Autonomics/Neurotransmitters 1 1 Autonomics/ Neurotransmitters G. Patrick Daubert, MD Sacramento, CA Some (most) material plundered from various mentors and other talented toxicologists, with permission 2 Autonomic Nervous System ACh CNS ACh NMJ ACh ACh ACh NE Muscarinic Nicotinic Hollow end-organs Courtesy Cynthia Aaron, MD 3 Sympathetic ganglion NE ACh CNS ACh ACh ACh Secreting hollow end- organs: Heart Lungs GI Sympathetic innervation to heart, lungs, etc ACh Striated muscle ACh Muscarinic Nicotininc Courtesy Cynthia Aaron, MD
Transcript
Autonomics/Neurotransmitters
1
1
Autonomics/ Neurotransmitters
G. Patrick Daubert, MD Sacramento, CA
Some (most) material plundered from various mentors and other talented toxicologists, with permission
2
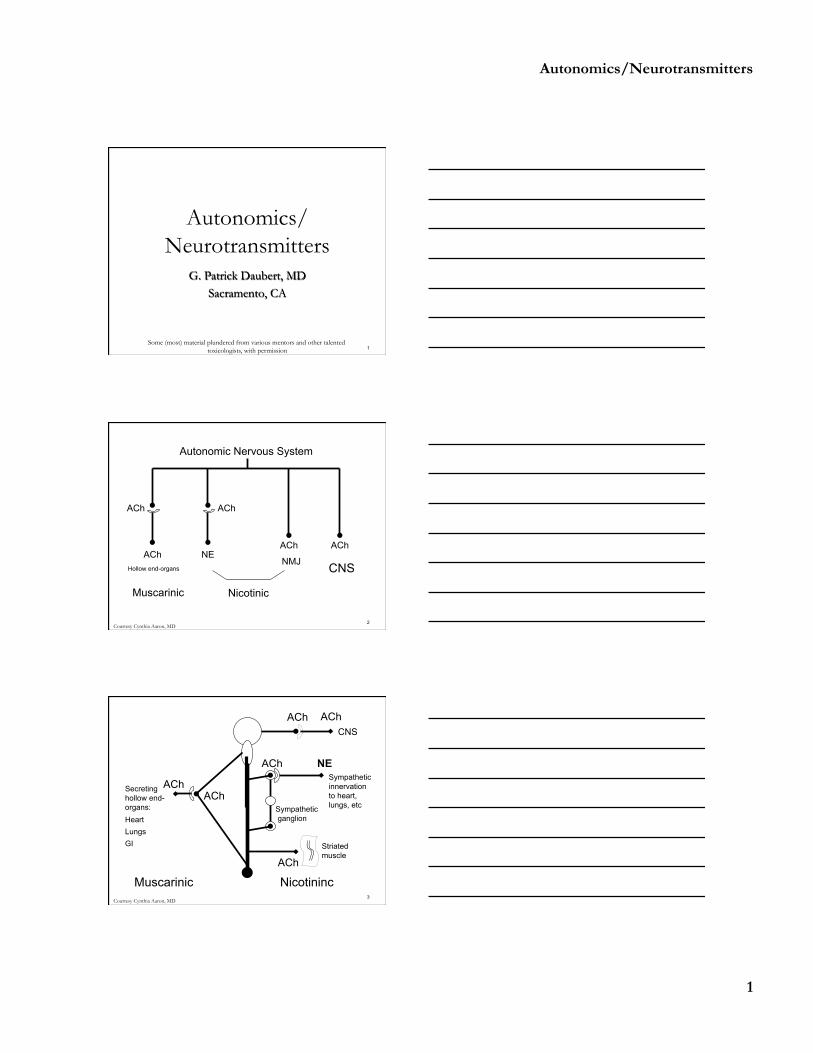
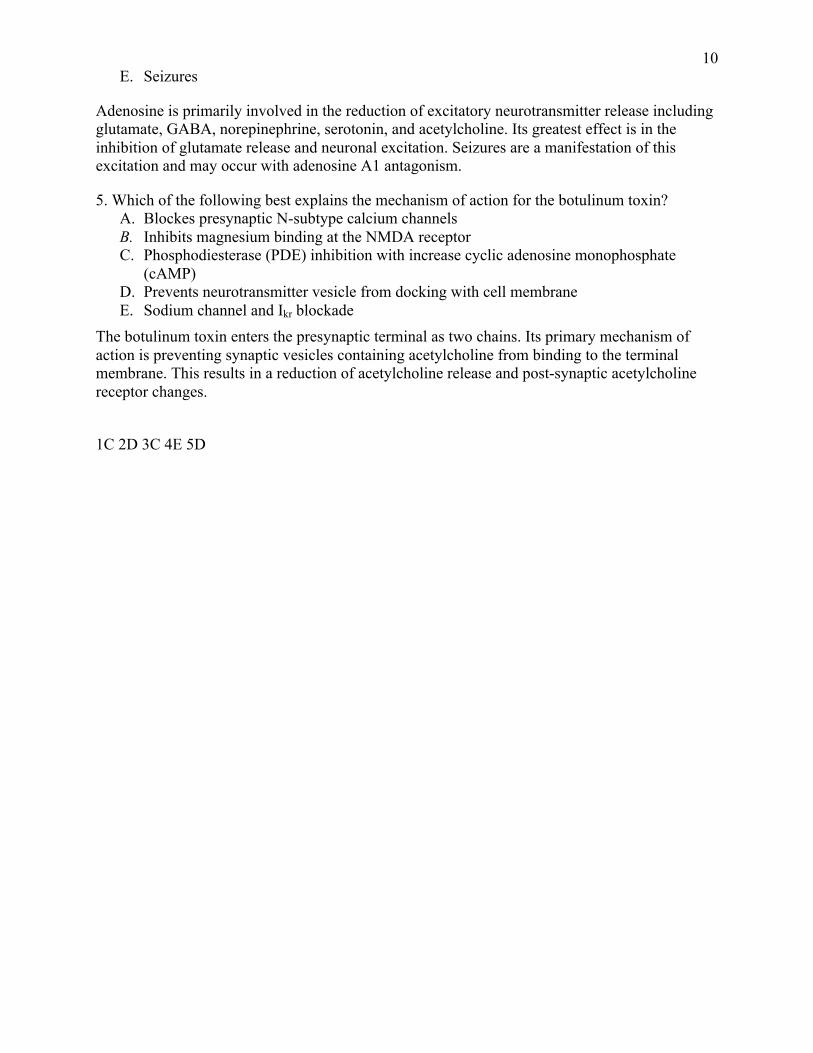
Autonomic Nervous System
ACh
CNS
ACh
NMJ
ACh ACh
ACh NE
Muscarinic Nicotinic
Hollow end-organs
Courtesy Cynthia Aaron, MD
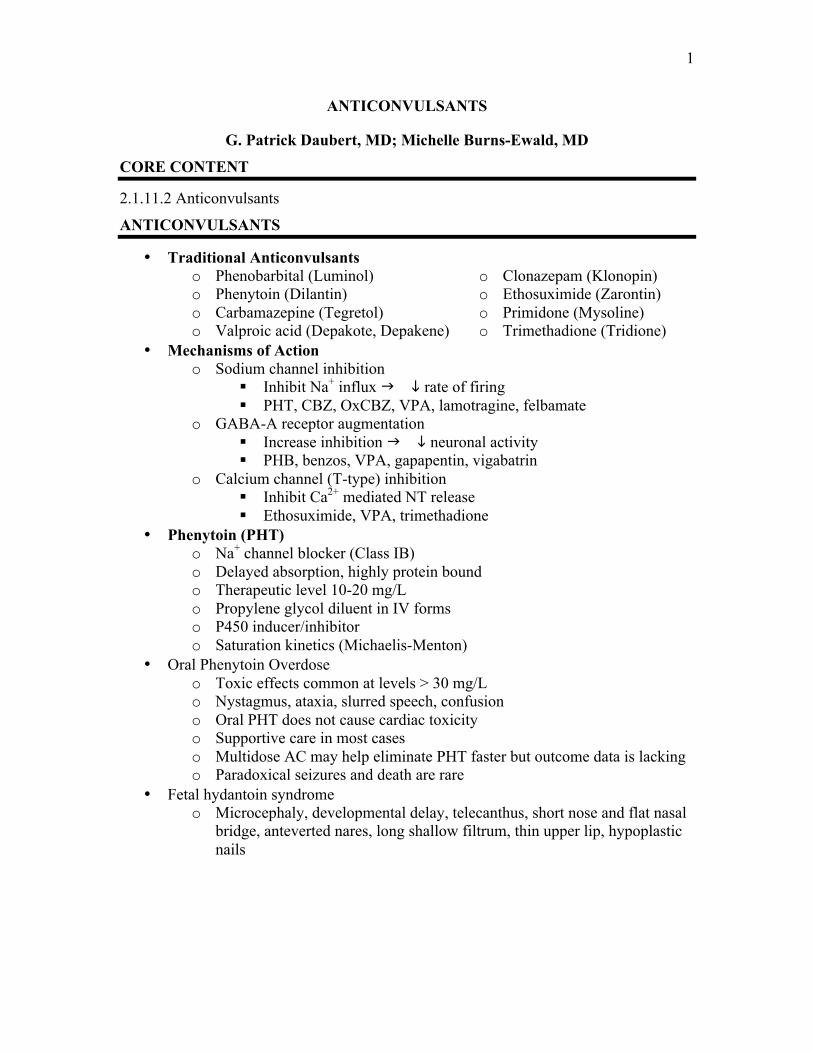
3
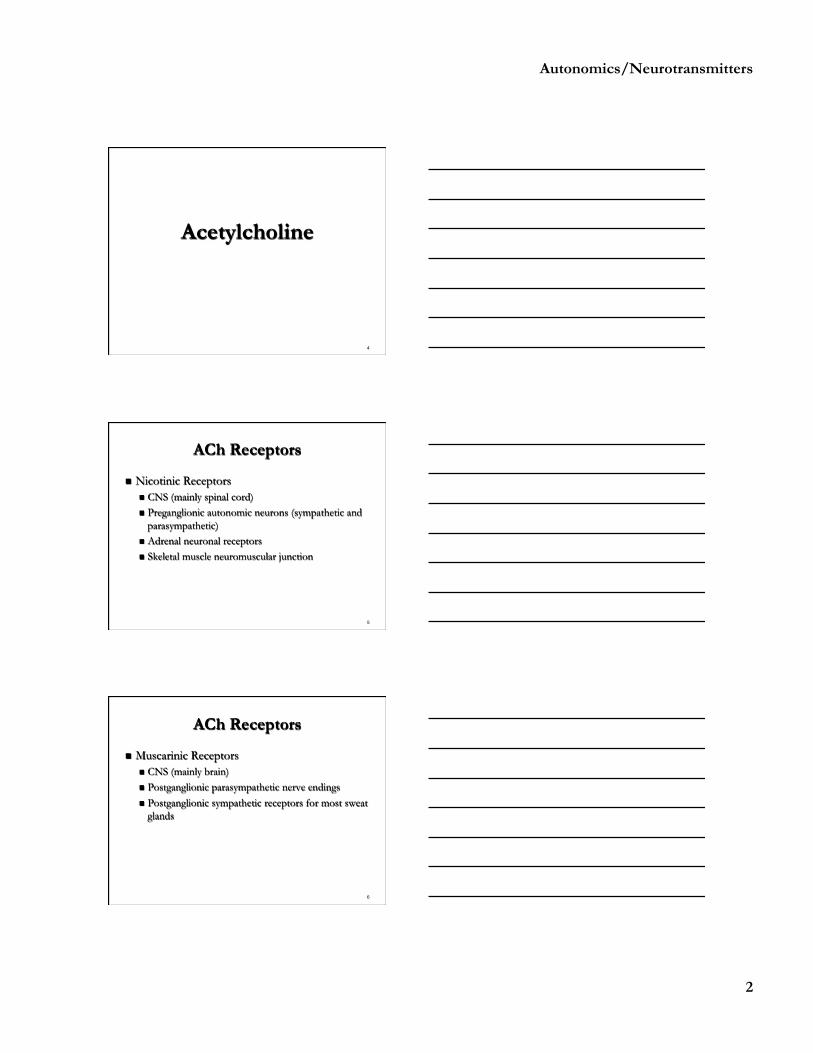
Sympathetic ganglion
NE ACh
CNS ACh
ACh
ACh
Secreting hollow end-organs: Heart Lungs GI
Sympathetic innervation to heart, lungs, etc
ACh
Striated muscle
ACh
Muscarinic Nicotininc Courtesy Cynthia Aaron, MD
Autonomics/Neurotransmitters
2
4
Acetylcholine
5
ACh Receptors
n Nicotinic Receptors n CNS (mainly spinal cord) n Preganglionic autonomic neurons (sympathetic and
parasympathetic) n Adrenal neuronal receptors n Skeletal muscle neuromuscular junction
6
ACh Receptors
n Muscarinic Receptors n CNS (mainly brain) n Postganglionic parasympathetic nerve endings n Postganglionic sympathetic receptors for most sweat
glands
Autonomics/Neurotransmitters
3
7
Agents that Induce ACh Release
n Aminopyridines n Latrodectus venom n Carbachol n Guanidine n Alpha2-adrenergic antagonists ( ACh release
from parasympathetic nerve endings)
8
Acetylcholinesterase Inhibitors
