Breast Cancer Yield after Short Interval Follow-up Compared to Return to Routine Annual Screen in Patients with Benign Stereotactic or Ultrasound-guided Biopsy Results
25
Breast Cancer Yield a/er Short Interval FollowUp Compared to Return to Rou=ne Annual Screen in Pa=ents with Benign Stereotac=c or Ultrasound Guided Biopsy Results JM Johnson, MD; AK Johnson, MD; ES O'Meara, PhD; D Migliore8, PhD; BM Geller, EdD; P Frawley, SD Herschorn, MD; EN Hotaling, MD RSNA 96 th Scientific Assembly & Annual Meeting, November 28 – December 3, Chicago, IL.
Transcript
Breast Cancer Yield a/er Short-‐Interval Follow-‐Up Compared to
Return to Rou=ne Annual Screen in Pa=ents with Benign Stereotac=c or Ultrasound Guided Biopsy Results JM Johnson, MD; AK Johnson, MD; ES O'Meara,
PhD; D Migliore8, PhD; BM Geller, EdD; P Frawley, SD Herschorn, MD; EN Hotaling, MD
RSNA 96th Scientific Assembly & Annual Meeting, November 28 – December 3, Chicago, IL.
Disclosures
• No contributors have any relevant disclosures.
Background
• Biopsy of breast lesions is increasingly being performed using ultrasound and stereotacKc guidance.
• Exact # of percutaneous breast biopsies performed annually in the US is unknown, esKmates range 500,000 -‐ 1,000,000.
• # of percutaneous breast biopsies performed in the US conKnues to increase; only 20 -‐ 33% of these biopsy samples prove to be cancer.
Accuracy
• Percutaneous breast biopsy has been shown to be a highly accurate procedure.
• With stereotac=c biopsies, reports of false-‐negaKve rates range from 2.9 –7.8%.
• With ultrasound guided core needle biopsy, reports of false-‐negaKve rates range from 0 -‐ 1.7%.
Concordance
• ConfirmaKon of lesion retrieval aYer biopsy is essenKal and can be confirmed by specimen radiography, post biopsy mammography and by correlaKon of histologic findings with imaging characterisKcs.
• Imaging–histologic discordance aYer breast biopsy occurs when histologic findings do not provide a sufficient explanaKon for imaging features.
• Imaging–histologic discordance at stereotacKc or ultrasound guided biopsy is an indica=on for re-‐biopsy.
Biopsy Follow-‐Up
• Li^le evidence to guide how to follow-‐up paKents with benign biopsies.
• Many centers recommend return for a six-‐month follow-‐up unilateral mammogram or ultrasound to ensure that there has been no change at the biopsy site.
• Other centers perform a four-‐month follow-‐up and others return paKents to annual screening.
Mo Screening ≠ Mo Be^er
• Using conservaKve esKmates, as many as 330,000 women annually receive a breast biopsy with benign pathology result.
• SIFU leads to increase healthcare uKlizaKon and increased paKent anxiety.
• There are adverse psychological and immunological impacts of biopsy that persist beyond the biopsy.
• The effects may be prolonged with the addiKon of short-‐term follow-‐up.
Purpose
• Our goal was to compare the cancer detecKon rate and nodal status, stage and tumor size following a benign stereotacKc or ultrasound guided breast biopsy between paKents with SIFU and RTAS.
DefiniKons
• SIFU and RTAS defined based on observed Kme since biopsy, not just radiologist recommendaKon or indicaKon.
• "SIFU" defined as (a) imaging 3-‐9 months aYer biopsy with (b) indicaKon "rouKne screening" or "short-‐interval follow-‐up".
• "RTAS" defined as (a) imaging 9-‐18 months aYer biopsy with (b) indicaKon "rouKne screening" or "short-‐interval follow-‐up".
Rules
• Cases with findings of atypical hyperplasia or lobular carcinoma in situ were excluded.
• If any cancer diagnosis was found to precede the benign biopsy or occurred within the following 90 days, the biopsy was excluded.
• We required 3 months of follow-‐up for cancer detecKon at post-‐biopsy imaging.
• We examined biopsies that resulted from both screening and diagnosKc evaluaKons.
Rules 2 • Only core biopsies with ultrasound or stereotacKc guidance were evaluated.
• Any cases in which there was a repeat biopsy within 3 months or before follow-‐up imaging were excluded due to the likelihood of represenKng discordant radiology-‐pathology results.
• Diagnosis of ipsilateral invasive cancer or DCIS within 3 months of the 1st follow-‐up imaging exam and tumor characterisKcs were determined through linkage with pathology databases and tumor registries.
