POCKET TOOL EMERGENCY 2nd edition Health Emergency Management Staff Depart of Health Manila, Philippines * * HE P T F H O IL C I IP L P B I N U P E E S R D H E T P L A A R E T H M F E O N T World Health Organization Western Pacific Region Emergency & Humanitarian Action Health Emergency Management Staff Depart of Health Manila, Philippines * * HE P T F H O IL C I IP L P B I N U P E E S R D H E T P L A A R E T H M F E O N T
Transcript
POCKET
TOOLEMERGENCY
2nd edition
Health Emergency
Management StaffDepart of HealthManila, Philippines
* *
F IL LO UR PE OA PT SS AA TL IBRU
HE PT F HO ILCI IPL PB INUP E
E S
R
D
HE
TP LA AR ET HM FE O NT
World HealthOrganization
Western Pacific Region
Emergency & Humanitarian ActionHealth Emergency
Management StaffDepart of HealthManila, Philippines
* *
F IL LO UR PE OA PT SS AA TL IBRU
HE PT F HO ILCI IPL PB INUP E
E S
R
D
HE
TP LA AR ET HM FE O NT
CO
NTEN
TS
Acknowledgements ....................................................................iiiIntroduction ...............Abbreviations ............Roles and Responsibilities
Coordinating with Other Agencies Drafting the Health Disaster Management Plan
Rapid Health Assessment Critical Incident Management Pre-Hospital Activities ....Hospital Activities Prevention and Control of Communicable Diseases Nutrition Concerns ...Environmental Health ....Water Supply ..........Sanitation and Waste Management Vector and Vermin Control Epidemiology and Surveillance Psychosocial Care and Mental Health Management of Dead Bodies Forensic Science Concerns in Mass Fatalities Resource Management ...Risk Communication
Emergency Manager Deployment Checklist Rapid Health Assessment Forms Reference Values for Rapid Health Assessment and
This pocket tool is a project of the Department of Health-Health Emergency Management Staff (DOH-HEMS), with support from the World Health Organization-Regional Office for the Western Pacific Region (WHO-WPRO).
The review and revision for this second edition was done through the efforts of Dr. Emmanuel S. Prudente, under the technical supervision of Dr. Arturo M. Pesigan of Emergency and Humanitarian Action (EHA) of the WHO-WPRO. Acknowledgement is also given to Dr. Carmencita A. Banatin, Dr. Marilyn V. Go, Dr. Teodoro J. Herbosa, Dr. Josephine H. Hipolito, Ms. Florinda V. Panlilio, Dr. Arnel Z. Rivera, Dr. Edgardo Sarmiento and Dr. Xiangdong Wang, who reviewed the text and provided valuable comments. Lay-out and cover design was done by Mr. Zando Escultura.
The first edition was through the efforts of the following individuals: Engr. Russell Abrams; Dr. Shigeki Asahi ; Dr. Carmencita A. Banatin ; Dr. Agnes B. Beñegas ; Mr. Miguel C. Enriquez ; Mrs. Guia P. Flores ; Dr. Raquel dR. Fortun ; Dr. Camilla A. Habacon ; Dr. Lourdes L. Ignacio ; Mrs. Elizabeth M. Joven; Dr. Susan P. Mercado; Dr. Daniel T. Morales; Dr. Jean-Marc Olivé; Dr. Hitoshi Oshitani; Dr. Arturo M. Pesigan; Dr. Manuel F. Quirino; Dr. Lilia M. Reyes; Dr. Arnel Z. Rivera; Dr. Edgardo Sarmiento; Dr. Enrique A. Tayag; Dr. Yoshihiro Takashima; Dr. Xiangdong Wang; Mrs. Zen Delica Willison; Mr. Robin Willison; and Dr. Ladislao N. Yuchongco, Jr.
AC
KNO
WLED
GEM
ENTS
iii
POCKET EMERGENCY TOOL
Human survival and health are the common objectives and measures of success of all humanitarian endeavors.
The goal of the Department of Health (DOH) through the Health Emergency Management Staff (HEMS) is to prevent or minimize the loss of lives during emergencies and disasters in collaboration with government, business and civil society groups. The main purpose of this pocket tool is to help guide and prepare health sector professionals in the field in the event that an emergency occurs. A compendium of recent DOH, WHO and other international agencies' guidelines, checklists and standards, this booklet provides essential pointers on how to carry out rapid health assessment, networking and coordination, planning, and other necessary tools especially in times of tragedies and adversities.
This pocket tool, however, neither provides nor claims to be the definite and only guideline to follow in emergencies. Thus, references to complementary documents and websites, where more detail can be found, are provided at the end of the booklet. Also, because every disaster is unique, some of the suggested procedures may need to be tailored to local conditions.
ndFurthermore, this pocket tool is an evolving text; this 2 edition was conceived from the lessons learned from the recent disasters that affected the country and the Western Pacific Region. Indeed, the success of this guide depends largely on the dynamics of its use and the tireless efforts of its users to improve it.
INTR
OD
UC
TIO
N
POCKET EMERGENCY TOOL
1
CDC Centers for Disease Control and Prevention (USA)
CHD Center for Health DevelopmentCMR Crude Mortality RateDND Department of National DefenseDOH-HEMS Department of Health-Health Emergency
Management StaffDOTC Department of Transportation and Communication DPWH Department of Public Works and HighwaysDSWD Department of Social Welfare and DevelopmentEHA Emergency and Humanitarian UnitEMS Emergency Medical ServicesEOC Emergency Operations CenterEPI Expanded Program of ImmunizationER Emergency RoomLGU Local Government UnitMUAC Mid-Upper Arm CircumferenceNBI National Bureau of InvestigationNDCC National Disaster Coordinating CouncilNEHK New Emergency Health KitNGO Nongovernmental organizationNNC National Nutrition CouncilNPDEP Nutrition Preparedness in Disasters and
Emergencies PlanOpCen Operation CenterPHC Primary Health CarePNRC Philippine National Red CrossWHO-WPRO World Health Organization-Office for the Western
Pacific Region
ABBREV
IATIO
NS
POCKET EMERGENCY TOOL
2
T.R.A.I.T. of a Health Emergency Manager/Coordinator
T ake the lead within the community in:
! health coordination and networking! rapid health assessment! disease control and prevention! epidemiologic and nutrition surveillance! epidemic preparedness! essential medicines management! physical and psychosocial rehabilitation! health risk communication! forensic concerns and management of mass casualties
R ecord and re-evaluate lessons learned to improve
preparedness in the future
A ssess and monitor health and nutrition needs so that they
are immediately dealt with
I mprove health sector reform and capacity building by
networking
T end and protect the practice of humanitarian access,
neutrality and protection of health systems in emergency situations
ROLE
S A
ND
RES
PON
SIBI
LITI
ES
POCKET EMERGENCY TOOL
3
Roles of Hospitals in Health Emergency Management
1. Observe all requirements and standards (hospital emergency plan, HEICS, Code Alert System, etc.) needed to respond to emergencies and disasters.
2. Ensure enhancement of their facilities to respond to the needs of the communities especially during emergencies.
3. Network with other hospitals in the area to optimize resources and coordinate transferring of victims to the appropriate facility.
4. Report all health emergencies to the Operation Center, and document all incidents responded.
ROLES A
ND
RESPON
SIBILITIES
POCKET EMERGENCY TOOL
4
PREPARING FOR EMERGENCIES
POCKET EMERGENCY TOOL
5
PREPARIN
G FO
R EMERG
ENC
IES
POCKET EMERGENCY TOOL
Steps in Preparing for Emergencies
1. Policy Formulation and Development! policy statement/implementing rules! guidelines, protocols, procedures! organizational structure! roles and functions! resource mobilization
2. Capability Building! training needs assessment! human resource development! training of trainers! database of experts! tabletop drills and exercises
3. Facilities Development! standardization/mprovement/upgrading of ER, ambulance,
Operation Center, hospitals! procurement of supplies, communications and equipment
4. Networking! organization of the health sector! coordination and planning! memorandum of agreement with stakeholders! networking activities
5. Disaster Planning! vulnerability and hazard assessment! all-hazards emergency operations plan! specialized planning for uncommon incidents (e.g. SARS,
6
PREP
ARI
NG
FO
R EM
ERG
ENC
IES
POCKET EMERGENCY TOOL
WMD)! communication plans! hospital preparedness and response plans
6. Public Information and Mass Media! advocacy activities! development of IEC's
7. Post-disaster Response Evaluation! monitoring and evaluation activities! postmortem evaluation
8. Systems Development! Logistics Management System! Management Information System! Communication System
9. Establishment of Emergency Operation Centers! Infrastructure, manpower, technology
10. Documentation and Research! publications! databanking! accomplishment reports! research studies! lessons learned
7
Roles of Centers for Health Development in Emergency Management
1. Serve as the DOH Coordinating Body in their region
2. Manintain updated hazard and vulnerability assessment of their catchment areas
3. Observe all requirements and standards needed to respond to emergencies (Regional Emergency Plan)
4. Organize health sector in the region and provide mechanism for coordination and collaboration. Provide advice to the RDCC for health emergency concerns
5. Maintain operation center as regional repository of vents for the health sector. Identify an official spokesperson to answer concerns by the public and the media
6. Provide technical assistance and empower all LGUs in the area on health emergency management
7. Report to the Central DOH (HEMS) for all emergencies and disasters and any incident with the potential of becoming an emergency
8. Document all health emergency events and conduct researches to support policies and program development.
(Based on DOH Administrative Order 168, s.2004)
PREPARIN
G FO
R EMERG
ENC
IES
POCKET EMERGENCY TOOL
8
At the Center for Health Development (CHD) level…
The following should be readily available
for reference and may be compiled in collaboration with other partners (government and non-government units). These information must be updated regularly:
Disaster profile of the regionPopulation size and distributionTopography and maps showing communication linesEpidemiologic profile of the regionLocation of health facilities and the services they provideLocation of potential evacuation areasLocation of stocks of food, medicine, health and water treatment and other sanitation supplies in government stores, commercial warehouses and international agencies and major NGOsKey people and organizations who would be responsible for/active in relief (contact phone numbers AND addresses)Individuals with special competencies and experience who may be mobilized on secondment from their institutions or as consultants in case of need (contact phone numbers AND addresses)A roster of regular resource persons ready to translate technical information materials into local dialect (i.e., traditional healers, indigenous health workers, barangay captain, etc.)
information
!
!
!
!
!
!
!
!
!
!
PREP
ARI
NG
FO
R EM
ERG
ENC
IES
POCKET EMERGENCY TOOL
9
The following should be readily available for use AT ALL TIMES:
1. Vehicles2. Communications equipment3. Back-up power supplies4. Computers, printers, facsimiles and photocopying machines5. Water testing sets6. Food supplements7. Temporary shelter capacities8. Funding requirements9. Personal protective equipment
resources
PREPARIN
G FO
R EMERG
ENC
IES
POCKET EMERGENCY TOOL
10
Prepare internal arrangements within the DOH and with other public health related government entities, UN agencies, NGOs, and other institutions in the country whose expertise and/or services may be called upon during emergencies (DND, NDCC, DSWD, DPWH, DOTC, PNRC, etc.)
Steps in Establishing Good Working Relationships with Other Groups or Entities
1. Have a common goal.2. Designate a good and strong facilitator.3. Define the parameters of the project. Reach a consensus
on objectives, strategies and plans. 4. Discuss needs and lines of action. 5. Have operating guidelines. 6. Encourage member participation.7. Build trust among members. Fix issues early on.8. Maintain regular communication and correspondence
among members.9. Give priority to the whole group. Each agency is vital.10. Develop clear and attainable mission statements from the
beginning of the project.11. Enlist and maintain the support of top-level-management.12. Educate all members about the range of services each
agency can provide.13. Make partners aware of policies and protocols.14. Adopt responsibilities in the context of what was agreed
upon15. Adjust to changes. Be flexible and be open to possibilities,
unforeseen events and new opportunities.
CO
ORD
INA
TIN
G W
ITH
OTH
ER A
GEN
CIE
S
POCKET EMERGENCY TOOL
11
16. For members to attend, allow adequate incentive.17. Have a product or concrete result showing the team's effort
and share among members so that there is a sense of accomplishment. Celebrate.
Ps of Facilitation:
1. PURPOSE explains the overall aim of the session.! Have ground rules, a clear agenda, and desired
outcomes.
2. PRODUCT describes the session's deliverables in specific outputs.! Discuss needs and lines of action.! Reach a consensus on objectives, strategies, and plans.
