64


FEATURES
Surgeons, other providers take the lead on integrating health care services 14 Megan M. Abbott, MD; Von Nguyen, MD, MPH; and John G. Meara, MD, DMD, FACS
The USS George Washington medical department: Medicine in motion 20 Jared L. Harwood, MD; and Viswanadham Pothula, MD, FACS
The quest for significance 28 Sherif Emil, MD, CM, FACS, FRCSC
Operation Hernia in Carpenter, Northern Ghana 33 Andrew Kingsnorth, MB, BS, FACS, FRACS; and Jonathan Yunis, MD, FACS
Statement on the physician acting as an expert witness 39
DEPARTMENTS
Looking forward 4 Editorial by David B. Hoyt, MD, FACS, ACS Executive Director
What surgeons should know about... 6 PQRS reporting of venous thromboembolism prophylaxis Caitlin Burley
What surgeons should know about... 12 Incentive payments for operations furnished in HPSAs Vinita Ollapally, JD
Socioeconomic tips 41 E/M coding can be easier than one might think Mark T. Savarise, MD, FACS; Linda M. Barney, MD, FACS; and Jenny Jackson, MPH
Advocacy advisor 44 Navigating the legislative process Charlotte Grill
Stephen J. Regnier Editor
Linn Meyer Director, Division of
Integrated Communications
Tony Peregrin Associate Editor
Diane S. Schneidman Contributing Editor
Tina Woelke Graphic Design Specialist
Charles D. Mabry, MD, FACS
Leigh A. Neumayer, MD, FACS
Marshall Z. Schwartz, MD, FACS
Mark C. Weissler, MD, FACS
Editorial Advisors
Tina Woelke Front cover design
Future meetingsClinical Congress2011 San Francisco, CA, October 23-27
2012 Chicago, IL, September 30– October 42013 Washington, DC, October 6–10
Letters to the Editor should be sent with the writer’s name, address, e-mail ad-dress, and daytime tele-phone number via e-mail to [email protected], or via mail to Stephen J. Regnier, Editor, Bulletin, American College of Surgeons, 633 N. Saint Clair St., Chicago, IL 60611. Letters may be edited for length or clarity. Permission to publish letters is assumed unless the author indicates otherwise.
APRIL 2011Volume 96, Number 4
On the cover: Providing medical care on a U.S. Navy aircraft carrier involves many exceptional challenges (see article, page 20). (U.S. Navy photo by Mass Communication Specialist Seaman Adam K. Thomas).

NEWS
FHA/ACS launch largest statewide surgical quality improvement initiative 46A look at The Joint Commission: Engaging physicians in hand hygiene challenges 48
Did you know... 48
ANZ Traveling Fellow selected for 2012 49
Joint trauma quality care initiative launched in Michigan 51
Report of the 2010 Oweida Scholar 53 Fernando Navarro, MD, FACS
NTDB® data points: The road to the Super Bowl 55 Richard J. Fantus, MD, FACS
Trauma meetings calendar 56
Chapter news 61 Rhonda Peebles
The American College of Surgeons is dedicated to improving the care of the sur-gical patient and to safeguarding standards of care in an optimal and ethical practice environment.
Bulletin of the American College of Surgeons (ISSN 0002-8045) is published monthly by the American Col-lege of Surgeons, 633 N. Saint Clair St., Chicago, IL 60611. It is distributed without charge to Fellows, Associate Fellows, Resident and Medical Student Members, Affiliate Members, and to medical libraries and al-lied health personnel. Periodi-cals postage paid at Chicago, IL, and additional mailing of-fices. POSTMASTER: Send ad-dress changes to Bulletin of the American College of Surgeons, 3251 Riverport Lane, Maryland Heights, MD 63043. Canadian Publications Mail Agreement No. 40035010. Canada returns to: Station A, PO Box 54, Wind-sor, ON N9A 6J5. The American College of Surgeons’ headquarters is lo-cated at 633 N. Saint Clair St., Chicago, IL 60611-3211; tel. 312-202-5000; toll-free: 800-621-4111; e-mail:postmaster@ facs.org; website: www.facs. org. Washington, DC, office is located at 20 F Street N.W. Suite 1000, Washington, DC. 20001-6701; tel. 202-337-2701; website: www.tmiva.net/20fstreetcc/home. Unless specifically stated otherwise, the opinions ex-pressed and statements made in this publication reflect the authors’ personal observations and do not imply endorsement by nor official policy of the American College of Surgeons.
©2011 by the American College of Surgeons, all rights reserved. Contents may not be reproduced, stored in a retrieval system, or transmit-ted in any form by any means without prior written permis-sion of the publisher. Library of Congress number 45-49454. Printed in the USA. Publications Agreement No. 1564382.

This survey of our membership provided the College’s leadership with a clearer image of our Fellows’ practice patterns, perceptions of the ACS, and concerns.’’
’’
Looking forward
The American College of Surgeons (ACS) recently undertook a membership sur-vey to determine what we need to do dif-ferently to better suit your needs. More
specifically, the College’s leadership sought to gain an understanding of our members’ practice environment, their informational and educa-tional needs, and their attitudes about ACS mem-bership. We gathered this information to help us design strategic action plans, to develop products and services that meet our members’ evolving challenges, and to take corrective actions that address the organization’s shortcomings.
The survey was distributed to ACS Fellows in the U.S. between the ages of 35 and 60. A total of 1,020 Fellows completed the survey, with a response rate of 50 percent. Anderson-Niebuhr & Associates, Inc., conducted the survey in consul-tation with ACS representatives.
This month’s column provides a summary of the study’s highlights. An upcoming column will focus on the steps the College’s leadership intends to take to ensure the long-term growth of this organization and the increased satisfaction of our membership.
Our FellowshipWith regard to practice environment, the sur-
vey shows that slightly more than one-quarter of our Fellows are in small-group practices, whereas 21 percent are in full-time academic practice, and another 20 percent are in solo practice.
The vast majority (92 percent) of Fellows re-ported that they take emergency call. On average, those respondents who do take call share this responsibility with approximately five other sur-geons. They also said they are on call an average of 10 nights per month.
Slightly fewer than half (47 percent) of the respondents said they limit their practices to specific areas in their specialty. Cardiothoracic surgeons were most likely to limit their practices.
Despite ongoing concerns about the Medicare physician payment system, 90 percent of ACS Fellows said they accept new Medicare patients. On average, more 33 percent of respondents’ practice revenue comes from Medicare, while just less than 40 percent comes from commercial insurance. Nearly 14 percent of their practice earnings come from Medicaid/TRICARE, and
more than 9 percent of the care that Fellows provide is uncompensated.
Most Fellows (54 percent) said their practice is physician-owned, whereas 21 percent are in hospital-based practices. However, more than one-third of the respondents receive financial support from a hospital, institution, or university.
Almost 40 percent of ACS Fellows devote 60 or more hours per week to patient care. When asked to compare the amount of time spent in direct patient care with what they were doing five years ago, one-third of the respondents said they spend more time with patients today, while nearly half said they spend about the same amount of time with patients. In a typical month, respondents perform an average of 29 procedures in hospi-tals, 10 in their offices, and nine in ambulatory surgery centers; they perform nine endoscopy procedures.
Member benefitsApproximately two-thirds of ACS Fellows are
very satisfied or satisfied with their membership in this organization. Indeed, 89 percent of ACS
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
4

If you have comments or suggestions about this or other issues, please send them to Dr. Hoyt at [email protected].
David B. Hoyt, MD, FACS
Fellows would recommend ACS Fellowship to a colleague.
Most Fellows said they joined the ACS for the following reasons: to show unified support for the surgical profession, to have the FACS designation, to stay abreast of issues that af-fect surgeons, and to have a representation in the federal and state governments. These same four factors are the most important reasons that Fellows continue their membership in the ACS.
SatisfactionFellows, however, reported greater satisfaction
with some member benefits than with others. At least 80 percent of the respondents are satisfied with ACS publications and educational programs. On the other hand, respondents expressed ongo-ing interest in improving the College’s advocacy efforts at both the national and the state level.
Approximately two-thirds of the respondents said they prefer live continuing medical educa-tion (CME) programs as opposed to printed materials and electronic learning instruments. Nonetheless, Fellows use a range of resources to fulfill their CME requirements. More than half of the respondents reported using journals, the Surgical Education and Self-Assessment Pro-gram™ (SESAP™), and hospital conferences as part of their CME regimen, with SESAP ranking highest in usefulness.
When asked about the usefulness of various publications or services in obtaining current in-formation about issues related to their practices, at least eight in 10 respondents indicated that they find the Journal of the American College of Surgeons, the Bulletin of the American College of Surgeons, and journals published by other associations to be very or somewhat useful. In contrast, fewer than half find social media, the College’s member-only Web portal, non-peer review publications published by commercial entities, Smartphone applications, and the public website useful in obtaining such information.
More than half of the respondents said that their practices compare or benchmark outcomes data and patient satisfaction information. Fur-thermore, approximately half of the survey par-ticipants report that their practices contribute to the ACS National Surgical Quality Improvement Program®, and approximately 40 percent said
their practices participate in hospital- or system-based quality improvement programs.
Nearly 75 percent of the respondents said that they consider Medicare reimbursement and pro-fessional liability/tort reform to be high-priority advocacy issues for the College to address. Fur-thermore, 70 percent of respondents support the College’s position on most advocacy issues, and more than half said that the ACS provides adequate information for them to effectively ad-vocate on issues. However, more than four in 10 respondents say they are too busy to participate in ACS advocacy efforts.
Moving forwardThis survey of our membership provided the
College’s leadership with a clearer image of our Fellows’ practice patterns, perceptions of the ACS, and concerns. We will use this information to improve our programs to best suit the needs of our Fellows as we move forward. In a future column, I will provide details about the actions we intend to take to make the ACS more respon-sive to the needs of all surgeons.
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
5

What surgeons should know about...What surgeons should know about...
Editor’s note: This is the fourth in an ongo-ing series of articles on the Physician Quality Reporting System (PQRS), formerly known as the Physician Quality Reporting Initiative (PQRI). These articles are intended to help surgeons understand and adapt to changes in the PQRS so that they can receive optimal Medicare Part B reimbursement.
The Centers for Medicare & Medicaid Services (CMS) has continued the PQRS into 2011 as required under the Medicare
Improvements for Patients and Providers Act (MIPAA) of 2008. PQRS links the reporting of quality data to physician payment by offering an incentive payment of 1 percent of the total allowed charges for Medicare Part B professional services covered under the physician fee sched-ule, and furnished during the 2011 reporting period.
For those eligible surgeons who have previ-ously reported in the PQRI program, it is im-portant to note that 2011 PQRS now includes 200 quality measures (including both individual measures and measures that are part of a 2011 measures group). Whereas 2010 PQRI quality measures may be continued in the 2011 PQRS, measures specifications may have been updated for the new program year. Surgeons who are currently reporting in 2010 PQRI should review the 2011 PQRS Measure Specifications Manual for Claims and Registry Reporting of Individual Measures (also known as the 2011 PQRS Mea-sure Specifications Manual) for updates and changes.
This article focuses on a specific PQRS mea-sure that surgeons are likely to use frequently— Measure #23: Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (when indicated in all patients). A previous article in
PQRS reporting of venous thromboembolism prophylaxis by Caitlin Burley
this series provided an overview of the changes in the PQRS for 2011 and was published in the February issue of the Bulletin of the American College of Surgeons.*
How do I use the measure specifications manual?
The first step for implementing PQRS in a surgeon’s office is to use the 2011 PQRS Mea-sure Specifications Manual to identify measures applicable for professional services that the
Abbreviations and acronyms used in this article
ASC X12N 837 electronic claim form
CMS Centers for Medicare & Medicaid Services
CMS 1500 standard claim form used by a non-institutional provider or supplier to bill Medicare carriers and durable medical equipment regional carriers
CPT Current Procedural Terminology
LDUH Low-Dose Unfractionated Heparin
LMWH Low Molecular Weight Heparin
MIPPA Medicare Improvements for Patients and Providers Act
N365 remittance advice denial remark code; N365 is listed for each QDC submitted
PQRS Physician Quality Reporting System
PQRI Physician Quality Reporting Initiative
QDCs quality data codes
VTE venous thromboembolism
*Burley C. PQRS reporting in 2011. Bull Am Coll Surg. 2011;96(2):6-11. continued on page 8
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
6

Source: CMS: 2011 PQRS Measure Specifications Manual. Available at http://www.cms.gov/PQRI/15_MeasuresCodes.asp#TopOfPage.
Surgical procedure CPT code
Neurological surgery 22558, 22600, 22612, 22630, 61313, 61510, 61512, 61518, 61548, 61697, 61700, 62230, 63015, 63020, 63047, 63056, 63081, 63267, 63276
Hip reconstruction 27125, 27130, 27132, 27134, 27137, 27138
Knee reconstruction 27440, 27441, 27442, 27443, 27445, 27446, 27447
Genitourinary surgery 50020, 50220, 50225, 50230, 50234, 50236, 50240, 50320, 50340, 50360, 50365, 50370, 50380, 50543, 50545, 50546, 50547, 50548, 50715, 50722, 50725, 50727, 50728, 50760, 50770, 50780, 50782, 50783, 50785, 50800, 50810, 50815, 50820, 50947, 50948, 51550, 51555, 51565, 51570, 51575, 51580, 51585, 51590, 51595, 51596, 51597, 51800, 51820, 51900, 51920, 51925, 51960, 55810, 55812, 55815, 55821, 55831, 55840, 55842, 55845, 55866
Gynecologic surgery 56630, 56631, 56632, 56633, 56634, 56637, 56640, 58200, 58210, 58240, 58285, 58951, 58953, 58954, 58956
Hip fracture surgery 27235, 27236, 27244, 27245, 27269
General surgery 19260, 19271, 19272, 19301, 19302, 19303, 19304, 19305, 19306, 19307, 19316, 19318, 19324, 19325, 19328, 19330, 19342, 19350, 19355, 19357, 19361, 19364, 19366, 19367, 19368, 19369, 19370, 19371, 19380, 38100, 38101, 38115, 38120, 38571, 38572, 38700, 38720, 38724, 38740, 38745, 38747, 38760, 38765, 38770, 38780, 39501, 39503, 39540, 39541, 39545, 39560, 39561, 43020, 43030, 43045, 43100, 43101, 43107, 43108, 43112, 43113, 43116, 43117, 43118, 43121, 43122, 43123, 43124, 43130, 43135, 43279, 43280, 43281, 43282, 43300, 43305, 43310, 43312, 43313, 43314, 43320, 43325, 43327, 43328, 43330, 43331, 43332, 43333, 43334, 43335, 43336, 43337, 43340, 43341, 43350, 43351, 43352, 43360, 43361, 43400, 43401, 43405, 43410, 43415, 43420, 43425, 43496, 43500, 43501, 43502, 43510, 43520, 43605, 43610, 43611, 43620, 43621, 43622, 43631, 43632, 43633, 43634, 43640, 43641, 43644, 43645, 43651, 43652, 43653, 43770, 43771, 43772, 43773, 43774, 43775, 43800, 43810, 43820, 43825, 43830, 43832, 43840, 43843, 43845, 43846, 43847, 43848, 43850, 43855, 43860, 43865, 43870, 43880, 43886, 43887, 43888, 44005, 44010, 44020, 44021, 44025, 44050, 44055, 44110, 44111, 44120, 44125, 44126, 44127, 44130, 44140, 44141, 44143, 44144, 44145, 44146, 44147, 44150, 44151, 44155, 44156, 44157, 44158, 44160, 44180, 44186, 44187, 44188, 44202, 44204, 44205, 44206, 44207, 44208, 44210, 44211, 44212, 44227, 44300, 44310, 44312, 44314, 44316, 44320, 44322, 44340, 44345, 44346, 44602, 44603, 44604, 44605, 44615, 44620, 44625, 44626, 44640, 44650, 44660, 44661, 44680, 44700, 44800, 44820, 44850, 44900, 44950, 44960, 44970, 45000, 45020, 45100, 45108, 45110, 45111, 45112, 45113, 45114, 45116, 45119, 45120, 45121, 45123, 45126, 45130, 45135, 45136, 45150, 45160, 45171, 45172, 45190, 45395, 45397, 45400, 45402, 45500, 45505, 45550, 45560, 45562, 45563, 45800, 45805, 45820, 45825, 46715, 46716, 46730, 46735, 46740, 46742, 46744, 46746, 46748, 46750, 46751, 46753, 46754, 46760, 46761, 46762, 47010, 47100, 47120, 47122, 47125, 47130, 47135, 47136, 47140, 47141, 47142, 47300, 47350, 47360, 47361, 47362, 47370, 47371, 47380, 47381, 47382, 47400, 47420, 47425, 47460, 47480, 47500, 47505, 47560, 47561, 47562, 47563, 47564, 47570, 47600, 47605, 47610, 47612, 47620, 47630, 47700, 47701, 47711, 47712, 47715, 47720, 47721, 47740, 47741, 47760, 47765, 47780, 47785, 47800, 47801, 47802, 47900, 48000, 48001, 48020, 48100, 48105, 48120, 48140, 48145, 48146, 48148, 48150, 48152, 48153, 48154, 48155, 48500, 48510, 48520, 48540, 48545, 48547, 48548, 48554, 48556, 49000, 49002, 49010, 49020, 49040, 49060, 49203, 49204, 49205, 49215, 49220, 49250, 49255, 49320, 49321, 49322, 49323, 49560, 49561, 49565, 49566, 49570, 50320, 50340, 50360, 50365, 50370, 50380, 60200, 60210, 60212, 60220, 60225, 60240, 60252, 60254, 60260, 60270, 60271, 60280, 60281, 60500, 60502, 60505, 60520, 60521, 60522, 60540, 60545, 60600, 60605, 60650
Table 1. 2011 PQRS Measure Specifications Manual (page 70): Measure #23: Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in All Patients)
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
7

