45
1 The California DUI Treatment System A Presentation for the California Behavioral Health Directors Association SAPT+ Committee March 26 2015
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | griffin-lee |
| View: | 219 times |
| Download: | 0 times |
1
The CaliforniaDUI Treatment System
A Presentation for the California Behavioral Health Directors AssociationSAPT+ CommitteeMarch 26 2015
2
Bob DorrisRetired, The High Road Program
CADTP Board of DirectorsCADTP Counselor Certification Board
Barbara Aday-GarciaOHS San Marcos
CADTP Board of [email protected]
Your Presenters
Teri KernsOHS
CADTP Board of DirectorsStrategic Highway Safety Plan
DHCS DUI Advisory [email protected]
Craig FrenchTwin Palms Recovery Center
CADTP Board of DirectorsDHCS DUI Advisory [email protected]
Todays Objectives
DUI Programs - The History and Current Story
Program Fees
Evaluation of Effectiveness
Client Services
Is the DUI Program Treatment
Standard Assessments
Collaboration 3
History In 1978 the California Legislature mandated development of
programs that would be designed to reduce the high level of recidivism of individuals arrested and convicted of driving-under-the-influence [DUI], endangering public safety by individuals consuming alcohol and drugs and driving on California streets and highways.
The legislature passed Senate Bill 38 creating a post-conviction program and assigned the Department of Alcohol and Drug Programs responsibility for developing regulations based on state law, i.e. §11836 – §11837 of the California Health and Safety Code, and §23161 – §23181 of the California Vehicle Code.
The initial focus of the legislature was on alcohol related offenses. Over the past thirty-six (36) years, program services have evolved to focus on any type of DUI offense, i.e. alcohol, licit [prescription] and/or illegal drugs.
4
The DUI System Today
DUI programs are licensed by the Department of Health Care Services to provide a less intensive level of outpatient alcohol and other drug treatment services focused on improving public health and safety by reducing and/or eliminating additional DUI offenses.
These services consist of education classes (prevention); individual and group counseling sessions (intervention); and in some counties individual client involvement in self-help programs to facilitate ongoing recovery from the abuse of alcohol and drugs.
Consistent with state regulations DUI treatment is provided by alcohol and other drug counselors certified under Chapter 8, Division 4, Title 9, California Code of Regulations.
5
The DUI System Today
DUI treatment programs collaborate with the Courts and the Department of Motor Vehicles to ensure client compliance with summary or formal probation requirements and prepare clients to regain their to drivers license by successfully completing their DUI treatment program.
While program services are focused on refraining from operating an automobile [or any mode of transportation] while under-the-influence, DUI services also provide clients with a new understanding of their individual responsibility to themselves, their families, and their community, and a healthy new approach to their use of alcohol and drugs.
6
7
DUI Program Fees
Myth vs. Fact
8
Myth:“DUI program providers are allowed to charge exorbitant fees and make huge profits”.
Fact:
DUI program fees are approved and controlled by the Department of Health Care Services and by law are limited to earning a maximum 10% profit/surplus of total DUI revenue
Fee Structure
DUI treatment program fees are regulated under §9878 – Chapter 3, Division 4, Title 9, California Code of Regulations. In part these regulations state:
The program fee shall be set at a level sufficient to cover the cost of program services, including each participant's share of personnel and operating expenses incurred by the program in providing program services.
The licensee shall charge only the program fee and any additional fees that have been approved by the Department pursuant to this section of regulation. The licensee shall not increase program fees unless a request has been submitted to the county alcohol and drug program administrator and approved by the Department.
The program shall establish and use a standardized payment schedule, approved by the Department in accordance with this subsection, to determine each participant's assessed program fee and schedule for payment of fees.
9
Myth vs. FactMyth“DUI treatment service providers receive state and/or county funding to provide services to clients.”
10
Fact
California’s DUI treatment system is one hundred percent (100%) self-funded by program fees paid by the client.
From inception of the system in 1978, the State Legislature made it mandatory that the system would be self-funded. That remains true today … there is no tax-payer money funding the system and its services.
The DUI Programs collect participant fees for providing program services plus fees to reimburse the State and County for their monitoring and compliance auditing services as required by state law.
