24
ALCOHOL ADVISORY COUNCIL OF NEW ZEALAND Kaunihera Whakatupato Waipiro o Aotearoa Feature It’s not the drinking: it’s how we’re drinking Young People Think… Consequences Vol 6 No 1 June 2005
| Date post: | 13-Apr-2018 |
| Category: |
Documents |
| Upload: | duongquynh |
| View: | 212 times |
| Download: | 0 times |

ALCOHOL ADVISORY COUNCIL OF NEW ZEALAND
Kaunihera Whakatupato Waipiro o Aotearoa
FeatureIt’s not the drinking:
it’s how we’re drinking
Young PeopleThink… Consequences
Vol 6 No 1 June 2005

The Alcohol Advisory Council of New Zealand was established by a 1976 Act of Parliament, under the name the Alcoholic Liquor Advisory Council (ALAC), following a report by the Royal Commission of Inquiry into the Sale of Liquor.
The Commission recommended establishing a permanent council whose aim was to encourage responsible alcohol use and minimise misuse.
ALAC’s aims are pursued through policy liaison and advocacy, information and communication, research, intersectoral and community initiatives, and treatment development. ALAC is funded by a levy on all liquor imported into, or manufactured in, New Zealand for sale and employs 30 staff. The Council currently has eight members and reports to the Minister of Health.
alcohol.org.nz is published quarterly by the Alcohol Advisory Council of New Zealand / te Kaunihera Whakatupato Waipiro o Aotearoa. An editorial committee oversees the newsletter.
The next issue of alcohol.org.nz will be published in September 2005. To receive a copy, contact:
Alcohol Advisory CouncilPO Box 5023Wellington New Zealand
Phone 04 917 0060Call free 0508 258 258Fax 04 473 0890Email [email protected]
© ALAC 2005alcohol.org.nzISSN 1175-2831Editor/writer: Lynne Walsh

1
WORDS FROM THE CEO I was pleased to see the recent announcement by the World Health Organisation (WHO) of a probe into alcohol and, in particular, their concern over what they describe as ‘trends in hazardous consumption’ or binge drinking.
The move by WHO shows the increasing globalisation of the issues surrounding alcohol-related harm and the worldwide recognition that it’s the patterns of hazardous drinking that lead to the most acute alcohol-related harm.
A resolution, initiated by Nordic countries, was adopted by ministers from WHO’s 192 member states on the final day of their annual 10-day assembly.
It expressed alarm at ‘trends in hazardous consumption’, or binge drinking, particularly among young people, and cited a growing risk in developing countries.
The United Nations agency will conduct further scientific studies and report back in two years on ways to reduce alcohol-related harm.
The move by WHO demonstrates the increasing acceptance that it’s the way we drink that causes the greatest acute alcohol-related harms, and that of course is the message ALAC has been promoting through our programme designed to change New Zealand’s risky drinking culture.
It’s this pattern of heavy per occasion consumption leading to drunkenness, and the social acceptance that this is an okay thing to do that we want to change.
This move by WHO gives us added assurance that the direction we are heading in this country is the right way to go.
My recent trip across the Tasman has also given us greater confidence that our programme of work is leading-edge. Australia is grappling with the same problems and at a recent meeting in New South Wales we received a great reception for the model we are adopting here.
June 2005
Contents
Features 2
It’s not the drinking:
it’s how we’re drinking
Maori Matters 5
Taumata kaumatua hui
Fifth “Healing our Spirit Worldwide”
gathering 7
Pacific Peoples 8
An exploration into Service Delivery
and Treatment Interventions of Pacific
AOD Services in New Zealand
Early Intervention 10
Alcohol & Drug Helpline update
Young People 13
Think… Consequences
Supply and Provision 14
Project Walk Through
Controlled Purchase Operations 16
Staff 18
New Appointments
Resources 20
Information Services
Dr Mike MacAvoy Chief Executive Officer.
Kia ora, Kia orana, Ni sa bula, Namaste, Taloha ni, Malo e lelei, Fakaalofa atu, Halo olaketa,
Talofa lava, Greetings...

