24
100+ Clinical Cases in Pediatrics
R Arvind mbbs dch dnb
consultant Pediatrician and neonatologistmedical director
Vathsalya speciality hospitalbengaluru, Karnataka, India
Fourth Edition
New Delhi | London | Philadelphia | PanamaThe Health Sciences Publisher
Jayp
ee B
rothe
rs
Jaypee Brothers Medical Publishers (P) Ltd
HeadquartersJaypee Brothers Medical Publishers (P) Ltd4838/24, Ansari Road, DaryaganjNew Delhi 110 002, IndiaPhone: +91-11-43574357Fax: +91-11-43574314Email: [email protected]
Overseas OfficesJ.P. Medical Ltd Jaypee-Highlights Medical Publishers Inc Jaypee Medical Inc83 Victoria Street, London City of Knowledge, Bld. 237, Clayton 325 Chestnut StreetSW1H 0HW (UK) Panama City, Panama Suite 412, Philadelphia, PA 19106, USAPhone: +44 20 3170 8910 Phone: +1 507-301-0496 Phone: +1 267-519-9789Fax: +44 (0)20 3008 6180 Fax: +1 507-301-0499 Email: [email protected]: [email protected] Email: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd Jaypee Brothers Medical Publishers (P) Ltd17/1-B Babar Road, Block-B, Shaymali Bhotahity, Kathmandu, NepalMohammadpur, Dhaka-1207 Phone +977-9741283608Bangladesh Email: [email protected]: +08801912003485Email: [email protected]
Website: www.jaypeebrothers.com Website: www.jaypeedigital.com
© 2016, Jaypee Brothers Medical Publishers
The views and opinions expressed in this book are solely those of the original contributor(s)/author(s) and do not necessarily represent those of editor(s) of the book.
All rights reserved. No part of this publication may be reproduced, stored or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission in writing of the publishers.
All brand names and product names used in this book are trade names, service marks, trademarks or registered trademarks of their respective owners. The publisher is not associated with any product or vendor mentioned in this book.
Medical knowledge and practice change constantly. This book is designed to provide accurate, authoritative information about the subject matter in question. However, readers are advised to check the most current information available on procedures included and check information from the manufacturer of each product to be administered, to verify the recommended dose, formula, method and duration of administration, adverse effects and contraindications. It is the responsibility of the practitioner to take all appropriate safety precautions. Neither the publisher nor the author(s)/editor(s) assume any liability for any injury and/or damage to persons or property arising from or related to use of material in this book.
This book is sold on the understanding that the publisher is not engaged in providing professional medical services. If such advice or services are required, the services of a competent medical professional should be sought.
Every effort has been made where necessary to contact holders of copyright to obtain permission to reproduce copyright material. If any have been inadvertently overlooked, the publisher will be pleased to make the necessary arrangements at the first opportunity.
Inquiries for bulk sales may be solicited at: [email protected]
100+ Clinical Cases in Pediatrics
Fourth Edition: 2016
ISBN: 978-93-5250-179-3
Printed at
Jayp
ee B
rothe
rs
Dedicated toMy Beloved Father
Late Shri N Rajasekhar
Jayp
ee B
rothe
rs
Preface to the Fourth Edition
100+ Clinical Cases in Pediatrics includes all the possible kind remarks and suggestions of the medical students in this revised fourth edition. All the cases have been thoroughly revised, especially with respect to diagnosis and management.
some uncommon clinical cases have been deleted and two new cases such as acute hemiplegia and human immunodeficiency virus (hIV) have been added in this edition.
clinical features of the cases have been illustrated with the diagrams in their respective cases. The salient laboratory findings and essential diagnostic criteria have been highlighted in the cases.
A comprehensive glossary has been completely elaborated, revised and updated. This helps as a ready reckoner for undergraduate and postgraduate students preparing for various competitive examinations.
The book attempts to improve the clinical and practical approach for undergraduate medical students, interns and residents in diagnosis and presentation of clinical cases. It will be helpful for the postgraduate students and practicing pediatricians as well.
R Arvind
Jayp
ee B
rothe
rs
Preface to the First Edition
With the new medical council of India (mcI) guidelines laying more emphasis on clinical and practical skill development rather than theoretical knowledge, there is immense need for a book on common clinical cases in pediatrics. The present book attempts to fulfill this need and aims to help the undergraduate medical students, interns and residents in diagnosis and presentation of clinical cases. It would also be helpful to the postgraduate students and the practicing pediatricians.
The most commonly encountered and typical cases have been grouped into 12 categories that include birth defects and genetic disorders, respiratory, cardiovascular, gastrointestinal, hematological, renal, central nervous system, endocrine and metabolic, nutritional, oncological disorders, disorders of connective tissue, bones and joints, and the infectious diseases. Each case has been discussed in detail under history, clinical features, differential diagnosis, complications and treatment. At the end of each case, multiple choice questions have been added to help the student in revision. A comprehensive and exhaustive glossary has also been included. The book is well illustrated with photographs wherever required.
I thank my wife dr chethana, for her suggestions and professional help. I am also thankful to Rachana and shikar, the gems of my family, for their cooperation.
I express my deep gratitude to m/s cyber Avenue, for typing the manuscript.
R Arvind
Jayp
ee B
rothe
rs
Acknowledgments
I thank my wife dr chethana, for her professional help. I am thankful to Rachana and shikar, for their cooperation. I express my deep gratitude to mr sarvesh hebber, for typing the manuscript.
my special thanks are due to shri Jitendar P Vij (Group chairman), mr Ankit Vij (Group President), mr Tarun duneja (director–Publishing) and staff of m/s Jaypee brothers medical Publishers (P) Ltd, new delhi, India, for publishing this book.