3. PARTICIPANTS push the issues. Know their perspectives and concerns. A designated and experienced chairperson should practice facilitative behavior: listening, encouraging participation, not being defensive, asking open-ended questions, and optimistic but realistic
4. PROBABLE ISSUES give an idea of the potential
5
Health coordination must start as soon as possible, it should be regular and frequent. At
the start of a crisis, changes are fast and many. To coordinate is to facilitate.
CO
ORD
INA
TING
WITH
OTH
ER AG
ENC
IES
POCKET EMERGENCY TOOL
12
roadblocks.! Sort issues by categories and types.! Approve the agenda before starting the meeting.
5. PROCESS is the detailed set of steps that will be taken to create the product.! Circulate information among partners.! Preliminary word clarification and definition, brainstorming,
rank order of issues according to importance to the group.! Have group memory by using flip charts or handouts.
Coordination is sharing information with other persons or organizations so they can work
together in harmony without friction or overlapping - based on regular communication
of relevant data.
The resulting consensus should be that everyone feels that he has been heard and that
everyone agrees and is willing to support the decision.
CO
ORD
INA
TIN
G W
ITH
OTH
ER A
GEN
CIE
S
POCKET EMERGENCY TOOL
13
Disaster Reaction Sequence:
! Surprise: Is it true? Has it really happened?! Lack of information: What is happening?! Events escalate: It's getting worse but I don't know ! the details?! Lack of control: I don't know therefore I cannot do.! Siege mentality: Why is this happening to us?! Panic: Will we ever recover from this?! Short term reaction: Get everyone away from me
Common Communication Concerns:
! “I don't have the correct facts.”! “I might upset other people with what I'll say.”! “There might be a better spokesperson.”! “There may be legal implications to what I say.”! “I might risk my reputation.”! “I might be asked something I cannot answer.”! “I might sound stupid.”
If you do not tell, information will be gathered elsewhere, leading to misinformation,
misunderstanding, and their consequences…
CO
ORD
INA
TING
WITH
OTH
ER AG
ENC
IES
POCKET EMERGENCY TOOL
14
You may follow the outline provided below; however, it is not meant to replace alternative outlines that you may deem more appropriate and useful.
I. BackgroundPresent the following:! geographic description ! disasters that have occurred ! gaps in response! hazard maps! vulnerabilities and risks
II. Goals and Objectives
III. Potential Problems Analysis
IV. Resource Analysis
V. Management Structurea. Explain the organization (an accompanying diagram is
essential)b. Specify command, control, lead organization and
coordination
VI. Roles and Responsibilities
VII. Strategies
VIII. Annexes (i.e., glossary, abbreviations, directory of contact persons)
DRA
FTIN
G T
HE
DIS
AST
ER H
EALT
H M
AN
AG
EMEN
T PL
AN
POCKET EMERGENCY TOOL
15
RESPONDINGTO EMERGENCIES
POCKET EMERGENCY TOOL
16
Steps in Responding to Emergencies
Immediate Response: 1. Assess the situation2. Contact key health personnel3. Develop initial health response objectives and establish an
action plan4. Establish communication and maintain close coordination
with the EOC5. Ensure that the site safety and health plan is established,
reviewed, and followed6. Establish communication with other key health and medical
organizations.7. Assign and deploy resources and assets to achieve
established initial health response objectives8. Address health-related requests for assistance and informa-
tion from other agencies, organizations and the public9. Initiate risk communications activities10.Document all response activities
Intermediate Response:1. Verify that health surveillance systems are operational2. Ensure that laboratories likely to be used during the response
are operational and verify their analytical capacity3. Ensure that the needs of special populations (e.g., children,
disabled persons, elderly, etc.) are being addressed4. Manage health-related volunteers and donations
Hours 0-2
Hours 2-12
RESP
ON
DIN
G T
O E
MER
GEN
CIE
S
POCKET EMERGENCY TOOL
17
5. Update emergency risk communication messages6. Collect and analyze data that are becoming available through
health surveillance and laboratory systems7. Periodically assess health resource needs and acquire as
necessary
Extended Response: 1. Address psychosocial and mental health concerns2. Prepare for transition to extended operations or response
disengagement3. Address risks related to the environment4. Continue health surveillance/epidemiologic services5. Ensure that local health systems are preserved and access to
health care, including essential drugs and vaccines, is guaranteed
(Adapted from CDC's Public Health Emergency Response Guide.)
Hours 12-24
RESPON
DIN
G TO
EMERG
ENC
IES
POCKET EMERGENCY TOOL
18
RAPI
D H
EALT
H A
SSES
SMEN
T
POCKET EMERGENCY TOOL
The following should be made available for reference from the event.
Basically, the following key questions need to be answered:! Is there an emergency or not? (If so, indicate type, date,
time and place of emergency, magnitude and size of affected area and population)
! What is the main health problem? ! What health facilities or services have been or may be
affected?! What is the existing response capacity? (actions taken by
the local authorities, by DOH-HEMS)! What decisions need to be made?! What information is needed to make these decisions?
Situation Report Outline:
1. Executive Summary2. Main Issue
a. Nature of the emergency (causative and additional hazards, projected evolution)
b. Affected area (administrative division, access)c. Affected health facilitiesd. Affected population (sex/age breakdown)
3. Health Impacta. Direct impact: reasons for alert (3 main causes of
b. Other reasons for concern (e.g., trauma, reports/rumors of outbreak)
critical information requiredwithin 24 hours
19
c. Indirect health impact (e.g., damage to critical infrastructures/lifelines)
d. Pre-emergency baseline morbidity and mortality (when available)
e. Projected evolution of health situation: main causes of concern if the emergency will be protracted
4. Vital Needs: current situationa. Waterb. Waste disposalc. Foodd. Shelter and environment on sitee. Fuel, electricity, and communicationf. Other vital needs (e.g., clothing and blankets)
5. Critical Constraintsa. Security: coordinate with the safety officer to identify
hazards or unsafe conditions associated with the incidentb. Transport and logisticsc. Social/political and geographical limitsd. Other constraints
6. Response Capacity: functioning resourcesa. Activities already underwayb. National protocols, contingency plansc. Operational support (command post, regional unit and
referral system, external assistance, state of communications)
d. Operational coordination (lead agencies, mechanisms, flow of information)
e. Strategic coordination (local/international relationships)7. Conclusions
a. Are the current levels of mortality and morbidity above-average for this area and this time of the year?
RAPID
HEA
LTH A
SSESSMEN
T
POCKET EMERGENCY TOOL
20
b. Are the current levels of morbidity, mortality, nutrition, water, sanitation, shelter and health care acceptable by international standards?
c. Is a further increase in mortality expected in the next 2 weeks?
8. Recommendations for Immediate Actiona. What must be put in place as soon as possible to reduce
avoidable mortality and morbidity?b. Which activities must be implemented for this to happen?c. What are the risks to be monitored?d. How can they be monitored?e. Which inputs are needed to implement all these?f. Who will be doing what?
9. Emergency Contacts: local donor representatives, DOH counterparts and neighboring regional directors.
10.Annexes: include all detailed information that are relevant
*See appendix for sample of rapid health assessment form.
Be honest in the conclusions and practical in the recommendations. Recommendations that cannot be put into practice quickly are useless.
Prioritize the health problems (in terms of magnitude and severity and of feasibility of
response interventions).
RAPI
D H
EALT
H A
SSES
SMEN
T
POCKET EMERGENCY TOOL
21
CRITIC
AL IN
CID
ENT M
AN
AG
EMEN
T
POCKET EMERGENCY TOOL
Steps as First Responders
a. Assume command (until a more senior personnel arrives) b. Assess the situation and advise the appropriate authorities
and agenciesc. Set perimeters! Identify and set perimeter (hot zone, warm zone, cold
zone)! Implement safety and security measures! Identify access and egress routes
d. Establish the initial medical command post e. Establish Safety Officerf. Establish Staging Officerg. Establish liaison with other services on siteh. Determine priorities and time constraintsi. Develop an incident plan in conjunction with members of the
Incident Management Teamj. Task response agencies and supporting servicesk. Coordinate resources and supportl. Monitor events and respond to changing circumstancesm. Report actions and activities to the appropriate agencies and
authorities
22
PRE-
HO
SPIT
AL
AC
TIV
ITIE
S
POCKET EMERGENCY TOOL
Triaging
Objective:To quickly identify victims needing immediate stabilization or
transport and the level of care needed by these victims by assessing airway, breathing, and circulation (ABC's).
Color Tagging
Ideally, the following information should be contained in the patient's color tag:
a. patient's sequence numberb. name of patientc. injuries identifiedd. previous interventions given at the scene
1st priority: Life-threatening - needs to be treated within 1-3 hoursa. obstruction/damage to airwayb. breathing disturbance (RR =30/min or RR <10/min)c. circulation disturbance (HR =100/min or weak pulses)d. altered level of consciousnesse. external bleeding with CVS collapse
RED TAG
Triaging is done if there are more victims than health responders. Reverse triaging is done
during the Search and Rescue stage where the priority is to get as much people out of danger
with the least effort.
23
YELLOW TAG
GREEN TAG
BLACK TAG
2nd priority: Urgent - needs to be treated within 4-6 hoursa. major burns: involving hands, feet or face (excluding
respiratory tract); complicated by major soft tissue traumab. spinal injuries; long bone or pelvic fracturesc. environmental injuries (heat/cold exposure)
3rd priority: Requires no treatment or can be delayeda. minor injuries not threatened by ABC instabilityb. minor fractures/soft tissue injuries/burnsc. injuries so severe that survival cannot be expected even
under the most ideal conditions; obviously mortal wounds where death is certain (such as head injuries or massive burns)
Last priority:a. death or moribund state
In emergency situations the most practical means of tagging may only be by color ribbons
or even pentel pens
PRE-HO
SPITAL A
CTIV
ITIES
POCKET EMERGENCY TOOL
24
HO
SPIT
AL
AC
TIV
ITIE
S
POCKET EMERGENCY TOOL
Color-Coded Alert Systems
The hospital alert status shall be declared either by the Secretary of Health, the HEMS Director, the Chief of Hospital or the HEMS Coordinator. The alert status shall continue to be in effect until cancelled by the Chief of Hospital or the HEMS Coordinator.
CODE WHITE
Alert Mode is called with any of the following conditions: ! a strong possibility of a military operation (e.g., coup
attempt) ! any planned mass action or demonstration within the area! forecasted typhoons, the path of which may affect the area! national or local elections or plebiscites! national holidays or celebrations (e.g., New Year's Eve,
Holy Week, etc.)! other conditions which may be declared as disasters by
the Chief of Hospital or other appropriate authority
There should be necessary preparations of the necessary equipment and even personnel. Aside from those who are on regular duty for the day, the following should be on-call anytime during his/her duty days: 1. surgeons2. orthopedic surgeons3. anesthesiologists4. internists5. O.R. nurses 6. ophthalmologists
25
7. otorhinolaryngologistsnd8. 2 response team should be on call
9. EMS, nursing personnel and administrative personnel residing at the hospital dormitory shall be placed on on-call status for immediate mobilization
Partial/Selective Activation is proclaimed when 20-50 casualties (red tags) are expected. This may require the activation of the hospital network or at the judgment of the director or the HEMS coordinator, may only involve the hospital nearest the emergency site.
The following should respond once CODE BLUE is on:1. on-scene response team2. medical officer in charge of the emergency room 3. ALL orthopedic residents 4. medical officer in charge of the operating room5. surgical team on duty for the day
CODE BLUE
HO
SPITAL A
CTIV
ITIES
POCKET EMERGENCY TOOL
The composition of the back-up and on-call teams would depend on the type and level of the hospital. The suggestions here are based on a general tertiary hospital. Each hospital can come up with its own team members. In some places like Metro Manila, there can also
be designated support hospitals (usually specialty hospitals). These specialty hospitals act as support to a receiving hospital (e.g., San Lazaro and Fabella Hospital supporting Jose
Reyes Memorial Medical Center).
26
6. officer in charge of supplies at the CSR7. surgical team on duty the previous day8. ALL anesthesiology residents9. nursing supervisor on duty10.operating nurses living within or in the vicinity of the hospital 11.ENTIRE security workforce12.ALL third and fourth year residents13.ALL O.R. nurses14.institutional workers on duty
Full Activation is put into effect when more than 50 (red tag) casualties are momentarily anticipated, expected or suddenly brought to the hospital. The situation may require more than one hospital to respond by sending an on-scene team.
