1 Thrombocytopenia with Thrombocytopenia with GP IIb/IIIa Inhibitors GP IIb/IIIa Inhibitors Robert P. Giugliano, MD, Robert P. Giugliano, MD, SM SM TIMI Study Chairman’s TIMI Study Chairman’s Office Office Cardiovascular Division Cardiovascular Division Brigham and Women’s Brigham and Women’s Hospital Hospital Harvard Medical School Harvard Medical School
• Hypersensitivity to drug, foodstuffs, chemicals, Hypersensitivity to drug, foodstuffs, chemicals, vaccines, and insect bites known to cause vaccines, and insect bites known to cause thrombocytopenia since early 1900’sthrombocytopenia since early 1900’s
• Drug-induced thrombocytopenia:Drug-induced thrombocytopenia:– Quinine purpura first reported in 1928Quinine purpura first reported in 1928– Sedermoid purpura, first detailed study (1949-55) by Sedermoid purpura, first detailed study (1949-55) by
Ackroyd -> Agglutination of normal human platelets Ackroyd -> Agglutination of normal human platelets with serum of pts with plts due to sedermoidwith serum of pts with plts due to sedermoid
• Hypersensitivity to drug, foodstuffs, chemicals, Hypersensitivity to drug, foodstuffs, chemicals, vaccines, and insect bites known to cause vaccines, and insect bites known to cause thrombocytopenia since early 1900’sthrombocytopenia since early 1900’s
• Drug-induced thrombocytopenia:Drug-induced thrombocytopenia:– Quinine purpura first reported in 1928Quinine purpura first reported in 1928– Sedermoid purpura, first detailed study (1949-55) by Sedermoid purpura, first detailed study (1949-55) by
Ackroyd -> Agglutination of normal human platelets Ackroyd -> Agglutination of normal human platelets with serum of pts with plts due to sedermoidwith serum of pts with plts due to sedermoid
3
Diagnosis of Drug-Induced Diagnosis of Drug-Induced ThrombocytopeniaThrombocytopenia
Diagnosis of Drug-Induced Diagnosis of Drug-Induced ThrombocytopeniaThrombocytopenia
1. Onset temporally related to drug initiation1. Onset temporally related to drug initiation
2. No alternative explanation2. No alternative explanation
3. Platelet count returns to normal once drug is 3. Platelet count returns to normal once drug is discontinueddiscontinued
4. Confirmation of diagnosis by either:4. Confirmation of diagnosis by either:» in vitroin vitro testing testing» rechallengerechallenge
1. Onset temporally related to drug initiation1. Onset temporally related to drug initiation
2. No alternative explanation2. No alternative explanation
3. Platelet count returns to normal once drug is 3. Platelet count returns to normal once drug is discontinueddiscontinued
4. Confirmation of diagnosis by either:4. Confirmation of diagnosis by either:» in vitroin vitro testing testing» rechallengerechallenge
4
Diagnosis is More Challenging TodayDiagnosis is More Challenging TodayDiagnosis is More Challenging TodayDiagnosis is More Challenging Today
1. “Modified indirect antiglobulin test”1. “Modified indirect antiglobulin test”Drug + pt serum (plasma) + nl donor pltsDrug + pt serum (plasma) + nl donor pltsLook for deposition of Ig’s or Look for deposition of Ig’s or complement on normal donor plts complement on normal donor plts
2. Platelet functional tests - altered results2. Platelet functional tests - altered results- plt activation- plt activation- release of dense granule contents- release of dense granule contents- release of cytoplasmic contents- release of cytoplasmic contents- stimulation of plt procoagulant activity- stimulation of plt procoagulant activity
1. “Modified indirect antiglobulin test”1. “Modified indirect antiglobulin test”Drug + pt serum (plasma) + nl donor pltsDrug + pt serum (plasma) + nl donor pltsLook for deposition of Ig’s or Look for deposition of Ig’s or complement on normal donor plts complement on normal donor plts
2. Platelet functional tests - altered results2. Platelet functional tests - altered results- plt activation- plt activation- release of dense granule contents- release of dense granule contents- release of cytoplasmic contents- release of cytoplasmic contents- stimulation of plt procoagulant activity- stimulation of plt procoagulant activity