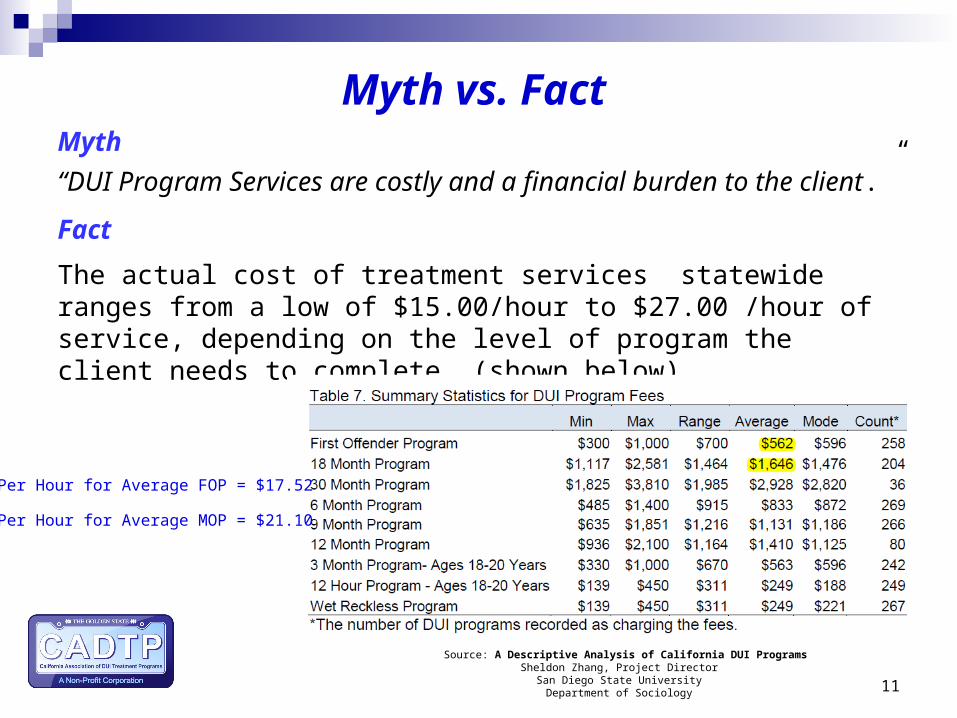
Myth vs. FactMyth
“DUI Program Services are costly and a financial burden to the client.”
Fact
The actual cost of treatment services statewide ranges from a low of $15.00/hour to $27.00 /hour of service, depending on the level of program the client needs to complete, (shown below).
11
Source: A Descriptive Analysis of California DUI ProgramsSheldon Zhang, Project Director
San Diego State University Department of Sociology
Per Hour for Average FOP = $17.52
Per Hour for Average MOP = $21.10
12
Evaluating the Effectiveness
Myth vs. FactMyth:
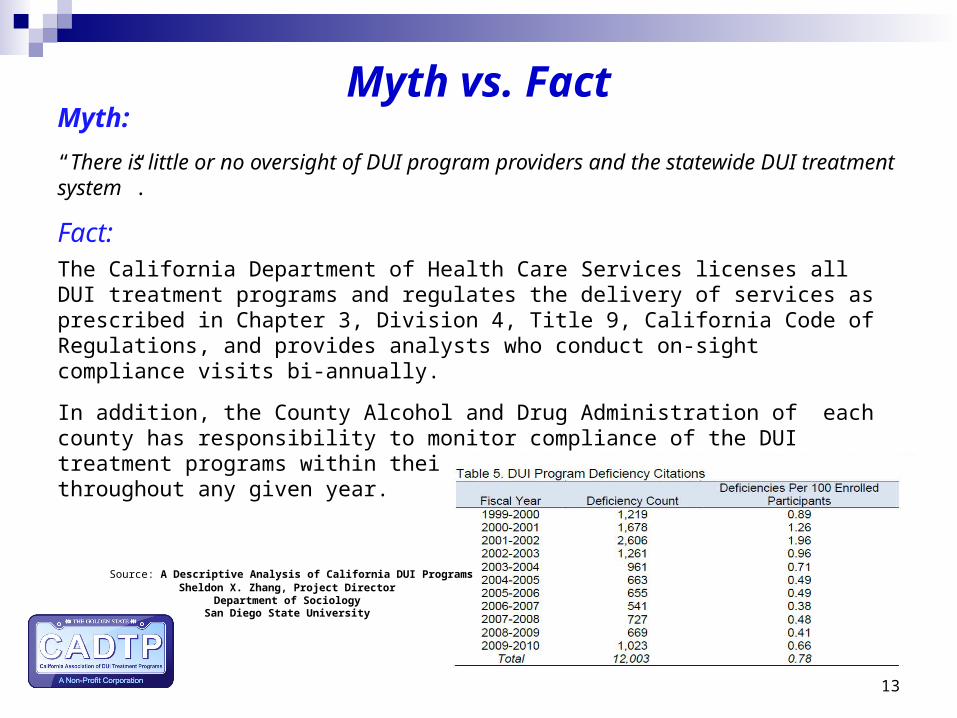
“There is little or no oversight of DUI program providers and the statewide DUI treatment system”.