practice routinely provides. Next, select those measures that make sense based upon preva-lence and volume in the practice, as well as each surgeon’s or the practice’s performance analysis and improvement priorities. The 2011 PQRS Measure Specifications Manual can be found at http://www.cms.gov/PQRI/15_MeasuresCodes.asp#TopOfPage.
What is the description of measure #23?
The specifications describe measure #23 as “Percentage of patients aged 18 years and older undergoing procedures for which VTE prophylaxis is indicated in all patients, who had an order for Low Molecular Weight Heparin (LMWH), Low-Dose Unfractionated Heparin (LDUH), adjusted-dose warfarin, fondaparinux or mechanical prophylaxis to be given within 24 hours prior to incision time or within 24 hours after surgery end time.” This text gives a high-level description of measure #23.
What are the instructions?
The instructions explain when and by whom the measure should be reported. According to the instructions, measure #23 should be reported “each time a procedure is performed during the reporting period for all patients who undergo surgical procedures for which VTE prophylaxis is indicated.” The instruc-tions further state that “there is no diagnosis associated with this measure.” Lastly, the instructions indicate who should be reporting measure #23: “It is anticipated that clinicians who perform the listed surgical procedures as specified in the denominator coding will submit this measure.”
What is the “frequency?”
The frequency refers to how often the measure should be reported. Measure #23 should be reported each time an applicable procedure is performed during the reporting period (full- or half-year).
How do I report measure #23 via claims?
The measure specifications for measure #23 indicate that it is a claims and registry mea-sure, meaning it can be reported using either the claims-based or the registry-based method. This article looks at the claims-based method only. The Current Procedural Terminology (CPT)* codes and patient demographics identify the patients who are included in measure #23, otherwise known as the “denominator.” For this measure, the denominator is defined as “all surgical patients aged 18 years and older undergoing procedures for which VTE prophy-laxis is indicated in all patients.” Measure #23 also includes specific denominator instructions to further define eligibility for reporting pur-poses: “CPT Category I procedure codes billed by surgeons performing surgery on the same patient, submitted with modifier 62 indicat-ing two surgeons (or dual procedures) will be included in the denominator population. Both surgeons participating in the PQRS will be fully accountable for the clinical action described in the measure.”
Beginning on page 70 of the 2011 PQRS Mea-sure Specifications Manual, there is a listing of all surgical procedures and CPT codes that qualify patients as eligible to meet this mea-sure’s inclusion requirements (see Table 1, page 7). It is important to review the CPT codes as-sociated with each measure reported. Also, note that the included procedure codes may change from year to year, so it is important to review the 2011 measure specifications before beginning to report for this year.
I’ve identified a patient in the denominator for measure #23. Now what?
CPT II codes, or quality data codes (QDCs), are used to report the clinical action required by the measure on the claims form, otherwise known as the “numerator.” For measure #23, the numerator is defined as “surgical patients who had an order for LMWH, LDUH, adjusted-dose Warfarin, Fondaparinux or mechanical prophylaxis to be given within 24 hours prior to incision time or within 24 hours after surgery
*All specific references to CPT (Current Procedural Terminology) terminology and phraseology are © 2010 American Medical Association. All rights reserved. continued on page 10
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
8
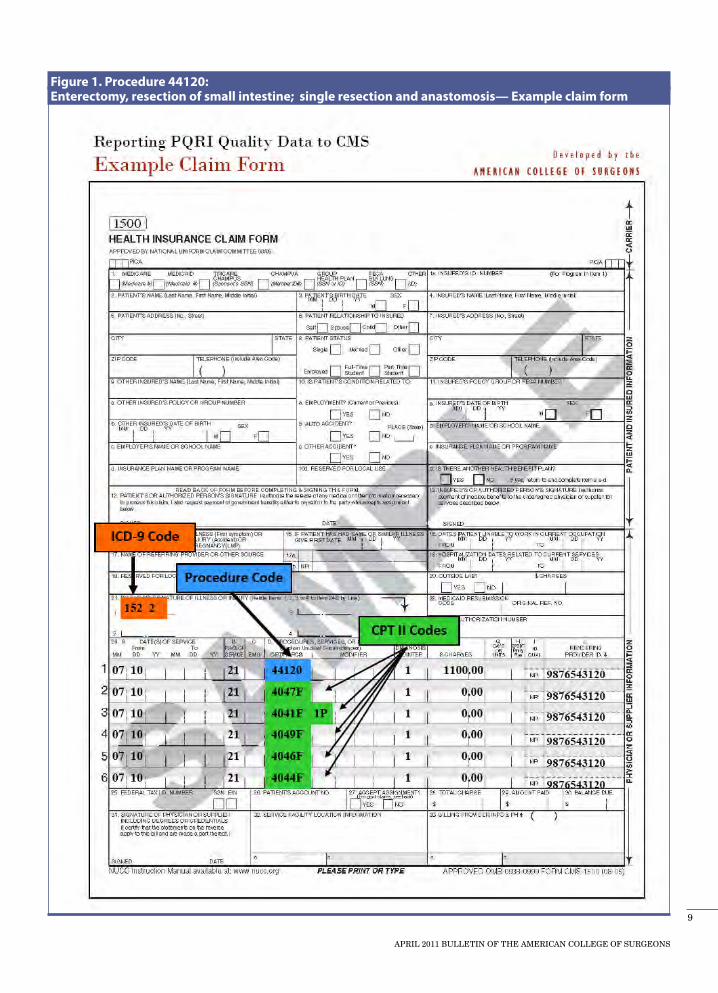
Figure 1. Procedure 44120: Enterectomy, resection of small intestine; single resection and anastomosis— Example claim form
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
9

end time.” Additional instructions state that “there must be documentation of order (written order, verbal order, or standing order/protocol) for VTE prophylaxis or documentation that VTE prophylaxis was given.” Further instructions define mechanical prophylaxis to not include thrombo embolic deterrent hose.
For measure #23, there are three choices for correct quality-data coding options: 4044F; 4044F with 1P; or 4044F with 8P. Code 4044F indicates documentation that an order was given for VTE prophylaxis to be given within 24 hours before incision time or 24 hours after the operation’s end time. Code 4044F with 1P indicates docu-mentation of medical reason(s) for patient not
Claims-based methods Registry-based methods EHR-based methods
Full-year period
Individual measures
1. At least three PQRS measures (one–two if fewer than three ap-ply), for 50% of applicable Medi-care Part B fee-for-service (FFS) patients of each eligible profes-sional
6. At least three PQRS mea-sures for 80% of applicable Medicare Part B FFS patients of each eligible professional
11. At least three PQRS mea-sures for 80% of applicable Medicare Part B FFS patients of each eligible professional
Measures groups
2. One measures group for at least 30 Medicare Part B FFS Pa-tients3. One measures group for 50% of applicable Medicare Part B FFS patients of each eligible profes-sional (at least 15 patients during reporting period)
7. One measures group for at least 30 Medicare Part B FFS patients 8. One measures group for 80% of applicable Medicare Part B FFS patients of each eli-gible professional (at least 15 patients during the reporting period)
Half-year period
Individual measures
4. At least three PQRS measures (one–two if fewer than 3 apply), for 50% of applicable Medicare Part B FFS patients of each eli-gible professional
9. At least three PQRS mea-sures for 80% of applicable Medicare Part B FFS patients of each eligible professional
Measures groups
5. One measures group for 50% of applicable Medicare Part B FFS patients of each eligible pro-fessional (at least eight patients during reporting period)
10. One measures group for 80% of applicable Medicare Part B FFS patients of each eligible professional (at least eight patients during the re-porting period)
Table 2. PQRS 2011 reporting options matrix
receiving any form of VTE prophylaxis (LMWH, LDUH, adjusted-dose Warfarin, Fondaparinux, or mechanical prophylaxis) within 24 hours before incision time or 24 hours after the operation’s end time. Code 4044F with 8P modifier indicates the order was not given for VTE prophylaxis to be administered within 24 hours before incision time or 24 hours after the operation’s end time, reason not otherwise specified. Both the CPT code and the appropriate CPT II code should be submitted on the same claim form.
Can you provide a step-by-step overview of the process for submitting a claim form?
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
10

CPT II codes can be reported on claim form CMS 1500 or via electronic form ASC X12N 837. Figure 1, page 9, is an example of the CMS 1500 claim form.
Based on Figure 1, the steps for reporting via claims include the following:
• Step1:Look in the measure specifications for measure #23 to see if this procedure, 44120, is listed in the table of surgical procedures for which there are indications for prophylactic parenteral antibiotics. If so, continue to step 2.
• Step2:On the CMS 1500 claim form, the CPT procedure code 44120 is listed on line 1.
• Step3: On line 2, the CPT II code, 4044F, is listed, which indicates documentation that an order was given for VTE prophylaxis to be given within 24 hours before incision time or 24 hours after the operation’s end time.
• Step4:Lines 2, 3, 4, and 5 are CPT II codes that correspond to other PQRS measures (#20, #21, and #22). Measures #20, #21, and #22 are often reported by eligible professionals when measure #23 is reported because these four mea-sures represent the perioperative care measures. CPT procedure code 44120 corresponds with these other PQRS perioperative measures as well, so the CPT II codes are listed on the same claim form.
• Step5:Be sure billing software and clear-inghouse can correctly submit PQRS CPT II codes, or quality-data codes (QDCs).
• Step 6: Regularly review the remittance advice notice from the carrier to ensure the denial remark code N365 is listed for each QDC submitted. This indicates that claims have made it to the CMS national claims history file.
Surgical practices that follow these steps should be able to successfully report via claims in PQRS 2011 to receive incentive payments. There are various ways to report for PQRS, and as pre-viously stated, this article has only covered the claims-based method for individual measures. Please refer to the correct measure specifica-tions manual if you choose another method, such as registry-based reporting. Table 2, page 10, is a matrix that lists all 11 options for reporting in PQRS 2011.
For more background information regarding the PQRS program, go to http://www.cms.hhs.gov/pqri/ and access the resources posted at
http://www.facs.org/ahp/pqri/index.html. If you have any further questions regarding PQRS, contact Caitlin Burley at [email protected].
Ms. Burley is Quality Associate, Division of Advocacy and Health
Policy, Washington, DC.
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
11
What surgeons should know about...What surgeons should know about...
Abbreviations and acronyms used in this article
ACA Affordable Care Act
CMS Centers for Medicare & Medicaid Services
HPSAs Health Professional Shortage Areas
HSIP HPSA surgical incentive payment
NPI National provider identifier
Section 5501(b) of the Affordable Care Act (ACA) authorizes a Medicare incentive pay-ment program for major surgical procedures
provided by general surgeons in Health Profes-sional Shortage Areas (HPSAs). This article summarizes this new initiative, called the HPSA Surgical Incentive Payment (HSIP) program.
What is the HSIP Program?
The HSIP program applies to major operations, defined as 10-day and 90-day global procedures, provided on or after January 1, 2011, and before January 1, 2016, by a general surgeon in an area designated as a HPSA. “General surgeons” are defined as surgeons who are enrolled in Medicare with a primary specialty code of 02 (General Sur-gery) identified by his or her National Provider Identifier (NPI).
To qualify for the bonus, the operation itself must be performed in a HPSA. For example, a physician office visit in a HPSA or the provision of any service other than the major operation in the HPSA will not be eligible for the HSIP bonus (although non-major surgical services provided in a HPSA could qualify for the HPSA physician bonus, a separate incentive program which is described later in this article).
How much is the bonus amount and when will I receive it?
The HSIP applies an additional 10 percent of the payment for physicians’ professional services under Medicare Part B for major surgical proce-dures performed in a HPSA. Medicare contrac-tors will compute the reimbursement total and pay general surgeons an additional 10 percent of the amount actually paid for the service, not of the Medicare approved payment amount. Claim adjustment reason code “LE” will identify the incentive payment as noted on the special remit-
Incentive payments for operations furnished in HPSAs by Vinita Ollapally, JD
The HSIP Program – At a glance
• Appliestomajoroperations (definedas10-dayand90-day global procedures)
• Providedbya surgeonwho isenrolled inMedicarewith primary specialty code of 02 (General Surgery)
• ProvidedinageographicHPSA• ProvidedbetweenJanuary1,2011,andJanuary1,2016• Bonuspaymentamountis10percentofamountactu-
ally paid for service
tance generated with the incentive payment. The ACA provides for payments to be made quarterly.
I am already receiving the HPSA physician bonus. Can I receive both the current HPSA physician bonus and the HSIP bonus for major surgical procedures performed in a HPSA?
Yes. The HSIP bonus payment is an additional bonus for major surgical procedures, without regard to other Medicare incentive payments. Before the implementation of the HSIP bonus payment, the Centers for Medicare & Medicaid Services (CMS) implemented the HPSA physician bonus. The HPSA physician bonus provides a 10 percent bonus payment to all physicians who furnish health care services in areas that are designated as geographic primary care HPSAs.
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
12

In addition, psychiatrists furnishing services in geographic mental health HPSAs are also eligible for 10 percent bonus payments on such services. On the other hand, the new HSIP bonus pay-ment provides an additional 10 percent for major surgical procedures performed in a geographic primary care or mental health HPSA. This provi-sion means a general surgeon may receive a 10 percent HPSA physician bonus payment under the already established Medicare HPSA physician bonus program, in addition to a HSIP 10 percent bonus under the new HSIP program that started on January 1, 2010.
What do I have to do to receive the HSIP bonus?
The following steps can help physicians deter-mine whether they are eligible for the HSIP bonus and, if so, how to receive the bonus from CMS:
1. Determine whether the physician provides services in a HPSA. The HSIP bonus payment only applies to major operations performed in primary care or mental health geographic HPSAs. To find out if a physician practices in a primary care or mental health geographic HPSA, go to http://datawarehouse.hrsa.gov/GeoAdvisor/ShortageDesignationAdvisor.aspx.
Note: The major operation must be performed in a primary care or mental health geographic HPSA. Other types of HPSAs also exist, namely population group and facility-based HPSAs, but only primary care and mental health geographic HPSAs are used to determine eligibility for the HSIP bonus payment.
2. Determine whether the physician already receives automatic payment under the HPSA physician bonus program. Each year, CMS pub-lishes a list of zip codes for automatic payment of the HPSA physician bonus payment at http://www.cms.gov/HPSAPSAPhysicianBonuses/01_ overview.asp. CMS will use this same list of zip codes for automatic payment of the HSIP incen-tive payment.
• If thephysicianprovidesservices inazipcode that is listed for automatic payment, then no further action is required. The physician is al-ready receiving the previously established HPSA bonus payment, and will automatically receive the new HSIP program’s additional 10 percent
bonus on major surgical procedures performed in a zip code listed at the CMS website above.
• Ifaphysicianprovidesservicesinanareathat is not on the list of zip codes for automatic payment, yet has been designated as a HPSA by December 31 of the preceding calendar year, he or she should append modifier “AQ” to the Medicare claim for major operations performed in that HPSA. These areas are often in zip codes that are only partially designated as HPSAs, such as zip codes that partially include urban areas. In these cases, the entire zip code cannot be eli-gible for automatic payment, but major surgical procedures provided in the HPSA portion of the zip code are still eligible for the 10 percent HSIP bonus (in addition to the HPSA bonus payment). The use of the AQ modifier is consistent with the current process for payment of the original HPSA physician bonus when the HPSA is not located in a zip code identified for automatic payment.
Note: Do not append the AQ modifier to claims for major surgical procedures performed in a zip code eligible for automatic payment. Based on a conversation that the American College of Surgeons (ACS) regulatory staff had with a rep-resentative from CMS, adding the AQ modifier to such claims will disrupt the automatic payment process and will cause a delay in reimbursement.
In addition, if the claim is submitted by a physi-cian group or practice, the NPI of the physician who provided the major surgical procedure must be included on the line-item for the major surgi-cal procedure in order for a determination to be
Ms. Ollapally is Senior Regulatory
Associate, Division of Advocacy and Health
Policy, Washington, DC.
continued on page 58
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
13

Surgeons, other providers take the lead on integrating health care services
14
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS

The term “value” has achieved buzzword status in health care. The word appears widely on the pages of medical, economic, and business journals, in reports by the
most respected figures in health care policy-making, and, quite prominently, in the Afford-able Care Act (ACA). Value is a concept that budget-conscious consumers often apply when making large purchases. These consumers tend to equate good value with products of the high-est quality for the lowest price. When applied to health care, value becomes a much more complex term. Both the consumer and the product can vary significantly. The “consumer” may be the patient, the physician, the insurer, the employer, the government, or anyone else who interacts with the health care system. The “product,” or patient outcome, can be defined using simple short-term measures, like survival, to long-term composite measures of quality, safety, and patient satisfaction.
In reviewing the myriad ways to define and measure health care value, some common themes recur. One equates value with the qual-ity of care relative to the cost of obtaining it. The basic idea that cost and quality determine value remains consistent regardless of whether the metrics are formulated from disease-, net-work-, or population-specific perspectives. The
second theme centers on the belief that the U.S. health care system must reorganize from its cur-rent fragmented state into integrated provider networks that coordinate care and share joint responsibility for patients.1-4 This position rests on the premise that many inputs into the health care system determine quality and cost, requiring multiple metrics across multiple providers for determination of value. Integrated measurement forms the basis of value-based payment reforms that have been touted as a means to improve quality and decrease costs in U.S. health care.5-7
Limited integration of the U.S. health care system will present problems for emerging value-based reform strategies, such as accountable care organizations (ACOs), value-based purchasing, and bundled payments. The necessary framework has yet to be developed in most institutions and health care networks, with a few notable excep-tions that have demonstrated success.3,8 Multiple components of the ACA will pilot strategies to provide financial incentives for networks of physicians, hospitals, and ancillary providers to better coordinate the delivery of health care services. It seems like placing the cart before the horse, but some experts believe that changing the payment methodology represents the only way to stimulate organizational change in the delivery system.1
by Megan M. Abbott, MD; Von Nguyen, MD, MPH; andJohnG.Meara,MD,DMD,FACS
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
15
Providers should lead
The authors, however, have taken a different view. What if, instead of the insurers taking the lead, providers took charge of improving value? What if hospitals and physicians that commonly work together as affiliates were to begin mea-suring value across organizational lines, coor-dinating care to benefit patients, and building integrated systems to measure value?
Analyzing care across physician and hospital services allows standardization of care protocols, system-wide outcomes and cost measurement, collaborative improvement efforts that prevent cost-shifting, coordination of care, and less du-plication of efforts. Payment reform may achieve some of these benefits, but creating incentives based on reimbursement rates rather than the desire to improve systems of care inevitably leads to shortcuts and incomplete solutions. Working together within a system before financial pres-sure mandates change puts physicians and hospi-tals in a better position to adapt to new realities. We have piloted this strategy at our institution, and in this article, we share our thoughts re-garding system-wide value measurement in a traditionally fragmented system.
Integrating the system
Children’s Hospital Boston and its affiliated physicians are organized within the traditional structure whereby the hospital contracts with an independent physician organization. Each entity operates independently from a financial, organiza-tional, and leadership standpoint. As a result, the concept of measuring value across multiple provid-ers and units in the hospital has been met with skepticism. Although patients often visit coordi-nated clinics for multidisciplinary care, outcomes are not measured consistently across all providers. Children’s Hospital Boston does not routinely measure the continuum of diagnosis-specific costs within a single specialty, let alone across multiple outpatient specialties and inpatient operations. These challenges defined the first step of the task: integrating a fragmented system.
The ability to build support among stakeholders rests with strong leaders who possess a clear vision of how to measure and improve value. Armed with
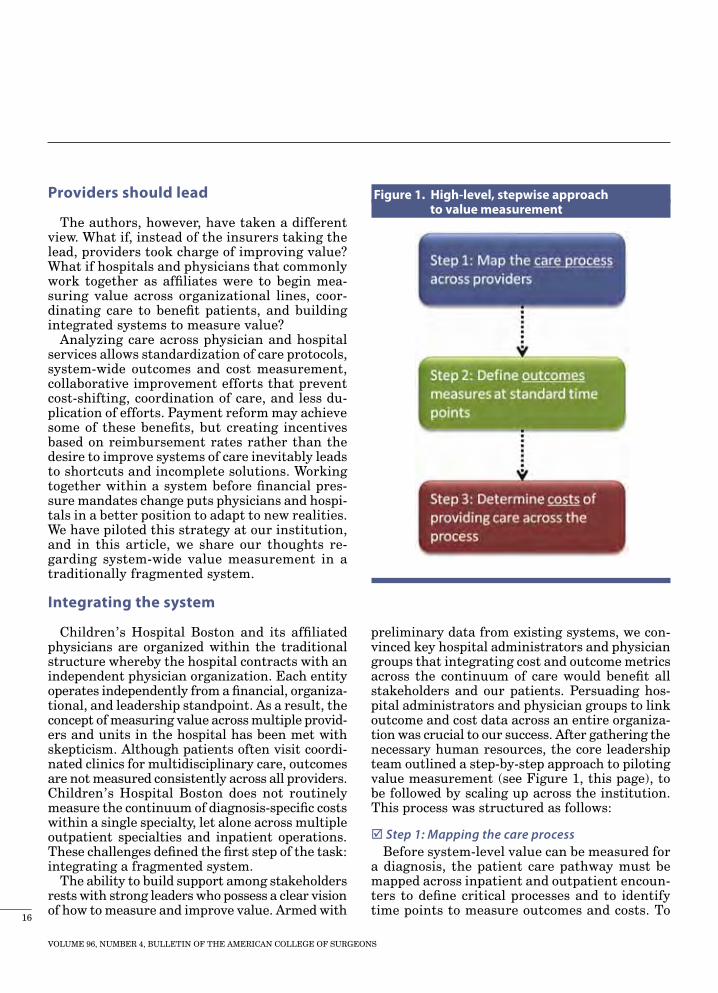
preliminary data from existing systems, we con-vinced key hospital administrators and physician groups that integrating cost and outcome metrics across the continuum of care would benefit all stakeholders and our patients. Persuading hos-pital administrators and physician groups to link outcome and cost data across an entire organiza-tion was crucial to our success. After gathering the necessary human resources, the core leadership team outlined a step-by-step approach to piloting value measurement (see Figure 1, this page), to be followed by scaling up across the institution. This process was structured as follows:
Step 1: Mapping the care processBefore system-level value can be measured for
a diagnosis, the patient care pathway must be mapped across inpatient and outpatient encoun-ters to define critical processes and to identify time points to measure outcomes and costs. To
Figure 1. High-level, stepwise approach to value measurement
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
16

map processes at our institution, we chose cleft lip and palate care as a multidisciplinary pilot di-agnosis (see Figure 2, this page). First, we identi-fied all major encounters between the patient and the health system using hospital and physician billing data over a predetermined period of time.
Next, we mapped each encounter in great detail to understand every action necessary for patient care, from insurance processing to operative cleft repair and follow-up clinic visits. Laying out the key functions required for each encounter requires considerable effort and collaboration among clinic, ward, and operating room staff. Variation and outliers inevitably emerge and should be noted.
To the extent possible, the “standard” care process at a particular institution for a particular disease process should be mapped. If providers use dif-ferent protocols, branch points can be added to note the major variants. Detailed process map-ping efforts were valuable not only for our pilot project, but such efforts helped each department to understand their process flow, which can be adapted to improve internal efficiency.
Step 2: Measuring outcomesOnce the pathway of care across providers has
been defined, clinically significant outcomes are linked to encounters for routine measurement.
Mapping the care process requires identification of billable encounters, followed by detailed mapping of all non-billable and billable activity within and between each encounter to capture all parts of the care pathway.
Figure 2. Mapping the care process
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
17

