Defining Standards for Effective Multi-Disciplinary Team Meetings John RT Monson, MD, FRCS (Ire, Eng, Ed (Hon), Glas (Hon)), FASCRS, FACS Executive Director Colorectal Surgery, AdventHealth Central Florida Region Chair, Digestive Health and Surgery Institute Professor of Surgery, University of Central Florida, College of Medicine
Transcript
Defining Standards for Effective Multi-Disciplinary Team MeetingsJohn RT Monson, MD, FRCS (Ire, Eng, Ed (Hon), Glas (Hon)), FASCRS, FACSExecutive Director Colorectal Surgery, AdventHealth Central Florida RegionChair, Digestive Health and Surgery InstituteProfessor of Surgery, University of Central Florida, College of Medicine
Objectives
§ Context and Background
§ Rectal Cancer Programs?
§ The Multi-Disciplinary Approach
§ Specialization
§ Carrots, Sticks and Nudges
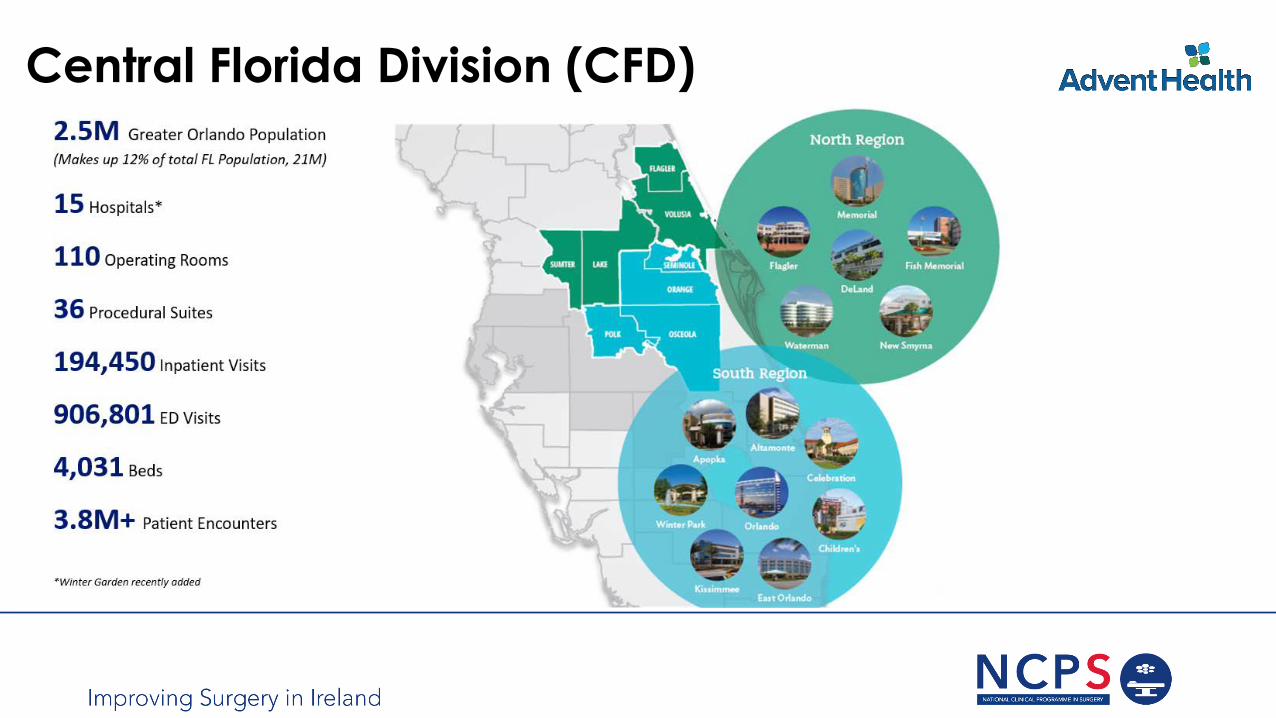
50Hospital campuses operated in nine states
80,000 Employees and physicians
10,500Staff physicians
5 million+Patients served annually
15Skilled nursing facilities
22Home health and hospice agencies
AdventHealth System
Central Florida Division (CFD)
North Region
South Region
Rectal Cancer - Are we doing well?