n [ACh] at both nicotinic and muscarinic receptors
n Produce a variety of CNS, sympathetic, parasympathetic, and NMJ effects n Carbamates n Organophosphorus compounds n Nerve agents n ‘Central’ AChE inhibitors (donepezil)
9
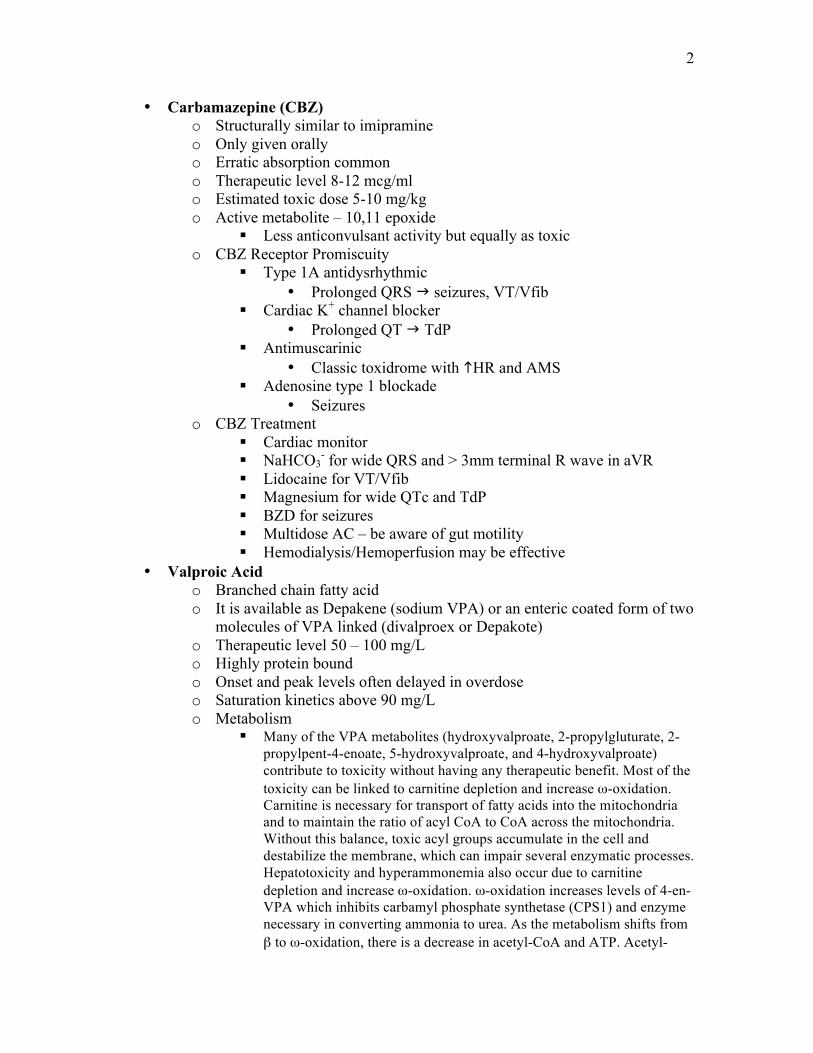
Autonomic Nervous System
ACh
CNS
ACh
NMJ
ACh ACh
ACh NE
Muscarinic Nicotinic
Hollow end-organs DUMBBELS
HTN, tachycardia, mydriasis
Fasciculations, respiratory paralysis
Seizures, coma
Courtesy Cynthia Aaron, MD
Autonomics/Neurotransmitters
4
10
Question
n Which one of the following agents inhibits acetylcholine release?
A. Bupropion B. Disulfiram C. Mirtazapine D. Tizanidine E. Yohimbine
11
Answer
n Which one of the following agents inhibits acetylcholine release?
A. Bupropion B. Disulfiram C. Mirtazapine D. Tizanidine E. Yohimbine
12
Agents that Block ACh Release
n Alpha2-adrenergic agonists n Botulinum toxin n Crotalinae venoms n Elapidae beta-neurotoxins n Hypermagnesemia
Autonomics/Neurotransmitters
5
13
Nicotinic Receptor Agonists
n Initial activation of receptors n Prolonged depolarization leads to inhibition
n Initial sympathomimetic, GI distress, fasciculations, seizures
n Then BP, HR, paralysis, coma
14
Nicotinic Receptor Agonists
n Nicotine alkaloids (nicotine, coniine) n Carbachol (mainly muscarinic effects) n Methacholine (minimal effects) n Succinylcholine (initial effects)
15
Nicotinic Receptor Antagonists
n NMJ blockers: weakness, paralysis n Curare, atracurium, alpha-bungarotoxin
n Peripheral neuronal blockers: autonomic ganglionic blockade n Trimethaphan (not entirely specific, may produce
NMJ blockade)
Autonomics/Neurotransmitters
6
16
Nicotinic Indirect Agonists
n Bind to distinct allosteric sites on the nicotinic receptor, not ACh binding site (enhanced channel opening) n Physostigmine n Tacrine n Galantamine
17
Nicotinic Indirect Antagonists
