56
Hypertensive Disorders in Pregnancy New Y ork State Department of Health May 2013 GUIDELINE SUMMARY
| Date post: | 03-Apr-2018 |
| Category: |
Documents |
| Upload: | maria-alejandra-guzman-quijada |
| View: | 229 times |
| Download: | 0 times |

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 1/56
HypertensiveDisorders
in Pregnancy
New York State Department of Health
May 2013
GUIDELINE SUMMARY

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 2/56

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 3/56
Contents
1. Background 5Introduction 5Purpose 5Process 6
2. Defnitions and stratifcation o hypertension in pregnancy 7a. Hypertension 7 b. Severe hypertension 8
3. Blood pressure measurement technique 9
4. Classifcation o Hypertensive Disorders in Pregnancy (HDP) 10a. Recommendation or classi cation 10b. Chronic (preexisting) hypertension 10c. Gestational Hypertension 11d. Preeclampsia and chronic (preexisting) hypertension with superimposed preeclampsia 11e. Signi cant proteinuria in pregnancy 13
. Severe preeclampsia 14g. Eclampsia 14h. HELLP syndrome 15
5. Assessment o HDP 15a. Assessment o risk or preeclampsia 15b. Assessment or presence/absence o preeclampsia 16c. Assessment o proteinuria 16d. Other assessments o women at risk or preeclampsia 18e. Fetal testing or women at risk or preeclampsia 19
6. Risk reduction or preeclampsia and other complications o HDP 19a. Aspirin 19b. Other pharmaceuticals 20c. Dietary calcium supplementation 20d. Other dietary supplements 21e. Anticipatory guidance 21. Diet/li estyle 22g. Re errals or at risk 23
7. Ambulatory care o HDP 23a. Preconception/initial visit counseling and evaluation 23b. Diet 24c. Li estyle 25d. Blood pressure threshold and targets or treatment 25e. Antihypertensive agents or non-acute blood pressure management 27 . Maternal surveillance: blood pressure monitoring 29g. Maternal surveillance: laboratory testing 30h. Fetal surveillance: tests o etal well being 30i. Frequency o etal testing and monitoring 32j. Re errals/consultations 32

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 4/56
8. Inpatient prenatal care o HDP-severe hypertension and preeclampsia 33a. Indications or inpatient care 33b. Critical care 33c. Communications 34d. Bedrest 34e. Acute hypertension management 34
. Inpatient maternal surveillance 37 g. Invasive hemodynamic monitoring 38h. Fetal surveillance 38i. Delivery timing/expectant management 38j. Antenatal steroids 39
9. Inpatient care specifc to preeclampsia 39a. Severity classi cation 39b. Seizure prophylaxis 40c. Thromboprophylaxis 40d. Re erral/consultation 41
10. Eclampsia/HELLP syndrome 41a. Management o seizures in eclampsia 41b. Delivery timing eclampsia 42c. Trans usion or HELLP syndrome 42d. Other therapy or HELLP syndrome 42
11. Delivery-intrapartum care or women with HDP 43a. Mode o delivery 43b. Intrapartum 43c. Anesthesia concerns 43d. Analgesia 44e. Fluid balance 44
12. Postpartum and ollow-up 45a. Postpartum evaluation/surveillance 45b. Postpartum antihypertensive therapy 46c. Follow up review/testing 47 d. Risk communication/li estyle counseling 47
13. Continuous Quality Improvement 48
Main Re erences 50
Endnotes 51
Acknowledgements 53

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 5/56
Hypertensive Disorders in Pregnancy (HDP)
Guideline Summary
1. Background
Introduction
Hypertensive disorders in pregnancy (HDP) are associated with severe maternal obstetriccomplications and are a leading contributor to maternal mortality.1Furthermore, HDP lead topreterm delivery, etal intrauterine growth restriction, low birth weight and perinatal death.2 Although the exact incidence is unknown, it has been estimated that 5-10% o US pregnancies are
complicated by HDP.3Data rom the Nationwide Inpatient Sample o the Healthcare Cost andUtilization Project and National Hospital Discharge Survey have shown marked increases in theincidence o gestational hypertension and preeclampsia in the past two decades, and more womenentering pregnancy with chronic (preexisting) hypertension.4,5Women with chronic (preexisting)hypertension have been shown to have a markedly increased risk o severe adverse outcomes, suchas maternal cerebrovascular accidents and placental abruption, compared to normotensive women.6 Te prevalence o HDP is believed to be increasing due to obesity trends and childbearing in olderaged women.7Due to the requent occurrence and potential sequelae o hypertensive disorders inpregnancy, prompt identi cation and appropriate management are essential.
Purpose
Tis guidance document is intended or healthcare providers who care or pregnant women in a variety o clinical settings. Te aim is to promote quality services and enhance communication amongthe myriad o providers who provide health care to pregnant women, including obstetricians, amily practice physicians, emergency department physicians, midwives, anesthesiologists, nurses and others.
Tis document summarizes existing guidelines or the diagnosis, evaluation and management o hypertensive disorders in pregnancy. Tis document is not intended to replace clinical judgmentin the care o women with hypertensive disorders in pregnancy. It should be noted that diagnosticand management strategies that are not recommended speci cally or their impact on outcomes o
hypertensive disorders in pregnancy may have other general bene ts in pregnancy.
Initiatives to standardize care have been shown to improve clinical outcomes.8For hypertensionin pregnancy, the introduction and dissemination o evidence-based clinical guidelines have beenassociated with improved maternal and perinatal outcomes.9,10E ective health care delivery orcomplex conditions such as HDP depends on a well- unctioning, coordinated care team o health careproviders. Collaboration and communication among care team members is essential or success ulmanagement and reducing error.11

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 6/56
Process
In 2010, the New York State Department o Health implemented a new Maternal Mortality Review (MMR) Initiative. Te new process is completed in conjunction with Island Peer Review Organization (IPRO) and an expert committee that includes representation rom AmericanCongress o Obstetricians and Gynecologists (ACOG) and many other pro essional organizationsand experts. Te updated initiative is intended to ensure a comprehensive review o actors leadingto maternal deaths in New York State, based on su cient in ormation to develop strategies andmeasures to decrease the risk o these deaths. Te rst meeting o the expert committee included areview o preliminary 2006-2008 data on 70 maternal deaths, showing leading causes o death to be:hypertension (20%), hemorrhage (19%) and embolism (17%). Chronic illness, obesity and prenatalrisk actors were identi ed as important circumstances in the cases reviewed. Tis resulted in theidenti cation o several priorities including management o hypertension, obesity and embolism/DVor development o clinical guidelines. Management o hypertension during pregnancy was selected asthe rst topic or development. A multidisciplinary subcommittee o the Expert Review Committeeand the Department worked with IPRO and the subcommittee to develop guidelines on the diagnosis,evaluation, and management o Hypertensive Disorders in Pregnancy.
Te updated maternal mortality review initiative is consistent with the department’s priorities o improvingbirth outcomes and decreasing maternal mortality in accordance with itle V Maternal and ChildHealth Services Block Grant and the department’s prevention agenda. Maternal and in ant mortality andmorbidity are key indicators o the health o a society. Tese measures are a refection o the current healthstatus o a large segment o the population and a predictor o the health o the next generation.
E ective and error- ree health care delivery or complex conditions such as HDP depends on a well- unctioning,coordinated care team that osters collaboration and communication among care team members.12
Te process or the development o this guidance document included a review o ACOG and American Academy o Pediatrics (AAP) guidelines, practice bulletins and committee opinions; theSeventh Report o the Joint National Committee ( JNC) on Prevention, Detection, Evaluation and reatment o High Blood Pressure; the 2000 Report o the National High Blood Pressure EducationProgram (NHBPEP) Working Group on High Blood Pressure in Pregnancy; Hypertension in DiversePopulations: a New York State Medicaid Clinical Guidance Document; Institute o Medicine (IOM)guidelines; Cochrane reviews and selected literature. International guidelines reviewed included thoseo the Royal College o Obstetricians and Gynaecologists National Institute or Health and ClinicalExcellence (NICE), Society o Obstetricians and Gynaecologists o Canada (SOGC), and Society o Obstetric Medicine o Australia and New Zealand (SOMANZ), with consideration o evidence
grading included in the documents. A bibliography o documents included in the guideline comparison is attached in Appendix A.
Subsequent to guideline review and comparison, ndings were discussed by the MMR HypertensionSubcommittee and consensus statements or areas without clear evidence were de ned. Tesummary document and MMR Hypertension Subcommittee recommendations were submitted tothe Expert Review Committee and subsequently to the NYSDOH or approval and nalization o recommendations. Final recommendations areitalicized or each section in the document.
7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 7/56
2. Defnitions and stratifcation o hypertension in pregnancy
Hypertensive Disorders in Pregnancy (HDP) are comprised o a spectrum o disorders typically classi ed into categories that include chronic (preexisting) hypertension, gestational hypertension,preeclampsia (including chronic (preexisting) hypertension with superimposed preeclampsia) andeclampsia. Hypertension and preeclampsia are strati ed according to severity. Clear de nitions andseverity strati cation are essential, because they orm the basis o management recommendationsand promote accurate, e ective communication among health care providers. While there is generalconsensus across guidelines or most major de nitions, including those o the NHBPEP WorkingGroup, there are some noteworthy di erences in de nitions and criteria or severity strati cation.
a. Hypertension
Hypertension in pregnancy is de ned as a systolic blood pressure ≥ 140 OR diastolic blood pressure ≥ 90
mmHg or both. Both systolic and diastolic blood pressure elevations are important in the identi cation
o HDP. Hypertensive blood pressure readings should be con rmed using appropriate measurement
technique as described below, and should be remeasured a ter 10-15 minutes o rest.
Tere is broad agreement across guidelines that hypertension in pregnancy is de ned as a diastolicblood pressure ≥ 90 mmHg or a systolic blood pressure ≥ 140 mmHg or both. Te inclusion o systolic blood pressure elevation in the de nition o hypertension in pregnancy refects evidencethat both diastolic and systolic elevated readings have been associated with adverse outcomes suchas perinatal morbidity.13Tere ore, systolic blood pressure readings are considered as important asdiastolic readings in the identi cation o HDP.
Although the NHBPEP report and ACOG practice bulletin or preeclampsia caution that a relativerise in systolic blood pressure o 30 mmHg or diastolic relative rise o 15 mmHg warrants close
observation, there is no systematic evidence that this relative rise in blood pressure is predictive o pregnancy outcomes. Tere ore, de ning hypertension in pregnancy by a relative rise is no longerendorsed in published guidelines. In addition, relative blood pressure rise as a criterion or de ninghypertension has a high alse positive rate, especially because o the variability o blood pressure acrosstrimesters o pregnancy. Blood pressure in healthy pregnancies decreases during the rst trimester,reaching its lowest point by mid-pregnancy, and typically returns to pre-pregnancy levels during thethird trimester. In women who develop preeclampsia, the pattern di ers, with blood pressure stableor the rst hal o pregnancy and then continuously rising until delivery.14Te ACOG practicebulletin regarding chronic hypertension notes that previously undiagnosed chronic (preexisting)hypertension may be masked by the normal decrease in blood pressure in women presenting or care
a ter 12 weeks gestation.15Elevated blood pressure readings should be con rmed, and should be remeasured a ter 15 minutes o rest. Te ACOG committee opinion Emergent Terapy or Acute Onset, Severe Hypertension withPreeclampsia or Eclampsia indicates that acute onset, severe hypertension that persists or 15 minutesor more is considered a hypertensive emergency,16and SOGC guidelines cite expert consensus thatsevere hypertension should be con rmed with remeasurement in 15 minutes.17