§Only 22% of proctectomy procedures performed by colorectal surgeons§ 40% of surgeons only perform non restorative procedures for
rectal cancer
Colorectal Procedures: What Proportion Is Performed by American Board of Colon and Rectal Surgery-Certified Surgeons? Etzioni DA, Cannom RR, Madoff RD, Ault GT, Beart RW Jr. Dis Colon Rectum. 2010 May;53(5):713-20Who Performs Proctectomy for Rectal Cancer in the United States? Ricciardi R, Roberts PL, Read TE, Baxter NN, Marcello PW, Schoetz DJ. Dis Colon Rectum. 2011 Oct;54(10):1210-5
Rectal Cancer - Are we doing well?
§ Restorative techniques used in only 50%
§ Some areas APER rates of 60%
Surgeon Influenced Variables in Resectional Rectal Cancer Surgery. Wexner SD, Rotholtz NA,. Dis Colon Rectum, 2000;43(11):1606-1627
Variability in Reconstructive Procedures Following Rectal Cancer Surgery in the United States. Ricciardi R, Roberts PL, Read TE, Marcello PW, Schoetz DJ, Baxter NN. Dis Colon Rectum. 2010 Jun;53(6):874-80
US Rectal Cancer Care
Low-volume hospitals
Inexperienced providers
High colostomy rates
Variation Still Exists – UK Data
What patients want!
The Modern World!
§Generalist vs. Specialist§ Generalism is in decline§ Generalists replaced by ever
increasing number of “ologists”
Generalism vs. SpecialismSecondary drivers also§Generalism has a low
status§More money in
specializing§Modern society has
come to venerate the specialist a proxy for “better”
Centralization in Other Cancers – The Evidence
§Pancreas § Significant association between hospital volume and postoperative mortality (odds ratio 0.32,
95 per cent confidence interval 0.16 to 0.64), and between hospital volume and survival (hazard ratio 0.79, 0.70 to 0.89).The effect of surgeon volume on postoperative mortality was not significant (odds ratio 0.46, 0.17 to 1.26).
Systematic Review and Meta-analysis of the Volume-Outcome Relationship in Pancreatic Surgery. Gooiker GA, van Gijn W, Wouters MW, Post PN, van de Velde CJ, Tollenaar RA. Br J Surg. 2011 Apr;98(4):485-94
Centralization in Cancer
§Esophagus – Same story!
The Effect of Provider Case Volume on Cancer Mortality: Systematic Review and Meta-Analysis. Gruen RL, Pitt V, Green S, Parkhill A, Campbell D, Jolley D. CA Cancer J Clin. 2009 May-Jun;59(3):192-211High-Volume Versus Low-volume for Esophageal Resections for Cancer: The Essential Role of Case Mix Adjustments Based on Clinical Data. Wouters MW, Wijnhoven BP, Karim-Kos HE, Blaauwgeers HG, Stassen LP, Steup WH, Tilanus HW, Tollenaar RA. Ann Surg Oncol. 2008 Jan;15(1):80-7
Overall Quality: Guideline Defined Care
§A 2006 RAND study showed that Americans receive only 55% of
recommended care.
§ 64.7% people with hypertension are well controlled
§ 53.5% people with asthma are well controlled
§ 39% for people with community-acquired pneumonia are well controlled
§Quality of care is an issue for all Americans
Specialization in Rectal Cancer
More complex now due to:§ Increasing obesity§Neo-adjuvant chemo-radiotherapy§ TME
§Not just a matter of the surgery§And it’s a Team approach
§ As noted by Freyer in 1912!!