Outcomes can be defined by validated national benchmarks, expert consensus statements, or home-grown metrics when no standard exists. Linking outcomes measures to encounters pro-vides two advantages. First, it improves docu-mentation of each patient’s care through routine measurements across all providers. This approach ensures that the system provides appropriate care to each patient with as little variation as pos-sible, preventing patients from slipping through the cracks and reducing duplication of effort. Second, outcomes are measured and recorded in a consistent manner for every patient, creating a prospective, standardized database with contribu-tions from all points of care. Outcomes can then be audited and used for internal improvement efforts, to answer research questions, or for public report-ing. To ensure a complete database, our institution is piloting a strategy in which data collection is linked to billing codes, so that a provider cannot bill without entering outcomes data. We recognize the workflow disruption these efforts may cause, but believe that the importance of outcomes data not only outweighs the added burden, but will become standard in the near future.
Step 3: Measuring costsThe terms “costs” and “charges” are frequently
used interchangeably, but are not the same thing.9 Charges are the list prices seen by insurers when hospitals and physicians generate bills for the services they provided. Large public and private insurers receive significant discounts based on negotiated contracts, whereas smaller insurers and self-pay patients do not have this bargain-ing power. From the insurer’s perspective, the discounted provider charge represents their cost or payment for services rendered. From the provider’s perspective, charges do not accurately represent the costs of providing patient care. Costs are derived from the inputs of resources used in the care of patients, including the cost of supplies, the cost of personnel, and the cost of shared capital expenses. Many factors may influ-ence charges, such as payor mix, local competition, regulations, and other political factors, but cost of inputs is rarely the main influence.9 Efforts to control costs must focus on accurate measurement of these inputs to identify and target the largest cost drivers within a system.
Measuring true input costs across a fragmented system is perhaps the most difficult component of our provider-led value measurement strategy. For integrated health care systems, such as Geisinger Health System, all providers are employed by the system and captured within an integrated cost accounting process. At our institution, and in the majority of U.S. health care markets, general led-gers, time sheets, and billing systems are separate between the hospital and physicians. Sharing of these data can be a sensitive issue and requires strong leadership with a focus on the collective goals among all stakeholders.
In our experience, hospitals possess more ad-vanced finance systems that account for patient-level costs. Physician groups, with limited econo-mies of scale, rely on the resource-based relative value scale (RBRVS) as a proxy for cost. The RBRVS was created to provide compensation for a wide variety of procedures across a wide variety of specialties throughout the country using relative value units (RVUs). However, RVU-based charges possess little relation to resources consumed at the diagnosis or patient level. In an era in which provider- and system-level variations have drawn the attention of policymakers in the fight to de-crease costs and increase quality, an aggregated RVU across all specialties is insufficient. Providers must learn to measure their individual resource use, including their time in relation to the types of patients they serve.
To address these complexities, we have begun a pilot project to measure individual resource inputs based on methodologies used in non-health care industries. Outside of health care, no accounting department would use an average price or cost for all similar products, regardless of the manu-facturer. Each company understands the detailed costs of inputs to produce their goods, and prices their product accordingly. Delivering high-quality health care services to patients is more complex than building a widget, but providers can take away some lessons from the system-level cost measurement method used outside of health care.
Next steps
We have developed a stepwise strategy to measure and improve health care value from the provider’s perspective and have made substan-
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
18
Dr. Meara is plas-tic surgeon-in-chief, Children’s Hospital
Boston, and associate professor of surgery and director of the program
in global surgery and social change, Harvard
Medical School, Boston, MA. He is Chair of the
College’s Legislative Committee.
Dr. Nguyen is a general internist at
Dorchester (MA) House Community Health
Center, and a research associate at Children’s
Hospital Boston. He has worked with McKinsey & Company on projects focused on health care reform and physician
payment.
Dr. Abbott is a resident in otolaryngology-head and neck surgery, Mas-sachusetts Eye and Ear
Infirmary/Harvard combined program in
Boston. She is currently completing a clinical
research fellowship at Children’s Hospital
Boston.
tial progress toward developing an integrated measurement protocol within a disjointed sys-tem. We recognize that our organization enjoys a close relationship between its physicians’ organization and the hospital. The diagnosis we chose to pilot—cleft lip and palate—is also well-known for having coordinated, multidisciplinary care. Despite these advantages, we believe that our experience can resonate with health care systems throughout the country.
In building the case for ACOs, research shows that the majority of patients and providers func-tion within a limited network.5 Therefore, with good leadership, a logical strategy, and collabo-ration, provider-led integrated measurements may be plausible even before payment reforms force us to create formal networks. At the very least, mapping the care process for specific di-agnoses and measuring integrated outcomes and costs will teach providers the skills to succeed in a future dominated by integrated systems and ensure appropriate compensation for necessary care when payment reform does arrive.
References
1. Guterman S, Davis K, Schoenbaum S, Shih A. Using Medicare payment policy to transform the health system: A framework for improving performance. Health Aff. 2009;28(s1):w238-w250.
2. Hackbarth G, Reischauer R, Mutti A. Collec-tive accountability for medical care—toward bundled Medicare payments. N Engl J Med. 2008;359(1):3-5.
3. Mechanic RE, Altman SH. Payment reform op-tions: Episode payment is a good place to start. Health Aff. 2009;28(s1):w262-w271.
4. Porter ME. What is value in health care? N Engl J Med. 2010;363(26):2477-2481.
5. Fisher ES, McClellan MB, Bertko J, Lieberman SM, Lee JJ, Lewis JL, Skinner JS. Fostering accountable health care: Moving forward in Medicare. Health Aff. 2009;28(s1):w219-w231.
6. Haywood T. The cost of confusion: Healthcare reform and value-based purchasing. Healthc Financ Manage. 2010;64(10):44-48.
7. Rosenthal MB. Beyond pay for performance—emerging models of provider-payment reform. N Engl J Med. 2008;359:1197-1200.
8. Casale AS, Paulus RA, Selna MJ, Doll MC, Bothe AE Jr., McKinley KE, Berry SA, Davis DE, Gilfillan RJ, Hamory BH, Steele GD Jr. “ProvenCareSM”: A provider-driven pay-for-performance program for acute episodic cardiac
surgical care. Ann Surg. 2007;246(4):613-621; discussion 621-623.
9. Finkler SA. The distinction between cost and charges. Ann Intern Med. 1982;96:102-109.
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
19

20

Being on the open ocean in any vessel is a unique experience that relatively few will ever be able to experience. Having this expe-rience while delivering superb medical care
onboard a Nimitz-class aircraft carrier, history’s largest war-fighting ship, is an experience worth sharing. The purpose of this article is to introduce life on the USS George Washington, with emphasis on the medical department and some of the chal-lenges staff members face. The authors hope to provide some additional insight into this modern marvel and its ability to provide world-class medi-cal care under exceptional circumstances.
The aircraft carrier
Since shortly after the advent of fixed-wing flight at the beginning of the twentieth century, aircraft have been flying off the decks of ships. The first launch of a plane from a stationary ship occurred in 1910, piloted by a civilian named Eugene Ely. The feat took place in Hampton Roads, VA, off of the U.S. Navy cruiser, the USS Birmingham.1
There have been many refinements and changes since that time, and today’s aircraft carriers are very different from those used in famous battles such as the Battle of Midway. For example, the sole survivor of the Yorktown-class aircraft carriers, the USS Enterprise (CVN-6), displaced 25,900 tons of water with a full load.2 Comparatively, the Nimitz-class supercarriers of the current U.S. Navy are much larger, displacing approximately four times as much water.3 They also feature improvements such as an angled flight deck, nuclear propulsion, and modern weapons/navigational systems that enhance their capabilities.
The aircraft carrier is a symbol of power and has served a vital role in all of the nation’s major conflicts, offering a sustainable strike capabil-ity on very short notice. This comes at a price, however. With an annual operating budget of approximately $450 million, over its lifetime of 50 years, a single nuclear aircraft carrier will cost the U.S. more than $22 billion.4
Though an aircraft carrier has an impressive amount of firepower, much of it is wrapped up in its aircraft. Therefore, the primary mission of the aircraft carrier is offensive firepower. Air-craft carriers have traditionally been escorted by an entourage of other ships and submarines
Opposite: The USS George Washington steams through the Pacific Ocean. (U.S. Navy photo by Mass Communication Specialist Seaman Adam K. Thomas). Other photos courtesy of the author.
LT Harwood standing in front of an F/A-18F.
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
21

The medical department
With approximately 10,000 personnel on the move during multi-country military exercises, a medical department equipped to address this unique challenge is a necessity. The medical divi-sion’s mission of providing world-class medical care to each of our dependents never changes, although the tasks at hand do vary from day to day. The medical staff has to be capable of re-sponding to mass casualties, treating critically ill patients for prolonged periods, and transporting patients quickly, when feasible. Unlike medical facilities on the ground, a number of factors change continuously aboard an aircraft carrier, necessitating the cooperation of many parties to optimize medical care. Collaboration is required and utilized whether inside the department, the ship, the battle group, the region, or hospitals and providers several thousand miles away. Coordination involves U.S. military, American assets, allied military units, international medi-cal evacuation firms, and foreign civilian health care facilities.
Of the 17 departments onboard the USS George Washington, the medical department, which the medical division shares with the dental division, is one of the smaller groups onboard, with ap-proximately 50 personnel. The staff comes from all four corners of the U.S. and are of different economic backgrounds, ethnicity, and gender.
With so much metal and movement around, people are bound to hurt themselves. Wound care, lacerations, and contusions accounted for almost 40 percent of our emergency room visits in 2008. In fact, the size of the ship or number of its aircraft are not the only im-pressive statistics: in 2008, the medical divi-sion drew 26,914 labs, had 15,372 outpatient
to minimize vulnerabilities. The primary role of these escorts is to protect the aircraft carrier against air, surface, and subsurface threats. This group of ships, classically referred to as a Carrier Battle Group, is now called a Carrier Strike Group or CSG. Our CSG is headed by Rear Admiral Dan Cloyd, who will be moving on to his next assignment shortly. He will be replaced by Rear Admiral John R. Haley.
CVN-73
The USS George Washington (CVN-73), af-fectionately known as “G.W.” or “G-Dub” by her crew, is the sixth ship in the Nimitz-class of nuclear-powered supercarriers. The aircraft carrier was built by Newport News Shipbuild-ing; was commissioned July 4, 1992; and is commanded by CAPT David A. Lausman, one of only 11 such captains in the world currently commanding a U.S. nuclear powered aircraft carrier.
Carrier Air Wing Five
Carrier Air Wing Five (CVW-5) was originally commissioned in 1943 as Carrier Air Group 5 (CVG-5), and was homeported out of San Diego, CA. The aircraft carrier saw early action in the Pacific Theatre of World War II, and has served in the Korean War, the Gulf War, and, today, the war on terrorism.
CVG-5 was redesignated in 1963 as CVW-5, and the aircraft carrier made history a decade later in 1973, when it embarked on the USS Mid-way and became the first carrier/air wing team to be permanently forward deployed overseas.5 CVW-5, now aboard the USS George Washing-ton, continues to hold this distinction today.
The inpatient ward. When the beds are not being used, they can be folded up or removed to allow space for other things.
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
22

erative care for anorectal procedures with sitz baths is challenging on board the aircraft car-rier. When traveling through rough waters, the ship heaves up and down significantly, and so performing surgery while maintaining balance becomes second nature.
We teach corpsmen surgical skills like cleansing dirty wounds, suturing lacerations, and stabiliz-ing fractures. These skills will likely be utilized when some of the corpsmen deploy with Marine ground troops and become first responders. Patients are kept longer on the ward postop-eratively than in most hospitals, due to the fact that climbing ladder wells is painful. The medical team has to take these additional variables into account when considering patient disposition.
The electrical systems have multiple backups and have never failed. Whether scheduling elec-tive surgeries or crash prepping for emergencies, the supply of consumable items is sometimes stressed. When an item runs out, the medical team does not have the luxury of ordering it overnight via Federal Express. The medical team spends considerable time before each underway period to ensure our supplies will last through that period, which is usually four to six months. If an item is running low during an underway period, it is possible to request a resupply; how-ever, it takes time for the supplies to arrive, often weeks to months.
Keeping broad surgical skills intact in the exist-ing environment is difficult. To mitigate the prob-lem, the surgeon spends time at naval hospitals when the ship is in port for extended periods of time and undergoing repairs. In addition, prior to boarding the ship, each member of the depart-ment’s core staff attends an annual trauma skills refresher course at the Navy Trauma Training
The operating room on board the USS George Washington.
visits, filled 9,969 prescriptions, took 2,312 X rays, and performed 65 operations.
The ship’s surgeon
The surgical team on the G.W. includes a general surgeon, an anesthesiologist or nurse anesthetist, two surgical technicians, and a critical care nurse. The ship features one main operating room with basic laparoscopic gear and gastrointestinal endoscopy instruments. In a mass casualty situation, the surgical team can run two operating rooms along with the oral and maxillofacial surgeon. The main goal of the sur-gical team is to provide damage control surgery for severely injured patients.
When flight deck operations are going on, there is always potential for mass casualties. At the peak of flight operations, planes are launched and recovered at a very quick pace. At any given time during the flight operations, there are ap-proximately 200 sailors on the flight deck, where planes are taking off, landing, or being moved around. Even a simple mistake can result in a catastrophe, and the surgical team is on standby 24/7 for any such incident. The medical team’s goal is to stabilize the patient, stop the bleed-ing, stop spillage, and evacuate the patient to the nearest hospital at the earliest opportunity.
Hand injuries are common; often the hand is crushed during the closing of hatches or in machinery workshops. The most common non-trauma emergency surgery is appendectomy. Though the medical team has the instrumenta-tion for laparoscopic appendectomy, the preferred method is to perform the procedure open. The surgeon also performs a limited range of elective surgery, including groin hernia repair, anorectal procedures, and vasectomies. Providing postop- continued on page 25
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
23

Sunset on board the flightdeck of the USS George Washington.
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
24

Center located in the Los Angeles County and University of Southern California Medical Center.
The flight surgeon: Neither surgeon nor pilot
Naval flight surgeons are assigned to squadrons in both the Navy and Marine Corps. Despite the common misnomer, flight surgeons do not perform surgeries in flight. Instead, they serve as the general doctors for the squadrons, special-izing in aviation medicine as it pertains to those individuals who fly. In essence, flight surgeons are in charge of maintaining the medical readiness of the air wing.
Flight involves several variables/forces that have their own set of unique medical conditions. Flight surgeons are sent to the Naval Aerospace Medical Institute in Pensacola, FL, for a six-month course during which they experience three phases of training: ground school (the same material that all Navy/Marine aviators learn); an abbreviated flight syllabus with flights in both fixed-wing and rotary-wing aircraft; and the flight physiology involved in aviation medicine. Topics studied include G-force–induced loss of consciousness, hypoxia, fatigue, and aeromedi-cal waivers. There have traditionally been three classes of approximately 30 flight surgeons each per year.
A flight surgeon’s time is scheduled to allow 50 percent of his or her time in the clinic and 50 per-cent of his or her time embedded in the squadrons. A big part of being a flight surgeon is forming relationships with those he or she treats, result-ing in patients being open and honest about any medical issues that arise. In as unforgiving an environment as naval aviation, it is imperative that everyone in the air wing, regardless of rank or rate, is healthy and focused.
Another important responsibility of the flight
surgeon is to serve on several different safety boards, especially the mishap safety review boards in charge of investigating the causal fac-tors of major mishaps. These safety review boards will submit a safety investigation report (SIR) to the Navy Safety Center that addresses the causal factors in detail to help prevent the same thing from happening again. One of the most important sections in the SIR is the aeromedical analysis in which human factors—those causal elements that involve or induce human error, the most common of which is fatigue—are discussed. Flight surgeons serve as subject matter experts for human factors, which account for a large majority of mishap causal factors.
A day in medical
A typical day in the medical department aboard the USS George Washington starts with the morning muster (gathering) of medical staff at 0715, where information is passed up and down the chain of command, and the plan of the day is discussed. The muster is immediately followed by the “executive officer’s happy hour.” This, by no means, consists of indulging in free or cheap drinks or coffee. In fact, at this point, every one participates in the cleaning of the ship, for a pe-riod of one hour. After making sure that the ship is spic and span, corpsmen get ready for patients who begin arriving, and continue to do so for the remainder of the day.
With our staff of doctors, we have all the re-quired expertise to stabilize and treat even very complex conditions. The medical department has all the ancillary services that one would expect to find in a small community hospital, including a full pharmacy, laboratory, plain film X rays, operating room, and inpatient and intensive care wards. The department also has other vital
The USS George Washington pulling into its homeport, Yokosuka, Japan, for the first time.
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
25

ancillary services, including radiation health, optometry, preventative health, mental health, and physical therapy.
Typically, days in the medical department are almost always bustling with activity; the variable is whether time is spent taking care of routine health problems or an unexpected medical emer-gency. The dreaded call message consists of the words “Medical emergency. Medical emergency in…” as the away team is directed to the site. Once this message is announced, the corpsmen grab a gurney and their bag and run out the hatch. However, locating the patient can some-times be a challenging task on such a large ship. After the patient is located, the military police secure a safe route back down to the medical department. Whether it is a patient who has been blown into an aircraft by a jet blast on the flight deck, or a patient pinned against the bulkhead by a heavy forklift, the human body tends to lose the battle against cold hard steel.
Once the advance team assesses the patient and finds the patient stable enough to bring him or her to medical on their own power, they are helped up or down the ladder wells. There are 10 decks above, and almost that many decks below, the hanger bay. Helping a patient up or down the ladder wells is a challenge. If the patient has to be brought on a stretcher to medical, the logistics are more complicated. The ship is made for war fighting, not for patient transport. At 45 degrees, the ladder wells are steep, and they are narrow. Navigating the stretcher on the ladder wells is potentially dangerous for the corpsmen
LT Harwood is the Senior Flight Surgeon
of Carrier Air Wing Five, based in Atsugi,
Japan.
as well as the patients. Patients who are being pulled from deeper spaces are sometimes hoisted up several decks through hatches.
One might wonder what ever happened to the elevators we all take for granted in tall buildings. In fact, the aircraft carrier does have a limited number of elevators that are used for transport-ing planes and ordnance. However, if the flight operations are in progress, hijacking one of the elevators will easily bring the entire process to a screeching halt. The flight operations amount to a carefully choreographed interplay involving hundreds of sailors and dozens of planes. (Flight operations are halted with the permission of the captain of the ship, if the situation requires such action.) Even seemingly simple tasks, such as transporting a patient via stretcher, require careful planning on an aircraft carrier.
Meanwhile, much of the medical department converges on the emergency room and prepares it to receive the casualty, prepping IVs, test tubes, monitors, and so on. Once the patient ar-rives, he or she is quickly assessed and treated by the team, which usually consists of the duty provider and several corpsmen, including those needed for ancillary services like the laboratory.
There are conditions outside the scope of our care. We will often coordinate with naval and civilian medical facilities in the various loca-tions we port to facilitate referrals to different specialties. Though our sailors do occasionally have to wait for logistics to work out, we are able to maintain standard of care to mimic closely what is available on the beach (shore).
Medical evacuation (medevac)
Operational medicine often requires a degree of improvisation. Even though the medical team on an air wing is not operating in the middle of a desert during combat, the open ocean can be every bit as desolate when the surgeon has exhausted his or her medical capabilities. One such case last year involved a young sailor with acute aspiration pneumonitis. He required a medevac on a ventilator to the nearest naval hospital, which at that point was Guam. It re-quired putting the patient in the back of a cargo plane on a stretcher. LT Harwood (a coauthor of this article) and a search and rescue corpsman
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
26

