53
DELIRIUM DEPRESSION, DEMENTIA
DELIRIUMDEPRESSION, DEMENTIA

Disclosure
1. What delirium is
2. Why we care about delirium in geriatric oncology
3. Causes and mechanisms of delirium
4. How delirium can be diagnosed
5. How delirium can be differentiated from dementia, depression, psychosis
6. How to treat delirium


Delirium
• Definition
– reduced ability to focus, sustain, or shift
attention
– change in cognition or the development of a
perceptual disturbance
– Acute onset (hours to days)
– Fluctuations
– Identifiable cause



• Hyperactive– Patient is hyperactive, agitated, not cooperative, combative
– Rapid speech, irritability, restlessness– Patient shows high resistance to care
Clinical Subtypes
• Hypoactive
– lethargy, apathy
– Inability to focus when awake
– Lack of appetite
– Slowed speech
– Decreased alertness
– Absence of care request
• Mixed
Shift between hyperactive and hypoactive states

In 12 studies the prevalence of delirium subtypes has varied widelya metanalysis of these studies suggests the following figures:
Prevalence (%) Range(%)
hypoactive 48 15-71
hyperactive 24 13-46
mixed 36 11-55
Clinical Subtypes

• Overall incidence among hospitalized geriatric patients (over 65) up to 56%
• 15-53% post surgery geriatric patients • 50% post hip fracture geriatric patients• 70-80% geriatric patients in ICU • 60% nursing home residents at least once during their stay
• Up to 30% hospitalized geriatric patients with cancer• Up to 44% of advanced cancer patients at the time of admission to an acute care hospital or palliative care unit
• Over 85% cancer patients in the days and hours before death
EPIDEMIOLOGY

• Mortality rate in hospitalized patients 22-76%
• One year mortality rate is 35-40%• Prolongs hospital course• Increased cost of care in hospital• Increased likelihood of disposition to nursing home, functional decline and loss of independence
CONSEQUENCES

– Delirium is not diagnosed in up to 70% of cases– Symptoms are mistakenly attributed to age, dementia or other mental disorders.
– It is common, serious, costly, under-recognisedand often fatal
– 164 billions per year in US, 182 billions per year in Europe:
Hospital costs (> $11 billion/year US)
Post-hospital costs (including rehospitalization, emergency department visits, institutionalization, rehabilitation, formal home care services (>$153 billion/year US)
DELIRIUM: WHY SHOULD WE CARE ?

• Strong association with underlying dementia
• Frequently, patient may never return to baseline or take months to over a year to do so
• Delirium is often the sole manifestation of serious underlying disease
More reasons to care

A multifactorial syndrome that arises from an interrelationship between:
• Predisposing factors� a patient’s underlying vulnerability
AND
• Precipitating factors� noxious insults
ETHIOLOGY

Precipitating factors
/insults
Predisposing factors
/vulnerability
High vulnerability
Low vulnerability
dementia
severe
illness
advanced
cancer
social
support
high self
efficacy
sleep
deprivation
Major
surgery
ICU stay
medications
High noxious insults
low noxious insults

• Age • Male gender• Neurosensorialimpairment
• Dementia• Depression • Brain diseases (including cancer, stroke)
• Major surgery
• Advanced cancer• Functional impairment
• Dehydration• Alcohol, drug abuse• Hip fracture• Polypharmacy
Predisposing factors

• Medications
• Bedrest
• Indwelling bladder catheters
• Physical restraints
• Organ failure
• Uncontrolled pain
• Fluid/electrolyte abnormalities
• Infections
• Medical illnesses
• Urinary retention and fecal impaction
• ETOH/drug withdrawal
• Environmental influences
Precipitating factors

D Drugs, Drugs and toxins, tooE Eyes, earsL Low O2 states (MI, ARDS, PE, CHF, COPD,
stroke, shock)
I InfectionR Retention (of urine or stool). RestraintsI IctalU Underhydration, UndernutritionM Metabolic (hypo/hyper glycemia, calcemia, uremia,
liver failure, thyroid disorders)
Cause

Medicationsaccount for 30% of all cases

• Medications with psychoactive effects: – 3.9-fold increased risk
– 2 or more meds: 4.5-fold
• Sedative-hypnotics: 3.0 to 11.7-fold
• Narcotics: 2.5 to 2.7-fold
• Anticholinergic drugs: 4.5 to 11.7-fold
• Risk of delirium increases as number of meds prescribed rises

