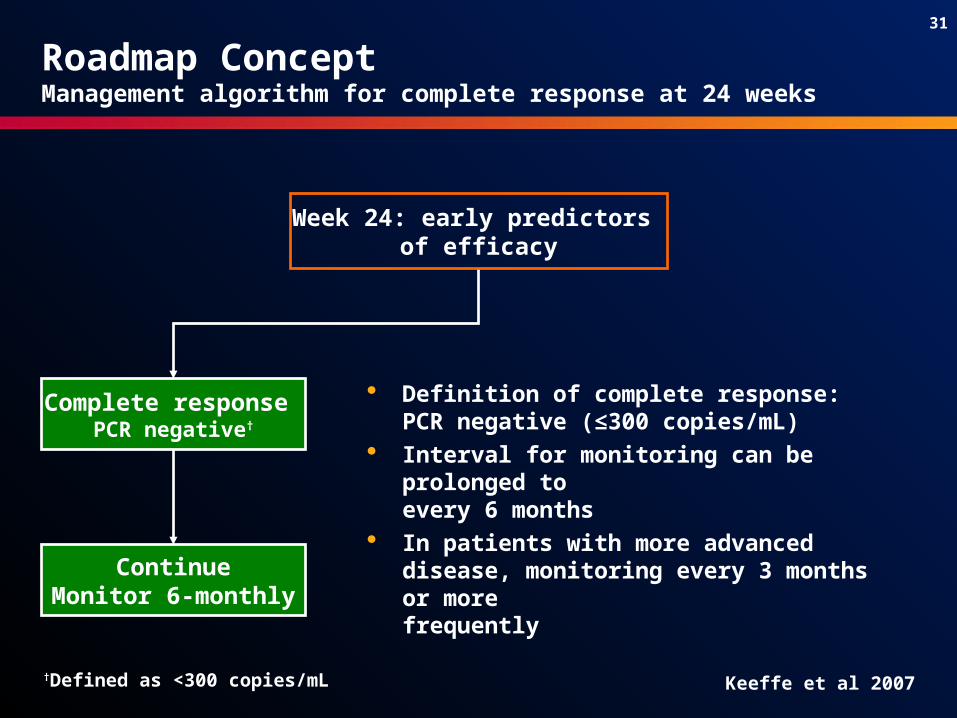
Roadmap ConceptManagement algorithm for complete response at 24 weeks
Complete response PCR negative†
ContinueMonitor 6-monthly
Definition of complete response: PCR negative (≤300 copies/mL)
Interval for monitoring can be prolonged to
every 6 months In patients with more advanced disease,
monitoring every 3 months or more frequently
Week 24: early predictors of efficacy
Keeffe et al 2007†Defined as <300 copies/mL

32
Roadmap ConceptManagement algorithm for partial response at 24 weeks
Week 24: early predictors of efficacy
Keeffe et al 2007
Partial response≥60–<2000 IU/mL or
≥300–<10,000 copies/mL
Add another drugwithout cross-
resistance or continueMonitor 3-monthly
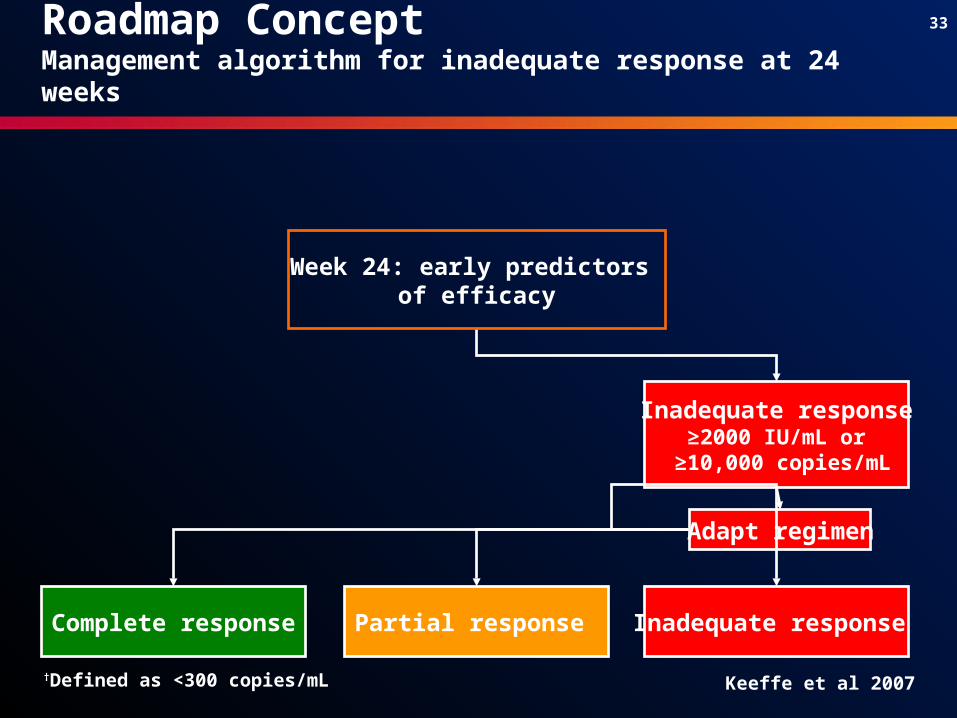
33
Inadequate response≥2000 IU/mL or
≥10,000 copies/mL
Adapt regimen
Complete response Partial response Inadequate response
Roadmap ConceptManagement algorithm for inadequate response at 24 weeks
Week 24: early predictors of efficacy
Keeffe et al 2007†Defined as <300 copies/mL
34
HBV Roadmap Proposal: Monitoring
Monitor every 3 months If patient achieves complete response by 48 weeks, follow
monitoring recommendation (6-monthly) If patient shows continuous decline up to 48 weeks, but still has
higher viral load than a complete responder, continue to monitor every 3 months
If patient shows an increase or ‘plateauing’ of viral level, they should be treated based on roadmap recommendation for inadequate or non-responder
In patients with more advanced disease, more frequent monitoring may be indicated
Keeffe et al 2007

35
Summary and ConclusionsImportance of early monitoring of virologic response to therapy
Early and sustained viral suppression has been associated with prevention of disease progression
HBV DNA is a critical signpost in the on-treatment management of CHB
On-treatment management offers opportunities to optimise treatment response– Essential to identify suboptimal responses– Modify management to enhance antiviral efficacy – Potential to improve long-term outcomes
36
How should the roadmap be applied to telbivudine?
37
37Conclusion fromReport of an International Workshop: Roadmap for Management
of Patients Receiving Oral Therapy for Chronic Hepatitis B
Early monitoring of the virologic response to therapy in chronic hepatitis B treated with oral nucleos(t)ides is essential…
Use of this roadmap should permit improved individualized on-treatment management designed to enhance long-term patient
outcomes
1.Keeffe EB, Zeuzem S, Koff RS, Dieterich DT, Esteban-Mur R, Gane E, Jacobson IM, Lim SG,Naoumov NN, Marcellin P, Piratvisuth T, Zoulim F. Clin Gastroenterol Hepatol. In press.