6
Drug-dependent Ab: Drug-dependent Ab: Five Potential MechanismsFive Potential Mechanisms
Drug-dependent Ab: Drug-dependent Ab: Five Potential MechanismsFive Potential Mechanisms
(1) Ab binds to drug in plasma to (1) Ab binds to drug in plasma to form circulating immune-complexes.form circulating immune-complexes.Change in IgG conformation then Change in IgG conformation then recognized by platelet Fc receptorrecognized by platelet Fc receptor
(1) Ab binds to drug in plasma to (1) Ab binds to drug in plasma to form circulating immune-complexes.form circulating immune-complexes.Change in IgG conformation then Change in IgG conformation then recognized by platelet Fc receptorrecognized by platelet Fc receptor
(2) Ab binds directly to drug which(2) Ab binds directly to drug whichis concentrated on plt surface (relativeis concentrated on plt surface (relativeto drug concentration in the plasma)to drug concentration in the plasma)
(2) Ab binds directly to drug which(2) Ab binds directly to drug whichis concentrated on plt surface (relativeis concentrated on plt surface (relativeto drug concentration in the plasma)to drug concentration in the plasma)
yyyy
yyyy
YYYY
YYYY
yyyy
yyyy
yyyy
yyyy
Adapted from McCrae KR and Cines DB, Ch 29, Adapted from McCrae KR and Cines DB, Ch 29, Thrombosis and HemorrhageThrombosis and HemorrhageAdapted from McCrae KR and Cines DB, Ch 29, Adapted from McCrae KR and Cines DB, Ch 29, Thrombosis and HemorrhageThrombosis and Hemorrhage
7
Drug-dependent Ab: Drug-dependent Ab: Five Potential MechanismsFive Potential Mechanisms
Drug-dependent Ab: Drug-dependent Ab: Five Potential MechanismsFive Potential Mechanisms
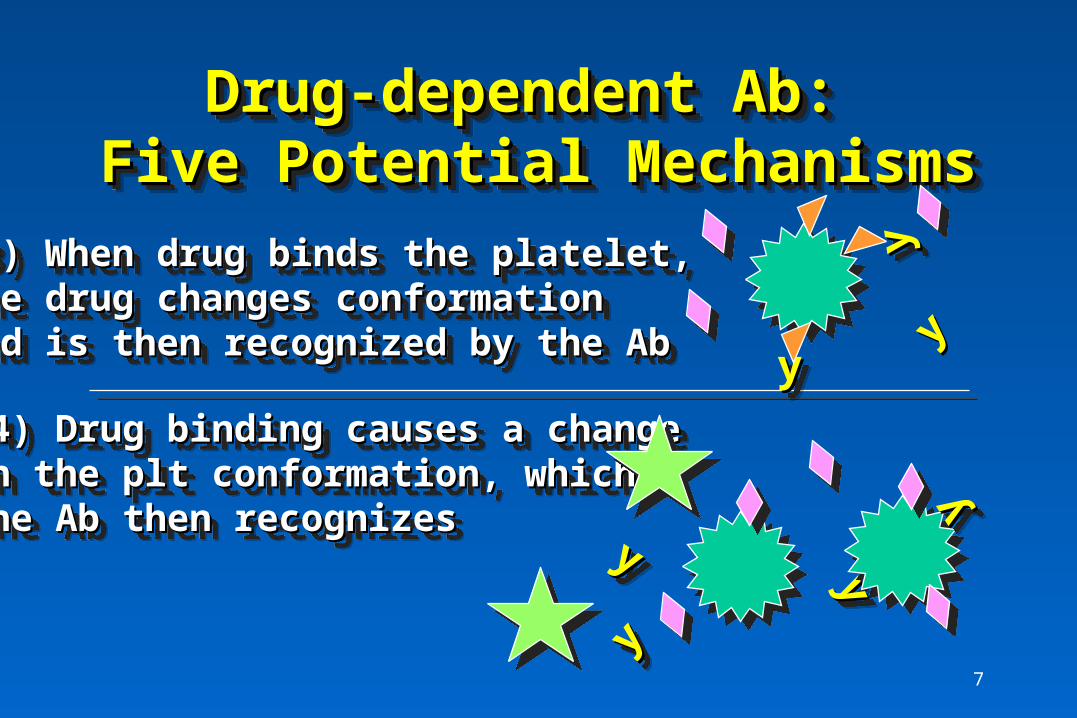
(3) When drug binds the platelet,(3) When drug binds the platelet,the drug changes conformation the drug changes conformation and is then recognized by the Aband is then recognized by the Ab
(3) When drug binds the platelet,(3) When drug binds the platelet,the drug changes conformation the drug changes conformation and is then recognized by the Aband is then recognized by the Ab
(4) Drug binding causes a change(4) Drug binding causes a changein the plt conformation, which in the plt conformation, which the Ab then recognizesthe Ab then recognizes
(4) Drug binding causes a change(4) Drug binding causes a changein the plt conformation, which in the plt conformation, which the Ab then recognizesthe Ab then recognizes
yyyy
yyyy
yyyy
yyyy
yyyy
yyyy
yy
8
Drug-dependent Ab: Drug-dependent Ab: Five Potential MechanismsFive Potential Mechanisms
Drug-dependent Ab: Drug-dependent Ab: Five Potential MechanismsFive Potential Mechanisms
(5) The Ab recognizes one or more neoepitopes comprised (5) The Ab recognizes one or more neoepitopes comprised of of bothboth platelet-derived and drug-derived determinants platelet-derived and drug-derived determinants(5) The Ab recognizes one or more neoepitopes comprised (5) The Ab recognizes one or more neoepitopes comprised of of bothboth platelet-derived and drug-derived determinants platelet-derived and drug-derived determinants
YYYY
YYYY
YYYY
9
Other Drugs: Other Drugs: What Have We LearnedWhat Have We Learned
Other Drugs: Other Drugs: What Have We LearnedWhat Have We Learned
• Plt counts for any one drug may (?often) have Plt counts for any one drug may (?often) have multiple mechanisms (e.g. EtOH)multiple mechanisms (e.g. EtOH)
• Contribution of suppressed plt production may Contribution of suppressed plt production may be underestimatedbe underestimated– Megakaryocytes in marrow = normal plt productionMegakaryocytes in marrow = normal plt production– Difficult to study megakaryocytopoiesis Difficult to study megakaryocytopoiesis in vitroin vitro
• Drug-dependent anti-plt Ab in early stages or Drug-dependent anti-plt Ab in early stages or non-existent for most drug (?sens, ?? specificity)non-existent for most drug (?sens, ?? specificity)
