41
Understanding and Influencing Consumer Behavior Nutrition Education and Counseling
| Date post: | 25-Dec-2015 |
| Category: |
Documents |
| Upload: | evan-nichols |
| View: | 223 times |
| Download: | 1 times |

1
Understanding and Influencing Consumer Behavior
Nutrition Education and Counseling

2
Topics to be covered
Factors Affecting Food Consumption Theories of behavior change Client-centered counseling Family-centered counseling Transcultural counseling

3
Topics to be covered
Factors Affecting Food Consumption Theories of behavior change Client-centered counseling

4
Why Do People Eat What They Eat?
Discuss this in terms of Maslow’s Hierarchy of Needs--Figure 8-1, page 240 Boyle and Morris
Using Figure 8-2, page 241, provide examples of ways that each factor affects food consumption

5
Theories of Behavior Change
Health Belief Model Thery of Reasoned Action
» Theory of Trying Consumer Information Processing Stages of Change Diffusion of Innovations

6
Health Belief Model (Table 8-2, p. 247)
In order to change a behavior a person must believe he/she is:
Susceptible to illness Occurrence of condition will have a
serious impact on life

7
Health Belief Model (con’t)
Following a particular set of health recommendations will be beneficial
Barriers to following to recommendations can be overcome
Recommendations will have psychological benefits

8
What are examples of how one would use this model?

9
Theory of Reasoned Action
Intentions are the best predictor of behavior
10
Theory of Trying: A modification of Theory of Reasoned Action
See model in figure 8-3, page 249 Various factors influence the strenght of the
intention to try a new behavior» Attitudes toward success or failure
» Expectation of success or failure
» Attitude toward the process of changing
» Emotional response to the new behavior Past experiences with trying the new
behavior

11
How might you apply this theory?
What techniques would you use to counsel a person who says “Well, I’ll try to reduce my fat intake, but my family will only eat fried foods.”

12
Social Learning Theory
Central premise: Personal knowledge and beliefs, the beliefs of important others, and the physical and emotional environment influences what a person eats. A change in one of these factors has implications for the other factors.

13
Social Learning Theory (con’t)
See Table 8-3, p 251 for concepts A strength of SLT if that it focuses on
behavior, rather than knowledge and attitudes The concepts, with their definitions and
implications, provide ways of addressing the physical and social environment, mastery of skills, self-monitoring, rewards and incentives, and small steps for goal completion.

14
How Would You Apply This Theory?

15
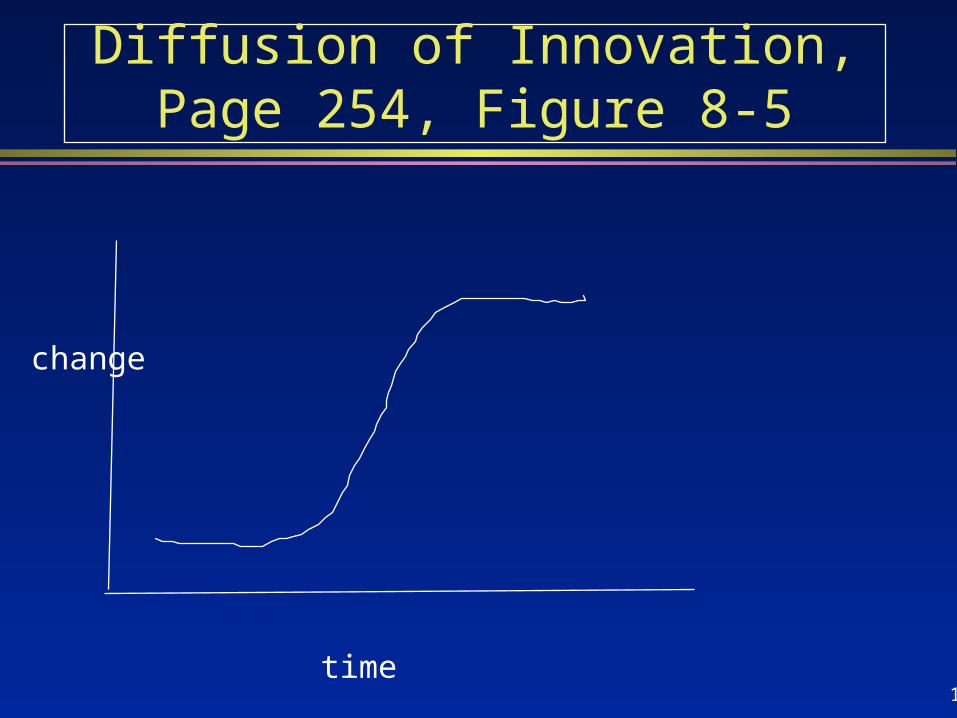
Diffusion of Innovation
Central premise:Most people do not change behavior easily or quickly. Some change earlier than others.
Very useful theory when planning an intervention addressing groups of people (macro level interventions).
16
Diffusion of Innovation, Page 254, Figure 8-5
time
change