2

Feature
3
New Zealand’s culture
change programme aimed at
changing the way we drink
was well received at meetings
in Canberra and New South
Wales late last month.
The Associate Minister of
Health and Minister in
charge of alcohol policy the
Hon Damien O’Connor
was invited to Canberra by
the Australian Ministerial
Council on Drug Strategy
to present to the group
the Government’s new
programme aimed at
changing New Zealand’s
risky drinking culture.
Mr O’Connor told the council, which is made up of Australian federal and state ministers, that he could see immense opportunity, and indeed necessity, for international alliances to be established to combat the worldwide epidemic of alcohol-related harm.
The World Health Organisation (WHO) had called for a global response and he believed that visiting our closest neighbour was a logical place for New Zealand to start.
Mr O’Connor said New Zealand and Australia had similar problems to address - both had drinking cultures that celebrated drunkenness and intoxication, and the cost of this culture in human and economic terms was too high to be ignored. He invited Australia to consider New Zealand’s programme.
However, he said that while there were strong similarities, he didn’t believe it was possible to uplift an entire programme and replicate it exactly across the Tasman. New Zealand and Australian drinking cultures were products of their own people, and their own unique histories, as well as the way alcohol was regulated in the two countries.
The specific solutions New Zealand had come up with were based on New Zealand research and analysis of those things.
But he said the principles were unquestionably transferable, as, he believed, was the model New Zealand was using and, most importantly, the goal.
Mr O’Connor referred to the way the then New Zealand Land Transport Safety
Authority had adopted the road safety model developed in Victoria to address New Zealand’s road safety issues. New Zealand adopted the Victorian blueprint but adapted it to suit the New Zealand culture and environment.
So too could the New Zealand culture change model be adapted to Australia, he told the Council.
Meanwhile members of ALAC’s executive team were also in Australia presenting the culture change programme to three groups in New South Wales.
ALAC was invited to present to the Australian group responsible for the implementation of the recommendations of the New South Wales Alcohol Summit in 2003. This influential group is made up of senior executives from the NSW Premier’s Department and the Department of Health. They also presented to the NSW Regional Alcohol Promotion Group and the Alcohol Education and Information Taskforce.
ALAC Chief Executive Officer Dr Mike MacAvoy says the response to the New Zealand programme was very enthusiastic.
“They were particularly interested in the way we have taken the whole-of-the-population approach that is focusing on the culture of drinking, the way we all drink, rather than what is often perceived to be only a young person’s problem. That along with the unbending commitment to ensuring a balance of investment and resource across the supply control, demand reduction and problem limitation areas makes this programme different.”
Culture Change in New Zealandit’s not the drinking:it’s how we’re drinking
4
Through the 1990s and
into 2000, public and
political concern over
youth drinking in New
Zealand increased. The
media had a constant
supply of stories about
youth drinking – from
out-of-control parties to
the 14-year-olds passed
out in the shopping malls
on Friday nights. Youth
drinking was on the public
agenda and everyone was
concerned.
In response to concerns, ALAC developed a new five-year strategy that targeted three key audiences – young people, M_ori and Pacific. To inform the development of strategies to address the alcohol-related issues for each group, ALAC completed in-depth research focused on the why, how, when and what of alcohol consumption for these groups. The general tone of the responses from those young people surveyed were:
• There’s nothing wrong with drinking lots – everyone does it.
• Drinking and drunkenness were part of the rites of passage in New Zealand.
• It was good fun.
• Adults did it too so why all the hypocrisy?
A decision was made to carry out further research to test the hypothesis that young people and adults were thinking and doing exactly the same when it came to drinking. This research looked at:
• why people drank and also what stopped them from drinking
• attitudes to drinking and drunkenness
• their behaviour when drinking.
That research led us to two conclusions:
• Adults model and create a drinking culture in New Zealand that supports intoxication as a social norm.
• It was the pattern of heavy per occasion consumption drinking that was causing most of the harm and needed to be addressed.
What’s more, these attitudes and behaviours go across all demographic groups.
At the same time, researchers asked people what would motivate them to change or moderate the way they drink. They told us that they would moderate their drinking on any one occasion for a range of reasons including family and financial reasons or because they didn’t want to look stupid in front of peers and family.
The ProgrammeOn the basis of this research, ALAC took a hard look at its strategic plan, rearticulated parts of it, set an ambitious goal and devised a comprehensive programme to achieve it. Government approved the funding and work began in earnest.
The goal is to enable New Zealanders to drink in a way that shows they believe that it is never okay to get drunk. It is a social marketing approach focused on attitudes and behaviour and must ultimately result in behaviour change. It concentrates on the cause of the harm (drunkenness) rather than targeting the vast range of harms that result.
In other words it is focused on changing the cause of harm rather than addressing the symptoms.
The programme is a full social marketing programme and incorporates all the strands required to achieve the desired change in behaviour across all population groups. What is known is that different people respond to different strategies and therefore it was essential that the programme included:
• communication and education
• policy changes to support behaviour change in the external environment
• provision of services for those who see the need for change and to support them through that change
• stimulating the desire for change.
How did ALAC develop its culture change programme?

The overall theme was ‘Arahingia nga mokopuna he taonga hoki’, that is, kaumatua will show leadership to strengthen mokopuna so they can be the leaders of the future.
Paki Keefe, chairperson for the steering committee which organised the hui, says it was very fruitful.
“Kaumatua identified that one of the major concerns within the Tairawhiti region was easy access to alcohol and other drugs for rangatahi,” she says. “Kaumatua believe that this problem needs to be addressed within the whanau if change is going to come.
“All kaumatua attending the three-day wananga were challenged and encouraged to become champions for change within their communities. To become champions for change, kaumatua need to have a strong belief in the kaupapa, therefore it’s equally important to walk the talk/ kia whakatinanahia te korero, to role model behaviour that will influence change in the whanau. Getting local kaumatua to play a role in spreading the message of moderation and providing advice and support to local alcohol and drug workers can help reduce alcohol-related harm.
“There was a lot of valued-based korero that set the benchmark and tone of the hui that related to tika, pono and aroha and the fact that these concepts are vital elements for Maori when working with whanau.”
Keynote speakers from Nga Manga Puriri of Te Taitokerau and He Oranga Pounamu of Te Waipounamu made a lasting impression on the Tairawhiti kaumatua inspiring them to encourage change and to activate themselves into accepting responsibility to help reduce alcohol-related harm amongst Maori.
5
Maori Matters
Taumata kaumatua huiA wananga was held in Gisborne recently to bring
together kaumatua to discuss how they can help their
young people overcome alcohol-and-drug-related harm.
The three-day taumata kaumatua hui was organised by
local health providers from throughout the Tairawhiti and
held at the Te Poho o Rawiri marae in early March.
The aim of the hui was to get kaumatua to recognise
their role in helping reduce alcohol-and-drug-related
harm within the whanau, hapu and iwi. The hui involved
representatives from Tairawhiti District Health, Turanga
Health, Te Aitanga a Hauiti Hauora, TDH Mental Health
and Addiction Service, Ngati Porou Hauora, Turanganui a
Kiwa Primary Health Organisation and the Tokomaru Bay
Community Charitable Trust.