• Plt counts for any one drug may (?often) have Plt counts for any one drug may (?often) have multiple mechanisms (e.g. EtOH)multiple mechanisms (e.g. EtOH)
• Contribution of suppressed plt production may Contribution of suppressed plt production may be underestimatedbe underestimated– Megakaryocytes in marrow = normal plt productionMegakaryocytes in marrow = normal plt production– Difficult to study megakaryocytopoiesis Difficult to study megakaryocytopoiesis in vitroin vitro
• Drug-dependent anti-plt Ab in early stages or Drug-dependent anti-plt Ab in early stages or non-existent for most drug (?sens, ?? specificity)non-existent for most drug (?sens, ?? specificity)
GP IIb/IIIa associated plts shares features with the GP IIb/IIIa associated plts shares features with the historical description for thiazides:historical description for thiazides:– cardiac patients appear at higher riskcardiac patients appear at higher risk– incidence may be 1-2%, but little prospective dataincidence may be 1-2%, but little prospective data– generally mild-mod (30-100K), occasionally severegenerally mild-mod (30-100K), occasionally severe– smear shows only reduced # pltssmear shows only reduced # plts– counts recover in 5-14 dayscounts recover in 5-14 days– mechanism(s): likely multiple, immune-destruction mechanism(s): likely multiple, immune-destruction
most frequent most frequent
GP IIb/IIIa associated plts shares features with the GP IIb/IIIa associated plts shares features with the historical description for thiazides:historical description for thiazides:– cardiac patients appear at higher riskcardiac patients appear at higher risk– incidence may be 1-2%, but little prospective dataincidence may be 1-2%, but little prospective data– generally mild-mod (30-100K), occasionally severegenerally mild-mod (30-100K), occasionally severe– smear shows only reduced # pltssmear shows only reduced # plts– counts recover in 5-14 dayscounts recover in 5-14 days– mechanism(s): likely multiple, immune-destruction mechanism(s): likely multiple, immune-destruction
• Incidence estimated at 1/1000 [though probably higher Incidence estimated at 1/1000 [though probably higher in cardiac pts]in cardiac pts]
• Drug-dependent Abs bind to epitopes within either the Drug-dependent Abs bind to epitopes within either the GP Ib/IX or GP IIb/IIIa complexesGP Ib/IX or GP IIb/IIIa complexes
• Bernard-Soulier Syndrome (GP Ib complex proteins Bernard-Soulier Syndrome (GP Ib complex proteins deficient) may have “no” receptor for quinidine/quinine deficient) may have “no” receptor for quinidine/quinine induced Ab (controversial)induced Ab (controversial)
• Hypothesis: Drug induces changes in plt GP that are Hypothesis: Drug induces changes in plt GP that are then recognized by Ab (mechanism 4 or 5)then recognized by Ab (mechanism 4 or 5)
• Incidence estimated at 1/1000 [though probably higher Incidence estimated at 1/1000 [though probably higher in cardiac pts]in cardiac pts]
• Drug-dependent Abs bind to epitopes within either the Drug-dependent Abs bind to epitopes within either the GP Ib/IX or GP IIb/IIIa complexesGP Ib/IX or GP IIb/IIIa complexes
• Bernard-Soulier Syndrome (GP Ib complex proteins Bernard-Soulier Syndrome (GP Ib complex proteins deficient) may have “no” receptor for quinidine/quinine deficient) may have “no” receptor for quinidine/quinine induced Ab (controversial)induced Ab (controversial)
• Hypothesis: Drug induces changes in plt GP that are Hypothesis: Drug induces changes in plt GP that are then recognized by Ab (mechanism 4 or 5)then recognized by Ab (mechanism 4 or 5)
• Typically occurs 1-2 wks after initiationTypically occurs 1-2 wks after initiation
• Severe cases not uncommonSevere cases not uncommon
• Ab have been found against metabolite as well Ab have been found against metabolite as well as drug (both components for TMP-SX)as drug (both components for TMP-SX)