38
38
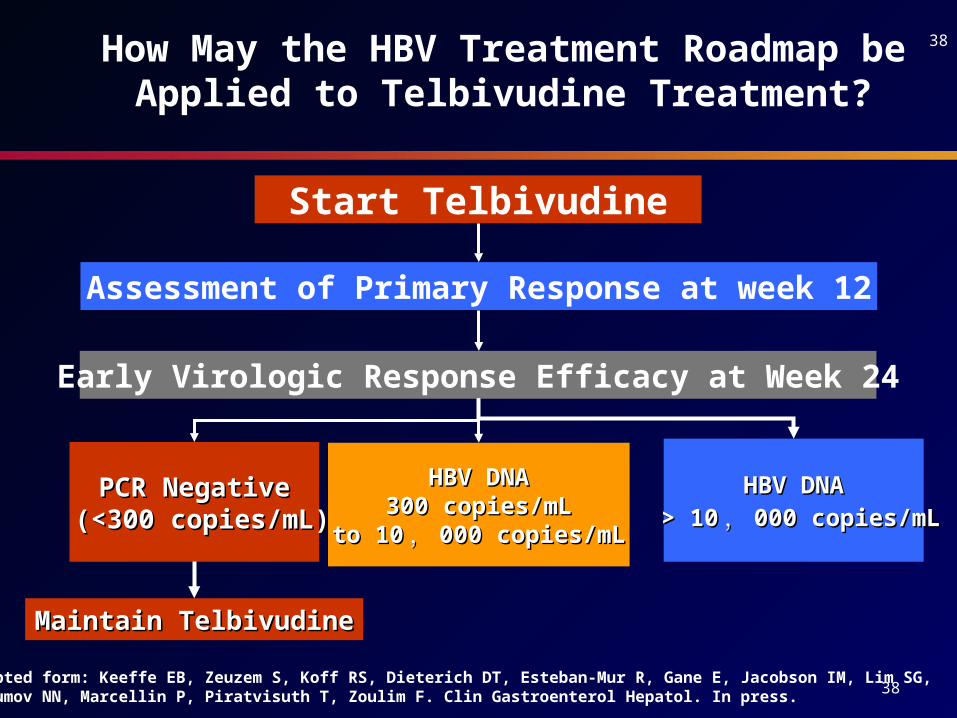
Adapted form: Keeffe EB, Zeuzem S, Koff RS, Dieterich DT, Esteban-Mur R, Gane E, Jacobson IM, Lim SG,Naoumov NN, Marcellin P, Piratvisuth T, Zoulim F. Clin Gastroenterol Hepatol. In press.
Start Telbivudine
Early Virologic Response Efficacy at Week 24
PCR NegativePCR Negative (<300 copies/mL)(<300 copies/mL)
HBV DNAHBV DNA300 copies/mL300 copies/mL
to 10to 10 ,, 000 copies/mL000 copies/mL
HBV DNAHBV DNA
> 10> 10 ,, 000 copies/mL000 copies/mL
Assessment of Primary Response at week 12
Maintain TelbivudineMaintain Telbivudine
How May the HBV Treatment Roadmap be Applied to Telbivudine Treatment?
39
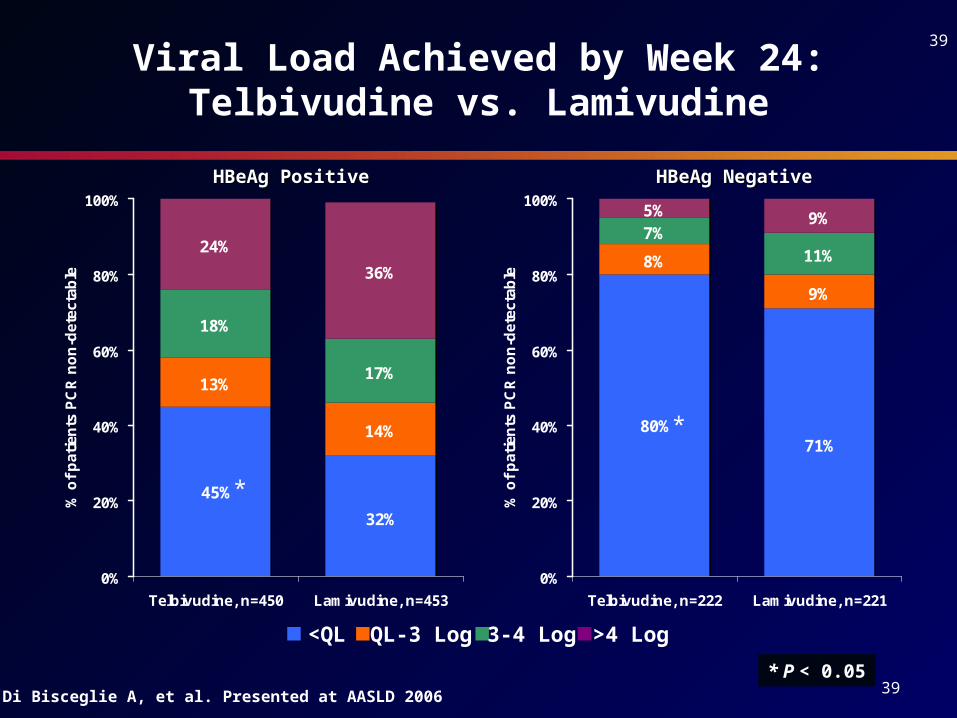
39Viral Load Achieved by Week 24:
Telbivudine vs. Lamivudine
13%
14%
18%
17%
24%
36%
32%
45%
0%
20%
40%
60%
80%
100%
Telbivudine, n=450 Lamivudine, n=453
% o