6
Some of the questions posed at the hui were:
• How can kaumatua impact on whanau, hapu and iwi about alcohol and other drug use?
• How can kaumatua raise awareness for themselves and others about alcohol and other drug use?
Paki believes a taumata kaumatua group should use traditional approaches for the betterment of whanau. Such an approach would assist kaumatua to identify key entry points with whanau, raise awareness, maintain supportive relationships with whanau and identify opportunities for service delivery.
“The kaumatua signalled their desire to take a leadership role in addressing alcohol, drug and mental health concerns in the region,” she says. “However, many wanted to know how they could do that.”
Over the past four years ALAC has been supporting hui around the country to define the role and responsibility for kaumatua in combating alcohol-related problems among whanau, hapu and iwi. The taumata kaumatua hui held in Gisborne was a consequence of that national movement, to engage local kaumatua to participate in wananga to help reduce alcohol related harm amongst whanau, hapu and iwi.
Former ALAC Group Manager Communities Te Atarangi Whiu says ALAC was pleased to sponsor this very successful hui.
“The kaumatua signalled their desire to take a leadership role in addressing alcohol, drug and mental health concerns in the region,”“Recent research commissioned by ALAC shows Maori and non-Maori drink in different ways,” she says. “Pakeha are more likely to drink alcohol and drink more often, but they drink less on a typical drinking occasion. So more Maori are non-drinkers but those that drink consume than Paheka.
“We know that most harms result from drinking too much on a single occasion. Since Maori binge more often than pakeha, the health effects from alcohol
are worse for Maori. The research released earlier this year showed that Maori had four times the number of alcohol-related death compared to non-Maori.
“The differences in the way we drink are such that average alcohol consumption per day between Maori and non-Maori is similar, but the impacts on health differ substantially.
“The harms range from injuries resulting from accidents or fights; problems with relationships because of alcohol; problems at work; neglect of family responsibilities; embarrassment from indulging in behaviours that you wouldn't normally indulge in - all are associated with excessive per occasion consumption.”
Te Atarangi says ALAC has spent considerable time working with Maori communities to build an appreciation of the value of addressing alcohol use because of the impact it has on a number of health and social issues Maori communities and providers are dealing with.
“However, we recognise the best solutions for Maori come from Maori, which is why we welcome local kaumatua working to solve local problems.”

7
Maori Matters
Planning is well underway for the fifth gathering of the Healing our Spirit Worldwide to be held in Edmonton, Alberta, Canada from 6th – 11th August 2006, returning to the place of the first gathering in 1992. The movement has gained momentum since its inception. Indigenous people from Australia (1994) New Zealand (1998) and the United States (2002) have also hosted this international event.
Healing our Spirit Worldwide is an international indigenous conference and a cultural celebration hosted by the International Indigenous Council for HOSW, supported and guided by a host of indigenous organisations worldwide. The conference will create an international forum focusing on programme successes, best practices, and common issues in health, healing and addictions within the indigenous population.
An international covenant was developed and presented during the 2002 conference in Albuquerque, New Mexico stating the need to recognise the role colonisation has played in the substance abuse and health issues experienced by indigenous peoples throughout the world. It further states that to heal and prevent addictions, indigenous people must gain self-determination in directed health services to meet specific cultural needs.
ALAC’s role is to co-ordinate a response to the international conference. A New Zealand project team is working the Maori part of the covenant which will be
presented to the Cutting Edge Conference later this year, before going to Edmonton.
Barry Bublitz (Tangahoe, Tainui) who has a long history working in the addictions and mental health field, is a member of the International Indigenous Council HOSW and has been working closely with his indigenous brothers and sisters in Canada, to ensure the fifth gathering is more than a reunion; that it is an international showcase of new and innovated ways of working with Indigenous peoples.
He works with the project team here helping to plan and coordinate New Zealand’s participation. There will be an opportunity at the Cutting Edge Conference in September to be updated on the HOSW gathering, as the Chairman of HOSW, Rod Jeffries will be present.
If you are considering presenting a paper, or want any other information about this gathering, please contact Barry J. Bublitz by email at [email protected] or call on 021-555-248.
Fifth “Healing Our Spirit”gathering

8
Census data indicates that there are
a growing number of Pacific people
residing in New Zealand (population
of 231, 801 (Statistics New Zealand,
2001). In adapting to life in New
Zealand alcohol consumption has become
part of Pacific hospitality practices and
has formed, for many, a normal part of
socialisation patterns in New Zealand
(Asiasiga, 1999). The role of alcohol for
many Pacific people in New Zealand has
changed as it has become more readily
accessible. Thus, problem drinking and
drug taking have emerged for Pacific
communities.
While there are studies exploring Pacific people’s drinking beliefs and attitudes about the importance of alcohol in their lives (Banwell, 1986; Neich and Park, 1988; ALAC, 1997), there remains a paucity of information on treatment interventions with Pacific people.
In order to address this, ALAC contracted the Clinical Research and Resource Centre (CRRC) to undertake a three-phased project aimed at exploring the current service delivery practices of Pacific AOD services in New Zealand. Entitled the Pacific Alcohol and Drugs Outcomes Project (PADOPT), it investigates issues pertinent to the Pacific population from various perspectives of service delivery.
PHASE IPhase I involved exploring Pacific AOD clinicians’ perceptions about service delivery practices and treatment approaches for Pacific people. Some 31 Pacific AOD staff from 13 services registered with the ALAC National Directory of Alcohol and Drug Services for Pacific people participated in individual or focus group interviews.
The key findings identified were:
• there is a ‘Pacific’ way of working with Pacific AOD clients
• there are elements of Pacific and Palagi understandings of AOD issues applied in their work
• there is no significant difference between Pacific interventions offered by NGO and DHB providers, but there are differences in resourcing and service structure
• it is important to include family in the treatment process
• an effective alcohol and drug worker is described as being Pacific, understanding AOD issues, knowing the Pacific culture and having the skills to integrate this knowledge.
PHASE IIPhase II involved gathering information from client and family perspectives on the effectiveness of treatment interventions provided by the identified services; and gathering information from managers or team leaders about service delivery, practices and assessment and treatment interventions being offered to Pacific clients, and also on workforce development issues.
An exploration into Service Delivery and Treatment Interventions of Pacific AOD Services in New Zealand