CAPT Pothula is a full-time student at
Naval War College, RI, pursuing a masters degree in National
Security and Strategic Studies. He is also a
practicing surgeon at New England Naval
Health Clinic and New-port Hospital, RI.
accompanied the patient to the facility in Guam. Fortunately, there was a portable ventilator avail-able for use, but the unknown variable was how long each oxygen canister would last. The team conducted some calculations with the assistance of the nurse anesthetist and took approximately twice the amount of what was considered neces-sary for the journey (nine canisters in total). Another variable that needed to be considered had to do with whether the patient could with-stand the “catapult shot” it would take to lift him off. Both the corpsman and LT Harwood would have to be strapped into their seats during the catapult shot, and would be unable to attend to the patient until the plane was safely in the air. Fortunately, the patient’s oxygen saturation was stable throughout the flight, and the physicians ended up only needing to replace the oxygen canister three times. The team was humbly re-minded of the necessity to be creative at every step of the process, in order to transfer a patient on a plane that accelerates from 0 to 150 miles in two seconds during take off.
Conclusion
Life at sea is a dynamic experience, and serv-ing aboard the USS George Washington involves many challenges. These challenges are met with honor, courage, and commitment, thus fulfilling the Navy’s core values every day. For those up to the challenge, G.W., affectionately called “Mom,” takes her crew, including her medical staff, from one point in our lives to another, arriving at our destination as better men and women ready to serve society’s needs.
DisclaimerThe comments, views, and information in this article
are those shared and collected by the authors, CAPT Pothula and LT Harwood, and do not necessarily reflect those of the U.S. Navy or U.S. Department of Defense.
Acknowledgments
The authors would like to thank CAPT Joseph T. LaVan, MD, the current senior medical officer of the USS George Washington, and CDR Royce Clifford, MD, former senior medical officer, for their unwavering support of this article.
References
1 Friedman N, Baker AD. U.S. Aircraft Carriers: An Illustrated Design History. Annapolis, MD: Naval Institute Press.1983:31.
2 Yorktown-class aircraft carriers. Available at: http://en.wikipedia.org/wiki/Yorktown_class_air-craft_carrier. Accessed August 8, 2009.
3 United States Navy Fact File: Aircraft carriers. Available at: http://www.navy.mil/navydata/fact_display.asp?cid=4200&tid=200&ct=4. Ac-cessed August 8, 2009.
4 United States General Accounting Office. Navy Aircraft Carriers: Cost Effectiveness of Conven-tionally and Nuclear-Powered Carriers (GAO Publication No. NSIAD-98-1). Washington, DC: U.S. General Accounting Office. 1998. Available at: http://www.gao.gov/archive/1998/ns98001.pdf. Accessed March 5, 2011.
5 Carrier Air Wing Five. Available at: http://en.wikipedia .org/wiki /Carrier_Air_Wing_Five#cite_note-CVW5-1. Accessed August 17, 2009.
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
27
Editor’s note: The following is adapted from Dr. Emil’s address delivered at the University of California, Irvine, School of Medicine commence-ment ceremonies, June 5, 2010.
I t is a profound honor for me to be here today at the University of California, Irvine (UCI), to speak to the class of 2010 on their com-mencement day. This is the most significant
event in my medical and surgical career, which spans two decades. It is so significant because the invitation to join you came from medical students, students who give me true hope for the future of medicine in this great country of ours, hope that American medicine’s best days are still ahead, that its most lasting accomplishments are still to be realized, and that one day the best health care in the world will be available to all our citizens without regard to financial means, personal circumstances, or status in society.
Medicine’s hope for the futureMy career in pediatric surgery began and ma-
tured at this university. I had wonderful men-tors, and superb colleagues. Here, I witnessed
an institution that serves as a source of hope for thousands of patients each year who are not wel-come elsewhere. Here, I learned one of the most profound lessons, a lesson that continues to guide me daily as an academic surgeon. This lesson, taught to me by the graduates on this platform, is that medical students are our greatest asset as a medical profession. Their attitudes, their values, their vision matter very much. They—not the pundits, not the economists, not the admin-istrators, not the politicians—are our country’s best hope for a health care system built on strong ethical principles. The graduates on this platform today have in many ways served as an example to their mentors. From the pharma-free movement that rejects pharmaceutical financial incentives to physicians, to volunteering in developing countries, to starting a clinic for the uninsured in Orange County, to the struggle for universal health coverage—this class of 2010 has led us in reclaiming our great tradition, and shedding the burdens that often hinder us from being the best we can be as healers.
I first engaged with UCI medical students dur-ing an embryology class in January 2005, shortly
The quest for significanceby Sherif Emil, MD, CM, FACS, FRCSC
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
28

after Martin Luther King Day. Embryology is a rather dry subject, and I decided to spice things up a bit at the end of the lecture by putting up a slide of one of my favorite Dr. King quotes: “Of all the forms of inequality, injustice in health care is the most shocking and inhumane.” Once the students recovered from their initial shock that a surgeon was speaking about social justice (I still use that term with no hesitation), their curiosity was aroused and I was invited to return. One of the most remarkable experiences of my early career was to watch students become pas-sionate about health care policy, ethics, their future patients, their community, their state, and their country.
The medical school experience And, so, today we mark a sentinel moment in
the lives of 104 individuals who are just heart-beats away from becoming America’s newest doctors. It is a moment of gratitude, a moment of celebration, and a moment of reflection. I re-member nineteen years ago, almost to the day, being a new medical graduate myself. Days after my graduation, I wrote an essay published in the Montreal Gazette, in which I tried to share my emotions. The following is an excerpt from that essay:
My medical school period, especially the last two years of clinical training, has involved me in the most intense human experiences. I shared the joy and excitement of childbirth and the sad-ness and pain of death, sometimes within the same 24-hour period. I sensed the terrible fear of a crippled child left alone in hospital and the loneliness and despair of the abandoned elderly in their final days. I worked with cocaine addicts and alcoholics, and saw first hand destroyed lives that were once prosperous, broken families that were once united, and humiliated people who were once proud. Medicine brought me face to face with the ugliness in our society—crime, suicide, rape, child abuse. It took me to the inner city ghettos and the Indian reservations, and taught me that pain and suffering know no racial, political, or economic boundaries. The breadth and diversity of this human experience always reminded me not to take my medical training for granted. Often after 36 hours or more straight in the hospital, I would
leave for an outside world that felt awkward. On the streets, life continued uneventfully and people went about their business as usual. But I often left the hospital in body while my mind was still within the boundaries of suffering and upheaval.1
The medical school period is indeed one of the most intense human experiences a young person can go through. In my opinion, how one emerges from this experience, and how one molds this experience into their early professional life as a young physician, dictates the type of physician that person will become.
Gratitude versus entitlementAnd so, I pray that you, the class of 2010,
have emerged from your medical school experi-ence as excited as the day you began, and filled with gratitude—gratitude for the patients who provided themselves as human classrooms, grati-tude for your mentors and teachers, gratitude for your families and friends who supported you these past four years, gratitude for the bonds of friendship you have formed, and gratitude for the power to cure and the privilege to heal that will be bestowed upon you today. And as you progress through your medical career, I pray that you will continue to find reason every day to be thankful for the people who trust their lives—and sometimes even more profoundly, their children’s lives—to you every day, thankful for the respect of your community, thankful for a comfortable and secure standard of living, and thankful for living in a free and open society that judges you by the power of your intellect, the intensity of your energy, and the honesty of your purpose. If you often remember to be thankful, I can promise you that gratitude will be your sustenance. Do not allow gratitude to be replaced by entitlement. Those who feel profoundly entitled have difficulty being of profound service. We physicians have much to be thankful for, and in the words of the greatest healer who walked this earth, “From those to whom much has been given, much will be expected” (Luke 12:48).
The essence of medicineIn the last meeting of the American Pediatric
Surgical Association, several colleagues shared their relief experiences in Haiti, in the middle of
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
29

the most devastating catastrophe in recent human memory. One experience in particular, however, stood out in my mind. It was that of Henri Ford, MD, FACS, surgeon-in-chief at Children’s Hospi-tal, Los Angeles, CA. Dr. Ford has attained the highest levels of recognition for his research and clinical practice, and is on the governing bodies and boards of many of the most prestigious surgi-cal organizations. Dr. Ford spoke about the sense of significance he had as a Haitian-American surgeon returning to Haiti in the middle of disas-ter. It was a sense of significance perhaps never duplicated in a long and illustrious career. He felt that, perhaps, all the accomplishments in his life were for a time such as this, and that he had been given so much and this was a time to give back. In Haiti, Dr. Ford was just a doctor taking care of human beings who needed him. That is where medicine starts, and that is where it ends. Those are the bookends, between which lie all other endeavors of a physician.
MotivationYou have been motivated by the pursuit of ex-
cellence. Without true excellence, you would not have been on this platform today. Although you may have some trepidation about the beginning of your residency, you will continue to be excellent. Excellence is part of your fiber. But is the contin-ued pursuit of excellence enough? Is it enough to keep you motivated? Is it enough to keep you at-tracted to medicine? Is it enough to see you wake up every morning excited about a new day?
In 2005, Josef Fischer, MD, FACS, a pillar of American surgery, stated the following: “There are only four forms of incentive that I, now in my 27th year as a surgical chair, recognize: cash, money, cash money, and anything that can be converted into cash money.”2 While I appreciated Dr. Fischer’s candidness and experience, and while his statement in many ways allowed me to better understand my work environment as a young surgeon, I disagreed. I had to disagree. I have to continue to disagree. Physicians should be compensated well for their delayed gratification, hard work, stressful lives, daunting responsibili-ties, and the debt burden carried by many. But if we decide that doctors can only, and will only, be motivated financially, then we will violate our core principle embodied in the oath you are about
to take: “I will practice medicine for people, not for things.” It is an oath that has kept us a noble and revered profession for centuries; an oath that motivated our predecessors to keep moving forward despite disappointment after disappoint-ment; an oath that has sent volunteer physicians to the far outreaches of this earth to take care of people whose language they could not speak and whose culture they could not understand; an oath that compels relief physicians and surgeons to risk their lives in war zones and violent regions in order to provide help; and an oath that contin-ues to attract the best and brightest to medicine. Therefore, if it is not money or cash or cash money, what can it be?
SignificanceI believe the age-old motivator of physicians is
significance. I believe that God almighty has en-dowed us with the desire to be of significance to other human beings. I believe that that desire is exceptionally strong among physicians. I believe that, as doctors, it is more important for us to be significant to even just one human being than it is to be irrelevant to multitudes. The most content and fulfilled physicians I have encountered have not been those who have amassed wealth, but rather those who have made the biggest difference in the lives of others, whether in the African bush, the Indian reservation, the inner city, or right here in Orange County. I grew up with two of those physicians, my parents, who served some of the neediest human beings in Egypt and Nigeria, with-out ever putting a price on their services. I also believe that the desire for significance can either be extinguished by cynicism, selfishness, greed, corruption, or it can be nurtured to create physi-cians who are significant to their patients, their practices, their communities, and their country.
And so, Class of 2010, how will you nurture your quest for significance?
The golden rule of medicine First, observe the golden rule of medicine. Treat
your patients as you wish yourself or your child or your parent or your sibling to be treated. There will be some patients who will remind you of that member of your family you may not be so fond of, but he or she is still a member of your family. When you can’t cure, remember that you can often
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
30

care, and always comfort. Don’t worry when you can share your patient’s emotions; worry when you can’t. The families I have bonded with the most have not been the ones who experienced fast cures, not the ones who underwent pioneering procedures, not the ones who benefited from the latest research findings, not even the ones whose children I saved from certain death. The families I have bonded with the most have been the ones whose children’s funerals I have attended. Be significant to your patients.
Second, pay your teachers and mentors forward by teaching and mentoring others. Despite all the advances in technology and teaching science, medicine remains an apprenticeship. We acquire it from our predecessors, and pass it to our succes-sors. You do not have to be an academic physician to teach. Regardless of the practice environment you will find yourself in, there will be someone around you hoping to learn from you. It may be a nursing student, a surgical tech, or a fellow phy-sician. Seek them out, encourage them, inspire them. Be significant to them.
Third, always be inquisitive. Research is the tool by which medicine continues to advance. Some of you will progress to become established and dedi-cated researchers, but research is a spectrum with plenty of room for different degrees of involvement and commitment. You can choose how much you want to do. Even the occasional case report adds something to the body of knowledge. Keep an open mind, [and] ask the difficult questions. If you have an idea, pursue it. Embrace innovation that truly benefits the patient. Evidence-based medicine is the call of the day. Seek the evidence. Use the evidence. Create the evidence. Be significant to your profession.
Finally, please stay involved in issues of health care policy. If you think we have passed health care reform, and can now rest easy, think again. We have not passed health care reform. We have only passed some health care expansion. It is too early to judge the effects of what has occurred, but it is not too early to be certain that much work still lies ahead. Make your voice heard in the national debate that started in your senior year, and will almost certainly rage on. It is interesting for me, as an American surgeon practicing in Canada, to see the negative depictions of the Canadian sys-tem in TV ads and [in the] lay media. My reality
is very different. I can see any patient and any patient can see me—total freedom of practice. My patients will still get the same care and see the same physicians if their parents change jobs or lose their job altogether in a bad economy. Micro- management of daily practice is nonexistent. There are no contracts, authorizations, deni-als, appeals, reviews, IPAs, HMOs, or PPOs. My relationship with the hospital administration is defined by strictly professional, not financial, standards. However, I do not practice in a medical utopia. The Canadian system has its own set of difficulties, challenges, and shortcomings. Waiting lists are, in many instances, unacceptably long, resources are stretched, many physical plants are outdated, and there is plenty of senseless govern-ment macro-management. Canadians are also looking to significantly reform their system. There are many valid points of view in the health care debate. As physicians, we have to join the debate and we have to join it objectively, salvaging it from the bias, misrepresentation, and demagoguery that characterize it. Health care should not be a liberal or conservative issue, for disease, disability, and death do not recognize political affiliations. As a socially conservative Christian, my personal belief that health care is a fundamental human right, best guaranteed through single-payor uni-versal health coverage, stems from my faith, and not despite it. My faith calls for personal morality, but also for societal morality—how do we treat the sick among us, the weak among us, the least among us?
The health care environment in the U.S. contains all the components of a stellar health care system—well-trained physicians, superbly equipped hospitals, the best research infrastruc-ture in the world, more than sufficient capacity, and resources and funding. Throughout the coun-try, we have many examples of what is truly the best health care in the world. But we have not been able to weave these components together into a health care system truly worthy of this nation. We have left too many people behind. Too many people go bankrupt, too many people suffer, too many people die—about 20,000 a year—because of lack of access.3 And while many are left behind, others are excessively treated. Atul Gawande, MD, FACS, found that the per capita expenditures on Medicare patients in the small town of McAllen,
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
31

TX, is double the national average, even though these patients had no better outcomes of care.4 Dissection of this phenomenon revealed the reason to be that patients received care that benefited the physician and the hospital, not the patients. In McAllen, medicine had become a huge industry. Unfortunately, McAllen medicine is prevalent throughout the country. It is part and parcel of what Thomas R. Russell, MD, FACS, former Executive Director of the American College of Surgeons, lamented as the corporatization of medicine. “Unfortunately, the practice of surgery today is as much a business as it is a science and art,” he wrote in one of his editorials.5 This corpo-ratization is pervasive. Too many physicians are resigned to it, too many have yielded to its power, too many have been seduced by its promises. It has resulted in many of the lapses of ethics and judgment that you fought against as students. The fight continues ahead, and in it, your enemies will not be administrators, insurance companies, pharmaceutical companies, or the government. Your enemies will be much more potent: apathy, indifference, loss of vision, loss of purpose. Do not be distracted, do not let up your fight, for we need you—we need you in a time such as this. Be significant to your country.
An American storyMy parents sacrificed much to send me, their
only child, to America at age 17 to start college. They believed, as had millions before them, that in the U.S. I would enjoy equal opportunity, and equal citizenship. My acceptance to North Ameri-can medical schools, while still an international student, was near miraculous. I have never taken for granted the opportunities I have enjoyed and the positions I have attained, for I would have most certainly been denied those in my native land. My story is an American story, no doubt the story of many who will receive their medical degree today, the story that continues to make the American experience the most profound in the history of mankind. In many ways, though, I am an improbable commencement speaker. I did not cure a disease or invent a drug or device. I did not start an organization or win an interna-tional prize. I am only here because I was able to tap into a deep desire to do good in these young physicians. But I am just another physician trying
to balance an academic surgical career with fam-ily obligations, struggling to maintain a healthy physical and spiritual life through an extremely demanding professional path—and often falling short. My challenges will soon be the challenges of these new doctors. And my hope, my wish, for them is that they will meet these challenges far more effectively than I have been able to meet mine. And in this task, they will need you—their spouses, parents, siblings, friends, and loved ones. They will need you to believe in their mission, to make it yours as well, to support them, to under-stand them, to be patient with them, to share in their lows, and to celebrate their highs. And they will also need you to remind them to take care of themselves and their families.
May God bless these new doctors, may He shed His light upon them, and may He endow them with the very best in their professional and personal journeys.
References
1. Emil S. Doctors need as much art as science: McGill graduate. The Montreal Gazette. June 2, 1991.D-2.
2. Fischer JE. Surgeons: Employees or professionals? Am J Surg. 2005;190:1-3.
3. Institute of Medicine (IOM). Insuring America’s health: Principles and recommendation. IOM Report. The National Academies Press, 2004.
4. Gawande A. The cost conundrum. The New Yorker. Available at: http://www.newyorker.com/reporting/2009/06/01/090601fa_fact_gawande. Accessed January 11, 2011.
5. Russell T. From my perspective. Bull Am Coll Surg. 2003;88(11):3-4.
Dr. Emil is associate professor of surgery and pediatrics, McGill Uni-versity, and director, di-vision of pediatric gen-eral surgery, Montreal Children’s Hospital of the McGill University
Health Centre, Mon-treal, QC. He also holds
an academic appoint-ment in the department of surgery, University of
California, Irvine.
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
32