n Bind to distinct allosteric sites on the nicotinic receptor, not ACh binding site (decreased channel opening) n Chlorpromazine n Ketamine n Phencyclidine (PCP) n Local anesthetics n Ethanol n Corticosteroids
18
Buzzwords
n Nicotine alkaloids (nicotine, coniine) n Trick to remember the hemlocks –
n Water Gate Candidate Scandal (Water hemlock, GABA, Cicutoxin, Seizures)
n Poison Control Network (Poison hemlock, Coniine, Nicotine)
Autonomics/Neurotransmitters
7
19
Muscarinic Agonists
n Peripheral: DUMBBELS n Central: Sedation, dystonia, coma, seizures
n Muscarine n Bethanachol n Pilocarpine
20
Question
n A 35-year-old man presents to hospital with vomiting, diarrhea, profuse sweating, and mild bradycardia. What is the most likely mushroom he ingested
A. Amanita phalloides B. Clitocybe dealbata C. Cortinarius orellanus D. Gyromitra esculenta E. Tricholoma equestre
21
Question
n A 35-year-old man presents to hospital with vomiting, diarrhea, profuse sweating, and mild bradycardia. What is the most likely mushroom he ingested
A. Amanita phalloides B. Clitocybe dealbata C. Cortinarius orellanus D. Gyromitra esculenta E. Tricholoma equestre
Autonomics/Neurotransmitters
8
22
Muscarinic Antagonists
n Peripheral: mydriasis, anhidrosis, tachycardia, urinary retention, ileus, dry and flushed skin
n Central: delirium, agitation, hallucinations, coma n Atropine n Benztropine n Scopolamine n Phenothiazines n Cyclic antidepressants
23
Histamine
24
H1 Receptor Antagonists
n 1st generation n Cross the BBB n Diphenhydramine
n 2nd generation n Classified as non-sedation n Selectively bind peripheral
H1 receptors n Lower binding affinity for
cholinergic receptors n Reduced antimuscarinic
effects and CNS depression
Autonomics/Neurotransmitters
9
25
H1 Receptor Antagonists
Terfenadine terfenadine carboxylate
Astemizole desmethylastemizole
n Parent compounds block Ikr n Increased risk of TdP n Withdrawn from market in 1998