f p
atie
nts
PC
R n
on
-det
ecta
ble
8%
9%
7%11%
5% 9%
71%80%
0%
20%
40%
60%
80%
100%
Telbivudine, n=222 Lamivudine, n=221
% o
f p
atie
nts
PC
R n
on
-det
ecta
ble
Di Bisceglie A, et al. Presented at AASLD 2006
<QL QL-3 Log 3-4 Log >4 Log
HBeAg Positive HBeAg Positive HBeAg Negative HBeAg Negative
*
*
* P < 0.05
40
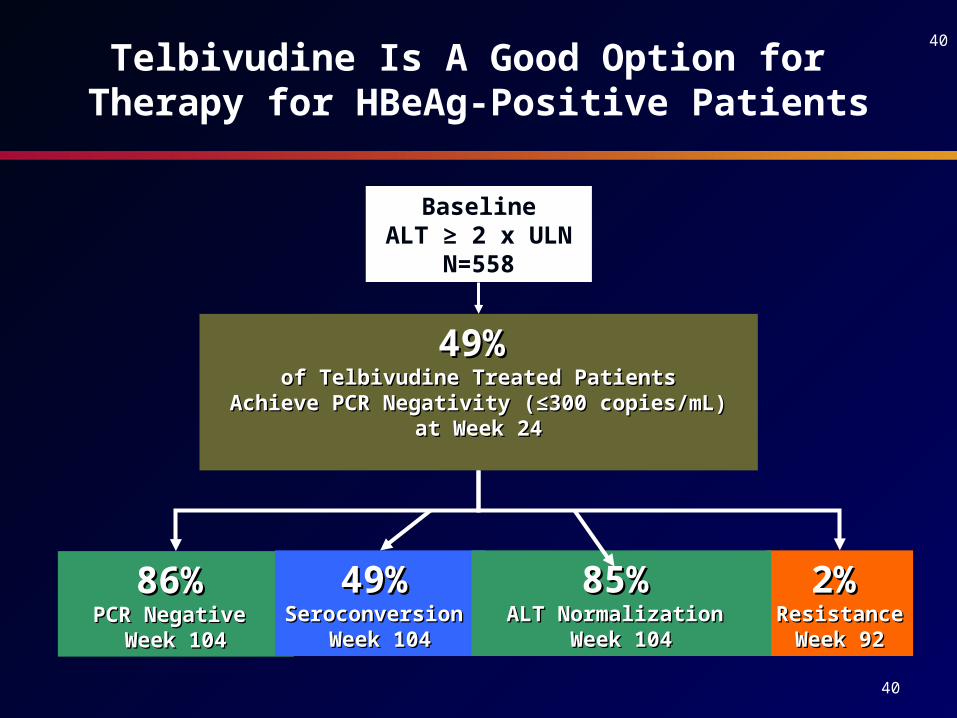
40Telbivudine Is A Good Option for Therapy for
HBeAg-Positive Patients
49%49% of Telbivudine Treated Patientsof Telbivudine Treated Patients
Achieve PCR Negativity (≤300 copies/mL)Achieve PCR Negativity (≤300 copies/mL) at Week 24 at Week 24
86%86% PCR Negative PCR Negative
Week 104Week 104
49%49% Seroconversion Seroconversion
Week 104Week 104
2%2% ResistanceResistance
Week 92Week 92
BaselineALT ≥ 2 x ULN
N=558
85%85% ALT Normalization ALT Normalization
Week 104Week 104

41