Jayp
ee B
rothe
rs
Contents
Case 1 down syndrome 1Case 2 Klinefelter syndrome 9Case 3 Turner’s syndrome 13Case 4 bronchial Asthma 17Case 5 bronchiectasis 27Case 6 bronchiolitis 32Case 7 croup 36Case 8 Empyema 40Case 9 Otitis media 45Case 10 Pneumonia 51Case 11 Tuberculosis 57Case 12 Atrial septal defect 69Case 13 coarctation of Aorta 73Case 14 Patent ductus Arteriosus 77Case 15 Pericarditis with Effusion 81Case 16 sydenham’s chorea 85Case 17 Tetralogy of Fallot 88Case 18 Ventricular septal defect 93Case 19 Acute Gastroenteritis 97Case 20 Appendicitis 110Case 21 congenital hypertrophic Pyloric stenosis 114Case 22 diaphragmatic hernia 118Case 23 Gastroesophageal Reflux 122Case 24 hepatitis 128Case 25 Intussusception 133Case 26 necrotizing Enterocolitis 138Case 27 Tracheoesophageal Fistula 142Case 28 Wilson’s disease 146Case 29 hemophilia 153Case 30 hemorrhagic disease of the newborn 161Case 31 hereditary spherocytosis 164Case 32 Idiopathic Thrombocytopenic Purpura 168
Jayp
ee B
rothe
rs
xiv 100+ Clinical Cases in Pediatrics
Case 33 Iron deficiency Anemia 173Case 34 Polycythemia 181Case 35 sickle cell Anemia 185Case 36 Thalassemia 194Case 37 Acute Poststreptococcal Glomerulonephritis 202Case 38 hemolytic Uremic syndrome 209Case 39 nephrotic syndrome 215Case 40 Urinary Tract Infection 225Case 41 Acute hemiplegia of childhood 235Case 42 cerebral Palsy 239Case 43 duchenne muscular dystrophy 247Case 44 Epilepsy 251Case 45 Febrile convulsions 262Case 46 Guillain-barré syndrome 268Case 47 hydrocephalus 273Case 48 meningitis 281Case 49 meningomyelocele 290Case 50 Ambiguous Genitalia 293Case 51 congenital Adrenal hyperplasia 298Case 52 cushing’s syndrome 305Case 53 diabetes Insipidus 309Case 54 diabetes mellitus 313Case 55 hypothyroidism 319Case 56 Precocious Puberty 324Case 57 congenital Rubella 329Case 58 congenital syphilis 333Case 59 dengue Fever 339Case 60 human Immunodeficiency Virus 344Case 61 malaria 349Case 62 measles 354Case 63 mumps 358Case 64 Osteomyelitis 361Case 65 Poliomyelitis 366Case 66 septic Arthritis 371Case 67 Tetanus neonatorum 375Case 68 Typhoid 380
Jayp
ee B
rothe
rs
contents xv
Case 69 Varicella 385Case 70 Whooping cough 390Case 71 birth Asphyxia 395Case 72 neonatal seizures 405Case 73 neonatal Pathological Jaundice 413Case 74 normal newborn 425Case 75 Premature Infant 437Case 76 Respiratory distress syndrome 448Case 77 Protein-Energy malnutrition 459Case 78 Rickets 468Case 79 scurvy 473Case 80 Ewing’s sarcoma 477Case 81 hodgkin’s disease 481Case 82 Leukemia 487Case 83 neuroblastoma 495Case 84 Osteosarcoma 502Case 85 Retinoblastoma 507Case 86 Wilms’ Tumor 511Case 87 Acute Rheumatic Fever 516Case 88 Juvenile Rheumatoid Arthritis 522Case 89 congenital dislocation of hip 526Case 90 Leprosy 530Case 91 marfan’s syndrome 535Case 92 Talipes 538Case 93 Infective Endocarditis 541Case 94 duodenal Atresia 549Case 95 hirschsprung’s disease 553Case 96 Liver Abscess 558Case 97 Undescended Testes 563Case 98 chikungunya 567Case 99 herpes Zoster 570Case 100 neonatal hypoglycemia 574Case 101 hurler’s syndrome 579Case 102 Osteogenesis Imperfecta 583
Glossary 587Index 607
Jayp
ee B
rothe
rs
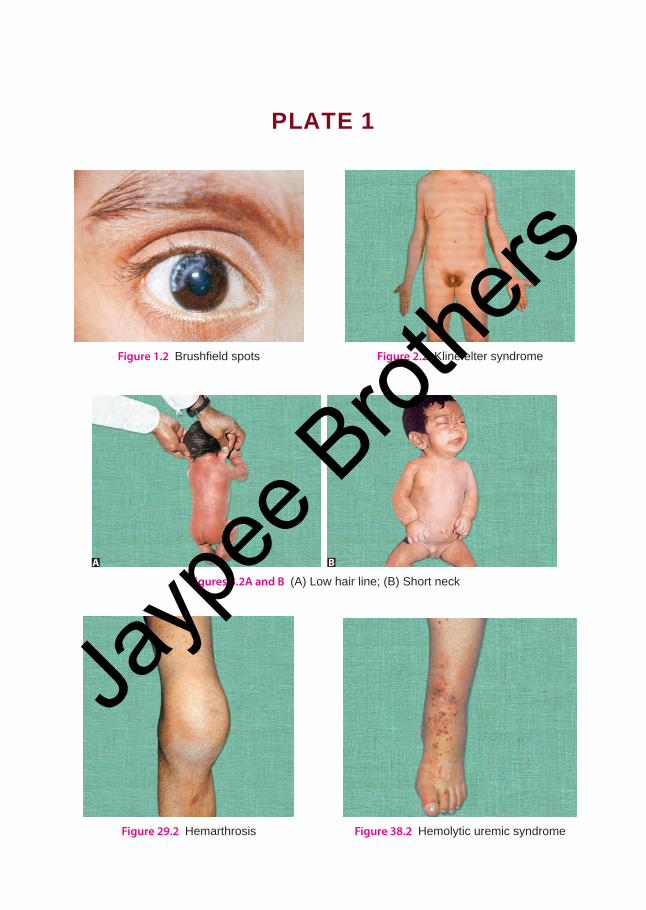
Plate 1
Figure 1.2 Brushfield spots Figure 2.2 Klinefelter syndrome
Figures 3.2A and B (A) Low hair line; (B) Short neck
A B
Figure 29.2 Hemarthrosis Figure 38.2 Hemolytic uremic syndrome
Jayp
ee B
rothe
rs
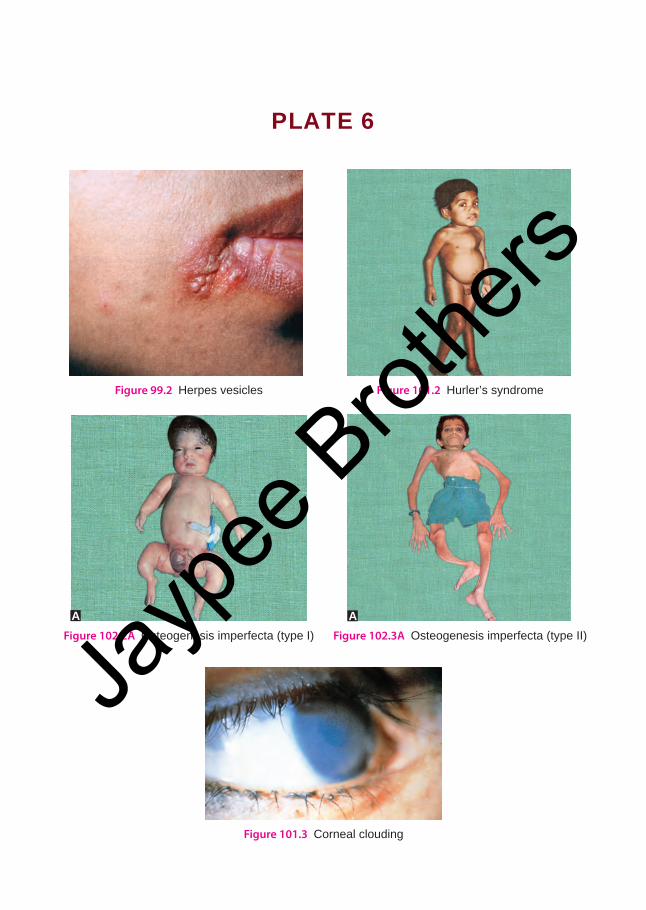
Plate 6
Figure 99.2 Herpes vesicles Figure 101.2 Hurler’s syndrome
Figure 101.3 Corneal clouding
Figure 102.2A Osteogenesis imperfecta (type I) Figure 102.3A Osteogenesis imperfecta (type II)
AA
Jayp
ee B
rothe
rs
case 74Normal Newborn
Presenting ComPlaintsNewborn child was brought for:• General check up.
History of Presenting Complaintsa newborn baby was brought to pediatric outpatient department for general check-up. Mother had delivered the baby in primary health center in village. This baby was the first sibling of consanguineous marriage. Mother had antenatal check-up in the primary health center. she was having regular check-up and had received immunization as per the advice. antenatal health check-up investigations were within normal range.