CYP3A4
CYP3A4
26
H1 Receptor Antagonists
n Clinical manifestations n CNS depression n Antimuscarinic effects n Cardiac
n Na and Ikr blockade with diphenhydramine (QRS and QT prolongation)
27
H2 Receptor Antagonists
n Hydrophilic – poor access to CNS n Alter gastric pH
n May impact absorption of acid-labile drugs n e.g., ketoconazole
Autonomics/Neurotransmitters
10
28
Cimetidine
n Only H2 receptor antagonist to inhibit P450 isozymes (specifically CPY3A4) n Useful in dapsone-induced methemoglobinemia n Useful in toxicity from Gyromitra esculenta
n Associated with myelosuppression if taken with drugs associated with BM suppression
n Rapid IV dosing has resulted in bradycardia, hypotension, and cardiac arrest
29
Serotonin
30
Serotonin
n Indole alkylamine n Synthesis from tryptophan n Central neurotransmitter n Precursor for melatonin n Serotonergic neurons lie in or near midline
nuclei in brainstem and project to various parts of cerebrum
n 7 classes of receptors with at least 15 subtypes
Autonomics/Neurotransmitters
11
31
Serotonin Synthesis & Metabolism
Tryptophan
5-OH-Tryptophan
Serotonin
5HIAA
tryptophan hydroxylase (rate limiting)
l-aromatic acid decarboxylase
MAO, aldehyde dehydroxylase
5HIAA: 5-OH-indoleacetic acid
32
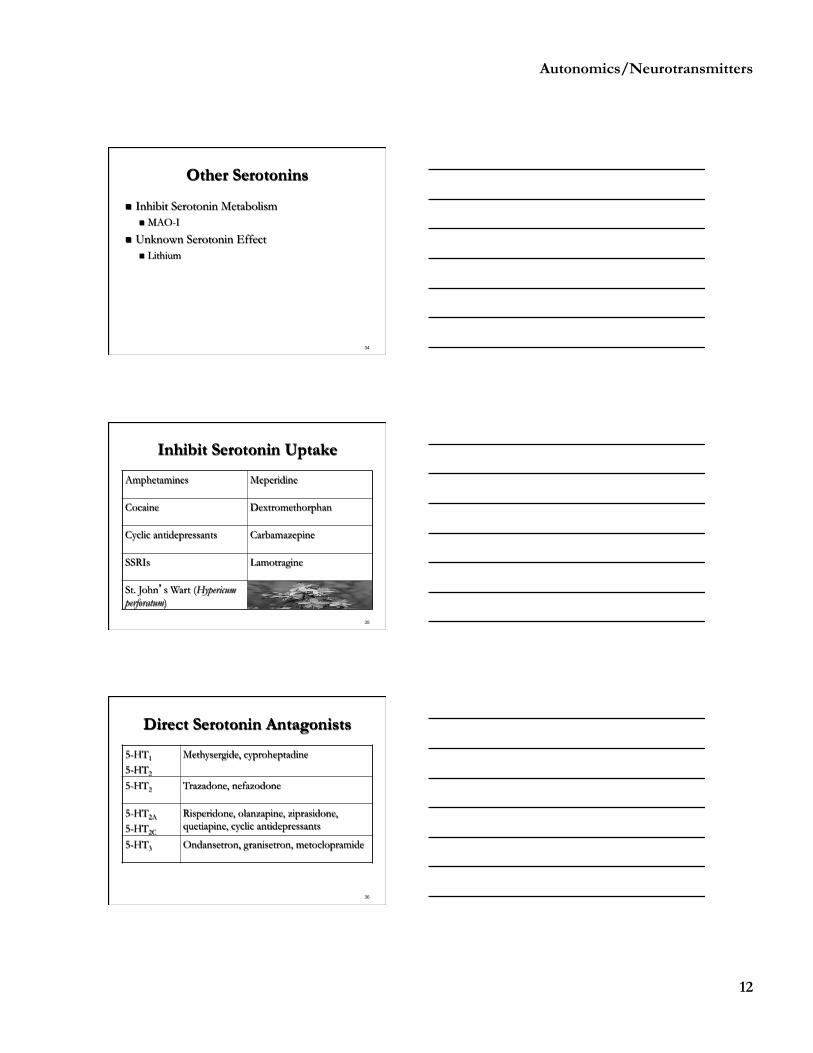
Serotonin Agonists
n Enhanced synthesis n L-tryptophan (associated with eosinophilia myalgia
syndrome) n 5-OH-tryptophan
33
Increased Serotonin Release
n Amphetamines (MDMA) n Cocaine n Codeine derivatives n Dexfenfluramine n Fenfluramine n L-Dopa
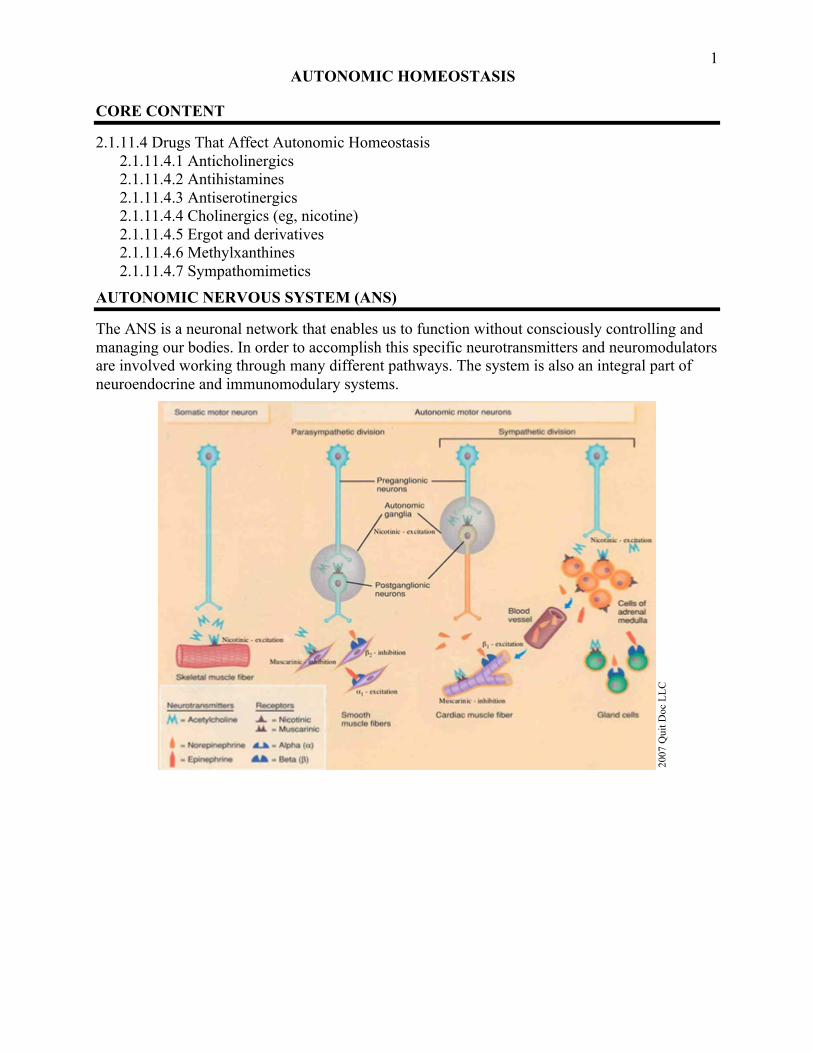
The ANS is a neuronal network that enables us to function without consciously controlling and managing our bodies. In order to accomplish this specific neurotransmitters and neuromodulators are involved working through many different pathways. The system is also an integral part of neuroendocrine and immunomodulary systems.