Fact:The California Department of Health Care Services licenses all DUI treatment programs and regulates the delivery of services as prescribed in Chapter 3, Division 4, Title 9, California Code of Regulations, and provides analysts who conduct on-sight compliance visits bi-annually.
In addition, the County Alcohol and Drug Administration of each county has responsibility to monitor compliance of the DUI treatment programs within their county on a consistent basis throughout any given year.
13
Source: A Descriptive Analysis of California DUI ProgramsSheldon X. Zhang, Project Director
Department of SociologySan Diego State University
Evaluating the System
For 23 years the California Department of Motor Vehicles [DMV] has conducted annual outcome studies on the effectiveness of the California DUI system in reducing recidivism.
The DMV Annual DUI MIS Reports can be found at:
http://www.dmv.ca.gov/portal/dmv/detail/about/profile/rd/toc
14
Evaluating the DUI System
15
2014 DMV DUI MIS Report:
The 1-year recidivism rates for all first DUI offenders decreased to the lowest level seen in the past 22 years. The DUI re-offense rate for first offenders arrested in 2011 was 50.0% lower than the re-offense rate for first offenders arrested in 1990
The 1-year re-offense rate for second DUI offenders also decreased about 50% in the past 22 years, from 9.7% in 1990 to 4.9%
Subsequent 1-year crash rates among second DUI offenders have declined from 4.0% in 1990 to 1.7% in 2011, a 57.5% relative decrease.
The crash rate for first offenders has also declined; their 2011 rate is 52.8% lower than their 1990 crash rate (see Figure 7 and Table 11a)