• Some donor plts serve as targets, other do Some donor plts serve as targets, other do not, ? Polymorphic determinants (?? Plnot, ? Polymorphic determinants (?? PlA2A2))
• Typically occurs 1-2 wks after initiationTypically occurs 1-2 wks after initiation
• Severe cases not uncommonSevere cases not uncommon
• Ab have been found against metabolite as well Ab have been found against metabolite as well as drug (both components for TMP-SX)as drug (both components for TMP-SX)
• Some donor plts serve as targets, other do Some donor plts serve as targets, other do not, ? Polymorphic determinants (?? Plnot, ? Polymorphic determinants (?? PlA2A2))
• Plt counts usually Plt counts usually << 2 wks, as late as 4 mths 2 wks, as late as 4 mths
• Spectrum of plt counts seen (severe - mild)Spectrum of plt counts seen (severe - mild)
• Mechanism(s) unclear, ? dose relatedMechanism(s) unclear, ? dose related
• Plt counts may return to normal despite Plt counts may return to normal despite continued therapy => implications for continued therapy => implications for mechanism(s)mechanism(s)
• Plt counts usually Plt counts usually << 2 wks, as late as 4 mths 2 wks, as late as 4 mths
• Spectrum of plt counts seen (severe - mild)Spectrum of plt counts seen (severe - mild)
• Mechanism(s) unclear, ? dose relatedMechanism(s) unclear, ? dose related
• Plt counts may return to normal despite Plt counts may return to normal despite continued therapy => implications for continued therapy => implications for mechanism(s)mechanism(s)
14
HeparinHeparinHeparinHeparin• At least two mechanisms (?spectrum of disease)At least two mechanisms (?spectrum of disease)
• Incidence varies (0-30%) among series: Incidence varies (0-30%) among series: – bovine vs porcine, LMWH, heparinoidsbovine vs porcine, LMWH, heparinoids– dose may be importantdose may be important– clinical factors (cardiac disease, surgery)clinical factors (cardiac disease, surgery)– method of diagnosismethod of diagnosis
• Ubiquitous use in hospital, esp cardiology may Ubiquitous use in hospital, esp cardiology may confound analysis of other drugsconfound analysis of other drugs
• At least two mechanisms (?spectrum of disease)At least two mechanisms (?spectrum of disease)
• Incidence varies (0-30%) among series: Incidence varies (0-30%) among series: – bovine vs porcine, LMWH, heparinoidsbovine vs porcine, LMWH, heparinoids– dose may be importantdose may be important– clinical factors (cardiac disease, surgery)clinical factors (cardiac disease, surgery)– method of diagnosismethod of diagnosis
• Ubiquitous use in hospital, esp cardiology may Ubiquitous use in hospital, esp cardiology may confound analysis of other drugsconfound analysis of other drugs
15
Mechanism of HITMechanism of HITMechanism of HITMechanism of HIT
• Type 1: mild, early onset, may resolve despite Type 1: mild, early onset, may resolve despite continued heparin, no thrombosis.continued heparin, no thrombosis.– plt agglutination due to (-) charge of heparinplt agglutination due to (-) charge of heparin
• Type 2: mild-severe (subtypes?), onset 7-14 d, may Type 2: mild-severe (subtypes?), onset 7-14 d, may be associated with fatal arterial/venous thrombosisbe associated with fatal arterial/venous thrombosis– Ab reacts with heparin and/or PF4 -> immune complex Ab reacts with heparin and/or PF4 -> immune complex
which then is recognized by Fc receptor on the pltwhich then is recognized by Fc receptor on the plt
• Type 1: mild, early onset, may resolve despite Type 1: mild, early onset, may resolve despite continued heparin, no thrombosis.continued heparin, no thrombosis.– plt agglutination due to (-) charge of heparinplt agglutination due to (-) charge of heparin
• Type 2: mild-severe (subtypes?), onset 7-14 d, may Type 2: mild-severe (subtypes?), onset 7-14 d, may be associated with fatal arterial/venous thrombosisbe associated with fatal arterial/venous thrombosis– Ab reacts with heparin and/or PF4 -> immune complex Ab reacts with heparin and/or PF4 -> immune complex
