Date of Release: July 1, 2010 Date of Expiration: June 30, 2011 This CME activity is jointly sponsored by Albert Einstein College of Medicine, Montefiore Medical Center, the West Virginia University School of Pharmacy Office of Continuing Education, and Asante Communications, LLC. This program is endorsed by the Society of Infectious Diseases Pharmacists (SIDP). Supported by an educational grant from Ortho-McNeil ™ , Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc., administered by Ortho-McNeil Janssen Scientific Affairs, LLC. 2010 - 2011
Transcript
Date of Release: July 1, 2010 Date of Expiration: June 30, 2011
This CME activity is jointly sponsored by Albert Einstein College of Medicine, Montefiore Medical Center, the West Virginia University School of Pharmacy Office of Continuing Education, and Asante Communications, LLC.
This program is endorsed by the Society of Infectious Diseases Pharmacists (SIDP). Supported by an educational grant from Ortho-McNeil™, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc., administered by Ortho-McNeil Janssen Scientific Affairs, LLC.
2010 - 2011
This CME activity is jointly sponsored by
Albert Einstein College of Medicine,
Montefiore Medical Center, the
West Virginia University School of Pharmacy
Office of Continuing Education, and
Asante Communications, LLC.
This program is endorsed by the Society of
Infectious Diseases Pharmacists (SIDP).
Supported by an educational grant from
Ortho-McNeil™, Division of Ortho-McNeil-
Janssen Pharmaceuticals, Inc., administered by
Ortho-McNeil Janssen Scientific Affairs, LLC.
SERIOUS INFECTIONS in the Critical Care Setting
Faculty and Reviewers ............................................... iv
Chapter 1: Epidemiology of Multidrug Resistance in Critical Care Settings .........................3
Ira Leviton, MD
Chapter 2: Meeting the Challenges of Multidrug-Resistant Pathogens ............7
Marin H. Kollef, MD
Chapter 3: Rational Dosing of Antibiotics in Critically Ill Patients ..............................23
Sandy J. Estrada, PharmD, BCPS
Chapter 4: A Practical Guide to Using Bundles in the ICU ...............................................33
Lisa G. Jones, RN, MS, CCRN
Table of Contents
Table of Contents
Chapter 5: Therapeutic Challenges in the ICU: 75-Year-Old Female With Acute Cholecystitis ..........................................37
Andrew F. Shorr, MD, MPH, FCCP
Chapter 6: Therapeutic Challenges in the ICU: 68-Year-Old Male With Recurrent Abdominal Pain .....................................45
Ira Leviton, MD
iv
SERIOUS INFECTIONS in the Critical Care Setting
Program Chair and Faculty
Marin H. Kollef, MD Virginia E. and Sam J. Golman Chair in Respiratory Intensive Care Medicine Professor of Medicine Division of Pulmonary and Critical Care Medicine Washington University School of Medicine Director, Medical Intensive Care Unit Director, Respiratory Care Services Barnes-Jewish Hospital St. Louis, Missouri
Faculty and Reviewers
Faculty
Sandy J. Estrada, PharmD, BCPSPharmacy Clinical Specialist Infectious Diseases Antimicrobial Stewardship Task Force, Co-Chair Lee Memorial Health System Fort Myers, Florida
Lisa G. Jones, RN, MS, CCRNGeneral Staff Nurse Medical Intensive Care UnitWestchester Medical Center Valhalla, New York
Andrew F. Shorr, MD, MPH, FCCPAssociate Director Pulmonary and Critical Care Medicine Department of Medicine Chief, Pulmonary Clinic Washington Hospital Center Washington, District of Columbia
CCME Reviewer and Faculty
Ira Leviton, MDAssociate Professor of Clinical Medicine Department of Medicine Infectious Diseases Albert Einstein College of Medicine of Yeshiva University Bronx, New York
CPE Reviewer
Virginia G. Scott, PhD, MS, RPhProfessor and Director of Continuing Education Department of Pharmaceutical Systems and Policy West Virginia University School of Pharmacy Morgantown, West Virginia
v
Download this and additional tools at
Activity GoalThe goal of this knowledge-based activity is to educate healthcare professionals on current strategies for the prevention and control of serious bacterial infections in the critical care setting, particularly with respect to potentially endemic multidrug-resistant (MDR) organisms.
Intended AudienceThis activity is intended for physicians, pharmacists, nurses, and other healthcare professionals involved in the prevention and control of serious bacterial infections in the critical care setting.There are no prerequisites for this educational activity.
Statement of NeedHospital-acquired infections (HAIs) impose a significant burden on patients, prescribers, and the healthcare system. Increasingly troublesome are MDR bacteria. Antibiotic prescribing is often inappropriate across treatment settings, particularly in critical care, where the risk of serious complications is elevated, comorbidities and presence of MDR pathogens often confound treatment, and the margin for error is exceedingly small. Drug resistance will continue to be a virtually inevitable consequence of antibiotic therapy absent rigorous source control programs and care pathways governing initial selection of an appropriately broad-spectrum antibiotic, pathogen-specific de-escalation, and timely cessation of treatment.
Learner’s GapHealthcare institutions should adapt evidence-based guidelines built on local microbiology. The proposed activity addresses strategies for individualizing infection surveillance protocols and management plans based on local microbiology. The activity will facilitate efforts to tailor prevention and control measures on a hospital-by-hospital basis. Elements of an effective antibiotic stewardship program, anchored by an infectious disease specialist and clinical pharmacist with infectious disease training, will also be addressed.
Learning ObjectivesAt the completion of this initiative, participants should be better prepared to: 1. Stratify patients with hospital-acquired infections for risk of multidrug-resistant,
Gram-negative and/or Gram-positive pathogens2. Select appropriate empiric antibiotic therapy based, in part, on comprehensive
patient assessment, infection type, and local susceptibility data3. Incorporate pharmacokinetic and pharmacodynamic data to optimize antibiotic
dosing strategies4. De-escalate broad-spectrum antibiotic therapy to pathogen-directed agents based
in part on culture information and patient status5. Implement evidence-based source control strategies and institutional best
practices to minimize the threat of multidrug-resistant organisms
Preamble Date of Release: July 1, 2010Date of Expiration: June 30, 2011
vi
SERIOUS INFECTIONS in the Critical Care Setting
Accreditation Statement and Credit DesignationThis activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint sponsorship of Albert Einstein College of Medicine, Montefiore Medical Center, the West Virginia University School of Pharmacy Office of Continuing Education (CE), and Asante Communications, LLC.
PhysiciansAlbert Einstein College of Medicine is accredited by the ACCME to provide continuing medical education (CME) for physicians. Albert Einstein College of Medicine designates this educational activity for a maximum of 1.0 AMA PRA Category 1 Credit™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
PharmacistsThe West Virginia University School of Pharmacy is accredited by the Accreditation Council of Pharmacy Education (ACPE) as a provider of continuing pharmacy education. This program (ACPE # 0072-9999-10-069-H01-P) is a knowledge-based program and approved for a total of 1.0 hours or 0.1 CEU of continuing pharmacy education (CPE) credit.
Method of ParticipationThere are no fees for participating in and receiving credit for this activity.
Participants should complete the self-report credit form, activity evaluation form, and receive at least 70% on the posttest. Participants receiving a grade less than 70% will be notified and permitted one retake of the exam. Completion of these forms is necessary to obtain credit for this activity. Your statement of credit will be issued immediately upon successful completion of the postttest and submission of the self-report credit and evaluation forms. The statement of credit specific to your discipline will appear on your screen and you will need to print a copy for your files. Duplicate statement of credit can be printed from CECity’s website at no additional cost.
Conflict of Interest StatementThe Conflict of Interest Disclosure Policy of Albert Einstein College of Medicine and West Virginia University School of Pharmacy Office of Continuing Education requires that faculty participating in any CME/CPE activity disclose to the audience any relationship(s) with a pharmaceutical, product, or device company. Presenters whose disclosed relationships prove to create a conflict of interest with regard to their contribution to the activity will not be permitted to present. Albert Einstein College of Medicine and West Virginia University School of Pharmacy Office of Continuing Education also require that faculty participating in any CME/CPE activity disclose to the audience when discussing any unlabeled or investigational use of any commercial product or device not yet approved for use in the United States.
Faculty and reviewers of this program have indicated the following disclosure information:
vii
Download this and additional tools at
Preamble
Sandy J. Estrada, PharmD, Has no conflict of interest(s) to report BCPS
Lisa G. Jones, RN, MS, CCRN Has no conflict of interest(s) to report
Albert Einstein College of Medicine and Montefiore Medical Center, Center for Continuing Medical Education (CCME) staff, the staff of West Virginia University School of Pharmacy Office of Continuing Education, and the staff of Asante Communications, LLC, have no conflicts of interest with commercial interests related directly or indirectly to this educational activity.
Alan Morrice, PhD, (Scientific Supervisor, Asante Communications, LLC) has no conflicts of interest with commercial interests related directly or indirectly to this educational activity.
Steven Jay Feld of Albert Einstein College of Medicine or a member of his household owns securities in Bioheart, Inc., Chelsea Therapeutics, Inc., and Pharmacopeia, Inc.
Online participation is also available via /cecompendium
ixFaculty Biographies
Sandy J. Estrada, PharmD, BCPSDr. Estrada received a Bachelor of Science in Pharmaceutical Sciences in 1999 and a Doctorate of Pharmacy in 2001 from the University of Toledo College of Pharmacy in Ohio. She completed her Critical Care and Infectious Disease residency from 2001 to 2002 and her fellowship in Infectious Diseases from 2002 to 2004, both at the University of Toledo.
Dr. Estrada is currently a Pharmacy Clinical Specialist in Infectious Diseases at Lee Memorial Health System in Fort Myers, Florida, where she provides consultations to an infectious diseases multidisciplinary team, participates in the antimicrobial steward-ship program, and is a preceptor to students and residents. She lectures frequently at regional and national meetings on MDR pathogens.
Lisa G. Jones, RN, MS, CCRNMs. Jones received a Bachelor of Science in Nursing from Pace University in Pleasantville, New York, and a Masters in Nursing Administration from Mercy College, Dobbs Ferry, New York. She is currently a general Staff Nurse in the Medical Intensive Care Unit (ICU) at Westchester Medical Center in Valhalla, New York.
Marin H. Kollef, MDDr. Kollef attended the US Military Academy at West Point for his undergraduate training and the University of Rochester for his MD degree. He completed his residency in Internal Medicine and his fellowship in Pulmonary and Critical Care Medicine at Madigan Army Medical Center in Tacoma, Washington. Dr. Kollef served as director of the medical ICU at Fitzsimons Army Medical Center
in Aurora, Colorado, from 1988 to 1992. During that time he also served as a general medical officer in support of the 1st Infantry Division during Operation Desert Storm. Dr. Kollef joined the faculty of Washington University and Barnes-Jewish hospital in 1992. He is currently Professor of Medicine at Washington University School of Medicine and Director of Medical Critical Care and Respiratory Care Services at Barnes-Jewish Hospital. Dr. Kollef was awarded the Virginia E. and Sam J. Golman Chair in Respiratory Intensive Care Medicine in 2009. He has received numerous teaching awards and is a recognized expert in the performance of clinical outcomes research in the ICU setting. His clinical research focuses on the understanding and prevention of nosocomial infections and the improved care of mechanically ventilated patients. Dr. Kollef has published extensively in the areas of ventilator-associated pneumonia prevention/treatment and the importance of antibiotic resistance in the ICU setting.
x
SERIOUS INFECTIONS in the Critical Care Setting
Ira Leviton, MDDr. Leviton received his MD degree from the Albert Einstein College of Medicine in 1984. He completed his internship and residency in Internal Medicine at Montefiore Hospital, followed by a fellowship in Infectious Diseases at both Einstein and Montefiore, during which he studied the mechanism of aminoglycoside trans-port across bacterial cell membranes. After completing his fellow-
ship, he joined the attending staff in the Division of Infectious Diseases at Montefiore and the faculty in the Department of Medicine at Einstein.He is currently Associate Professor of Clinical Medicine at the Albert Einstein College of Medicine and Adjunct Clinical Assistant Professor in the Department of Pharmacology at the Sophie Davis School for Biomedical Education of City College of New York. He lectures medical students on antibiotics at both of these schools during their pre-clinical courses in microbiology and infectious diseases. At Montefiore, he is Chairman of the Pharmacy and Therapeutics Committee as well as its Antibiotic Subcommittee, directs the Infectious Diseases Inpatient Consultation Service at its Einstein Hospital Division, and is a member of the Institutional Review Boards at both Montefiore and Biomedical Research Alliance of New York. He is also Director of the fellowship pro-gram for the Division of Infectious Diseases at Montefiore and Einstein. Since 2006 he has been a counselor for the Infectious Diseases Society of New York, and is president of the Society for 2010-2011.