9
Pacific Peoples
Seven clients and five family members were invited to participate in either a focus group or individual interview. Those who participated were ethnically diverse and came from Auckland, Hamilton, Wellington and Christchurch regions. Managers or team leaders from each of the participating services (representing both district health board-based and non-government organisation-based services) were asked to fill out a survey form.
The issues raised in this phase of the study included: (a) being culturally responsive; (b) issues related to young clients; (c) assessment and treatment interventions; (d) family involvement; (e) service users being informed; (f) workforce development; (g) supervision requirements; (h) database issues; (i) outcomes measures; and (j) inter-sectoral collaboration. Four of these areas are addressed below:
PHASE IIIThis phase is currently in progress. The aim of Phase III is to develop and pilot an evaluation framework that will allow Pacific people to measure and evaluate their service provision and responsiveness to the needs of Pacific AOD clients. It specifically aims to provide a tool that can be used to assess a range of service models of care, tools and/or processes used by Pacific providers. Phase III is expected to be completed by early next year.
Figure 1. PADOPT project phases I - III.
An exploration into Service Delivery and Treatment Interventions of Pacific AOD Services in New Zealand Kathleen Samu, Gail Robinson, Helen Warren, Tamasailau
Suaalii-Sauni, Amanda Wheeler, Havila Matangi-Karsten.
PHASE IInterviews with
clinicians
PHASE IIInterviews with
clients and families
PHASE IIIDesigning and
piloting
80
70
60
50
40
30
20
10
0DHB male
NGO male
DHB female
NGO female
Total male
Total female
Per
cent
age
35
30
25
20
15
10
5
0
Per
cent
age
Sam
oan
Tong
an
Coo
k Is
land
Niu
ean
Fijia
n
Toke
laua
n
Tuva
lu
Mao
ri
Pal
agi
Eur
opea
n Eth
opia
n

Helpline Update
10
This November the Alcohol & Drug
Helpline will celebrate the 10th
anniversary of the commencement of the
Helpline as a Canterbury Pilot Project.
In its first week the service received up
to three calls a day. Now, 10 years on,
the Helpline receives 60 to 80 calls a
day, and recent changes to the Helpline
infrastructure and staffing to cope with
increasing call volumes will allow the
Helpline respond to up 120 calls a day.
The Alcohol Helpline, funded by ALAC, began as a national service in February 1996. The Drugline, funded by the Ministry of Health, was launched in 2002 and the service renamed the Alcohol & Drug Helpline. The Helpline is a service provided by the Alcohol Drug Association New Zealand (ADANZ).
The Helpline is a confidential information and referral service for people with questions about their own or someone else’s drinking or drug use. The service is available 12 hours a day, seven days a week.
People who call the Alcohol & Drug Helpline fall into three main groups: those who are concerned about their own drinking or drug use; with concerns about or affected by someone else’s drinking or drug use; and those wanting basic information. This third group includes General Practitioners, alcohol and drug and allied health professionals, and students at secondary and tertiary levels.
Before 2002, the Alcohol Helpline, while responding to drug-related calls, primarily received calls on alcohol, reflecting the extent of alcohol misuse in our community. The shape of alcohol and other drug use in New Zealand has changed in recent years. The lowering of the legal purchase age, increased awareness of risky drinking patterns, the ‘P’ scourge, drugs such as NOS and party pills have resulted in the Helpline increasingly responding to more complex calls, necessitating information development and a broader range of interventions, including referrals to crisis services.
Call volumes have increased steadily from 11,019 (2002) to 12,529 (2003) with a large increase to 17,034 calls in 2004. This year (2005) calls are slightly down and to May 2005 the Helpline has responded to 12,306 calls.
The alcohol-related call volume remained steady at 8000-9000 calls, with the percentage of alcohol calls changing in response to the overall increase in calls. Cannabis-related calls in 2004 comprised 11 percent of all calls, and methamphetamine-related calls comprised 9 percent of calls.
Alcohol & Drug Helpline Update
Helpline Update
11
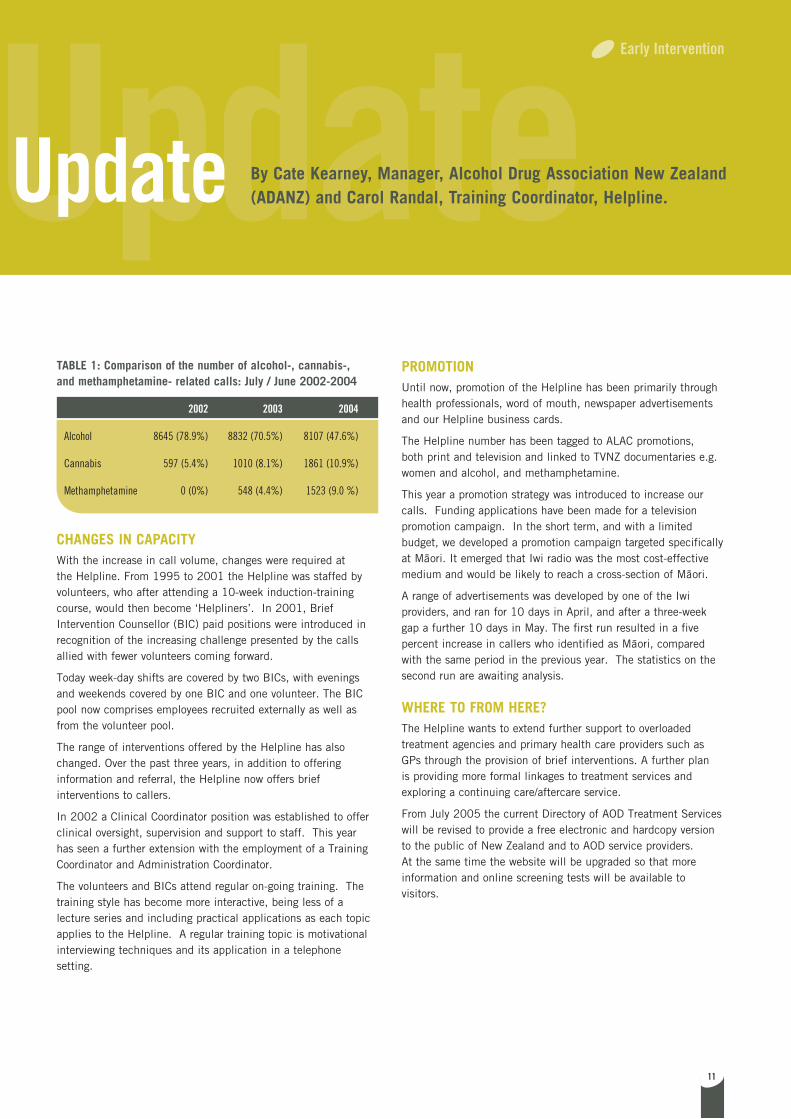
TABLE 1: Comparison of the number of alcohol-, cannabis-, and methamphetamine- related calls: July / June 2002-2004
2002 2003 2004
Alcohol 8645 (78.9%) 8832 (70.5%) 8107 (47.6%)
Cannabis 597 (5.4%) 1010 (8.1%) 1861 (10.9%)
Methamphetamine 0 (0%) 548 (4.4%) 1523 (9.0 %)
CHANGES IN CAPACITYWith the increase in call volume, changes were required at the Helpline. From 1995 to 2001 the Helpline was staffed by volunteers, who after attending a 10-week induction-training course, would then become ‘Helpliners’. In 2001, Brief Intervention Counsellor (BIC) paid positions were introduced in recognition of the increasing challenge presented by the calls allied with fewer volunteers coming forward.
Today week-day shifts are covered by two BICs, with evenings and weekends covered by one BIC and one volunteer. The BIC pool now comprises employees recruited externally as well as from the volunteer pool.
The range of interventions offered by the Helpline has also changed. Over the past three years, in addition to offering information and referral, the Helpline now offers brief interventions to callers.
In 2002 a Clinical Coordinator position was established to offer clinical oversight, supervision and support to staff. This year has seen a further extension with the employment of a Training Coordinator and Administration Coordinator.
The volunteers and BICs attend regular on-going training. The training style has become more interactive, being less of a lecture series and including practical applications as each topic applies to the Helpline. A regular training topic is motivational interviewing techniques and its application in a telephone setting.
PROMOTIONUntil now, promotion of the Helpline has been primarily through health professionals, word of mouth, newspaper advertisements and our Helpline business cards.
The Helpline number has been tagged to ALAC promotions, both print and television and linked to TVNZ documentaries e.g. women and alcohol, and methamphetamine.
This year a promotion strategy was introduced to increase our calls. Funding applications have been made for a television promotion campaign. In the short term, and with a limited budget, we developed a promotion campaign targeted specifically at Maori. It emerged that Iwi radio was the most cost-effective medium and would be likely to reach a cross-section of Maori.
A range of advertisements was developed by one of the Iwi providers, and ran for 10 days in April, and after a three-week gap a further 10 days in May. The first run resulted in a five percent increase in callers who identified as Maori, compared with the same period in the previous year. The statistics on the second run are awaiting analysis.
WHERE TO FROM HERE?The Helpline wants to extend further support to overloaded treatment agencies and primary health care providers such as GPs through the provision of brief interventions. A further plan is providing more formal linkages to treatment services and exploring a continuing care/aftercare service.
From July 2005 the current Directory of AOD Treatment Services will be revised to provide a free electronic and hardcopy version to the public of New Zealand and to AOD service providers. At the same time the website will be upgraded so that more information and online screening tests will be available to visitors.
Early Intervention
Alcohol & Drug Helpline Update By Cate Kearney, Manager, Alcohol Drug Association New Zealand (ADANZ) and Carol Randal, Training Coordinator, Helpline.