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 8/56
Te ACOG practice bulletin Chronic Hypertension in Pregnancy recommends documentation o blood pressure levels that meet criteria or hypertension on more than one occasion, at least 4 to6 hours apart. SOGC guidelines also recommend basing the identi cation o hypertension on anaverage o two readings more than 4 hours apart or non-severe hypertension, noting high rates o normal readings on subsequent measurements, which is consistent with NYSDOH recommendations
or diverse populations.18When con rming elevated blood pressure readings, blood pressure shouldbe measured in both arms and appropriate measurement technique as described below should beensured. Tere is greater variation in systolic than diastolic blood pressure.
In the setting o pregnancy, SOMANZ guidelines cite reports that isolated o ce hypertension, or“white coat hypertension,” con ers some risk o adverse outcomes, and there ore women with isolatedo ce hypertension warrant monitoring. Ascribing a hypertensive blood pressure reading to “white coathypertension” in pregnant women is discouraged. Women with isolated hypertensive blood pressurereadings should be urther evaluated with determination o risk or HDP, including consideration o conditions that con er risk, such as obesity and lupus, as well as assessment o proteinuria.
b. Severe hypertension
Severe hypertension in pregnancy is de ned as systolic blood pressure ≥160 mmHg or diastolic blood
pressure ≥110 mmHg, or both. The SOGC expert consensus suggests that a single reading at this level
be con rmed within 15 minutes. Severe hypertension in pregnancy is considered to be a hypertensive
emergency that requires urgent intervention. The ACOG Committee Opinion “Emergent Therapy
or Acute Onset, Severe Hyper tension with Preeclampsia or Eclampsia” recommends that severe
hypertension that persists or 15 minutes or more in the setting o preeclampsia or eclampsia is a
hypertensive emergency that requires immediate intervention. 19
Although de nitive evidence is lacking or a threshold blood pressure to de ne severe hypertension,there is consensus across most guidelines that severe hypertension is de ned as a systolic bloodpressure ≥ 160 mmHg or diastolic blood pressure ≥ 110 mmHg, or both. Women with con rmedblood pressure readings consistent with severe hypertension require immediate intervention. Te ACOG Committee Opinion “Emergent Terapy or Acute Onset, Severe Hypertension withPreeclampsia or Eclampsia” recommends that severe hypertension that persists or 15 minutes ormore in the setting o preeclampsia or eclampsia is a hypertensive emergency that requires immediateintervention. Te immediate goal o management o severe hypertension in pregnant women ispredominantly related to maternal sa ety, such as the prevention o stroke, rather than the preventiono the long term sequelae o hypertension. Tere is evidence that cerebral autoregulation is alteredin severe preeclampsia and eclampsia, and there ore acute intervention thresholds based on cerebralautoregulation studied in other populations may not be applicable.20Tere have been reports o strokeassociated with elevated systolic blood pressure without elevated diastolic blood pressure in women with severe preeclampsia.21Te prevailing de nition o severe hypertension is based on air evidencethat there is an increased risk o stroke in pregnancy with systolic blood pressure readings ≥ 160mmHg, although there is no de nitive evidence or any discrete threshold.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 9/56
3. Blood pressure measurement technique
Appropriate blood pressure measurement technique is essential or identi ying and monitoring HDP.
Blood pressure is highly variable within subjects; appropriate care must be taken to standardize practice
in order to minimize various actors that a ect clinic blood pressure measurement, especially choice o
cu size, degree o stimulation, posture, and talking.
Ca eine and tobacco should be avoided or at least 30 minutes prior to measurement. Ideally, prior to
blood pressure measurement, the patient should be undisturbed and at rest or at least 5 minutes, in a
quiet room i possible. Neither the patient nor the trained observer should talk during the measurement
itsel . Blood pressure should be measured with the patient sitting in a chair with eet at on the oor
and back supported. I upright sitting posture is not possible, blood pressure should be measured in the
le t, lateral recumbent position, and it should be recognized that blood pressure will be reduced by a
ew mmHg i taken in the ree arm. The blood pressure cu should be appropriate in size such that the
in atable bladder covers 75%-100% o the circum erence o the upper arm.
Blood pressure should be measured in both arms at the initial visit ideally, with the higher valuetaken as the blood pressure o record and that arm noted in the record as the basis or all subsequent
determinations.
Diastolic readings should re ect Korotko phase V readings (disappearance o tones), i blood pressure is
measured with a manual device. Semi-automated oscillometric devices should be checked periodically
or accuracy. Ofce BP remains the gold standard or detection o HDP despite the increasing use o
non-ofce BP values (sel -determined home blood pressure and 24-hour ambulatory) in non-pregnant
individuals with hypertension. Observational studies have shown that sel -determined home blood
pressure and 24-hour ambulatory blood pressure monitoring may be use ul in the identi cation and
surveillance o HDP. Ambulatory blood pressure monitors are ully automatic and are capable o
recording blood pressure or 24 hours or longer while patients conduct their normal daily activities.
Tere are several general recommendations or blood pressure measurement technique in pregnant women that are consistent with recommendations or the general population as outlined by the JNC and NYSDOH Medicaid documents. Tere is consensus across HDP guidelines that bloodpressure should be measured with women seated and upright, when possible. I upright posture is notpossible, blood pressure should be measured in the le t lateral recumbent position, though it should berecognized that modestly lower blood pressure readings can result in this position, because the rightarm is usually elevated above heart level. Standard technique requires that the patient rest undisturbed,not talking, or 5 to 10 minutes with eet on the foor and back supported. Ca eine and tobaccoshould be avoided or at least 30 minutes prior to blood pressure measurement. It is critical that ablood pressure cu size appropriate to patient size be used to ensure accurate readings. Blood pressureshould be measured with a cu with a cu bladder that encircles 75-100% o the upper arm, with thecu midpoint and the arm at the level o the heart. Diastolic readings should refect Korotko phase V readings (disappearance o tones), i blood pressure is measured with a manual device.
Although automated oscillometric blood pressure readings can reduce operator error, and are now most commonly used, automated and aneuroid devices require periodic validation against mercury

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 10/56

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 11/56
(preexisting) hypertension who have evidence o target organ damage in management considerations,though not speci cally de ned as a subgroup. ACOG notes that the incidence o adverse pregnancy outcomes appears to be related to the duration o chronic (preexisting) hypertension, which is likely aproxy or end-organ damage.
c. Gestational Hypertension
Gestational hypertension is de ned as new hypertension (systolic blood pressure ≥ 140 mmHg or
diastolic blood pressure ≥ 90 mmHg or both) presenting at or a ter 20 weeks gestation without
proteinuria or other eatures o preeclampsia; this terminology replaces the term “Pregnancy Induced
Hypertension.”
Gestational hypertension is de ned as new hypertension presenting a ter 20 weeks gestation withoutproteinuria or other eatures o preeclampsia; this terminology replaces the term Pregnancy InducedHypertension (PIH) that was widely used in older guidelines and literature.
d. Preeclampsia and chronic (preexisting) hypertension with superimposed preeclampsia
Preeclampsia is de ned as hypertension plus signi cant proteinuria, speci cally gestational hypertension
plus new onset proteinuria, or chronic (preexisting) hypertension with new or worsening proteinuria. When
preeclampsia develops in women with chronic (preexisting) hypertension, the classi cation o disease is
chronic (preexisting) hypertension with superimposed preeclampsia. Preeclampsia can also occur without
proteinuria, with hepatic, hematopoietic, or other mani estations. Edema is no longer considered a speci c
diagnostic criterion or preeclampsia. Pregnant women with hypertension plus other adverse conditions
but no proteinuria should have urther evaluation or preeclampsia.
Early identi cation and management is essential or preeclampsia, which is characterized by acomplex group o multi-organ processes and variable presentation. raditionally, preeclampsia hasbeen de ned as hypertension plus signi cant proteinuria. Women with gestational hypertensionplus new onset o 300 mg or more o urinary protein in a 24 hour period are classi ed as havingpreeclampsia. Women with chronic (preexisting) hypertension with new or worsening proteinuriaare classi ed as having chronic (preexisting) hypertension with superimposed preeclampsia. Tisde nition, which is cited in ACOG and JNC documents based on the NHBPEP Working Groupde nition, is typically used in research protocols, and there ore refects the characteristics o pregnant women who comprise the study population in most published studies o preeclampsia. In addition,this traditional de nition o preeclampsia is based on the most common maternal mani estations o preeclampsia: hypertension and proteinuria. Up to 30% or more o women with chronic (preexisting)
hypertension or gestational hypertension also develop preeclampsia. Women with mild chronic(preexisting) hypertension have a 20% risk o developing superimposed preeclampsia, and those withsevere chronic (preexisting) hypertension have a 50% risk o superimposed preeclampsia. Women with chronic (preexisting) hypertension and end-organ disease, severe hypertension or secondary hypertension are at greatest risk or superimposed preeclampsia.23
Te development o new proteinuria or sudden increase over baseline proteinuria should triggeran assessment or superimposed preeclampsia in women with chronic (preexisting) hypertension.
7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 12/56
JNC guidelines de ne worsening proteinuria in women with chronic (preexisting) hypertension as asudden, 2-3 old increase in proteinuria.
Preeclampsia can also occur without proteinuria, and mani est as hypertension plus other adverseconditions, refecting the multi-organ processes that characterize this disorder. SOGC and SOMANZguidelines de ne preeclampsia as hypertension with proteinuria or other adverse conditions, since thereis evidence that end-organ complications can occur without proteinuria. It has been reported that upto 20% o women with eclampsia have hypertension without proteinuria in the week preceding theonset o eclampsia.24Te de nition or preeclampsia in the ACOG preeclampsia practice bulletin andNHBPEP Working Group report speci y proteinuria as a required element. Te NHBPEP WorkingGroup report notes that preeclampsia should be suspected even without proteinuria in the presenceo other adverse conditions. Te ACOG practice bulletin or chronic hypertension in pregnancy indicates that women with chronic (preexisting) hypertension who develop abnormal laboratory valuesor clinical symptoms such as headache, right upper quadrant pain or an increase in blood pressure warrant consideration o superimposed preeclampsia. For women presenting with hypertension withadverse conditions but without proteinuria, a diagnosis o preeclampsia should be entertained toensure identi cation o women at risk; however, the diagnosis would be uncertain and would requireurther investigation and consideration o other possible conditions that the signs and symptomsmay represent. In cases identi ed as suspected preeclampsia in the absence o proteinuria, medicalsubspecialty or maternal- etal medicine consultation should be considered.
Tere are various adverse conditions identi ed across SOGC, SOMANZ, JNC and ACOGguidelines as criteria that should raise suspicion or preeclampsia in the absence o proteinuria. Severalo the identi ed conditions also comprise criteria or severe preeclampsia in these guidelines. Adverseconditions included in the consideration o preeclampsia center on maternal end-organ dys unction,maternal symptomatology, abnormal maternal laboratory testing and evidence o etal morbidity.
Adverse conditions that are refective o maternal end-organ dys unction include eclampsia, pulmonary edema, stroke, placental abruption and severe hypertension. For women with chronic (preexisting)hypertension, SOGC guideline-cited adverse conditions include resistant hypertension, de ned ashypertension requiring three medications or blood pressure control a ter 20 weeks gestation.
Maternal symptoms that guidelines identi y as adverse conditions that raise suspicion orpreeclampsia are generally not speci c or preeclampsia. Tese symptom-based adverse conditionsinclude symptoms that may refect occipital cortical or other cerebral ischemia or edema (severeheadache, visual disturbance), hepatic capsular irritation (epigastric or right upper quadrant pain) orpulmonary edema (dyspnea). Other maternal symptoms cited as adverse conditions that could raise
suspicion or preeclampsia include severe nausea and vomiting and chest pain. SOGC guidelinesspeci cally note that adverse conditions di er in signi cance, and that maternal symptoms suchas headache do not have the same weight as signs o maternal end-organ dys unction such as themani estation o eclampsia.
Abnormal maternal laboratory testing refecting end-organ dys unction includes elevated liver enzymesand thrombocytopenia, which are cited by SOGC, JNC, ACOG and SOMANZ guidelines as possiblemani estations o preeclampsia. SOGC guidelines also cite elevated serum creatinine and serum