Andrew F. Shorr, MD, MPH, FCCPDr. Shorr received his AB, magna cum laude, in Public and Inter-national Affairs from Princeton University in New Jersey in 1989. He received an MPH from the Johns Hopkins University, School of Hygiene and Public Health in Baltimore, Maryland, and an MD from the University of Virginia School of Medicine in Charlottes-ville. Thereafter, he completed his residency in Internal Medicine
and fellowship in Pulmonary and Critical Care Medicine, both at Walter Reed Army Medical Center in Washington.Dr. Shorr is currently Associate Director of Pulmonary and Critical Care Medicine and Chief of the Pulmonary Clinic at Washington Hospital Center. Additionally, he is Associ-ate Professor of Medicine, Clinician Scholar Track, at Georgetown University in Washing-ton, DC. Dr. Shorr is the recipient of numerous awards, including the 2009 Alfred Soffer Research Award of the American College of Chest Physicians and the 2007 Society of Critical Care Medicine Research Abstract Competition. He serves on the editorial board of Critical Care Research and Practice and of Critical Care Medicine, and is a reviewer for numerous other journals.
1
Download this and additional tools at
Hospital-acquired infections (HAIs) are a major cause of morbidity and mortality. According to most recent estimates, 1.7 million
HAIs occur yearly, resulting in 98,987 deaths.1 The highest infection rate (13 per 1000 patient-days) occurs in ICUs.1 These units are also major sources of MDR pathogens.2 ICUs are characterized by critically ill patients who may already be colonized by resistant organisms, are in close quarters, and require antibiotic therapy—a nearly optimal environment for resistance.2 With treatment options narrowing as MDR pathogens gain ascendancy and the pace of antimicrobial development slows, clinicians must develop innovative approaches to infection control. For example, the once traditional concept of empiric therapy with a narrow-spectrum agent, with subsequent antibiotic escalation, has been replaced with broad-spectrum initial therapy and rapid de-escalation based on culture results. Antibiotic selection and dosing can now be made rationally on the basis of combined pharmacokinetic (PK) and pharmacodynamic (PD) data. Hospitals are instituting comprehensive infection control (antibiotic stewardship) programs. The need to not only continue but even expand these efforts is critical in light of the morbidity/mortality associated with HAIs. Too, the pharmacoeconomic burden is considerable; estimated direct costs of HAIs range from $28.4 billion to $33.8 billion.3 Worse yet, Medicare decided that as of October 2008 several HAI-related costs will no longer be reimbursed.4
This compendium is designed to educate healthcare professionals on the scope of this public health challenge and to provide them with the resources to address the issue. Critical care specialists, infectious disease specialists, pharmacists, physician assistants, nurse practitioners, nurses, and other members of the multidisciplinary team who manage these patients are encouraged to utilize this resource compendium, a multimedia companion to which is available online. In chapter 1 of this compendium, Dr. Ira Leviton presents compelling evidence of the enormous scope of the
IntroductionMarin H. Kollef, MD
2
SERIOUS INFECTIONS in the Critical Care Setting
clinical challenge presented by MDR pathogens. No hospital has escaped the spread of these pathogens. In chapter 2, I review the identification of patients at risk for MDR-related infections, strategies for empiric therapy and de-escalation, effective use of antibiograms, and antibiotic stewardship programs. Not only do patterns of resistance change from hospital to hospital, they may even change from unit to unit within a particular hospital. Infection control programs must be developed with this reality in mind. In chapter 3, Dr. Sandy J. Estrada provides practical guidance on applying PK-PD data in an infection control program; effective use of these data can help blunt the continued rise of resistant pathogens through selection of the right dose and dosing interval. In chapter 4, registered nurse Lisa Jones discusses selection and implementation of care bundles in the ICU, stressing the critical role of the nurse in patient monitoring and in infection control measures. Finally, challenging cases of hospital-acquired pneumonia (HAP), ventilator-associated pneumonia (VAP), and intra-abdominal infection (IAI) are discussed by Drs. Andrew F. Shorr and Leviton in chapters 5 and 6, respectively.
References1. Klevens RM, Edwards JR, Richards CL Jr, et al. Estimating health care-associated
infections and deaths in U.S. hospitals, 2002. Public Health Rep. 2007;122:160-166.
2. Kollef MH. Bench-to-bedside review: antimicrobial utilization strategies aimed at preventing the emergence of bacterial resistance in the intensive care unit. Crit Care. 2005;9:459-464.
3. Scott RD II. The Direct Medical Costs Of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. Atlanta, GA: Centers for Disease Control and Prevention; 2009. Available at: http://www.cdc.gov/ncidod/dhqp/pdf/Scott_CostPaper.pdf. Accessed April 16, 2010.
4. Brown J, Doloresco IF, Mylotte JM. “Never events”: not every hospital-acquired infection is preventable. Clin Infect Dis. 2009;49:743-746.
3
Download this and additional tools at
Common MDR organisms are encapsulated by the acronym ESKAPE: Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumo-
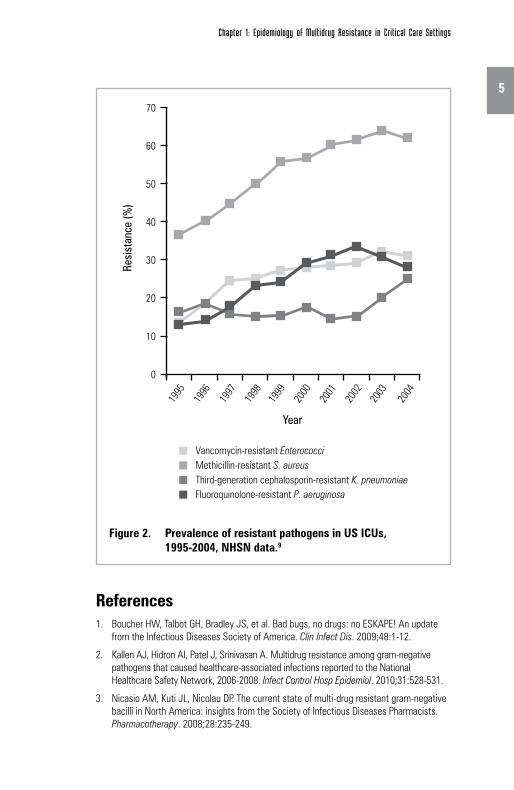
niae, Acinetobacter baumannii, Pseudomonas aeruginosa, Enterobacter spp.1 National Healthcare Safety Network (NHSN) susceptibility reports obtained between January 2006 and December 2008 showed that 15% of K. pneumoniae, 60% of A. baumannii, and 10% of P. aeruginosa isolates were resistant to 3 classes of antibiotics.2 While the prevalence of MDR pathogens was highest in the Northeast, the problem is nationwide.
Vancomycin-resistant enterococci (VRE) now represent the fourth leading cause of HAIs in this country and are found most commonly in the ICU. The Gram-negative members of this group are also a particular concern. As a group, these pathogens cause more cases of HAP and intra-abdominal, bloodstream, and skin infections.3 Studies have shown higher mortality with ICU infections associated with resistant Gram-negative organisms compared with susceptible organisms.4,5 In hospital settings, P. aeruginosa is one of the most common pathogens, and is implicated in a broad range of infections, particularly in lower respiratory tract infections, accounting for 20% of noso-comial pneumonia, according to recent NHSN data.6 In VAP, P. aeruginosa and S. aureus are important pathogens; in late-onset VAP, these pathogens are likely to be MDR.6 K. pneumoniae carbapenemase (KPC) enzymes are becoming increasingly troublesome because, like extended-spectrum b-lactamases (ESBLs), KPC enzymes hydrolyze extended-spectrum cepha-losporins, but unlike ESBLs, they also weakly hydrolyze carbapenems. A. baumannii has been associated with pneumonia, skin infections, urinary tract infections, peritonitis, meningitis, and bacteremia. Finally, Enterobacter spp, which are common causes of infection in the ICU, are intrinsically resistant to aminopenicillins and third-generation or expanded-spectrum cephalosporins via production of ESBL and AmpC b-lactamases.7,8 This has led to increased carbapenem usage, since their stability against ESBL and AmpC b-lactamases make them an effective option for MDR organisms.
Chapter 1: Epidemiology of Multidrug Resistance in Critical Care SettingsIra Leviton, MD
4
SERIOUS INFECTIONS in the Critical Care Setting
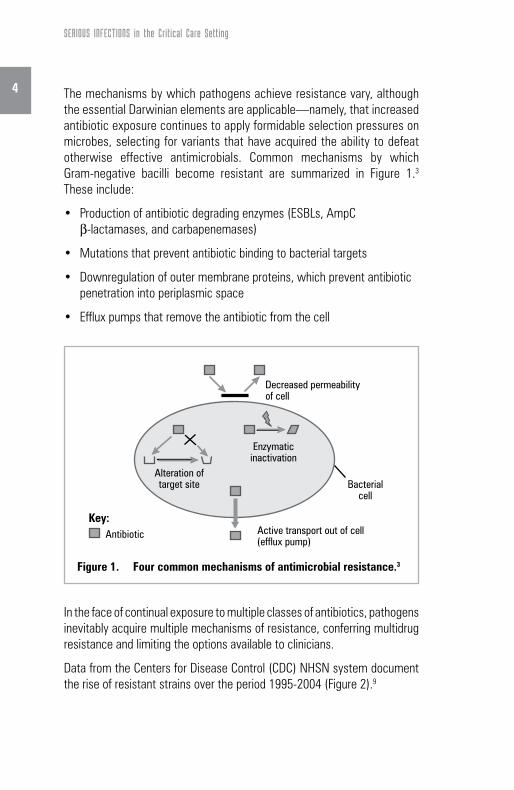
The mechanisms by which pathogens achieve resistance vary, although the essential Darwinian elements are applicable—namely, that increased antibiotic exposure continues to apply formidable selection pressures on microbes, selecting for variants that have acquired the ability to defeat otherwise effective antimicrobials. Common mechanisms by which Gram-negative bacilli become resistant are summarized in Figure 1.3 These include:
• Productionofantibioticdegradingenzymes(ESBLs,AmpCb-lactamases, and carbapenemases)
• Downregulationofoutermembraneproteins,whichpreventantibioticpenetration into periplasmic space
• Effluxpumpsthatremovetheantibioticfromthecell
In the face of continual exposure to multiple classes of antibiotics, pathogens inevitably acquire multiple mechanisms of resistance, conferring multidrug resistance and limiting the options available to clinicians.