12

13
A resource to help make
parents aware of the
consequences of supplying
alcohol to young people
has been developed by
ALAC for the country’s
Youth Access to Alcohol
(YATA) groups.
The YATA groups are a
community action project
supported by ALAC, which
aims to reduce the illegal
and/or irresponsible supply
of alcohol by adults to
young people.
“This new resource is really an extension of the ‘Think Before you Supply to Under 18s’ campaign already run by many YATA groups,” says ALAC Project Manager Community Action, Sam Clark.
“That campaign was developed to raise awareness around the issues of supplying alcohol to minors and it targets the general public and, in particular, retailers of alcohol.
“What the YATA groups were telling us was they wanted some kind of resource to address the issue of parental supply of alcohol to teenagers.
“The THINK …CONSEQUENCES resource is a series of radio and print advertisements designed to draw the attention of parents to the possible harmful consequences of supplying alcohol and their responsibilities to their children.”
The resource consists of a series of templates of three press advertisements and three radio advertisements. Templates were designed in response to the request of YATA teams.
The advertisements are designed to be used in conjunction with and to strengthen other YATA strategies such as parent forums, public meetings and controlled purchase operations as well as during the after-ball and Christmas party seasons.
They feature the consequences of supplying large amounts of alcohol to under 18s.
One titled ‘His Dad Put Him Here’ shows a youth whose father supplied him with a bottle of rum to take to a party who was arrested after getting into a fight. Another titled ‘His Mum Did This’ shows a youth knocked unconscious after getting into a fight. His mother had supplied him with a dozen beers to take to town.
Sam says many of the YATA communities told ALAC that parents have been the most difficult audience to reach. They also said that when they talked with parents they found that parents felt very disempowered about this issue and they often don’t know the laws surrounding the supply of alcohol to teens.
“Parents also say they have difficulties setting boundaries with their children. They are unsure of what other parents are doing with regard to the supply of alcohol to teens and are exposed to constant pressure by their teens.”
YATA communities are being encouraged to contact their local radio stations to play the radio advertisements. The press advertisements are intended for newspapers but can also be used to develop other print resources such as flyers, posters, billboards etc.
The templates have been designed so that communities can add their own logo to the advertisements. It is essential that a logo is added to ensure that the public is aware of whom to contact locally should they want to comment on the advertisements.
Young people
Think… CONSEQUENCES
Project Walk ThroughThe project was a joint initiative involving Counties/Manukau Police, the Manukau City Council, Accident Compensation Corporation and ALAC and involved the Maori wardens in Mangere East checking licensed premises for a number of compliance issues particularly in relation to intoxication and the presence of minors.
The Maori Wardens are legislated under the Maori Community Development Act 1963 to monitor licensed premises but there has been limited activity around New Zealand of Maori Wardens utilizing their powers Act to monitor licensed premises, says New Zealand Police Counties Manukau District Iwi Liaison Officer and project steering committee member Maryanne Rapata.
“There was a similar project in Rotorua several years ago and the Mangere group, with the support of the Rotorua wardens, took this model and further developed it.”
Maryanne says aim of the project was to reduce alcohol-related harm and to build the capacity and capability of Maori Wardens to utilize their powers.
“The visible presence of a group monitoring compliance with the Act and the identification and on-reporting of problem premises reduces the potential risk of alcohol-related harm occurring
Project Walk Through
14
ALAC has been contracted by Te Puni Kokiri to expand on a
recent project utilising the powers of the Maori Wardens.
Project Walk Through involved using the Mangere East
Maori Wardens and their existing powers under the Maori
Community Development Act, to monitor licensed premises
for compliance with the Sale of Liquor Act.