The following should respond once Code Red is on: 1. ALL persons enumerated under Code Blue2. ALL institutional workers3. ALL nursing attendants4. ALL nurses5. ALL medical interns and clinical clerks
CODE RED
HO
SPIT
AL
AC
TIV
ITIE
S
POCKET EMERGENCY TOOL
27
If there is a strong possibility that there would be a need to change the alert status from code white to blue to red, the Chief of Hospital is authorized to:1. Cancel all leaves of personnel and for them
to report to the hospital.2. Put back-up teams on standby within the
hospital for rapid deployment.3. Take other steps necessary to respond to
the emergency situation (e.g. cancel elective surgeries, etc.).
HO
SPITAL A
CTIV
ITIES
POCKET EMERGENCY TOOL
28
Steps in Ensuring Communicable Disease Control in Emergencies
1. Conduct rapid health assessment (see previous section)2. Provide general prevention measures in coordination with
other sectors, including:! Food security, nutrition and food aid! Water and sanitation! Shelter
3. Provide community health education messages including information on how to prevent common communicable diseases and how to access relevant services! Encourage people to seek early care for fever, cough,
diarrhea, etc., (especially children, pregnant women and older people)
! Promote good hygienic practice! Ensure safe food preparation techniques! Ensure boiling or chlorination of water
4. Implement as indicated, specific prevention measures, such as mass measles vaccination campaign, Expanded Program on Immunization, and vector control.
5. Provide essential clinical services6. Provide basic laboratory facilities7. Set-up surveillance/early warning systems
a. Detect outbreaks earlyb. Report diseases of epidemic potential immediatelyc. Monitor disease trends
8. Control outbreaksa. Preparationb. Detectionc. Confirmation
PREV
ENTI
ON
AN
D C
ON
TRO
L O
F C
OM
MU
NIC
ABL
E D
ISEA
SES
POCKET EMERGENCY TOOL
29
d. Investigatione. Control measuresf. Evaluation
Notes on Immunization
! A single suspected measles case is sufficient to prompt an immediate immunization response. Life-saving measles vaccine should be made available immediately targeting all infants and children 6-59 months of age. The suggested target age group may be expanded up to 15 years, if feasible, in areas where there is substantial crowding.
! Each visit to health care facilities should be seen as an opportunity to vaccinate for routine EPI regardless of the reason for the visit. Vaccination program activities should be included as part of basic emergency health care services.
! Mass vaccination against cholera and typhoid fever is not recommended. The most practical and effective strategy to prevent cholera and typhoid is to provide clean water in adequate quantities and adequate sanitation. Sufficient soap and hygiene education will further prevent the transmission of both diseases.
! Mass tetanus vaccination programs are not indicated. However, tetanus boosters may be indicated for previously vaccinated people who sustain open wounds or for other injured people depending on their tetanus immunization history.
! Mass vaccination for Hepatitis A is not recommended.
PREVEN
TION
AN
D C
ON
TROL O
F CO
MM
UN
ICA
BLE DISEA
SES
POCKET EMERGENCY TOOL
30
Nutrition Preparedness
1. Planning: Every effort should be done to formulate an inter-sectoral and comprehensive plan (i.e., NNC's Nutrition Preparedness in Disasters and Emergencies Plan or NPDEP).
2. Nutritional Management: Is an institutional and multi-sectoral concern. It is equally the responsibility of the national government, local government and even non-government units. Disaster Coordinating Teams implement the NPDEP while involving the Municipal Nutrition Action Officer in the creation of Disaster Response Teams.
3. Adequate Nutrition: During emergencies, infants (<1y/o) and children (<5y/o) are the most vulnerable group. Interrupted breastfeeding and inappropriate complementary feeding will heighten the risk for malnutrition, illness and mortality.
4. Resource Generation and Mobilization: Maintain a stockpile of culturally acceptable food items that can be stored for a long period of time such as rice, canned goods, noodles, dried fish and canned/powdered milk. Intensify campaign on creating vegetable gardens in schools and backyards. Identify and coordinate with donor agencies and companies that can donate food during disasters.
5. Public Education: Promote the acceptability and utilization of donated foods ideal for disasters (i.e. compact food). Support the innovation of nutritionally dense ready-to-eat foods.
NU
TRIT
ION
CO
NC
ERN
S
POCKET EMERGENCY TOOL
31
6. Cultural and Indigenous Habits: Customs should be taken into consideration in food management.
7. Gate Keepers: Identification of local/tribal leaders are critical for nutrition education, supplementation, and resettlement feeding.
NU
TRITION
CO
NC
ERNS
POCKET EMERGENCY TOOL
! Following a major sudden disaster, some people may have no access to food and/or be unable to prepare food for a few days at least.
! In slow-onset crisis or in situations where the livelihood of the community is greatly undermined, particularly in areas where nutritional status was already poor, it will be important to monitor nutritional status and households' access to food, and to initiate remedial action (e.g. through supplementary feeding) if nutritional status is at risk.
! In extreme cases, nutritional rehabilitation through intensive, supervised therapeutic feeding (TF) may be required.
! Because the number of caregivers is reduced during emergencies and their ability to cope is diminished by physical and mental stress, strengthening caregiving capacity is an essential part of promoting good feeding practices for infants and young children.
! Healthy workers are essential. Aside from looking after the basic health and nutritional needs of the displaced population, health workers have to be debriefed to look after their personal health as well.
32
NU
TRIT
ION
CO
NC
ERN
S
POCKET EMERGENCY TOOL
Energy Requirements
For initial planning purposes:! Average daily energy requirement : 2,100 kcal/person/
day ! When the data are available, the planning figure should be
adjusted according to:! Physical activity level add 140 kcal for moderate activity,
350 kcal for heavy activity (e.g., during construction or land preparation works)
! Age/sex distribution when adult males make up more than 50% of the population, requirements are increased; when the population is exclusively women and children, requirements are reduced.
! Special needs of pregnant and lactating women a. Pregnant women? Need an additional 300 kcal/day? If malnourished, need another 500 kcal/day? Should receive iron and folate supplements
b. Lactating women? Need an additional 500 kcal/day? If malnourished, need another 500 kcal/day? Should receive sufficient fluids, taking into account
activity
Other nutritional requirements:! Protein: 10 to 12% of diet (i.e. 52 to 64 g)! Fat/oil: = 17% of diet (i.e. 50 g)! Micronutrients: a range of micronutrients (vitamins and
minerals) are required for survival and good health
33
Ideal Foods for Disaster! Carbohydrate sources rice, root crops, bread, noodles ! Protein sources eggs, canned meat and fish, fresh meat and
fish, dried meat and fish, milk! Fat sources cooking oil, margarine! Vitamin and mineral sources fruits and vegetables! Others coffee and other beverages
* see appendix for examples of rations.
Nutritional Assessment
The most widely accepted practice is to assess malnutrition levels in children aged 6-59 months as a proxy for the population as a whole. Reports should always describe the probable causes of malnutrition, and nutritional edema should be reported separately.
NU
TRITION
CO
NC
ERNS
POCKET EMERGENCY TOOL
Two-stage cluster sampling is normally used: 30 clusters are selected, then 30 children
within each cluster.
Edema of both feet
Weight-for-Height*
MUAC
Body Mass Index
Mild Malnutrition
No
80-90%
(-1 to -2 SD)
12.5 to 13.5 cm
17 to <18.5
Moderate
Malnutrition
No
70-79%
(<-2 to -3 SD)
12.0 to 12.5 cm
16 to <17
Severe
Malnutrition
Yes
< 70%
(<-3 SD)
<12 cm
<16
Classification of Acute Malnutrition
34
Age
6-11 months
1-5 years
Dose
100,000 IU
200,000 IU
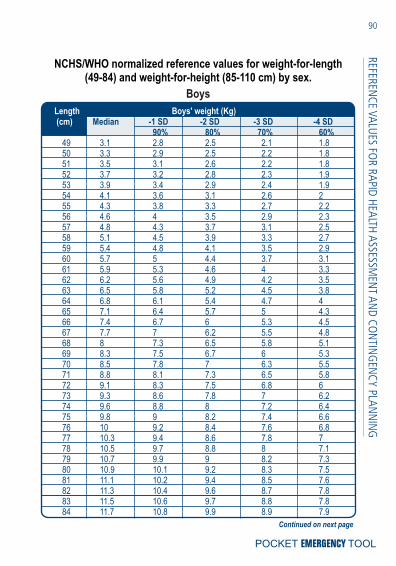
*see appendix for length-for-weight/height-for-weight reference values**see appendix for decision framework for implementing feeding programs.
Feeding Recommendations
! Up to 6 months of age: Encourage mothers to exclusively breastfeed as often as the child wants, day and night, at least 8 times in 24 hours. Do not give any other fluid or food.
! 6 months to 12 months: Breastfeed as often as the child wants. In addition, give adequate servings of locally available complementary foods at least 3 times a day.
! 12 months to 2 years: Breastfeed as often as the child wants. Give adequate serving of locally available complementary food at least 5 times a day.
Give vitamin A if a child has severe malnutrition. Give one dose in your presence and give one dose to the mother to give it to
the child at home the next day.
There should be a continual search for malnourished children so that their condition
can be identified and treated before it becomes severe.
NU
TRIT
ION
CO
NC
ERN
S
POCKET EMERGENCY TOOL
35
! 2 years and older: Give three meals of family food per day. Also, give nutritious snacks, twice daily.
Notes on Breastfeeding
! Breastfeeding's multiple advantages are especially important during emergencies (i.e., protection from infection and its consequences, contraceptive effect, privileged nurturing moment important for both mother and child). Every effort should be made to identify ways to breastfeed infants whose mothers are absent or incapacitated. Every effort should be made to create and sustain an environment that encourages frequent breastfeeding for children under two years of age.
! A nutritionally adequate breast-milk substitute, fed by cup, should be available for infants who do not have access to breast milk. The use of infant-feeding bottles and artificial teats in emergency settings should be actively discouraged.
! Emergencies do not justify routine distribution of breast-milk substitutes. Formula feeding may increase the considerable risk of child morbidity and mortality.
! The nutritional status of breastfeeding women should be protected as an end in itself, and as a means of maintaining the adequate growth and development of their children.
NU
TRITION
CO
NC
ERNS
POCKET EMERGENCY TOOL
36
ENV
IRO
NM
ENTA
L H
EALT
H
POCKET EMERGENCY TOOL
Minimum level of necessary services to be provided:1. Adequate shelter for displaced persons! Evacuees should be protected from the elements! Secure against violence! Provide allocations for privacy! Avoid overcrowding.! Floor area per person: 3.5 square meters! Fresh air ventilation per person per hour: 20-30 cubic
meters! Lighting: adequate (minimum is a 5-foot candle)! Ventilation: adequate (combined openings at least 10% of
floor area)2. Sufficient quantities of accessible drinking water 3. Facilities for excreta and liquid waste disposal4. Protection of food supplies against contamination5. Protection of individuals in affected population against vector-
borne diseases through vector control activities and through chemoprophylactic methods.
37
WA
TER SUPPLY
POCKET EMERGENCY TOOL
Assessment
1. Assess water resources for human consumption to ascertain the availability of water (quantity and quality) in relation to the demand.
2. Estimate the demand, identify possible sources and assess the possibility of developing these resources.
3. Consult local people in the identification of water sources to be developed.
4. Tap the expertise of the local Sanitary Engineer in the assessment of the water resources and the conduct of sanitary survey.
5. Always consider seasonal factors in the assessment.
Organization1. Organize water allocations between the host community and
the evacuees to prevent overstraining water resources.2. Evaluate the technology used in the water supply system to
ensure that continuous and long-term operational needs are within reach of the community and the evacuees.
3. From the start, involve the evacuees in the maintenance and operation.
Provision of adequate amounts of drinking water is of utmost importance after disaster. It should first be made accessible to victims and relief workers and in essential locations, such
as hospitals and treatment centers. After drinking water is secured within stricken areas, making water available for domestic uses (such
as cleaning and washing) should be considered.
38
4. Train evacuees without prior experience.5. Combine water control and treatment with improved personal
hygiene and environmental health practices.6. The design and construction of the water supply system must
be closely coordinated with evacuation camp planning and layout as supported by health promotion and sanitation.
7. Consider using pumps and other mechanical equipment attainable in the area where fuel and spare parts are available, and maintenance is not a complicated aspect. Technical breakdown should be quickly repaired.
8. Monitor both the organizational and technical aspects of the complete water supply system.
Immediate Action after a Disaster
1. Estimate water requirements and assess water supply possibilities.
2. Make an inventory of water sources and assess all sources in terms of their quality and yield.
3. Protect water sources from pollution. Provide water in good quantities and reasonable quality.
4. Improve access to supplies by developing water sources and a storage and distribution system to deliver sufficient amounts of safe water, including reserve.