Data from the Centers for Disease Control (CDC) NHSN system document the rise of resistant strains over the period 1995-2004 (Figure 2).9
Figure 1. Four common mechanisms of antimicrobial resistance.3
Decreased permeabilityof cell
Enzymaticinactivation
Bacterialcell
Alteration oftarget site
AntibioticKey:
Active transport out of cell(efflux pump)
5
Chapter 1: Epidemiology of Multidrug Resistance in Critical Care Settings
References1. Boucher HW, Talbot GH, Bradley JS, et al. Bad bugs, no drugs: no ESKAPE! An update
from the Infectious Diseases Society of America. Clin Infect Dis. 2009;48:1-12.
2. Kallen AJ, Hidron AI, Patel J, Srinivasan A. Multidrug resistance among gram-negative pathogens that caused healthcare-associated infections reported to the National Healthcare Safety Network, 2006-2008. Infect Control Hosp Epidemiol. 2010;31:528-531.
3. Nicasio AM, Kuti JL, Nicolau DP. The current state of multi-drug resistant gram-negative bacilli in North America: insights from the Society of Infectious Diseases Pharmacists. Pharmacotherapy. 2008;28:235-249.
Figure 2. Prevalence of resistant pathogens in US ICUs, 1995-2004, NHSN data.9
Third-generation cephalosporin-resistant K. pneumoniae Methicillin-resistant S. aureusVancomycin-resistant Enterococci
Fluoroquinolone-resistant P. aeruginosa
Year
0
10
20
30
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
Res
ista
nce
(%)
40
50
60
70
6
SERIOUS INFECTIONS in the Critical Care Setting
4. Shorr AF. Review of studies of the impact on gram-negative bacterial resistance on outcomes in the intensive care unit. Crit Care Med. 2009;37:1463-1469.
5. Rogers CA, Weston JS, Caeiro J-P, Garey KW, Chang K-T, Tam VH. Impact of multi-drug resistant Pseudomonas aeruginosa bloodstream infections on patient outcomes. Presented at the 49th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC); September 12-15, 2009; San Francisco, CA.
6. Burgess DS. Curbing resistance development: maximizing the utility of available agents. J Manag Care Pharm. 2009;15(suppl):S5-S9.
7. Livermore DM. Has the era of untreatable infections arrived? J Antimicrob Chemother. 2009;64(suppl 1):i29-i36.
8. Pournaras S, Iosifidis E, Roilides E. Advances in antibacterial therapy against emerging bacterial pathogens. Semin Hematol. 2009;46:198-211.
9. Centers for Disease Control. Antimicrobial-resistant organisms among ICU patients, 1995-2004. Available at: http://www.cdc.gov/ncidod/dhqp/ar.html. Accessed April 16, 2010.
7
Download this and additional tools at
Chapter 2: Meeting the Challenges of Multidrug-Resistant Pathogens Marin H. Kollef, MD
Identifying the at-risk patient
A number of issues need to be considered when evaluating patients at risk for an MDR bacterial infection (Table 1).1 First, sicker patients
are more likely to be treated with antibiotics. As they receive antibiotic therapy, particularly repeated courses of antibiotics or more prolonged courses of antibiotic therapy, we are more likely to see the emergence of resistant bacteria. This is particularly problematic in situations where patients have tubes or devices in place, such as central venous catheters or endotracheal tubes. These devices provide an environment for the development of biofilms, microscopic areas where antibiotics do not penetrate well and, consequently, where bacteria are exposed to only low levels of antibiotics.2 Second, the sicker a patient is, the more likely he/she will be infected with an MDR pathogen. Studies have demonstrated that
Table 1. Risk factors for MDR HAP, HCAP, and VAP infections1
Antimicrobial therapy in preceding 90 days
Current hospitalization of ≥5 days
High frequency of antibiotic resistance in the community or in the specific hospital unit
Presence of risk factors for HCAP:•Hospitalizationfor≥2 days in the preceding 90 days•Residenceinanursinghomeorextendedcarefacility•Homeinfusiontherapy(includingantibiotics)•Homewoundcare•FamilymemberwithMDRpathogen
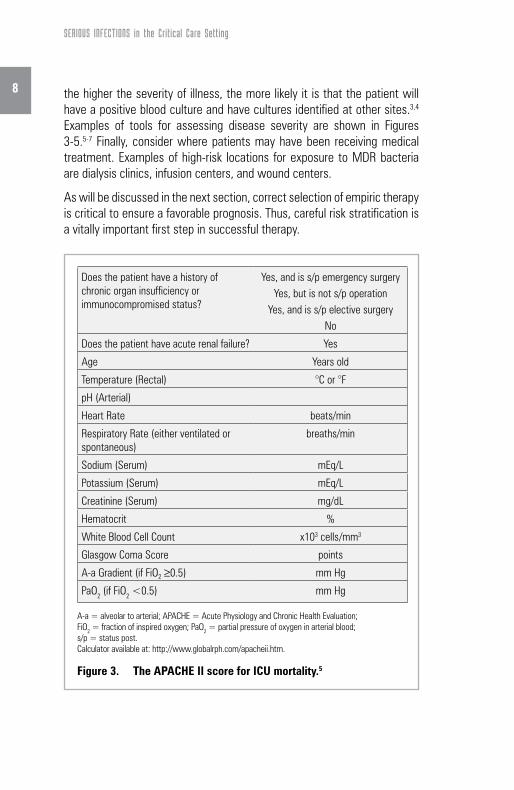
the higher the severity of illness, the more likely it is that the patient will have a positive blood culture and have cultures identified at other sites.3,4 Examples of tools for assessing disease severity are shown in Figures 3-5.5-7 Finally, consider where patients may have been receiving medical treatment. Examples of high-risk locations for exposure to MDR bacteria are dialysis clinics, infusion centers, and wound centers.
As will be discussed in the next section, correct selection of empiric therapy is critical to ensure a favorable prognosis. Thus, careful risk stratification is a vitally important first step in successful therapy.
Does the patient have a history of chronic organ insufficiency or immunocompromised status?
Yes, and is s/p emergency surgeryYes, but is not s/p operation
Yes, and is s/p elective surgeryNo
Does the patient have acute renal failure? Yes
Age Years old
Temperature (Rectal) °C or °F
pH (Arterial)
Heart Rate beats/min
Respiratory Rate (either ventilated or spontaneous)
breaths/min
Sodium (Serum) mEq/L
Potassium (Serum) mEq/L
Creatinine (Serum) mg/dL
Hematocrit %
White Blood Cell Count x103 cells/mm3
Glasgow Coma Score points
A-a Gradient (if FiO2 ≥0.5) mm Hg
PaO2 (if FiO2 <0.5) mm Hg
A-a = alveolar to arterial; APACHE = Acute Physiology and Chronic Health Evaluation; FiO2 = fraction of inspired oxygen; PaO2 = partial pressure of oxygen in arterial blood; s/p = status post. Calculator available at: http://www.globalrph.com/apacheii.htm.
Figure 3. The APACHE II score for ICU mortality.5
9
Chapter 2: Meeting the Challenges of Multidrug-Resistant Pathogens
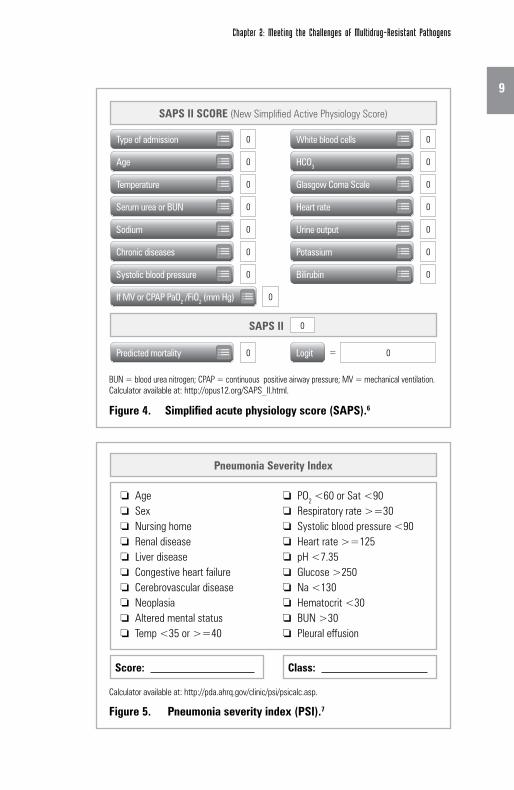
BUN = blood urea nitrogen; CPAP = continuous positive airway pressure; MV = mechanical ventilation. Calculator available at: http://opus12.org/SAPS_II.html.
Calculator available at: http://pda.ahrq.gov/clinic/psi/psicalc.asp.
Figure 5. Pneumonia severity index (PSI).7
Score: Class:
Pneumonia Severity Index
SAPS II SCORE (New Simplified Active Physiology Score)
Age ❏
Sex ❏
Nursing home ❏
Renal disease ❏
Liver disease ❏
Congestive heart failure ❏
Cerebrovascular disease ❏
Neoplasia ❏
Altered mental status ❏
Temp <35 or >=40 ❏
PO ❏ 2 <60 or Sat <90Respiratory rate >=30 ❏
Systolic blood pressure <90 ❏
Heart rate >=125 ❏
pH <7.35 ❏
Glucose >250 ❏
Na <130 ❏
Hematocrit <30 ❏
BUN >30 ❏
Pleural effusion ❏
Predicted mortality Logit0 0
Type of admission 0
If MV or CPAP PaO2 /FiO2 (mm Hg) 0
Age 0
White blood cells 0
Temperature 0
Serum urea or BUN 0
HCO30
Glasgow Coma Scale 0
Sodium 0
Heart rate 0
Chronic diseases 0
Urine output 0
Systolic blood pressure 0
Potassium 0
Bilirubin 0
SAPS II 0 0
10
SERIOUS INFECTIONS in the Critical Care Setting
References1. American Thoracic Society/Infectious Diseases Society of America. Guidelines for the
management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388-416.
2. Adair CG, Gorman SP, Feron BM, et al. Implications of endotracheal tube biofilm for ventilator-associated pneumonia. Intensive Care Med. 1999;25:1072-1076.
3. Kollef MH. The prevention of ventilator-associated pneumonia. N Engl J Med. 1999; 340:627-634.
4. Craven DE, Steger KA. Nosocomial pneumonia in mechanically ventilated adult patients: epidemiology and prevention in 1996. Semin Respir Infect. 1996;11:32-53.
5. Wagner DP, Draper EA, Abizanda Campos R, et al. Initial international use of APACHE. An acute severity of disease measure. Med Decis Making. 1984;4:297-313.
6. New simplified acute physiology score (SAPS II). Available at: http://opus12.org/ SAPS_II.html. Accessed April 16, 2010.
7. Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997;336:243-250.