Project Walk ThroughProject Walk Through
15
Supply and Provision
with, from and around licensed premises. And the training the wardens received provided them with the information, resources and skills to support their existing activities.”
The overall goal of this project is Maryanne says the primary focus of the Mangere project (and where it differed from the Rotorua project) was its emphasis on observation and reporting rather than direct action.
The project ran from December 2004 to February 2005 with the all women team of Maori wardens visiting licensed premises on Thursday and Saturday nights, initially between the hours of 8pm and 2am. They reported any improprieties to the Duty Manager and any breaches of the Act to the District Licensing Agency and the police.
“As well as checking for intoxication and the presence of minors, the wardens reported on a range of other safety issues such as Host Responsibility practices and whether door staff were checking identification.”
Prior to the implementation of the project, the wardens undertook a training programme through the Manukau Institute of Technology. Wardens received training on Host Responsibility, central government legislation, occupational
safety and health for volunteers, police training packages and received information on council bylaws, policies and contracts. Wardens could qualify for New Zealand Qualification Authority credits to gain their general manager’s licence.
Maryanne says the wardens monitored both on and off licences and sports clubs within the Mangere ward. They also monitored compliance with liquor bans in the Mangere town centre area.
Licensed premises were asked to fill in a perception survey before and after the project began
Reports were written for every licensed property that the wardens check. The DLA served three suspension letters for sellers given on the information obtained by the wardens.
“The types of issues they faced included young kids left in cars outside pubs, fighting, people urinating in public spaces, dairies selling alcohol and under age drinking,” says Maryanne.
Maryanne emphasises the project was not about intervention, but about checking for safety, like walking into a pub and checking for alcohol signs, then monitoring and passing the information on to the right organisation. “In effect, the wardens are the ‘eyes and ears’ of the
Council and the police providing these agencies with information that is used for further monitoring of the Sale of Liquor Act.”
ALAC has now been contracted by Te Puni Kokiri to facilitate the development of a training package that could be used by other wardens who may wish to use the model in their own area.
ALAC is currently working with the Maori Wardens Association to assess the capability/capacity issues of utilising the powers of the wardens to address alcohol-related harm. ALAC has also agreed to work with other agencies to look at the long-term sustainability for Mangere and similar projects. Maryanne has been seconded from the police to ALAC for three days a week to work on the project.

Controlled PurchaseControlled Purchase Operations
16
The issue of whether teenage volunteers
used in controlled purchase operations
(CPOs) should lie about their age is to go
before the High Court.
The police are appealing a recent Liquor
Licensing Authority (LLA) decision where
the authority turned down an application
to suspend the licence of an outlet caught
selling alcohol to a minor because the
volunteer lied about her age.
CPOs are planned operations designed to monitor and enforce the provisions relating to the sale of liquor to minors in the Sale of Liquor Act 1989 (SOLA). They involve supervised volunteers aged under 18 attempting to buy alcohol from licensed premises, particularly off-licence premises such as supermarkets, bottle stores and grocery stores. Should a volunteer’s purchase prove successful, the premises’ operator, manager or licensee is liable to prosecution or other sanction via the LLA or the District Court. CPOs can also be used as an educative tool for retailers and their staff and for the wider community.
The appeal, which will go before the High Court in September, follows a CPO carried out in Taupo last year where a volunteer aged 17 years and five months attempted to buy alcohol. The volunteer was asked if she was over 25 to which she replied ‘of course’.
In its ruling the authority said it believed the licensed premises was in breach of the Act. The issue for it to consider was whether it was desirable to make a suspension order. The main question to be considered was the instruction to the volunteer to lie about her age.
“There are many who argue that deception is precisely the way that youngsters go about acquiring liquor illegally, and that therefore a test where the volunteer lies about his or her age, is a fair test. Indeed in June 2004, the Alcohol Advisory Council of New Zealand (ALAC) produced a comprehensive set of Controlled Purchase Operation Guidelines. The booklet recognised that "CPOs" can be used as an educative tool for retailers and their staff and the wider community. The guidelines recommend that requesting the volunteers to falsely state their ages was the preferred option because it was a superior and more realistic test of compliance as it then "requires retailers to meet the statutory standard of sighting an evidence of age document”. In passing we note that there is no requirement to sight an evidence of age document. To do so provides a “safe harbour” defence for the seller.
“If the reason for the controlled purchase operation is to test, educate, and even deter licensees, and obtain sanctions against the salespersons, then we would be prepared to accept such a proposition as stated above. However, in our view the
Controlled PurchaseControlled Purchase Operations
17
Supply and Provision
position becomes much more debateable when the licence can be suspended because of the actions of an employee. We have consistently taken the view that any suspensions of off-licences in respect of incidents where a volunteer encourages any sale by deception would not be desirable. We think that any suspension of the off-licence in such circumstances would be counter-productive to the establishment and maintenance of the reasonable system of control over the sale and supply of liquor to the public as set out in s.4 of the Act.”
The authority went out on to ask “If a policy of deception becomes acceptable nationally, then the question must be asked, what other types of behaviour will be used to encourage the illegal sale? May we then expect the production of false identification documents, and other forms of misleading conduct?
“We have consistently taken the view that the only way that standards will be raised in the industry, is if examples are made when the law is breached. We have no difficulty in suspending licences where salespersons are negligent, and the playing field is reasonably level. However, where the odds are consciously altered in favour of the purchaser, as in this case, we would like to send out a clear message. Until the High Court tells us otherwise, it is unlikely that any order against the licensee will follow. “
This approach was followed in a recent case in Auckland where the LLA suspended the off-licences of three Auckland outlets after they were found to have sold liquor to minors. The authority also suspended the certificates for five general managers.
A fourth off-licence escaped suspension because the authority said it did consider it desirable to suspend a licence where the breach of the Act resulted from the actions of an employee, and the volunteer has been untruthful. In its decision the authority said;
“Any concerns about whether the volunteer is untruthful do not apply to the holders of General Manager’s Certificates. They have the ability to request identification, and make an assessment of the age of the purchaser. They have been given the 'evidence of age' tools to test any age claim. In particular a certificated manager has the advantage of training. Finally,
he or she carries the responsibility under s.115 of the Act of complying with the Act, and the conditions of the licence. The buck literally stops with them. To add a further cliché, they are the front line in the campaign to reduce liquor abuse. If the holders of General Manager’s Certificates cannot live up to the standards expected of them, then it would be almost impossible to expect bar persons, checkout operators, and other salespersons to be vigilant.”
ALAC Deputy Chief Executive Officer Sandra Kirby said the ALAC CPO guidelines addressed the question of what a volunteer should say if asked ‘You’re 18 aren’t?’
“The guidelines suggest volunteers should say they are over 18. This is because the CPO should mimic a normal situation as much as possible and, any minor attempting to buy alcohol, when asked if they are over 18, would of course say yes.”
The admissibility of the evidence when volunteers give a false age has been supported by the High Court. However, the High Court has not ruled on whether it is desirable to make orders for suspension or cancellation following findings based on such evidence, she said.
“What has been highlighted in both the Taupo and Auckland CPO is the distinction between a manager/ licensee and an employee of the licensee. The LLA says that a manager has the position to make an assessment of the age of a purchaser because they have the benefit of training and have been given the 'evidence of age tools' to test any age claim. They carry the responsibility under section 115 to comply with the Act and the conditions of the license.
“We continue to stand by the CPO guidelines that were written in response to community's requests last year. The guidelines are just that "guidelines" and every case is different and the guidelines are constantly being reviewed to reflect changes.
“We would still encourage agencies to support volunteers to state their age falsely to act like the majority of teenagers and also to maintain standards within the industry but await with interest to see the High Court decision.”