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 13/56
albumin less than 2.0 g/dl, which SOGC guidelines indicate has been associated with an increased risk o pulmonary edema and other complications. SOGC guidelines note that hyperuricemia has beenassociated with perinatal complications, but there is no evidence that it is predictive o adverse maternaloutcomes, and it has there ore not been included as laboratory evidence o adverse conditions.
Signs o etal morbidity are included as adverse conditions in both SOGC and SOMANZ guidelinesand include oligohydramnios, intrauterine growth restriction, abnormal Doppler umbilical artery velocimetry and intrauterine etal death. As diagnostic criteria have evolved over the past decade,edema is no longer cited as a required criterion or preeclampsia in guidelines, since there is evidencethat edema is neither a sensitive nor speci c indicator or preeclampsia.25Te absence o edema doesnot exclude a diagnosis o preeclampsia.
e. Signi cant proteinuria in pregnancy
In the context o identi cation o preeclampsia, signi cant proteinuria is present when 24 hour urine
protein is equal to or exceeds 300 mg o protein. The spot urine protein: creatinine ratio has also been
used to de ne signi cant proteinuria in the identi cation o preeclampsia. The ACOG practice bulletin“Chronic Hypertension in Pregnancy” notes that a protein : creatinine ratio in the range o 0.15 to 0 .3 g
protein/g creatinine has been used to identi y women who should be urther evaluated. 26The SOGC and
the National Collaborating Centre or Women’s and Children’s Health, National Institute or Health and
Clinical Excellence (NICE) identi y signi cant proteinuria as a protein: creatinine ratio o ≥30 mg protein/
mmol creatinine. 27
Signi cant proteinuria is de ned across guidelines as greater than or equal to 300 mg o protein in a24 hour urine collection. Te ACOG practice bulletin Chronic Hypertension in Pregnancy identi esa spot urine protein: creatinine ratio in the range o 0.15 to 0.3 g protein/g creatinine as an indicatorthat has been used to identi y pregnant women who warrant urther evaluation, but notes that there hasnot been consensus on the best cuto value. Other guidelines (SOGC and NICE) identi y a spot urineprotein: creatinine ratio o ≥ 30 mg protein/mmol creatinine as signi cant proteinuria in the context o identi ying preeclampsia among pregnant women. Morris et al., in a systematic review and meta-analysiso diagnostic accuracy o spot urinary protein and albumin to creatinine ratios in suspected preeclampsiaound that the optimum threshold (maximal sensitivity and speci city) or signi cant proteinuria in theidenti cation o preeclampsia was a protein: creatinine ratio in the range o 0.30 and 0.35.28
“Proteinuria”, a term that is commonly used in medical practice, is not ully interchangeable with“albuminuria.” otal urinary protein includes globulins and other substances and is there ore higherin amount than urinary albumin excretion. It is the abnormal ltration o albumin that de nes
the presence o any glomerulopathy. Accordingly, standards have been established by the NationalKidney Foundation KDOQI guidelines such that albuminuria in women is de ned as urinary albumin excretion >300 mg/day or >355 mg/g creatinine.29SOGC guidelines note that moreevidence is needed regarding the clinical use o urinary albumin: creatinine ratio (ACR) in identi yingpreeclampsia among women at risk. Morris et al. in their systematic review, concluded that there wasinsu cient evidence or the clinical use o ACR in diagnosis o suspected preeclampsia; meta-analysis was not possible due to di ering thresholds and characteristics across studies.30

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 14/56
. Severe preeclampsia
ACOG parameters should be used to de ne severe preeclampsia; ACOG criteria or severe preeclampsia
include the presence o any one o the ollowing: severe hypertension (systolic blood pressure ≥ 160
mmHg or diastolic blood pressure ≥ 110 mmHg, or both), cerebral or visual disturbance, epigastric
or right upper quadrant pain, oliguria, pulmonary edema, cyanosis, impaired liver unction,
thrombocytopenia or intrauterine growth restriction (IUGR).
It is important to identi y severe preeclampsia, since crucial management decisions such as seizureprophylaxis depend on severity strati cation. ACOG parameters should be used to de ne severepreeclampsia; these parameters overlap adverse conditions noted in guidelines or the identi cationo preeclampsia in the absence o proteinuria. ACOG criteria or severe preeclampsia includematernal symptoms (cerebral or visual disturbance, epigastric or right upper quadrant pain), evidenceo maternal end-organ complications (severe hypertension, oliguria, pulmonary edema or cyanosis),abnormal maternal laboratory tests (impaired liver unction, thrombocytopenia) and etal morbidity (intrauterine growth restriction).
Tere is no strong evidence or a de ned cuto point or the prognostic value o degrees o proteinuria, and quanti cation has not proven use ul or prognostic determinations; however, thereis evidence that the risk or adverse outcome increases as proteinuria increases.31Several guidelinesinclude the degree o proteinuria in the de nition o severe preeclampsia, including the ACOGpreeclampsia practice bulletin that cites proteinuria o 5 grams or more in a 24 hour urine sample andSGOC guidelines, which include “heavy” proteinuria o 3-5 grams/day despite an acknowledgemento the lack o clear evidence.
Although ACOG does not include the early onset o preeclampsia in its de nition o severepreeclampsia, SOGC guidelines include the onset o preeclampsia prior to 34 weeks gestation as a
marker o severe preeclampsia. Recent evidence has suggested that early and late preeclampsia shouldbe di erentiated, since onset prior to 34 weeks gestation is associated with more severe disease,perhaps due to etiological di erences between early and late onset preeclampsia.32Early onsetpreeclampsia is postulated to be mediated by placental actors with resultant adverse outcomes, withlate onset more likely associated with maternal actors such as obesity and perhaps with outcomesthat are less severe.33Although there is no de nitive evidence to support this approach, health careproviders may want to consider hospitalizing women presenting with suspected preeclampsia at lessthan 34 weeks gestation or monitoring.
g. Eclampsia
Eclampsia is de ned as new onset grand mal seizures in women with preeclampsia. Some women
presenting with eclampsia do not have diagnosed preeclampsia, and some women may present with
eclampsia in the post-partum period.
Eclampsia and HELLP syndrome are two severe conditions that can mani est in women withpreeclampsia, and each triggers distinct management considerations. Eclampsia is de ned as new onset grand mal seizures in women with preeclampsia. Eclampsia may mani est in women with

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 15/56
preeclampsia post partum, but ACOG guidelines note that other causes may be more likely i seizuresoccur beyond 48-72 hours postpartum.
h. HELLP syndrome
HELLP syndrome is a serious systemic disorder associated with preeclampsia and mani ested by
hemolysis, elevated liver enzymes and a low platelet count.
HELLP syndrome mani ests with hemolysis, elevated liver enzymes and a low platelet count.HELLP syndrome can mani est with or without proteinuria. HELLP syndrome has been noted tooccur in approximately 20% o women with severe preeclampsia, as noted in the ACOG preeclampsiapractice bulletin.
5. Assessment o HDP
Assessment o HDP includes assessment o the risk or preeclampsia, the severity o preeclampsia, and the
presence o additional relevant ndings, including identi able causes o hypertension or kidney disease.
a. Assessment o risk or preeclampsia
Various conditions predispose to preeclampsia, including chronic (preexisting) hypertension, previous
preeclampsia, autoimmune disease/antiphospholipid antibodies, chronic kidney disease, and
preexisting diabetes mellitus. Women with these conditions are considered to be at high risk or HDP.
Other actors that increase the risk or HDP include, but are not limited to, multi etal pregnancy, elevated
pre-pregnancy Body Mass Index (BMI), maternal age ≥ 40, nulliparity, vascular and connective tissue
disease, amily history o preeclampsia, thrombophilia and interpregnancy interval o greater than 10
years. Black race has also been associated with increased risk or preeclampsia. Consideration should be
given to risk actors or preeclampsia when developing surveillance and monitoring strategies, including
visit requency.
Tere has been substantial study in the past decade regarding the identi cation o risk actors orpreeclampsia, since early identi cation o women at risk is essential or prevention and or reducingthe risk o some preeclampsia-associated complications.34,35Risk actors cited in guidelines refectetiological theories, including abnormal trophoblastic invasion, infammatory and immune responseand genetics. In addition to recommendations or prophylaxis, the nature o maternal testing or thepresence o preeclampsia, such as proteinuria, is also guided by the degree o risk.
Tere are several risk actors or preeclampsia that are commonly cited across guidelines to identi y women at risk; these include actors that con er high risk and actors that con er moderate risk. Tereis consensus that chronic (preexisting) hypertension, previous preeclampsia, autoimmune disease/antiphospholipid antibodies, chronic kidney disease, and preexisting diabetes mellitus all con er highrisk or preeclampsia, increasing the relative risk o developing preeclampsia two to our old.36
Moderate risk actors or preeclampsia or which there is consensus across guidelines include vasculardisease, thrombophilia, rst pregnancy, older age (most o ten de ned as ≥ age 40 years, ACOG

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 16/56
de ned as ≥ 35 years), multi etal pregnancy and obesity (de ned variably across guidelines). Family history o preeclampsia is also commonly cited, refecting a theory o genetic predisposition, as isinterpregnancy interval o greater than 10 years.
Some o the guidelines also include race/ethnicity (Black race in ACOG and SOGC guidelines),low socioeconomic status, increased triglycerides pre-pregnancy, amily history o early onset o cardiovascular disease, cocaine or methamphetamine use, interpregnancy interval less than 2 years,assisted reproductive technology, excessive weight gain and in ections such as urinary tract in ectionor periodontal in ection. I multiple moderate risk actors are present, they should be considered inplanning or maternal monitoring and proteinuria testing.
SOGC and NICE guidelines cite air evidence that women with onset o gestational hypertensionprior to 34 weeks gestation are more likely to develop preeclampsia than women with later onsethypertension, and that these women have an increased risk o complications such as IUGR. Tisevidence is consistent with the distinction between early and late presenting disease that has beenrecently considered.
Tere are several investigational laboratory markers or risk o preeclampsia, such as leptin, placentalgrowth actor and plasminogen activator inhibitor, which have not been shown individually to havesu cient predictive value to be clinically use ul.
b. Assessment or presence/absence o preeclampsia
All women diagnosed with hypertension in pregnancy should be assessed or the presence or absence
o preeclampsia. Women with high risk or preeclampsia should have more de nitive evaluation o
proteinuria than women at low risk, and high-risk women should be evaluated or preeclampsia through
other clinical and laboratory evaluations.
All women diagnosed with hypertension in pregnancy should be assessed or the presence or absenceo preeclampsia. Many women with HDP will develop preeclampsia, and the JNC report notes thatup to 25% o women with chronic (preexisting) hypertension will develop preeclampsia. Women withsevere hypertension should be care ully monitored or the development o preeclampsia. Women with high risk or preeclampsia should have more de nitive evaluation o proteinuria than women atlow risk, and high-risk women should also be evaluated or preeclampsia through other clinical andlaboratory evaluations as discussed below.
c. Assessment o proteinuria
Proteinuria testing is a priority area or the identi cation and management o HDP. All women should have standard dipstick screening or proteinuria at each prenatal visit. Women diagnosed with
hypertension in pregnancy and other women at high risk or preeclampsia should have more de nitive
evaluation o proteinuria than women at low risk, with either 24-hour urine collection or protein or spot
urinary protein: creatinine ratio to quanti y the amount o proteinuria.
Tough it is widely accepted that all pregnant women should be assessed or proteinuria, the currentevidence or recommending speci c measurement methods and thresholds to identi y women at risk