which then is recognized by Fc receptor on the pltwhich then is recognized by Fc receptor on the plt
YYYYUUUU UUUU YYYY
YYYY
16
Thrombocytopenia with GP Thrombocytopenia with GP IIb/IIIa inhibitors:IIb/IIIa inhibitors:
A Meta-analysisA Meta-analysis
Thrombocytopenia with GP Thrombocytopenia with GP IIb/IIIa inhibitors:IIb/IIIa inhibitors:
A Meta-analysisA Meta-analysis
Robert P. Giugliano, M.D., S.M.Raymond R. Hyatt, Jr., S.M.
Brigham and Women’s HospitalHarvard Medical School
Robert P. Giugliano, M.D., S.M.Raymond R. Hyatt, Jr., S.M.
Brigham and Women’s HospitalHarvard Medical School
17
BackgroundBackgroundBackgroundBackground
• Hemorrhage and thrombocytopenia ( plt) Hemorrhage and thrombocytopenia ( plt) are major safety concerns with GP IIb/IIIa are major safety concerns with GP IIb/IIIa
• Comprehensive review of plt lackingComprehensive review of plt lacking
• Hemorrhage and thrombocytopenia ( plt) Hemorrhage and thrombocytopenia ( plt) are major safety concerns with GP IIb/IIIa are major safety concerns with GP IIb/IIIa
• Comprehensive review of plt lackingComprehensive review of plt lacking
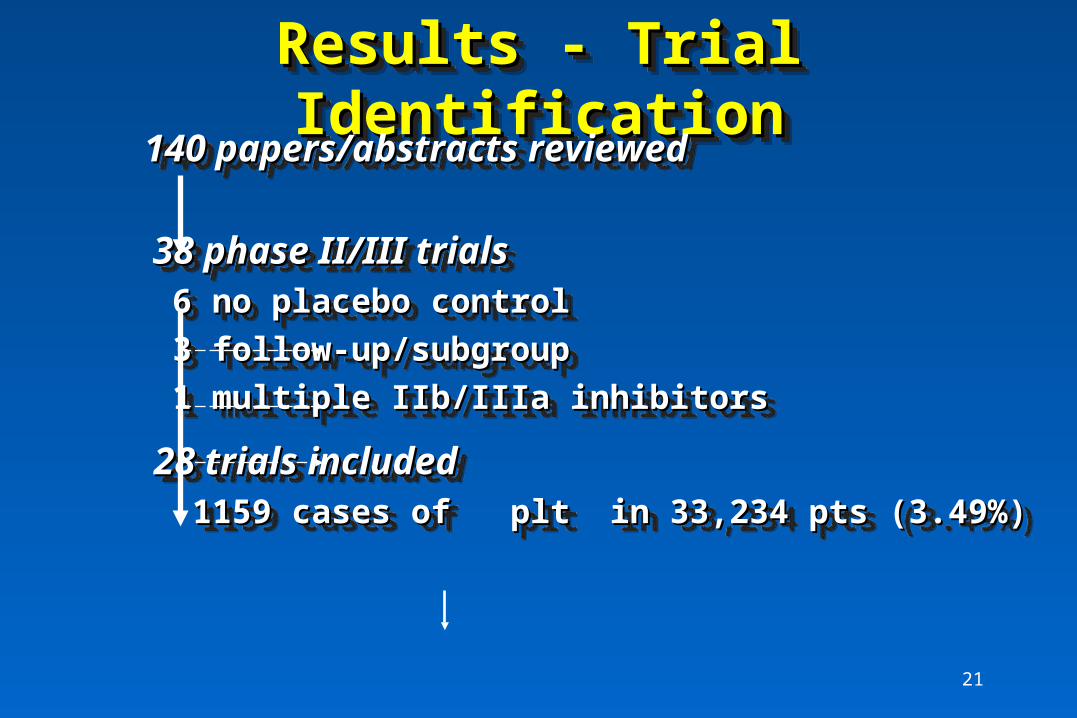
• Exclusion: No placebo control, Exclusion: No placebo control, >> 2 GP IIb/IIIa inhibitors, 2 GP IIb/IIIa inhibitors, secondary reportssecondary reports
• PARAGON treated as 2 separate trialsPARAGON treated as 2 separate trials
• Outcome measurement: Odds ratio of plt (defined as plt Outcome measurement: Odds ratio of plt (defined as plt ct < 100K [if available])ct < 100K [if available])
• Abstract and manuscripts thru AUG 1997 (Medline, Abstract and manuscripts thru AUG 1997 (Medline, ACC/AHA, references)ACC/AHA, references)
• Exclusion: No placebo control, Exclusion: No placebo control, >> 2 GP IIb/IIIa inhibitors, 2 GP IIb/IIIa inhibitors, secondary reportssecondary reports
• PARAGON treated as 2 separate trialsPARAGON treated as 2 separate trials
• Outcome measurement: Odds ratio of plt (defined as plt Outcome measurement: Odds ratio of plt (defined as plt ct < 100K [if available])ct < 100K [if available])
– By drug: 4 most widely studied agentsBy drug: 4 most widely studied agents– Heparin required vs. not requiredHeparin required vs. not required– Pt population: interventional, lytic, otherPt population: interventional, lytic, other– Trial design: dose-ranging vs. fixed dose (Trial design: dose-ranging vs. fixed dose (<<2)2)
• DerSimonian and Laird random effects model to DerSimonian and Laird random effects model to estimate combined OR (95%CI)estimate combined OR (95%CI)
• 1/6th added if zero cell1/6th added if zero cell• Sensitivity analyses: Fail-safe N, publication bias, Sensitivity analyses: Fail-safe N, publication bias,
excluding trialsexcluding trials
• Subgroup analyses: Subgroup analyses: – By drug: 4 most widely studied agentsBy drug: 4 most widely studied agents– Heparin required vs. not requiredHeparin required vs. not required– Pt population: interventional, lytic, otherPt population: interventional, lytic, other– Trial design: dose-ranging vs. fixed dose (Trial design: dose-ranging vs. fixed dose (<<2)2)
• DerSimonian and Laird random effects model to DerSimonian and Laird random effects model to estimate combined OR (95%CI)estimate combined OR (95%CI)
• 1/6th added if zero cell1/6th added if zero cell• Sensitivity analyses: Fail-safe N, publication bias, Sensitivity analyses: Fail-safe N, publication bias,
Sensitivity AnalysesSensitivity AnalysesSensitivity AnalysesSensitivity Analyses• Over >100,000 pts per arm, 0% plt with IIb/IIIa Over >100,000 pts per arm, 0% plt with IIb/IIIa
inhibitor => negate overall result inhibitor => negate overall result • Fail-safe N: 3 trials of 10,000 pts, 0% plt with IIb/IIIa Fail-safe N: 3 trials of 10,000 pts, 0% plt with IIb/IIIa
• Add 1/2 to zero cellsAdd 1/2 to zero cells 1.40 (1.09, 1.80) 1.40 (1.09, 1.80)