Evaluating the DUI Program
16
2014 DMV DUI MIS Report:
Alcohol or drug reckless offenders assigned to a DUI program show a 17.2% lower crash rate than those not assigned to the program.
Alcohol or drug-reckless offenders assigned to a DUI program show a statistically fewer number of DUI incidents in the 1 year following their assignment than those who were not assigned
Of the DUI offenders arrested in 2011 who enrolled in a DUI intervention program, 87.8% of first offenders and 41.1% of second offenders completed their program assignment
Among convicted DUI offenders arrested in 2011, 73.7% were first offenders and 26.3% were repeat offenders (one or more prior convictions within the previous 10 years). The proportion of repeat offenders has decreased considerably since 1989, when it stood at 37%,even though prior DUI convictions are counted over 10 years now, but only over 7 years in 1989
17
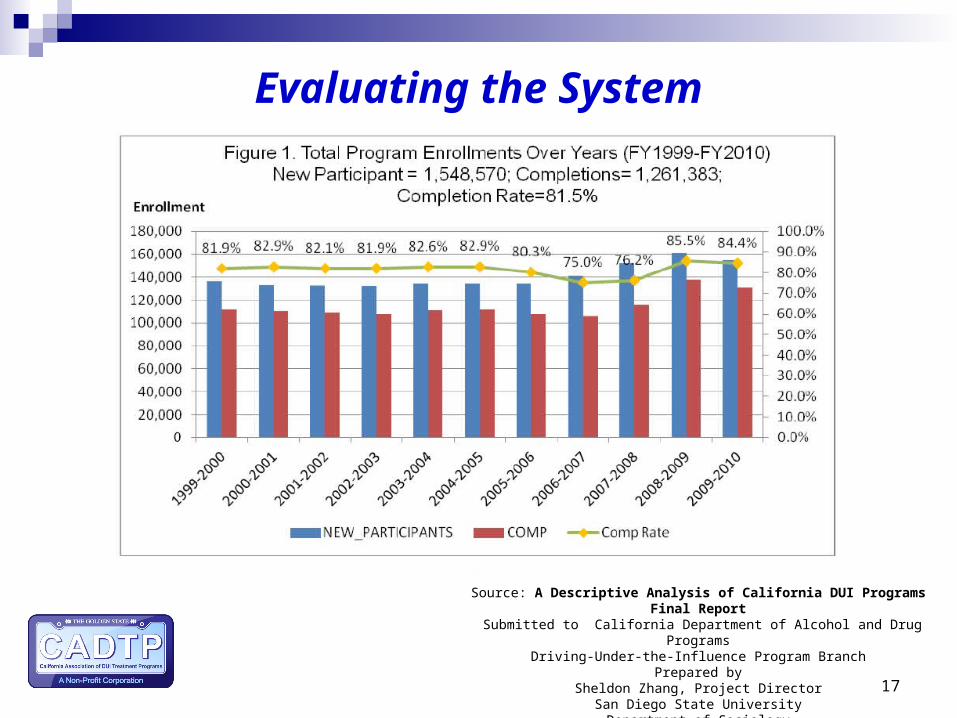
Evaluating the System
Source: A Descriptive Analysis of California DUI Programs Final Report
Submitted to California Department of Alcohol and Drug Programs Driving-Under-the-Influence Program Branch
Prepared by Sheldon Zhang, Project Director
San Diego State University Department of Sociology
18
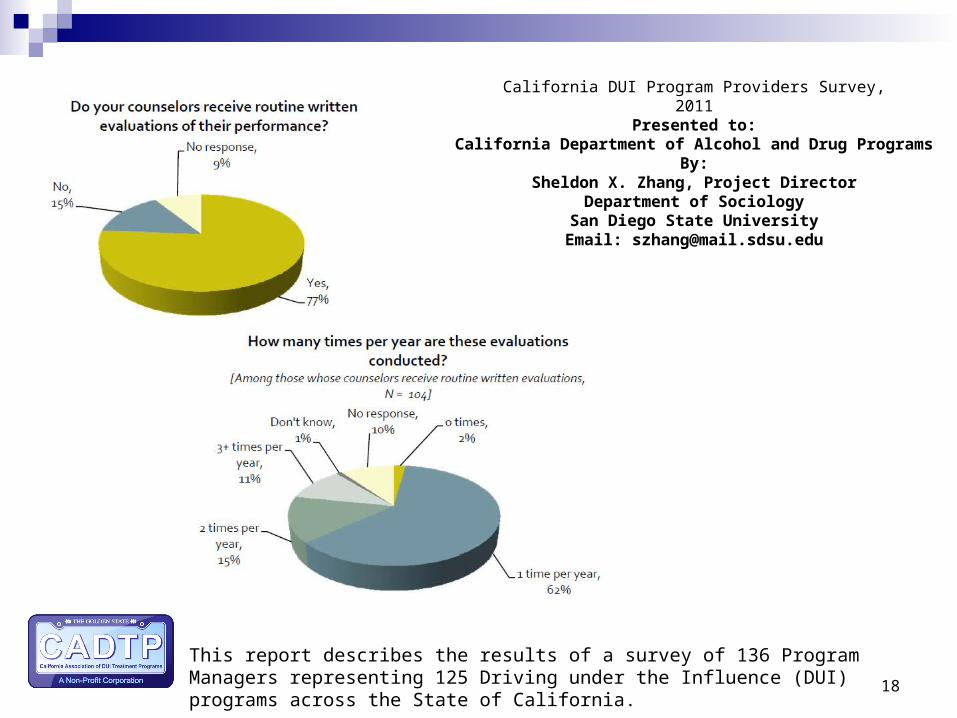
California DUI Program Providers Survey,2011
Presented to:California Department of Alcohol and Drug Programs
By:Sheldon X. Zhang, Project Director
Department of SociologySan Diego State University
Email: [email protected]
This report describes the results of a survey of 136 Program Managers representing 125 Driving under the Influence (DUI) programs across the State of California.