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 17/56
or complications is o poor quality. For low-risk women with low suspicion o preeclampsia, standarddipstick screening is logistically easy and inexpensive. Automated reagent-strip reading devices canenhance the per ormance o dipstick screening, and several studies have noted superior sensitivity andspeci city o automated reagent-strip reading devices relative to visual strip readings.37I a screeningstandard dipstick reading is 1+ or more, urther testing or proteinuria should be undertaken, since
a standard dipstick reading o 1+ is correlated with 0.3 g or more in a 24 hour urine but requirescon rmation. 38Further testing or a positive screening result should be conducted and could include aspot urinary protein: creatinine ratio or 24-hour urine collection to quanti y the amount o proteinuria.
All women diagnosed with hypertension in pregnancy should be assessed or the presence orabsence o preeclampsia, including de nitive assessment or proteinuria. Women with risk actors orpreeclampsia should also undergo de nitive testing or proteinuria, since the use ulness o dipstick screening in women with hypertension or other increased risk or preeclampsia is unclear romcurrent evidence.39Tere is good evidence to recommend more de nitive testing with either a spoturinary protein: creatinine ratio or 24-hour urine collection i there is a suspicion o preeclampsia,although there is no de nitive evidence or which method is best to identi y women at risk orcomplications. Te ACOG practice bulletin Chronic Hypertension in Pregnancy identi es the 24-hour urine collection as the pre erred method or quanti ying proteinuria. While a 24-hour urinecollection or protein is o ten the gold standard to which other tests are compared, samples are o tenincomplete and logistically di cult to collect. SOGC guidelines note that the National Kidney Foundation avors spot urine samples over 24-hour urine collections or quanti ying proteinuria dueto these logistical issues. I a 24-hour urine collection is the testing method chosen, a recognizedmethod o evaluating completeness o the sample should be used. o veri y appropriate collection, ACOG recommends that measurement o creatinine is included to ensure excretion is in the rangeo 10-15 mg/kg. SOGC guidelines note that the use o urinary albumin: creatinine ratio (ACR)to identi y signi cant proteinuria in assessing or preeclampsia has been reported, but that more
in ormation is needed regarding the clinical use o ACR in this context. Morris et al. also concludedin a systematic review that there was insu cient evidence available regarding the diagnostic useo ACR in suspected preeclampsia; meta-analysis o ACR was not possible in this review due todi ering thresholds and characteristics across studies.40
Signi cant proteinuria or the identi cation o preeclampsia is de ned across guidelines as greaterthan or equal to 300 mg o protein in a 24 hour urine collection. Te ACOG practice bulletinregarding chronic hypertension notes that although protein: creatinine ratios o .15 to .3 have beenused to identi y women who should be evaluated with a 24 hour urine or proteinuria, there is noconsensus or the best cuto value.
Standards have been established by the National Kidney Foundation KDOQI guidelines suchthat albuminuria in women is de ned as urinary albumin excretion >300 mg/day or >355 mg/gcreatinine. Microalbuminuria, 30-300 mg albumin/day or ACR o 30-300 mg albumin/g creatinine(American Diabetes Association cuto ), is also a known marker o incipient renal disease.41Evidenceor the use o albumin: creatinine ratio in identi ying preeclampsia has been limited, and di erentthresholds have been used across studies.42SOGC guidelines cite insu cient evidence or a speci crecommendation regarding the clinical use o urinary ACR in the identi cation o preeclampsia.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 18/56
d. Other assessments o women at risk or preeclampsia
Baseline renal unction assessment, including serum creatinine, blood urea nitrogen and 24-hour
urinary protein or spot urine or protein: creatinine ratio, is recommended or all pregnant women with
chronic (preexisting) hypertension. Most guidelines recommend additional laboratory testing or women
at risk or preeclampsia, including but not limited to complete blood count, platelet count, aspartate
aminotrans erase (AST), alanine aminotrans erase (ALT), lactate dehydrogenase (LDH), bilirubin and
serum uric acid. Uterine Doppler velocimetry is not recommended in the assessment o women at low
risk or preeclampsia.
In addition to speci c testing or proteinuria, SOGC and SOMANZ guidelines recommend that women with risk actors should receive a strati ed clinical and lab evaluation work-up beyond routinebaseline antenatal lab tests; this recommendation is based on air evidence. Such testing or womenat risk would include complete blood count and di erential, blood lm, platelet count, coagulationstudies, serum creatinine, glucose, liver enzymes, and serum albumin. SOGC guidelines include uricacid in testing or women at risk due to a reported association o elevated uric acid and perinatal
complications. Te ACOG practice bulletin Chronic Hypertension in Pregnancy notes that serumuric acid may be help ul in diagnosing superimposed preeclampsia.
Te ACOG practice bulletin Chronic Hypertension in Pregnancy recommends evaluation or end-organ damage in women with chronic (preexisting) hypertension, based on consensus and expertopinion, since women with end-organ damage are at increased risk or adverse outcomes. Evaluationdepends on severity, but could include assessment o renal unction, electrocardiography andophthalmologic evaluation. ACOG recommends baseline renal assessment or all pregnant women with chronic (preexisting) hypertension, including serum creatinine, blood urea nitrogen, creatinineclearance and 24-hour urinary protein or spot urine or protein: creatinine ratio.
ACOG and SOGC guidelines recommend consideration o an evaluation o secondary causes in women with chronic (preexisting) hypertension, with only a basic workup or secondary causes i suspicion is low. Te ACOG practice bulletin or chronic hypertension notes that while many women with chronic (preexisting) hypertension have previously been under care or their hypertension, young women who are rst diagnosed with severe hypertension early in pregnancy are candidatesor evaluation o secondary causes o hypertension, since they are among those more likely to havesecondary hypertension. ACOG notes that consultation with maternal- etal medicine or a medicalsubspecialist should be sought when secondary causes o hypertension are being evaluated. Renalartery stenosis should be considered, as it would be the most likely secondary cause o hypertension,and testing could include renal artery velocimetry or magnetic resonance angiography, which is noted
in the ACOG practice bulletin.
Both ACOG and SOGC note that though pheochromocytoma is rare, it is associated with highmorbidity and mortality in pregnancy, and recommend catecholamine testing i there is a concern.43 SOGC guidelines also recommend considering additional baseline testing or women with conditionsthat may make later lab investigation di cult to interpret. Such testing could include liver unctiontesting or obese women, who may have associated non-alcoholic steatohepatitis.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 19/56

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 20/56
moderate risk actors or preeclampsia. Tere is no clear evidence to di erentiate among individualmoderate risk actors, but a higher risk or preeclampsia is associated with the presence o more thanone moderate risk actor. SOGC guidelines recommend low-dose aspirin or women with one high-risk actor or more than one moderate risk actor. Low-dose aspirin is commonly de ned as 75 mg/day. Although a range o aspirin dosages rom 50-150mg/day has been investigated, there is no clear
evidence or a dosage cuto or evidence to recommend higher dosages. Given available preparations,low-dose aspirin in high-risk women should be administered at a dosage o 81 mg/day. Enteric coatedaspirin should be avoided.
Tere is expert consensus that aspirin therapy should begin as early as possible or maximal bene tand should continue to delivery, supported by evidence that has shown the most bene t in risk reduction may be achieved i aspirin therapy is begun be ore 16 weeks gestation. Te WHOrecommends initiation prior to 20 weeks gestation. Tere is good evidence to support continuingaspirin therapy to delivery, and no reported increased bleeding complications with therapy. SOGCguidelines cite air evidence rom randomized controlled trials to recommend administration o aspirin prophylaxis at bedtime.
b. Other pharmaceuticals
There is no evidence to recommend pharmaceuticals other than low-dose aspirin in the prevention o
preeclampsia or its complications.
Other than low-dose aspirin, there are no pharmaceuticals recommended in current guidelines orthe prevention o preeclampsia or its complications. Antihypertensive therapy speci cally to preventpreeclampsia is not recommended.
Tere is limited evidence regarding the bene t o low-molecular-weight heparin (LMWH), and
there is insu cient evidence to recommend it or preventing preeclampsia, even among women with thrombophilia or previous preeclampsia. Other pharmaceutical agents or which evidence islimited include nitric oxide donors, diuretics and progesterone; none o these are recommended inguidelines, and diuretics are speci cally not recommended in WHO guidelines or the prevention o preeclampsia or its complications.
c. Dietary calcium supplementation
Adequate calcium intake (1300 mg/day or women age 14-18 and 1000 mg/day or women over age
18) is necessary or maternal health, and women with low dietary intake o calcium should receive
calcium supplementation. There is no clear evidence or the bene t o calcium or the reduction o the
risk o preeclampsia in the general US population. There is no evidence to support recommending other
supplements or the prevention o preeclampsia.
Many supplements that have been investigated or potential bene t in decreasing the risk o hypertensive disorders o pregnancy are known to be o general bene t in pregnancy. Tough calciummay be o general bene t or pregnant women, evidence has been mixed regarding the bene to calcium supplementation or reducing the risk o preeclampsia. Calcium in the prevention o

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 21/56
preeclampsia has been identi ed as a key area or research in NICE guidelines, since current evidenceis lacking due to variability in study populations. Te greatest e ect o calcium supplementation hasbeen shown in high-risk women with poor intake, and has included a small decrease in the incidenceo preeclampsia, and also a decrease in maternal death and serious morbidity.45
While ACOG guidelines published in 2002 indicate that there is no evidence or thebene it o calcium or the reduction o the risk o preeclampsia, the more recent SOGC andSOMANZ guidelines recommend calcium supplementation or women at risk who have low dietary calcium intake. Recommendations are based on randomized, controlled trials andinclude at least 1g/d supplementation orally or women with low dietary intake o calcium,de ined as ≤600 mg/d). WHO guidelines recommend supplementation with 1.5-2 gramselemental calcium per day or pregnant women, particularly those at high risk or preeclampsia,in areas where dietary calcium intake is low.
d. Other dietary supplements
There is no evidence to support recommending supplements other than calcium or the prevention o preeclampsia.
Tere is no evidence or the bene t o magnesium in the prevention o preeclampsia, and it is notrecommended or this purpose. Other supplements that are speci cally not recommended based onstrong evidence include vitamin C and E, and prostaglandin precursors such as sh oils or algal oils. Although Vitamins C and E had previously shown promise, as noted in the ACOG preeclampsiapractice bulletin, there is now good quality evidence that Vitamin C and E have no e ect onprevention o preeclampsia, and indeed some adverse e ects have been noted; there ore, VitaminC and E are not recommended or the prevention o preeclampsia. Tere is insu cient evidence torecommend garlic, zinc, pyridoxine or selenium. WHO guidelines do not recommend Vitamin Dsupplementation or the prevention o preeclampsia and its complications.
Although o general periconceptional bene t in the prevention o neural tube and other anomalies,there is poor evidence or the use o olic acid in the prevention o HDP.
e. Anticipatory guidance
Pregnant women at risk or preeclampsia should be provided with anticipatory guidance regarding
symptoms o preeclampsia to be reported to the physician, midwi e, nurse practitioner or physician assistant.
Only NICE guidelines include a recommendation to provide anticipatory guidance relating tosymptoms o preeclampsia, including severe headache, vision problems (blurring, fashing) and severepain below the ribs. While not explicit in other guidelines, identi cation o the signs and symptomsto be reported to the physician or midwi e is an essential part o patient education in general. It isimportant that women at risk or preeclampsia be alerted to symptoms o preeclampsia and advised when to contact their health care provider.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 22/56
. Diet/li estyle
A healthy li estyle is generally recommended or pregnant women, including moderate exercise.
Appropriate weight gain based on pre-pregnancy BMI as per Institute o Medicine (IOM) guidelines is
recommended.
A healthy li estyle is generally recommended or pregnant women and is important or a woman’slong term health. ACOG-AAP guidelines recommend providing all pregnant women within ormation regarding balanced nutrition or maternal and in ant health, and ACOG-AAPguidelines recommend nutrition consultation or obese women. Calorie restriction during pregnancy or overweight or obese women is not recommended, as it has not been associated with a decreasedincidence o preeclampsia or gestational hypertension, and there are concerns that calorie restrictionmay contribute to starvation ketosis in the etus and resultant neurodevelopmental problems.
Tere is consensus across guidelines that salt restriction is not recommended solely to preventgestational hypertension or preeclampsia, since there is no clear evidence to support its e ectiveness
in high-risk women.46,47Tere is good evidence against recommending dietary salt restriction inlow-risk women. A reexamination o the Institute o Medicine guidelines or weight gain duringpregnancy published in 2009 established a range o appropriate weight gain based on pre-pregnancy Body Mass Index (BMI), and includes a relatively narrow range o weight gain or obese women.48 Te IOM noted that women whose weight gain exceeds recommended ranges may have an increasedrisk o gestational hypertension and preeclampsia, but the evidence is limited and o air to poorquality. Tere ore, associations o these conditions and gestational weight gain are not clear. Tealterations in the normal maternal plasma volume expansion and vascular permeability seen inpreeclampsia con ound the monitoring o weight gain in women with preeclampsia.
Advice on rest, exercise and work or women at risk or preeclampsia is the same as the advice
generally given or healthy pregnant women; moderate exercise is recommended. Tere areobservational studies suggesting there may be an association between exercise and reducedpreeclampsia risk in low-risk women, but no speci c evidence to recommend exercise to low-risk women to prevent preeclampsia. However, low to moderate intensity exercise is o bene t or generalhealth. Te 2002 ACOG Committee Opinion on exercise during pregnancy identi es preeclampsiaand gestational hypertension as absolute contraindications to aerobic exercise in pregnancy and poorly controlled chronic (preexisting) hypertension as a relative contraindication to aerobic exercise inpregnancy.49SOGC guidelines cite insu cient evidence or exercise in high-risk women.
Tere is insu cient evidence to recommend rest or women at risk or preeclampsia. SOGCguidelines cite conficting evidence or increased rest at home in the third trimester or women at risk. WHO guidelines do not recommend rest at home or the prevention o preeclampsia in women atrisk. Other li estyle actors that have been investigated or the prevention o HDP, such as abstentionrom alcohol and tobacco, do not have speci c evidence or a reduction o the risk o preeclampsia buthave other known bene ts in pregnancy.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 23/56