Methods
Results
• Total of 19,598 benign biopsies among 18,367 women were idenKfied. – Post-‐biopsy imaging
• SIFU 7397 • RTAS 3604 • Other 8597
Demographics SIFU (N = 7397) RTAS (N = 3604)
CharacterisKc % %
Age
<40 6 5.5
40-‐49 34 35.3
50-‐59 31.8 31.7
60-‐69 16.6 16
70-‐79 9.3 9
≥80 2.3 2.5
Race/ethnicity
White, non-‐hispanic 90.5 89
Black, non-‐hispanic 3.6 4.1
Asian/Pacific Islander 2 2.7
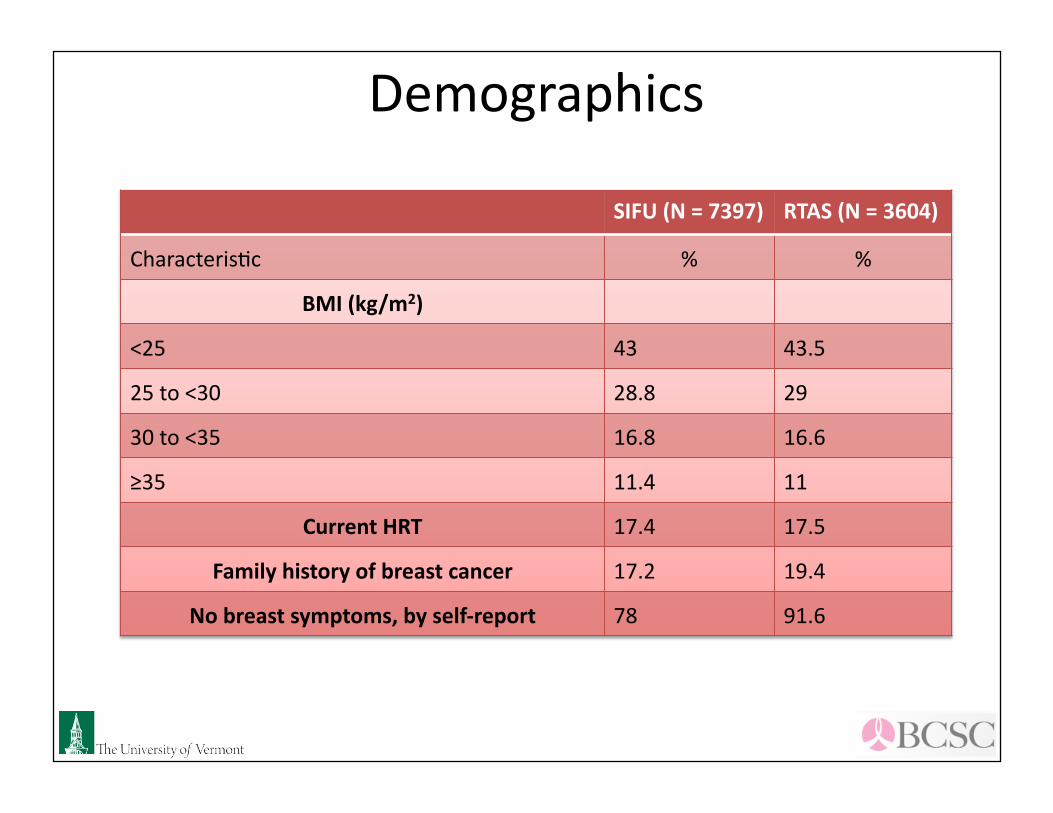
Demographics
SIFU (N = 7397) RTAS (N = 3604)
CharacterisKc % %
BMI (kg/m2)
<25 43 43.5
25 to <30 28.8 29
30 to <35 16.8 16.6
≥35 11.4 11
Current HRT 17.4 17.5
Family history of breast cancer 17.2 19.4
No breast symptoms, by self-‐report 78 91.6
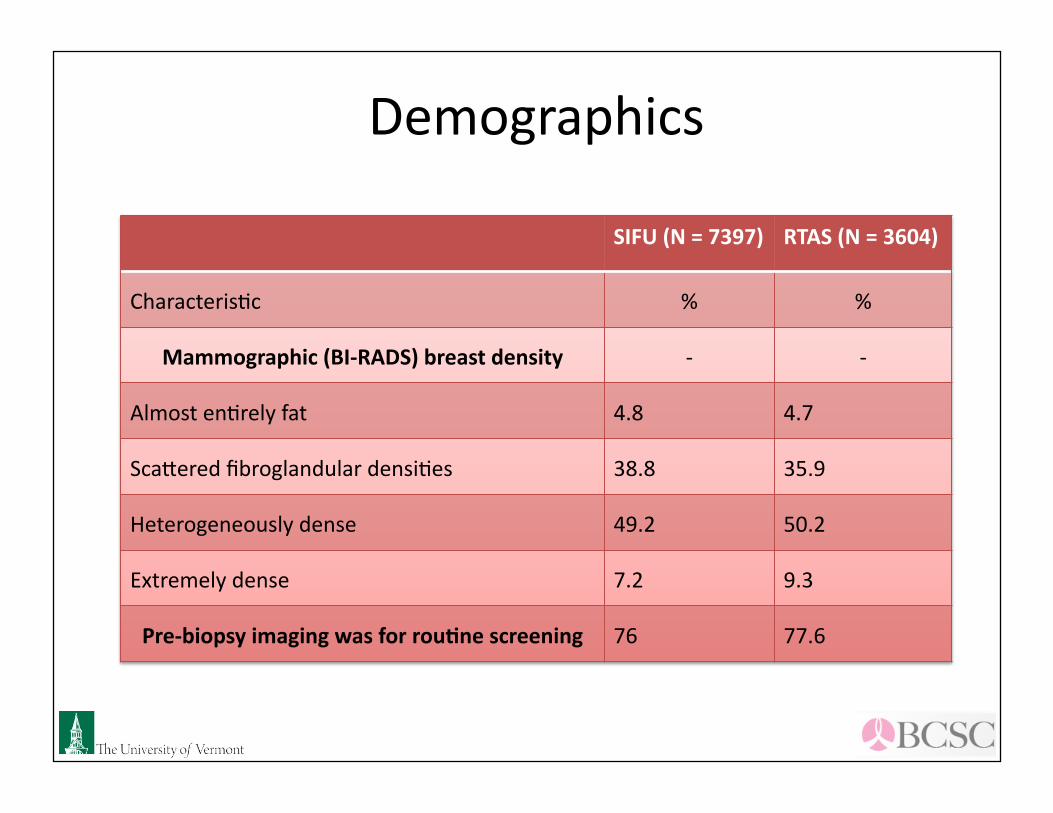
Demographics
SIFU (N = 7397) RTAS (N = 3604)
CharacterisKc % %
Mammographic (BI-‐RADS) breast density -‐ -‐
Almost enKrely fat 4.8 4.7
Sca^ered fibroglandular densiKes 38.8 35.9
Heterogeneously dense 49.2 50.2
Extremely dense 7.2 9.3
Pre-‐biopsy imaging was for rou=ne screening 76 77.6
Breast Cancer w/in 3 months aYer post-‐biopsy imaging
SIFU RTAS
N benign biopsies 7397 3604
Incident ipsilateral breast cancer cases diagnoses w/in 3 months a/er post-‐biopsy imaging, N
Breast Cancer w/in 3 months aYer post-‐biopsy imaging
SIFU RTAS
Among invasive cancers
Node posi=ve (non missing), N 7 (23) 3 (10)
Percent (95% CI) 30% (13%, 53%) 30% (7%, 76%)
Late stage (III or IV) (non missing), N 4 (22) 3 (10)
Percent (95% CI) 18% (5%, 40%) 30% (7%, 65%)
Large size (≥20 mm) (non missing), N 4 (22) 3 (11)
Percent (95% CI) 18% (5%, 40%) 27% (6%, 61%)
Conclusion
• Our results do not show a staKsKcally significant difference in the rate of ipsilateral cancer detecKon between SIFU and RTAS following a benign breast biopsy.