41Telbivudine Is A Good Option for Therapy for
HBeAg-Negative Patients
80%80% of Telbivudine Treated Patientsof Telbivudine Treated Patients
Achieve PCR Negativity (≤300 copies/mL)Achieve PCR Negativity (≤300 copies/mL) at Week 24 at Week 24
88%88% PCR Negative PCR Negative
Week 104Week 104N=78/86N=78/86
2%2% Resistance at Resistance at
92 weeks92 weeks
49%49% Seroconversion Seroconversion
Week 104Week 104
All telbivudine-treatedHBeAg-Negative Patients
N=588
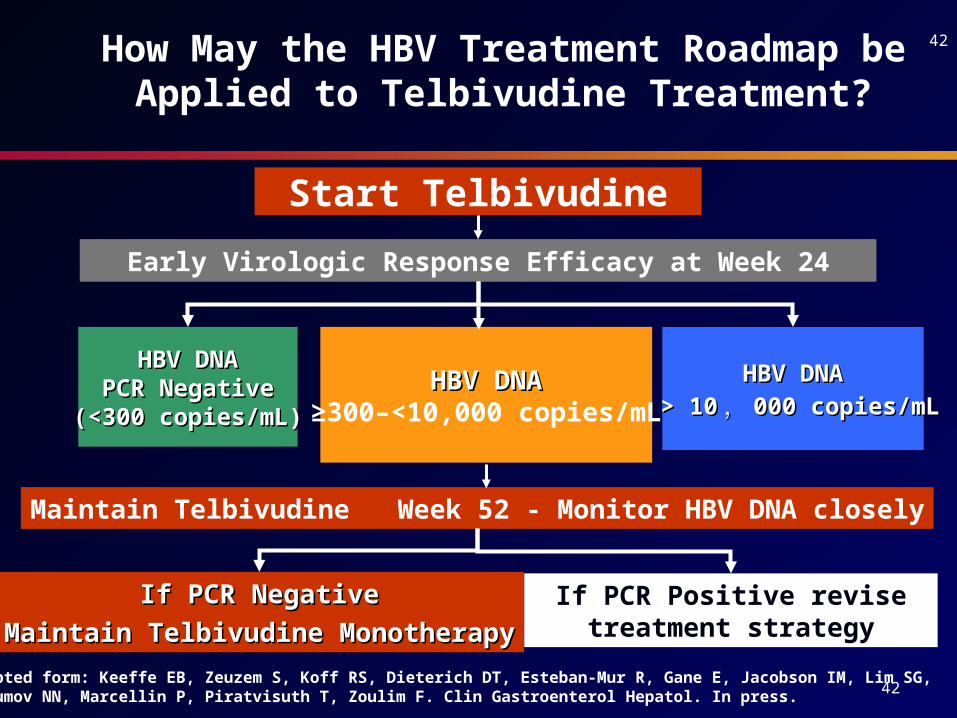
42
42
Start Telbivudine
Early Virologic Response Efficacy at Week 24
HBV DNAHBV DNAPCR NegativePCR Negative
(<300 copies/mL)(<300 copies/mL)
HBV DNAHBV DNA≥300–<10,000 copies/mL
HBV DNAHBV DNA
> 10> 10 ,, 000 copies/mL000 copies/mL
Maintain Telbivudine Week 52 - Monitor HBV DNA closely
How May the HBV Treatment Roadmap be Applied to Telbivudine Treatment?