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 24/56
Te authors concluded that the risk or mal ormation was likely due to the underlying hypertensivecondition rather than ACE inhibitor therapy in the rst trimester. Tis nding provides somereassurance or women who become pregnant while taking ACE inhibitors. Tis study did not address ACE inhibitor use in the second and third trimesters, or which a category D (known etal risk)classi cation rom the US Food and Drug Administration has previously been assigned. Te FDA
currently notes that when used in pregnancy during the second and third trimesters, ACE inhibitorscan cause injury and even death to the developing etus, and that when pregnancy is detected, the ACE inhibitor should be discontinued as soon as possible. Tere ore, since there is some evidence thatthere may be no added risk rom RAAS inhibitors during the rst trimester o pregnancy, but risk isclearly present in the second and third trimesters, women should be changed rom RAAS inhibitorsto alternative therapy upon discovery o intrauterine pregnancy.
Te ACOG practice bulletin or chronic hypertension notes consensus and expert opinion that women with chronic (preexisting) hypertension should be evaluated or end-organ damage, whichincreases the risk o adverse outcomes, and possible secondary causes or hypertension, ideally be oreconception. Te JNC report and SOGC guidelines also recommend a preconception evaluation orpossible secondary causes o hypertension and or end-organ dys unction or women with chronic(preexisting) hypertension. Te ACOG Chronic Hypertension in Pregnancy practice bulletin notes thatrenal artery stenosis should be considered in women younger than 30 years with severe hypertension who have not been previously evaluated, especially i there is no amily history o hypertension. Te JNC notes the high morbidity and mortality o pheochromocytoma i not diagnosed antepartum, andthe need to evaluate those women or whom suspicion is high. ACOG recommends evaluation orpheochromocytoma or women with paroxysmal hypertension, requent hypertensive crises, seizuredisorders, anxiety attacks, palpitations or headaches.
Women with HDP should be educated about their condition, including sel management and signs
or symptoms o concern. It is important to note that ACOG recommends that all health encountersduring a woman’s reproductive years, particularly those that are a part o preconception care, shouldinclude counseling on appropriate health behaviors to optimize pregnancy outcomes.
b. Diet
Appropriate weight gain according to Institute o Medicine (IOM) guidelines is recommended. There is
insufcient evidence regarding salt restriction in women with chronic (preexisting) hypertension.
Appropriate weight gain or healthy pregnancy outcomes has been de ned by the Institute o Medicine (IOM). Dietary salt restriction is not recommended or gestational hypertension, and there
is insu cient evidence to recommend dietary salt restriction or women with chronic (preexisting)hypertension. However, the JNC notes that despite sparse data, many experts advise salt restriction to2.4g sodium daily or women with chronic (preexisting) hypertension as is recommended or primary hypertension in the general population, and NICE guidelines also base recommendations on generaladult hypertension guidance. Salt restriction has a variable e ect on blood pressure among individuals. Women with chronic (preexisting) hypertension who are on a DASH (Dietary Approaches to StopHypertension) diet are advised to continue it in SOGC guidelines, although there is no de nitiveevidence to support this recommendation.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 25/56
Weight reduction and calorie restriction are not generally recommended or overweight and obese women with HDP.
c. Li estyle
A healthy li estyle is recommended or women with HDP. Moderate exercise is o ten part o the care
plan or women with well-controlled chronic (preexisting) hypertension. There is insufcient evidence
or a recommendation regarding optimal activity levels or women newly diagnosed with gestational
hypertension. Aerobic exercise is not recommended or women with preeclampsia.
Physical activity is part o a healthy li estyle and there is insu cient evidence to recommend rest oractivity limitation or women with HDP. However, the 2002 ACOG Committee Opinion on exerciseduring pregnancy recommends restricting aerobic exercise in women who develop preeclampsia orgestational hypertension, and the JNC or women with chronic (preexisting) hypertension, based ontheoretical concerns regarding its potentially negative impact on placental blood fow and consequentincreased risk o preeclampsia.
Te JNC notes that it is particularly important to strongly discourage the use o alcohol and tobaccoby women with HDP.
d. Blood pressure threshold and targets or treatment
i. Non-severe hypertension
Non-severe hypertension: There is no de nitive evidence or optimal blood pressure targets in
hypertensive disorders in pregnancy; there is a particular lack o clear evidence regarding the optimal
management o women with non-severe hypertension. Some experts in the U.S., including the Joint
National Committee on Prevention, Detection, Evaluation and Treatment o High Blood Pressure intheir Seventh Report, have recommended treating women with chronic (preexisting) hypertension
and no evidence o end-organ damage whose blood pressure is 150-160 mmHg systolic or 100-110
mmHg diastolic.
Te goal o blood pressure management in hypertensive disorders in pregnancy is to optimizepregnancy outcome, which requires consideration o minimizing maternal risk while maintainingplacental/ etal per usion. Intervention decisions or abnormal blood pressure readings are dependenton consideration o gestational age. Tere is no de nitive evidence or optimal blood pressuretargets in hypertensive disorders in pregnancy; there is a particular lack o clarity regarding theoptimal management o women with non-severe hypertension (systolic blood pressure 140-159mmHg or diastolic blood pressure 90-109 mmHg). Tere is some evidence that implementingantihypertensive therapy or non-severe hypertension may decrease the relative risk o maternalsevere hypertension, but there is no evidence or a positive impact on adverse maternal or perinataloutcomes such as stroke, preterm birth or perinatal death. Furthermore, there is some evidence tosuggest that antihypertensive therapy or non-severe hypertension and the resultant decrease in bloodpressure therapy may cause some harm, such as an increased risk o small or gestational age or low birthweight births.51
7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 26/56
Te threshold or administering antihypertensive therapy or women with non-severe chronic(preexisting) hypertension is not clear rom existing evidence, and it is generally acknowledgedthat more evidence is needed. Tere is limited, good quality evidence against treating mild ormoderate hypertension. Tere is insu cient evidence regarding the bene t o pharmacologicaltreatment o non-severe chronic (preexisting) hypertension in the prevention o maternal stroke or
other maternal morbidity or in the prevention o adverse neonatal outcomes. Te JNC report citesevidence that there is a linear relationship between the all in blood pressure induced by treatmentand an increase in the proportion o small or gestational age (SGA) births in women with chronic(preexisting) hypertension. Te JNC notes that women with Stage 1 blood pressure (140-159/90-99 mmHg) are at low risk or developing cardiovascular complications during pregnancy and arecandidates or li estyle modi cation rather than antihypertensive therapy. Tis recommendationis supported by the act that blood pressure usually alls during the rst hal o pregnancy, whichmay acilitate control with reduced or no medication; this observation is also cited in SOGCguidelines. Further, JNC guidelines cite the lack o evidence o improved neonatal outcomes withpharmacological treatment. Te ACOG practice bulletin or chronic (preexisting) hypertension in
pregnancy suggests that it is reasonable to withhold antihypertensive therapy, and stop or reducemedication or those women already taking antihypertensive therapy, i blood pressure is less than150/100 mmHg, and there are no complicating actors such as cardiovascular or renal disease.For women with target organ damage or who required multiple antihypertensive agents or bloodpressure control prior to pregnancy, the JNC recommends continuing antihypertensive medicationto maintain blood pressure control.
Te JNC report advocates reinstituting antihypertensive therapy or any woman with chronic(preexisting) hypertension when blood pressure reaches systolic readings o 150-160 mmHg ordiastolic o 100-110 mmHg.52Te recommendation or instituting treatment at this thresholdis geared toward preventing severe hypertension during pregnancy, since there are reports o
high rates o etal loss and maternal mortality among women with severe chronic (preexisting)hypertension in the rst trimester. Tis threshold or treatment is also cited by NICE guidelinesor both chronic (preexisting) and gestational hypertension. ACOG stresses that women withsevere chronic (preexisting) hypertension (systolic blood pressure 160 mmHg or greater or diastolicblood pressure 110 mmHg or greater) should have antihypertensive therapy initiated or continuedto reduce the risk o maternal stroke.
Tere is lack o clarity in the literature regarding optimal targets or blood pressure control i treatment is instituted. Based on expert consensus, SOGC guidelines cite a blood pressure targeto 130-155/80-105 mmHg or both chronic (preexisting) and gestational hypertension i thereare no comorbid conditions, although noting that it is not critical to maintain normal bloodpressure over the ew months that compromise the duration o pregnancy. NICE guidelines citea target o less than 150/100 mmHg. Both NICE and SOGC guidelines identi y a lower limito diastolic blood pressure o 80 mmHg or any woman being treated or hypertension, based ona concern that controlling blood pressure to lower levels will limit uteroplacental per usion. For women with chronic (preexisting) hypertension with target organ damage, such as renal disease,SOGC guidelines recommend tighter control, with a target o blood pressure 130-139/80-89mmHg based on expert consensus. For women with gestational hypertension and comorbid

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 27/56
conditions that increase cardiovascular risk, tighter control is controversial due to the known risk o IUGR; however, SOGC guidelines cite the same target or these women o 130-139/80-89mmHg. Re erenced comorbid conditions include those or which there is a compelling reasonor more aggressive therapy beyond improving short term pregnancy outcomes, such as majorcardiovascular risk actors including preexisting diabetes, vascular disease or renal disease. A 2011
Cochrane review o two small randomized controlled trials revealed that there was no di erencein the incidence o severe preeclampsia between groups o women with low-risk gestational orchronic (preexisting) hypertension whose blood pressure was tightly controlled (blood pressure< 140 mmHg systolic and < 90 mmHg diastolic) compared to those whose blood pressure was very tightly controlled (blood pressure ≤ 130mmHg systolic and ≤ 80mmHg diastolic), and nodi erence in perinatal deaths or other etal adverse outcomes. However, there were no cases o stroke, eclampsia or maternal deaths in these studies.53For women with non-severe hypertensionand preeclampsia, SOGC guidelines do not speci y targets, noting that consideration must begiven to maternal and etal clinical conditions.
ii. Severe hypertension
Acute management should be initiated or severe hypertension, de ned as systolic blood pressure
> 160 mm Hg or diastolic blood pressure > 110 mmHg or both.
Tere is consensus across guidelines or the need to acutely manage severe hypertension, de nedas systolic blood pressure ≥ 160 mm Hg or diastolic blood pressure ≥ 110 mmHg or both, withthe goal o preventing maternal stroke and avoiding intrauterine growth restriction (IUGR). Te ACOG Committee Opinion on therapy or acute, severe hypertension notes that acute onseto persistent, severe systolic or diastolic hypertension in pregnant or postpartum women withpreeclampsia or eclampsia constitutes a hypertensive emergency.54Women presenting with acuteonset, severe hypertension in an o ce setting should be rapidly re erred to a hospital settingor treatment. Te JNC report notes that it is important to treat severe chronic (preexisting)hypertension in the rst trimester since there are high rates o etal loss and risk o maternalmortality in these patients.55
Tere is a lack o clear evidence regarding the goals o therapy in acute hypertension management. argets or acute management across guidelines include lowering blood pressure to less than severelevels (less than 160/110 mmHg), with caution to avoid a precipitous or extreme drop in bloodpressure. Te ACOG Committee Opinion on therapy or acute, severe hypertension recommendsa blood pressure control goal o 140-160/90-100 mmHg to avoid prolonged exposure to severesystolic hypertension and loss o maternal cerebral vascular autoregulation. Te target or severe
hypertension cited by NICE guidelines, < 150/100 mmHg but not lower than 80 mmHg diastolic,does not di er rom the NICE target or non-severe hypertension.
e. Antihypertensive agents or non-acute blood pressure management
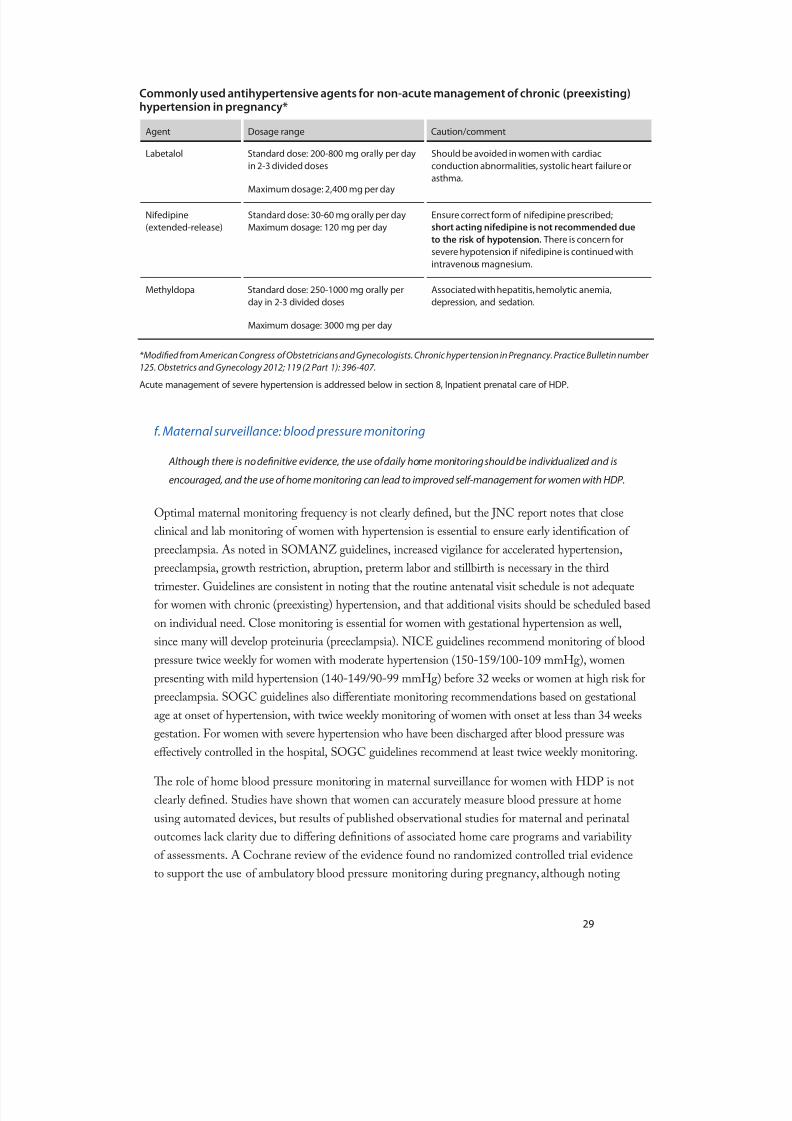
In the absence o contraindications, labetalol is pre erred or management o hypertension in pregnancy.
I labetalol is contraindicated, extended-release ni edipine is commonly used in pregnant women
with chronic (preexisting) hypertension. Methyldopa has also been used in HDP. Women with chronic