Above: Dr. Kingsnorth (right) teaching a local medical officer in Carpenter.
OperatiOn Hernia in Carpenter, northern Ghana
by andrew Kingsnorth, MB, BS, FaCS, FraCS;
and Jonathan Yunis, MD, FaCS
Hernias result in a considerable limitation of activity, and the number of days of work lost to this condition is higher than for any other chronic digestive condition.1 In Ghana, ingui-
nal hernia represents the bulk of a general surgeon’s workload, with 20 percent presenting as acute abdomi-nal emergencies, either obstructed or strangulated.2 Due to poor nutrition and late presentation, a quarter of the emergency cases result in death, and 10 percent present with enterocutaneous fistula from perforation. Lack of awareness of this condition and limitations resulting from poverty are the major factors in this delayed presentation.
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
33

A patient gowned and ready for his operation. He had a large, typical “below the knees” hernia, of a type prevalent in the Bole District of Ghana.
Dr. Kingsnorth contemplating the operative strategy for a large inguinoscrotal hernia.
In a recent mission to deliver free surgical treatment to the rural poor in neighbouring Nigeria, patients with surgical problems were ad-vised to assemble at one of nine zone locations.3 More than 1,000 patients were treated in a nine-week period; two-thirds of these procedures were for inguinal hernia. Free rotational surgical care such as this can help the poor in third-world countries receive treatment that they would otherwise not be able to afford. However, even with dedicated human resources, the poor state of equipment, even in major centers, is a major constraining factor.4
Compared with inguinal hernias in Europe, Ghanaian hernias are significantly larger, and the patients are significantly thinner (see photo, top right). As a result, 16 percent of patients are unable to work, and 64 percent have limited daily activities; 85 percent have had the hernia for more than one year, and in 37 percent the hernia has been present for more than five years.5 Failure to treat ju-venile hernias results in a large percentage of indirect hernias, many of which, after years of failure to receive operative treatment, represent a major surgical challenge (see photo, bottom right). A clinical clas-sification has been developed for these hernias to assist in the stratification and the tim-ing of surgical intervention.6
The true incidence of ingui-nal hernia in Africa has not been recently quantified. In the U.S. and Europe, the ap-proximate rate of inguinal her-nia repair is 150 per 100,000 population. A U.S. population of African-American men and women has a less than 60 percent incidence of inguinal hernia, compared to the Cauca-sian population.1 This statistic would imply that the expected incidence in Sub-Saharan Afri-can countries could be approxi-
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
34

mately 100 per 100,000 population. With timely surgical intervention, the incidence (number of cases arising each year) and the prevalence (the actual number in a population at a given time) should be approximately equal.
Operation Hernia
Operation Hernia was initiated in 2005, specifically to treat groin hernia patients and teach surgical techniques in rural Africa, and is supported by the European Hernia Society (see photo, this page).7 The idea for this project was conceived in 2002 by Prof. Leon Herszage of Buenos Aires, who travelled 1,600 kilome-tres (1,000 miles) to the north eastern part of Argentina to perform hernia operations with a team of 19 surgeons, nurses, and health care professionals.8 The team operated on 83 cases in four days, with successful outcomes. This mission was followed by a collaborative effort of the American Hernia Society (AHS), Institute of Latin American Concerns (ILAC), medical industries, U.S. Peace Corps, physicians, surgi-cal residents, and nurses from many institu-tions (11 surgeons, 8 anaesthetists, 5 residents,
20 nurses, 15 ILAC volunteers), who traveled to Santiago in the Dominican Republic for a five-day period to perform inguinal hernia repair.9 The AHS/ILAC team utilized a new outpatient surgical facility built in 2003 with three operating rooms and 10 examining rooms, which served as the facility for the hernia clinic.
Operation Hernia was estab-lished in 2005 as part of the Plymouth-Takoradi (Ghana) link to provide cultural, educa-tional, and medical exchanges between the two cities. In 2005, the first medical team made up of five surgeons, a resident, six nurses, and an administrator performed 130 hernia opera-tions during a 10-day mission in Takoradi. In 2006, with funding provided by the Brit-
The District Medical Officer of Western Ghana, accompanied by the British High Commissioner, welcomes Operation Hernia for the first mission to Takoradi in 2005.
ish High Commission and the medical industry, an unused wing of Takoradi hospital was refur-bished to create a Hernia Treatment Center. Redundant surgical equipment from Derriford Hospital, Plymouth, U.K., was transported to Takoradi and installed to provide facilities at a much higher standard than is usual in Ghanaian hospitals (see photo, page 36). Surgeons from the European Hernia Society-GREPA were then actively encouraged to volunteer for week-long missions, during which they were also expected to take time to teach mesh hernioplasty to the local surgeons and provide lectures on basic surgical topics.
The regional medical officers have assisted in this development by sanctioning time off for these activities. Four missions were accom-plished in 2007, and 10 teams used the facility in 2008. In 2009, Operation Hernia accepted invitations to support missions to Côte d’Ivoire and Nigeria, and other countries in West Africa have expressed an interest in these services. To date, more than 35 missions have been completed by surgeons from 12 countries, and more than 3,000 hernias have been repaired using modern mesh techniques, which are now well-accepted
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
35

in developing countries (see photo, this page).10-12 Most teams have written about their experience, and these expressive narratives have been posted on the Operation Hernia Foundation’s website (http://www.operationhernia.org.uk). Financial support for several U.K. trainees has been pro-vided by the Association of Surgeons of Great Britain and Ireland.
The Commission for Africa has stressed the importance of the development of partnerships, such as Operation Hernia, which support African institutions and regional organizations, and sup-plement the deficit in the workforce.13 Africa’s health care workforce is rapidly depleting, and its health systems are weak, unsustainable, and
unavailable to the majority of the population. Even interventions with proven effectiveness cannot be delivered in a setting of poverty and poor living conditions. The practical difficulties are legion, with poor infrastructure, bad sys-tems for information and communication, travel complications, high foreign exchange rates, and safety concerns. Effective health care has become a victim of political instability, unemployment, foreign debt burden, and poorly performing industry.14 Those in the poorest socioeconomic conditions suffer the most because the most dis-advantaged countries are least likely to attract health care workers.
the surgical workforce
The Republic of Ghana has a population of 20 million and is divided into 10 health regions and 170 districts. The Ministry of Health repre-sented by the Ghana Health Service owns half of the country’s health facilities, the private sector (including private maternity homes) owns 21 percent, and the Christian Health Association of Ghana owns the remainder.15 In 2005, there were 2,026 medical officers and 200 expatriate
First inguinal mesh hernioplasty in rural Africa by Operation Hernia, in Takoradi in 2005: Classic Lichtenstein repair under local anaesthesia applied to groin hernias.
Aided by a grant from the British High Commission, Operation Hernia arranged for the refurbishment of a wing of the District hospital in Takoradi.
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
36

Dr. Kingsnorth is a professor of surgery and
president of the Euro-pean Hernia Society,
Peninsula Medical School, Derriford Hos-
pital, Plymouth, U.K.
doctors, compared with the 21,182 traditional practitioners. In Sub-Saharan Africa, 1 million health care workers are needed to bridge the gap in this region—while it has 11 percent of the world’s population and 24 percent of the global burden of disease, it has only 3 percent of the world’s health care workers.16 Tragically, more than two-thirds of young Ghanaian doctors leave the country within three years of graduation, to seek better conditions and better salaries in the developed world.17 To compensate, a major ex-pansion of medical assistants (specially trained, registered nurses) is planned to double their output in the next two years, and to improve salary levels of health care workers. Since 1960, the West African College of Surgeons has lobbied governments to support faculty development, increase resident salaries, and improve health services. In spite of this, the surgical specialist cadre has been decimated by emigration, which has led to a depletion of top-level manpower.18
Operation Hernia in Carpenter
Carpenter is 500 kilometres (400 miles), and approximately 12 hours by car, from Accra, the capital of Ghana. The location for Operation Hernia was chosen in February 2008 on the site of the Northern Empowerment Association (NEA)–Ghana Rural Integrated Development (NEA-GRID) organization. The NEA was initi-ated by David Mensah, PhD, to help improve the lives of the rural poor around the desperately underprivileged area of Carpenter. The NEA improves lives of the local community by provid-ing infrastructure with such items as fresh water from wells, training of farmers in modern agri-culture, school buildings, fish farming, poultry husbandry, and disbursement of microcredit to women’s groups.19
No clinic or hospital had previously existed within 30 kilometres (25 miles) of the Carpen-ter community. In the months preceding the visit by Operation Hernia, redundant equip-ment was assembled from Derriford Hospital, and transported to Carpenter. A 13-member team, including four surgeons, an anaesthetist, and operating theatre nurses, was recruited. In addition, generous support was provided by the medical industry, and financial support was also
received from the British and European Hernia Societies.
Carpenter is situated in the Bole District and has a population of approximately 50,000. Prior to the mission, the medical assistants counted at least 700 inguinal hernias in this population. The prevalence was, therefore, approximately 1,400/100,000, which is far in excess of the ex-pected 100/100,000 incidence, indicating a near total neglect of elective hernia surgery for many years. This data indicates that in the Bole Dis-trict, inguinal hernia affects 2.7 percent of males, which makes it more common than the official numbers of the population with HIV infection.
During a two-week period, 76 patients received hernia surgery; 93 procedures were performed, including several giant inguinoscrotal hernias.
Conclusion
Volunteer teams should not be regarded as a permanent solution to solve the problem of limited resources in developing countries.20 The Ghanaian government has a vision to bring the country to middle-income status by 2015, which will require a healthy population.15 The govern-ment accepts that the primary difficulty is get-ting surgeons to take up rural postings, where many vacancies exist, and where many zones are not even functioning.
Operation Hernia is continuing to build its ac-tivities not only in West Africa, but also in other low-income countries such as Ecuador, Mongolia, and Kenya. More volunteers are coming forward
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
37

Dr. Yunis is staff sur-geon, Sarasota Medical
Center, Sarasota, FL.
than there are opportunities presently available; therefore, an expansion of the sites will continue through 2011. Operation Hernia hopes to join the myriad other opportunities that exist for volun-teer surgeons of the College through Operation Giving Back. Such missions will only have suc-ceeded when they are no longer required.
References
1. Ruhl CE, Everhart JE. Risk factors for inguinal hernia among adults in the U.S. population. Am J Epidemiol.2007;165(10):1154-1161.
2. Mbah N. Morbidity and mortality associated with inguinal hernia in Northwestern Nigeria. W Afr J Med. 2007;26(4):288-292.
3. Aderounmu ACA, Afaolayau SA, Nasiru TA, Olaore JA, Adeoti ML, Adelasoye M. Rotational rural surgery for the poor in developing countries. Trop Doc. 2003; 38(3):141-144.
4. Archampong EQ. Surgery in developing nations. Br J Surg 2000;93(5):516-517.
5. Sanders DL, Porter CS, Mitchell KCD, King-snorth AN. A prospective cohort study compar-ing the African and European hernia. Hernia. 2008;12(5):527-529.
6. Kingsnorth AN. A clinical classification for patients with inguinal hernia. Hernia. 2004; 8(3):283-284.
7. Kingsnorth AN, Oppong C, Akoh J, Stephenson B, Summermacher R. Operation Hernia in Ghana. Hernia. 2006;10(5):376-379.
8. Herszage L. Hernia surgery in the South Ameri-can woodlands: A surgical adventure in Argen-tina. Hernia. 2004;8(4):306-310.
9. Turaga KK, Garg N, Coeling M, Smith K, Amir-lak B, Juszczak N, Elliott B, Manion J, Filipi C. Inguinal hernia repair in a developing country. Hernia. 2006;16(4):294-298.
10. Tongaonkar RR, Reddy BV, Mehta VK, Singh NS, Shivade S. Preliminary multicentric trial of cheap indigenous mosquito-net cloth for tension-free hernia repair. Indian J Surg. 2003;65(1):89-95.
11. Freudenberg S, Sano D, Ouangré E, Weiss C, Wilhelm TJ. Commercial mesh versus nylon mosquito net for hernia repair. A randomized double-blind study in Burkina Faso. World J Surg. 2006;30(10):1784-1789.
12. Clarke MG, Oppong C, Simmermacher R, Park K, Kurzer M, Vanotoo L, Kingsnorth AN. The use of sterilized polyester mosquito net for inguinal hernia repair in Ghana. Hernia. 2009;13(2):155-159.
13. Dare L, Buch E. The future of health care in Africa. BMJ. 2005;331(7507):1-2.
14. Editorial: Feature Health in Africa. BMJ. 2005;351(7507):705-785.
15. World Health Organization 2008: Global Health Workforce Alliance: Ghana: Implementing a na-
tional human resources for health plan. Available at: www.who.int/workforcealliance/knowledge/case_studies/Ghana.pdf. Accessed March 5, 2011.
16. Wasswa H. Rich states “snatch” trained doctors from poor countries. BMJ. 2008;336(7644):579.
17. Coombes R. Developed world is robbing African countries of health staff: New ways of delivering health care are needed in developing countries. BMJ. 2005;330(7497):923-b.
18. Bode CO, Nwawolo CC, Giwa-Osagie O. Surgical education at the West African College of Surgeons. World J Surg. 2008;32(10):2162-2166.
19. Operation Hernia Foundation. Available at: http://www.operationhernia.org.uk. Accessed June 6, 2010.
20. Duda RB, Hill AG. Surgery in developing countries: Should surgery have a role in population-based health care? Bull Am Coll Surg. 2007;92(5):12-18.
21. Russell TR. From my perspective. Bull Am Coll Surg. 2007;92(5):4-7.
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
38

This statement was originally published in the June 2000 issue of the Bulletin. This revised statement incorporates revisions recommended by the College’s Central Judiciary Committee and was approved by the Board of Regents at its February 2011 meeting.
Physicians understand that they have an obligation to testify in court as expert witnesses on behalf of the
plaintiff or defendant as appropriate. The physician who acts as an expert witness is one of the most important fig-ures in malpractice litigation. In response to the need to define the recommended qualifications for the physician expert witness and the guidelines for his or her behavior, the Patient Safety and Professional Liability Committee of the American College of Surgeons has issued the following statement.
Failure to comply with either the recommended qualifica-tions for the physician who acts as an expert witness, or with the recommended guidelines for behavior of the physician acting as an expert witness, may constitute a violation of one or more of the Bylaws of the American College of Surgeons.
Recommended qualifications for the physician who acts as an expert witness:• The physician expert witness must have had a current,
valid, and unrestricted state license to practice medicine at the time of the alleged occurrence.• The physician expert witness should have been a dip-
lomate of a specialty board recognized by the American Board of Medical Specialties at the time of the alleged occurrence and should be qualified by experience or dem-onstrated competence in the subject of the case. • The specialty of the physician expert witness should
be appropriate to the subject matter in the case. • The physician expert witness who provides testimony
for a plaintiff or a defendant in a case involving a specific surgical procedure (or procedures) should have held, at the time of the alleged occurrence, privileges to perform those same or similar procedures in a hospital accredited by The Joint Commission or the American Osteopathic Association. • The physician expert witness should be familiar with
the standard of care provided at the time of the alleged occurrence and should have been actively involved in the clinical practice of the specialty or the subject matter of
Statement on the physician acting as an expert witness
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
39

the case at the time of the alleged occurrence. • The physician expert witness should be
able to demonstrate evidence of continuing medical education relevant to the specialty or the subject matter of the case. • The physician expert witness should be
prepared to document the percentage of time that is involved in serving as an expert witness. In addition, the physician expert witness should be willing to disclose the amount of fees or compensation obtained for such activities and the total number of times he or she has testified for the plaintiff or defendant.
Recommended guidelines for behavior of the physician acting as an expert witness:• Physicians have an obligation to testify in
court as expert witnesses when appropriate. Physician expert witnesses are expected to be impartial and should not adopt a position as an advocate or partisan in the legal proceedings. • The physician expert witness should review
all the relevant medical information in the case and testify to its content fairly, honestly, and in a balanced manner. In addition, the physician expert witness may be called upon to draw an inference or an opinion based on the facts of the case. In doing so, the physician expert witness should apply the same standards of fairness and honesty. • The physician expert witness should be
prepared to distinguish between actual negli-gence (substandard medical care that results in harm) and an unfortunate medical outcome (recognized complications occurring as a result of medical uncertainty). • The physician expert witness should review
the standards of practice prevailing at the time
and under the circumstances of the alleged oc-currence. • The physician expert witness should be
prepared to state the basis of his or her testi-mony or opinion and whether it is based on personal experience, specific clinical references, evidence-based guidelines, or a generally ac-cepted opinion in the specialty. The physician expert witness should be prepared to discuss important alternate methods and views. • Compensation of the physician expert wit-
ness should be reasonable and commensurate with the time and effort given to preparing for deposition and court appearance. It is unethical for a physician expert witness to link compensa-tion to the outcome of a case. • The physician expert witness is ethically
and legally obligated to tell the truth. Transcripts of depositions and courtroom testimony are public records and subject to independent peer reviews. Moreover, the physician expert witness should willingly provide transcripts and other documents pertaining to the expert testimony to independent peer review if requested by his or her professional organization. The physician expert witness should be aware that failure to provide truthful testimony exposes the physi-cian expert witness to criminal prosecution for perjury, civil suits for negligence, and revocation or suspension of his or her professional license.
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
40