5. Conduct regular sample collection and testing of water quality.
6. If possible, use water sources that do not need treatment. If there is a large number of evacuees, decontamination of water is necessary. Treat water according to the characteristics of the raw water.
7. Set up schedules for operation and maintenance.
WA
TER
SUPP
LY
POCKET EMERGENCY TOOL
39
8. Maintain and update information on water resources obtained during needs assessment, planning, construction, operation and maintenance.
Intermediate Response
1. If the minimum amount of water cannot be made available from local sources, recommend transfer to another evacuation camp.
2. If storing the water in tanks is employed, the storage should be tested periodically.
3. Domestic hygiene and environmental health measures should be observed in order to protect the water between collection and use.
Organize a distribution system that prevents pollution of the source and ensures equity if water is insufficient.
Water Need
1. Minimum Demand (per person per day); calculate the following:a. 2 liters for drinkingb. 10 liters for food preparation and cookingc. 15 liters for bathingd. 15 liters for laundrye. 10 liters for sanitation and hygiene
2. Quality: To preserve public health, a large amount of reasonably safe water is preferred over a small amount of purified water.
3. Control: Bacteriological, biological, chemical, physical and
WA
TER SUPPLY
POCKET EMERGENCY TOOL
40
radiological quality of water must be deemed safe.! There are no fecal coliforms per 100 ml at the point of
delivery.! People drink water from a protected or treated source in
preference to other readily available water sources,! Steps are taken to minimize post-delivery contamination.! No negative health effect is detected due to short-term use
of water contaminated by chemical (including carry-over of treatment chemicals) or radiological sources, and assessment shows no significant probability of such an effect.
4. Other Needs:a. Hospital and Clinics:! Out-Patient: 5 liters per patient per day! In-Patient: 40-60 liters per patient per day
b. Mass Feeding Centers: 20-30 liters per person per dayAnimals! Cow/Carabao: 30 liters per day! Pig: 1.5 liters per day! Goat: 1.5 liters per day! Poultry: 2 liters per day
5. Water Decontamination/Disinfectants:! Water Purifier: 2 tablets per person per day! HTH (high-test hypochlorite) Stock Solution: 1 liter/20
families/5 days! Shock Disinfection: 50-100 parts per million (ppm) of 60-
70% of available chlorine! Environmental Cleaner-Sanitizer
6. Drinking Water Container: one container of 10 liters per family7. Communal Water Storage Tank: 10 liters per person per day.
Volume of tank good for 2 days demand; half full in the
WA
TER
SUPP
LY
POCKET EMERGENCY TOOL
41
evening; with free residual chlorine of 0.7 ppm.8. Shallow Well: for toilet flushing and cleaning9. Water Points:! Distance between Water Point and Users: 150 m (max.)! Minimum Number of Water Points: 1 tap per 250 users! Queuing time at a water source is no more than 15
minutes.! It takes no more than three minutes to fill a 20-liter
container.
WA
TER SUPPLY
POCKET EMERGENCY TOOL
42
SAN
ITA
TIO
N A
ND
WA
STE
MA
NA
GEM
ENT
POCKET EMERGENCY TOOL
Assessment
Excreta Disposal1. What is the current defecation practice (including anal
cleansing)? If it is open defecation, is there a designated area?
2. Is the current defecation practice a threat to water supplies (surface or ground water) or living areas?
3. Are there any existing facilities? If so, are they used, are they sufficient and are they operating successfully? Can they be extended or adapted?
4. What is the ratio of domestic facilities to population?5. What is the maximum one-way walking distance for users?6. Are people prepared to use pit latrines, defecation fields,
trenches, etc.?7. What is the level of the groundwater table?8. Are soil conditions suitable for on-site excreta disposal?9. Do current excreta disposal arrangements encourage
vectors?10. Are there materials or water available for anal cleansing?
How do people normally dispose of these materials?11.How do women manage issues related to menstruation? Are
there appropriate materials available for this?
Drainage1. Is there a drainage problem (e.g. flooding of dwellings or
toilets, vector breeding sites, polluted water contaminating living areas or water supplies)?
2. Is the soil prone to water logging?3. Do people have the means to protect their dwellings and
toilets from local flooding?
43
SAN
ITATIO
N A
ND
WA
STE MA
NA
GEM
ENT
POCKET EMERGENCY TOOL
Solid Waste Management 1. Is solid waste a problem?2. How do people dispose of their waste? What type of how
much solid waste is produced?3. Can solid wastes be disposed of on-site, or does it need to be
collected and disposed of off-site?4. Are there health facilities and activities producing waste?
How are wastes being disposed of? Who is responsible?
Immediate Action
1. Localize defecation and prevent contamination of water supply.
2. Collect baseline data of the site and locate zones for sanitary facilities.
3. Develop appropriate systems for the disposal of excreta, refuse and wastewater.
4. Plan the number and location of sanitary facilities and services to be established and provided.
5. Establish sanitation teams for the construction and mainte-nance of facilities.
6. Set up services for vector and vermin control. 7. Set up services for management of dead bodies 8. Establish a monitoring and reporting system.9. Include environmental health as an integral part of health
promotion.
Excreta Facilities1. Communal Trench Latrine: for 50 persons, 1.2 m x 0.3 m x
0.6 m. Use only soil for cover.2. Pit Latrine: 1 seat for 20 persons, 1.2 m x 0.6 m x 0.6 m
44
3. Ventilated Improved Pit: 1 seat for 20 persons, 0.8 m x 0.7 m x 3.0 m
4. Pour-Flush Water-Sealed Toilet: 1 seat for 20 persons.5. Others: “Antipolo,” Aqua Privy, Deep Pit Latrine, Reed Odorless
Earth Closet (ROEC), Chemical Toilet: 1 seat for 20 persons.6. Urinals: Urine Soakage, Four-Funnel Urinal7. Children's Feces: should be disposed of immediately and
hygienically8. Distance of Latrines:! From users: 250 m (max.)! From shelters: 30 m (min.)! From any water source: 25 m radial distance
Liquid Waste Facilities
1. Infiltration Trench, Grease Trap and Soakage Pit, Baffle Grease Trap, and Cold Water Grease Trap.
2. Locate not less than 25 meters radial distance from any source of water supply.
3. Protect from vermin harborage and breeding.4. There should be no standing wastewater around water points
or elsewhere in the settlement.5. Drainage: Run-in and run-off water management.6. Shelters, paths, water and sanitation facilities should not be
flooded or eroded by water.
Bottom of any latrine should be at least 1.5 meters above the water table. Drainage or
spillage from defecation systems must not run towards any surface water source or shallow
groundwater source
SAN
ITA
TIO
N A
ND
WA
STE
MA
NA
GEM
ENT
POCKET EMERGENCY TOOL
45
Solid Waste Facilities
1. Storage:! 100-liters capacity per 10 families! Distance from users: 15 m (max.)! Bulk storage bin: centralized bin for temporary storage
before collection! No contaminated or dangerous health waste in living or
public spaces2. Collection: organize a camp refuse collection team3. Disposal:! Burial: Communal Open Pit, 1.2 m x 1.2 m x 1.8 m ! Cross Fire Trench Incinerator: for 20 families (2.4 m x 0.3
m x 0.3 m)! Barrel and Trench Incinerator, Bailleul Incinerator, Inclined
Plane Incinerator, Open Corrugated Iron Incinerator, Rock Pit Incinerator, Drying Pan Incinerator and Open Turf Incinerator: for 10 families
! Final disposal does not create health or environmental problems
Health-care Wastes
1. Be aware of the public health and occupational risks from health-care waste
a. Vaccination, notably for Hepatitis B should therefore be provided to waste handlers.b. All waste handlers should wear protective clothing. c. Hand-washing and disinfection are a must.
2. Minimize health-care waste3. Segregate:
SAN
ITATIO
N A
ND
WA
STE MA
NA
GEM
ENT
POCKET EMERGENCY TOOL
46
! To be done at point of generation using dedicated, colored and/or marked containers
! Separate wastes into three main categories:i. infectious sharps (collect sharps in puncture proof
containers with a lid that can be closed, mark with biohazard symbol)
ii. non-sharp infectious wastesiii. non-infectious wastes
! If no separation of wastes takes place, the whole mixed volume of health care waste needs to be considered as being infectious.
1. Dispose properly. Wastes to be buried and should not be incinerated:
a. used infectious plastic syringes and needlesb. other infectious PVC plastics such as tubing, catheters, IV setsc. anatomical wastes
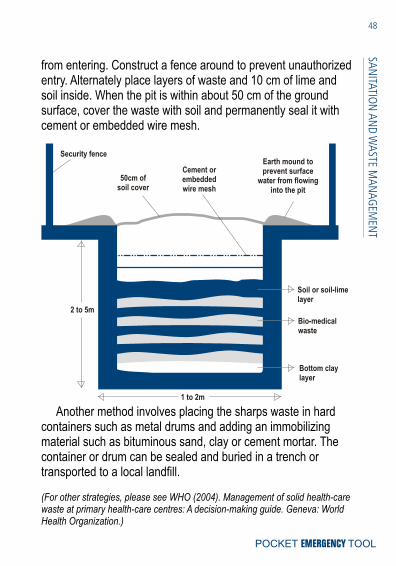
All these should be buried in a sharps waste burial pit.
Dig a pit 1 to 2 meters wide and 2 to 5 meters deep. Line the bottom of the pit with clay or low permeable material. Construct an earth mound around the mouth to prevent to prevent water
SAN
ITA
TIO
N A
ND
WA
STE
MA
NA
GEM
ENT
POCKET EMERGENCY TOOL
Non-infectious waste 80%
Pathological waste and infectious waste 15%
Sharps waste 1%
Chemical or pharmaceutical waste 3%
Pressurized cylinders, broken Less than 1% thermometers…
Approximate percentage of waste types per total waste in PHC centers
47
from entering. Construct a fence around to prevent unauthorized entry. Alternately place layers of waste and 10 cm of lime and soil inside. When the pit is within about 50 cm of the ground surface, cover the waste with soil and permanently seal it with cement or embedded wire mesh.
Another method involves placing the sharps waste in hard containers such as metal drums and adding an immobilizing material such as bituminous sand, clay or cement mortar. The container or drum can be sealed and buried in a trench or transported to a local landfill.
(For other strategies, please see WHO (2004). Management of solid health-care waste at primary health-care centres: A decision-making guide. Geneva: World Health Organization.)
Security fence
50cm of soil cover
Cement orembeddedwire mesh
Earth mound to prevent surface
water from flowing into the pit
2 to 5m
1 to 2m
Soil or soil-lime layer
Bio-medical waste
Bottom clay layer
SAN
ITATIO
N A
ND
WA
STE MA
NA
GEM
ENT
POCKET EMERGENCY TOOL
48
VEC
TOR
AN
D V
ERM
IN C
ON
TRO
L
POCKET EMERGENCY TOOL
Assessment
1. What are the vector-borne disease risks and how serious are these risks?
2. If vector-borne disease risks are high, do people at risk have access to individual protection?
3. Is it possible to make changes to the local environment (by drainage, excreta disposal, refuse disposal, etc.) to discour-age vector breeding?
4. Is it necessary to control vectors by chemical means? 5. What information and safety precautions need to be provided
to households?
Preventive Measures
a. Conduct vermin population density survey.b. Vulnerable populations are settled outside of the malar-
ial/dengue zone. In areas of known malaria risk: ! spraying of shelters with residual insecticide and/or
retreatment/distribution of insecticide-treated mosquito nets in areas where their use is well-known.
In areas endemic of dengue: ! water storage containers should be covered to prevent
them from becoming mosquito-breeding sites. Attempts should be made to eliminate pooled water which may be gathering amongst the debris.
c. Vector breeding or resting sites modified.d. Screening of living quarters.e. Rats, flies and other mechanical nuisance pests kept within
49
VEC
TOR A
ND
VERM
IN C
ON
TROL
POCKET EMERGENCY TOOL
acceptable levels.f. Intensive fly control is carried out in high-density settlements
when there is risk or presence of diarrhea outbreak.g. Removal of breeding and harborage places of vectors and
maintenance of sanitation. Garbage must be collected and appropriately disposed to discourage rodent vector breeding.
h. Larvi-trapping
Chemical Control
a. 1 sprayer for every 50 familiesb. 1 misting machine for every 50 familiesc. 1 fogging machine for every 500 familiesd. Fumigation for the camp, if needed (with proper precautions);
done under the supervision of an emergency Sanitary Engineer
e. Adulticides: for crawling and flying insectsf. Rodenticide: for rats and mice (under some conditions)g. Larviciding: introduction of local bioremediation microbes
Estimation of Vector Population
Mosquitoes: 1. Select several shelters in the camp.2. In the shelter, close all openings, windows, holes, etc.3. Spread a white sheet on the floor of the rooms.4. Spray the insecticide and wait 20 minutes until the insecticide
has killed the mosquitoes.5. Count the number of killed adult mosquitoes and record.6. The following can be determined:
50
! The number of killed adult mosquitoes divided by the number of inspected shelters will give the average mosquito density per shelter.