she went to the primary health center with the delivery pain and there was drainage of the amniotic fluid. Fluid was clear. she delivered vaginally with vertex presentation. The delivery was conducted by the sister. Baby cried immediately after the delivery. cry of the baby was good. Neonatal reflexes were satisfactory. Baby was put to breast immediately. Baby started to take the feeds regularly. Later the baby was sent to pediatric OPD the next day for general check-up.
examination Newborn child was moderately built and moderately nourished. Baby was active, alert, and was crying. The anthropometric measurements included, the weight of the child
was 3 kg (50th centile), length was 51 cm (75th centile) and the head circumference was 35 cm.
child was afebrile, the heart rate was 140 per minute, the respiratory rate was 24 per minute. Blood pressure was 50/40 mm Hg, there was no pallor, acrocyanosis was present, no edema, and no lymphadenopathy.
Neonatal reflexes (NNR) were satisfactory. anterior fontanelle was normal, skin and spine were normal. There were no clinically evident congenital anomalies. The baby was appropriate-for-gestational age.
Case at a Glance
Basic FindingsWeight : 3 kg (50th centile)Length : 51 cm (75th centile) Temperature : 37°CPulse rate : 140 per minuteRespiratory rate : 24 per minuteBlood pressure : 50/40 mm HgPositive FindingsHistory• FTND• Delivered in PHC• Antenatal care was presentExamination• Normal child• NNR satisfactory• No evidence of congenital anomalyInvestigation• Normal
Jayp
ee B
rothe
rs
426 100+ Clinical Cases in Pediatrics
cardiovascular system revealed first and second heart sounds heard. No murmur– suggestive of congenital heart disease. Respiratory system revealed presence of crepitation and rhonchi. Per abdomen examination showed mild distension of the abdomen. There was no significant organomegaly. Bowel sounds were normal.
investigationHemoglobin : 14 g/dLTLc : 12,3000 cells/cu mmDLc : P72 L24 e2 M2Blood culture and sensitivity : sterileUrine culture sensitivity : sterileBlood group and Rh typing : O +vechest X-ray : NaD
DiscussionIt includes history taking and physical examination. History dates from the day of conception till the delivery, and also few days after the delivery. Birth history includes antenatal, natal and postnatal events. Family history of other sibling should also be ascertained.
antenatal history includes previous obstetric history, number of gravida and para. History suggestive of abortion and still-birth should be sought. chronic disease of the mother such as cardiac disease, tuberculosis, hypertension should be ascertained. History of any drug intake, and antenal investigation should be noted.
Natal history includes birth of the child. Mode of delivery, place of the delivery, presentation of the baby, direction of the labor should be ascertained.
In postnatal history birth asphyxia should be noted down. apgar scoring at one minute and 5 minutes should be sought. History of passing of urine and meconium should be ascertained. Presence of jaundice and time of onset of jaundice should be noted.
gestational age assessment (table 1)Two methods that are commonly used clinically for the assessment of gestational age are: Parkin method and new Ballard method.
Gestational age assessment again depends on skin texture, skin color, breast size and breast firmness.
Skin Textureskin texture is tested by picking up the fold of abdominal skin between fingers and thumb and by inspection.score 0 – very thin and gelatinous feel1 – Thin and smooth3 – slight thickening and stiff feeling4 – Thick and parchment-like with superficial
or deep cracking.
Skin Color0 – Dark red1 – Uniformly pink2 – Pale pink3 – Pale.
Breast SizeMeasured by feeling the breast nodule by finger and thumb.0 – No breast tissue palpable1 – Not more than 0.5 cm in diameter2 – 0.5–1 cm in diameter3 – More than 1 cm in diameter.
Ear Firmness
Tested by palpation and folding of the upper pinna and notching and recoiling
score 0—Pinna feels soft and is easily folded in bizarre position without springing back into position spontaneously.
score 1—Pinna feels softer along the edge and easily folded and return slowly to the correct position spontaneously.