11
Chapter 2: Meeting the Challenges of Multidrug-Resistant Pathogens
Selecting initial empiric therapy
T here are several fundamental issues here. In the hospital and ICU in particular, selecting an “appropriate” antibiotic agent is a critical deter-
minant for treatment success. Appropriate therapy is defined as an antibiotic that has activity against the bacteria or organisms causing the infection. In vitro testing determines the susceptibility of the organism for the empirically prescribed agents. A number of studies have demonstrated that appropriate initial treatment significantly influences mortality (Figure 6)1-7 and length of hospital stay.8 Importantly, outcome is not improved if inappropriate therapy is later changed in response to bacteriologic findings (Figure 7).9 Therefore, the best approach to empiric therapy is thought to be the selection of an appropriate, broad-spectrum regimen.10,11 This approach has recently been confirmed in a study demonstrating improved survival among patients (mean age: 71 years) who were admitted to the ICU with community-acquired pneumonia and who received guideline-concordant antibiotic therapy.12
Figure 7. Switching from initial inappropriate antibiotic therapy does not improve outcome in patients with pneumonia. Attributable mortality (death from pneumonia-related complications) was significantly higher in the group receiving inappropriate initial antibiotic therapy.9
Figure 8. Importance of prompt antibiotic therapy.13 Results of a study in 107 consecutive patients with VAP. Mean time from initially meeting diagnostic criteria for VAP was 28.6 hours in the delayed group compared with 12.5 hours in the non-delayed group.
34.9%
51/146
32.4%
92/284
24.7%
36/146
16.2%
46/2840
20
10
30
40
All-cause Mortality(P=NS)
Attributable Mortality(P=0.034)
Patie
nts
(%)
Inappropriate initial antibiotic coverage
Appropriate initial antibiotic coverage
Non-delayed
28.4
Delayed
69.7
0
20
40
60
80
Delay in initial appropriate antibiotic treatment
Mor
talit
y (%
)
The second issue involves timing of that therapy. For every hour that goes by before initiation of therapy, the risk of mortality increases dramatically (Figure 8).13
13
Chapter 2: Meeting the Challenges of Multidrug-Resistant Pathogens
Clinicians also need to be aware of their local antibiogram. Within a particular hospital or clinic, there may be specific pathogens that account for most of the problematic infections. Clinicians should know these pathogens and their susceptibilities to formulate the best empiric antibiotic regimen. This approach often requires the use of combination agents, particularly for patients at risk for MDR pathogens, to increase the likelihood of providing appropriate antimicrobial coverage. In my hospital, our antibiogram is regularly updated, so, for example, when we use a combination regimen of an aminoglycoside plus a carbapenem, a cephalosporin, or a b-lactam/b-lactamase inhibitor combination, we are using up-to-date institutional data to provide appropriate therapy for our patients at risk for MDR infections. Finally, a number of adjunctive measures may also be necessary, including source control (through debridement or drainage) and resuscitation (Table 2). Clinicians in the ICU are therefore continually integrating their institution’s local flora and resistance patterns into clinical decision making, predicated of course on thorough, patient-specific risk stratification for MDR pathogens.
References1. Luna CM, Vujacich P, Niederman MS, et al. Impact of BAL data on the therapy and
outcome of ventilator-associated pneumonia. Chest. 1997;111:676-685.
2. Rello J, Gallego M, Mariscal D, Soñora R, Valles J. The value of routine microbial investigation in ventilator-associated pneumonia. Am J Respir Crit Care Med. 1997; 156:196-200.
3. Kollef MH, Ward S. The influence of mini-BAL cultures on patient outcomes: implications for the antibiotic management of ventilator-associated pneumonia. Chest. 1998;113:412-420.
Table 2. Additional steps to consider beyond antibiotic selection
Source control
DebridementAbscess drainageRemoval of any devices that may be contributing to the infectious burden
Resuscitation
Evidence of hemodynamic instability should trigger prompt resuscitation measures guided by central venous pressure and/or central venous oxygen saturation
14
SERIOUS INFECTIONS in the Critical Care Setting
4. Ibrahim EH, Sherman G, Ward S, Fraser VJ, Kollef MH. The influence of inadequate antimicrobial treatment of bloodstream infections on patient outcomes in the ICU setting. Chest. 2000;118:146-155.
5. Vallés J, Rello J, Ochagavía A, Garnacho J, Alcalá MA. Community-acquired bloodstream infection in critically ill adult patients: impact of shock and inappropriate antibiotic therapy on survival. Chest. 2003;123:1615-1624.
6. Harbarth S, Garbino J, Pugin J, Romand JA, Lew D, Pittet D. Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis. Am J Med. 2003;115:529-535.
7. Kumar A, Ellis P, Arabi Y, et al. Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock. Chest. 2009;136:1237-1248.
8. Houck PM, Bratzler DW, Nsa W, Ma A, Bartlett JG. Timing of antibiotic administration and outcomes for Medicare patients hospitalized with community-acquired pneumonia. Arch Intern Med. 2004;164:637-644.
9. Alvarez-Lerma F. Modification of empiric antibiotic treatment in patients with pneumonia acquired in the intensive care unit. ICU-Acquired Pneumonia Study Group. Intensive Care Med. 1996;22:387-394.
10. Höffken G, Niederman MS. Nosocomial pneumonia: the importance of a de-escalating strategy for antibiotic treatment of pneumonia in the ICU. Chest. 2002;122:2183-2196.
11. Ferrer R, Artigas A, Suarez D, et al. Effectiveness of treatments for severe sepsis: a prospective, multicenter, observational study. Am J Respir Crit Care Med. 2009; 180:861-866.
12. Frei CR, Attridge RT, Mortensen EM, et al. Guideline-concordant antibiotic use and survival among patients with community-acquired pneumonia admitted to the intensive care unit. Clin Ther. 2010;32:293-299.
13. Iregui M, Ward S, Sherman C, Fraser VJ, Kollef MH. Clinical importance of delays in the initiation of appropriate antibiotic treatment for ventilator-associated pneumonia. Chest. 2002;122:262-268.
15
Chapter 2: Meeting the Challenges of Multidrug-Resistant Pathogens
Tailoring an antibiotic regimen
D e-escalation reduces unnecessary exposure to antibiotics and has therefore not surprisingly emerged as an effective strategy to
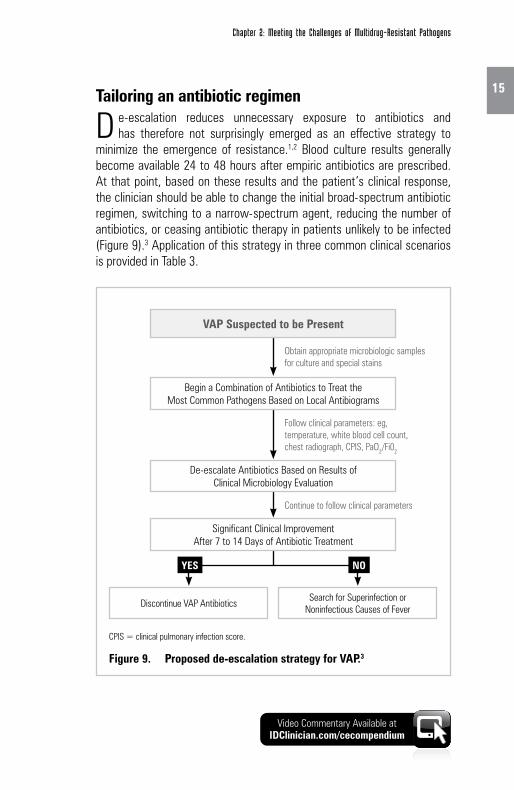
minimize the emergence of resistance.1,2 Blood culture results generally become available 24 to 48 hours after empiric antibiotics are prescribed. At that point, based on these results and the patient’s clinical response, the clinician should be able to change the initial broad-spectrum antibiotic regimen, switching to a narrow-spectrum agent, reducing the number of antibiotics, or ceasing antibiotic therapy in patients unlikely to be infected (Figure 9).3 Application of this strategy in three common clinical scenarios is provided in Table 3.
Video Commentary Available at IDClinician.com/cecompendium
CPIS = clinical pulmonary infection score.
Figure 9. Proposed de-escalation strategy for VAP.3
Obtain appropriate microbiologic samples for culture and special stains
Begin a Combination of Antibiotics to Treat the Most Common Pathogens Based on Local Antibiograms
Significant Clinical Improvement After 7 to 14 Days of Antibiotic Treatment
Discontinue VAP AntibioticsSearch for Superinfection or
Noninfectious Causes of Fever
De-escalate Antibiotics Based on Results of Clinical Microbiology Evaluation
NOYES
16
SERIOUS INFECTIONS in the Critical Care Setting
Reducing the duration of antibiotic treatment is an increasingly important approach to minimizing unnecessary antibiotic utilization and antimicrobial resistance that may otherwise develop. The longer the patient is exposed to antibiotics, particularly in the ICU and in the hospital setting, the greater is the likelihood for that patient to become colonized with drug-resistant pathogens.4,5 Prolonged antibiotic therapy eliminates normal flora in the gastrointestinal tract, allowing colonization with drug-resistant pathogens. Still, the evidence supports patient-specific considerations. For instance, for certain types of infections—pyelonephritis,6 VAP, 7 or HAP, 8 to name a few—a shorter-course regimen of 7 to 8 days is sufficient. However, for patients infected with nonfermenting Gram-negative organisms such as P. aeruginosa, a 15-day course is still warranted.9
Table 3. Application of the de-escalation strategy in clinical practice
Clinical scenario Empiric therapyCulture results and de-escalation response
Patient presents with septic shock.
Empiric therapy includes a drug active against methicillin-resistant Staphylococcus aureus (MRSA), plus a drug active against Gram-negative organisms and an antifungal agent.
Blood culture is positive for MRSA. Eliminate all but the MRSA coverage.
Patient presents with ventilator-associated pneumonia and is at risk for MDR infection.
Empiric therapy includes an agent with antipseudomonal activity (such as a cephalosporin, a carbapenem, or a b-lactam/b-lactamase inhibitor) plus an aminoglycoside.
All blood cultures are negative. Stop the aminoglycoside on the second day. Continue with Gram-negative coverage.
Patient develops complicated intra-abdominal infection 7 days postsurgery. Medical history includes prior exposure to broad-spectrum antibiotic.
Empiric therapy with a carbapenem is selected.
Blood culture is negative for MDR organisms. If patient’s condition has improved, switch to amoxicillin/clavulanic acid or other narrower-spectrum regimen.
17Culture results or biomarkers such as procalcitonin may facilitate de-escala-tion and shorter courses of antibiotic regimens. For instance, in a patient with suspected VAP, empiric antibiotic therapy can be stopped if a lower respiratory tract culture is negative.4 However, it is important to note that routine monitoring of lower respiratory tract cultures prior to development of HAP or VAP is not recommended.4 In one study, 38% (47/125) of culture results obtained before VAP onset were either sterile or identified bacteria that were not involved in the subsequent infection; only 31% (39/125) of cultures identified all the organisms ultimately responsible for the infection.10 Procalcitonin is a biomarker that is elevated in the serum of patients who are exposed to a bacterial pathogen or have an active bacterial infection.11 Two recent studies demonstrated that for patients who have persistently low serum levels of procalcitonin, it is safe to discontinue antibiotics (Figure 10).12,13
Chapter 2: Meeting the Challenges of Multidrug-Resistant Pathogens
Figure 10. Proposed algorithm for procalcitonin-guided antibiotic treatment in ICU patients.13
If blood sample taken for calculation of procalcitonin concentration at early stage of episode, obtain a second procalcitonin concentration 6-12 hr later
Guidelines for starting antibiotic therapy*
Guidelines for continuing or stopping antibiotic therapy
Concentration <0.25 mg/L
Stopping of antibiotics strongly
encouraged
Decrease by ≥80% from peak concentration, or
concentration ≥0.25 and <0.5 mg/L
Stopping of antibiotics
encouraged
Decrease by <80% from peak
concentration, and concentration
≥0.5 mg/L
Continuing of antibiotics encouraged
Increase of concentration
compared with peak concentration, and
concentration ≥0.5 mg/L
Changing of antibiotics strongly
encouraged
Concentration <0.25 mg/L
Antibiotics strongly discouraged
Concentration ≥0.25 and <0.5 mg/L
Antibiotics discouraged
Concentration ≥0.5 and <1 mg/L
Antibiotics encouraged
Concentration ≥1 mg/L
Antibiotics strongly encouraged
18
SERIOUS INFECTIONS in the Critical Care Setting
Clinicians in the ICU must balance the need to treat early and aggres-sively using broad-spectrum, empiric antimicrobial agents with the equally important need to avoid emergence and spread of resistant bacteria. Application of current evidence-based recommendations can help clinicians achieve the balance, shaped always by good clinical judgment.