2007
Qui
t Doc
LLC
2
ACETYLCHOLINE
Acetylcholine (ACh) was the first neurotransmitter (NT) discovered and is the major NT in the peripheral nervous system (PNS)
• Acetylcholine o Produced from acetyl-CoA (glucose metabolism) and choline o Acetyl-CoA and choline are independently synthesized in the neuronal cell body
and transported along the axon to the synapse for conjugation into ACh o Release is mediated via Ca influx and presynaptic vesicles interacting with cell
membrane docking complex (process disrupted by botulinum toxin) o In order to allow repolarization, ACh must be removed rapidly (ie, AChE) o Two classes of ACh receptors
Nicotinic Muscarinic
Nicotinic Receptors (nAChRs) o CNS (mainly spinal cord) o Preganglionic autonomic neurons (sympathetic and parasympathetic) o Adrenal neuronal receptors o Skeletal muscle neuromuscular junction
• Nicotinic Receptor Agonists o Initial activation of nicotinic receptors
Prolonged depolarization leads to inhibition Initial sympathomimetic, GI distress, fasciculations, seizures Then i BP, i HR, paralysis, coma
o Nicotine alkaloids (nicotine, coniine) Trick to remember the hemlocks –
• Water Gate Candidate Scandal (Water hemlock, GABA, Cicutoxin, Seizures)
• Poison Control Network (Poison hemlock, Coniine, Nicotine) o Carbachol (mainly muscarinic effects, primarily in ophthalmic use) o Methacholine (minimal effects, does not cross BBB, methacholine test in asthma) o Succinylcholine (initial effects)
Trimethaphan (not entirely specific, may produce NMJ blockade) • Nicotinic Indirect Agonists
o Bind to distinct allosteric sites on the nicotinic receptor, not ACh binding site (enhanced channel opening)
Physostigmine Tacrine Galantamine
3 • Nicotinic Indirect Antagonists
o Bind to distinct allosteric sites on the nicotinic receptor, not ACh binding site (decreased channel opening)
Chlorpromazine Ketamine Phencyclidine (PCP)
Local anesthetics Ethanol Corticosteroids
• Muscarinic Receptors o CNS (mainly brain) o Postganglionic parasympathetic nerve endings o Postganglionic sympathetic receptors for most sweat glands
• Muscarinic Agonists o Peripheral: DUMBBELS o Central: Sedation, dystonia, coma, seizures o Muscarine o Bethanachol o Pilocarpine
• Muscarinic Antagonists o Peripheral: mydriasis, anhidrosis, tachycardia, urinary retention, ileus, dry and
flushed skin o Central: delirium, agitation, hallucinations, coma
Atropine Benztropine Scopolamine
Phenothiazines Cyclic antidepressants
• Agents that Induce ACh Release o Aminopyridines o Latrodectus venom (acts as a transmembrane pore and allows Ca influx into cells) o Carbachol o Guanidine o Alpha2-adrenergic antagonists (h ACh release from parasympathetic nerve
endings) • Acetylcholinesterase Inhibitors
o h [ACh] at both nicotinic and muscarinic receptors o Produce a variety of CNS, sympathetic, parasympathetic, and NMJ effects
(DUMBBELS) o Carbamates o Organophosphorus compounds o Nerve agents o ‘Central’ AChE inhibitors (donepezil)
• Agents that Block ACh Release o Alpha2-adrenergic agonists o Botulinum toxin (prevents NT vesicle from docking with cell membrane) o Crotalinae venoms o Elapidae beta-neurotoxins o Hypermagnesemia (blocks presynaptic N-subtype calcium channels)
4
HISTAMINE
Histamine interacts with four types of receptors H1-4. H1 receptors use G-protein second messenger systems. H1 receptors are diverse and have the most clinical toxicity in overdose. They are located in the CNS, heart and vasculature, airways, sensory nerves, Gastrointestinal smooth muscles cells, immune cells, and adrenal medulla. H2 receptors are located mainly in the gastric mucosa, but also exist in the heart, lungs, CNS, uterus, and immune cells. H3 receptors serve as neuromodulators for the release of other NT, including histamine. H4 receptors are involved in hematopoietic functions and eosinophil chemotaxis.