Jayp
ee B
rothe
rs
Case 74 : Normal Newborn 427
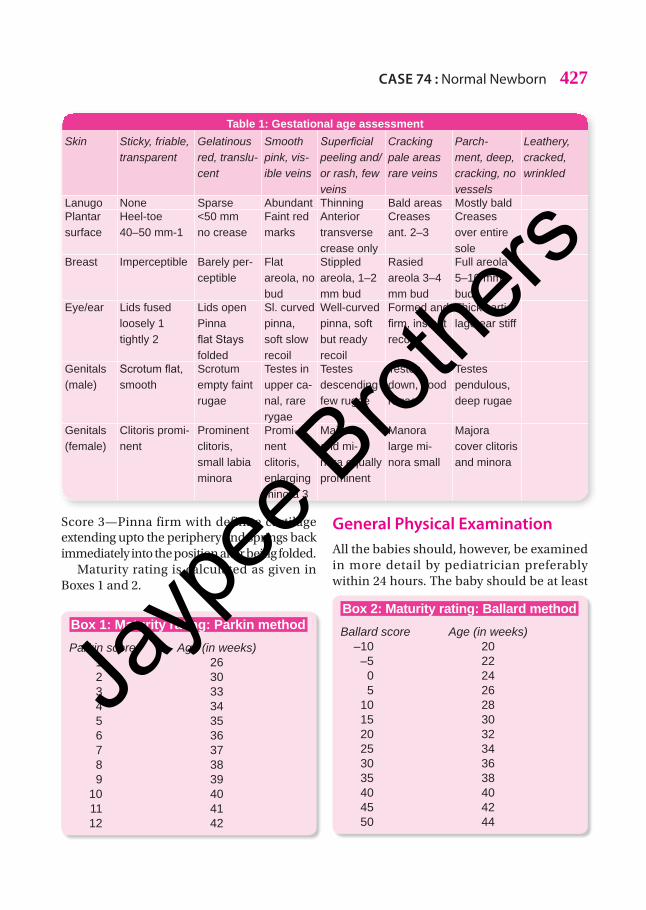
Box 1: Maturity rating: Parkin methodParkin score Age (in weeks) 1 26 2 30 3 33 4 34 5 35 6 36 7 37 8 38 9 39 10 40 11 41 12 42
Box 2: Maturity rating: Ballard methodBallard score Age (in weeks) –10 20 –5 22 0 24 5 26 10 28 15 30 20 32 25 34 30 36 35 38 40 40 45 42 50 44
Table 1: Gestational age assessmentSkin Sticky, friable,
transparentGelatinous red, translu-cent
Smooth pink, vis-ible veins
Superficial peeling and/or rash, few veins
Cracking pale areas rare veins
Parch-ment, deep, cracking, no vessels
Leathery, cracked, wrinkled
Lanugo None Sparse Abundant Thinning Bald areas Mostly baldPlantar surface
Heel-toe 40–50 mm-1
<50 mm no crease
Faint red marks
Anterior transverse crease only
Creases ant. 2–3
Creases over entire sole
Breast Imperceptible Barely per-ceptible
Flat areola, no bud
Stippled areola, 1–2 mm bud
Rasied areola 3–4 mm bud
Full areola 5–10 mm bud
Eye/ear Lids fused loosely 1 tightly 2
Lids open Pinna flatStaysfolded
Sl. curved pinna, soft slow recoil
Well-curved pinna, soft but ready recoil
Formed and firm,instantrecoil
Thick carti-lage ear stiff
Genitals (male)
Scrotumflat,smooth
Scrotum empty faint rugae
Testes in upper ca-nal, rare rygae
Testes descending few rugae
Testes down, good rugae
Testes pendulous, deep rugae
Genitals (female)
Clitoris promi-nent
Prominent clitoris, small labia minora
Promi-nent clitoris, enlarging minora 3
Majora and mi-nora equally prominent
Manora large mi-nora small
Majora cover clitoris and minora
score 3—Pinna firm with definite cartilage extending upto the periphery and springs back immediately into the position after being folded.
Maturity rating is calculated as given in Boxes 1 and 2.
general Physical examinationall the babies should, however, be examined in more detail by pediatrician preferably within 24 hours. The baby should be at least
Jayp
ee B
rothe
rs
428 100+ Clinical Cases in Pediatrics
6 hours old before preliminary detailed examination. However, the examination of the child should be conducted usually for 3 times, i.e.• at birth• after 24 hours• at the time of discharge.
The main objective of the examination is to screen hidden abnormalities of the heart, abdomen and hips and reassure parents about the minor abnormalities and normal variants. Mother should always be at the bedside, so that she is allowed to express her concern. as soon as the baby is delivered baby should be taken in prewarmed baby tray. cord is clamped and cut. Baby should never be kept naked for more than one minute.
Once the respiratory status of the child is settled, then the routine examination of the child is designed to assess the general status of health and to detect the hidden congenital anomalies.
Much of the time is devoted to inspection of the child. It includes awareness and activity of the child. Peripheral cyanosis is normal in newborn, but central cyanosis will indicate cardiac or respiratory disease. cyanosis in the mucous membrane is more reliable in dark neonate. Presence of jaundice in first 24 hours is pathological and should be investigated.
Vernix caseosa, a greasy cheese-like material which disappears after few hours is present at the folds of the neck and groin. Newborn will have extremely smooth skin. Thin gelatinous skin is seen in preterm babies. Dry and cracked skin which tend to peel are seen in post-mature child. abnormally high pitched cry indicates cNs insult. Weak and feeble cry should be investigated.
Next anthropometric measurement of the neonate should be done. These include length, weight, head circumference, chest circumference, and upper segment and lower segment ratio. The vital parameters indicate status of the neonate. The normal ranges are given in Box 3.
Box 3: Normal vital data of newbornCore temperature – 36.5–37°C Respiratory rate – 40 per minute Heart rate – 120–140 per minute Blood pressure – 60/40 mm Hg
after glancing through the inspectory findings and recording the vital parameters, any clues regarding congenital anomalies in the baby should be looked for. History suggestive of the amount of the amniotic fluid should be ascertained. Polyhydramnios in the mother is associated with upper intestinal obstruction like esophageal atresia and duodenal atresia. Oligohydramnios is associated with bilateral renal agenesis and obstructive uropathy.