19
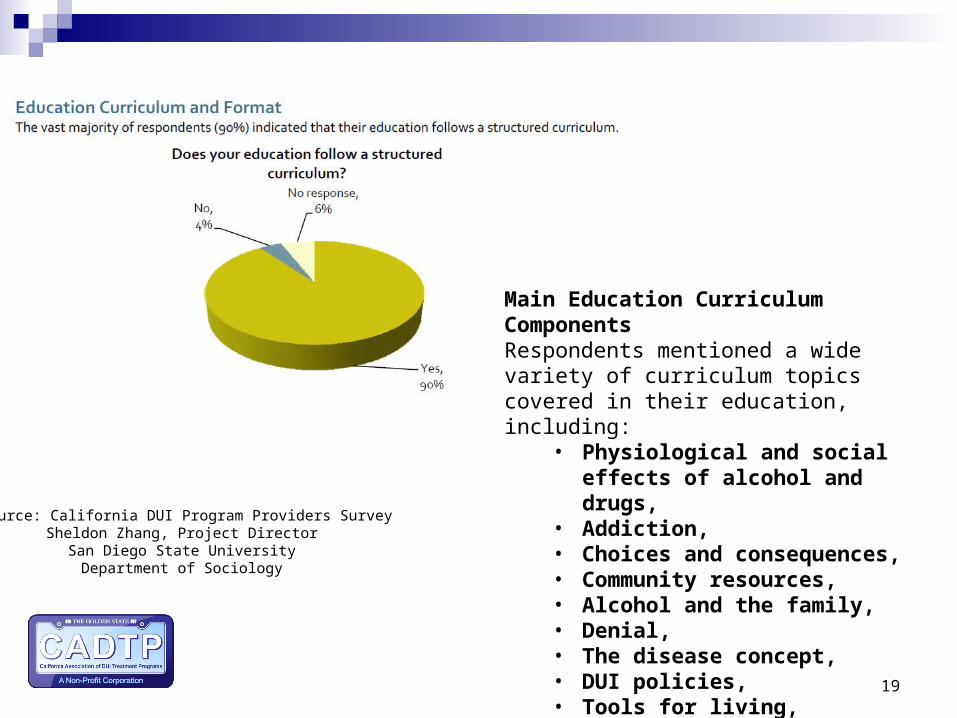
Main Education Curriculum ComponentsRespondents mentioned a wide variety of curriculum topics covered in their education, including:
• Physiological and social effects of alcohol and drugs,
• Addiction, • Choices and consequences, • Community resources, • Alcohol and the family, • Denial, • The disease concept, • DUI policies, • Tools for living, • Relapse prevention, • Recovery.
Source: California DUI Program Providers SurveySheldon Zhang, Project Director
San Diego State University Department of Sociology
20
Recommendations
D.1. DUI Program Providers
Short-term measures: (1) establish performance benchmarks; (2) increase transparency in program fees and administrative fees; and (3) increase web presence for all DUI programs.
Long-term measures: (1) establish a mechanism for outcome assessment.
D.2. ADP Oversight (DHCS)
Short-term measures: (1) achieve greater consistency in curriculum development; (2) compile and disseminate vital statistics for statewide DUI programs; (3) compile and publish DUI program fees; (4) assemble and publish an online spreadsheet containing standard programmatic information for all DUI programs.
Long-term measures: (1) establish a more rational fee review and approval procedure; (2) create a rating system using monitoring results to encourage self-improvement through an open and transparent grading system; (3) increase ADP oversight through an updated data tracking system; (4) realign programs that are rarely used and have low completion rates; and (5) invest in research and evaluation of DUI program services.
D.3. County Alcohol and Drug Services
Greater involvement from county alcohol and drug services is needed to mediate emerging or on-going issues between DUI program providers and the state oversight agency.
Source: A Descriptive Analysis of California DUI ProgramsSheldon Zhang, Project Director
San Diego State University Department of Sociology
Court Referral System
21
Title 9 - § 9801.5. County Responsibilities
(b) The county alcohol and drug program administrator shall:
(8) Carry out liaison activities with the courts, the county probation department, DUI programs, and interested parties at the county level.
(9) Develop and insure the implementation of a court referral system as described in Health and Safety Code Section 11837.2.
Strategic Highway Safety PlanChallenge Area 1
22
CADTP Best Practice Document
The best practice document was a collaboration of DUI program representatives who each took a section and the committee agreed upon content to ensure generic enough for implementation.
The intent of this document is to present a set of suggested best practices for licensed DUI Treatment Programs to follow in order to provide quality services and regulatory compliance, resulting in safer communities and healthier individuals at no cost to the tax-payer.

23
Client Services
DUI Program Services
The DUI programs primary goal is to assist participants to explore their relationships with alcohol/drugs and the inherent risks involved
The desired result is modified drinking and/or drug use in high-risk situations such as driving
Our programs provide counseling and education to assist in reducing the recidivism rate of DUI offenders
24
Myth vs. Fact
Orientation to DUI laws, Alcohol & Drug Impairment and the DUI Program
Patterns Of Consumption, Chemical Dependency And Assessment
Medical Aspects Of Alcohol And Other Drugs
Social Aspects Of Alcohol And Other Drugs
Addiction And The Family
Recovery, Resources And Options For ChangeInstructors are certified counselors who must have 2 years of experience providing Alcohol and Other Drugs Education.