DELIRIUM
Cancer byproducts,
proinflammatory cytokines
Medications, opioids,
corticosteroids, others
Side effects of radiation,
chemotherapy
Other medical
conditions e.g.
nutritional deficiencies,
anemia, other
hypoxemia
infections
Endocrine
e.g.hypoglicemia,
hypothyroidism
Paraneoplastic syndromes
Organ failure (hepatic, renal,
cardiac
Electrolyte imbalance
e.g. hypercalcemia,
hyponatremia,
hypernatremia,
hypomagnesemia
Intracranial disease
e.g. primary and metastatic
brain tumor, leptomeningeal
disease, stroke
Factors contributing to delirium in cancer patients

Maldonado J. Am J Geriatr Psych 2013

• Involves– Neurotransmission
– Inflammation
– Chronic/acute stress
Pathophysiology

• Neurotransmission– Cholinergic deficiency
• Anticholinergics can precipitate delirium
• Serum anticholinergic activity increased in those with delirium
• Cholinesterase inhibitors can reverse this effect
– Dopaminergic excess
– Neuropeptides, endorphins, serotonin, NE, GABA , histamine, may play a role.

A schematic diagram showing how various risk factors can affect acetylcholine and dopamine levels, leading to delirium.
Benjamin D. Robertson, and Timothy J. Robertson J Bone Joint Surg Am 2006;88:2060-2068
©2006 by The Journal of Bone and Joint Surgery, Inc.
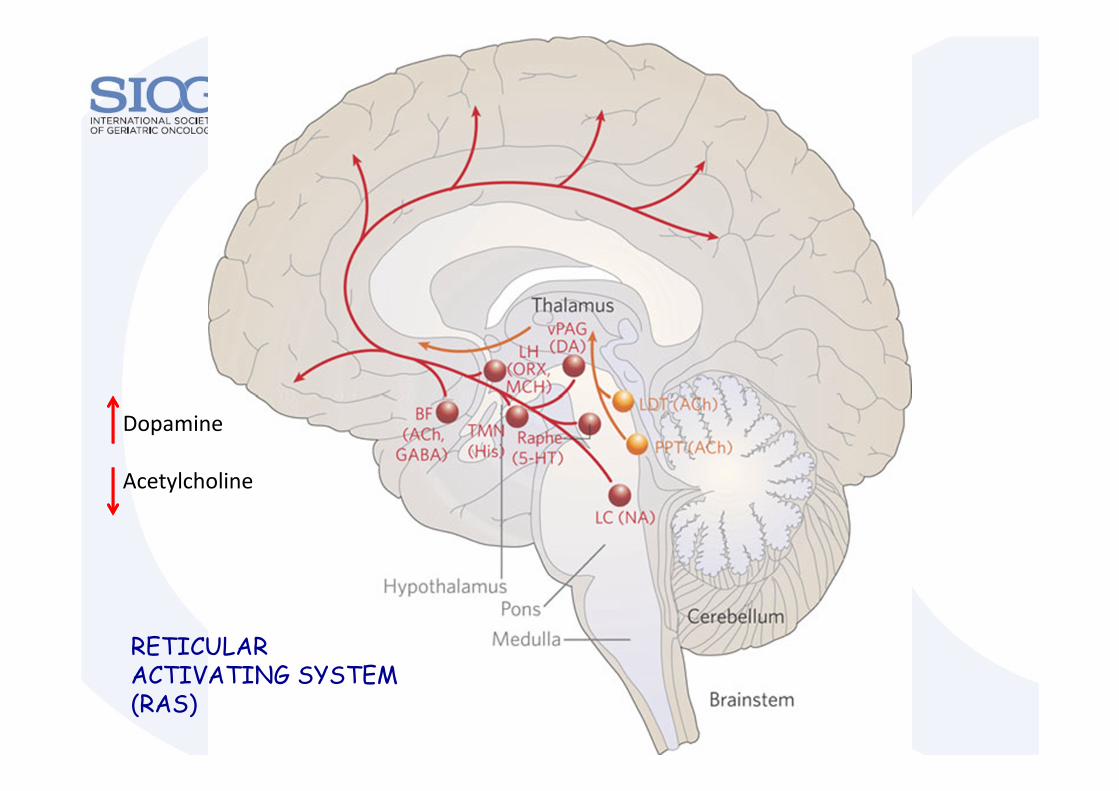
Dopamine
Acetylcholine
RETICULAR ACTIVATING SYSTEM (RAS)
INFLAMMATION
• Cytokines– Interleukins and interferons, often elevated in Delirium, have known strong CNS effects
– Increased blood brain barrier permeability
– Primary role – sepsis, bypass surgeries, dialysis, cancers