Incidence of congenital anomalies are common among preterm babies. Usually one congenital anomaly will be associated with other congenital anomalies. Hypoplastic type of small-for-the date babies are prone to have congenital anomalies.
single umbilical artery is usually associated with imperforate anus, genitourinar y abnormalities and esophageal atresia. asymmetry of the face occurs as a result of congenital hypoplasia of depressor anguli oris muscle. single palmar crease is seen in Down’s syndrome. Potency of all the orifices and midline abnormalities should be seen.
Heart should be examined when the child is calm. some systolic murmurs are common during first 48 hours. Breath sounds are equal and clear on both the sides. Faint crepitations heard are due to retained lung fluids. This will be absorbed spontaneously. coarse crepitations are due to loose secretion in the upper airway and throat.
regional Physical examination
Head The shape and symmetry of the newborn vary considerably. Many factors are responsible for these variabilities. These include intrauterine
Jayp
ee B
rothe
rs
Case 74 : Normal Newborn 429
position and pressure, presentation at the time of the delivery and the amount of molding during labor and delivery. The shape returns to normal within 3 days.
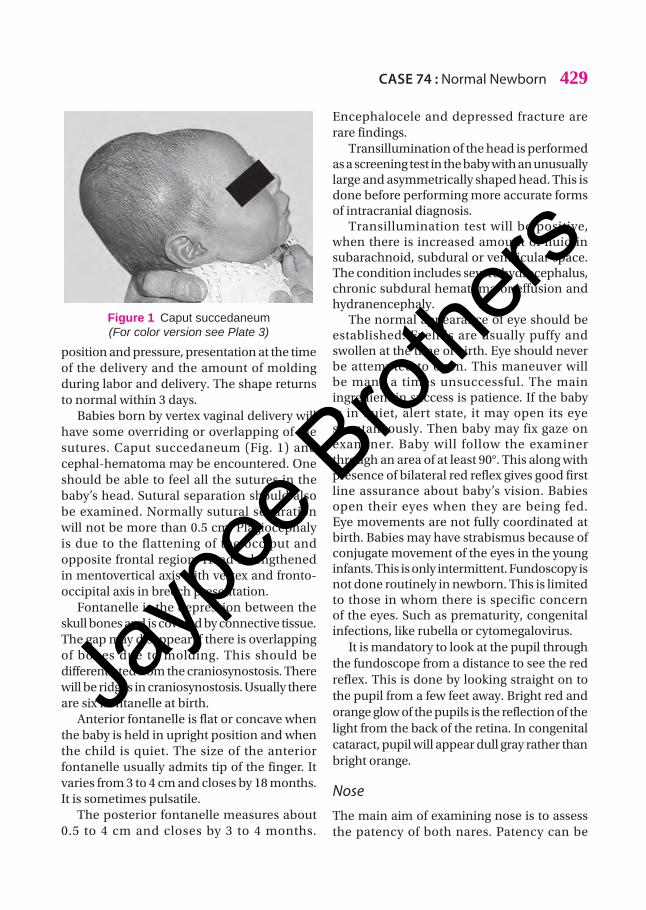
Babies born by vertex vaginal delivery will have some overriding or overlapping of the sutures. caput succedaneum (Fig. 1) and cephal-hematoma may be encountered. One should be able to feel all the sutures in the baby’s head. sutural separation should also be examined. Normally sutural separation will not be more than 0.5 cm. Plagiocephaly is due to the flattening of the occiput and opposite frontal region. Head is lengthened in mentovertical axis with vertex and fronto-occipital axis in breech presentation.
Fontanelle is the depression between the skull bones and is covered by connective tissue. The gap may disappear if there is overlapping of bones due to molding. This should be differentiated from the craniosynostosis. There will be ridges in craniosynostosis. Usually there are six frontanelle at birth.
anterior fontanelle is flat or concave when the baby is held in upright position and when the child is quiet. The size of the anterior fontanelle usually admits tip of the finger. It varies from 3 to 4 cm and closes by 18 months. It is sometimes pulsatile.
The posterior fontanelle measures about 0.5 to 4 cm and closes by 3 to 4 months.
encephalocele and depressed fracture are rare findings.
Transillumination of the head is performed as a screening test in the baby with an unusually large and asymmetrically shaped head. This is done before performing more accurate forms of intracranial diagnosis.
Transillumination test will be positive, when there is increased amount of fluid in subarachnoid, subdural or ventricular space. The condition includes severe hydrocephalus, chronic subdural hematoma or effusion and hydranencephaly.
The normal appearance of eye should be established. eyelids are usually puffy and swollen at the time of birth. eye should never be attempted to open. This maneuver will be many a times unsuccessful. The main ingredient in success is patience. If the baby is in quiet, alert state, it may open its eye spontaneously. Then baby may fix gaze on examiner. Baby will follow the examiner through an area of at least 90°. This along with presence of bilateral red reflex gives good first line assurance about baby’s vision. Babies open their eyes when they are being fed. eye movements are not fully coordinated at birth. Babies may have strabismus because of conjugate movement of the eyes in the young infants. This is only intermittent. Fundoscopy is not done routinely in newborn. This is limited to those in whom there is specific concern of the eyes. such as prematurity, congenital infections, like rubella or cytomegalovirus.
It is mandatory to look at the pupil through the fundoscope from a distance to see the red reflex. This is done by looking straight on to the pupil from a few feet away. Bright red and orange glow of the pupils is the reflection of the light from the back of the retina. In congenital cataract, pupil will appear dull gray rather than bright orange.
NoseThe main aim of examining nose is to assess the patency of both nares. Patency can be
Figure 1 Caput succedaneum (For color version see Plate 3)
Jayp
ee B
rothe
rs
430 100+ Clinical Cases in Pediatrics
established by blocking one nostril and then the other with finger while the baby’s mouth is closed. air movements in each nostril is heard either directly or by stethoscope.
In a suspected case of choanal atresia or stenosis, a soft catheter is passed through the passage. a baby with bilateral choanal atresia usually presents with respiratory distress and cyanosis. Distress and cyanosis will be relieved when baby opens the mouth or while crying.
Mouthepithelial cells, i.e. epstein pearls on the palate or gum margins are normally found. Tongue-tie will be associated with frenulum. Uvula configuration is noted. The bifid uvula may be the only sign of submucus cleft of the palate.