Myth: DUI Programs are Education not Counseling
Fact: All AOD Treatment Programs have an Educational Component and so do DUI Treatment Programs
25
26
DUI Programs take a proactive stance in helping those with alcohol and/or drug dependency problems make life-affirming changes.
DUI Programs recognize that substance use behavior exists along a continuum, ranging from non pathological use at one end, to problematic or substance abuse in the middle to chronic substance dependence on the other.
DUI services are designed to address this continuum of use through the education, group and individual case management sessions.
DUI Program Philosophy of Services
27
Wet Reckless Program: Blood Alcohol Content under .08
12 hours of education
3-month First Offender Program - 37.5 % education, 62.5% counseling
Blood Alcohol Content .08 and above 12 hours of education 10 hours of group counseling 3 individual sessions (face to face) Eight additional hours of program services,
consisting of educational sessions, group counseling sessions, or a combination of the two
DUI Program Levels
6-month First Offender Program 26.7% education, 73.3% counseling
Blood Alcohol Content .15 - .19 12 hours of education 28 hours of group counseling Minimum of 4 individual sessions Four additional hours of program services,
consisting of educational sessions, group counseling sessions, face-to-face interviews or a combination of the three
9-month First Offender Program 19.1% education, 80.9% counseling
Blood Alcohol Content .20 and above 12 hours of education 44 hours of group Minimum of 5 individual sessions Four additional hours of program services,
consisting of educational sessions, group counseling sessions, face-to-face interviews or a combination of the three
DUI Program Levels
29
18-month Multiple Offender Program 15.4% education, 84.6% counseling
2 or more DUI’s in a 10 year period The first 12 months of the 18 month program
12 hours of education,
52 hours of group counseling
1 individual session every other week.
The last 6 months of the 18-month program includes up to 6 hours of services.
Each program and/or county determines how to structure the last 6 months of service
DUI Program Levels
30
30-Month Multiple Offender Program 7.9% education, 92.1% counseling
3 or more DUI Offenses in a 10 year period 1st 18 months = 12 hours of education, 78 hours of group
counseling and one face to face session every other week
Last 12 months – DUI Program must continue to monitor compendium of evidence, can credit some time towards last 12 months for residential or in-patient AOD Treatment with court approval
Client must show a compendium of evidence, on a tri-monthly basis, of performance of voluntary community service for one-half of the time served (not less than 120 hours and not more than 300 hours, as determined by the court) demonstrating:
1. The prevention of driving-under-the-influence, promotion of safe driving, and responsible attitude toward the use of chemicals of any kind.
2. Significant improvement in occupational performance (including efforts to obtain gainful employment), physical and mental health, family relations, and financial affairs and economic stability.
DUI Program Levels
* Not available in all Counties in California
Myth: DUI Counselors are not Certified Alcohol & Other Drug Counselors
Fact: Title 9 California Code of Regulations - Staff Qualifications
DUI program staff who conduct educational sessions shall have a minimum of two years of experience in providing alcohol and/or drug education and information to persons with alcohol and/or other drug problems in a classroom setting or meet the staff qualifications required in Section 9846(c) or Section 9846(f).
All DUI program staff who provide counseling services (as defined in Section 13005(a)(4)) shall be licensed, certified, or registered to obtain certificationpursuant to Chapter 8 (commencing with Section 13000) or meet thequalifications required in subdivision (f).
DUI program staff who provide counseling services (as defined in Section13005(a)(4)) shall comply with the code of conduct, pursuant to Section 13060,developed by the organization by which they were certified or registered
Myth vs. Fact
31
32
Individual Counseling Sessions
Face to face sessions address the following questions,
1. “Discuss and identify problems which may be barriers to program completion, including progress in group and other counseling sessions.”
2. “Evaluate the client’s need for referral to ancillary services.”
3. “Discuss and encourage client attendance in educational and counseling sessions.”
4. “Monitor payment of fees.”
A formal substance abuse assessment is conducted within 60 days from enrollment, discussed with the client and appropriate referrals are provided and documented.
33
Objectives of individual and group counseling
1. To assist clients in recognizing and eliminating high risk behavior associated with alcohol and drug use i.e. drinking and driving.
2. To provide clients with assessment and referral services to address life management issues that impact healthy functioning and wellbeing.