! The number of killed adult mosquitoes divided by the number of persons occupying each shelter will give the average number of mosquitoes per person.
! The number of mosquitoes found with blood in the abdomen (red or black) divided by the number of person living in the shelter will give the average number of bites per person.
7. Send the collected mosquitoes to a laboratory for identifica-tion.
Flies:1. Count the average number of flies that land on a grill placed
where flies congregate during three 30-second periods.
(from: Lacarin, CJ and Reed RA (1999) Emergency Vector Control Using Chemicals, Water, Engineering and Development Center (WEDC), Loughborough.)
VEC
TOR
AN
D V
ERM
IN C
ON
TRO
L
POCKET EMERGENCY TOOL
51
EPIDEM
IOLO
GY A
ND
SURV
EILLAN
CE
POCKET EMERGENCY TOOL
Epidemiologic Methods of Emergency Management
Objectives:! Assess the urgent needs of human populations! Match available resources to needs! Prevent further adverse health effects! Monitor and evaluate program effectiveness! Improve contingency planning! Optimize each component of emergency management
Application:! Hazard mapping! Analysis of vulnerability! Assessment of the flexibility of the existing local system for
emergency! Assessment of needs and damages! Monitoring health problems! Implementation of disease-control strategies! Assessment of the use and distribution of health services! Etiological research on the cause of mortality and morbidity! Follow-up long-term impacts of health, etc.
Steps in Developing a Surveillance System After a Disaster
1. Establish objectives! Detect epidemics ! Monitor changes in the population? Numbers
52
EPID
EMIO
LOG
Y A
ND
SU
RVEI
LLA
NC
E
POCKET EMERGENCY TOOL
? Health status including nutritional conditions? Security? Access to food? Access to water? Shelter and sanitation? Access to health services
! Facilitate the management of relief
2. Develop Case Definitions (Request NEC)! Standard case definitions of health conditions simplify
reporting and analysis
3. Choose the Indicators! Indicators must:? Illustrate the status of the population ? (e.g., death rates)? Measure the effectiveness of relief ? (e.g., immunization coverage)
4. Determine Data Sources! Data can come from health-care facilities (“passive
surveillance”) and from surveys in the community (“active surveillance”)
! Involve those who provide health care! Health surveillance in an emergency requires input from
all sectors
“Case definitions” and “Indicators” need to be agreed upon by all those involved in the relief
operations.
53
5. Develop Data Collection Tools and Flows! Use pre-existing local formats and/or international
standards! Use formats that facilitate data entry (EpiInfo):! Utilize existing process flows
6. Field-Test and Conduct Training! Can these data produce the information required?! Training field workers will improve data facility and local
analysis
7. Develop and Test the Strategy of Data Analysis! Data analysis should cover:? Hazards and impact on the population's health? Quality and quantity of services provided? Impact of services on population's health? Relation between services provided to different groups
(evacuees and hosts)? Deployment and utilization of resources
! Major operations may require a central epidemiological unit
8: Develop Mechanisms for Disseminating Information (Risk Communication)! Who will receive the information?! For the information to be useful, it must be disseminated
widely and in a timely fashion:? Feedback will sustain data collection and the
performance of field workers? Health information is important for the activities of other
sectors
EPIDEM
IOLO
GY A
ND
SURV
EILLAN
CE
POCKET EMERGENCY TOOL
54
! Sharing information is good coordination
9: Monitor and Assess Usefulness of the System! Is everybody reporting on time? Which data are missing?! Lack of information in areas or programs that have
problems! Is the system useful?! Is the information generated by the system being used for
decision making?! If not, readjust the system
EPID
EMIO
LOG
Y A
ND
SU
RVEI
LLA
NC
E
POCKET EMERGENCY TOOL
55
PSYCH
OSO
CIA
L CA
RE AN
D M
ENTA
L HEA
LTH
POCKET EMERGENCY TOOL
Steps in Promoting Psychosocial and Mental Health
1. Assess psychosocial and mental health concerns. Schedule consultative meetings with the provincial and municipal health workers in the affected area to:! Estimate the psychosocial problems experienced by the
people, guided by the classification of people at high risk ! Estimate available resources for mental health/social
services
* see appendix for Summary Table on Projecting Mental Health Assistance
2. Brief field officers in the areas of health and social welfare regarding issues of fear, grief, disorientation and need for active participation. Mobilize informal human resources in the community (e.g., Red Cross volunteers, religious and political leaders).
3. Conduct mostly social interventions that do not interfere with acute needs such as the organization of food, shelter, clothing, PHC services, and, if applicable, the control of communicable diseases.
The impact of a traumatic event is likely to be greatest in persons who had a pre-existing
mental health problem, a history of prior trauma, greater exposure to the disaster and its aftermath, and those who lack family and peer
support.
56
PSYC
HO
SOC
IAL
CA
RE A
ND
MEN
TAL
HEA
LTH
POCKET EMERGENCY TOOL
4.Establish contact with PHC. ! Develop the availability of mental health care for a broad
range of problems through general health care and community-based mental health services.
! Manage urgent psychiatric complaints (i.e., dangerous-ness to self or others, psychoses, severe depression, mania, epilepsy) within PHC.
! Ensure availability of essential psychotropic medications at the PHC level. Many persons with urgent psychiatric complaints will have pre-existing psychiatric disorders and sudden discontinuation of medication needs to be avoided.
5. Start planning medium- and long-term development of community-based mental health services and social interventions needed during recovery and rehabilitation. This is vital since it is during this phase that survivors will be rebuilding their lives amidst the grief from the loss of loved ones, property, and livelihood.
6. If the acute phase is protracted, start training and supervising PHC workers and community workers (e.g., provision of appropriate psychotropic medication, 'psychological first aid', supportive counselling, working with families, suicide prevention, management of medically unexplained somatic complaints, substance use issues and referral).
As far as possible, manage acute distress without medication. It is also not advisable to
organize single session psychological debriefing to the general population as an early interven-
tion after exposure to trauma.
57
7. Educate other humanitarian aid workers as well as community leaders (e.g., village heads, teachers, etc.) in core psychological care skills (e.g., 'psychological first aid', emotional support, providing information, sympathetic reassurance, recognition of core mental health problems) to raise awareness and commu-nity support and to refer persons to PHC when necessary.
8. Carefully educate the public on the difference between psychopathology and normal psychological distress, avoiding suggestions of wide-scale presence of psychopathology and avoiding jargon and idioms that carry stigma.
9. Facilitate creation of community-based self-help support groups. The focus of such self-help groups is typically problem sharing, brainstorming for solutions or more effective ways of coping (including traditional ways), generation of mutual emotional support and sometimes generation of community level initiatives.
10.Provide support to caregivers who, because of the exhaustion and enormity of the job, may experience "burn-out."
Interventions for Children Affected by Emergencies
1. Encourage parents, teachers, and other caregivers to understand and monitor child emotional reactions. Remember that children's reactions vary with age.
2. Help reduce effects by offering emotional support and security to the child.
PSYCH
OSO
CIA
L CA
RE AN
D M
ENTA
L HEA
LTH
POCKET EMERGENCY TOOL
58
3. Facilitate recovery by modelling healthy coping strategies.
* See “Mental health and psychosocial care of children in disasters” (WHO, 2005) for further guidance.
Valuable social interventions include:
! Ensuring ongoing access to credible information on the emergency, on the availability of assistance, and on the location of relatives to enhance family reunion
! Establishing access to communication with absent relatives, if feasible
! Organizing family tracing for unaccompanied minors, the elderly and other vulnerable groups.
! Giving 'psychological first aid':? basic, non-intrusive pragmatic care with a focus on
listening but not forcing talk? assessing needs and ensuring basic physical needs are
met? providing or mobilizing company (preferably family or
significant others)? encouraging but not forcing social support? protecting from further harm
! Widely disseminating uncomplicated, empathic information on normal stress reactions and culturally appropriate relaxation techniques to the community at large
! Public education should focus primarily on normal reactions, because widespread suggestion of physical and mental disease may potentially lead to unintentional harm.
! The information should emphasize an expectation of hope, resilience and natural recovery.
! Promote community self-help activities- conceived and
PSYC
HO
SOC
IAL
CA
RE A
ND
MEN
TAL
HEA
LTH
POCKET EMERGENCY TOOL
59
managed by communities themselves.! Discouraging unceremonious disposal of corpses. Facilitate
conditions for maintaining or re-establishing appropriate cultural practices, including grieving and burial rituals by relevant practitioners.
! Assuming the activity is safe:1. Encouraging activities that facilitate the inclusion of the
bereaved, orphans, widows, widowers, or those without their families into social networks
2. Encouraging the organization of normal recreational activities for children and encouraging starting schooling for children, even partially
3. Involving adults and adolescents in concrete, purposeful, common interest activities (e.g., assist in caring for the ill especially if people are cared for at home, construct-ing/organizing shelter)
! Strengthening the community's and the family's ability to take care of children and other vulnerable persons.
Specific Concerns for Victims of Attacks Involving Biochemical Weapons
Attacks involving biochemical weapons may induce significant mental and social effects.1. Exposure to any stressor is a risk factor for a range of long-
term social and mental problems (including anxiety and mood disorders as well as non-pathological trauma and grief reactions)
2. Physical exposure to agents may induce organic mental disorders
PSYCH
OSO
CIA
L CA
RE AN
D M
ENTA
L HEA
LTH
POCKET EMERGENCY TOOL
60
3. Attacks are associated with experience of intense social and psychological distress, especially fear
4. Fear of biochemical attacks may be associated with epidemics of medically unexplained illness
5. Social problems may emerge after exposure to agents (e.g., population displacement; breakdown of community support systems; and social stigma associated with contagion or contamination)
! In case of quarantine or evacuation, enhance access to communication with absent relatives and friends.
! If appropriate and feasible, set-up telephone support systems to reduce isolation of people who are isolating themselves to reduce the chance of infection.
! Manage medically unexplained symptoms immediately to prevent potential chronicity of such symptoms.
! Public education campaigns may need to be organized to reduce social stigma and related social isolation of ex-patients and health workers who may be shunned because of undue public fear of contagion or contamination.
Psychosocial Concerns for Disaster Workers
Burnout or Disaster Fatigue:! state of extreme exhaustion or depletion, physically,
emotionally, mentally and socially! person feels worn-out and depleted of energy but feels that
he/she has not done enough
Signs of Burnout:! Low energy and exhaustion
PSYC
HO
SOC
IAL
CA
RE A
ND
MEN
TAL
HEA
LTH
POCKET EMERGENCY TOOL
61
! Detachment and separation from one's self; increasing feeling of “non-feeling,” “deadness,” indifference and even skepticism
! Aloneness, feeling unappreciated and mistreated! Impatience, heightened irritability! Increasing anger, suspiciousness! Confusion, agitation, limiting ability to focus mind and
behavior! Depression, psychosomatic complaints! Denial that anything is wrong; “I don't care”
Management of Burnout! Rotation of work assignments to allow time away from the
daily routine of disaster work for those in the field ! Rest and recreation program for those in active duty! CISD sessions should be done regularly for those in the field! Superiors and the agency itself should provide for situations
to give credit, express appreciation and recognition of their disaster workers at regular intervals
! Provision of appropriate assistance for those who might require counseling and/or specialist psychiatric attention
PSYCH
OSO
CIA
L CA
RE AN
D M
ENTA
L HEA
LTH
POCKET EMERGENCY TOOL
Historical research on group behavior has shown that contrary to common expectations,
public panic is uncommon. Disasters may leave some communities with increased social coherence. Community members often show great altruism and cooperation, and people
may experience great satisfaction from helping each other.
62
MA
NA
GEM
ENT
OF
DEA
D B
OD
IES
POCKET EMERGENCY TOOL
Health Considerations in Cases of Mass Fatalities
Emphasize that, in general, the presence of exposed corpses poses no threat of epidemics. The corpse has a lower risk for contagion than an infected living person. The key to preventing disease is to improve sanitary conditions and to educate the public.If death resulted from trauma, bodies are quite unlikely to cause outbreaks of diseases. They may, however, transmit gastroenteritis or food poisoning syndrome to survivors if they contaminate streams, wells, or other water sources. Thus, any bodies (or dead animals) lying in water sources should be removed as soon as possible.