References1. Höffken G, Niederman MS. Nosocomial pneumonia: the importance of a de-escalating
strategy for antibiotic treatment of pneumonia in the ICU. Chest. 2002;122:2183-2196.
2. Rello J, Vidaur L, Sandiumenge A, et al. De-escalation therapy in ventilator-associated pneumonia. Crit Care Med. 2004;32:2183-2190.
3. Iregui M, Ward S, Sherman C, Fraser VJ, Kollef MH. Clinical importance of delays in the initiation of appropriate antibiotic treatment for ventilator-associated pneumonia. Chest. 2002;122:262-268.
4. American Thoracic Society/Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388-416.
5. Kollef MH. What is ventilator-associated pneumonia and why is it important? Respir Care. 2005;50:714-721.
6. Kyriakidou KG, Rafailidis P, Matthaiou DK, Athanasiou S, Falagas ME. Short- versus long-course antiobiotic therapy for acute pyelonephritis in adolescents and adults: a meta-analysis of randomized controlled trials. Clin Ther. 2008;30:1859-1868.
7. Chastre J, Wolff M, Fagon J-Y, et al, for the PneumA Trial Group. Comparison of 8 vs 15 days of antibiotic therapy for ventilator-associated pneumonia in adults: a randomized trial. JAMA. 2003;290:2588-2598.
8. Pugh RJ, Cooke RP, Dempsey G. Short course antibiotic therapy for Gram-negative hospital-acquired pneumonia in the critically ill. J Hosp Infect. 2010;74:337-343.
9. Peleg AY, Hooper DC. Hospital-acquired infections due to Gram-negative bacteria. N Engl J Med. 2010;362:1804-1813.
10. Hayon J, Figliolini C, Combes A, et al. Role of serial routine microbiologic culture results in the initial management of ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165:41-46.
11. Müller F, Christ-Crain M, Bregenzer T, et al; for the ProHOSP Study Group. Procalcitonin levels predict bacteremia in patients with community-acquired pneumonia: a prospective cohort trial. Chest. 2010; epublished ahead of print, Mar 18.
12. Burkhardt O, Ewig S, Haagen U, et al. A simple procalcitonin-guided strategy results in safe reductions of antibiotic use in patients with symptoms of acute respiratory tract infections in primary care. Eur Respir J. 2010; epublished ahead of print, Feb 25.
13. Bouadma L, Luyt CE, Tubach F, et al; PRORATA trial group. Use of procalcitonin to reduce patients’ exposure to antibiotics in intensive care units (PRORATA trial): a multicentre randomised controlled trial. Lancet. 2010;375:463-474.
19
Chapter 2: Meeting the Challenges of Multidrug-Resistant Pathogens
Effective use of antibiograms
A hospital’s antibiogram provides information on the overall antimi-crobial susceptibility of Gram-negative and Gram-positive bacteria.
Understanding local susceptibility data helps intensivists, hospitalists, and other clinicians select antibiotic regimens that are more likely to provide appropriate initial treatment and minimize unnecessary antibiotic exposure.
Hospitals within the same city can have very different antibiograms.1 This is often due to the patient mix, as well as antibiotic prescribing practices within those institutions. Even within a hospital, particularly larger hospitals that have specialized units, there can be significant differences in the pathogens and their antimicrobial susceptibilities from one unit to the other.1
Recent studies have demonstrated the potential for inadequate dosing of antibiotics in patients who have high volumes of distribution, such as the trauma patient or the patient in septic shock.2,3 Such patients may have worse clinical outcomes; in part because the antibiotic is diluted out and the concentration of that drug is diminished, relative to the minimum inhibitory concentration (MIC) of the isolates. For example with amikacin, peak blood concentrations of ≥64 mg/kg are required to be effective against important ICU pathogens such as Enterobacteriaceae and P. aeruginosa.3 In patients with severe sepsis or septic shock, an amikacin dose of ≥25 mg/kg is required to reach therapeutic peak concentrations instead of the dose of 15-20 mg/kg customarily recommended.3,4
These and related examples underscore the clinical utility of antibiograms. In-depth familiarity with the flora of an ICU—as presented within the antibiogram—can prove essential to resolution of a broad array of serious infections, particularly for very sick patients.
References1. Kollef MH. What is ventilator-associated pneumonia and why is it important?
Respir Care. 2005;50:714-721.2. Mohr JF III, Ostrosky-Zeichner L, Wainright DJ, Parks DH, Hollenbeck TC, Ericsson CD.
Pharmacokinetic evaluation of single-dose intravenous daptomycin in patients with thermal burn injury. Antimicrob Agents Chemother. 2008;52:1891-1893.
3. Taccone FS, Laterre PF, Spapen H, et al. Revisiting the loading dose of amikacin for patients with severe sepsis and septic shock. Crit Care. 2010;14:R53. epublished ahead of print, Apr 6.
4. Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis. 2010;50:133-164.
Video Commentary Available at IDClinician.com/cecompendium
20
SERIOUS INFECTIONS in the Critical Care Setting
Implementing an antimicrobial stewardship program in the ICU
A ntimicrobial stewardship involves a multifaceted approach that optimizes antibiotic efficacy, minimizes the emergence of drug
resistance, and controls costs (Figure 11).1 While these goals apply to all hospital units and involve infectious disease specialists, intensivists, and hospitalists alike, they are particularly relevant to the ICU, because of the frequency with which antibiotic therapy is prescribed in this unit. The goals are not mutually exclusive, but rather demand a collaborative, multidisciplinary commitment to understanding the forces that govern dynamic changes in institutional flora and resistance patterns, and adapting institutional policies, prescribing practices, and care bundles accordingly.
Specific components and systems of antimicrobial stewardship programs are necessarily tailored to the needs and resources of a specific institution.1-3 Two components of antibiotic therapy are consistently applied across all types of academic and community-based hospitals and long-term care facilities1:
• Empirictherapyshouldbe appropriate and based on an informed understanding of the likely causal pathogens and their local susceptibility profiles.
• Empirictherapyshouldbeadequate—that is, dosed and administered in such a manner that sufficient concentrations are achieved at the infection site.
At our hospital, the stewardship program also stresses the importance of antimicrobial de-escalation, which occurs as soon as culture results become available and encourages the shortest possible course of antibiotics.
Figure 11. Goals of antimicrobial stewardship.1
Antimicrobial Stewardship
Combat the Emergence of Resistance
Improve Clinical Outcomes
Control Costs
21
Chapter 2: Meeting the Challenges of Multidrug-Resistant Pathogens
It should be emphasized that this is a hospital-wide effort. New data show that spread of MDR organisms in the ICU is influenced by infections and invasive procedures elsewhere in the hospital.4 Therefore, whether it’s a hospital unit or an ICU, the clinician is expected to be the local champion, ensuring that proper infection control practices are carried out.
Ultimately, the linchpin to successful antibiotic stewardship is institutional acceptance and familiarity, with all clinicians endorsing its fundamental tenets and recommendations, the compliance to which are monitored longi-tudinally across all units. If you have an antimicrobial stewardship program in place, yet you continue to see escalating problems with the emergence of drug-resistant isolates within your hospital, then the program needs to be revisited to ensure that it is being applied in an optimal manner (Figure 12).5
Figure 12. A conceptual framework for antibiotic use in an antimicrobial stewardship program.5
Physician’s Attitude
Patient’s Attitude and Desires
Availability of Antibiotics
Cultural Results
Decision to Use Antibiotics
Refine Choice of Antibiotics
Choice of Antibiotics
Knowledge of Infectious Diseases
Knowledge of Patient
Knowledge of Antibiotics
2,3,5,6
2,3,5,6
4,6
4,5,6
3,5,6
1,6
1,61,6
1,6
22
SERIOUS INFECTIONS in the Critical Care Setting
References1. Lawrence KL, Kollef MH. Antimicrobial stewardship in the intensive care unit.
Am J Respir Crit Care Med. 2009;179:434-438.
2. Dellit TH, Owens RC, McGowan JE, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44:159-177.
3. Fishman N. Antimicrobial stewardship. Am J Infect Control. 2006;34:S55-S63.
4. Jacoby TS, Kuchenbecker RS, Dos Santos RP, Magedanz L, Guzatto P, Moreira LB. Impact of hospital-wide infection rate, invasive procedures use and antimicrobial consumption on bacterial resistance inside an intensive care unit. J Hosp Infect. 2010;75:23-27.
5. Owens RC Jr, Shorr AF, Deschambeault AL. Antimicrobial stewardship: shepherding precious resources. Am J Health Syst Pharm. 2009;66(suppl 4):S15-S22.
23
Download this and additional tools at
Chapter 3: Rational Dosing of Antibiotics in Critically Ill PatientsSandy J. Estrada, PharmD, BCPS
Role of PK-PD strategies
I n the ICU, patients are by definition at risk for serious, even life-threat-ening nosocomial infections. The dynamic relationship between PK and
PD parameters decisively shapes the course of infection and ultimately patient outcomes.1 This interrelationship varies with the pharmacological properties of an antibiotic, its route of administration, and a broad array of patient-specific variables including age, health and immune status, and genetic polymorphisms. Rational application of an antimicrobial agent’s PK and PD properties is therefore critical and can help guide antibiotic selection, dosing strategies, and, ultimately, blunt the continued rise of resistant pathogens.2,3 Dosing regimens, in particular, must be formu-lated to address the rise of MDR pathogens in the ICU. Concentrations of an antibiotic in serum, tissues, and the site of infection significantly influence the ability of pathogens to evade antimicrobial agents through various resistance mechanisms. An empiric broad-spectrum antibiotic regimen must therefore achieve adequate (clinically effective) tissue penetration. Gaps in antimicrobial coverage should be addressed as well, and can be filled with combination strategies, with each agent requiring similarly effective tissue penetration. To optimize treatment response and minimize resistance, empiric therapy should be reviewed daily by the multidisci-plinary ICU team and revised to reflect culture results, impact of appropriate surgical source control measures, and signs and symptoms associated with clinical improvement or toxicity. This daily review should be consistent with evidence-based national and institutional guidelines, stewardship programs, and formulary considerations. In short, and as discussed recently by Joseph and colleagues, clinical decision making in the hospital and especially in the ICU, where the margin for error is at times vanishingly small, necessarily addresses the right Drug, right Dose, De-escalation, and adequate Duration of therapy, or the four D’s of optimal antimicrobial therapy.4
24
SERIOUS INFECTIONS in the Critical Care Setting
Antibiograms
C ontinual consideration of antibiogram data is critical for patients in the ICU. Bacterial susceptibility breakpoints are derived from semi-
quantitative in vitro measurements, indicating the percentage of isolates of a particular organism that are susceptible to select antibiotics in a given institution or unit (Figure 13). Incorporating real-time MIC data or similar results from longitudinal surveillance of pathogen susceptibility into the therapeutic plan is also an essential component of infectious disease management. Clinical and Laboratory Standards Institute (CLSI) breakpoints for the ESKAPE pathogens and antibiotics commonly used to treat them are given in Table 4.5
Ideally, >30 isolates should be tested for susceptibility to ensure accurate data.