• Rates of invasive cancer and posiKve nodal status also did not achieve staKsKcal significance between the groups.
Conclusion 2
• Having a benign breast biopsy is a posiKve risk factor for breast cancer (Breast Cancer Risk Assessment Tool and Gail Model).
• Despite the posiKve relaKve risk factor associated with a biopsy, the ideal method of follow-‐up for women with benign concordant breast biopsies has not been studied.
• Our results suggest that the pracKce of SIFU following a benign biopsy may not offer significant advantage over RTAS considering the cost and Kme involved.
Strengths
• Large sample of both paKents and radiologists which is representaKve of diverse US pracKces.
• To our knowledge, this is the first study to assess the outcome differences between SIFU and RTAS following a benign concordant breast biopsy.
• PaKent, radiologic, and cancer data within the BCSC provides an opportunity to examine follow-‐up outcomes in a large data set collected in a common format.
Weaknesses
• Small # of cancers detected precludes sub-‐groups analysis for difference in outcome between groups (i.e., older versus younger, white versus non-‐white, HRT vs. no HRT, etc.).
• RetrospecKve nature has inherent weaknesses including possibility of incorrectly filed data and missing data points.
• Predominance of White, non-‐Hispanic paKents (~85%) in our data set limits generalizability of our data to non-‐Whites.
Clinical Relevance
• These results suggest that the pracKce of SIFU following a benign biopsy may not offer significant advantage over RTAS considering the cost and Kme involved.