• Antihistamines o 1st generation
Cross the BBB Diphenhydramine most clinically relevant for boards
o 2nd generation Classified as non-sedating Selectively bind peripheral H1 receptors Lower binding affinity for cholinergic receptors Reduced antimuscarinic effects and CNS depression
• H1 Receptor Antagonists o Historical perspective
• Parent compounds block Ikr • Increased risk of TdP • Withdrawn from market in 1998
o Clinical manifestations Rapid onset with potential for long duration CNS depression Antimuscarinic effects Cardiac
• Sodium channel and Ikr blockade with diphenhydramine (QRS and QT prolongation)
o H2 Receptor Antagonists Hydrophilic – poor access to CNS Alter gastric pH May impact absorption of acid-labile drugs
• e.g., ketoconazole Cimetidine
• Only H2 receptor antagonists to inhibit P450 isozymes (specifically CPY3A4)
• Useful in dapsone-induced methemoglobinemia • Useful in toxicity from Gyromitra esculenta • Associated with myelosuppression if taken with drugs associated
with BM suppression • Rapid IV dosing has resulted in bradycardia, hypotension, and
cardiac arrest
5
ADENOSINE
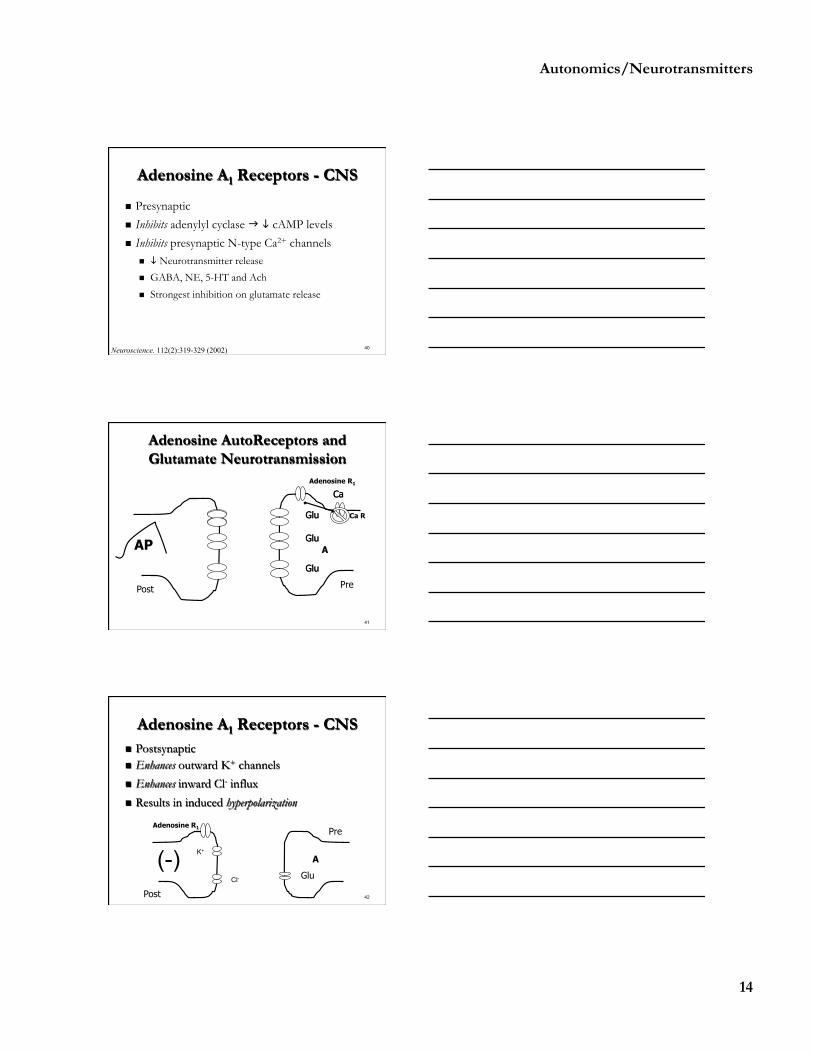
Adenosine is a neuromodulator primarily involved in the reduction of excitatory NT release including glutamate, GABA, norepinephrine, serotonin, and ACh. Its greatest effect is in the inhibition of glutamate release and neuronal excitation.
• Adenosine receptor antagonism o CNS: excitation due to sustained and unmodulated release of glutamate and other
excitatory neurotransmitters (A1 receptors) o Cardiac: tachycardia due to an increase rate of signaling in pacemaker cells (A1
receptors) o Vasculature: vasoconstriction of CNS, cardiac, and peripheral vascular (A2
receptors) • Adenosine A1 Receptors - CNS
o Postsynaptic o Enhances outward potassium channels o Enhances inward Chloride influx o Results in induced hyperpolarization
• Adenosine A2 Receptors - CNS o Presynaptic o Activates adenylyl cyclase increasing cAMP levels o Inhibits L-type & N-type calcium channels o Vasodilation o Only the A2A subtype of A2 receptors have significant activity
• Effects of A1 receptors predominate over A2A o A1 receptors are more numerous o Adenosine affinity for A1 > A2A receptors o Adenosine A2A Receptors o Adenosine A2A receptors are prominent in endothelial cells (vasodilation) o A2A receptor activity inhibits locomotor activity by inhibiting dopamine at D2
receptors o A2A receptors serve as check-balance for A1
• Adenosine A1 Antagonism o Cardiac
h HR h Atrial inotropicity h Response to epinephrine
o CNS h Excitatory amino acid (EAA) release
o Renal Diuresis
• Other methylxanthine effects o Increased catecholamine release o Phosphodiesterase (PDE) inhibition: results in increased levels of cyclic
adenosine monophosphate (cAMP) that serves to augment adrenergic effects o Increased intracellular calcium uptake and storage: clinical significance is
unknown
6
SEROTONIN
Serotonin is an indole alkylamine synthesized from tryptophan. Serotonergic neurons lie in or near midline nuclei in brainstem and project to various parts of cerebrum. There are 7 current serotonin receptor classes (5-HT1-7) with at least 15 subtypes. Serotonin has a wide variety of functions including vasoconstriction, inhibition of gastric secretion, enhanced platelet aggregation, stimulation of smooth muscle, and is naturally present in the central nervous system (CNS) as a neurotransmitter. Hallucinogenic drugs produce their electrophysiologic effects primarily through partial agonism at 5-HT2 receptors. Serotonin syndrome involves 5-HT1A and 5-HT2A receptors.
• Serotonin synthesis and metabolism
• Serotonin Agonists
o Enhanced synthesis L-tryptophan (associated with Eosinophilia Myalgia Syndrome – see
• Nicotine and similar alkaloids first stimulate then inactive nAChRs • Botulinum toxin prevents release of ACh • Alpha-latrotoxin (black widow) stimulates release of ACh and NE • Cimetidine CYP3A4 inhibitor
o Useful in dapsone-induced methemoglobinemia o Useful in toxicity from Gyromitra esculenta
• Terfendine and astemizole withdrawn for increased risk of TdP • Hallucinogenic drugs produce their effects primarity through 5-HT2 receptors • Serotonin syndrome primarily involves 5-HT1A and 5-HT2A receptors • Methysergide (serotonin antagonist) linked to retroperitoneal fibrosis • Fenfluramine and phentermine: weight loss drugs linked thickening of the leaflet and
chordae tendineae of aortic and mitral valves, withdrawn from U.S. market in 1997 • Nicotine alkaloids (nicotine, coniine)
o Trick to remember the hemlocks – Water Gate Candidate Scandal (Water hemlock, GABA, Cicutoxin,
Seizures) Poison Control Network (Poison hemlock, Coniine, Nicotine)
9
QUESTIONS
1. A 22-year-old woman with resistant depression discontinued her phenelzine (Nardil) last week and arrives to hospital after using crack cocaine with complaints of abdominal pain. The medical resident prescribes the patient meperidine. She becomes agitated, hyperthermic, rigid, and hyperreflexic with a profound startle response. What best explains her reaction?