Since production of ESBL is an important mechanism of resistance, it may be useful to include these data.
Data are quoted as percentage of isolates that are susceptible.
Empiric therapy for complicated intra-abdominal infections (healthcare associated) should have substantial antipseudomonal activity. Thus, piperacillin-tazobactam or a carbapenem would be suitable choices. If multidrug resistance is suspected, an extended infusion of carbapenem may be necessary.
25Table 4. CLSI breakpoint values for antibiotics commonly used
Chapter 3: Rational Dosing of Antibiotics in Critically Ill Patients
Ensuring adequate therapy
A n antibiogram can help select appropriate therapy, but other consid-erations are involved in ensuring that therapy is adequate. In the case
of b-lactams, which have time-dependent antimicrobial activity, the dosing interval is the key parameter; that is, if a dose is sufficient to achieve a concen-tration above the MIC, increasing the dose will not increase the antibacterial effect.6 Therefore, time over the MIC (T>MIC) is the preferred PK-PD metric for assessing efficacy (Table 5). For most b-lactams, a T>MIC for 40% to 50% of the dosing interval is generally considered effective, with the exception of the carbapenems, which may require lower values.2 An effective T>MIC
26
SERIOUS INFECTIONS in the Critical Care Setting
may be achieved via shorter dosing intervals or with extended infusions.2
Infusion time should be tailored to the MIC, particularly when MIC values are at or near the breakpoint. In one study of carbapenem dosing, a 1-hour infusion met the T>MIC target against pathogens with an MIC of 1 mg/mL, but against pathogens with MICs of 2 mg/mL and 4 mg/mL, infusions of 3 hours and 5 hours, respectively, were required.7 A recent trial in patients with VAP compared two different carbapenem dosing strategies8:
• Doripenem500mgadministeredasanextended,4-hourinfusion, with 4 hours between infusions (ie, equivalent to 500 mg q8h)
• Dependingonstandardpracticeateachstudysite,imipenemwasgiven at a dosage of either 500 mg q6h via a 30-minute infusion or 1000 mg q8h, administered as a 60-minute infusion (pharmaco- dynamically equivalent regimens)
Notably, the extended-infusion regimen was associated with significantly lower length of hospital stay and time on mechanical ventilation and demonstrated noninferior clinical cure rates when compared to the short infusion regimens.6,9 These data support the hypothesis that extending the T>MIC for select patient populations may be associated with favorable outcomes. Additional well-designed studies comparing extended infusions to traditional dosing are needed.
For antibiotics with a concentration-dependent pattern of antimicro-bial activity, the drug dose is the essential determinant of bacteriologic and clinical efficacy. Consequently, the peak concentration to MIC ratio (Cmax:MIC) is the preferred metric. For example, the antipseudomonal break-point for gentamicin and tobramycin is <4 mg/mL, with a desired Cmax 10-12 times this value. Traditional dosing will yield a peak of 8-10 mg/mL, which is sufficient for an MIC of 0.5 mg/mL, although it would be inadequate for an MIC of 2 mg/mL. If the optimal value of Cmax:MIC cannot be achieved, time should be factored in and area under the concentration-time curve (AUC) to MIC ratio should be used (Table 5).2,3 Fluoroquinolone levels exceeding a specific AUC:MIC ratio proved critical in one recent study of nosocomial pneumonia patients. Even when the dosing interval and dose are appropriate, tissue penetration should be taken into consideration. For example, vancomycin is a large molecule and penetrates poorly into some tissues, particularly the lungs.6
27
Chapter 3: Rational Dosing of Antibiotics in Critically Ill Patients
Table 5. PK-PD metrics that are best measures of clinical efficacy for each antimicrobial class2,3
Antimicrobial agent
Pattern of in vitro antibacterial activity
PK-PD measure(s) Target value
AminoglycosidesConcentration
dependentAUC0-24:MIC,
Cmax:MICCmax:MIC 10-12
b-Lactams
Penicillins Time dependent T>MIC T>MIC for 40% of dosing interval (carbapenems) or
40%-50% of dosing interval (all others)
Cephalosporins Time dependent T>MICCarbapenems Time dependent T>MICMonobactams Time dependent T>MIC
Clindamycin Time dependent AUC0-24:MIC N/A
Glycopeptides/lipopeptides
DaptomycinConcentration
dependentAUC0-24:MIC,
Cmax:MICN/A
OritavancinConcentration
dependentT>MIC, Cmax:MIC
Vancomycin Time dependent AUC0-24:MIC
Macrolides
Azithromycin Time dependent AUC0-24:MIC
AUC:MIC>25Clarithromycin Time dependent AUC0-24:MIC
TelithromycinConcentration
dependentAUC0-24:MIC
MetronidazoleConcentration
dependentAUC0-24:MIC,
Cmax:MICN/A
Oxazolidinones
Linezolid Time dependent AUC0-24:MIC N/A
QuinolonesConcentration
dependentAUC0-24:MIC,
Cmax:MIC
AUC:MIC≥125 (Gram-negative) or ≥33.7 (Gram-
positive)
Tetracyclines
Doxycycline Time dependent AUC0-24:MICN/A
Tigecycline Time dependent AUC0-24:MIC
28
SERIOUS INFECTIONS in the Critical Care Setting
cfu = colony-forming units.
Figure 14. Time-kill assay showing synergistic activity of colistin plus doripenem against pan-resistant Acinetobacter.10
S uggestions for Gram-negative HAIs based on PK-PD principles have recently been published (Tables 6 and 7).12
Revisiting old therapies
C olistin is associated with significant neurotoxicity and nephrotoxicity and has therefore been reserved for extreme cases of MDR
A. baumannii and P. aeruginosa strains that are not susceptible to other anti-biotics. A recent study demonstrated synergistic effects when colistin was used in combination with carbapenems, permitting use of lower colistin dosages (Figure 14).10,11
29
Chapter 3: Rational Dosing of Antibiotics in Critically Ill Patients
Table 6. Suggested empirical therapies to cover Gram-negative HAIs*
Recommended therapy and dosage
Hospital-acquired pneumonia (includes VAP and HCAP)
Length of hospital stay <5 days before pneumonia developed
One of the following regimens: ceftriaxone, •1 g given intravenously every 24 hr; ampicillin–sulbactam, 3 g given intravenously every 6 hr; levofloxacin, 750 mg given orally or intravenously every 24 hr; moxifloxacin, 400 mg given orally or intravenously every 24 hr; or ertapenem, 1 g given intravenously every 24 hr
Length of hospital stay ≥5 days before pneumonia developed or diagnosis of HCAP
One of the following antipseudomonal • b-lactam regimens: cefepime, 2 g given intravenously every 12 hr; ceftazidime, 2 g given intravenously every 8 hr; piperacillin–tazobactam, 4.5 g given intravenously every 6–8 hr; ticarcillin–clavulanate, 3.1 g given intravenously every 6 hr; meropenem, 1–2 g given intravenously every 8 hr; imipenem, 500 mg given intravenously every 6 hr; doripenem, 500 mg given intravenously every 8 hr or as a 1-hr or 4-hr infusion; or aztreonam, 1 g given intravenously every 8 hrPlus one of the following regimens: ciprofloxacin, •400 mg given intravenously every 8–12 hr; levofloxacin, 750 mg given intravenously every 24 hr; gentamicin or tobramycin, 5–7 mg/kg of body weight given intravenously every 24 hr; or amikacin, 15–20 mg/kg given intravenously every 24 hr
One of the following regimens: cefepime, 1 g given •intravenously every 12 hr; ceftazidime, 1 g given intravenously every 8 hr; piperacillin–tazobactam, 3.75 g given intravenously every 8 hr; meropenem, 500 mg given intravenously every 8 hr; imipenem, 500 mg given intravenously every 8 hr; doripenem, 500 mg given intravenously every 8 hr; aztreonam, 500 mg given intravenously every 8 hr; ciprofloxacin, 400 mg given orally or intravenously every 12 hr; or gentamicin, 5–7 mg/kg given intravenously every 24 hr
Meropenem, 1–2 g given intravenously •every 8 hr; or imipenem, 500 mg given intravenously every 6 hr; doripenem, 500 mg given intravenously every 8 hr or as a 1-hr or 4-hr infusion
Carbapenemase–producing Enterobacteriaceae
Colistin, 2.5–5.0 mg of colistin base/kg of •body weight/day given in 2 to 4 divided doses (equivalent to 6.67–13.3 mg of colistimethate sodium/kg/day); or tigecycline, 100 mg given intravenously as a loading dose, then 50 mg given intravenously every 12 hr
Carbapenem-resistant Pseudomonas aeruginosa and Acinetobacter baumannii
For • P. aeruginosa: Colistin as for carbapenemase–producing Enterobacteriaceae For • A. baumannii: Colistin as for carbapenemase–producing Enterobacteriaceae; or ampicillin–sulbactam, up to 6 g of sulbactam given intravenously per day; or tigecycline, 100 mg intravenous loading dose, then 50 mg given intravenously every 12 hrPossible alternatives: Extended infusion of •meropenem, 1–2 g given as an intravenous infusion over a 3-hr period every 8 hr; of doripenem, 500 mg–1 g given as an intravenous infusion over a 4-hr period every 8 hr; or of imipenem, 1 g given as an intravenous infusion over a 3-hr period every 8 hr; combination therapy with a nontraditional antibiotic, including rifampin, minocycline or doxycycline, or azithromycinFor pneumonia: Nebulized colistimethate •sodium, 1 million to 3 million IU/day in divided doses (diluted in sterile normal saline), administered with a conventional nebulizer; or nebulized aminoglycosides
31
Chapter 3: Rational Dosing of Antibiotics in Critically Ill Patients
References1. Burgess S. Curbing resistance development: maximizing the utility of available agents.
J Manag Care Pharm. 2009;15(5 suppl):S5-S9.
2. Owens RC Jr, Shorr AF. Rational dosing of antimicrobial agents: pharmacokinetic and pharmacodynamic strategies. Am J Health Syst Pharm. 2009;66(suppl 4):S23-S30.
3. Ambrose PG, Bhavnani SM, Rubino CM, et al. Pharmacokinetics-pharmacodynamics of antimicrobial therapy: It’s not just for mice anymore. Clin Infect Dis. 2007;44:79-86.
4. Joseph J, Rodvold KA. The role of carbapenems in the treatment of severe nosocomial respiratory tract infections. Expert Opin Pharmacother. 2008;9:561-575.
5. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Testing; 19th Informational Supplement. Wayne, PA: CLSI; 2009. CLSI document M100-S19.
6. Barlow G, Nathwani D. Is antibiotic resistance a problem? A practical guide for hospital clinicians. Postgrad Med J. 2005;81:680-692.
7. Bhavnani SM, Hammel JP, Cirincione BB, Wikler MA, Ambrose PG. Use of pharmacokinetic-pharmacodynamic target attainment analyses to support phase 2 and 3 dosing strategies for doripenem. Antimicrob Agents Chemother. 2005;49:3944-3947.
8. Chastre J, Wunderink R, Prokocimer P, Lee M, Kaniga K, Friedland I. Efficacy and safety of intravenous infusion of doripenem versus imipenem in ventilator-associated pneumonia: a multicenter, randomized study. Crit Care Med. 2008;36:1089-1096.
9. Merchant S, Gast C, Nathwani D, et al. Hospital resource utilization with doripenem versus imipenem in the treatment of ventilator-associated pneumonia. Clin Ther. 2008;30:717-733.