Socioeconomic tips
Surgeons and their coding staff sometimes find evaluation and management (E/M) codes difficult to understand. However, the fact of the matter is that insufficient
or incorrect documentation of E/M services results in payment denials as well as sanctions and penalties.
This article addresses the use of the consulta-tion codes and summarizes the changes in the 2011 Current Procedural Terminology (CPT)* manual that pertain to general surgery and closely related specialties.
Consultation codesOutpatient consultations for Medicare patients
are reported with new patient (99201–99205) or established patient (99212–99215) CPT codes. For non-Medicare patients (unless otherwise instructed by a payor), office or other outpatient consultations are reported with codes 99241–99245. The guidelines for all patients (Medicare and non-Medicare) indicate: If the patient has not received any professional service from the physician or another physician in the group of the exact same specialty within the last three years, the patient is considered a new patient. If the patient was seen by a physician in the group, but of a different specialty (for example, a plas-tic surgeon and a general surgeon), or different subspecialty (for example, a hand surgeon or a burn surgeon), the patient is considered a new patient. However, if the patient was seen by a physician of the exact same specialty and exact same subspecialty in the group within the last three years, the patient is considered an estab-lished patient.
E/M coding for Medicare outpatients seen in the emergency department (ED) poses a unique
E/M coding can be easier than one might thinkby Mark T. Savarise, MD, FACS; Linda M. Barney, MD, FACS; and Jenny Jackson, MPH
set of challenges. For Medicare patients, these visits should be reported with the ED codes (99281–99285). For non-Medicare patients (un-less otherwise instructed by a payor), outpatient consultations provided in the ED are reported with codes 99241–99245. Example: A general surgeon is called to the ED to see a 75-year-old Medicare fee-for-service patient for assessment of abdominal distention, nausea, and vomiting. The surgeon documents a detailed history and performs a detailed examination. The medical decision making is of moderate complexity. The
Coding highlight
Your specialty is general surgery. Your plastic surgeon partner saw a patient for an abomino-
plasty two years ago. The 65-year-old fee-for-service Medicare patient is now complaining of breast pain. Your partner refers the patient to you for a consult. You conduct a comprehensive history and examination, and the medical decision making is of moderate complexity.
Reportable procedure:99204–Office or other outpatient visit for the evaluation and management of a new patient.
The patient was referred to the general surgeon by a plastic surgeon for a consultation. However, the patient is a fee-for-service Medicare patient, and Medicare no longer pays for consultations. Office consultations are reported with the new patient (99201–99205) or established patient (99212–99215) CPT codes. Although this patient has been seen by another physician in the same group practice in the past three years, the physician is of a different specialty. As a result, this patient is considered a new patient for the general surgeon.
*All specific references to CPT (Current Procedural Terminology) terminology and phraseology are © 2010 American Medical Association. All rights reserved. continued on page 43
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
41

How to code consultations
Consultation code History Exam Medical decision
making
New patient(not seen in
the past three years)
Established patient (seen in the past
three years)
Outpatient
99241 Problem focused Problem focused Straightforward 99201 99212
99242 Expanded problem focused
Expanded problem focused Straightforward 99202 99213
99243 Detailed Detailed Low complexity 99203 99214
99244 Comprehensive Comprehensive Moderate complexity 99204 99215
99245 Comprehensive Comprehensive High complexity 99205 99215
Inpatient
99251 Problem focused Problem focused Straightforward
99252 Expanded problem focused
Expanded problem focused Straightforward
99253 Detailed Detailed Low complexity 99221 99221
99254 Comprehensive Comprehensive Moderate complexity 99222 99222
99255 Comprehensive Comprehensive High complexity 99223 99223
CPT code Subsequent observation
99224 Subsequent observation care, per day, for the evaluation and management of a patient, which requires at least 2 of these 3 key components: Problem focused interval history; Problem focused examination; Medical decision making that is straightforward or of low complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is stable, recovering, or improving. Physicians typically spend 15 minutes at the bedside and on the patient’s hospital floor or unit.
99225 Subsequent observation care, per day, for the evaluation and management of a patient, which requires at least 2 of these 3 key components: An expanded problem focused interval history; An expanded problem focused examination; Medical decision making of moderate complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is responding inadequately to therapy or has developed a minor complication. Physicians typically spend 25 minutes at the bedside and on the patient’s hospital floor or unit.
99226 Subsequent observation care, per day, for the evaluation and management of a patient, which requires at least 2 of these 3 key components: A detailed interval history; A detailed examination; Medical decision making of high complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is unstable or has developed a significant complication or a significant new problem. Physicians typically spend 35 minutes at the bedside and on the patient’s hospital floor or unit.
Source: American Medical Association (AMA). Current Procedural Terminology. Chicago, IL: AMA. 2010.
Source: American Medical Association (AMA). Current Procedural Terminology. Chicago, IL: AMA. 2010.
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
42

patient has never been seen by the general sur-geon in the office or at the hospital. The patient is sent home from the ED. For a Medicare fee-for-service patient, this case would be coded as 99284. For a non-Medicare patient, this would be coded as 99243.
Initial inpatient consultations for Medicare patients should be reported with the initial hospital care codes (99221–99223), even when someone other than the admitting physician con-ducts the consultation. The admitting physician uses modifier “AI” to designate that he or she is the principal physician of record. For example, take the same patient mentioned in the previ-ous example, seen in the ED. However, this time after the exam, the surgeon decides to admit the patient. In this instance, the surgeons should use code 99221 with the AI modifier. On the other hand, if the Medicare patient was admitted by a gastroenterologist and later the general surgeon sees the patient for surgical assessment, performs a detailed history and a detailed examination, and the medical decision making is low complexity, the general surgeon would report 99221 without modifier AI. For non-Medicare patients, the cor-rect code to report for the inpatient consultation would be 99253.
Subsequent observationSubsequent observation care, per day, is now
reported with a series of new codes (99224, 99225, 99226), meaning that surgeons now can report observation services that extend beyond the initial day of care. These codes are com-parable to subsequent hospital care, but are reported for patients admitted for observation instead of inpatient facility status. All levels of subsequent observation care include reviewing the medical records, results of diagnostic stud-ies, and changes in the patient’s status (such as changes in patient history, physical condition, and response to management) since the physi-cian’s last assessment.
As an example, a general surgeon performs a comprehensive history on a 78-year-old patient who fell and suffered contusions to the head and shoulder, but no fractures. The patient, who has a history of stroke, is currently on Warfarin. Medi-cal decision making is of high complexity. The patient is admitted to observation care. On the
next day, the surgeon performs a detailed interval history and medical decision making continues to be of high complexity, with assessment for stability and possible intervention for internal bleeding. The patient remains in observation sta-tus and is not discharged. The initial observation care visit on the first day is coded as 99220. The subsequent observation care visit on the second day is coded as 99226. The subsequent observa-tion care codes would be reported daily until the patient is discharged. The code for observation care discharge day management is 99217.
If you have any questions or comments on this article, contact Jenny Jackson at [email protected] or 202-672-1506. If you have additional coding questions, contact the Coding Hotline at 800-227-7911 between 8:00 am and 5:00 pm CST, excluding holidays.
Dr. Savarise is a general surgeon in Sandpoint, ID. He is the ACS Alternate Advisor to the AMA CPT Advisory Committee, and a member of the ACS General Surgery Coding and Reimbursement Committee
Dr. Barney is a general surgeon and associate professor of surgery, Wright State University Boonshoft School of Medicine, and associate director for the general surgery residency program, Miami Valley Hospital, Dayton, OH. She is the ACS Advisor on the AMA CPT Advisory Com-mittee, and a member of the ACS General Surgery Coding and Reimbursement Committee.
Ms. Jackson is Practice Affairs Associate, Division of Advocacy and Health Policy, Washington, DC.
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
43

Advocacy advisor
Now, more than ever, it is important that surgeons serve as advocates for their profession and their patients. To truly
navigate the legislative process and be a strong advocate for surgery, it is helpful to understand how the U.S. Congress and the state legislatures function. This article offers some insight into how these different levels of government work, their power structures, and the roles and respon-sibilities of state and federal legislators.
U.S. House of RepresentativesThe legislative branch of the federal govern-
ment is divided into two chambers: the House of Representatives and the Senate. The number of representatives who serve each state varies based on population, but each state has at least one House member representing approximately 700,000 people. The size of each state’s congres-sional delegation may change every 10 years, depending on the population results from the U.S. Census, with the total number of voting representatives in the House set at 435 members. House members serve two-year terms, and elec-tions are held every November of even-numbered years. The qualifications for a representative include the following: he or she must be at least 25 years of age, be able to demonstrate U.S. citizenship for the past seven years, and be a resident of the state (not district) during the time of the election.1
The House initiates and passes many pieces of legislation, but it has the exclusive power to initiate revenue bills. Therefore, any bill that proposes an increase or change in federal taxes must start in the House.1 The House also has the ability to impeach officials and to declare the president in an Electoral College deadlock.
The party with the majority of seats in the House elects one of its members to be the Speak-er and to serve as leader of the majority party. The Speaker of the House is charged with the following responsibilities: he or she designates all the committee chairs, who are usually mem-
Navigating the legislative processby Charlotte Grill
bers of the majority party; determines which bills each committee will review; and acts as the presiding officer over the House. No member may speak or make a motion without permission from the presiding officer, and the Speaker may delegate that responsibility to other members in the House.2
Many other leadership roles exist within the House, reaching down to the level of committee and subcommittee chairs. The House of Rep-resentatives’ website (http://www.house.gov) provides useful information on these roles, as well as details on the House legislative process, committee assignments, contact information for members and their staff, and bill assignments to committees.
U.S. Senate The Senate is the upper chamber of Congress.
Each state has two U.S. senators who serve six-year terms. Senators often are perceived as having more clout and prestige than represen-tatives due to their longer terms, smaller group size, larger state-wide constituencies, and less pressure to vote along party lines.
Senators draft, introduce, and amend legisla-tion along with the exclusive duties of agreeing to treaties as a precondition to their approval, and vetting and approving Cabinet appoint-ments, federal judges, military officers, ambas-sadors, and other federal and regulatory officials. The qualifications to serve in the Senate are also slightly more stringent than in the House. Senators must meet the following criteria: he or she must be at least 30 years old, demonstrate U.S. citizenship for the past nine years, and be a resident of the state during the time of election.3 Elections for senators are also held in Novem-ber, and in the event that a senate seat becomes vacant, 46 states permit the governor to appoint the seat, while Oregon and Wisconsin require special elections. Other exceptions to the gover-nor appointing a vacant senate seat are in place in Oklahoma, where the governor appoints the
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
44

winner of a special election, and Massachusetts, where a governor appoints a temporary replace-ment until a special election is held.3
As in the House, the majority party holds the positions of leadership such as the committee chair seats. The presiding officer of the Senate is technically the vice-president; however, the vice-president does not attend most session days. The Senate elects a president pro tempore who fills in when the vice-president is absent and typically delegates the responsibility of presiding to junior senators so they can learn the procedures of the Senate floor.3 The powers of the presiding officer are far less extensive than those of Speaker of the House. The presiding officer calls on senators to speak, determines the order that objections are voiced, and announces the outcomes of votes. The Senate majority leader controls the agenda, and schedules debates and votes.3
For more details about the Senate, visit http://www.senate.gov.
State governmentEach state government is its own entity and
has its own state constitution and rules for governing. State governments are organized and structured in a way that mirrors the federal government, although state legislatures can function on either a full-time or part-time basis. The part-timers usually convene every other year and meet in the January of odd-numbered years.4 State representatives and senators in these states usually have full-time employment outside of their state position. Full-time legisla-tures often have full-time legislators, and their sessions may run all year with periodic breaks. Depending on the length of their legislative ses-sion and salary, legislators in these states may have outside employment.4
The primary function of state legislatures is to write and vote on state-level legislation introduced by legislators or the governor. They approve operating and capital budgets and de-cide how the state will raise and spend money. In addition, they have the power to impeach and convict executive and judicial office holders. Generally speaking, state senates have the exclu-sive power to confirm appointments made by the governor and to try articles of impeachment, and most states have given the house/assembly the
exclusive power to initiate tax bills. Beyond law-making, legislators have other responsibilities back in their districts, such as making speeches at public events, meeting with community orga-nizations and groups, and serving as a liaison on behalf of their constituents to resolve problems with state agencies and inform constituents of available state programs and services.4
Each state has an executive branch, which is led by the governor. Other elected officials in the executive branch include the lieutenant governor, attorney general, secretary of state, and other auditors and commissioners. These officials serve four-year terms.
Every state has a two-chamber legislature modeled after the U.S. Congress. The smaller chamber is the senate and the larger chamber is most often called the house of representatives. (Nebraska is the only exception to this rule, and they have only one chamber, the senate.4) Five states call the larger chamber the assembly (California, Nevada, New Jersey, New York, and Wisconsin), and three call it the house of del-egates (Maryland, Virginia, and West Virginia).4
A speaker usually presides over the house/ assembly, and a senate president presides over the senate. State senators serve four-year terms and house/assembly members serve two-year terms.4 In most states, each senate district is divided into two house/assembly districts. Committees are assigned in a similar manner to Congress in that chairs are determined by seniority, and the majority party and bills are assigned to particular committees. State legis-latures also rely heavily on party affiliation to determine how responsibilities and power are delegated and which bills are pushed to the front of the agenda.4
A couple of useful websites are available to surgeons who want to contact state representa-tives and senators and to get detailed informa-tion on a state’s legislative process. The Surgery State Legislative Action Center is a convenient place to identify state legislators and their contact information (http://www.facs.org/sslac/index.html), and the National Conference of
Ms. Grill is State Affairs Associate, Division of Advo-cacy and Health Policy, Chicago, IL.
continued on page 60
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
45

College news
Current ACS NSQIP participants and leaders shared advice and tips with Florida’s new surgeon champions and surgical clinical reviewers. Speakers included (left to right): Jillian Knight, RN, surgical clinical reviewer at Baptist Hospital of Miami; Jennifer Ritz, RN, project manager, Surgical Quality Improvement, Henry Ford Hospital, Detroit, MI; Dr. Morton; and Dr. Ko.
More than 170 Florida surgeons, nurses, and quality improvement leaders heard from local and national speakers during the day-long FSCI kickoff event, including Bruce Spurlock, MD (standing), president and CEO of Convergence Health Consulting, Inc., and a national expert on collaborative quality improvement.
More than 170 physicians, nurses, and administrative leaders convened at the Orlando Hyatt on February 3 to launch the Florida Surgical Care Initia-tive (FSCI). This collaboration of the Florida Hospital Associa-tion (FHA) with the American College of Surgeons (ACS) rep-resents the largest group of hos-pitals from a single state to use the National Surgical Quality Improvement Program® (ACS NSQIP®) methodology to track performance and drive surgical quality improvement across all areas of the state.
Introducing the program, Bruce Rueben, chief executive officer of the FHA, and Ernest Block, MD, FACS, President of the College’s Florida Chapter, affirmed the commitment of both the association and sur-geons in the state of Florida to meet head-on the issues that relate to surgical care across a state with a population that is now the fourth largest in the country. Specifically focusing on issues that define the unique characteristics of the surgical patient in Florida, Mr. Rueben emphasized that this project is a unique opportunity for physi-cians and hospital leadership to apply objective clinical data to define best practice and ensure that quality is both optimal and continuously improving.
Speaking on behalf of Blue Cross Blue Shield of Florida, which has committed to provide funding support for the project’s
FHA/ACS launch largest statewide surgical quality improvement initative
first two years, Brian Kiss, MD, senior medical director, empha-sized the critical importance of defining optimal outcomes. He said that determining effective
strategies to minimize compli-cations will yield better patient care, control cost, and enable more resources to be used to broaden the spectrum of clini-
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
46

cal care. In addition, Dr. Kiss stated that accurate assessment of the disease profile of surgical patients in Florida will provide a more accurate, clinically rel-evant definition of risk and will stimulate prevention strategies that will control or eliminate risk before it contributes to potentially catastrophic periop-erative complications.
Clifford Ko, MD, FACS, Di-rector of the College’s Division of Research and Optimal Pa-tient Care, which includes ACS NSQIP as one of the programs it oversees, described the basic process of the FSCI. Dr. Ko emphasized that ACS NSQIP program experience clearly shows that hospitals performing above expectation continue to improve, and that all other hos-pitals demonstrate significant improvement in their overall performance. He explained that a study in the September 2009 issue of Annals of Surgery found that ACS NSQIP partici-pants prevent between 250 to 500 complications per hospital per year and save 13–27 lives.*
The FSCI will focus on factors that are somewhat unique to the Florida population, Dr. Ko said, including surgical site in-fection, urinary tract infection,
colorectal surgery outcomes, and “elderly surgery outcomes.” He added that the last factor is critically important in defining relevance, applicability, and outcomes in surgical treatment of our aging population.
The four FSCI measures were developed by the College in collaboration with the Centers for Medicare & Medicaid Ser-vices (CMS), following studies showing that process mea-sures—such as those used in the Surgical Care Improvement Project (SCIP)—do not neces-sarily correlate with improved patient outcomes.† The CMS is currently considering the four measures for possible national implementation as early as January 2012. As regulators and policymakers focus on risk-adjusted, outcomes-based quality measurement, surgeons have the opportunity to pro-vide a national model for how to improve the quality of care, while reducing the added costs of preventable complications.
Joseph J. Tepas III, MD, FACS, FAAP, project coordina-tor for the Florida Chapter, emphasized that much of the information that will emerge from this statewide program will help guide transformation of the Florida Medicaid Man-aged Care program into a more cost-effective, evidence-based, integrated health care delivery system. He explained that clini-cal data compiled by surgical case registrars will precisely define profiles of patient co-morbidities, produce objective measures of surgical risk, and support definition of disease-based, integrated clinical care. Objective assessment of surgical
outcomes throughout the state will help define best practice and stimulate dissemination of efficient, cost-effective care. Dr. Tepas added that this program is the core from which this new system of health care delivery will emerge, and is an outstand-ing opportunity for all Florida surgeons to begin actively par-ticipating in this process.
The 102 hospitals that have expressed interest in partici-pating in FSCI will focus on any or all of the four measures described earlier in this article. Surgeon champions from these hospitals will also function as a statewide users group to facili-tate the process and to collabo-rate with leaders of the FHA in results analysis and ongoing direction of the project. John Morton, MD, FACS, Associate Chairman of the ACS NSQIP Surgeon Champions, reviewed the role of the surgeon champi-on in monitoring data collection and providing meaningful feed-back of results to colleagues. Included in this initiative, he said, is the intent to ensure that active involvement in this ACS NSQIP process meets criteria for Maintenance of Certifica-tion. He added that participat-ing members of the Florida Chapter will also function as a users group that will guide continued growth of surgical quality throughout the state.
The inaugural meeting of this group was held during a session on current and future challenges to delivery of surgi-cal care that took place as part of the Florida Chapter’s annual meeting in March.
*Hall BL, Hamilton BH, Richards K, Bilimoria KY, Cohen ME, Ko CY. Does surgical quality improve in the American College of Surgeons National Surgical Quality Improvement Program: An evaluation of all participating hospitals. Ann Surg. 2009; 250(3):363-376. †Ingraham AM, Cohen ME, Bilimoria KY, Dimick JB, Richards KE, Raval MV, Fleisher LA, Hall BL, Ko CY. Association of surgical care improvement project infection-related process measure compliance with risk-adjusted outcomes: Implications for quality measurement. J Am Coll Surg. 2010;211(6):705-714.
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
47