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 28/56
(preexisting) hypertension who are well controlled on diuretics prior to pregnancy do not need to have
the diuretic discontinued during pregnancy. Atenolol is not recommended or use during pregnancy due
to association with IUGR. Discussion with Maternal Fetal Medicine regarding optimal blood pressure
management or women with chronic (preexisting) hypertension may be help ul.
Tere is insu cient evidence to identi y a single pre erred agent or non-acute blood pressuremanagement. However, there is consistency across guidelines regarding the acceptability o orallabetalol, ni edipine and methyldopa or non-acute treatment o hypertension in pregnancy, based ongood quality evidence. Labetalol, a combinedα and β receptor blocker, and methyldopa, a centrally acting α agonist, are most requently cited as pre erred agents. However, labetalol is pre erred dueto ewer adverse e ects than methyldopa, and is recommended by ACOG as a good option or rstline treatment o chronic (preexisting) hypertension in pregnancy. ACOG and the JNC cite reportso stable uteroplacental fow and etal hemodynamics, as well as an absence o reports o long termadverse developmental e ects in children, as reasons that methyldopa is pre erred by many clinicians.However, the use o methyldopa has been associated with serious adverse e ects, including hepatitis,hemolytic anemia, depression, central nervous system sedation and a lupus-like syndrome.56Orallabetalol is considered rst line by NICE, with a recommendation to consider alternatives methyldopaand ni edipine only a ter considering maternal, etal and neonatal side e ect pro les.
RAAS active drugs, including ACE inhibitors, ARB and renin inhibitors, have been associated withetal abnormalities, although the evidence is o poor quality. All guidelines recommend discontinuingthese agents and not initiating them during pregnancy.
SOGC guidelines cite the acceptability o the beta blockers acebutolol, metoprolol, pindolol andpropranolol, while SOMANZ guidelines note the possible association o IUGR with highly selectivebeta blockers. Atenolol has been associated with low birth weight when used rom early pregnancy,and it is not recommended or use during pregnancy. A possible association o metoprolol and IUGR has also been reported, and metoprolol may also exacerbate asthma.57
Te evidence or long acting calcium channel blockers is more limited than the evidence or labetalol,but they appear to be sa e.58Ni edipine has been the most commonly studied. ACOG notes atheoretical concern regarding potential synergy between magnesium and other calcium channelblockers with resultant severe hypotension. SOGC guidelines recommend that prazosin not be usedbased on an association with stillbirth in one trial. Some o the reviewed guidelines recommend againstusing diuretics, due to their contribution to a restriction o the normal plasma volume expansiono pregnancy; ACOG and the JNC report note that they are not rst line agents but probably sa e.Other possible adverse e ects o thiazide diuretics include hypokalemia and carbohydrate intolerance.
Te ACOG practice bulletin or chronic (preexisting) hypertension lists hydrochlorothiazide, as wellas hydralazine, as adjunctive agents among oral antihypertensives used commonly in pregnancy. Asummary o standard and maximum dose ranges o common agents is noted below.
7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 29/56

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 30/56
that observational studies suggests that it may be o use in assessing blood pressure in pregnancy.32 In women with HDP, the role o home blood pressure surveillance is unclear. Based on the levelo blood pressure control and other comorbid conditions, use o daily home monitoring should beindividualized, and may be appropriate or some patients. Monitoring o blood pressure at least twicea week or women with HDP undergoing home blood pressure surveillance should be considered.
Daily monitoring may be appropriate or some patients.
g. Maternal surveillance: laboratory testing
Women with HDP should have periodic, de nitive proteinuria testing (24 hour urine collection or spot
urinary protein: creatinine ratio to quanti y the amount o proteinuria) as indicated.
For women with con rmed hypertensive disorders without preeclampsia, de nitive proteinuria testing isrecommended. SOGC guidelines recommend proteinuria testing using spot urinary protein: creatinineratio or 24-hour urine collection i there is a suspicion o preeclampsia, including or women whoare normotensive with symptoms or signs suggestive o preeclampsia, and or hypertensive pregnant
women with a rising blood pressure. Neither SOGC nor ACOG, which recommends periodic testing with spot urine protein: creatinine ratio, cite a speci c requency o proteinuria testing or women withhypertensive disorders. NICE guidelines recommend the use o an automated reagent strip readingdevice or urinary protein: creatinine ratio twice weekly or women with non-severe hypertensionpresenting be ore 32 weeks and other women at high risk o preeclampsia.
In women with con rmed HDP, testing should be conducted or end-organ dys unction. Other thanproteinuria testing, there is insu cient evidence to de ne which lab assessments are most use ul inmonitoring women with hypertensive disorders o pregnancy, and the validity o tests alone or incombination has not been reported. Tere is poor quality evidence regarding the predictive value o speci c positive tests, although negative tests can be use ul.33In addition to routine antenatal labtesting, most guidelines recommend that women with suspected preeclampsia should be evaluated with a complete blood count (hemoglobin, white blood cell count and di erential, platelet count,blood lm), electrolytes and renal unction (serum creatinine), and liver unction tests (transaminases,bilirubin). SOGC guidelines also recommend coagulation studies (INR and aP , brinogen) andserum uric acid, glucose and urinalysis, with additional baseline labs as indicated. ACOG notes thatelevated serum uric acid may be particularly use ul in distinguishing preeclampsia in women withchronic (preexisting) hypertension who rst present late in pregnancy.
SOGC guidelines note that there is no clear evidence to de ne the requency o surveillance i preeclampsia is suspected, but cite changes in maternal or etal clinical status as reasonable indications
to repeat tests. NICE guidelines recommend repeat testing i there is ongoing concern, and theseguidelines speci y weekly testing or women presenting with severe hypertension.
h. Fetal surveillance: tests o etal well being
Tere is no de nitive evidence regarding the most appropriate way to conduct etal surveillancetesting or women with HDP. Fetal growth should be assessed with ultrasonography in all women with HDP. Non-stress test, biophysical pro le, deepest amniotic fuid pocket assessment and

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 31/56
umbilical artery Doppler velocimetry are commonly used tests, but there is no evidence to determine which test or group o tests is most appropriate or etal surveillance. Fetal testing should beconducted in the context o a coordinated system, with involvement o obstetricians and maternal-etal medicine subspecialists based on the patient’s degree o control and risk.
ACOG-AAP Guidelines for Perinatal Care note the lack o randomized clinical trials regarding thee ect o prenatal tests o etal well being on outcomes. ACOG and other guidelines note that etalsurveillance has become central to the care o high-risk pregnancies, and hypertensive disorders inpregnancy are an indication or initiating tests o etal well being. Evidence is lacking regarding how to conduct etal surveillance in women with HDP, such as which tests should be per ormed and whenthey should be initiated. ACOG notes that testing should be individualized, and NICE guidelinesrecommend development o an individual care plan or women with HDP that includes the natureand timing o etal monitoring. It is essential that etal testing be conducted in the context o acoordinated system, with involvement o obstetricians and maternal- etal medicine subspecialists asindicated.
Due to a lack o randomized controlled trials, there is no evidence that any single test o etal well being is superior to others. ests are o low speci city, and the meaning o abnormal resultsat early gestational ages is unclear. Tere ore, tests should be corroborated when possible to avoidunnecessary intervention. Commonly recommended tests across guidelines include non-stress test(NS ), biophysical pro le (BPP) without non-stress test, ultrasound assessment o etal growth,amniotic fuid assessment (deepest amniotic fuid pocket measurement), and umbilical artery Doppler velocimetry.
NS is the most common antepartum screening test; it is easily per ormed on an outpatient basisand requires minimal sta . BPP has a lower alse positive rate than NS alone, and is supplantingcontraction stress test as ollow up to a nonreactive NS. BPP includes the individual componentso NS , etal breathing movements, etal movement, etal tone, and quanti cation o amnioticfuid volume. ACOG recommends NS or BPP requently i IUGR is suspected or or women with preeclampsia. Modi ed BPP that includes NS and assessment o amniotic fuid depth oroligohydramnios appears to be as predictive as other approaches.34
SOGC cites evidence to avor deepest amniotic fuid pocket over amniotic fuid index or assessingamniotic fuid volume. Fetal growth should be monitored with ultrasonography assessments in women with hypertension. Although not a good screening test in the general population, umbilicalartery Doppler velocimetry can be used or women at high risk o IUGR in combination withother biophysical tests, and it has been shown to reduce the need or etal intervention, improve
neonatal outcome and predict adverse perinatal outcomes.35Te ACOG practice bulletin orchronic (preexisting) hypertension indicates that the use o umbilical vessel Doppler velocimetry is appropriate or women with chronic (preexisting) hypertension. For women with early onsetpreeclampsia, which is thought to be placental mediated, uterine artery Doppler may be particularly use ul or predicting complications.36Tere is a lack o evidence or the timing or requency o umbilical artery Doppler velocimetry, and it is o limited value a ter 36 weeks gestation.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 32/56
SOGC guidelines also include etal movement counts in etal surveillance. ACOG guidelines indicatethat maternal perception o etal movement may precede etal demise, but the e ect o maternalperception on outcomes is unclear. Tere is no de ned normal cuto o etal movement counts, andmaternal perception o a relative decrease may be more important.
ACOG notes that the prognosis or survival i action is taken or abnormal results o etal tests o well-being must be considered in the timing o initiation o testing, as well as severity o maternaldisease and risk o etal death. ACOG recommends initiation o etal tests o well being at 32-34 weeks as appropriate or most pregnancies, with initiation at 26-28 weeks or multiple gestation or very high risk conditions. NICE guidelines recommend initiation at 28-30 weeks, or 2 weeks be orethe gestational age o onset o previous episodes o HDP i earlier.
i. Frequency o etal testing and monitoring
There is no de nitive evidence regarding the most appropriate timing o initiation or interval o testing
in women with HDP. It is reasonable to initiate etal testing beginning no later than 32 weeks and to
conduct etal tests o well-being once to twice weekly in women with HDP. Surveillance or etal growthshould be conducted with ultrasonography at least monthly or women with HDP, and ultrasound
should be initiated earlier than 32 weeks or etal indications such as evidence o IUGR or maternal
indications such as comorbid conditions, or example, diabetes.
NICE guidelines recommend repeat etal testing 4 weeks a ter initiation. ACOG-AAP guidelinesrecommend repeating NS, BPP or both weekly through delivery once initiated i results arereassuring and twice weekly or very high-risk women or or changes in maternal condition. Te ACOG practice bulletin or chronic hypertension notes that monitoring o women with chronic(preexisting) hypertension may include twice weekly NS or BPP. Te recommendation or weekly testing is based on the low likelihood o intrauterine etal death in the 7 days ollowing a reassuringtest in most clinical conditions. However, ACOG-AAP guidelines suggest twice weekly testing may be indicated or high-risk conditions, which include gestational hypertension and IUGR.
j. Re errals/consultations
Consultation/re erral to an obstetrician/gynecologist is recommended or women with HDP. Maternal-
etal medicine telephone consultation is always available with the regional perinatal center. Consider
maternal/neonatal needs and availability o ICU when considering trans er to a regional perinatal
center. Control o severe hypertension and seizure prophylaxis must be initiated at the re erring hospital
prior to maternal transport.
NICE guidelines recommend a specialist or women with secondary chronic (preexisting)hypertension (by consensus) and assessment by a pro essional trained in management o HDP or women with preeclampsia. ACOG-AAP guidelines recommend consultation with a maternal- etalmedicine subspecialist or women with chronic (preexisting) hypertension and renal or heart disease,and or severe preeclampsia remote rom term. Te ACOG practice bulletin Chronic Hypertension inPregnancy suggests consideration o consultation or women with chronic (preexisting) hypertensionand superimposed preeclampsia. Obstetric or maternal etal medicine consultation/re erral or