10. Shields RK, Potoski BA, Clancy CJ, et al. Microbiologic and clinical evidence supporting the combination of doripenem and colistin for the treatment of pan-resistant Acinetobacter. Presented at the 49th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC); Sept 12-15, 2009; San Francisco, CA.
11. Pankuch GA, Appelbaum PC. Activity of doripenem, with and without levofloxacin and amikacin, against 25 P. aeruginosa by synergy time-kill. Presented at the 49th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC); Sept 12-15, 2009; San Francisco, CA.
12. Peleg AY, Hooper DC. Hospital-acquired infections due to Gram-negative bacteria. N Engl J Med. 2010;362:1804-1813.
32
SERIOUS INFECTIONS in the Critical Care Setting
33
Download this and additional tools at
Chapter 4: A Practical Guide to Using Bundles in the ICULisa G. Jones, RN, MS, CCRN
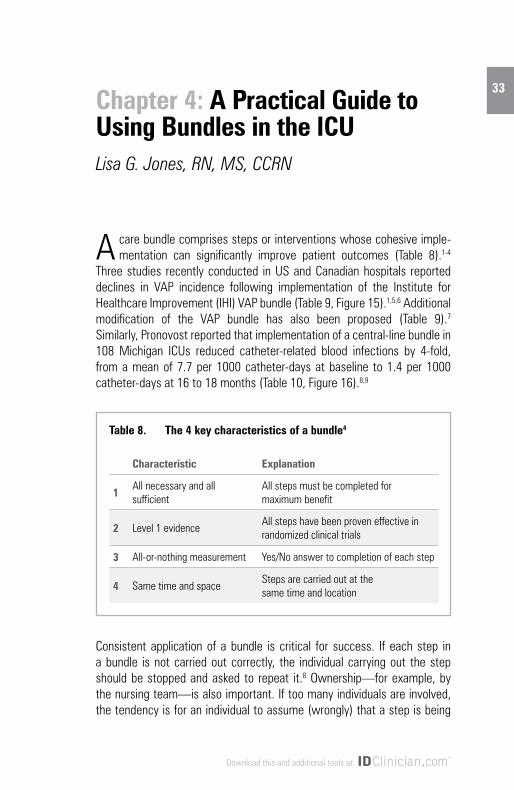
A care bundle comprises steps or interventions whose cohesive imple-mentation can significantly improve patient outcomes (Table 8).1-4
Three studies recently conducted in US and Canadian hospitals reported declines in VAP incidence following implementation of the Institute for Healthcare Improvement (IHI) VAP bundle (Table 9, Figure 15).1,5,6 Additional modification of the VAP bundle has also been proposed (Table 9).7 Similarly, Pronovost reported that implementation of a central-line bundle in 108 Michigan ICUs reduced catheter-related blood infections by 4-fold, from a mean of 7.7 per 1000 catheter-days at baseline to 1.4 per 1000 catheter-days at 16 to 18 months (Table 10, Figure 16).8,9
Consistent application of a bundle is critical for success. If each step in a bundle is not carried out correctly, the individual carrying out the step should be stopped and asked to repeat it.8 Ownership—for example, by the nursing team—is also important. If too many individuals are involved, the tendency is for an individual to assume (wrongly) that a step is being
Table 8. The 4 key characteristics of a bundle4
Characteristic Explanation
1All necessary and all sufficient
All steps must be completed for maximum benefit
2 Level 1 evidenceAll steps have been proven effective in randomized clinical trials
3 All-or-nothing measurement Yes/No answer to completion of each step
4 Same time and spaceSteps are carried out at the same time and location
34
SERIOUS INFECTIONS in the Critical Care Setting
carried out by someone else. However, all ICU personnel should be involved in refining the process. For example, when an infection is posted, multidisci-plinary discussion can help identify areas where a bundle can be improved. Only through continued education and feedback can optimal care (and zero infections) be achieved.
Figure 15. Reduction in VAP incidence following implementation of the IHI VAP bundle in US and Canadian ICUs.1,5,6
Table 9. The modified IHI VAP bundle
√ Elevation of the head of the bed
IHI bundle4√ Daily “sedation vacations” and assessment of
readiness to extubate
√ Peptic ulcer disease prophylaxis
√ Deep venous thrombosis prophylaxis
√ Oral decontamination with chlorhexidine antiseptic Proposed additional
steps7√ Continuous aspiration of subglottic secretions
0
2
4
6
8
10
Resar et al1
VAP
Inci
denc
e (p
er 1
000
vent
ilato
r day
s)
Before After
6.6
Berriel-Cass et al5
Youngquist et al6
8.2
2.73.3
6.1
2.7 2.7
0
35
Chapter 4: A Practical Guide to Using Bundles in the ICU
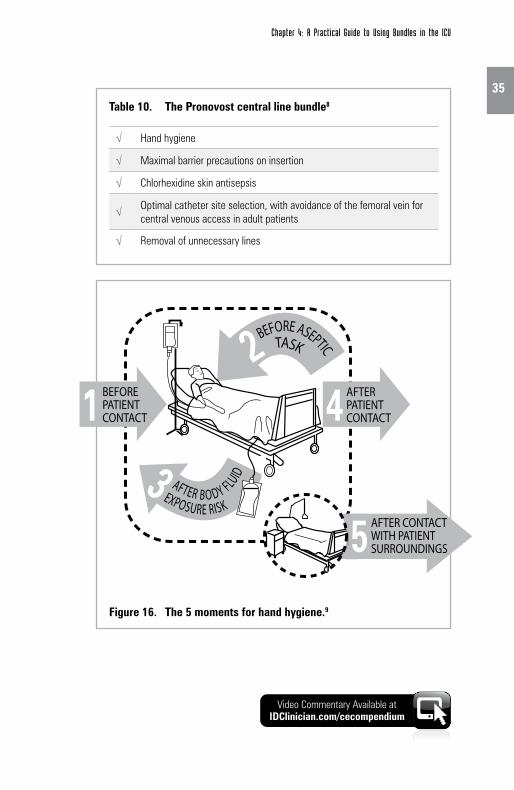
Table 10. The Pronovost central line bundle8
√ Hand hygiene
√ Maximal barrier precautions on insertion
√ Chlorhexidine skin antisepsis
√ Optimal catheter site selection, with avoidance of the femoral vein for central venous access in adult patients
√ Removal of unnecessary lines
Figure 16. The 5 moments for hand hygiene.9
BEFORE ASEPTICTASK
AFTER B O DY FLUID
EXPOSURE RISK
Chapter 4Figure 16
AFTER PATIENTCONTACT
AFTER CONTACT WITH PATIENTSURROUNDINGS
BEFORE PATIENTCONTACT1
51
4
3
2
Video Commentary Available at IDClinician.com/cecompendium
36
SERIOUS INFECTIONS in the Critical Care Setting
References1. Resar R, Pronovost P, Haraden C, Simmonds T, Rainey T, Nolan T. Using a bundle
approach to improve ventilator care processes and reduce ventilator-associated pneumonia. Jt Comm J Qual Patient Saf. 2005;31:243-248.
2. Cocanour CS, Peninger M, Domonoske BD, et al. Decreasing ventilator-associated pneumonia in a trauma ICU. J Trauma. 2006;61:122-129.
3. Galpern D, Guerrero A, Tu A, Fahoum B, Wise L. Effectiveness of a central line bundle campaign on line-associated infections in the intensive care unit. Surgery. 2008;144: 492-495.
4. Institute for Healthcare Improvement. What is a bundle? Available at: www.ihi.org/IHI/Topics/CriticalCare/IntensiveCare/ImprovementStories. Accessed April 23, 2010.
5. Berriel-Cass D, Adkins FW, Jones P, Fakih MG. Eliminating nosocomial infections at Ascension Health. Jt Comm J Qual Patient Saf. 2006;32:612-620.
6. Youngquist P, Carroll M, Farber M, et al. Implementing a ventilator bundle in a community hospital. Jt Comm J Qual Patient Saf. 2007;33:219-225.
7. Wip C, Napolitano L. Bundles to prevent ventilator-associated pneumonia: how valuable are they? Curr Opin Infect Dis. 2009;22:159-166.
8. Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006;355:2725-2732.
9. World Health Organization. Available at: http://www.who.int/gpsc/tools/ 5momentsHandHygiene_A3.pdf. Accessed April 23, 2010.
37
Download this and additional tools at
Chapter 5: Therapeutic Challenges in the ICU: 75-Year-Old Female With Acute CholecystitisAndrew F. Shorr, MD, MPH, FCCP
• 75-year-oldfemalewithacutecholecystitisadmittedfor open gall bladder surgery
• Historyoftype2diabetesandhypertension – Previous bouts of diabetic foot infection
fever of 99.8o F • Day5:patientcomplainsofchestpainandshortnessofbreath – Fever, 101.3o F – Coughing produces a small amount of sputum
This patient’s history is notable for multiple bouts of diabetic foot infection requiring antibiotic treatment. Her surgery is uneventful; she recovers in the postanesthesia care unit (PACU); and she is transferred to the wards, where she is transitioned early to oral intake and begins to ambulate.
She is expected to remain in the hospital for 3 to 4 days, but on the fourth postop day her condition worsens.
COMMENTARY
Video Commentary Available at IDClinician.com/cecompendium
decreased breath sounds • Laboratory – WBC, 18.6 x 103 cell/mL with a left shift – Sodium, 145 mEq/L – Potassium, 4.5 mEq/L – BUN, 25 mg/dL; creatinine, 1.8 mg/dL
On examination, her blood pressure is satisfactory, but she has tachycardia. Her respiratory rate is elevated, and she has borderline hypoxemia. There is evidence of right lower lobe consolidation with right lower lobe crackles and decreased breath sounds. The lab studies that morning revealed a newly-elevated WBC count and normal sodium and potassium, but an elevated BUN and renal insufficiency with a creatinine of 1.8 mg/dL.
She is placed on supplemental oxygen and a chest x-ray is ordered.
COMMENTARY
The chest x-ray reveals some haziness in her right lower lobe. This suggests a right lower lobe infiltrate.
COMMENTARY
39
Chapter 5: Therapeutic Challenges in the ICU: 75-Year-Old Female With Acute Cholecystitis
making process?• Howdocomorbidconditionsinfluenceyourtreatmentregimens?
Because this patient developed her infection after several days of hospitalization (even though it was following a low-risk surgical procedure), one must consider an MDR pathogen.
It is important to know your institution’s antibiogram. In our institution, ESBL pathogens are common, while K. pneumoniae with carbapenemases are not.
Where the patient developed her infection may also be important. In my ICU, resistance patterns are quite different from what we see in the wards.
The patient’s diabetes and hypertension indicate that she is at risk for developing renal insufficiency. This must be kept in mind when selecting an antibiotic regimen. In addition, her history of antibiotic exposure indicates that the clinician should review her medical record for the specific antibiotics used. With that information, one can select a regimen distinct from what she may have had before.
COMMENTARY
The paradigm that we follow is to start with a broad-spectrum regimen that targets the most likely pathogens. In our hospital, cefepime, amikacin, and vancomycin represent a combination that ensures that the patient receives initial appropriate therapy.
COMMENTARY
40
SERIOUS INFECTIONS in the Critical Care Setting
Another important point is to obtain a lower airway culture, using one of the available bronchoscopic techniques. Such cultures help identify those pathogens that are involved and those that are not, thereby permitting clinicians to de-escalate and narrow the antibiotic regimen.