The Damascene Experience – The TME
§ Bill Heald§APER 11%§ Local recurrence 3% in curative resections§ 80% disease free survival
Recurrence and Survival After Total Mesorectal Excision for Rectal Cancer. Heald RJ, Ryall RD Lancet. 1986 Jun 28;1(8496):1479-82Rectal Cancer: The Basingstoke Experience of Total Mesorectal Excision, 1978-1997. Heald RJ, Moran BJ, Ryall RD, Sexton R, MacFarlane JK. Arch Surg. 1998 Aug;133(8):894-9Colorectal Cancer Treatment, Clinical Evidence. Asad Qureshi, Anjali Verma, Paul Ross, David Landau., BMJ Publishing Group, August 2008. (Systematic review)The Impact of the Introduction of Total Mesorectal Excision on Local Recurrence Rate and Survival In Rectal Cancer: Long-term Results. Maurer CA, Renzulli P, Kull C, Käser SA, Mazzucchelli L, Ulrich A, Büchler MW. Ann Surg Oncol. 2011 Jul;18(7):1899-906
Pathology – The Missing Piece
§High quality TME is a surrogate for high quality surgery § Large reduction in local recurrence§ 20% increase in survival
Effect of the plane of surgery achieved on local recurrence in patients with operable rectal cancer: a prospective study using data from the MRC CR07 and NCIC-CTG CO16 randomized clinical trial MRC CR07/NCIC-CTG CO16 Trial Investigators; Quirke P, Steele R, Monson J, Grieve R, Khanna S, Couture J, O'Callaghan C, Myint AS, Bessell E, Thompson LC, Parmar M, Stephens RJ, Sebag-Montefiore D; NCRI Colorectal Cancer Study GroupTraining and Quality Assurance for Rectal Cancer: 20 Years of Data is Enough. Quirke, P. (2003). Lancet Oncol 4(11): 695-702
Specialization, volume and outcomes
Rectal Cancer Program
§Programs in Rectal Cancer are centers that utilizes a multitude of processes to improve outcomes for patients with rectal cancer
§ These include but are not limited to§ MDT- individualized care by way of collaboration and coordination § Standardized imaging techniques and interpretation § Proper and timely use of neo adjuvant and adjuvant chemo