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 33/56
high-risk hypertensive disorders in pregnancy is encouraged and should be considered. Maternal-etal medicine telephone consultation is available with the regional perinatal center. ACOG notesthat severe preeclampsia remote rom term is best managed in a tertiary care setting. Maternal andneonatal needs should be considered when evaluating the need or trans er to a regional perinatalcenter (RPC), as well as actors such as availability o ICU care.
8. Inpatient prenatal care o HDP-severe hypertension and preeclampsia
a. Indications or inpatient care
Inpatient care is generally recommended or all women with severe hypertension or preeclampsia.
Hospitals should have written protocols to identi y indications or outpatient care and to outline how
home monitoring will be conducted. Patients with HDP being discharged to home should have ormal
written instructions or how their outpatient monitoring and management will be conducted.
Inpatient care is recommended or women with identi ed severe hypertension or preeclampsia acrossguidelines. ACOG, SOGC and SOMANZ guidelines all advise consideration o the rare homemanagement or non-severe preeclampsia a ter initial inpatient care, and or women hospitalized orsevere hypertension a ter control o blood pressure i seriously remote rom term. NICE guidelinesrecommend that hospitalization continue or women with severe hypertension until blood pressureis 159/109 mmHg or lower. ACOG guidelines note that a ter hospitalization and serial assessmento maternal and etal condition, mild preeclampsia remote rom term may be managed with care ulhome observation, with mild preeclampsia de ned as blood pressure less than 160/110 mmHg,proteinuria less than 5g/d, and absence o oliguria or other maternal/ etal symptoms or signs.
Home management should include access to health care providers and requent maternal and etalevaluation. Women undergoing home observation should be hospitalized i they are noted to haveany progression or mani estation o severe disease by lab ndings, symptoms or signs, or i they havedi culty with compliance. Hospitals should have written protocols to identi y which patients arecandidates or home monitoring and to de ne how home monitoring will be conducted.
ACOG urther advises that severe preeclampsia remote rom term is best managed in a tertiary caresetting or in consultation with an obstetrician trained and experienced in high-risk pregnancies, suchas a maternal- etal medicine subspecialist.
b. Critical care
SOMANZ guidelines recommend admission to critical care or intensive monitoring andmanagement or women with HDP and organ ailure, severe pulmonary edema or sepsis, intractablehypertension, anuria or renal ailure, repeated seizure, massive blood loss with DIC, neurologicimpairment requiring ventilation, or critical abdominal pathology.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 34/56
c. Communications
Hospitals should have written protocols or management o HDP that are available to all care team members.
Clear communication among care team members is essential or optimal, sa e and consistentmanagement o women with HDP. SOGC, NICE and SOMANZ guidelines all recommendthat acilities develop protocols that can be accessed by all sta to ensure consistent, quality care.Guidelines recommend that acilities have protocols in place that include general managementprotocols or preeclampsia, protocols or severe hypertension management, and indications or seizureprophylaxis in preeclampsia. SOMANZ guidelines recommend that OB units post protocols or theadministration o LMWH when epidural anesthesia or analgesia is administered.
ACOG-AAP guidelines recommend in orming the obstetrician, midwi e or nurse practitioner o any woman presenting to labor and delivery who is ound to have hypertension on initial evaluation.Other communications among team members recommended in guidelines include in orminganesthesia when women with preeclampsia are admitted, and discussion among the patient and
neonatal, obstetric and anesthesia team members i birth be ore 34 weeks is considered. Written careplans with parameters or maternal and etal surveillance and maternal ollow-up are advocated inNICE guidelines.
Hospitals should have written protocols that are evidence-based or management o HDP,including protocols or treatment o severe hypertension, eclamptic seizures, fuid management,thromboprophylaxis, and home monitoring. Noti cation procedures should be part o writtenprotocols, and written plans or discharge should be part o the discharge process.
d. Bedrest
Although JNC guidelines recommend hospitalization or preeclampsia or bedrest, most guidelinesrecommend against strict bedrest or inpatient care o women with HDP. Te role o bedrest intreatment o preeclampsia has been identi ed as a priority area or research by the SOGC. SOGCand SOMANZ guidelines cite air evidence against recommending strict bedrest or women withpreeclampsia who are hospitalized, with no di erence in maternal or perinatal outcomes oundcompared to some bedrest. SOGC guidelines note insu cient evidence or the use ulness o bedrestin all other women with HDP. NICE guidelines cite one small randomized controlled trial (RC )that showed no bene t rom hospital bedrest or pregnant women with chronic (preexisting)hypertension in reducing the risk o preeclampsia, but NICE and SOGC guidelines suggest thatsome hospital bedrest may be use ul or women with gestational hypertension without preeclampsia when compared with unrestricted activity at home, based on an observed reduced risk o severehypertension with hospitalization plus bedrest. Prolonged bedrest can increase the risk o venousthromboembolism. Tromboprophylaxis may be considered when bedrest is prescribed.
e. Acute hypertension management
Severe hypertension, systolic blood pressure ≥ 160 mmHg or diastolic blood pressure ≥ 110 mmHg or
both, requires urgent management. Intravenous labetalol is recommended or initial therapy or severe
hypertension. Hydralazine is also acceptable or initial therapy or severe hypertension.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 35/56
Tere is general consensus in guidelines that acute management should be instituted or severehypertension (systolic blood pressure ≥ 160 mmHg or diastolic ≥ 110 mmHg or both), and that bloodpressure should be lowered to systolic < 160 mmHg and diastolic < 110 mmHg. Hospitalized patients with preeclampsia who are identi ed with either systolic blood pressure o 160 mmHg or diastolicblood pressure o 110 mmHg should ideally receive an intravenous (IV) antihypertensive agent
within 15 minutes. Te goal or treatment o severe hypertension is to decrease maternal morbidity and mortality, since antihypertensive treatment has not been shown to a ect perinatal outcome andmay negatively impact uteroplacental blood fow. Most women presenting with severe hypertension will have had a recently normal blood pressure, and the commonly abrupt, marked increase in bloodpressure heightens the urgency o treating severe hypertension in pregnant women even in theabsence o symptoms. Te ACOG Committee Opinion on management o acute severe hypertensionrecommends a target blood pressure o 140-160/90-100 mmHg. Women undergoing acutehypertension management require monitoring o blood pressure response and o maternal/ etal status.Continuous maternal blood pressure and etal heart rate monitoring are indicated, since all shortacting agents have been shown in observational studies to be associated with maternal hypotension in
women with preeclampsia. Tere are no controlled studies or the rapidity o blood pressure reduction,but care must be taken to avoid maternal hypotension or a precipitous decrease, since this could resultin impaired placental per usion. Blood pressure should be controlled prior to delivery.
Tere is a consistent recommendation across guidelines that labetalol intravenously (IV) isrecommended or initial therapy or severe hypertension. ACOG guidelines note that labetalol andhydralazine have been shown to be equally e ective; the 2011 ACOG Committee Opinion ortreatment o acute, severe hypertension recommends use o one or both o these agents as rst linetherapy. Hydralazine has been associated with more severe adverse e ects than other agents based onresults o a meta-analysis. Parenteral hydralazine causes severe maternal hypotension and signi canttachycardia, particularly in volume-depleted women, and has been associated with marked, severe
etal tachycardia. Tere ore, hydralazine should only be used in a volume-repleted patient and only i there is a clear contraindication to labetalol. It should be noted that the same meta-analysis showedan association o labetalol and increased risk o neonatal bradycardia. Labetalol should be avoided in women with cardiac conduction abnormalities, systolic heart ailure or asthma, and monitoring shouldbe conducted or possible neonatal bradycardia. Te ACOG committee opinion or acute severehypertension notes that labetalol can be administered orally i IV access has not been establishedand treatment is urgently needed, and the ACOG practice bulletin or chronic hypertension inpregnancy includes hydralazine intramuscularly (IM) as an option or urgent control o severe acutehypertension.
ACOG indicates that there is less evidence regarding calcium channel blockers or acute, severehypertension, though other guidelines cite good evidence to support the use o ni edipine capsules oracute blood pressure management in women with severe hypertension. Te ACOG practice bulletinor chronic hypertension includes oral ni edipine as a possible agent or urgent control o severe,acute hypertension in pregnancy, noting possible inter erence with labor as an adverse e ect. Te JNCreport notes that short acting ni edipine is not FDA approved or managing hypertension. Ni edipineused concurrently with magnesium can cause a precipitous drop in blood pressure. Tere is a high risk o precipitous drop in blood pressure with ni edipine in the preeclamptic patient.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 36/56