• Chronic/Acute stress– Untreated pain / analgesia are strong risk factors
– Elevated cortisol associated with delirium
– Sympathetic system activation
– Hypothalamic pituitary adrenal axis hyperactivity

Diagnosis
• History (previous mental status, medications)
• Physical exam, lab test, other test to identify medical cause (infections, hydration status, other).
• Mental status exam: inattention, decreased level of consciousness, disordered speech, disorganizedthinking

30
Delirium: Physical Exam
Examine for signs of: � Hypoxia� Volume depletion/overload� Cardiovascular injury� Metabolic encephalopathy � Alcohol withdrawal� Hypo- or hyperthermia� New onset incontinence� Urinary retention or fecal impaction

31
Delirium: Diagnostic Tests
Choice based on history and physical findings Baseline laboratory studies:• Urinalysis• Basic or Comprehensive Metabolic Panel• Blood work: CBC, Thyroid function test
Further diagnostic testing (based on exam):• Head CT• EKG • Chest X-Ray

32
• When difficult to
differentiate delirium
from acute psychotic
state
Electroencephalography
The electroencephalogram reveals:
Diffuse slowing in most cases of delirium
Fast activity in cases of delirium related to drug withdrawal
Normal patterns in patients with acute functional psychosis
Delirium: Diagnostic Tests

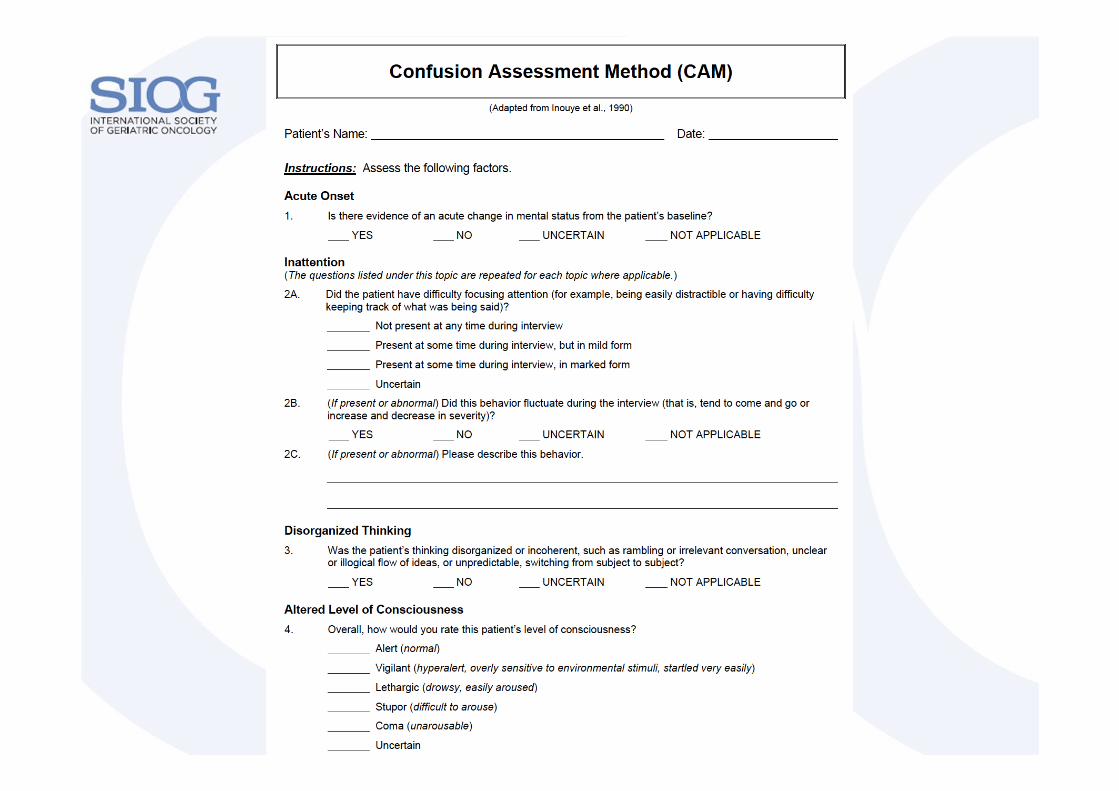
Delirium Assessment Tools
Diagnostic interview instruments:
- Confusion Assessment Method (CAM)
- Delirium Symptom Interview (DS)
Delirium Rating Scales:
- Delirium rating scale (DRS)
- Confusion Rating Scale (CRS)
- Memorial Delirium Assessment Scale (MDAS)
Cognitive status screening tools:
- Mini Mental State Examination (MMSE)
- Short portable mental status questionnaire (SPMSQ)