18
Sandra KirbySandra Kirby has been appointed ALAC’s new Deputy Chief Executive Officer. She replaces Paula Snowden, who has moved on to the New Zealand Housing Corporation.
Sandra is a familiar face at ALAC. A trained teacher who has worked in the health sector since 1989, Sandra joined ALAC in 1997 as Manager Southern Region based in Christchurch. She moved back to Wellington in 2002 to become ALAC Manager Supply and Provision and later Group Manager Population Strategies.
Sandra says she is passionate about ALAC’s work. “I have worked at the operational level at ALAC for the last seven to eight years and I relish the opportunity to continue the work more at the development end and support others to do the delivery.
“One of the roles I see for myself is furthering the ambitious cultural change programme aimed at changing New Zealand’s risky drinking culture.”
Sandra has been closely involved in the development of the programme and says the success of the programme will be determined by “how much traction we get. We are in it for the long haul.”
Sandra says some have dismissed ALAC’s culture change programme as just an advertising campaign.
“This is a short-sighted and blinkered approach to the programme.
“What we have likened the programme to is the efforts to curb drink/driving and smoking where enforcement and
other structural change are at least as significant as the advertising component of the programme.
“What differs between the ALAC campaign and those campaigns is that ALAC is not delivering all parts of the programme. We have partnerships with a variety of groups from police, to government agencies and non-government agencies, who are all delivering parts of the package.”
Oriana ChinOriana Chin is ALAC’s new Reference Librarian. Oriana comes to ALAC with a wealth of experience in reference work and collection development across the sectors of health, finance, labour, social welfare and economics. She has worked both in New Zealand and overseas.
Oriana says she was attracted to ALAC because it’s a smaller organisation than many of the places she has worked before. “This allows a greater opportunity to work closely with staff and provides a clear strategic focus.”
Oriana is the first port of call with any requests for information on alcohol, library items, or ALAC resources. Her role encompasses answering queries from A&D workers, health promoters, licensees, researchers, students, members of the public, government agencies and ALAC staff. She is responsible for ensuring the ALAC Library collection meets the needs of our audiences’ requirements.
Te Rina MokeTe Rina is the latest member to join ALAC’s Maori whanau team.
She was born and raised in Porirua and is of Te Rarawa, Waikato/Maniapoto, Ngati Toa and Ngai Tahu descent.
Her previous role was Resource Development and Community Liaison Coordinator for Suicide Prevention Information New Zealand (SPINZ) based in Auckland.
Prior to that Te Rina worked for two years as a youth coordinator and team leader with Whakatohea Iwi Social and Health Services in Opotiki and one year as the SKIP (Safer Kawerau Kids Injury Prevention Coordinator), based in Kawerau.
Te Rina says she has experience working in rural and Maori communities in mental health promotion, Maori health promotion, Maori youth suicide prevention and injury prevention.
“I have been away for the past four to five years and I am excited about returning to Wellington and my new role as Kaiwhakarite with ALAC.”
Te Rina has a six-year-old son, Kahura Moke.
Alcohol and Other Drugs Treatment Leadership ProjectPeter Barnett has just been appointed Project Manager for a new joint project between the Mental Health Commission (MHC) and ALAC. The project will facilitate leadership and provide advice on alcohol and drug treatment to both agencies and to the mental health and drug treatment fields. Peter will be located at the Commission, but ALAC and MHC will manage the project jointly.
Staff UpdateStaff Update