!
!
!
! The National Disaster Plan/Emergency Operations Committee should specify the institution that will coordinate all processes related to the management of dead bodies.
! The health sector should take the leading role in:1. Addressing concerns about the
supposed epidemiological risks posed by dead bodies
2. Providing medical assistance to family members of the victims.
! The work of handling, identifying, and disposing of dead bodies is based on forensic sciences and requires a multidisciplinary team. However, in the absence of medico-legal experts, the health officer may need to carry out these tasks to the best of his or her abilities.
63
MA
NA
GEM
ENT O
F DEA
D BO
DIES
POCKET EMERGENCY TOOL
!
!
The risk posed by bodies buried by a landslide or mudslide is nonexistent.It should be noted that in areas where certain diseases are endemic, the disposal of bodies may become a priority. However, even in such cases the presence of dead bodies should not be considered an important public health risk.
Principal diseases that should be avoided by those responsible for managing corpses in order to prevent possible contagion:
1. streptococcal infection2. gastrointestinal infection (e.g., cholera, salmonellosis)3. Hepatitis B and C4. HIV
64
FORE
NSI
C S
CIE
NC
E C
ON
CER
NS
IN M
ASS
FA
TALI
TIES
POCKET EMERGENCY TOOL
Practical Approach to a Multiple Fatality Incident
1. Initial Concerns! Type of incident (natural hazards, e.g., flood, landslide,
earthquake, epidemics; human-generated, e.g., fire, land/sea/air transport crash, accidental or deliberate use of biochemical/radionuclear agents)
! Probable condition of remains (e.g. burnt, with severe trauma, decomposed, contaminated)
! Estimated number of fatalities! Location of incident! Local authority in-charge! Budget
2. Personnel ! Tap medico-legal officers from the NBI or PNP and local
government doctors.! Mobilize volunteers like medical and dental students or
specialists from the area.
Ideally a list of the people involved and their contact numbers should have been prepared beforehand.
3. Handling of the Bodies at the Scene! As much as possible document the location and position
of each body at the scene prior to removal.! Mark bodies/body parts to preserve their relationship to
one another.! Sketch and photograph for documentation.
65
FOREN
SIC SC
IENC
E CO
NC
ERNS IN
MA
SS FATA
LITIES
POCKET EMERGENCY TOOL
! Every effort must be taken to identify the bodies at the site where they are found. Tags should be attached to the bodies that provide the name (if known), approximate age, sex, and location of the body.
4. Evidence and Property! All items of property that are on the body should remain on it.! Other items associated with a body should be collected as
property and tagged with the body.! The location of loose items (e.g., proximity to which body)
should be documented prior to collection.
5. Removal and Transport of Remains! Before removing any body, body part or property, there
should be adequate documentation.! Care must be taken not to lose, contaminate or switch
such body, body parts or property to be removed and transported.
! Properly labeled separate bags must be used.! Be particularly careful of potential loss of teeth if they are
loose (e.g., badly burned or crushed remains); put a bag around the head.
! When adapting vehicles to transport dead bodies, it is advisable to use trucks or vans, preferably closed, with floors that are either waterproof or covered with plastic
! Using health service vehicles—specifically, ambu-lances—to transfer human remains from the site of the disaster is ill-advised.
Before anything else, observe and record first.
66
6. Temporary Mortuary Facility! Identify a place that can be converted into a makeshift
! Basic requirements:? Security? Adequate lighting, ventilation, water supply? Examining tables? Instruments for examining the remains and documenta-
tion! Ideally, should consist of a reception, a viewing room, a
storage chamber for bodies not suitable for viewing and a room to store personal possessions and records.
7. Examination of Remains! Objectives of the postmortem examination:? Identification of the remains? Cause of death determination? Manner of death determination? Collection of forensic evidence
! In emergency situations, usually the critical need is to identify the victims.
! Identification through visual identification by the next-of-kin should be limited to bodies that are suitable for viewing (i.e., not decomposed, burnt or mangled) and should be subject to verification by other means.
! A more reliable system of identification entails an objective comparison of antemortem and postmortem information.
! Because of limited resources, not all bodies can undergo a full autopsy; priority may be given to certain remains (such
POCKET EMERGENCY TOOL
67FO
REN
SIC
SC
IEN
CE
CO
NC
ERN
S IN
MA
SS F
ATA
LITI
ES
as those of transport operators driver, pilot/ship captain and crew).
! A detailed examination of the external body is done; marks such as tattoos, scars, moles and deformities are searched.
! Fingerprints are obtained and dental charting is done.! Blood and other tissue/fluid samples are collected for
possible tests (e.g., histopathology, DNA analysis, toxicology).
! Property collected from each body (e.g., clothes, jewelry, wallets, IDs) must be described and inventoried.
8. Preservation of the Body! Remains are best stored refrigerated (e.g., in rented
refrigerated storage trucks) while awaiting examination.! After the postmortem examination, embalming can be
done.
9. Dealing with Claimants! Notify family members of the death or disappearance of
victims in a clear, orderly, and individualized manner.! Organize a separate area where the next-of-kin can be
systematically interviewed for data.! Useful antemortem information to get:
Name, age, sex, height, buildAppearance when last seenDistinguishing features (tattoos, scars, moles, deformities, etc.)Significant medical history
! Ask the next-of-kin to submit the following:Medical records including x-ray films
POCKET EMERGENCY TOOL
68FO
RENSIC
SCIEN
CE C
ON
CERN
S IN M
ASS FA
TALITIES
Dental recordsClear photograph with teeth baredFingerprints on file
! Note that personal items that a person believed to be among the victims could have used (e.g., toothbrush, hairbrush, other items), could potentially contain reference fingerprints or DNA samples.
10.Death Certification and Release of Bodies! Properly identified victims shall be issued death certifi-
cates and the bodies released to the next-of-kin.! Maintain a record of how the bodies are disposed of
including information regarding the claimants' names, addresses and contact numbers.
! Bodies could remain unidentified in case of insufficient antemortem and postmortem data; these remains should be buried separately (not cremated!) and their postmortem records stored for future evaluation.
! Court proceedings could be initiated according to Philippine laws that would legally declare dead the unidentified and missing victims.
11.Disposal of Dead! Respond to the wishes of the family and provide all
possible assistance in final disposition of the body.! Burial is the preferred method of body disposal in
emergency situations unless there are cultural and religious observances that prohibit it. ? The location of graveyards should be agreed upon by
the community and attention should be given to ground conditions, proximity to groundwater drinking sources
POCKET EMERGENCY TOOL
69FO
REN
SIC
SC
IEN
CE
CO
NC
ERN
S IN
MA
SS F
ATA
LITI
ES
(which should be at least 50 m) and to the nearest habitat (500 m).
? Burial depth should be at least 1.5 m above the groundwater table, with at least 1 m of soil cover.
? If coffins are not available, corpses should be wrapped in plastic sheets to keep the remains separate from the soil.
? Burials in common graves and mass cremations are rarely warranted and should be avoided.
! Reject unceremonious and mass disposal of unidentified corpses. As a last resort, unidentified bodies should be placed in individual niches or trenches, which is a basic human right of the surviving family members.
12.Other concernsEnsure that there is a plan for the psychological and
physical care for the relief workers. Handling a large number of corpses can have an enormous impact on the health of the working team.
Give priority to the living over the dead: The priority is to treat survivors and re-establish the
health care system as soon as possible!
POCKET EMERGENCY TOOL
70FO
RENSIC
SCIEN
CE C
ON
CERN
S IN M
ASS FA
TALITIES
The arrival of inappropriate relief donations can cause major logistic chaos.
RESO
URC
E M
AN
AG
EMEN
T
POCKET EMERGENCY TOOL
Supply Management General Guidelines:
! Only a single government official should be made responsi-ble for channeling requests to avoid duplication and confusion.
! Donors should be asked to provide large amounts of a few items to simplify and expedite transfers.
! Requests should indicate clearly the order of priority, amounts, and formulations (compatible with the size of the affected population).
! Do not request perishable products and vaccines unless refrigeration and special handling facilities are available.
Guidelines for Drug Donations
! Based on expressed needs of the affected population.! Sent only with prior consent of recipient.! Based on the list of essential drugs.! Obtained from a quality source with quality standards.! Formulation and efficacy of foreign donations should be
similar to those commonly used in the country.! Label should at least contain generic name, dosage forms,
strength, quantity in container, and expiry date.! After the arrival of foreign drug donations, the medicines must
have a remaining shelf life of at least 1 year.
71
RESOU
RCE M
AN
AG
EMEN
T
POCKET EMERGENCY TOOL
Donation Labeling and Donation Marking
— foodstuff
— clothing and household items
— medical supplies/equipment
1. Labeling:! Consignments of medicines branded green should
indicate expiry date and temperature controls.! English should be used on all labels.
2. Size and weight! Goods should be in a 25-50 kg container, manageable by
a single person.
3. Contents! Relief supplies must be packed by type in separate
containers.! Value of relief goods is lost if there is no color-coding.! Give advance notice to the health relief coordinator and
supply information about the package (e.g., name and contact number of donor, date, method of transport, details of contents, and other special requirements for handling).
RED
BLUE
GREEN
Upon arrival of the donations/ consignments, acknowledge their receipt. Call or write the
senders and thank them.
72
RISK
CO
MM
UN
ICA
TIO
N
POCKET EMERGENCY TOOL
Communication Objectives:
! Acknowledge the event with empathy.! Establish spokesperson credibility! Explain and inform the public, in simplest terms, about the
risk! Provide emergency courses of action (including how/where
to get more information)! Commit to partners and public to continued
communication.! Listen to feedback and correct misinformation.! Empower risk/benefit decision-making.
Steps in Communicating Risks
1. Verify situation! Get the facts.! Obtain information from additional sources to put the
event in perspective.! Review and critically judge all information. Determine
credibility.! Clarify information through subject matter experts.! Begin to identify staffing and resource needs to meet the
expected media and public interest.! Determine who should be notified of this potential
emergency.
2. Conduct notifications
3. Activate Crisis Plan! Ensure direct and frequent contact with the EOC
73
RISK CO
MM
UN
ICA
TION
POCKET EMERGENCY TOOL
! Determine what your organization is doing in response to the event.
! Determine what other agencies/organizations are doing.! Determine who is being affected by this crisis. What are
their perceptions? What do they want and need to know?
! Determine what the public should be doing.! Determine what's being said about the event. Is the
information accurate?
4. Organize assignments! Identify the spokesperson for this event.! Determine if subject matter experts are needed as
additional spokespersons.! Determine if the organization should continue to be a
source of information to the media about this emergency, or would some issues be more appropriately addressed by other government entities?
5. Prepare information and obtain approvals
6. Release information to media, public and partners through arranged channels! Provide only information that has been approved by the
appropriate managers. Don't speculate! Repeat the facts about the event! Describe the data collection and investigation process! Describe what your organization is doing about the
emergency.! Describe what other organizations are doing.! Explain what the public should be doing
74
! Describe how to obtain more information about the situation
7. Obtain feedback and conduct communication evaluation
8. Conduct public education
9. Monitor events
(Adapted from CDC (2002). Crisis and Emergency Risk Communication.)
Media Management
What makes a “good” spokesperson?! Media savvy/rapport! Versatility to be a statesman or a brawler! Consistent and continuous authority! Sufficient knowledge and information! Available anytime (24 hours/day, 7 days/week)
Stick to facts, and put them in context! There is no such thing as 'off-the-record'.
Everything you say and do can be reported. Be careful with what you say in the presence of journalists, even after a formal interview is finished and at social gatherings
! Never make disparaging or critical remarks about local authorities or international partners
! Do not mention weaknesses they might be all that is reported
RISK
CO
MM
UN
ICA
TIO
N
POCKET EMERGENCY TOOL
75
Spokespersons must be supported with
the following:! Information and facts! Resources and contacts! Equally competent alternate
What do the people want to know?! What has happened? (Incident and Scope)! Why did it happen? (Cause)! Who or what should be held responsible? (Blame)! What is being done about it? (Action)! What will prevent it from recurring? (Result)
Press Releases:! Titles and opening lines are the most important parts grab
attention and encourage awareness! Put key points in first paragraph! Text needs to be brief (max. A4)! Use language appropriate for the audience! Advocate for health in general! Share credit and visibility with partners
by authority
RISK CO
MM
UN
ICA
TION
POCKET EMERGENCY TOOL
76
APPENDICES
POCKET EMERGENCY TOOL
77
EMERG
ENC
Y MA
NA
GER D
EPLOYM
ENT C
HEC
KLIST
POCKET EMERGENCY TOOL
This list contains basic supplies, materials, equipment needed in the field.