Delirium
Rating
Scale

Mini Mental State
Examination (MMSE)
Folstein 1975

Recognize KEY symptoms• Disturbance in attention and consciousness • Cognitive changes
– Attention – poor– loss of mental clarity
• Patient “isn’t acting right”– Disordered speech– Disorganized thought– Acute memory loss– Disorientation
• Acute/subacute onset• Perceptual disturbances (delusions, hallucinations)• Fluctuating course throughout a day

39
Differentiating Delirium from Dementia
• Chronic cognitive impairment seen in dementia typically:
– Occurs gradually over time
– Persists greater than one month
– Starts with memory impairment
– Is irreversible
• Most older adults with dementia are alert and able to maintain attention in the early stages of dementia
• Dementia with Lewy Bodies includes fluctuating cognition and visual hallucinations
– 2.5 fold increased risk of delirium in dementia patients
– 25-31% of delirious patients have underlying dementia
– DSD has been associated with worse recovery and higher mortality compared to dementia or delirium
Delirium superimposed on dementia(DSD)


42
Differentiating Delirium from Depression
• Depression may also present acutely with deficits in ability to sustain attention.
• Depression may present similar to hypo- or hyper-active delirium; therefore, it is important to screen for depression in older adults who present with a mixed picture (previous medical history, mood status assessment).
• Severe cognitive and psychotic symptoms are rare in mild depression.

Keys to Effective Management
• Find and treat the underlying disease(s) and contributing factors– Comprehensive history and physical
– Including neurological and mental status exams
– Choose lab tests and imaging studies based on the above
– Review medication list

Nonpharmacologic Measures First
• Presence of family members
• Interpersonal contact and reorientation
• Provide visual and hearing aids
• Remove indwelling devices: i.e. Foley catheters
• Mobilize patient
• A quiet environment with low-level lighting
• Uninterrupted sleep
Pharmacologic Management
• Use drugs only if absolutely necessary• First line agent: haloperidol (IV, IM, or PO)
– For mild delirium: • Oral dose: 0.25-0.5 mg• IV/IM dose: 0.125-0.25 mg
– For severe delirium: 0.5-1 mg IV/IM repeated q30 min until calm
• Patient will likely need 2-5 mg total as a loading dose
– Maintenance dose: 50% of loading dose divided BID
• May use olanzapine and risperidone (Lonergan E et al. Cochrane Database Syst Rev. 2007 Apr 18; (2): CD05594)

Fig.8
Dopaminergic Pathways

haloperidol Clozapine
Olanzapine Risperidone
Alpha 1
D1
D2
D4
5-HT2A
5-HT2C
H1
M1
J Pharmacol Exp Ther 1996;277:968;J Clin Pharmacol 1999;39:1S;Psychopharmacology 1993;112:S60;Am J Psychiatry 1997;154:782.
Antipsychotic receptor profiles
Conventional antipsychotic side effects
Anticholinergic
• Dry Mouth
• Constipation
• Cardiovascular (Othostatichypotentions, QT interval)
Antihistaminic
• Sedation, Weight Gain
Dopamine Blockade:
• ExtrapyramidalSide Effects
• Hyperprolctinemia• NeurolepticMalignant Syndrome

Metabolic Syndrome, Hyperglycemia,HyperlipidemiaWeight GainQT Interval Prolongation, Torsade des Pointes(ECG should be monitored daily during delirium treatment)Consider interactions with other agents thatprolong QTEPS dose dependentIncreased risk of stroke and death
Atypical antipsychotic side effects