17
Stages of Innovation
Knowledge--Individual is aware of innovation and has acquired some information about it
Persausion--Individual forms an attitude about the innovation--either in favor of or against it

18
Stages of Innovation (con’t)
Decision--Individual performs activities that lead to either adopting or rejecting the innovation
Confirmation--Individual looks for reinforcement for his decision and may change it if he is exposed to counter-reinforcing messages

19
Diffusion of Innovations
Innovations that are successful must meet certain criteria:
Compatible with existing value systems and lifestyles
Flexible Appear more advantageous than
previous practices

20
Diffusion of Innovations (con’t)
Criteria (con’t) Reversible Low risk Perceived as having greater benefits
than costs

21
Stages of Change
Central premise: Changes in eating patterns involve multiple steps and adaptation over time. These steps form a continuum. A person may or may not be ready to try to change at a given time. Education and counseling strategies must match stage person is at.

22
Stages of Change
Very useful in individual counseling situations (micro-interventions)
As you counsel individuals in your community rotation, determine at what stage the person is.
Your approach should reflect that stage.

23
Stages of Change
Stages: 1. Precomtemplation: unaware/not
interested 2. Comtemplation: thinking about
change 3. Determination or preparation:
becoming determined to change

24
Stages of Change (con’t)
4. Action: Actively modifying habits 5. Maintenance: Maintaining new,
healthier habits 6. Relapse: Returning to old behavior

25
How might you approach a person at each stage?
Precontemplation Comtemplation Determination Action Maintenance Relapse

26
Relapse Prevention
Central premise: Addictive behaviors are habit patterns that have been overlearned. These habits can be changed through self-management or self-control, particularly through developing ways to change expectations of oneself.

27
Skills one might develop to prevent relapse
Planning to order the low-fat entree at a restaurant
Planning what to eat at a party Not feeling guilty for eating a high-
calorie meal Taking a low calorie snack when
shopping

28
Client-Centered or Non-directive Counseling

29
Client-Centered Counseling
Client-centered counseling allows the client to take responsibility and to set goals that he/she can embrace.

30
Methods to Acheive Client-Centered Counseling
Establish rapport with client Involve client--allow him/her to ventilate
problems Demonstrate empathy toward client Beaware of nonverbal behaviors that
assure client that you accept him/her

31
Nonverbal Behaviors
Eye contact Posture Sitting across desk Leaning forward Phone ringing Looking at clock/watch Voice

32
Methods to Acheive Client-Centered Counseling
(con’t)
Use empathetic statements to keep client talking
Explore problem to determine possible alternatives
Use open-ended questions» Begin with how, what, and why» Have you ever been on a diet ?vs How
have you tried to control your weight?

33
Methods to Acheive Client-Centered Counseling
(con’t)
Use directives» “Talk about _____”» I want to know what you think about ---”» “Tell me more about -----”
Use encouragers» “yes, yes”, “ah ha”» Lean forward or nod your head» Remain silent after client finishes

34
Consumer Information Processing (CIP)
Central premise: Individuals can process only a limited amount of information at one time.
This thery is very helpful when planning a nutrition class or deciding what information to share in a couseling session.

35
CIP (con’t)
In order to be used nutrition information should be:
Available Considered useful Not confusing Tailored to the comprehension level of
the audience

36
CIP (con’t)
Accessible at the time of decision making
Matched to the person’s past experiences

37
Methods to Acheive Client-Centered Counseling
(con’t)
Practice active listening» Rephrase what client has said» “Let me see if I understand what you are
saying---” Practice self- monitoring--be aware of the
effect of your reactions Resolve--Agree with client on goals Closure--Make plans for next visit

38
Family-Centered Counseling
Recognizes that the family unit is a system that is affected by the behavior and development of each member
The family is the constant in the client’s life, whereas the service systems and personnel within those systems may be involved episodically

39
Family-Centered Counseling (con’t)
Empowers families by making them a partner in the decision-making process
Enables families by fostering their independence and existing skills and helping them to develop additional skills

55
Primary Sources Used
Frankle and Owen. Nutrition in the community. Mosby, St. Louis, 1993.
Hertzler AA, Stadler KM, Lawrence R, Alleyne LA, Mattioli LD, Majidy M. Enpowerment: a food guidance process for cross-cultural counseling. J Family and Consumer Sciences, summer, 1995 45-50.
56
Primary Sources (con’t)
Brownell J. Relational listening: fostering effective communication practices in diverse organizational environment. Hospitality and Tourism Educator. 6(4):11-16; 1994.
Boyle MA, Morris DH. Community Nutrition in Action an Entrepreneurial Approach. West Publishing, Minneapolis. 1994

