Didyou know... THAT THE COMPREHENSIVE
GENERAL SURGERy REVIEW COURSE sponsored by the American College of Surgeons (ACS) will be offered twice in 2011? The course—which is being held in response to the demand for last year’sinauguralcourse—willbeofferedMay19–22andJune23–26,inChicago, IL. The intensive four-day review course will cover the essen-tial content areas in general surgery, including Abdomen, Alimentary Tract, Breast, Endocrine, Oncology, Perioperative Care, Skin and Soft Tissue,SurgicalCriticalCare,Trauma,andVascular.CourseChairJohnA. Weigelt, MD, FACS, and a distinguished faculty will use didactic and case-based formats for a comprehensive and practical review. Course features include a variety of self-assessment materials, and four addi-tional monthly online modules following the course. Organized by the ACS Division of Education, this course will help fulfill the requirements for Maintenance of Certification, Part 2, and should be helpful in pre-paring for recertification examinations. For more information, contact [email protected], call 312-202-5018, or visit http://www.facs.org/ education/reviewcourse.html.
Although hand hygiene has become such a standard practice in operating rooms (ORs) that going into the OR and touch-ing a patient without having performed preoperative hand prep would almost certainly not be tolerated, surgeons still need information about how their behavior impacts outcomes. For example, the Joint Commission Center for Transforming Health-
A look at The Joint Commission
Engaging physicians in hand hygiene challenges
care recently found that some of the nation’s leading hospitals and health systems had hand hygiene compliance rates of less than 50 percent due to issues such as ineffective placement of dispensers or sinks, a lack of accountability and just-in-time coaching, and a safety culture that did not stress hand hygiene at all levels.
To build on the work of the center and show physicians how infection prevention interven-tions, such as rigorous hand hy-giene, impact their work and the care of their patients—which, in
turn, promotes greater physician interest and involvement—orga-nizations should share informa-tion such as the following:
• Forsurgeons,specificsur-gical site infection rates
• Rates for central line- associated bloodstream infec-tions, vascular catheter-asso-ciated infections, Clostridium difficile, multidrug-resistant organisms, surgical site in-fections, ventilator-associated pneumonia, and catheter- associated urinary tract infec-tions
• Sentinel event figures re-lated to health care-associated infections, along with root cause analyses findings
• Policiesaffectingphysicianpractice, along with requests for input on new or proposed poli-cies
In addition, physicians need continuing education regarding current best practices and new guidelines or strategies. For example, studies have shown that physician compliance with hand hygiene increases when the physicians believe the following:
• Theyarebeingobserved• They are serving as role
models for colleagues• Patientsbenefitfromeffec-
tive hand hygiene• Alcohol-based hand rubs
are easily accessible• Their performance is not
up to par as compared with peers*
*Pittet D, Simon A, Hugonnet S, Pessoa-Silva C, Sauvan V, Perneger T. Hand hygiene among physicians: Performance, beliefs, and perceptions. Ann Int Med. 2004;141(1):1-8.
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
48

Surgeons also can play a crucial role in implementing the center’s hand hygiene solutions, which are available through the Targeted Solu-tions Tool™ (TST), by serving as a physician champion on a
multidisciplinary committee.Next month’s column (May
2011) will feature information about the TST and how sur-geons can participate in organi-zation-wide efforts through the TST to prevent hand hygiene related infections. For more in-formation on the TST process, see the December 2010 issue of the Bulletin.†
For more information about the causes of hand hygiene failures and targeted solu-tions to address these fail-ures, visit the Joint Com-mission Center for Center for Transforming at http://www.centerfortransforming healthcare.org.
†A look at The Joint Commission: Center for Transforming Healthcare releases targeted solutions tool. Bull Am Coll Surg. 2010;95(12):39.
Vikram S. Kashyap, MD, FACS, co-director of the Uni-versity Hospitals Harrington- McLaughlin Heart & Vascular Institute, Case Medical Center, Cleveland, OH, has been selected as the ACS Traveling Fellow to Australia and New Zealand (ANZ) for 2012.
As the Traveling Fellow, Dr. Kashyap will participate in the annual Scientific Congress of the Royal Australasian College of Surgeons in Kuala Lumpur, Malaysia, May 7–11, 2012. He will address the ANZ Chapter meeting during that congress and will then travel to several surgical centers in Australia
ANZ Traveling Fellow selected for 2012and New Zealand.
Dr. Kashyap’s research focus-es on the interaction between arterial thrombosis and endo-thelial function, and he looks forward to sharing ideas with ANZ colleagues at the cutting edge of endovascular therapies.
The application deadline for the 2013 ANZ Traveling Fellowship is November 15, 2011. The requirements for the 2013 Traveling Fellow-ship will appear later this year in the Bulletin, and will also be posted on the Col-lege’s Scholarships Web page, http://www.facs.org/member services/research.html.
Dr. Kashyap
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
49

A m e r i c A n c o l l e g e o f S u r g e o n S ● D i v i S i o n o f e D u c A t i o n
Medical student
guide to residency training
So, You Want to Be a Surgeon...
The online resource, So, You Want to Be a Surgeon…A
Medical Student Guide to Finding and Matching with the
Best Possible Surgery Residency, is now available on the
American College of Surgeons Web site at:
http://www.facs.org/residencysearch
This online, contemporary version of the popular “Little
Red Book” has proved to be an invaluable resource for
medical students seeking opportunities in graduate medi-
cal education. The revised online version of this helpful
reference includes a searchable database containing a
complete list of accredited surgical specialty residency
programs, as well as a section devoted to assisting
students in choosing a residency program that is their
best match.
For further information, contact Elisabeth Davis, MA,
Education Research Associate, Division of Education,
at 312-202-5192, or via e-mail at [email protected].
Little Red Book-Bulletin (rev 06-07).indd 1 3/2/2010 3:16:34 PM

ACS Members who are recertifying can now enjoy the ease of submitting their ACS CME credits directly to the American Board of Surgery (ABS).
From members’ MyCME page, click on the “Send CME to ABS” option at the top of the page.
Submission is quick and easy:→ Review your transcript for accuracy
and authorize transfer of credits→ Have your ABS 13-digit
authorization number ready
Now AvAilABlE from the American College of Surgeons
Transfer your ACS CME credit to the American Board of Surgery electronically!
!
MyCMEY o u r C M E @ Y o u r C o n v E n i E n C E
log into the member web portal at www.eFACS.org to get started
A M E R i C A N C o l l E g E o F S u R g E o N S • D i v i S i o N o F E D u C A t i o N
CME to ABS ad - June 2010 BULLETIN (4 inches deep).indd 1 7/29/2010 11:12:44 AM
The first statewide initiative in the nation to focus on mea-suring and improving safety and quality of care for trauma patients has been launched by Blue Cross Blue Shield of Michigan, Blue Care Network, and 22 trauma centers through-out the state, in partnership with the American College of Surgeons (ACS). The Michigan Trauma Quality Improvement Program will create a statewide infrastructure for trauma hos-pitals to measure and improve patient outcomes, identify best practices for quality and safety of care, and share data to make trauma care more effective.
Joint trauma quality care initiative launched in Michigan
Each participating hospital will enroll in the national ACS Trauma Quality Improvement Program.
According to the National Trau-ma Institute (http://www.national traumainstitute.org/the_case_for_trauma_funding.html):
...traumatic injury is a major public health problem in the United States. Each year, trauma ac-counts for 37 million emergency department visits and 2.6 million hospital admissions. The effect of trauma on productive life years lost exceeds that of any other disease. The economic cost in the year 2000 was $406 billion, which includes
estimates of $80 billion in medical care costs.
Mark Hemmila, MD, FACS, associate professor of surgery at the University of Michigan, Ann Arbor, is serving as the collaborative’s program direc-tor. The University of Michigan Health System will act as the coordinating center, and will collect and analyze clinical data from participating hospitals. The first phase of the initiative launched in January 2011. The second phase is expected to be completed by January 2012. To learn more, go to http://www.valuepartnerships.com.
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
51

VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
52
You’re reading articles every month in theJournal of the American College of Surgeons...
Why not get Maintenance of Certification self-assessment CME credit?
Need to earn CME credit?
We make it easy!
Visit
http://jacscme.facs.org for more information
Convenient ◆ Free For FeLLoWS and SUBSCriBerS
each completed article receives 1.0 CMe-1 credit
track your CMe online at the “My CMe” page at www.e-FaCS.org
JACS online CME - Feb 2010 - Bulletin REVISED.indd 1 2/17/2010 2:27:40 PM

Every year as the American College of Surgeons (ACS) Clini-cal Congress approaches, I begin to wonder what this meeting will offer me. How can the Clinical Congress impact the way I prac-tice surgery? And most impor-tantly, how am I going to take the best advantage of the opportuni-ties and information presented at this annual meeting?
As I reflect on my experiences at the 2010 Clinical Congress in Washington, DC, I would say, without a doubt, that the Nizar N. Oweida, MD, FACS, Scholar-ship made this meeting the most fruitful and memorable I have attended thus far.
I have to start by expressing my gratitude for the finan-cial support that was provided through the scholarship, which allowed me the opportunity to attend excellent postgraduate courses. The skills-oriented postgraduate courses I was most interested in were Fundamen-tals of Breast Imaging for the General Surgeon and Thyroid and Parathyroid Ultrasound. I was able to see an immediate benefit for my patients once I returned to my practice in Maine. I am now able to perform ultrasound-guided biopsies more precisely and more efficiently.
The Nizar N. Oweida Schol-arship made it possible for me to continue maintaining some of my skills at the highest level, and allowed me to obtain educational materials that I am constantly reviewing, such
Report of the 2010 Oweida Scholarby Fernando Navarro, MD, FACS
as the Surgical Education and Self-Assessment Program™14, and ACS webcasts and audio recordings from the meeting. The scholarship also gave me the freedom to enjoy other courses and sessions that I have always been interested in, such as Surgeons As Effective Com-municators: Sharpening Skills for Critical Moments, among others.
I was also invited to partici-pate in the Scholarships Com-mittee meeting and the Rural Surgery Symposium. At the Scholarships Committee meet-ing, other awardees discussed fascinating research projects sponsored by the College. I was given the opportunity to talk about my general surgery practice and to share some of my day-to-day experiences with a very distinguished audience.
I enjoyed answering audience members’ questions about dif-ferent facets of rural surgery, but most important for me was the opportunity to voice how important it is for rural surgeons to continue getting support from the College. The Rural Surgery Symposium was very informative. It was im-portant for me to be educated on the current state of rural surgery and what the College’s leadership is doing for these patients.
It was a great honor to be the recipient of the Nizar N. Oweida Scholarship, and I would like to deeply thank the Oweida family for their support and generosity.
Dr. Navarro is a general surgeon in a small town in western Maine that provides services to approximately 15,000 people in the region.
Dr. Navarro speaking at the 2010 Clinical Congress, as Stephen E. Olson, MD, FACS, Chair of the Rural Surgery Subcommittee of the Advisory Council for General Surgery, looks on.
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
53

.gov .net .com .edu .gov .net .com .e .gov .net .com .edu .gov .net .com .
edu .gov .net .com .edu .gov .net .com om .edu .gov .net .com .edu .gov .net et .com .edu .gov
.net .com .edu .gov .net .com .edu .gov .net .com .edu .com .edu .gov .net .com .edu .gov
.net .gov .net .com .edu .gov .net .com .e .gov .net .com .edu .gov .net .com .
edu .gov .net .com .edu .gov .net .com om .edu .gov .net .com .edu .gov .net et .com .edu .gov
.net .com .edu .gov. .net .com .edu .gov .net .com .edu .com .edu .gov .net .com .edu .gov
.net .gov .net .com .edu .gov .net .com .edu .gov .net .com .edu gov .net .com .edu .gov .net
.com .edu .gov .net .com om .edu .gov .net .com .edu .gov .net et .com .edu .gov .net .com
.edu .gov .net .com .edu .gov .net .com .edu .gov .net .com .edu .gov .net com .edu .gov .net .com
.edu .gov .net com .edu .gov .net .com .edu .gov
@We need your help!Don’t miss out on important communications from the American Collegeof Surgeons.
Send us your e-mail address today.
Current events in Washington, DC, and in all sectors of our society are changing with dizzying rapidity, and the College is working to keep you informed.
The most timely and efficient way to do that is via e-mail. So it’s very important that we have
your current e-mail address in our database.
Not sure if we have your current address? Go to the “My Page” area of the ACS Members-only Web portal at
www.efacs.orgto see what’s currently in our database and
to make necessary changes.
If you have questions or problems, contact [email protected].
Include your Fellowship ID number in your note.
Important note:the american College of
Surgeons does not provide your e-mail address to outside
entities. e-mail addresses are used only for College communications.
E-mail 2009 ad - Bulletin.indd 1 8/18/2009 3:15:30 PM

NTDB® data points
The road to the Super Bowlby Richard J. Fantus, MD, FACS
Hospital discharge statusI could not help but feel that I was at work as I sat at frigid Soldier Field watching the Chi-cago Bears battle the Seattle Seahawks in the playoffs this past January—where players left a trail of traumatic injuries in their wake. The first play of the game resulted in a Seahawk being taken off the field on a backboard with a cervical col-lar, after being hit by a defender and getting slammed into the frozen turf. Later in the game, another untimely departure happened after a second Seattle player was knocked out by the knee of a large tight end. For-tunately, these players were released from a local hospital the following day. Bone-jarring tackles and impacts such as these take place close to 100 times in each National Football League (NFL) game.
The impact of an average defensive back who is about six feet tall and 200 pounds, run-ning a four-and-one-half second 40-yard dash, can produce 1,600 pounds of tackling force. The shock absorbency of the field’s landing surface is measured by a metric called G-Max. To
configure the G-Max, one drops an object that approximates the human head and neck (20 square inches and 20 pounds) from a height of two feet. A low G-Max score implies a softer and more absorbent surface. Grass fields run about 60 on the G-Max scale, while synthetic turf is 120; frozen grass has the highest G-Max score.
When thinking about high G-Force activities, a fighter pi-lot doing a jet roll often comes to mind. A jet roll produces a G-Force of 9.0; however, the aforementioned football im-pact on a frozen field can result in a G-Force as high as 150 (http://www.popularmechanics. com/outdoors/sports/physics/ 4212171).
It is no wonder, then, that in 2009 there were more than 300,000 football-related concus-sions and 45,000 head injuries that were serious enough to require treatment in U.S. emer-gency rooms.* The alarming numbers have led the NFL to take a stronger stance against helmet-to-helmet contact inju-ries. The organization is also requiring a more in-depth medi-cal evaluation regarding when a player can be cleared to return to play after sustaining a con-cussion. A joint effort between the NFL, the NFL Players Asso-ciation, the Centers for Disease Control and Prevention, the Professional Football Athletic Trainers Society, and the NFL Physicians Society resulted in
*American Association of Neurological Surgeons. Back to school means football and cheerleading: Injury prevention pips from the AANS. Press release. Available at: http://www.aans.org/~/media/Files/Patient%20Information/Neurosurgery%20Outreach%20Month/NeurosurgeryOutreachMonth.ashx. Accessed on February 21, 2011.
Hospital discharge status
99.1%
0.7%
0.2%
Home
Acute care/rehab
Nursing home
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
55

the development of a poster in early 2010, titled “Concussion— Let’s take brain injuries out of play,” which now hangs in every NFL locker room in the country. A similar poster that is aimed at younger athletes involved in virtually every sport was developed by several of the previously mentioned organizations, in addition to 14 national governing bodies for sports, and is endorsed by the American College of Emergency Physicians and the American Association of Neurologic Surgeons (http://www.cdc.gov/concussion/sports/nfl_poster.html).
In order to examine the occurrence of concussions in football in the National Trauma Data Bank® research dataset 2009, admissions re-cords were searched utilizing the International Classifica-tion of Diseases, Ninth Revi-sion, Clinical Modification (ICD-9-CM) cause of injury code 850 (concussion), which included a place of injury E-code E849.4 (recreation area)
and also had one of the follow-ing cause of injury E-codes: E917.0 (striking or struck ac-cidentally by objects or persons in sports without subsequent fall), E917.6 (with subsequent fall), or E886.0 (fall in sports). There were 704 records that include the subset of football concussions. A total of 536 records had discharge status recorded, including 531 dis-charged to home, four to acute care/rehab, and one sent to a nursing home; none died. These patients were 83 percent male, on average 18.3 years of age, had an average length of stay of 1.5 days, and an average injury severity score of 5.44. Fortunately, almost all were discharged to home and no one died. (These data are depicted in the figure on page 55.)
No one will argue that foot-ball is a contact sport. Unfor-tunately, injuries occur at all levels of football, from pee wee all the way to the pros. By sheer numbers and attrition as athletes ascend through the ranks of high school and
collegiate football, there are far more youths injured while playing football than adults at the professional level. Concus-sions are widespread and know no age limit. It is about time that the seriousness of football concussions has made it into prime time. This stance on protecting players from serious permanent injury by recogniz-ing the signs and symptoms of traumatic brain injury has fortunately trickled all the way down to the pee wees. After all, the road to the Super Bowl should be one of glory, not one littered with head-injured players.
Throughout the year, we will be highlighting data through brief reports that will be found monthly in the Bulletin. The NTDB Annual Report 2010 is available on the ACS website as a PDF file and a PowerPoint presentation at http://www.ntdb.org. In addition, informa-tion is available on our website about how to obtain NTDB data for more detailed study. If you are interested in submitting your trauma center’s data con-tact Melanie L. Neal, Manager, NTDB, at [email protected].
Acknowledgment
Statistical support for this ar-ticle has been provided by Chrystal Price, data analyst, NTDB.
Dr. Fantus is director, trauma ser-vices, and chief, section of surgical critical care, Advocate Illinois Ma-sonic Medical Center, and clinical professor of surgery, University of Illinois College of Medicine, Chi-cago, IL. He is Past-Chair of the ad hoc Trauma Registry Advisory Committee of the Committee on Trauma.
The following continuing medi-cal education courses in trauma are cosponsored by the American College of Surgeons Committee on Trauma and Regional Com-mittees:
• Point/ Counterpoint, June 13–15, 2011, National Har-bor, MD.
• Advances in Trauma,
December 9–10, 2011, Kansas City, MO.
Complete course informa-tion can be viewed online (as it becomes available) through the American College of Surgeons’ website at http://www.facs.org/trauma/cme/traumtgs.html, or contact the Trauma Office at 312-202-5342.
Trauma meetings calendar
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
56
Sponsored by
American College of Surgeons
The Doctors Company is devoted to helping doctors avoid potential lawsuits. For us, this starts with patient safety.
In fact, we have the largest Department of Patient Safety/Risk Management of any medical malpractice insurer.
And, local physician advisory boards across the country. Why do we go this far? Because sometimes the best
way to look out for the doctor is to start with the patient. Our medical professional liability program has been
sponsored by ACS since 2002. To learn more about our program for ACS members, call (800) 862-0375 or visit
us at www.thedoctors.com.
We hate lawsuits. We loathe litigation. We help doctors head off claims at the pass. We track new treatments and analyze medical advances. We are the eyes in the back of your head. We make CME easy, free, and online. We do extra homework. We protect good medicine. We are your guardian angels. We are The Doctors Company.
Donald J. Palmisano, MD, JD, FACSBoard of Governors, The Doctors CompanyPast President, American Medical Association
A2649_ACS_Bulletin_Protect.indd 1 3/2/09 3:55:40 PM

made regarding whether the procedure is eligible for payment under the HSIP program.
How did this new HSIP general surgery bonus payment program originate?
The concept of a bonus payment to promote general surgery in rural and other underserved areas is one that the ACS staff promoted during the early discussions about health care reform with Senate Committee on Finance advisors. Due to the fact that the Chairman of the Senate Com-mittee on Finance is Sen. Max Baucus (D-MT), from a rural state facing surgeon shortages, the Senate Committee on Finance staff members have been sympathetic to the College’s concerns about a diminishing number of general surgeons in rural and frontier areas. In April 2009, the ACS advocacy staff met with Senate Committee on
Finance advisors to propose legislative language with the purpose of encouraging general surgeons to provide surgical care in areas where there is a general surgery workforce shortage. These discus-sions led to the inclusion of the HSIP provision in the ACA, which establishes the bonus payment to general surgeons for major procedures performed in geographic HPSAs between January 1, 2011, and January 1, 2016.
Where can I read more?
For more information on the implementa-tion of the HSIP bonus payment, review the Medicare Learning Network Matters document at https://www.cms.gov/MLNMattersArticles/downloads/SE1023.pdf or Change Request 7063 at http://www3.cms.gov/transmittals/downloads/R2040CP.pdf.
WHAT SURGEONS SHOULD KNOW ABOUT..., from page 13
More than 11,000 kits have already been distributed.
Future kits: Central Line • Feeding Tubes • Thoracic Surgery
Surgical Patient Education Program
Thesupports patients with education and simulation materials to learn and practice the skills needed for optimal postoperative recovery.Skills kit contains:• Practice equipment (pouch, scissors, stoma model, measure-
ment guide, surgical marker)• DVD with skill demonstration• Skills instruction booklet with images• Self-assessment checklist• References for additional support
Professional training guide contains:• Directions for use• Evalution criteria
• Measurement guidelines for documenting quality improvement
H e l p i n g y o u w i t h h o m e c a r e
AMERICAN COLLEGE OF SURGEONS
DIVISION OF EDUCATION
HomeSkillsKit
O s t o m y
Patient Education Partners in Your Surgical Care©
This program is funded by a grant from Coloplast Corp.
Ostomy Skills Kit
For all of your surgical patient education needs, visit www.SurgicalPatientEducation.facs.org
Patient Education - Ostomomy Skill Kit ad - BULLETIN - FINAL (25 p deep) _REV 03-11.indd 1 3/9/2011 8:55:19 AMVOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
58