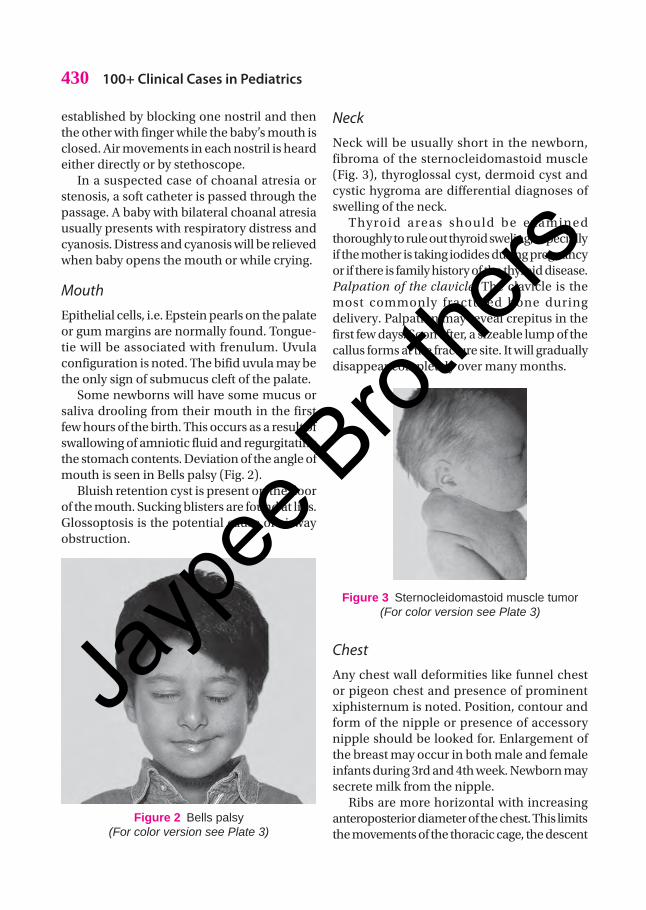
some newborns will have some mucus or saliva drooling from their mouth in the first few hours of the birth. This occurs as a result of swallowing of amniotic fluid and regurgitating the stomach contents. Deviation of the angle of mouth is seen in Bells palsy (Fig. 2).
Bluish retention cyst is present on the floor of the mouth. sucking blisters are found at lips. Glossoptosis is the potential cause of airway obstruction.
Neck Neck will be usually short in the newborn, fibroma of the sternocleidomastoid muscle (Fig. 3), thyroglossal cyst, dermoid cyst and cystic hygroma are differential diagnoses of swelling of the neck.
Thyroid areas should be examined thoroughly to rule out thyroid sweling, especially if the mother is taking iodides during pregnancy or if there is family history of the thyroid disease.Palpation of the clavicle: The clavicle is the most commonly fractured bone during delivery. Palpation may reveal crepitus in the first few days. soon after, a sizeable lump of the callus forms at the fracture site. It will gradually disappear completely over many months.
Figure 3 Sternocleidomastoid muscle tumor (For color version see Plate 3)
Chestany chest wall deformities like funnel chest or pigeon chest and presence of prominent xiphisternum is noted. Position, contour and form of the nipple or presence of accessory nipple should be looked for. enlargement of the breast may occur in both male and female infants during 3rd and 4th week. Newborn may secrete milk from the nipple.
Ribs are more horizontal with increasing anteroposterior diameter of the chest. This limits the movements of the thoracic cage, the descent
Figure 2 Bells palsy (For color version see Plate 3)
Jayp
ee B
rothe
rs

Case 74 : Normal Newborn 431
of the diaphragm, the abdominal controls and pushes the abdominal wall forward.
In newborn, respiration is normally irregular in both amplitude and frequency. This is associated with the pauses lasting less than 10 seconds. Irregular breathing pattern is more marked in prematures. The respiratory rate averages 30 to 40 breath per minute, in a resting full-term baby. Breath sounds should be heard well in the front and the back, few crackles may be heard immediately after the birth within few hours.
Intercostal indrawing is very common among the preterm babies because of the softness of the ribs. Overinflated chest is seen in meconium aspirated newborn.
Cardiovascular systemWhen the baby is quiet, the heart should be auscultated to find out whether it is present in left side or right side. Heart rate should be counted. The normal range is 160 beats per minute in a calm child. It will vary when the child is crying and taking feeds. Occasional extra systoles are common. The two heart sounds are usually equal in intensity. The normal variation of the width of the split in the second sound with the respiration may be difficult to appreciate because the respiratory or heart rate is rapid.
sometimes, in the first few days, it is common to hear soft precordial systolic murmurs. This is probably due to flow through ductus arteriosus, that remain patent immediately after the birth. This closes gradually over the hours or days. cardiac murmur heard during first 48 hours can be transient or a significant murmur.
Criteria for significant murmur• Loud grade III murmur. abnormal second
heart sound• associated ejection click.
cyanosis in neonate indicates hypoxemia. It is due to shunting of the venous blood from pulmonary to systemic circulation, i.e. right to left shunt.
Radial and femoral pulses should be palpated and compared to the other side. absence of femoral pulse, brachiofemoral delay indicates the coarctation of aorta.
Abdomenabdomen of the normal baby looks slightly protuberant. slight separation is frequently felt between the recti muscles, i.e. diastasis recti (Fig. 4). Upper abdominal wall distension is common after feeds. absence of lower abdominal distension with marked peristaltic movement and gross distension without peristaltic movement is an indication for immediate investigation.
Umbilical cord should be inspected for number of vessels present in it. shrinkage of the cord with the drying occurs rapidly after the birth as a result of closure of umbilical arteries. This produces deprivation of the blood supply to tissues. separation of cord generally takes place between 5th and 10th day. application of local antiseptics prevents the delay in separation. a discharge from the cord stump should exclude infant with persistent urachus. Umbilical granuloma is a firm tissue present at the site of separation. This has to be distinguished from the polyp in the persistent part of mesenteric duct. This requires surgical removal. cord granuloma can be treated with cooper sulphate granule application.
Figure 4 Diastasis recti (For color version see Plate 3)
Jayp
ee B
rothe
rs

432 100+ Clinical Cases in Pediatrics
In intrauterine growth retarded baby, the cord is often thin and stingy with little Wharton’s jelly. In baby who has been bathed in meconium in utero for more than few hours, the cord may be stained green.