YES NO1. Did you receive your orders?2. Is/are the mission objective/s clear? 3. Did you inform your family?4. Do you have with you
a. Mission order? b. Identification card? c. Emergency call number directory?d. Mission area map?e. List of contact persons/numbers?f. Communication equipment?g. Cell phone? Mobile phone? h. Handheld radio & accessories?i. Pocket notebook & ball pen? j. Laptop computer?k. Transistor radio (with extra batteries)?l. Basic PPE (cap, mask, gloves)?m. Cash & reimbursement vouchers?n. Water canteen?o. Food provisions?p. First aid kit?q. Backpack with clothing & blanket?r. Flashlight/candles & matches?s. Portable tent (if available)?t. Mosquito repellent?u. Pocket knife?v. Digital camera?w. Pocket Emergency Tool?
78
POCKET EMERGENCY TOOL
RAPI
D H
EALT
H A
SSES
SMEN
T FO
RMS HEMS FORM 1
RAPID HEALTH ASSESSMENT(To be submitted within 24 hrs)
as of ____________________.
Nature of Event: ___________________________________________Date and Time of Occurrence: ________________________________Region: __________________________________________________
A. Magnitude of Event
B. Consequences
No. of Families &
No. of No. of No. of IndividualsMunicipality Families Individuals Evacuation in Evac'n
Province /City Affected Affected Centers Centers
TOTAL
Municipality /City No. of Death/s No. of Injured No. of Missing
TOTAL
79
C. Health Facilities Available in Affected Area
D. Lifelines Available in Affected Area
E. Status of Essential Drugs/Suppliers
Stock level good for ________________________________ (no. of cases/no. of days/weeks/month)
F. Actions Taken
\
G. Problems Encountered
Total No. No. of Functional No. of Non Functional RemarksHospitalsGov'tPrivateRHUOthers
Type Yes No RemarksCommunicationsElectric PowerWaterRoads/BridgesOthers
Nature of the Event: ________________________________Time of the Event: _________________________________Date of the Event: _________________________________Place of the Event: _________________________________
Treated on site: _________________________________Referred to hospital: _____________________________OPD: _________________________________________Admitted: ______________________________________
* Please fill up Form A for the listing of cases.HEMS FORM III
RAPID HEALTH ASSESSMENTFOR OUTBREAKS
A. Description of the Event
Nature of the Event: _______________________________Time of the Event: _________________________________
RAPID
HEA
LTH A
SSESSMEN
T FORM
S
POCKET EMERGENCY TOOL
82
Date of the Event: _________________________________Place of the Event: ________________________________
B. Consequences
Population Exposed: _______________________________Number of Death/s: ________________________________Number of Cases: _________________________________
Age Groups Average % in Population 0 — 4 years 12.45 — 9 years 11.710 — 14 years 10.515 — 19 years 9.520 — 59 years 48.6*Pregnant women 2.4
WaterQuantityQuality
SanitationLatrine
Waste disposal
SoapShelter
Individual requirementsCollective requirements
Household fuelWeight of firewood
20 L/person/day200 persons/water pointIn hospital settings more water per person is needed
Ideally one per family; minimum of one seat per 20 persons 6 to 50 meters from housing1 communal pit per 500 persons; size: 2 m x 5 m x 2 m250 g/per person/per month
24m /person
230m /personincluding shelter, sanitation, services, community activities, warehousing access
15 kg/household/daywith one economic stove per family, the needs may be reduced to 5 kg/stove/day
Average Requirements
85
REFERENC
E VALU
ES FOR RA
PID H
EALTH
ASSESSM
ENT A
ND
CO
NTIN
GEN
CY PLA
NN
ING
POCKET EMERGENCY TOOL
Emergency Food Requirements
Recommended ration person/day: 2,116 kcalTotal kg/person/month for alimentation: 16.4 kg
Examples of Rations for General Food Distribution(Providing 2100 kcal/person/day)
Micronutrients (e.g., iodine, Vit. A) are important.
Food kcal content g/person/month
Cereals 350/100 g 13.5Pulses 335/100 g 1.5Oil (vegetable) 885/100 g 0.8Sugar 400/100 g 0.6
- As available -
Continued on next page
Commodities
Meal with ricePulses
(i.e. peas, beans, mongo)
Oil/fat
Fortified cereal
Canned fish/meat
Sugar
Salt
Vegetables/fruits
Ration 1
(g)45050
25
-
-
20
5
Ration 2
(g)42060
30
-
30
20
5
Ration 3
(g)40060
25
50
-
15
5
Function
Main source of energy and proteinProvide protein and various micronutrients
Concentrated source of energy for palatability and the absorption of Vit. AProvides essential vitamins and minerals, and is useful as weaning foodNeeded for proteins and minerals (including iron)Needed for cultural habits, palatability, and home oral rehydrationProvides sodium, and is needed for home oral rehydrationValuable source of vitamins and minerals
86
Condiments/spicesApproximate food
value:Energy (kcalProtein (gFat (g)
21165141
20924538
21135843
Needed because of cultural habits and for palatability
50% of pregnancies/month1/12 of total group per month1.5 per person/yr0.13 per person/month4 per outpatient consultation
30% per month
1/12 of total group per month1/12 of total group per month1/12 of total group per month1/12 of total group per month
POCKET EMERGENCY TOOL
REFE
REN
CE
VALU
ES F
OR
RAPI
D H
EALT
H A
SSES
SMEN
T A
ND
CO
NTI
NG
ENC
Y PL
AN
NIN
G87
Hospital:Population ratio 1:150,000 to 300,000
Normal staffing:2 medical officers 1:500 or 1:100060-100 other staff CHWs
(or home visitors) or 1 person/day = 7 hoursHealth Information Teams of field work
Health Personnel Requirements
Health Workers Emergency requirements (e.g. refugee camp) for treatments, management and clerical duties: 60 staff x 10,000 population
Health Supplies Requirements
Essential drugs and medical equipment
Safe water
WHO Basic NEHK UnitWHO Supplementary NEHK Unit
Preparing 1 L of stock solution 1%
Using the stock solution
1 kit for 10,000 pop for 3 mos.1 kit for 10,000 pop for 3 mos.
calcium hypochlorite 70%: 15 g/L of waterbleaching powder 30%: 33 g/L of watersodium hypochlorite 5%: 250 ml/L of watersodium hypochlorite 10: 110 ml/L of water0.6 ml or 3 drops/liter of water60 ml/100 liters of water
Allow the chlorinated water to stand at least 30 minutes before using.
POCKET EMERGENCY TOOL
REFERENC
E VALU
ES FOR RA
PID H
EALTH
ASSESSM
ENT A
ND
CO
NTIN
GEN
CY PLA
NN
ING
88
Health Status
Daily Crude Mortality RateDaily Under-5 Mortality RateAcute Malnutrition (W/H or MUAC) in
Under-5Growth Faltering Rate in Under-5Low Weight at Birth (<2.5 kg)
More than
1 per 10,000 population2 per 10,000 children <5 y/o10% of children <5 y/o
30% of monitored children7% of live births
Cut-off Values for Emergency Warning
POCKET EMERGENCY TOOL
REFE
REN
CE
VALU
ES F
OR
RAPI
D H
EALT
H A
SSES
SMEN
T A
ND
CO
NTI
NG
ENC
Y PL
AN
NIN
G89
NCHS/WHO normalized reference values for weight-for-length (49-84) and weight-for-height (85-110 cm) by sex.
1. Length is generally measured in children below 85 cm, and height in children 85 cm and above. Recumbent length is on average 0.5 cm greater than standing height; although the difference is of no importance to the individual child, a correction may be made by deducting 0.5 cm from all lengths above 84.9 cm if standing height cannot be measured.
POCKET EMERGENCY TOOL
REFE
REN
CE
VALU
ES F
OR
RAPI
D H
EALT
H A
SSES
SMEN
T A
ND
CO
NTI
NG
ENC
Y PL
AN
NIN
G93
2. SD = standard deviation score (or Z-score). The relationship between the percentage of median value and the SD-core or Z-score varies with age and height, particularly in the first year of life, and beyond 5 years. Between 1 and 5 years median -1 SD and median -2 SD correspond to approximately 90% and 80% of median (weight-for-length, and weight-for-age), respectively. Beyond 5 years of age or 110 cm (or 100 cm in stunted children) this equivalence is not maintained; median 02 SD is much below 80% of media. Hence the use of “percentage-of-median” is not recommended, particularly in children of school age. Somewhere beyond 10 years or 137 cm, the adolescent growth spurt begins and the time of its onset is variable. The correct interpretation of weight-for-height data beyond this point is therefore difficult
POCKET EMERGENCY TOOL
REFERENC
E VALU
ES FOR RA
PID H
EALTH
ASSESSM
ENT A
ND
CO
NTIN
GEN
CY PLA
NN
ING
94
Decision Framework for Implementing Selective Feeding Programs
Findings
Serious situation:Malnutrition rate: = 15%or 10-14%, plus aggravating
factors
Alert/Risky situation:Malnutrition rate: 10-14% Or 5-9%, plus aggravating
factors
Unsatisfactory situation:Food availability at household level below 2100 kcal per person per dayAcceptable situation:Malnutrition rate: < 10% with no aggravating
factors
Actions Required
! 'Blanket' supplementary feeding for all members of vulnerable groups (especially children, pregnant and lactating women, adults showing signs of malnutrition)
! Therapeutic feeding programs for severely malnourished individuals
! Targeted supplementary feeding for individuals identified as malnourished in vulnerable groups (mildly to moderately malnourished children under 5 years, selected other children and adults)
! Therapeutic feeding programs for severely malnourished individuals
! Improve general rations until local food availability and access can be made adequate
! No need for population interventions! Attention for malnourished
individuals through regular community services
POCKET EMERGENCY TOOL
REFE
REN
CE
VALU
ES F
OR
RAPI
D H
EALT
H A
SSES
SMEN
T A
ND
CO
NTI
NG
ENC
Y PL
AN
NIN
G95
1. Malnutrition rate: defined as the percentage of the child population (6 months to 5 years) who are below either the reference median weight-for-height minus 2 SD or 80% of reference weight-for height and/or with edema.
2. Aggravating factors: ! Food availability at household level less
than the mean energy requirement of 2100 kcal/person/day
! Crude mortality rate more than 1 per 10,000 per/day
! Epidemic of measles or whooping cough! High incidence of respiratory or
diarrheal diseases
POCKET EMERGENCY TOOL
REFERENC
E VALU
ES FOR RA
PID H
EALTH
ASSESSM
ENT A
ND
CO
NTIN
GEN
CY PLA
NN
ING
96
Description
Severe disorder (e.g., psychosis, severe depression, severely disabling form of anxiety disorders, etc.)Mild or moderate mental disorder(e.g., mild and moderate forms of depression and anxiety disorders including PTSD)
Moderate or severe psychological distress that does not meet criteria for disorder, that resolves over time ormild distress that does not resolve over timeMild psychological distress, that resolves over time
Before Disaster: 12 month
prevalence rates
2-3 %
10%
No estimate
No estimate
After Disaster: 12 month
prevalence rates
3-4%
20%(which over the years reduces to 15% through natural recovery without intervention)
30-50%(which over the years will reduce to an unknown extent)
20-40%(which over the years increase as people with severe problems recover)
Type of aid recommendations
Make mental health care available through general health services and in community mental health services1. Make mental health care available through general health services and in community mental health services2. Make social interventions and basic psychological support interventions available in the communityMake social interventions and basic psychological support interventions available in the community
No specific aid needed
Summary Table on Projecting Psychosocial/Mental Health Assistance
These rates vary with setting (e.g. sociocultural factors, previous and current disaster
exposure) and assessment method but give a very rough indication what WHO expects the
extent of morbidity and distress to be.
POCKET EMERGENCY TOOL
REFE
REN
CE
VALU
ES F
OR
RAPI
D H
EALT
H A
SSES
SMEN
T A
ND
CO
NTI
NG
ENC
Y PL
AN
NIN
G97
Good communications are essential for management and security. Use the correct prowords and phonetic alphabet. Spell only important words.
Numerals should be transmitted digit by digit except round figures as hundreds and thousands. Repeat only important numbers.
Check your equipment regularly.