The CD-ROM provides the learner with basic education and train-ing in ultrasound imaging as a foundation for specific clinical applications.
The National Ultrasound Faculty of the American College of Surgeons has developed “Ultrasound for Surgeons: The Basic Course, 2nd Edition” on CD-ROM for surgeons, surgical residents, and anyone interested in ultrasound imaging.
The 2nd Edition includes:
♦ Updated graphics using 3-D medical modeling devel-oped by NASA researchers to teach ultrasound and rapidly demonstrate key ultrasound skills
♦ Targeted clinical applications are highlighted, including Head and Neck, Breast, Vascular, Abdominal, Thoracic, Critical Care/Trauma, Foreign Objects, and Fractures
♦ Cue Cards to view and print to prompt learners onthree commonly performed scans
♦ Easier navigation and support of the CD-ROM
♦ Four CME credits available
To purchase the NEW edition, go to www.acs-resource.orgor call 888-711-1138.
A M E R i C AN CO llEg E O F SU R g EO N S ♦ D i V i S i O N O F E D U C AT i O N
U l t r a s o U n df o r s U r g e o n s :T H E B A S i C C O U R S E , 2 n d E D i T i O N
Thomas R. Russell, MD, FACS Executive Director, American College of Surgeons
Ajit K. Sachdeva, MD, FACS, FRCSC Director, Division of Education
Kathleen A. Johnson, EdM Senior Manager, Accredited Education Institutes and Skills Courses
Olivier Petinaux, MS Senior Manager, Distance Education and E-Learning
Sangkhom Ratsavong Administrator, Distance Education and E-Learning
Margaret Goslin Administrative Assistant
The ACS acknowledges the National Aeronautics and Space Administration (NASA), the U.S. Olympic Committee and the National Space Biomedical Research Institute for contributing images. AmericAn college of SurgeonS ♦ DiviSion of eDucAtion
U l t r a s o U n d f o r s U r g e o n s :t h e B A S i c co u r S e , 2 nd e D i t i o n
E-L e a r n i n g p r o d u c t s :E F F E C T I V E ♦ E F F I C I E N T ♦ E X C E P T I O N A L
N E W
UltrasoundAd 2009 BULLETIN.indd 1 9/22/2009 2:33:53 PM

State Legislatures’ website contains a wealth of information related to various aspects of state legislatures (http://www.ncsl.org/).
What surgeons can doFederal and state governments share similar
structures and responsibilities. While both Congress and state legislatures address vari-ous issues, they offer different venues to effect policy change and legislation. To be successful in advocating for a surgical agenda, it is important to understand the legislative dynamics in each setting and to find out which elected officials are in positions of leadership. Leadership in state legislatures are the major players in determining which bills are considered and receive attention. Building relationships with committee chairs
and party leaders is an integral step in fostering long-term effective advocacy efforts.
References
1. U.S. House of Representatives. Legislative re-sources. Available at: http://www.house.gov. Ac-cessed January 24, 2011.
2. U.S. Senate. What happens when a new Congress begins? Available at: http://www.senate.gov. Ac-cessed January 24, 2011.
3. National Conference of State Legislators. Legis-latures: Organization, procedure and facilities. Available at: http://www.ncsl.org/Default.aspx?TabID=746&tabs=1116,112,768#1116. Accessed January 24, 2011.
4. The White House. Our government: State and local government. Available at: http://www.whitehouse.gov/our-government/state-and-local-government. Accessed January 24, 2011.
ADVOCACY ADVISOR, FROM PAGE 45
American College of Surgeons Official Jewelry & Accessoriesdesigned, crafted and produced exclusively by Jim Henry, Inc.
The Tac/Lapel Pin #S1 Dbl. Gold-Filled $65 #S2 Solid 14K Gold $275
Cuff Links #S3 Dbl. Gold-Filled $175 #S4 Solid 14K Gold $1175
Key (shown actual size of 3/4 0) #S5 Dbl. Gold-Filled $100 #S6 Solid 14K Gold $575
Miniature Key (Not Shown) #S7 Dbl. Gold-Filled $75 #S8 Solid 14K Gold $350
Charm (Not Shown) #S9 Dbl. Gold-Filled $100 #S10 Solid 14K Gold $475
Miniature Charm #S11 Dbl. Gold-Filled $65 #S12 Solid 14K Gold $275 #S13 Sterling Silver w/ 180 Sterling Silver Neckchain $65
Ring #S14 Solid 14K Gold $1525 #S14.1 Solid 10K Gold $1100 (Indicate finger size)
Tie Bar #S15 Gold-Filled Emblem $60
Necktie #S16A Dark Blue $35 #S16B Light Blue $35 #S17 Maroon $35 Extra long add $5.00
Diploma Plaques #S18 Satin Gold Finish $375 #S19 Satin Silver Finish $375 8-1/20 x 120 metal plaque on 110x14-1/20 walnut. Specify name, day, month, year selected.
Women’s Bow Tie (Pretied) (Not Shown) #S20 Dark Blue $35 #S21 Maroon $35
Men’s Bow Tie (Untied) (Not Shown) #S22 Dark Blue $35 #S23 Maroon $35
Women’s Scarf - Silk (Not Shown) #S24 300x300 cream $35 w/ blue border
Rollerball Pen - Chrome #S25 Cross Townsend Medalist with 23/K Gold Plated Emblem $120
Money Clip (Not Shown) #S26 With Gold-Filled emblem $60
Desk Set (Not Shown) #S27 Solid Walnut with Cross Gold-Filled Pen & Pencil/Gold-Filled emblem; name and year elected a Fellow engraved on gold polished plate $275
Wallet (Not Shown) #S28 Black cowhide with Gold-Filled emblem $70
Blazer Buttons (Not Shown) #S29 Gold Electroplated (set of 9) $35
Blazer Patch #S30 Hand embroidered $35
Shipping/Handling/Insurance Domestic (48 contingent states) $12 Alaska, Hawaii, Puerto Rico $30 Foreign $40
Jim Henry, Inc. 435 Thirty-Seventh Avenue St. Charles, Illinois 60174 phone 630 584 6500 fax 630 584 3036 www.jimhenryinc.com e-mail: [email protected]
• Please use model # and item description when ordering• Include payment with order• VISA, American Express, & MasterCard accepted• Prices subject to major changes in gold prices• Send order directly to Jim Henry, Inc.• Illinois residents add 8% sales tax
#S15
#S14
#S16A
#S18 #S19
#S3 #S4
#S1 #S2
#S5 #S6
#S11 #S12 #S13
#S25#S16B
#S17
Designed expressly for the American College of Surgeons, these emblematic items are crafted to perfection in the Jim Henry tradition of excellence.
The American College of Surgeons receives a royalty for allowing Jim Henry, Inc. the use of the American College of Surgeons marks and other intellectual property.
Form No. 912009-08/10
Excellence in Awards and Recognition Since 1938
JIM HENRY, INC.
#S30
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
60

To report your chapter’s news, contact Rhonda Peebles toll-free at 888-857-7545 or via e-mail at [email protected].
Massachusetts member honored for advocacy efforts
The Arthur Ellenberger Award for Excellence in State Advocacy was presented to Peter Masiakos, MD, FACS, at the Massachusetts Chapter annual meeting on December 4, 2010. The award was presented to Dr. Masiakos by Andrew Warshaw, MD, FACS, American College of Surgeons (ACS) Treasurer (see photo, this page).
The award recognizes individuals who have demonstrated outstanding leadership skills, dis-tinguished service, and a commitment to protect-ing patient access to high-quality surgical care. Dr. Masiakos has demonstrated these qualities in his dedicated efforts to pass legislation in Massachu-setts that bans the use of all-terrain vehicles by children under the age of 14. For more informa-tion on this topic, refer to the article written by Dr. Masiakos in the February 2011 issue of the Bulletin (Bull Am Coll Surg. 2011;96[2]:31-35).
Chapter news
by Rhonda Peebles
Wisconsin Surgical Society–Wisconsin Chapter: At the 2010 chapter education program, governing council members and committee members. Left to right, first row: Karen Brasel, MD, FACS; Marilu Bintz, MD, FACS, Immediate Past-President. Second row: Eric Anderson, MD; Mark Abraham, MD; Benjamin Jarman, MD, FACS; Rodney Malinowski, MD, FACS, President; Charles Cheng, MD, FACS; Barbara Zarebczan, MD; Jennifer Roberts, MD; Shanu Kothari, MD, FACS, Secretary/Treasurer. Third row: Gary Seabrook, MD, FACS, Governor; Nicholas Kitowski, MD; Ron Wenger, MD, FACS; Michael Garren, MD, FACS; Tina Yen, MD, FACS. Fourth row: Ron Martin, MD, FACS; Len Go, MD, FACS; Brian Lewis, MD, FACS; Steve Shapiro, MD, FACS; Steve Kappes, MD, FACS.
Massachusetts Chapter: Left to right: Dr. Masiakos, his son Andreas, and Dr. Warshaw.
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
61

Wisconsin conducts annual meetingThe Wisconsin Surgical Society–A Chapter of
the ACS held its annual fall conference at The American Club in Kohler, WI, November 5–6, 2010. Margaret Knudson, MD, FACS, University of California–San Francisco, served as the William Beaumont guest lecturer; Dr. Knudson spoke of her recent experiences as a civilian trauma sur-gical advisor to the uniformed services trauma surgeons in the Middle East and Landstuhl, Ger-many. Also, Mark Malangoni, MD, FACS, a Regent of the College from Philadelphia, PA, presented an update on College activities and new initia-tives. The two-day conference serves as a forum for residents and medical students from the four Wisconsin surgical residency programs to present their clinical and laboratory research papers to an audience of community and academic surgeons. More than 135 member surgeons and residents attended the event (see photo, page 61).
Illinois hosts 60th annual meetingAt the 60th annual meeting of the Illinois
Chapter, Richard Anderson, MD, FACS, accepted the nomination as 46th president of the Chapter. He succeeds Keith Thomae, MD, FACS, who has served the downstate chapter since 2008. A total of 21 speakers were on hand to give lively didactic presentations. In addition, the Illinois Chapter recognized many past-presidents who attended the event.
Virginia continues humanitarian travel awards for residents
In 2009, the American College of Surgeons’ Vir-ginia Chapter (VA-ACS) established the VA-ACS Humanitarian Surgical Resident Travel Scholar-ship Program. This program was established to offset travel expenses for residents in Virginia who are interested in participating in programs to deliver surgical care as part of humanitarian mis-sions to underdeveloped countries. Each recipient receives $250 to offset travel expenses. For 2011, four recipients have been selected for the travel scholarships:
• DanielA.Barker,MD, from the University of Virginia, Charlottesville, will join the medical team traveling to the Mission of Hope in Bolivia,
an organization that runs a free medical clinic in Santa Cruz, Bolivia. The team consists of otolar-yngologists, anesthesiologists, and nurses from across the U.S. who volunteer their time and service to provide free surgical care for the needy patients in the clinic.
• MichaelDeMarcantonio,MD, from Eastern Virginia Medical School, Norfolk, will travel to Loma de Luz Hospital in Balfate, Honduras, and will staff ear, nose, and throat (ENT) clinics and be involved in the medical and surgical treatment of a variety of patients afflicted with ENT disorders.
• FrancellRichard,MD,* from Eastern Virginia Medical School, will travel to the Dominican Re-public with Medical Ministries International, which provides spiritual and physical health care to the world’s poorest nation by mobilizing volunteers on one-to-two week medical projects. The group will serve the local population, providing basic surgical care to include general surgery, urology, pediatric surgery, and basic head and neck surgery.
• MichaelC.Soult,MD,* from Eastern Virginia Medical School, will travel to Ecuador to provide general surgical services to the indigent popula-tions of the Ecuadorian Andes. While in Ecuador, the services that will be provided include a daily surgical clinic for consultation, and operative in-tervention with procedures ranging from hernia repairs, to general pediatrics, to hysterectomies, and all postoperative care.
For more information, contact Craig S. Derkay, MD, FACS, Chair, Humanitarian Surgical Resi-dent Travel Scholarship Committee, at [email protected], or Susan McConnell, VA-ACS Executive Director, at [email protected].
ACS Foundation calls chapters “champions” in philanthropy
Even before the Development Committee was active in the mid-1990s, the College’s chapters have made annual donations to support the work of the ACS. This tradition continues even in difficult times, when chapters are challenged to maintain their membership and avoid dues increases. The philanthropic spirit lives in many of the chapters, and this is most admirable. These donations are not only important in themselves, but also signal that the leadership and members of the chapters recognize the need to address important issues that
*Denotes Resident Membership in the College. continued on page 64
VOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
62

Date Chapter Location/information
May 05, 2011 - May 07, 2011
Illinois & Metropolitan Chicago (AP)
Location: Loyola Medical Center, Maywood, IL Contact: Beth Mahlo, 309-236-6122, e-mail: [email protected] ACSRepresentative(s):RichardJ.Finley,MD,FACS
May 05, 2011 - May 07, 2011
West Virginia (AP) Location: The Greenbrier, White Sulphur Springs, WV Contact: Sharon Bartholomew, 304-293-1258, e-mail: [email protected] ACS Representative(s): David B. Hoyt, MD, FACS and Charlotte Grill
May 06, 2011 - May 07, 2011
Ohio (AP) Location: Hyatt Regency Cincinnati, Cincinnati, OH Contact: Brad Feldman, MPA, CAE, IOM, 877-677-3227, e-mail: [email protected] ACSRepresentative(s):PatriciaJ.Numann,MD,FACS
May 13, 2011 - May 15, 2011
Virginia (AP) Location: Hilton Richmond Hotel & Spa, Richmond, VA Contact: Susan McConnell, 804-643-6631, e-mail: [email protected]
May 14, 2011 Northern California (AP)
Location: Marines Memorial Hotel, San Francisco, CA Contact: Annette Bronstein, 650-992-1387, e-mail: [email protected]
May 19, 2011 Vermont (AP) Location: Lake Mansfield Trout Club, Stowe, VT Contact:JeanneJackson,802-847-9440,e-mail:[email protected]
May 19, 2011 - May 20, 2011
Michigan Location: Amway Grand Plaza Hotel, Grand Rapids, MI Contact: Angie Kemppainen, 517-336-7586, e-mail: [email protected]
May 19, 2011 - May 21, 2011
Mexico, Federal District
Location: Acapulco, Mexico Contact: Rosa Aurora Ruiseco, e-mail: [email protected] ACS Representative(s): L.D. Britt, MD, MPH, FACS
May 23, 2011 Metropolitan Philadelphia (AP)
Location: Union League of Philadelphia Contact:JenniferKeeler,717-558-7850,e-mail:[email protected] ACS Representative(s): David B. Hoyt, MD, FACS
May 26, 2011 - May 27, 2011
JapanLocation:Tokyo,Japan Contact: Kyoichi Takaori, MD, FACS, 81-75-751-4323, e-mail: [email protected]
May 26, 2011 - May 28, 2011
Argentina Location: National Academy of Medicine Headquarters, Buenos Aires, Argentina Contact: Alberto Raul Ferreres, MD, FACS, 5411-4801-2820, e-mail: [email protected] ACS Representative(s): Carlos A. Pellegrini, MD, FACS
June08,2011 Brooklyn-Long Island Location: Garden City Hotel, Garden City, Ny Contact: Teresa Barzyz, 516-741-3887, e-mail: [email protected]
June17,2011- June20,2011
Washington & Oregon (AP)
Location: Lake Chelan, WA Contact: Susan Lentz, 425-953-4757, e-mail: [email protected] ACS Representative(s): David B. Hoyt, MD, FACS
July15,2011- July17,2011
North Carolina & South Carolina (AP)
Location: Grove Park Inn, Asheville, NC Contact: Brad Feldman, MPA, CAE, IOM, 877-859-4561, e-mail: [email protected] ACSRepresentative(s):LazarJ.Greenfield,MD,FACS
July29,2011- July31,2011
Tennessee (AP) Location: Memphis, TN Contact:WandaJohnson,931-967-4700,e-mail:[email protected] ACS Representative(s): David B. Hoyt, MD, FACS
Chapter meetingsFor a complete listing of the ACS chapter education programs and meetings, visit the ACS website at http://
www.facs.org/about/chapters/index.html.(AP) following the chapter name indicates that the ACS is providing AMA PRA Category 1 Credit™ for this
activity.
APRIL 2011 BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
63

cannot be accomplished without philanthropic sup-port. The ACS Foundation recognizes and thanks those chapters, as well as their leadership and members, who are champions for philanthropy.
In 2010, 16 chapters contributed a total of $26,500 to the Foundation. The ACS Foundation has a single beneficiary: The American College of Surgeons and, by extension, all those who benefit from its programs in optimal patient care, profes-sional education, and advocacy.
The chapters that contributed during 2010 include:
Donors Circle (gifts $1,000 or above): Arizona, Hawaii, Indiana, Japan, Kansas, Massachusetts, Michigan, Nebraska, North Carolina, Ohio, South Carolina, South Dakota, South Florida, Southwest-ern Pennsylvania, Tennessee, and the Wisconsin Surgical Society—A Chapter of the ACS.
The ACS Foundation thanks each and every
chapter and its officers and members for this great support.
Chapter anniversaries
Month Chapter Years
March Brazil 59 Southern California 59 Massachusetts 57 Nevada 46 New Hampshire 59 Puerto Rico 61 South Dakota 59April Metropolitan Chicago 56 Mississippi 58 Oklahoma 61
Ms. Peebles is in the Division of Member Services, Chicago, IL.
Publication: the breast JournalVol: 15 issue: 2half Page nonbleed
ad: naPbcclient: american college of surgeons
PROVIDE YOUR PATIENTS WITH LEADING-EDGE, HIGH-QUALITY BREAST CARE
Seek accreditation from the National Accreditation Program for Breast Centers (NAPBC).naPbc accreditation is the best way for your center to offer patients every significant advantage in their battle against breast disease.naPbc-accredited centers:
• demonstrate a commitment to high standards of clinical practice and quality improvement by utilizing nationally recognized, multidisciplinary quality performance measures.• Participate in data collection to monitor outcomes
and improve the quality of care at local, state, and national levels.• Promote patient and professional education for
the treatment of breast disease.Join the nationally recognized network of breast centers dedicated to providing quality breast health care with the full scope of resources and services to support the continuum of care.
NAPBCNATIONAL ACCREDITATION PROGRAM FOR BREAST CENTERS
To learn about the accreditation process, visit: www.accreditedbreastcenters.org
Make a coMMitMent to provide high quality breast care to your patients. APPLY fOR NAPBC ACCREDITATION TODAY!
NAPBC half page for Breast Journal.indd 1 5/21/2010 9:00:03 AMVOLUME 96, NUMBER 4, BULLETIN OF THE AMERICAN COLLEGE OF SURGEONS
64

