Umbilical hernia may be present at birth. It is more common among preterm and low birth weight babies. Gastroschisis or omphalocele can occur due to diversification of recti.
Palpation of the abdomen is simple during the feed, but care must be taken not to cause vomiting.
LiverNormally liver is palpable in epigastrium. Poorly defined liver edge is palpable in the right upper quadrant by applying the thumb or fingers gently to the surface of the skin. The edge is normally felt 1–2 cm below the right costal margin in the midaxillary line.
Spleenspleen may or may not be palpable in newborn. It is enlarged more laterally than in the older children. Tip points to the left rather than the right loin. ability to palpate the tip of the spleen on deep inspiration is not always an indication of abnormality. But this should be considered along with other findings. Palpation should also include a search for unusual masses.
KidneysBoth the kidneys are readily palpable during first and second day before the bowels are fully distended. During the third day, only the lower pole is palpable. Unless they are enlarged and abdomen is unusually soft, bladder is usually palpable in infancy.
GenitaliaGenitalia examination will help to estimate the gestational age. In male, glans penis is normally covered completely by prepuce that
should not be fully retracted. Penile foreskin is adherent. Normally, urine should pass in full stream without ballooning the prepuce.
Identification of the urethral opening is important. Hooded prepuce is present with hypospadias.
scrotum is best examined with the quiet baby and warm hand. scrotum is usually large as it is the embryonic analog of the tibia of female. scrotum in a full-term boy is pendulous and rugosity is well formed. It may be more pigmented than the rest of the skin.
Both the gonads should be palpable and capable of being brought into the scrotum. The testes should be completely descended. The normal testis is 1–2 cm long and should be identical in size, neither soft nor hard in consistency.
In hydrocele of the tunica vaginalis, small collection of fluid disappear within few days if it is communicating type. Large collection of fluid around the cord should lead to hernia.
In female newborn, genitalia will have relatively large labia majora, that cover and occlude the labia minora and vaginal introitus. considerable thick vaginal discharge may be present, especially on the second and third day. Minor bleeding is also noted. This is normal unless there is more blood loss in the urine. Mucosal tag from wall of the vagina is seen. These are common abnormalities. In girls, clitoris is prominent. If the infant is premature labia minora is also seen covered by labia majora. In case of ambiguous genitalia, a chromosomal analysis should be done.
Rectal prolapse (Fig. 5) occurs because of weakness of pelvic floor muscle. This is in malnutrition and chronic diarrhea.
ExtremitiesUpper limb abnormalities of the hand are common features of dysmorphism. Number of the fingers and toes, presence of syndactyly should be looked and noted. slight syndactyly
Jayp
ee B
rothe
rs
Case 74 : Normal Newborn 433
of the second and third toes is a common minor congenital anomaly.
Most normal newborns have slight bowing of legs. This disappears gradually as the child gets older. This reflects intrauterine position.
Postural talipes should be differentiated from true talipes. Postural type can always be straightened. It usually reverts to normal within few weeks.
Rudimentary skin tags at the lateral border of either fifth finger or toe may represent rudimentary supernumerary digits. extra long nails are common in post-term infants.
BackBack is completely examined till down the natal cleft. congenital defects in the dorsal surface may give clue for internal anomalies. Pilonidal sinus is the common finding present. This may disappear gradually and has no special significance (Fig. 6).
any hemangioma, lipoma or tuft of hair that crosses the midline of the lower back has high probability of internal structural spinal abnormalities.
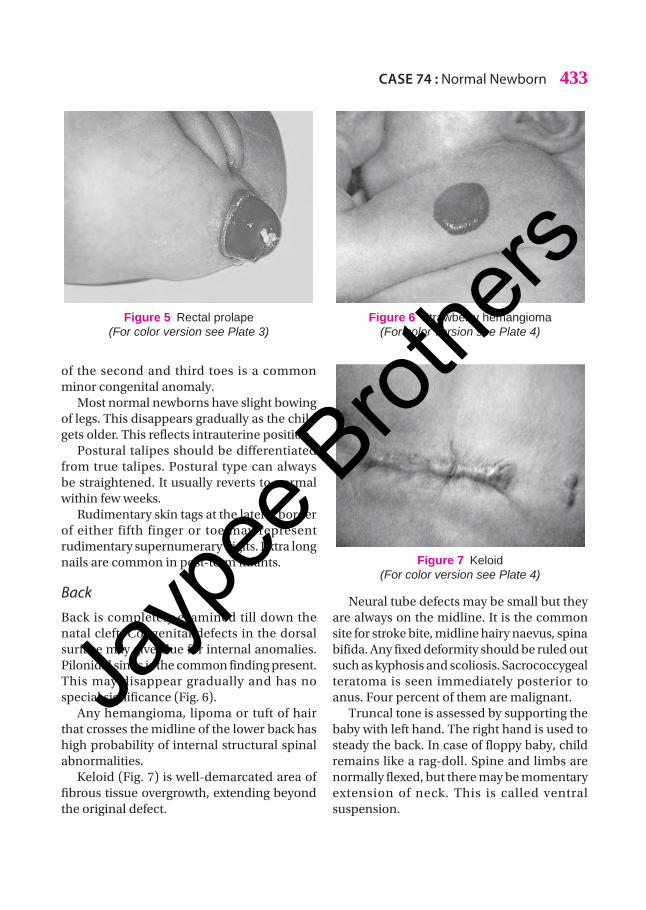
Keloid (Fig. 7) is well-demarcated area of fibrous tissue overgrowth, extending beyond the original defect.
Neural tube defects may be small but they are always on the midline. It is the common site for stroke bite, midline hairy naevus, spina bifida. any fixed deformity should be ruled out such as kyphosis and scoliosis. sacrococcygeal teratoma is seen immediately posterior to anus. Four percent of them are malignant.
Truncal tone is assessed by supporting the baby with left hand. The right hand is used to steady the back. In case of floppy baby, child remains like a rag-doll. spine and limbs are normally flexed, but there may be momentary extension of neck. This is called ventral suspension.