• Over >100,000 pts per arm, 0% plt with IIb/IIIa Over >100,000 pts per arm, 0% plt with IIb/IIIa inhibitor => negate overall result inhibitor => negate overall result
• Fail-safe N: 3 trials of 10,000 pts, 0% plt with IIb/IIIa Fail-safe N: 3 trials of 10,000 pts, 0% plt with IIb/IIIa inhibitorinhibitor
• Add 1/2 to zero cellsAdd 1/2 to zero cells 1.40 (1.09, 1.80) 1.40 (1.09, 1.80)
30
ConclusionsConclusionsConclusionsConclusions
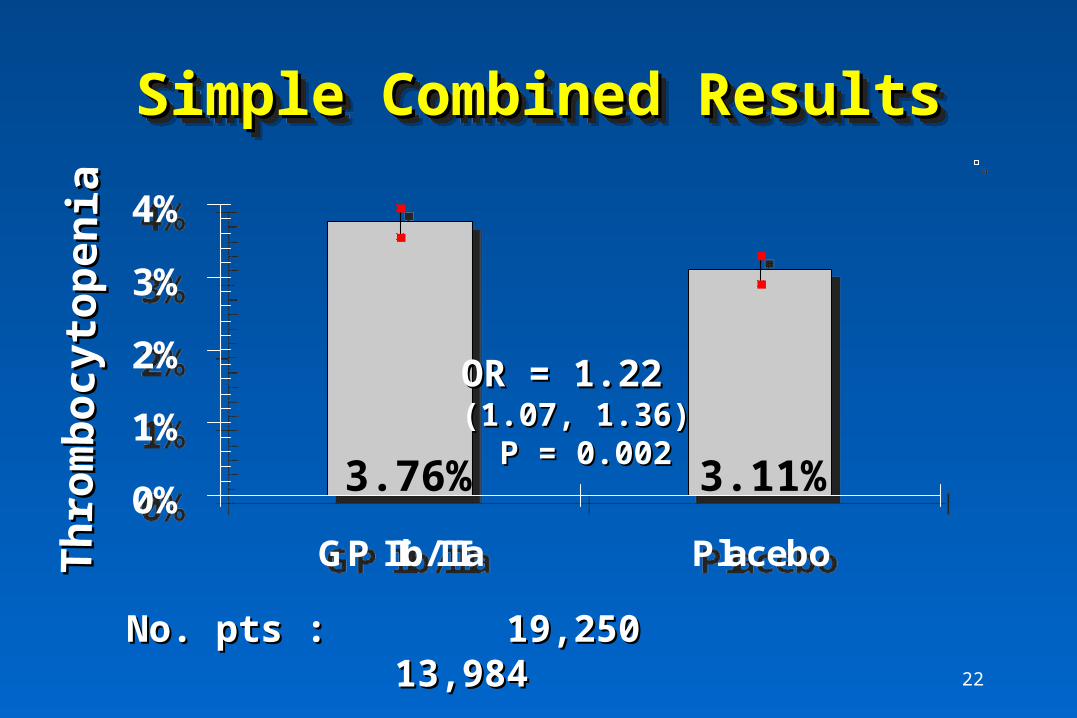
• GP IIb/IIIa inhibitors associated with an approx 50% in plt GP IIb/IIIa inhibitors associated with an approx 50% in plt compared to placebo (or an extra 1-2 cases per 100 pts treated compared to placebo (or an extra 1-2 cases per 100 pts treated with GP inhibitor)with GP inhibitor)
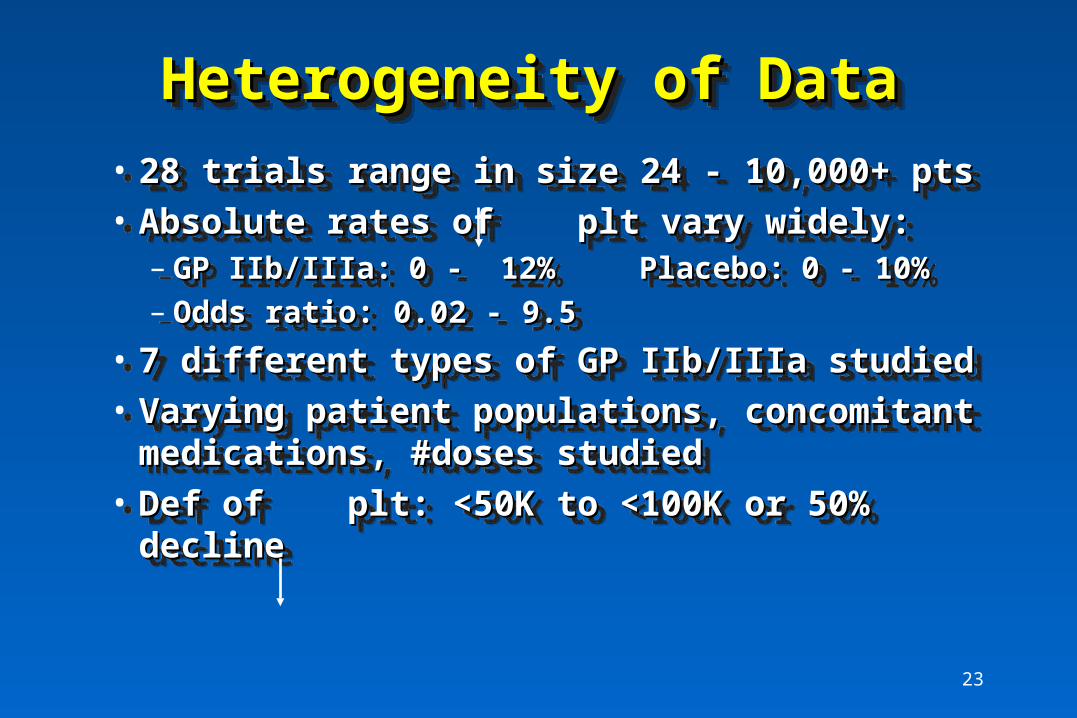
• Heterogeneity marked esp. in small trialsHeterogeneity marked esp. in small trials
• Odds of plt similar in 4 most widely studied drugsOdds of plt similar in 4 most widely studied drugs
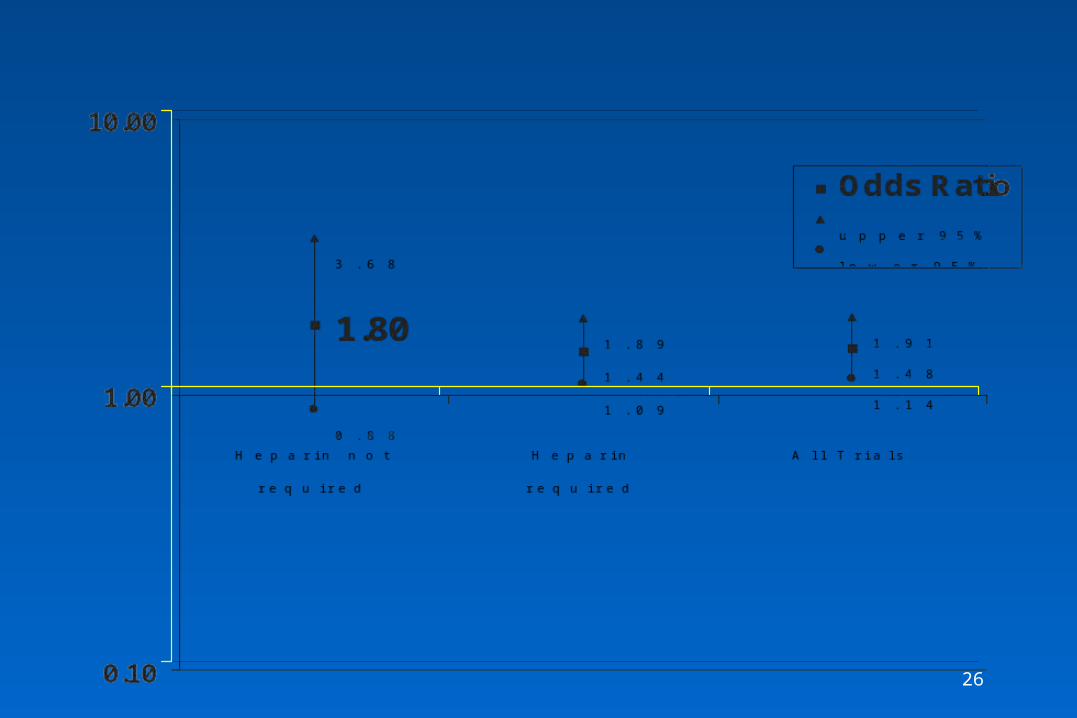
• No strong evidence for confounding by heparin, patient No strong evidence for confounding by heparin, patient population, or trial design population, or trial design
• Sensitivity analyses => main finding is robustSensitivity analyses => main finding is robust
• GP IIb/IIIa inhibitors associated with an approx 50% in plt GP IIb/IIIa inhibitors associated with an approx 50% in plt compared to placebo (or an extra 1-2 cases per 100 pts treated compared to placebo (or an extra 1-2 cases per 100 pts treated with GP inhibitor)with GP inhibitor)
• Heterogeneity marked esp. in small trialsHeterogeneity marked esp. in small trials
• Odds of plt similar in 4 most widely studied drugsOdds of plt similar in 4 most widely studied drugs
• No strong evidence for confounding by heparin, patient No strong evidence for confounding by heparin, patient population, or trial design population, or trial design
• Sensitivity analyses => main finding is robustSensitivity analyses => main finding is robust
• 23 trials with data on platelet counts < 50K23 trials with data on platelet counts < 50K
• 11 trials had no cases in either treatment group11 trials had no cases in either treatment group
• Only 7 trials had cases in both treatment groupsOnly 7 trials had cases in both treatment groups
• GP IIb/IIIa: GP IIb/IIIa: 101 cases in 17330 pts (0.58%)101 cases in 17330 pts (0.58%)
• Placebo:Placebo: 40 cases in 12280 pts (0.33%) 40 cases in 12280 pts (0.33%)
• OR (metanalysis): 1.30 (0.84, 2.03)OR (metanalysis): 1.30 (0.84, 2.03)
• 23 trials with data on platelet counts < 50K23 trials with data on platelet counts < 50K
• 11 trials had no cases in either treatment group11 trials had no cases in either treatment group
• Only 7 trials had cases in both treatment groupsOnly 7 trials had cases in both treatment groups
• GP IIb/IIIa: GP IIb/IIIa: 101 cases in 17330 pts (0.58%)101 cases in 17330 pts (0.58%)
• Placebo:Placebo: 40 cases in 12280 pts (0.33%) 40 cases in 12280 pts (0.33%)
• OR (metanalysis): 1.30 (0.84, 2.03)OR (metanalysis): 1.30 (0.84, 2.03)
32
2.01 2.21
1.12 1.151.48 1.30
4.033.25 3.57
0.59
1.69
0.63
1.91 2.03
0.89
0.62
8.36
0.75
2.08
1.14
0.84
1.891.43
0.1
1
10Odds Ratioupper 95%lower 95%
2.01 2.21
1.12 1.151.48 1.30
4.033.25 3.57
0.59
1.69
0.63
1.91 2.03
0.89
0.62
8.36
0.75
2.08
1.14
0.84
1.891.43
0.1
1
10Odds Ratioupper 95%lower 95%
OR
wit
h 9
5% C
IO
R w
ith
95%
CI
OR
wit
h 9
5% C
IO
R w
ith
95%
CI
100,000 vs. 50,000 Threshold 100,000 vs. 50,000 Threshold (preliminary)(preliminary)100,000 vs. 50,000 Threshold 100,000 vs. 50,000 Threshold (preliminary)(preliminary)
Required Heparin - 100K vs 50KRequired Heparin - 100K vs 50K (preliminary)(preliminary) Required Heparin - 100K vs 50KRequired Heparin - 100K vs 50K (preliminary)(preliminary) 25
Heparin notHeparin not Heparin requiredHeparin required All Trials All Trials requiredrequiredHeparin notHeparin not Heparin requiredHeparin required All Trials All Trials requiredrequired
34