A. Excessive GABA release from the meperidine B. Excessive glutamate stimulation in the cerebellum from cocaine C. Excessive serotonin release from the cocaine and meperidine D. Serotonin antagonism from the phenelzine E. Probable concomitant methamphetamine abuse
This patient’s symptoms are consistent with excessive serotonin or serotonin syndrome. The recent use of phenelzine along with the exposure to cocaine and administration of meperidine likely lead to significant amounts of serotonin in the CNS.
2. Which of the following statements is correct regarding neurotransmitters? A. Acetylcholine release is mediated via transmembrane pores unlike other
neurotransmitters that use synaptic vesicles B. Adenosine antagonism leads to reduction in glutamate transmission C. Hallucinogenic drugs produce their effects primarily through partial agonism at 5-HT4
receptors D. Nicotine first stimulates but then blocks nicotinic receptors both in the CNS and in
skeletal muscle E. Norepinephrine is the neurotransmitter of preganglionic sympathetic neurons
Nicotine first stimulates but then blocks nicotinic receptors both in the CNS and in skeletal muscle. Acetylcholine uses synaptic vesicles primarily for its release. Adenosine antagonism leads to an increase glutamate transmission. Hallucinogenic drugs primarily stimulate 5-HT2 receptors. Norepinephrine is a neurotransmitter of postganglionic sympathetic neurons.
3. Which of the following systems is involved with an organophosphate poisoning but not encountered in a diphenhydramine overdose?
A. Central nervous system B. Glands (salivary, sweat, lacrimal) C. Skeletal muscle D. Stomach and intestines E. Urinary (bladder)
All of the organ systems listed except skeletal muscles contain muscarinic receptors. The nicotinic receptors of skeletal muscles would no be effected with an exposure to a drug with antimuscarinic properties such as diphenhydramine.
4. The antagonism of adenosine A1 receptors is most likely to result in which of the following clinical manifestations?
A. Bradycardia B. Diaphoresis C. Hyperkalemia D. Hypotension
10 E. Seizures
Adenosine is primarily involved in the reduction of excitatory neurotransmitter release including glutamate, GABA, norepinephrine, serotonin, and acetylcholine. Its greatest effect is in the inhibition of glutamate release and neuronal excitation. Seizures are a manifestation of this excitation and may occur with adenosine A1 antagonism.
5. Which of the following best explains the mechanism of action for the botulinum toxin? A. Blockes presynaptic N-subtype calcium channels B. Inhibits magnesium binding at the NMDA receptor C. Phosphodiesterase (PDE) inhibition with increase cyclic adenosine monophosphate
(cAMP) D. Prevents neurotransmitter vesicle from docking with cell membrane E. Sodium channel and Ikr blockade
The botulinum toxin enters the presynaptic terminal as two chains. Its primary mechanism of action is preventing synaptic vesicles containing acetylcholine from binding to the terminal membrane. This results in a reduction of acetylcholine release and post-synaptic acetylcholine receptor changes.
1C 2D 3C 4E 5D
1
ANTICONVULSANTS
G. Patrick Daubert, MD; Michelle Burns-Ewald, MD
CORE CONTENT
2.1.11.2 Anticonvulsants
ANTICONVULSANTS
• Traditional Anticonvulsants o Phenobarbital (Luminol) o Phenytoin (Dilantin) o Carbamazepine (Tegretol) o Valproic acid (Depakote, Depakene)
o Clonazepam (Klonopin) o Ethosuximide (Zarontin) o Primidone (Mysoline) o Trimethadione (Tridione)
• Mechanisms of Action o Sodium channel inhibition
Inhibit Na+ influx g i rate of firing PHT, CBZ, OxCBZ, VPA, lamotragine, felbamate
o GABA-A receptor augmentation Increase inhibition g i neuronal activity PHB, benzos, VPA, gapapentin, vigabatrin
o Calcium channel (T-type) inhibition Inhibit Ca2+ mediated NT release Ethosuximide, VPA, trimethadione
• Phenytoin (PHT) o Na+ channel blocker (Class IB) o Delayed absorption, highly protein bound o Therapeutic level 10-20 mg/L o Propylene glycol diluent in IV forms o P450 inducer/inhibitor o Saturation kinetics (Michaelis-Menton)
• Oral Phenytoin Overdose o Toxic effects common at levels > 30 mg/L o Nystagmus, ataxia, slurred speech, confusion o Oral PHT does not cause cardiac toxicity o Supportive care in most cases o Multidose AC may help eliminate PHT faster but outcome data is lacking o Paradoxical seizures and death are rare
• Fetal hydantoin syndrome o Microcephaly, developmental delay, telecanthus, short nose and flat nasal
bridge, anteverted nares, long shallow filtrum, thin upper lip, hypoplastic nails
2
• Carbamazepine (CBZ) o Structurally similar to imipramine o Only given orally o Erratic absorption common o Therapeutic level 8-12 mcg/ml o Estimated toxic dose 5-10 mg/kg o Active metabolite – 10,11 epoxide
Less anticonvulsant activity but equally as toxic o CBZ Receptor Promiscuity
Type 1A antidysrhythmic • Prolonged QRS g seizures, VT/Vfib
Cardiac K+ channel blocker • Prolonged QT g TdP
Antimuscarinic • Classic toxidrome with hHR and AMS
Adenosine type 1 blockade • Seizures
o CBZ Treatment Cardiac monitor NaHCO3
- for wide QRS and > 3mm terminal R wave in aVR Lidocaine for VT/Vfib Magnesium for wide QTc and TdP BZD for seizures Multidose AC – be aware of gut motility Hemodialysis/Hemoperfusion may be effective
• Valproic Acid o Branched chain fatty acid o It is available as Depakene (sodium VPA) or an enteric coated form of two
molecules of VPA linked (divalproex or Depakote) o Therapeutic level 50 – 100 mg/L o Highly protein bound o Onset and peak levels often delayed in overdose o Saturation kinetics above 90 mg/L o Metabolism
Many of the VPA metabolites (hydroxyvalproate, 2-propylgluturate, 2-propylpent-4-enoate, 5-hydroxyvalproate, and 4-hydroxyvalproate) contribute to toxicity without having any therapeutic benefit. Most of the toxicity can be linked to carnitine depletion and increase ω-oxidation. Carnitine is necessary for transport of fatty acids into the mitochondria and to maintain the ratio of acyl CoA to CoA across the mitochondria. Without this balance, toxic acyl groups accumulate in the cell and destabilize the membrane, which can impair several enzymatic processes. Hepatotoxicity and hyperammonemia also occur due to carnitine depletion and increase ω-oxidation. ω-oxidation increases levels of 4-en-VPA which inhibits carbamyl phosphate synthetase (CPS1) and enzyme necessary in converting ammonia to urea. As the metabolism shifts from β to ω-oxidation, there is a decrease in acetyl-CoA and ATP. Acetyl-
3
CoA is needed to synthesize N-acetyl glutamic acid (NAGA). NAGA activates CPS1, which again is an enzyme necessary in converting ammonia to urea.