Figure 6 Strawberry hemangioma (For color version see Plate 4)
Figure 7 Keloid (For color version see Plate 4)
Figure 5 Rectal prolape (For color version see Plate 3)
Jayp
ee B
rothe
rs
434 100+ Clinical Cases in Pediatrics
Nervous SystemNervous system starts with the sensorium of the child. It is otherwise, the alertness of the child. It is classified as:
State of wakefulness in neonatestate I – Deep sleep with regular
respirationstate II – Light sleep with regular
respirationstate III – eyes open with no gross
body movementsstate IV – eyes open with gross body
movementsstate V – eyes open or closed and
crying
motor Functionsspontaneous movements normally take place when the baby is awake consisting of alternating flexion and extension. Normally the tone of the newborn is hypertonia and that of preterm is hypotonia. Deep tendon reflexes are usually brisk and variable. Normally ankle clonus may be present with 6 to 8 jerks uninterrupted.
sensory function has limited value in newborn. anal reflex should be tested in neural tube defects. Vision is very difficult to test. It is told that visual acuity in newborn is 6/45.
Hearing is judged by startle response including blinking of the eye and changes in the heart rate. These changes are seen as response to 500 to 1000 cycles per second.
Behavior of the Newborn InfantIt is determined by internal resources and the response to external environment. Infant’s behavior can be judged at rest after stimulation. The mother and child can start with positive attitude.
Examination of the Cranial NerveFirst cranial nerve cannot be tested in the newborn or neonate. second cranial nerve
can be examined by the way the child turns to diffuse light. If both the eyes rotate in the same direction, it suggests that the IIIrd, IVth, VIth cranial nerves are intact. Doll’s eyes response in turning of the eye in the opposite direction involves the integrity of III, IV and VI cranial nerves. Ptosis and pupillary reaction signify IInd cranial nerve.
Presence of the rooting reflex indicates that Vth nerve is intact and crying and grimace suggest the VIIth cranial nerve.
Optokinetic nystagmus is elicited by holding the baby on the back on outstretched arms, hands supporting the occiput and gently turning slowly in clockwise direction. This suggests the intact vestibular part of the VIIIth nerve. startle response indicates auditory part of the VIIIth nerve. IX and Xth cranial nerves are judged by gag reflex. Vigorous sucking and striping action by tongue suggests that XIIth cranial nerve is intact.
Hip Joint examination Stability of the JointThe most common screening maneuver combines those described by Ortalani and Barlow. With the baby supine on a firm surface, flex its thighs to right angle to the abdomen and its knees to the right angle to thighs. Then, the thigh is grasped with the examiner’s fingers along the outside of the shaft of the femur, with the middle fingertips on the greater trochanter, and examiner’s thumb medially in the femoral triangle.
With the baby at rest, first femur is adducted completely and gently abducted from the position of full adduction so that knees come to lie laterally on the mattress. During abduction, greater trochanter is pushed medially with the fingers. If there is a click either during adduction or abduction or if there is resistance as the knee approaches full abduction or if there is a spasm or discomfort of the abductor muscles of the femur, the baby probably has congenitally dislocated or dislocatable hip.
Jayp
ee B
rothe
rs
Case 74 : Normal Newborn 435
Unstable hips: Many unstable joints, following breech delivery become stable within few days. It is prudent to re-examine the hips after 24 to 48 hours.Dislocated hips: Here abduction at the affected hip is limited and difficulty in abducting either hip to 80° should arise the suspicion of congenital dislocation.
Pediatrician should be alerted of some of the signs or symptoms listed in the box are noticed:
Alarming Signs in Neonate
• Bleeding from any site• Appearance of jaundice within 24 hours• Poor feeding• Lethargy• Excessive crying• Respiratory distress or cyanosis• Convulsions• Not passing urine within 72 hours• Not passing motion within 24 hours
ReflexesGrasp reflex: This is elicited in hand and feet. This is done by pressing the finger lightly against the palm and sole. The lightness of the grasp in often sufficient. This is enough for tractions response. It is generally safer to do this by holding the infant’s wrist and pulling him slowly to the sitting posture. The infant flexes his elbows as if he is trying to assist the movements. Hence, attempt should be made to hold the head in line with the trunk as it is raised.
Moro reflex: This is elicited by allowing the head to fall back unsupported for a short distance. sudden extension and abduction of the limbs followed by slower adduction and flexion to the resting position.
Rooting reflex: This is elicited by touching the infant’s cheeks to turn eagerly to the side. This is stimulated in the hope of finding the nipple.
Crossed extension response: This is elicited by extending one leg and tickling the other sole. a positive response is movement of extension possibly with the adduction to the lower leg.
Stepping movements: When the child is held erect with the feet on a firm surface, a full-term infant attempts to straighten trunk and make a stepping movement with his legs.
skin of the newborn
Vernix Caseosaat birth the normal full-term infant is covered by vernix caseosa. It is a greasy substance that protects the skin during the lengthy immersion in amniotic fluid. This is the normal sebaceous secretion of the skin. The skin of the face and head may exhibit a variety of changes. It is important to reassure the parents.
Angiomatous LesionThese are small, flame-shaped, flat hem-angioma over the eyelids and the roof of the nose. These should be differentiated from port-wine stains. These are larger, permanent and may involve areas of face or head in a particular nerve distribution, especially trigeminal nerve distribution.
MiliaThese are small white spots on the face. These represent hyperactive sebaceous glands with visible retained secretion.
PetechiaePetechiae on the face are quite common. These are pinpoint in size. They do not blanch with pressure. They usually result from increased presence in the venous system during a vertex vaginal delivery. They may appear on the face on face presentation, on buttocks after breech delivery. Bruising, i.e. ecchymoses may be related to delivery trauma.
Jayp
ee B
rothe
rs
436 100+ Clinical Cases in Pediatrics
Erythema ToxicumIt is a newborn rash which is extremely common in full-term infants. The lesions usually appear as white pustules on an erythematous base. These are 1–3 mm in diameter and occur singly or in groups. The lesions contain many eosinophils. In case of pustules, lesions contain gram-positive cocci like characteristic pustules.
The skin changes seen in post-maturity are dryness, flakiness or cracking of the skin. The skin lesions that should cause concern and warrant close observation, investigation and treatment often include vesicles, pustules, areas of absent skin (either congenital or aquired) and large, bulky subcutaneous hemangioma.
Jayp
ee B
rothe
rs

