3. To facilitate the reduction or elimination of alcohol or drug use as appropriate.
4. To stimulate positive behavioral change resulting in increased well-being and functioning in major life areas.
Problem recognition
Taking responsibility
Self-regulation
Harm reduction
The DUI Client
34

35
A Preventable Tragedy
36
The California DUI client is as unique and diverse as the State’s population
The California DUI client runs the full spectrum of cultural, ethnic, and educational background.
The DUI offenses occur with no respect to age or gender
California DUI clients are from every walk of life and income level, i.e., students, blue collar workers, white collar workers, agricultural businesses , small business, manufacturing, unemployed, health care professionals, retirees and politicians
The DUI clients participating in our program mirror the communities we live in
WHO IS THE “TYPICAL" DUI CLIENT?
37
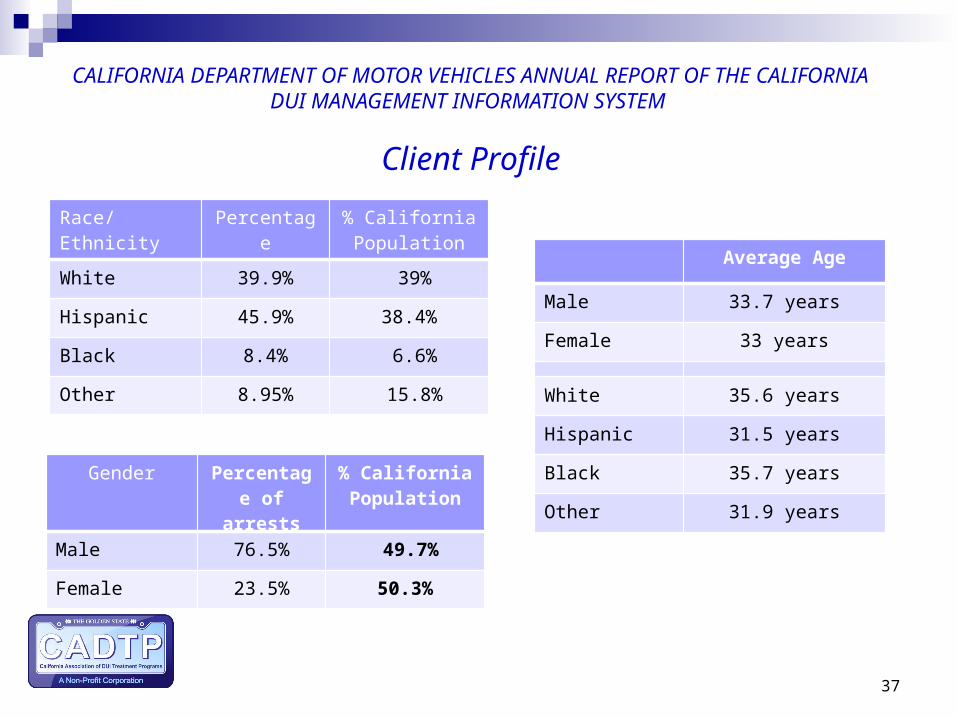
Race/Ethnicity
Percentage % California Population
White 39.9% 39%
Hispanic 45.9% 38.4%
Black 8.4% 6.6%
Other 8.95% 15.8%
CALIFORNIA DEPARTMENT OF MOTOR VEHICLES ANNUAL REPORT OF THE CALIFORNIA DUI MANAGEMENT INFORMATION SYSTEM
Client Profile
Gender Percentage of arrests
% California Population
Male 76.5% 49.7%
Female 23.5% 50.3%
Average Age
Male 33.7 years
Female 33 years
White 35.6 years
Hispanic 31.5 years
Black 35.7 years
Other 31.9 years
38
Myth vs. Fact
Myth:
All DUI Clients are Alcoholics or Addicts
Fact:
What we know as providers of DUI services is that our clientele run the full spectrum regarding use/abuse of alcohol and drugs.
Some clients do not have a substance use disorder and others may require additional services to address addictive behaviors.
39
Myth vs. Fact
Myth:
DUI Providers have a Singular Mission to Provide DUI Services Only
Fact:
DUI Programs are mandated by Regulations to “Evaluate the client’s need for referral to ancillary services”
The referral to ancillary services are based upon the clients assessed needs. i.e. an appropriate level of AOD Treatment, medical issues, food bank, financial assistance, etc.