If PCR NegativeIf PCR Negative
Maintain Telbivudine MonotherapyMaintain Telbivudine MonotherapyIf PCR Positive revise
treatment strategy
Adapted form: Keeffe EB, Zeuzem S, Koff RS, Dieterich DT, Esteban-Mur R, Gane E, Jacobson IM, Lim SG,Naoumov NN, Marcellin P, Piratvisuth T, Zoulim F. Clin Gastroenterol Hepatol. In press.
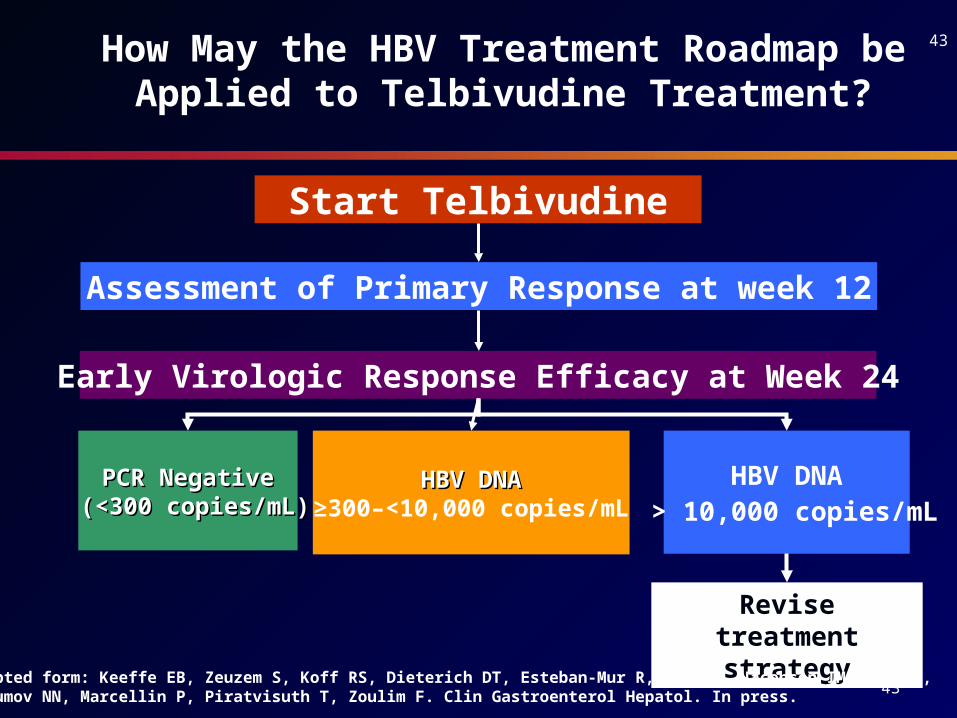
43
43
Start Telbivudine
Early Virologic Response Efficacy at Week 24
PCR NegativePCR Negative (<300 copies/mL)(<300 copies/mL)
HBV DNAHBV DNA≥300–<10,000 copies/mL
HBV DNA > 10,000 copies/mL
Assessment of Primary Response at week 12
How May the HBV Treatment Roadmap be Applied to Telbivudine Treatment?
Revise treatment strategy
Adapted form: Keeffe EB, Zeuzem S, Koff RS, Dieterich DT, Esteban-Mur R, Gane E, Jacobson IM, Lim SG,Naoumov NN, Marcellin P, Piratvisuth T, Zoulim F. Clin Gastroenterol Hepatol. In press.
44
44







![Model CHB-100 CHB-130 - Utica Boilers IOM Rev...cod. 3541F240 WALL MOUNTED GAS BOILER INSTALLATION, OPERATION & MAINTENANCE MANUAL P/N# 240010633, Rev. B [07/17/2014] Model CHB-100](https://static.documents.pub/doc/80x56/5e53722938b2520b2c184679/model-chb-100-chb-130-utica-boilers-iom-rev-cod-3541f240-wall-mounted-gas.jpg)