19
Peter is originally from Dunedin but has recently arrived back in New Zealand after a rather longer than usual OE of 25 years in London. He brings with him extensive experience of managing and commissioning substance misuse services, and also of high-level involvement in national, regional and local strategic/policy development and implementation in England.
He was involved as an expert advisor in the United Kingdom Government/Cabinet Office Strategy Unit project to research and develop the first Alcohol Harm Reduction Strategy for England and was a member of Alcohol Concern’s Commission on the Future of Alcohol Services. His latest job in London was setting up and developing the new post of Drug and Alcohol Action Team (DAAT) Young People’s Coordinator in Lambeth, a high-need, multi-racial/multi cultural inner city borough, and prior to that he managed a large and highly successful drugs and alcohol NGO with a range of adult and young people’s treatment/intervention services.
Tuari PotikiTuari Potiki is ALAC’s new project manager Southern region.
Tuari is of Kai Tahu, Kati Mamoe and Waitaha descent. He is no stranger to
ALAC having been seconded to ALAC from Healthlink South in 2000 2001 as Maori Development Co-ordinator involved in ALAC’s Manaaki Tangata programme and co-ordinating a series of regional hui round the country.
Tuari has a strong background in the alcohol and drug sector. He served as manager of the Taha Maori Programme at Queen Mary Hospital in Hamner from 1994 to 1997. As Kaiwhakahaere for Healthlink South, he was responsible for the development of services for Maori and Pacific clients.
He has also worked in the academic world as tutor and lecturer for the Central Institute of Technology and the Christchurch and Dunedin campuses of the University of Otago. Tuari was also a kaiako for Te Ngaru Learning Systems delivering Kaupapa Maori training courses throughout Te Waipounamu.
Just prior to joining ALAC, Tuari was a member of the senior management team at Ngai Tahu Development Corporation and managed social development and Runanga development sectors for the corporation.
Tuari says he was attracted to ALAC because he wanted to get back into the field. “I wanted to get my feet back on the ground. I was at Ngai Tahu for four years in more of a strategic development role.
“This position has a good mixture of high level strategic and policy work plus networking and relationship building.”
Tuari is married with four children. He is based in ALAC’s Christchurch office.
Marlane Welsh-MorrisMarlane Welsh-Morris is ALAC's new Group Manager Community Strategies
Ko Tokatoka te MaungaKo te Wairoa te AwaKo te Uri o Hau te HapuKo Ngati Whaatua te Iwi
Ko Hikurangi te MaungaKo Waiapu te AwaKo te Whanau a Ruataupare te HapuKo Ngati Porou te IwiKo Marlane Welsh-Morris
E nga mana, E nga reo, E nga Iwi huri noa te motuTena koutou katoa
It is with great anticipation I join the ALAC team. I have come from a
professional background in the social services sector. I have been a social worker and supervisor, trainer, bicultural policy advisor and a forensic Interviewer of children who had been seriously abused. Most recently as the Team Leader of Public Education for Child, Youth and Family, I led the development and implementation of Everyday Communities, a programme that engages the community to prevent child abuse, neglect and family violence.
I understand that the people working in the ALAC team are passionate and committed to reducing harm from alcohol in our communities. Recently a young person in the Wairarapa -Reihana Rimene-Mclean said ‘Werohia te taniwha’ in relation to preventing the abuse of children. I believe his korero resonates for alcohol as well.
I have two awesome daughters Te Aroha (15 years) and Julia (13 years) and a wonderful whanau who nourish my spirit and passion to serve the people.
I look forward to working with you all.
Staff
Staff UpdateStaff Update
ALAC now boasts a full
complement of Information
Services staff. With
three full- time staff, the
team has a collective
experience of 55 years
in the information
management field.
The team is made up of
Oriana Chin, Reference
Librarian; Susan McBride
System Librarian; and
Annette Beattie Manager
Information Services.
How does Information Services make my job easier?ALAC is the place to find information on alcohol in New Zealand. The library is home to a core collection of alcohol-related texts, journals and videos. Some are unique to ALAC’s library. In the coming year, the focus will be on updating the heavily used video collection.
The library collection is used extensively by alcohol and other drug workers, health
promoters, researchers and government agencies. The collection is accessible via the www.alac.org.nz website (http://www.alac.org.nz/LibraryCatalogue.aspx), and items can be borrowed from it.
How do I borrow something from ALAC’s Library?In keeping with standard library practice, ALAC operates a policy of inter-library lending. If you wish to borrow any of the library collection items, simply let your own organisation or public library know, and they will arrange for them to be sent. Inter-library loans ensure that library items are the responsibility of the borrowing library, rather than the individual. Interloaning also helps in making sure that precious items stay available to all borrowers.
ALAC recognises that throughout New Zealand there a number of independent alcohol and other drug workers for whom access to an organisation or public library is not always an option. For those few, we provide the option of signing up as a direct borrower.
To borrow from the Library collection or to find out if ALAC has useful items on a particular topic contact Oriana at [email protected]
If you are an alcohol and other drug worker having a hui seminar or training day and would like this to be promoted on the ALAC web site please email [email protected] or [email protected] with the details. This community news section of the website receives around 350 hits a month so it is a great way to promote your event.
information@alac
20
RESOURCES

Two electronic mailing lists have been set up to enable individuals to communicate via email with other alcohol and drug professionals in New Zealand.
You can either subscribe to a general mailing list or register to connect to a network of M≠ori alcohol and drug workers.
Electronic mailing lists for the alcohol and drug field
REGIONAL OFFICES
AUCKLAND 09 916 0330 [email protected] CHRISTCHURCH 03 365 8540 [email protected] WELLINGTON 04 917 0060 [email protected] CALL FREE 0508 258 258
SUBSCRIBE NOWSUBSCRIBE NOW
Contact other alcohol and drug professionals:
1. If you have access to the web, subscribe by going to http://lists.iconz.co.nz/mailman/listinfo/aandd
You will find a form to fill out. You will need to choose a password.
2. If you don’t have access to the web, send an email message to [email protected] leaving the subject line blank.
In the body of the message type: Subscribe ***** (where ***** is an alphanumeric
password of your choice between 4 and 8 characters).
If you have any problems with the above, or for further information, please contact Susan McBride.
Email: [email protected]
Phone: 04 917 0060
Join a network of Maori alcohol and drug workers:
1. If you have access to the web, subscribe by going to http://lists.iconz.co.nz/mailman/listinfo/te_kupenga_hauora
You will find a form to fill out. You will need to choose a password.
2. If you don’t have access to the web, send an email message to [email protected]
Phone: 04 917 0060


