• Clinical Presentation o CNS depression/coma
Common with ingestions > 30 mg/kg Ataxia, nystagmus, slurred speech generally do not occur
o Other less common findings Hypernatremia, hypoglycemia, hypoglycemia, QT prolongation Pancreatitis Bone marrow suppression days 3-5 after ingestion
• VPA Hepatitis o Transient elevation of enzymes o Reversible elevation of ammonia o Frank hepatitis o Reye-like steatosis
• Treatment o Supportive care for CNS depression o Multi-dose charcoal o Hemodialysis for levels 800-1000 mg/L o L-carnitine o Probably not beneficial in CNS depression alone o Children < 2, multiple anticonvulsants, ketogenic diet, malnourished o Elevated ammonia, CNS depression, hepatitis deserve consideration
• Anticonvulsant Hypersensitivity Syndrome o Insufficient detoxification of epoxide hydrolase o Aromatic stuctures
o Diagnosis: lymphocyte killing assay with mouse microsomes • New Anticonvulsants
o Felbamate (Felbatol) o Fosphenytoin (Cerebyx) o Gabapentin (Neurontin) o Lamotragine (Lamictal) o Levetiracetam (Keppra)
o Oxcarbazepine (Trileptal) o Tiagabine (Gabitril) o Topiramate (Topamax) o Vigabatrin (Sabril) o Zonisamide (Zonegran)
4
• New Anticonvulsant Pearls o Felbamate (Felbatol)
Mild CNS depression Aplastic anemia
o Gabapentin (Neurontin) Decreased bioavailability in OD Not metabolized - no interactions
o Lamotragine (Lamictal) Coma, seizures, QRS prolongation Hypersensitivity Syndrome
o Oxcarbazepine (Trileptal) Inhibits CYP2C19 Hyponatremia (SIADH), seizures
o Tiagabine (Gabitril) Coma, seizures
o Topiramate (Topamax) Removed by hemodialysis Renal nephrolithiasis-calcium phosphate Acute angle closure glaucoma Hyperammonemia - carbonic anhydrase inhibition slows ammonia
urinary excretion o Vigabatrin (Sabril)
Agitation and psychosis o Zonisamide (Zonegran)
Carbonic anhydrase Inhibitor Nephrolithiasis
QUESTIONS
1. A 37-year-old male is transported to the emergency department via ambulance because of decreased mentation. His vital signs are normal and his physical exam is unremarkable except for a decreased level of consciousness and asterixis. His ammonia level is 145 ug/dL (normal < 20 ug/dL). His friend tells you that he is on a medication for seizures. Which anticonvulsant is he most likely taking?
A. Carbamazepine (Tegretol) B. Lamotrigine (Lamictal) D. Phenytoin (Dilantin) C. Phenobarbital (Luminal) E. Valproic acid (Depakote)
The patient’s presentation is consistent with valproic acid toxicity. The most distinctive feature is the elevated ammonia level. None of the other medications would produce this in acute toxicity.
2. What is the diluent found in intravenous phenytoin that is responsible for cardiotoxicity with rapid infusions and production of lactic acid with prolonged infusions?
5
A. Ethylene glycol B. Propylene glycol C. Polyethylene glycol D. Diethylene glycol E. Ethylene glycol monobutyl ether
The diluent in intravenous phenytoin is propylene glycol. Ethylene glycol would not be used as a pharmaceutical diluent. Diethylene glycol has been used as a diluent with disastrous results. Diethylene glycol poisoning causes severe renal failure and acidosis following exposure.
3. Which of the following anticonvulsant drugs is most likely to require cardiac monitoring in acute oral overdose?
A. Carbamazepine B. Gabapentin C. Levetiracetam D. Phenytoin E. Valproic acid
Carbamazepine is the most cardiac active of the medications listed with its cyclic antidepressant structure. Valproic acid can cause prolonged QT intervals but is not expected to be as problematic as carbamazepine. Gabapentin and levetiracetam are not known to cause cardiac toxicity. Oral exposures to phenytoin do not result in cardiac toxicity as apposed to rapid intravenous administration of phenytoin (due to propylene glycol).
4. A patient presents to you from an outside clinic where she was receiving follow-up for post-traumatic seizures. She was taking phenytoin (Dilantin) 300 mg TID but developed break-through seizures prompting the family physician to increase her dose to 400 mg TID. She is now ataxic, with slurred speech, notable incoordination, and horizontal nystagmus. Her phenytoin level is 48 mg/L. What is the likely cause of this patient’s phenytoin toxicity?
A. Auto-inhibition of phenytoin on P450 due to the increase in dose resulting in elevated levels B. Her symptoms are likely due to the diluent propylene glycol C. Poor outpatient compliance with her medication D. She has been consuming alcohol with her medication E. She is demonstrating Michaelis-Menton kinetics with the increase dose of phenytoin
Phenytoin demonstrates Michaelis-Menton kinetics at serum levels greater that approximately 20 mg/L. Serum levels will decrease at a much slower rate than levels in the therapeutic range. 1E 2B 3A 4E



















![AnOverviewoftheClinicalUseofAntimuscarinicsin ...2 Advances in Urology antimuscarinic action, oxybutynin in high doses exerts muscle-relaxant and local anaesthetic effects [5–8].](https://static.documents.pub/doc/80x56/60c45d5c03186b0ad2131222/anoverviewoftheclinicaluseofantimuscarinicsin-2-advances-in-urology-antimuscarinic.jpg)