radiotherapy§ Minimally invasive TME by a trained surgeon§ Standardized pathological interpretation OSTRiCh
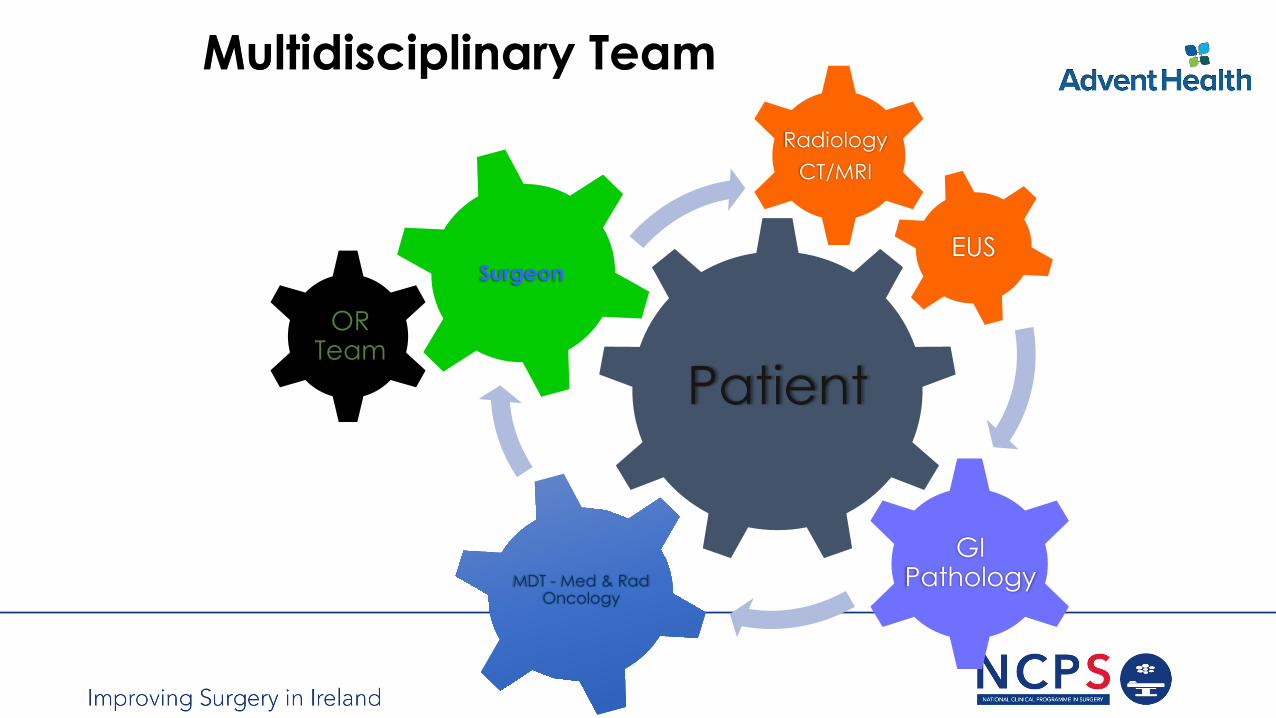
Multidisciplinary Team
OR Team
Patient
SurgeonEUS
RadiologyCT/MRI
MDT - Med & Rad Oncology
GI Pathology
Multidisciplinary Case Conference
Source: Lamb et al, Ann Surg Oncol 2011.
Telemedicine is effective with no detriment in quality
Clear and efficient structured review of cancer cases with key specialists present
Can change cancer management decisions in up to 50% of cases
MDT Management - Evidence
§ In management of patients with breast cancer multidisciplinary teams result in more evidence based recommendations and more timely treatment.
Multidisciplinary Breast Cancer Clinics. Do They Work? Gabel M, Hilton NE, Nathanson SD. Cancer. 1997 Jun 15;79(12):2380-4.The Impact of a Multidisciplinary Breast Cancer Center on Recommendations for Patient Management: The University of Pennsylvania Experience. Chang JH, Vines E, Bertsch H, Faker DL, Czerniecki BJ, Rosato EF, Lawton T, Conant EF, Orel SG, Schuchter L, Fox KR, Zieber N, Glick JH, Solin LJ. Cancer. 2001 Apr 1;91(7):1231-7.
MDT Management - Evidence
§Benefit of MDT has also been demonstrated to improve quality of care in other malignancies
Multidisciplinary Team Management is Associated with Improved Outcomes After Surgery for Esophageal Cancer. Stephens MR, Lewis WG, Brewster AE, Lord I, Blackshaw GR, Hodzovic I, Thomas GV, Roberts SA, Crosby TD, Gent C, Allison MC, Shute K. Dis Esophagus. 2006;19(3):164-71Effect of Process Standards on Survival of Patients with Head and Neck Cancer in the South and West of England. Birchall M, Bailey D, King P. Br J Cancer. 2004 Oct 18;91(8):1477-81
Systematic Review of Multidisciplinary Teams in the Management of Lung Cancer. Coory M, Gkolia P, Yang IA, Bowman RV, Fong KM. Lung Cancer. 2008 Apr;60(1):14-2
§ Implementation of a multidisciplinary approach has led to an improvement in both the processes and outcome for colorectal cancer patients.