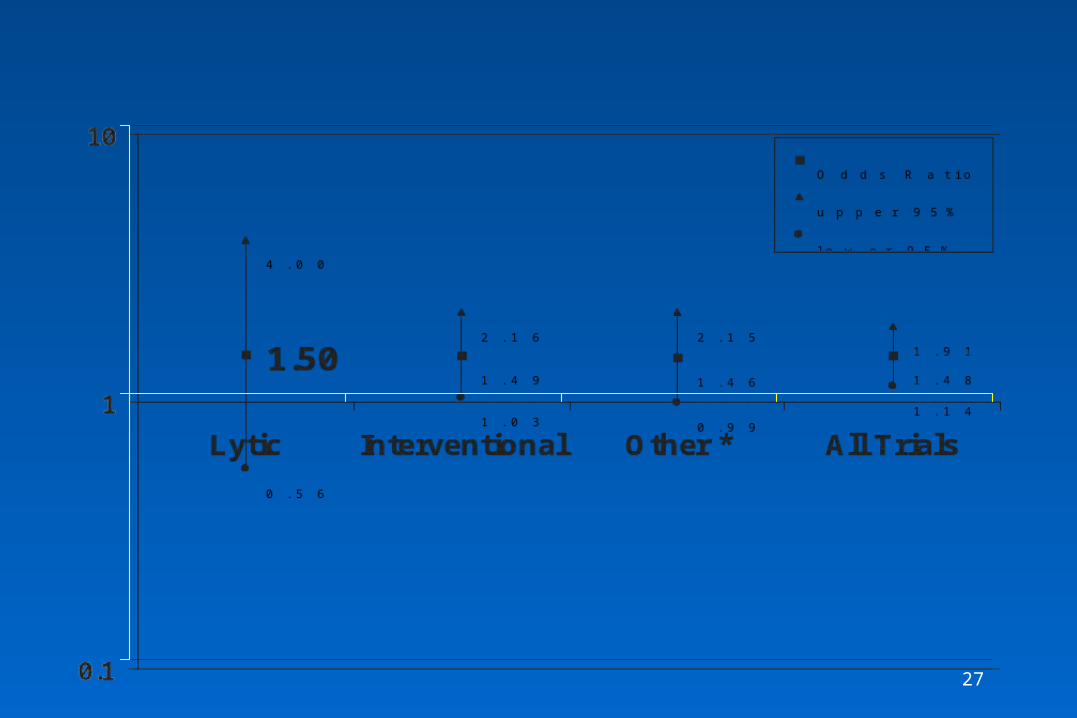
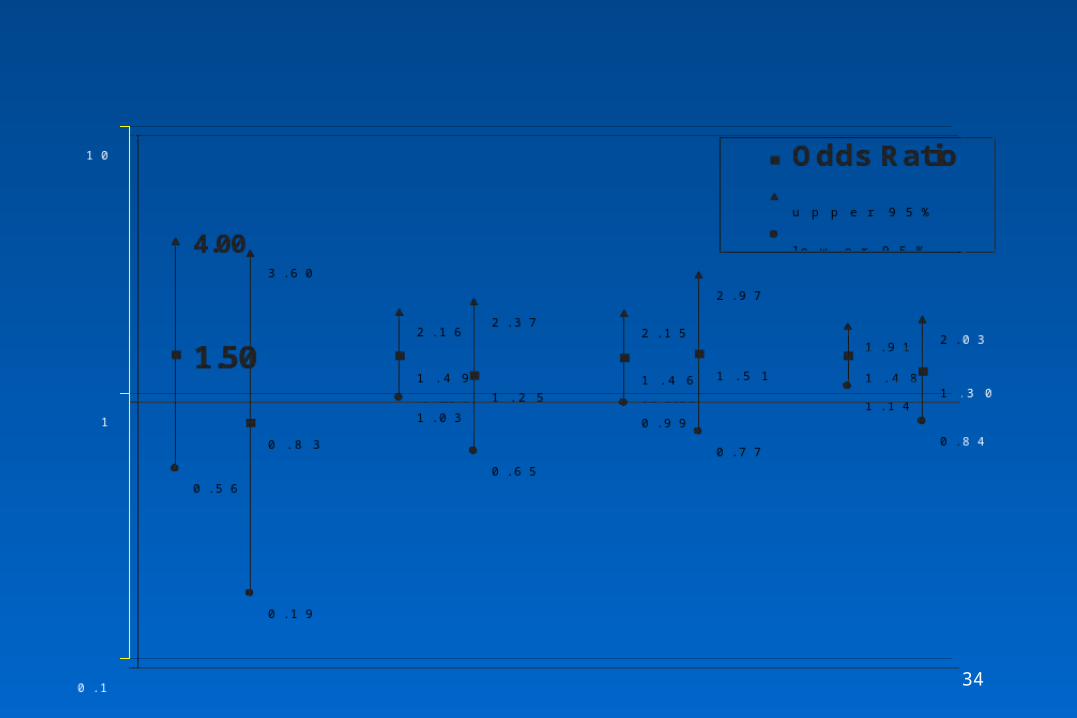
1.50
0.83
1.491.25
1.46 1.51 1.48 1.30
4.00 3.60
2.16 2.37 2.15
2.97
1.91 2.03
0.56
0.19
1.03
0.65
0.990.77
1.14
0.84
0.1
1
10Odds Ratioupper 95%lower 95%
1.50
0.83
1.491.25
1.46 1.51 1.48 1.30
4.00 3.60
2.16 2.37 2.15
2.97
1.91 2.03
0.56
0.19
1.03
0.65
0.990.77
1.14
0.84
0.1
1
10Odds Ratioupper 95%lower 95%
OR
wit
h 9
5% C
IO
R w
ith
95%
CI
OR
wit
h 9
5% C
IO
R w
ith
95%
CI
Patient Population - 100K vs 50KPatient Population - 100K vs 50KPatient Population - 100K vs 50KPatient Population - 100K vs 50K
Lytic trials Intervention Other* All trials
*Other includes acute and stable coronary syndromes
Lytic trials Intervention Other* All trials
*Other includes acute and stable coronary syndromes
35
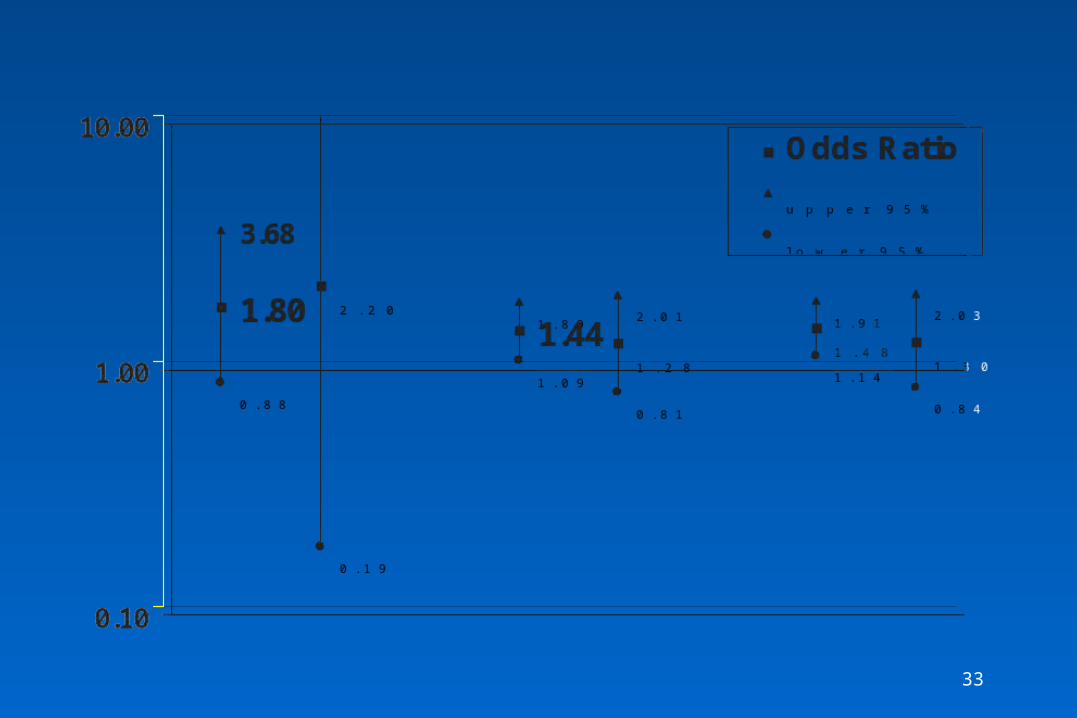
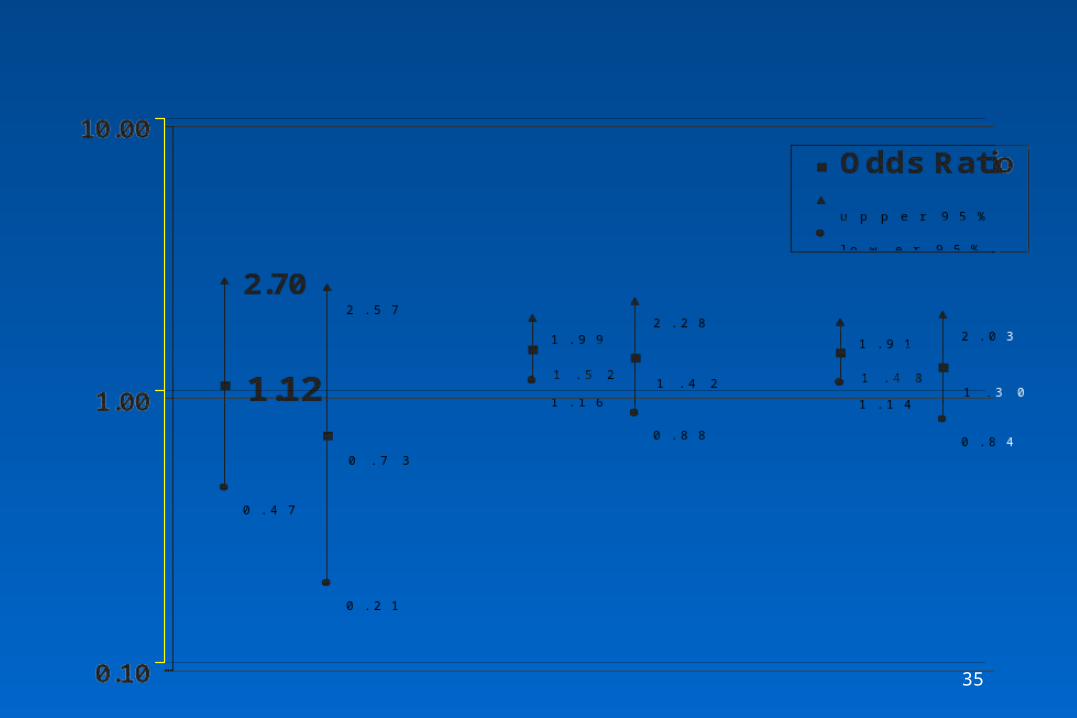
1.12
0.73
1.52 1.42 1.48 1.30
2.70 2.571.99
2.281.91 2.03
0.47
0.21
1.160.88
1.140.84
0.10
1.00
10.00
Odds Ratioupper 95%lower 95%
1.12
0.73
1.52 1.42 1.48 1.30
2.70 2.571.99
2.281.91 2.03
0.47
0.21
1.160.88
1.140.84
0.10
1.00
10.00
Odds Ratioupper 95%lower 95%
OR
wit
h 9
5% C
IO
R w
ith
95%
CI
OR
wit
h 9
5% C
IO
R w
ith
95%
CI
Effect of Trial DesignEffect of Trial DesignEffect of Trial DesignEffect of Trial Design
Dose ranging Fixed-dose All trialsDose ranging Fixed-dose All trialsDose ranging Fixed-dose All trialsDose ranging Fixed-dose All trials
36
Is Thrombocytopenia Dose-related?Is Thrombocytopenia Dose-related?(Preliminary Results)(Preliminary Results)
Is Thrombocytopenia Dose-related?Is Thrombocytopenia Dose-related?(Preliminary Results)(Preliminary Results)
• 14 trials with 14 trials with >> 2 doses of IIb/IIIa inhibitor that 2 doses of IIb/IIIa inhibitor that reported plt by dosereported plt by dose
• Highest dose compared to lowest doseHighest dose compared to lowest dose
• High dose: 389 cases in 7737 pts (5.0%)High dose: 389 cases in 7737 pts (5.0%)
• Low dose: 215 cases in 4511 pts (4.8%)Low dose: 215 cases in 4511 pts (4.8%)
• 3 largest trials: More cases in low dose group3 largest trials: More cases in low dose group
• Metanalytic OR [high:low] = 0.73 (0.51, 1.04)Metanalytic OR [high:low] = 0.73 (0.51, 1.04)
• High-degree of heterogeneity of trialsHigh-degree of heterogeneity of trials
• 14 trials with 14 trials with >> 2 doses of IIb/IIIa inhibitor that 2 doses of IIb/IIIa inhibitor that reported plt by dosereported plt by dose
• Highest dose compared to lowest doseHighest dose compared to lowest dose
• High dose: 389 cases in 7737 pts (5.0%)High dose: 389 cases in 7737 pts (5.0%)
• Low dose: 215 cases in 4511 pts (4.8%)Low dose: 215 cases in 4511 pts (4.8%)
• 3 largest trials: More cases in low dose group3 largest trials: More cases in low dose group
• Metanalytic OR [high:low] = 0.73 (0.51, 1.04)Metanalytic OR [high:low] = 0.73 (0.51, 1.04)
• High-degree of heterogeneity of trialsHigh-degree of heterogeneity of trials
37
ReoPro Readministration Registry (RReoPro Readministration Registry (R33))(Tcheng JE, JACC ‘98;31(Suppl A):55A)(Tcheng JE, JACC ‘98;31(Suppl A):55A)
ReoPro Readministration Registry (RReoPro Readministration Registry (R33))(Tcheng JE, JACC ‘98;31(Suppl A):55A)(Tcheng JE, JACC ‘98;31(Suppl A):55A)
• 27% developed human anti-chimeric 27% developed human anti-chimeric antibodies (HACA)antibodies (HACA)
• No anaphylaxis observedNo anaphylaxis observed
• Rate of thrombocytopenia is approx 3x in pts Rate of thrombocytopenia is approx 3x in pts that are HACA + (7.2% vs 2.3%, p =.06) that are HACA + (7.2% vs 2.3%, p =.06)
• 27% developed human anti-chimeric 27% developed human anti-chimeric antibodies (HACA)antibodies (HACA)
• No anaphylaxis observedNo anaphylaxis observed
• Rate of thrombocytopenia is approx 3x in pts Rate of thrombocytopenia is approx 3x in pts that are HACA + (7.2% vs 2.3%, p =.06) that are HACA + (7.2% vs 2.3%, p =.06)
38
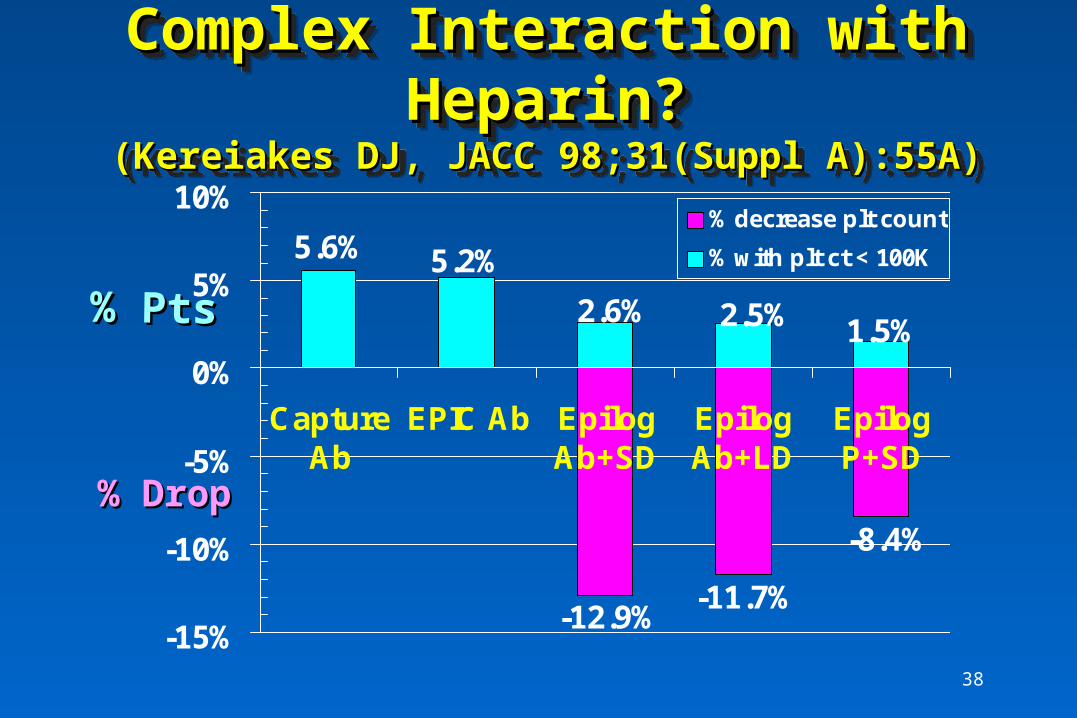
Complex Interaction with Complex Interaction with Heparin?Heparin?