A — Alpha N — November
B — Bravo O — Oscar
C — Charlie P — Papa
D — Delta Q — Quebec
E — Echo R — Romeo
F — Foxtrot S — Sierra
G — Golf T — Tango
H — Hotel U — Uniform
I — India V — Victor
J — Juliet W — Whiskey
K — Kilo X — X-ray
L — Lima Y — Yankee
M — Mike Z — Zulu
RAD
IO PRO
CED
URES
POCKET EMERGENCY TOOL
98
METRIC TO ENGLISH ENGLISH TO METRIC
Length
Surfaces
Volumes
Weights
To convert into Multiply by To convert into Multiply by
mm inches 0.03937 inches mm 25.4cm inches 0.3937 inches cm 2.54meters inches 39.37 inches meters 0.0254meters feet 3.281 feet meters 0.3048meters yards 1.0936 yards meters 0.9144km yards 1093.6 yards km 0.0009144km miles 0.6214 miles km 1.609
2 2cm sq. inches 0.155 sq. inches cm 6.4522 2m sq. feet 10.764 sq. feet m 0.09292 2m sq. yards 1.196 sq. yards m 0.8361
2 2km sq. miles 0.3861 sq. miles km 2.59hectares acres 2.471 acres hectares 0.4047
3 3cm cubic inches .06102 cubic inches cm 16.3873 3m cubic feet 35.314 cubic feet m 0.0283173 3m cubic yards 1.308 cubic yards m 0.76463 3m gallons (US) 264.2 gallons (US) m 0.003785
grams grains 15.432 grains grams 0.0648grams ounces 0.03527 ounces grams 28.35kg ounces 35.27 ounces kg 0.02835kg pounds 2.2046 pounds kg 0.4536kg ton (US) 0.001102 ton (US) kg 907.44kg ton (long) 0.000984 ton (long) kg 1016.0metric ton pounds 2204.6 pounds metric ton 0.0004536metric ton ton (US) 1.1023 ton (US) metric ton 0.9072metric ton ton (long) 0.9842 ton (long) metric ton 1.0160
POCKET EMERGENCY TOOL
CO
NV
ERSI
ON
TA
BLE
99
TemperatureCentigrade to Fahrenheit: Multiply by 1.8 and add 32Fahrenheit to Centigrade: Subtract 32 and multiply by 0.555
Weight of water by volume (at 16.7°C or 62°F):1 liter = 1 kg 1 UK gallon = 10 pounds1 UK gallon = 1.2 US gallons 1 UK gallon = 4.54 liters1 US gallon = 0.8333 UK gallons 1 US gallon = 8.33 pounds1 US gallon = 3.79 liters 1 liter = 0.26 gallons1 cubic foot = 62.3 pounds
CO
NV
ERSION
TABLE
POCKET EMERGENCY TOOL
100
NAME ADDRESSNational
Asian
WHO
Other UN Agencies
Department of Health-Philippines (DOH) http://www.doh.gov.phNational Disaster Coordinating Council (NDCC) http:/www.ndcc.gov.phPhil. Atmospheric, Geophysical and Astronomical http://www.pagasa.dost.gov.ph
Services Administration (PAGASA)Phil. Institute of Volcanology & Seismology http://www.phivolcs.dost.gov.ph
(PHIVOLCS)Phil. Nuclear Research Institute (PNRI) http://www.dost.gov.ph/pnriPhil. National Red Cross http://www.redcross.org.ph
Asian Disaster Preparedness Center (ADPC) http://www.adpc.ait.ac.thAsian Disaster Reduction Center (ADRC) http://www.adrc.or.jpAsian Disaster Reduction & Response Network http://www.adrrn.net
Emergency and Humanitarian Action (EHA) http://www.who.int/disastersRegional Office for the Western Pacific http://www.wpro.who.int/sites/eha
and Response ProgrammePan-American Health Organization http://www.paho.org/english/ped
(PAHO)- Disasters & Humanitarian AssistanceRegional Office for the South-East Asia (SEARO) http://w3.whosea.org/index.htmEssential Drugs and Medicines policy http://www.who.int/medicinesInjuries and Violence Prevention http://www.who.int/violence_injury_
preventionMental Health http://www.who.int/mental_healthNutrition http://www.who.int/nutReproductive Health http://www.who.int/reproductive_healthWater and Sanitation http://www.who.int/water_sanitation
_healthPAHO SUMA http://www.disaster.info.de
sastres.net/SUMACentro Regional de Informacion Sobre Desastres http://www.crid.or.cr/cridHealth Library for Disasters http://www.helid.desastres.net
UNAIDS http://www.unaids.orgUN Disaster Management Training Program http://www.undmtp.org
(UNDMTP)UN Environmental Programme http://www.unep.orgUN High Commissioner for Refugees (UNHCR) http://www.unhcr.chUN International Children's Educational Fund http://www.unicef.org
(UNICEF)
Continued on next page
POCKET EMERGENCY TOOL
WEB
SITE
S101
NAME ADDRESS
Other International Organizations
UN International Strategy for Disaster Reduction http://www.unisdr.orgUN Population Fund http://www.unpfa.orgUN Office for the Coordination of Humanitarian http://ochaonline.un.org
Affairs (UN-OCHA)World Bank http://www.worldbank.orgWorld Food Programme http ://www.wfp.org
Emergency Management Australia (EMA) http://www.ema.gov.auFederal Emergency Management Agency http://www.fema.gov
(FEMA), USACenters for Disease Control & Prevention http://www.cdc.gov
(CDC), USAAgency for Toxic Substances and Disease Registry http://atsdr1.atsdr.cdc.gov:8080/
hazdat.htmlEM-DAT: Center for Epidemiology and Disaster http://www.cred.be/emdat/
(CRED) International Disaster DatabaseDatabases on Emergency Statistics and http://www.md.ucl.ac.be/entites/
Bibliographic References (CRED) esp/epid/missionInternational Directory of Emergency Centers http://www.oecd.org/dataoecd/
for Chemical Accidents (2000) 0/39/1933385.pdfWorld Meteorological Organization http://wmo.ch/web/www/reparts/
expert-ERA-0498.htmlAlertnet http://www.alertnet.orgDisaster Relief http://www.disasterrelief.orgInternational Committee of the Red Cross http://www.icrc.orgInternational Federation of Red Cross and Red http://www.ifrc.org
Crescent SocietiesMedecins Sans Frontiers http://www.msf.orgOne World http://www.oneworld.netOrganization for Economic Co-operation http://www.oecd.org
and Development Relief Web http://www.reliefweb.intRefugee Nutrition Information System http://acc.unsystem.org/scn/
publications/html/rnis.htmlReproductive Health for Refugee Consortium http://www.rhrc.org
(RHRC)Sphere Project http://www.sphereproject.orgAmerican College of Emergency Physicians (ACEP) http://www.acep.orgNatural Hazards Center at the University http://www.colorado.edu/hazards
of ColoradoCentral Investigation Agency (CIA) Factbook http://www.cia.gov/cia/publications/
factbook
Websites continued
WEBSITES
POCKET EMERGENCY TOOL
102
General1. WHO. Essentials for emergencies.2. WHO. (2003). Emergency response manual (provisional version).3. CDC. Public health emergency response guide for State, Local, and
Tribal Public Health Directors Version 1.0. Atlanta, Georgia: Centers for Disease Control and Prevention.
4. Sphere Project (2004). Humanitarian charter and minimum standards in disaster response. Geneva: The Sphere Project.
5. UP Open University/DOH/WPRO. Emergency Medical Services System Manual. Postgraduate Course in Health Emergency Management, Module 3: Public Health Issues in Emergencies. August 14-20, 1999.
6. UP Open University/DOH/WPRO. Emergency Medical Services System Manual. Postgraduate Course in Health Emergency Management, Module 5: Emergency Medical Services System. August 14-20, 1999.
Communicable Diseases1. WHO (2005). Communicable disease control in emergencies: A field
manual. Geneva: World Health Organization.2. WHO (2004). Technical note: Post-tsunami flooding and
communicable disease risk in affected Asian countries. Geneva: World Health Organization.
Nutrition1. WHO (2003). Guiding principles for feeding infants and young
children during emergencies. Geneva: World Health Organization.2. Joint UNICEF WHO ISP (2005). Recommendations on infant
feeding in emergencies. Jakarta, Indonesia January 7, 2005.
Environmental Health1. WHO (2004). Management of solid health-care waste at primary
health-care centres: A decision-making guide. Geneva: World Health Organization.
POCKET EMERGENCY TOOL
REFE
REN
CES
103
2. WHO/SEARO. (2005) Planning Emergency Sanitation. Technical Notes in Emergencies, Technical Note No. 12. India: WHO/Regional Office for South Asia.
3. Lacarin, CJ and Reed RA (1999) Emergency Vector Control Using Chemicals, Water, Engineering and Development Center (WEDC), Loughborough.
Psychosocial Care and Mental Health1. WHO. (2003). Mental health in emergencies: psychological and
social aspects of health of populations exposed to extreme stressors. Geneva: World Health Organization.
2. WHO. (2005). Mental health and psychosocial care of children in disasters. Geneva: World Health Organization.
3. WHO. (2005). Mental health of populations exposed to biological and chemical weapons. Geneva: World Health Organization.
Management of Dead Bodies1. PAHO (2004). Management of dead bodies in disaster situations.
Washington DC: Pan American Health Organization.2. WHO/SEARO. (2005), Disposal of dead bodies in emergency
conditions. Technical Note No.8. India: WHO/Regional Office for South Asia.
Resource Managementnd1. WHO. (1999). Guidelines for drug donation 2 ed. Geneva: World
Health Organization.
Risk Communication1. CDC (2002). Crisis and emergency risk communication. Atlanta,
Georgia: Centers for Disease Control and Prevention.
REFERENC
ES
POCKET EMERGENCY TOOL
104
Organization Hotline Number/sAFR Reserve Command-Rescue and Emergency Medical Team 921-3746AFP-Office of the Surgeon General (AFP-OTSG) 911-6509
911-6001 loc. 6416Assoc. of Phil. Volunteer Fire Brigades, Inc. 522-2222Assoc. of Volunteer Fire Chiefs & Firefighters of the Phil., Inc. 160-16Bureau of Fire Protection (BFP) 928-8363EARNET Network 911-9009DOH-Dengue 723-2493DOH OPCEN 929-6919/929-6853
743-1937/741-7048Metro Manila Development Authority (MMDA)
Road Emergency Group 882-0851EARNET Network 136
National Disaster Coordinating Council (NDCC) 912-5668National Poison Control Control & Information Service 524-1078/404-0257
5218450 local 2311National Voluntary Blood Center 929-6274Office of Civil Defense (OCD) Operation Center 911-1406/912-2556Philippine Atmospheric, Geophysical and Astronomical 929-4570/927-1541
Coast Guard Medical 301-9369Philippine General Hospital (PGH)
EARNET Network 523-5350521-8450 loc. 3166
Philippine Institute of Volcanology and Seismology (PHIVOLCS) 426-1468/927-1104Philippine Long Distance Telephone Company (PLDT) 171Philippine National Police (PNP) Patrol 117 117Philippine National Red Cross (PNRC)
EARNET Network 527-0864Disaster Management 527-8384 loc 133/134PNP Firearms and Explosives 724-8085Quezon City Rescue-Sagip Buhay
EARNET Network 928-4396
POCKET EMERGENCY TOOL
EMER
GEN
CY
CA
LL N
UM
BER
DIR
ECTO
RY105
CHD Coordinator Tel No./Cell No.CHD I Ms. Michelle Dumbrique (075) 515-6842
0928-2979687CHD II Dr. Baldomero Lasam (078) 844-6585
0927-3046479CHD III Dr. Nemesio Santos (045) 961-3802
0917-4586351CHD IV-A CALABARZON Dr. Noel Pasion (02) 913-0864
0920-2290001CHD IV-B MIMAROPA Dr. Aurora Enojado (02) 995-0827
020-9242841CHD V Dr. Juancho Gideon Torres (052) 483-0840 loc 513
0919-4704465CHD VI Mr. Jerry Porras, RN (033) 321-0607 loc 15
0919-5555194CHD VII Mr. Rennan Cimafranca, RN (032) 418-7629
0917-3248741CHD VIII Atty. Anabelle De Veyra, RN (053) 323-5025
0920-2587119CHD IX Dr. Marcos Redoble Jr. (062) 9911313
0919-3424124CHD X Dr. Marianne Trabajo (088) 350-4322
0918-4477173CHD XI Dr. Paolo Pantojan (082) 224-3011
0927-7798177CHD XII Mr. Leo Chiong, RN (064) 421-4583
0920-2031559CHD-Metro Manila Dr. Marilyn Go (02)535-1488