Pharmacologic Management
• second line agent: BDZ( e.g. lorazepam)
– Reserve for: • Sedation
• Alcohol/drug withdrawal syndrome
• Parkisnon’s disease
SSRI for hypoactive delirium
Cholinesterase inhibitors, anticonvulsants, antihistamines, clonidine have not beenassessed in delirium
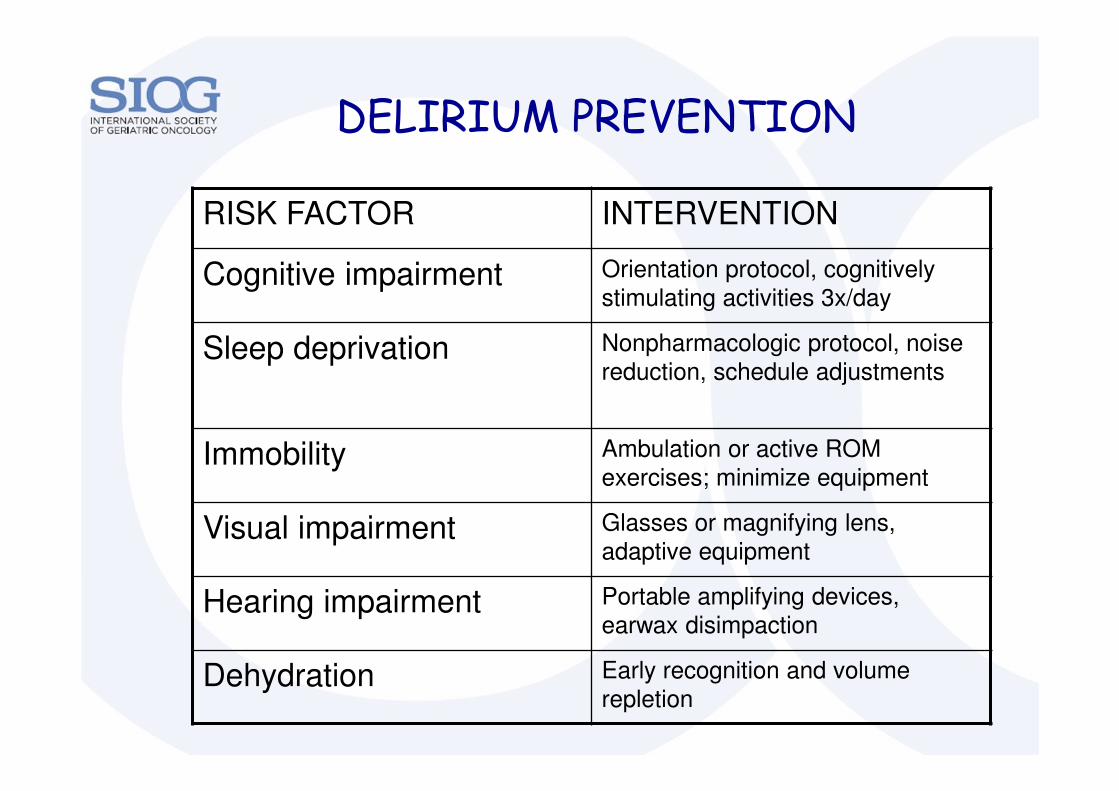
DELIRIUM PREVENTION
RISK FACTOR INTERVENTION
Cognitive impairment Orientation protocol, cognitively
stimulating activities 3x/day
Sleep deprivation Nonpharmacologic protocol, noise
reduction, schedule adjustments
Immobility Ambulation or active ROM
exercises; minimize equipment
Visual impairment Glasses or magnifying lens, adaptive equipment
Hearing impairment Portable amplifying devices, earwax disimpaction
Dehydration Early recognition and volume repletion

AVOID RESTRAINTS AT ALL COSTS:Measure of LAST(!!!) resort

Take Home Points
• Delirium is common among elderly patients with advanced cancer
• It is a multifactorial syndrome: predisposing vulnerability and precipitating insults
• Prevention should be the goal
• If delirium occurs, treat the underlying causes
• Always try non-pharmacologic approaches
• Use low dose antipsychotics in severe cases

