40
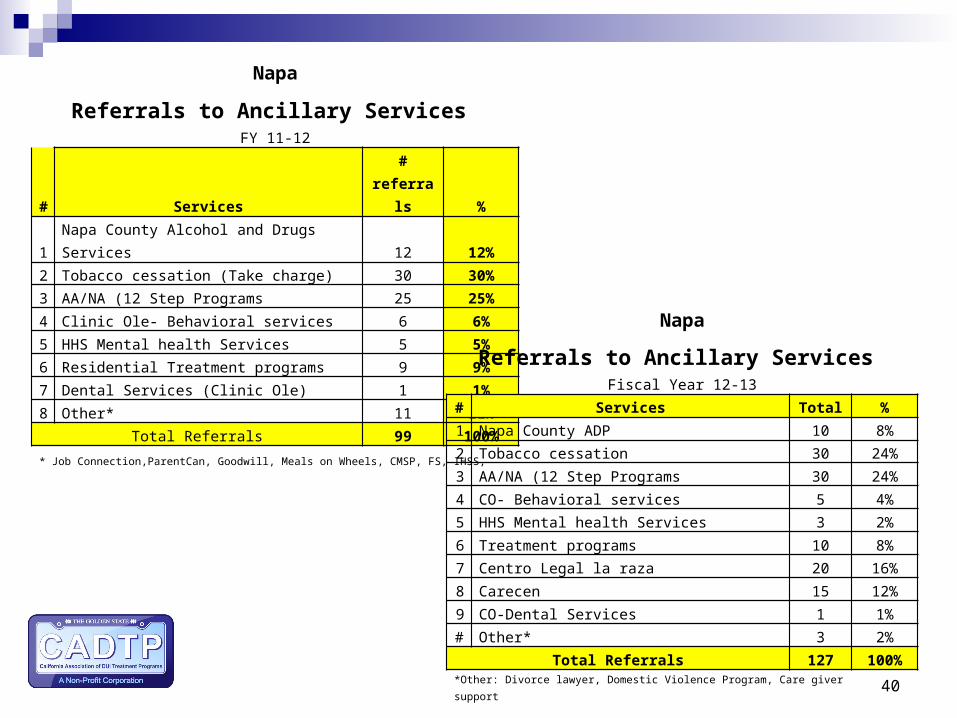
Napa
Referrals to Ancillary Services FY 11-12
# Services # referrals %
1 Napa County Alcohol and Drugs Services 12 12%
2 Tobacco cessation (Take charge) 30 30%
3 AA/NA (12 Step Programs 25 25%
4 Clinic Ole- Behavioral services 6 6%
5 HHS Mental health Services 5 5%
6 Residential Treatment programs 9 9%
7 Dental Services (Clinic Ole) 1 1%
8 Other* 11 11%Total Referrals 99 100%
* Job Connection,ParentCan, Goodwill, Meals on Wheels, CMSP, FS, IHSS,
Napa
Referrals to Ancillary Services Fiscal Year 12-13
# Services Total %
1 Napa County ADP 10 8%
2 Tobacco cessation 30 24%
3 AA/NA (12 Step Programs 30 24%
4 CO- Behavioral services 5 4%
5 HHS Mental health Services 3 2%
6 Treatment programs 10 8%
7 Centro Legal la raza 20 16%
8 Carecen 15 12%
9 CO-Dental Services 1 1%
# Other* 3 2%
Total Referrals 127 100%
*Other: Divorce lawyer, Domestic Violence Program, Care giver support
41
DUI Programs are: Prevention, Assessment , Early Intervention, and
Treatment
Approximately 150,000 court ordered DUI participants per year are provided support for positive changes in life style to facilitate reduction or elimination of alcohol/drug problems by the DUI Program Providers. This is accomplished through the AOD education, group and individual counseling session , the assessment of their substance use/abuse and the evaluation of the participant’s need for referral to ancillary services.
CADTP is in process of evaluating the types of assessments currently being used in the DUI programs and initial findings are that DUI programs are using different proven assessments used in the AOD treatment field.
How Clients Fit into DHCS’S Continuum of Care
Summary of DUI Services
Alcohol and drug outpatient treatment and education services
1st stage treatment program – primary gate keeper Prevention specialists, education, assessment Intervention Continuum of care Totally self-funded Effective at reducing recidivism Protect public safety
42
43
DUI Offender
The Wheel of Collaboration
44

45
A Successful Client
= A Safer Community

