Finally, it should be emphasized that traditional recommendations for relatively long-duration therapy were based principally on expert opinion. We now have randomized studies demonstrating that short-course (7 to 8 days) therapy is adequate, so long as a patient has gotten initially appropriate therapy and there is no involvement of non-lactose fermenting Gram-negative rods.1,2
• BroughttoICUandputonventilator• Conditionworsensafter48hr – New fever to 101.2o F – WBC increases to 15 x 103 cells/mL – BUN 30 mg/dL, creatinine 1.9 mg/dL
The discussion above represented a case of HAP leading to respiratory failure and mechanical ventilation. But what if there were a very different clinical course following surgery? An alternative scenario for this case involves the need for ventilation immediately following surgery and subsequent infection during the stay in the ICU.
COMMENTARY
41
Chapter 5: Therapeutic Challenges in the ICU: 75-Year-Old Female With Acute Cholecystitis
Her chest x-ray clearly shows a right-sided infiltrate, suggesting that she has VAP. Patients with VAP are at high risk for death.3 Computed tomography (CT) angiography ruled out pulmonary embolism and confirmed VAP.
She is placed on the same empiric therapy as the previous case scenario (cefepime, amikacin, and vancomycin).
A bronchoscopy is also ordered, since a sputum sample may not be indicative of pathogen involvement in the lower airway.
COMMENTARY
• LowerairwaypositiveforAcinetobacter baumannii – Resistant to fourth-generation cephalosporins – Resistant to quinolones – Sensitive to carbapenems
• Antibiotictherapyisnarrowed – Carbapenem is added (doripenem, imipenem, or meropenem) – Cefepime, vancomycin are discontinued
A lower airway sample was obtained via “blind” bronchial brush and revealed the presence of A. baumannii. A carbapenem is added and the cefepime and vancomycin discontinued. Because carbapenem-resistant Acinetobacter has occasionally been isolated at our hospital, the amikacin was continued. The result is clinical improvement. Figures 17 and 18 and Table 11 are resources to aid in pneumonia diagnoses.4,5
Figure 17. Centers for Disease Control (CDC)/National Healthcare Safety Network (NHSN) algorithms for diagnosis of pneumonia type PNU 1, 2, 3.4
Serial x-rays (≥2 in patients with underlying disease, ≥1 in patients without underlying disease) with 1 of the following:•Neworprogressiveandpersistentinfiltrate/consolidation/cavitation/pneumatoceles
(aged ≤1 year)
And 1 of the following clinical criteria:•Fever(>38°C/100.4°F)withnoothercause•Leukopenia(<4000/mm3) or leukocytosis (≥12,000/mm3) •Alteredmentalstatuswithnoothercause(inpersonsaged≥70 years)
And 2 of the following clinical criteria:•Newpurulentsputumorchangeincharacter/↑ respiratory secretions/ ↑ suction requirement•Neworworseningcoughordyspnea/tachypnea•Ralesorbronchialbreathsounds•Worseninggasexchange(desats,PaO2 /FiO2 ≤ 240, ↑ O2 required or ventilation demand)
Clinical criteria for PNU1 plus 1 of the following laboratory criteria
PNU1
PNU2, PNU3
•Hemoptysisorpleuritic chest pain
•Matchingculturesofblood and sputum for Candida spp
•BAL/PSBforPneumocystis carinii or fungi
•Directmicroscopicexamination or culture
•AnyofthePNU2laboratory criteria
PNU3 (immuno- compromised patients)
•Bloodculturenotrelatedto another infection
•Pleuralfluidculture•Quantitativeculture
from BAL/PSB •≥5% intracellular
organisms in BAL cells •Histology(1offollowing) - Abscess formation
or consolidation with intense PMN accumulation
- Positive quantitative culture
- Fungal invasion of parenchyma
PNU2 (bacterial or fungal pathogens)
•Cultureofrespiratorysecretions (virus or Chlamydia)
•ViralAg/Abinsecretions•4-foldriseofpathogenIgG•PCR(Chlamydia or
Mycoplasma)•Micro-IFtest(Chlamydia)• Legionella - Positive culture or micro-
IF test from respiratory secretions or tissue
- Serogroup 1 Ag in urine (RIA/EIA)
- 4-fold rise (to ≥1:128) of L. pneumophila Ab (indirect IFA)
PNU2 (viral or uncommon pathogens)
43
Table 11. Threshold values for cultured specimens used in the diagnosis of pneumonia4
Nonbronchoscopically obtained (blind) specimensBALProtected BAL
≥104 cfu/mL≥104 cfu/mL
*Open-lung biopsy specimens and immediate postmortem specimens obtained by transthoracic or transbronchial biopsy. cfu = colony-forming units.
Chapter 5: Therapeutic Challenges in the ICU: 75-Year-Old Female With Acute Cholecystitis
*Clinical response indicated by temperature, WBC count, chest x-ray, oxygenation, purulent sputum, hemodynamic changes, and organ function. LRT = lower respiratory tract; WBC = white blood cell.
Figure 18. American Thoracic Society (ATS) guidelines for initial management of HAP, VAP, and HCAP.5
Clinical improvement at 48-72 hours
Search for other pathogens,
complications, diagnoses, or sites
of infection
Cultures –
Adjust antibiotic therapy; same measures as shown in the
box at left
Cultures +
Consider stopping antibiotics
Cultures –
De-escalate antibiotics; if possible, treat select patients
for 7-8 days
Cultures +
HAP, VAP, or HCAP suspected
Obtain LRT sample for culture microscopy
Days 2 and 3: Check cultures and assess clinical response*
Unless there is both low clinical suspicion for pneumonia and negative microscopy of LRT sample, begin antimicrobial therapy
NO YES
44
SERIOUS INFECTIONS in the Critical Care Setting
References1. Chastre J, Wolff M, Fagon J-Y, et al, for the PneumA Trial Group. Comparison of 8 vs
15 days of antibiotic therapy for ventilator-associated pneumonia in adults: a randomized trial. JAMA. 2003;290:2588-2598.
2. Pugh RJ, Cooke RP, Dempsey G. Short course antibiotic therapy for Gram-negative hospital-acquired pneumonia in the critically ill. J Hosp Infect. 2010;74:337-343.
3. Kollef KE, Schramm GE, Wills AR, Reichley RM, Micek ST, Kollef MH. Predictors of 30-day mortality and hospital costs in patients with ventilator-associated pneumonia attributed to potentially antibiotic-resistant gram-negative bacteria. Chest. 2008;134:281-287.
4. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36:309-332.
5. American Thoracic Society/Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388-416.
45
Download this and additional tools at
Chapter 6: Therapeutic Challenges in the ICU: 68-Year-Old Male With Recurrent Abdominal PainIra Leviton, MD
• PatientpresentstotheEmergencyRoomwithabdominal pain, diarrhea, sweating, and weakness, with onset the previous evening
• Historyofdiverticulosis,diverticulitis,type2diabetes,hyperlipidemia, and coronary artery disease
• Medicationsincludeamlodipine,aspirin,exenatide,glimepiride,metoprolol, and simvastatin
This patient’s history is notable for a diagnosis of diverticulitis following an episode of abdominal pain and diarrhea requiring hospitalization 1 year ago. Since then he had three more episodes with similar symptoms. He was given a 7-day postdischarge course of antibiotics each time.
He is also at high cardiovascular risk, having suffered a myocardial infarction 3 years previously.
COMMENTARY
Video Commentary Available at IDClinician.com/cecompendium
The patient is awake but able to give only 1- or 2-word responses to questions or pay attention for more than 5 to 10 seconds. He is also too weak to get out of bed.
Initial clinical impressions are very important in the diagnostic work-up for potential IAI. This patient’s history of diverticulitis leads us to suspect that the initial locus of the problem was in the colon. He is delirious, which suggests a systemic rather than localized infection.
Since sepsis is suspected, intravenous fluid therapy should be started in preparation for anticipated surgery.
COMMENTARY
His white blood cell count is very high, confirming the presence of infection. An elevated creatinine indicates acute renal insufficiency. This patient has severe sepsis.
COMMENTARY
47
Chapter 6: Therapeutic Challenges in the ICU: 68-Year-Old Male With Recurrent Abdominal Pain
Issues for selection of empiric antibiotic therapy
• Nonspecificbowelgaspattern,withgasandstoolpresent in rectum
• Noevidenceofobstructionorperforation
This decision has to be made rapidly (Figure 19, Table 12). Indeed, in sepsis cases any delay can prove fatal. Decisions regarding antibiotic therapy, fluid resuscitation, and imaging tests have to be made more or less simultaneously.In general, the most common pathogens implicated in IAIs are Gram-negative rods such as E. coli, Klebsiella spp, and Proteus mirabilis, anaerobes such as Bacteroides fragilis, and Gram-positive organisms such as Enterococci spp. Reasonable choices for the patient’s infection include any of the following:• Cefoxitin• Piperacillin-tazobactam• Ceftriaxoneplusmetronidazole• AcarbapenemHowever, when selecting antibiotic therapy, remember that all micro-biology is local. Knowledge of your hospital’s antibiogram is critical to success, since in severe sepsis there is no room for error in the selection of empiric therapy. With regard to dosing, the patient’s renal insufficiency and the potential for interactions with his cardiovascular and antidiabetic medications should be considered.
COMMENTARY
In general, CT is the preferred imaging technology.1 Since CT technology may not be available at all hours in some hospitals, an x-ray can provide important information quickly—for example, a perforation with free intraperitoneal air, or gas, or feces in the colon. However, subsequent CT imaging should be considered, as it can provide information that can help guide surgery.
COMMENTARY
48
SERIOUS INFECTIONS in the Critical Care Setting
Figure 19. CDC/NHSN algorithm for diagnosis of intra-abdominal infection.2
Patient must meet at least 1 of the following clinical criteria:•Organismsculturedfrompurulentmaterialfromintra-abdominalspaceobtained
during a surgical operation of needle aspiration
•Abscessorotherevidenceofintra-abdominalinfectionseenduringasurgicaloperation or histopathologic examination
•Atleast2ofthefollowingsigns/symptomswithnootherrecognizedcause:fever(>38oC), nausea, vomiting, abdominal pain, or jaundice, and at least 1 of the following:
– Organisms cultured from surgically placed drain
– Organisms seen on Gram’s stain of drainage or tissue
– Organisms cultured from blood and radiographic evidence of infection
Table 12. Surgical Infection Society (SIS)/Infectious Diseases Society of America (IDSA) recommendations for empiric antimicrobial therapy for healthcare-associated complicated intra-abdominal infection.1
Organisms seen in healthcare–associated infection at the local institution
Regimen
Carb
apen
ema
Pipe
raci
llin-
tazo
bact
am
Cefta
zidim
e or
ce
fepi
me,
eac
h w
ith m
etro
nida
zole
Amin
ogly
cosi
de
Vanc
omyc
in
<20% Resistant P. aeruginosa, ESBL-producing Enterobacteriaceae, Acinetobacter, or other MDR GNB
R R R NR NR
ESBL-producing Enterobacteriaceae R R NR R NR
P. aeruginosa >20% resistant to ceftazidime
R R NR R NR
MRSA NR NR NR NR R
ESBL = extended-spectrum b-lactamase; GNB = Gram-negative bacilli; MDR = multidrug resistant; MRSA = methicillin-resistant Staphylococcus aureus; NR = not recommended; R = recommended.
“Recommended” indicates that the listed agent or class is recommended for empiric use, before culture and susceptibility data are available, at institutions that encounter these isolates from other healthcare–associated infections. These may be unit- or hospital-specific.aImipenem-cilastatin, meropenem, or doripenem.
49
Chapter 6: Therapeutic Challenges in the ICU: 68-Year-Old Male With Recurrent Abdominal Pain
References1. Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of
complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis. 2010;50:133-164.
2. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36:309-332.