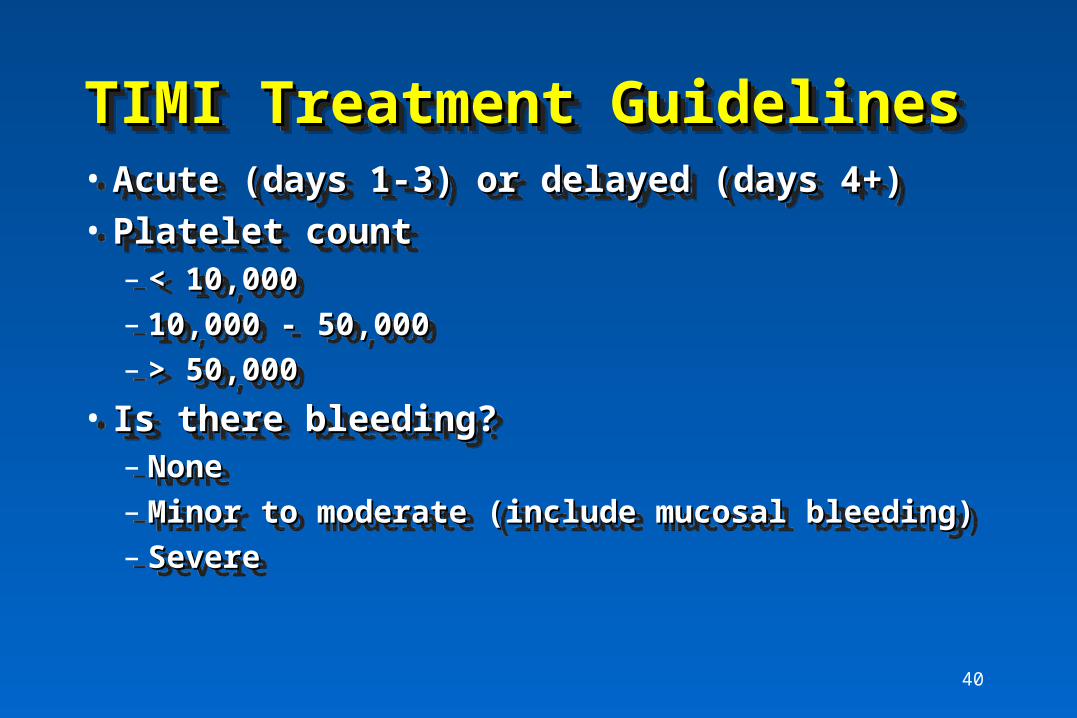
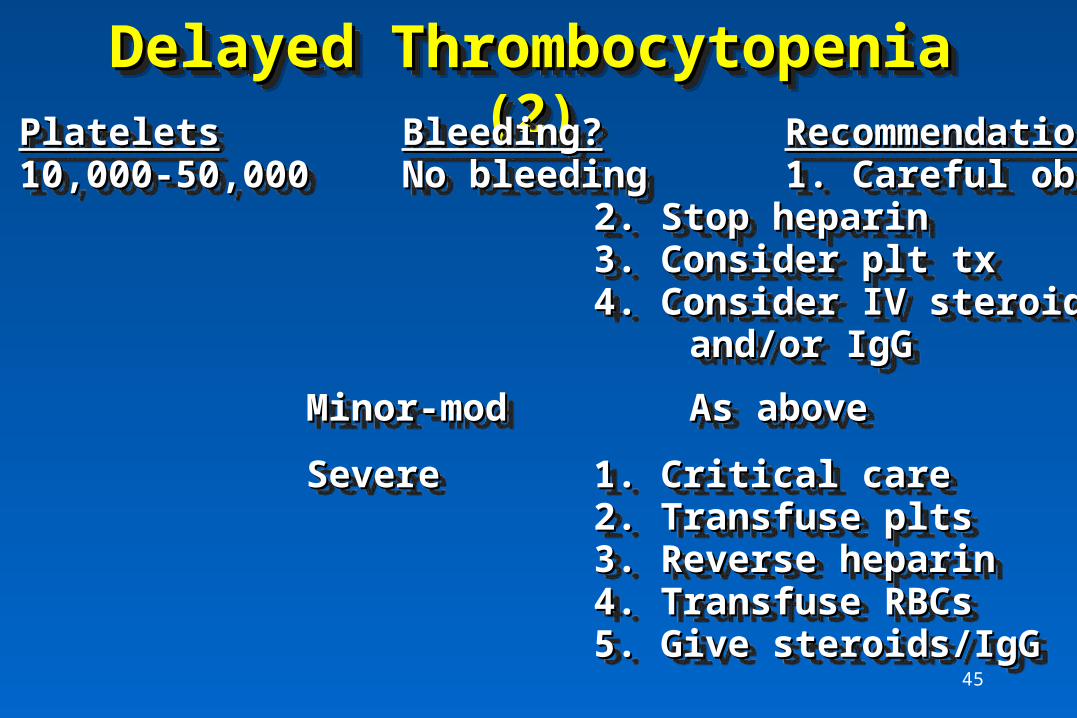
• Is there bleeding?Is there bleeding?– NoneNone– Minor to moderate (include mucosal bleeding)Minor to moderate (include mucosal bleeding)– SevereSevere
• Acute (days 1-3) or delayed (days 4+)Acute (days 1-3) or delayed (days 4+)
• Is there bleeding?Is there bleeding?– NoneNone– Minor to moderate (include mucosal bleeding)Minor to moderate (include mucosal bleeding)– SevereSevere
If no response to above measures, consider:If no response to above measures, consider:– emergent hemodialysisemergent hemodialysis– plasmapheresisplasmapheresis
(neither of proven benefit)(neither of proven benefit)
If no response to above measures, consider:If no response to above measures, consider:– emergent hemodialysisemergent hemodialysis– plasmapheresisplasmapheresis
(neither of proven benefit)(neither of proven benefit)