References 1. Kwan S, Bhargavan M, Kerlan R, Sunshine J. Effect of Advanced Imaging Technology on How Biopsies Are Done
and Who Does Them 1. Radiology. 2010. 2. Weaver DL, Vacek PM, Skelly JM, Geller BM. Predicting biopsy outcome after mammography: what is the
likelihood the patient has invasive or in situ breast cancer? Ann Surg Oncol. 2005;12(8):660-73. 3. Crystal P, Koretz M, Shcharynsky S, Makarov V, Strano S. Accuracy of sonographically guided 14-gauge core-
needle biopsy: results of 715 consecutive breast biopsies with at least two-year follow-up of benign lesions. J Clin Ultrasound. 2005;33(2):47-52.
4. Dillon MF, Hill AD, Quinn CM, O'Doherty A, McDermott EW, O'Higgins N. The accuracy of ultrasound, stereotactic, and clinical core biopsies in the diagnosis of breast cancer, with an analysis of false-negative cases. Ann Surg. 2005;242(5):701-7.
5. Parker SH, Jobe WE. Percutaneous breast biopsy. New York City: Raven Press, Ltd., 1993: 76-78. 6. Schueller G, Jaromi S, Ponhold L, et al. US-guided 14-gauge core-needle breast biopsy: results of a validation
study in 1352 cases. Radiology. 2008;248(2):406-13. 7. Parker SH, Lovin JD, Jobe WE, et al. Stereotactic breast biopsy with a biopsy gun. Radiology. 1990;176(3):741-7. 8. Elvecrog EL, Lechner MC, Nelson MT. Nonpalpable breast lesions: correlation of stereotaxic large-core needle
automated large-core biopsies. Radiology. 1991;180(2):403-7. 10. Gisvold JJ, Goellner JR, Grant CS, et al. Breast biopsy: a comparative study of stereotaxically guided core and
excisional techniques. AJR Am J Roentgenol. 1994;162(4):815-20. 11. Dershaw DD, Morris EA, Liberman L, Abramson AF. Nondiagnostic stereotaxic core breast biopsy: results of
rebiopsy. Radiology. 1996;198(2):323-5. 12. Berg WA, Hruban RH, Kumar D, Singh HR, Brem RF, Gatewood OM. Lessons from mammographic-
histopathologic correlation of large-core needle breast biopsy. Radiographics. 1996;16(5):1111-30.
References
13. Liberman L, Drotman M, Morris EA, et al. Imaging-‐histologic discordance at percutaneous breast biopsy. Cancer. 2000;89(12):2538-‐46.
14. Philpo^s LE, Hooley RJ, Lee CH. Comparison of automated versus vacuu m-‐assisted biopsy methods for sonographically guided core biopsy of the breast. AJR Am J Roentgenol. 2003;180(2):347-‐51.
15. Parker SH, Klaus AJ, McWey PJ, et al. Sonographically guided direcKonal vacuum-‐assisted breast biopsy using a handheld device. AJR Am J Roentgenol. 2001;177(2):405-‐8.
16. Philpo^s LE, Shaheen NA, Carter D, Lange RC, Lee CH. Comparison of rebiopsy rates aYer stereotacKc core needle biopsy of the breast with 11-‐gauge vacuum sucKon probe versus 14-‐gauge needle and automaKc gun. AJR Am J Roentgenol. 1999;172(3):683-‐7.
17. Meyer JE, Smith DN, Lester SC, et al. Large-‐needle core biopsy: nonmalignant breast abnormaliKes evaluated with surgical excision or repeat core biopsy. Radiology. 1998;206(3):717-‐20.
18. Liberman L, Dershaw DD, Glassman JR, et al. Analysis of cancers not diagnosed at stereotacKc core breast biopsy. Radiology. 1997;203(1):151-‐7.
19. Gail MH, Brinton LA, Byar DP, et al. ProjecKng individualized probabiliKes of developing breast cancer for white females who are being examined annually. J Natl Cancer Inst. 1989;81(24):1879-‐86.
20. Decarli A, Calza S, Masala G, Specchia C, Palli D, Gail MH. Gail model for predicKon of absolute risk of invasive breast cancer: independent evaluaKon in the Florence-‐European ProspecKve InvesKgaKon Into Cancer and NutriKon cohort. J Natl Cancer Inst. 2006;98(23):1686-‐93.
21. Bre^ J, Austoker J, Ong G. Do women who undergo further invesKgaKon for breast screening suffer adverse psychological consequences? A mulK-‐centre follow-‐up study comparing different breast screening result groups five months aYer their last breast screening appointment. J Public Health Med. 1998;20(4):396-‐403.
22. Witek-‐Janusek L, Gabram S, Mathews HL. Psychologic stress, reduced NK cell acKvity, and cytokine dysregulaKon in women experiencing diagnosKc breast biopsy. Psychoneuroendocrinology. 2007;32(1):22-‐35.