The Impact of the Calman-Hine Report on the Processes and Outcomes of Care for Yorkshire’s Colorectal Cancer Patients. Morris E, Haward RA, Gilthorpe MS, Craigs C, Forman D. Br J Cancer. 2006 Oct 23;95(8):979-85
The Long-Term Survival of Rectal Cancer Patients Following Abdominoperineal and Anterior Resection: Results of a Population Based Observational Study. Haward RA, Morris E, Monson JRT, Johnston C, Foreman D. Eur J Surg Oncol 2005;31:22-8
MDT Management - Evidence
MDT Management § Practical and most decisions are implemented §Analysis of the implementation serves as an auditing tool to
measure its quality§ Timely delivery of treatment§ Better with collaboration amongst the specialists§ Recommendations are evidence based § Performance improves with time
An Evaluation of Treatment Decisions at a Colorectal Cancer Multi-Disciplinary Team. Wood JJ, Metcalfe C, Paes A, Sylvester P, Durdey P, Thomas MG, Blazeby JM. Colorectal Dis. 2008 Oct;10(8):769-72National Cancer Action Team, National Cancer Peer Review Programme 2004-2007. National Report: An Overview of the Findings from the Second National Round of Peer Review of Cancer Services in England. NCAT, 2008Colorectal MDTs: The Team’s Perspective. Sharma A, Sharp DM, Walker LG, Monson JR. Colorectal Dis. 2008 Jan;10(1):63-8
Specialization/TME
§ Implementation across Europe§Development of CoE’s§ Implementation of standardized radiology and pathology§ Referral guidelines for chemo radiotherapy§MDT coordination of care§Major investment in process implementation
How do we Develop Implementation?European Efforts…
Rectal Cancer StandardizationEuropean Experience- Why has it worked?
• Initiated by the clinicians, not imposed by health –care authorities• Constant feedback of the results to each clinician and
each instituion• Multidisciplinary approach to the project from the
onset• Process based and NOT personal
So Now We Know – How Do We Do It?
§ Rectal cancer management requires multi-disciplinary delivery of care.§ Ideally, in a rectal cancer program§ Can this be achieved anywhere?§ What is transferable?§ How can we achieve this?
The Principles
§ Inclusive and process based§ Anyone can join – just follow the process§ Natural selection will occur in most instances§ Don’t let Perfect get in the way of Better§ Must be clinician led with regular feedback§ Internally audited and externally validated§ It will take a decade!!
§ Most people genuinely want to do the right thing for the right reasons§ Misaligned incentives can be obvious or sub-conscious
The Practice
§ There are some resource implications – overall small!§ Essential:
§ MDT Co-Ordinator • Manages meeting and ensures case submission on time• Can function for other tumor types based on volume
§ Patient co-Ordinator• Ensures the recommended pathway happens• Herds the cats (doctors)• Identifies missing pieces and timelines
§ IT Infrastructure• Video conferencing (not telephone)
The Process…
Should it be Carrot or Stick –or Both??
What any policy seeks to address
Spiraling Health Care Costs
Accessibility to Health Care
Uneven Quality
Changes to Health Care Delivery System
Improve quality and uniformity of rectal cancer care in the U.S. - OSTRiCh
• Established in 2011• Members represent all facets of U.S. healthcare delivery system
• Private clinics, academic centers, community hospitals
• Diverse in size and geography
Carrots
Would it not be best if people simply did the right thing??
Nudge Theory§ Libertarian Paternalism
§ Default minimal tax deferred retirement savings plans with an opt out
§Choice Architecture§ Modify results by changing the way options are presented§ Putting healthy food in cafeteria at eye level and unhealthy food in
difficult to reach places§ Question about organ donor asked with driving license
Nudge Theory n Practice
Nudge – 80% reduction in misses!
Possible Real Carrots
§ Increased market share and income§ Potentially increased tariff from payers§ Better value of care §Opportunities for externally funded research §CPT code (and fee) for MDT conferences?§ Reputation increase – Accreditation Programs
BUT…
Do you want a piece of
me?
What possible sticks?
§Lower reimbursement of care outside program§Disincentives for not adhering to all the components of
The Process!§The payers are on the case§Bundled payments are coming!!
Conclusion §MDT should be the standard for the management of all cancers §We should work towards establishing more process based care
§ Evidence based, Inclusive, audited and validated
§Combination of carrots, sticks and nudges§ Incentives must be in line with the best interest of the patient§We should use process standards and program implementation in
order to implement change – its truly deliverable§ For the patient – it is definitely personal§ For the profession – its an obligation