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 37/56

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 38/56
For women with early development o severe preeclampsia, ACOG and SOMANZ guidelinesrecommend evaluation or lupus anticoagulant and anticardiolipin antibodies.
g. Invasive hemodynamic monitoring
Invasive hemodynamic monitoring is not routinely done or women with HDP. ACOG and SOGCguidelines note that invasive monitoring may be use ul in critical cases such as acute renal ailure orhemodynamic instability to monitor response to treatment based on limited evidence.
h. Fetal surveillance
Tere is consensus across guidelines to recommend continuous etal monitoring or women withsevere hypertension. Although serial surveillance o etal well being is generally recommended, thereis no speci c evidence or the type and requency o tests. For severe preeclampsia, SOGC guidelinesrecommend monitoring etal movement count, NS , BPP, deepest amniotic fuid pocket, ultrasoundassessment o etal growth and umbilical artery Doppler velocimetry, with requency based on
ongoing concern. Tese guidelines suggest weekly Doppler interrogation o the umbilical artery orevaluation o IUGR in women with gestational hypertension and preeclampsia. ACOG monitoringrecommendations or severe preeclampsia include daily etal movement assessments and weekly NSor BPP, with twice weekly NS or BPP or IUGR or oligohydramnios, or more requent assessmentsdepending on severity and progression.
i. Delivery timing/expectant management
Determination o delivery timing in women with HDP is a complex decision that requires consideration o
gestational age, degree o hypertension control, and patterns o maternal and etal adverse conditions.
Preeclampsia is a maternal indication or delivery, and delivery should take place by 37 weeks. Delivery
should not be de erred to 39 weeks or women with preeclampsia. Delivery at 37 weeks or mild
preeclampsia is an indicated delivery and is not considered elective. Delivery should not be de erred to
await antenatal steroid administration i delivery is warranted or severe maternal indications.
Determination o delivery timing in women with HDP is a complex decision that requiresconsideration o gestational age, degree o hypertension control, and patterns o maternal and etaladverse conditions such as HELLP syndrome, deteriorating renal unction, and etal distress orIUGR.37Te ACOG practice bulletin or chronic hypertension notes that chronic (preexisting)hypertension with superimposed preeclampsia is particularly complex. Gestational age is a majordriver o decisions regarding expectant management or women with preeclampsia, since there is
evidence o an association o delivery be ore 34 weeks with neonatal morbidity, but the impact onmaternal risk is less clearly de ned in published trials. wo small trials cited by SOGC have suggestedthat expectant management o women with preeclampsia at less than 32-34 weeks gestation may decrease the risk o NICU admission, respiratory distress syndrome, and necrotizing enterocolitis.Guidelines recommend expectant management be ore 34 weeks a ter evaluation o etal and maternalstatus and weighing o maternal risk actors such as severe hypertension re ractory to treatment;SOGC guidelines suggest expectant management should only take place in perinatal centers capableo caring or very preterm neonates.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 39/56
ACOG guidelines note that severe preeclampsia usually warrants delivery, and eclampsia andHELLP syndrome are indications or delivery. Te ACOG practice bulletin or chronic hypertensionnotes that it is prudent to per orm delivery in women with chronic (preexisting) hypertension withsuperimposed preeclampsia at 34 weeks, as in women with severe preeclampsia. I birth is o eredbe ore 34 weeks or maternal or etal indications, antenatal steroids should be administered, and some
guidelines recommend discussion with neonatal and anesthesia teams. NICE guidelines recommenddocumentation o maternal (biochemical, hematologic, and clinical) and etal thresholds or electivebirth be ore 34 weeks in women with preeclampsia.
SOGC guidelines note that there is insu cient evidence to make recommendations about thebene t o expectant management or women at 34-36 weeks gestation with non-severe preeclampsia,though there is no expected perinatal bene t i pregnancy is prolonged. NICE guidelines recommendo ering birth to women with preeclampsia and mild or moderate hypertension at 34-36 weeksgestation based on maternal and etal status, risk actors, and NICU availability. Guidelines generally recommend o ering birth immediately or within 24-28 hours or women with severe or non-severepreeclampsia at ≥ 37 weeks gestation.
Evidence rom the HYPI A trial cited in NICE guidelines revealed that there were no maternalor neonatal disadvantage to delivery or these women, but progression o preeclampsia and resultantadverse consequences are a risk i delivery is not o ered. Tere is no evidence or biochemical orhematological thresholds or delivery.
j. Antenatal steroids
Antenatal steroids should be considered or women at risk or preterm delivery who present between 24
and 34 weeks gestation.
Antenatal steroids should be considered or women at risk or preterm delivery who present between24 and 34 weeks gestation. Tere is strong evidence to recommend steroids or all women presenting with preeclampsia be ore 34 weeks gestation. Te evidence is less clear regarding antenatal steroidsor women presenting with gestational hypertension without evidence o preeclampsia at less than 34
weeks gestation; although one third o these women will develop preeclampsia, it is unlikely that they will deliver within 7 days o presentation. SOGC guidelines recommend consideration o antenatalsteroids or women with gestational hypertension without signs or symptoms o preeclampsia whopresent at less than 34 weeks gestation i delivery is contemplated within the next 7 days based onexpert consensus, and some guidelines recommend discussion with the neonatal team.
9. Inpatient care specifc to preeclampsia
a. Severity classi cation
Severity classi cation o preeclampsia a ects management decisions. Criteria or severe preeclampsiadescribed in guidelines include severe hypertension, maternal symptoms, maternal biochemical
7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 40/56
and hematological impairment, and etal compromise. ACOG parameters should be used to de nesevere preeclampsia. It should be noted that several o these parameters are based on level C (expertconsensus) evidence. Tese parameters include one or more o the ollowing:
• Blood pressure ≥ 160/110 on two occasions 6 hours apart while patient on bedrest
• Proteinuria 5g or higher on 24 hour urine or 3+ or greater on two random urine samples 4 hoursapart
• Oliguria (<500mL in 24 hours)
• Cerebral or visual disturbance
• Pulmonary edema or cyanosis
• Epigastric or right upper quadrant pain
• Impaired liver function
• rombocytopenia or evidence of hemolysis
• Fetal growth restriction
Tese parameters are or the most part consistent with those cited in other guidelines. NICEguidelines note that although recommended as a criterion or severe preeclampsia, there is weak evidence or the association o >5 g/d o proteinuria and adverse outcomes.
SOGC guidelines also de ne preeclampsia with onset be ore 34 weeks’ gestation as severe preeclampsia.
b. Seizure prophylaxis
Seizure prophylaxis with magnesium sul ate is recommended or women with severe preeclampsia.
Seizure prophylaxis may also be considered or women with preeclampsia that is not classi ed as severe.
Guidelines uni ormly recommend magnesium sul ate in severe preeclampsia to prevent seizures;however, as noted above, severe preeclampsia de nitions are not all consistent. ACOG guidelines notethat respiration and deep tendon refexes and urine output should be monitored or women receivingmagnesium sul ate. Seizure prophylaxis should be considered or all women with preeclampsia whoare in labor.
Tere is no de nitive evidence or seizure prophylaxis in women with non-severe preeclampsia. Although there is a reported reduced risk o seizure with magnesium sul ate prophylaxis in non-severe preeclampsia, there have also been reports o an increase in cesarean delivery and other adversematernal e ects; there ore, the overall bene t o magnesium sul ate in non-severe preeclampsia isunclear. SOGC guidelines recommend consideration o magnesium sul ate in non-severe preeclampsia.
WHO guidelines recommend a ull regimen o magnesium sul ate or prevention as well as treatment.
c. Thromboprophylaxis
Preeclampsia and associated risk actors, such as obesity and immobility, increase the risk or
thromboembolic disease. These risks or thromboembolic disease should be considered when
determining the need or prophylaxis.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 41/56
Recommendations or thromboprophylaxis di er among guidelines. ACOG-AAP guidelinesrecommend thromboprophylaxis with low-dose heparin pre and postpartum or women with ahistory o thrombosis related to pregnancy or thrombosis with underlying thrombophilia. TeRoyal College o Obstetricians and Gynaecologists Guideline or Reducing the Risk o Trombosisand Embolism during Pregnancy and the Puerperium recommends assessment o risk or venous
thromboembolism (V E) and antenatal prophylaxis with low-molecular-weight heparin (LMWH)as early in pregnancy as possible or women with the ollowing risk actors: previous recurrentV E, previous unprovoked or estrogen or pregnancy-related V E, previous V E and a history o V E in a rst degree relative or documented thrombophilia. 60Tis guideline, which is usedby many New York hospitals, also recommends consideration o thromboprophylaxis antenatally or women with three or more current or persistent risk actors that include preeclampsia and risk actors or preeclampsia, such as medical comorbidity, obesity, older age and multi etal pregnancy.SOGC guidelines also note that preeclampsia and preeclampsia risk actors such as obesity, olderage and thrombophilia increase the risk or thromboembolic disease, as do other actors that may bepertinent or women with preeclampsia, such as bedrest or more than 4 days prior to delivery and
cesarean delivery. SOGC guidelines recommend consideration o thromboprophylaxis when bedresthas been prescribed. SOMANZ guidelines recommend consideration o compression stockingsor hospitalized women. Both SOGC and SOMANZ guidelines recommend consideration o postpartum thromboprophylaxis or women with preeclampsia unless it is contraindicated. RoyalCollege o Obstetricians and Gynaecologists recommend postpartum thromboprophylaxis or women with risk actors that include class three obesity (BMI > 40kg/m2), women undergoing emergency cesarean delivery, and women with two or more persistent risk actors such as preeclampsia, medicalcomorbidity, obesity, and smoking. Post partum low-molecular-weight heparin (LMWH) should notbe administered until two hours a ter epidural catheter removal.
d. Re erral/consultation
ACOG AAP guidelines recommend management o severe preeclampsia in a tertiary care setting or inconsultation with a maternal- etal medicine subspecialist. SOGC guidelines recommend mandatory OBconsultation or women with severe preeclampsia, and advise subspecialty consultation.
10. Eclampsia/HELLP syndrome
Eclampsia and HELLP syndrome are two severe mani estations o preeclampsia that require
additional management considerations.
a. Management o seizures in eclampsia
Seizures in eclampsia should be treated with magnesium sul ate.
Magnesium sul ate is rst line treatment or eclampsia, and it is administered by an IV loading doseollowed by IV in usion. Guideline-recommended dosages or magnesium sul ate administration

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 42/56
or eclampsia range rom 4 grams to 6 grams in 100cc delivered IV over 15 minutes, ollowed by anIV in usion o 1-2 grams per hour. Blood pressure, respiratory rate, urine output and deep tendonrefexes should be monitored during magnesium sul ate administration. Repeat boluses o 2-4 gramscan be administered or recurrent seizures. Other agents are considered in SOGC guidelines only i magnesium sul ate is ine ective or contraindicated, and include phenytoin and benzodiazepines.
b. Delivery timing eclampsia
Considerations or delivery timing in eclampsia include assessment o stability with regard to bloodpressure, urinary output and etal heart rate. A consensus recommendation is delivery two hours a terstability is achieved.
c. Trans usion or HELLP syndrome
SOGC guidelines cite expert consensus that platelet trans usion is indicated when platelet count is <50 x 109/L and alling, and/or there is coagulopathy. Some experts recommend platelet trans usion or
platelet count <40 x 109 prior to intubation or cesarean section. Platelet trans usion is recommendedprior to delivery or any woman with HELLP syndrome and platelet count <20 x 109/L.
HELLP syndrome has been shown to occur in approximately 20% o women with severepreeclampsia. SOGC guidelines recommend platelet trans usion when platelet count is <50 x 109/Land alling, and/or there is coagulopathy based on expert consensus. SOGC guidelines recommendconsideration o platelet trans usion or women with platelet count less than 20 x 109/L prior to vaginal delivery or cesarean section based on expert consensus o risk o pro ound hemorrhage.Prophylactic platelet trans usion is not recommended, even prior to cesarean delivery, i platelet countis >50 x 109/L and there is no excessive bleeding or evidence o platelet dys unction according toSOGC guidelines, based on air evidence. Some experts have recommended platelet trans usion orplatelet count <40 x 109 prior to intubation or cesarean section.61
d. Other therapy or HELLP syndrome
There is no clear evidence or the use o corticosteroids in HELLP syndrome.
Te use o corticosteroids or HELLP syndrome is not well de ned in the literature. Only SOGCguidelines recommend consideration o corticosteroids or HELLP syndrome or women withplatelet counts less than 50 x 109/L based on expert opinion; other guidelines, including those o the WHO, do not recommend the use o corticosteroids in HELLP syndrome. SOGC guidelinesnote insu cient evidence or plasma exchange or plasmapheresis, noting that observational studieshave suggested improved hematological and biochemical indicators, but small RCs have ound nomaternal or perinatal outcome improvement.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 43/56
11. Delivery-intrapartum care or women with HDP
a. Mode o delivery
Vaginal delivery is pre erred unless there is another indication or cesarean section.
For women with any HDP, vaginal delivery is pre erred unless cesarean delivery is required or otherindications. SOGC cites strong evidence or cervical ripening i the cervix is un avorable and vaginaldelivery is planned, based on pregnancy experience in normotensive women.
Tird stage management with oxytocin is recommended to avoid hemorrhage due to the risk o thrombocytopenia and coagulopathy in preeclampsia. Oxytocin should be administered in slow, smalldoses to minimize signi cant hemodynamic e ects.
b. Intrapartum
Tere is consensus across guidelines that antihypertensive therapy should be continued through laborand delivery to maintain blood pressure at less than 160/110. Tere is a lack o good quality RC sregarding antihypertensive treatment a ter birth.
c. Anesthesia concerns
Regional anesthesia is pre erred in women with HDP unless it is contraindicated by coagulopathy or
other condition.
All reviewed guidelines note that regional anesthesia is pre erred in women with HDP unless itis contraindicated by coagulopathy or other condition. All regional techniques appear sa e withappropriate fuid management; low-dose aspirin is not a contraindication to regional anesthesiai the platelet count is adequate and there is no coagulopathy. Regional anesthesia should not beadministered to women treated with LMWH or 12 hours a ter a prophylactic dose, and 24 hoursa ter a therapeutic dose due to the possibility o a small, but increased risk or the development o epidural hematoma in these patients. SOGC cites a threshold platelet count or regional anesthesiao >75 x 109/L unless there is coagulopathy, alling platelets, or co-administration o an anti-plateletagent (ASA) or anticoagulant (heparin). Regional anesthesia is generally sa e when platelet count is>75 x 109/L and generally contraindicated when platelet count is <50 x 109/L. For cesarean delivery,i there are no contraindications, epidural, spinal and combined spinal-epidural anesthesia is all notedto be acceptable in SOGC guidelines.
General anesthesia may pose a risk to women with chronic (preexisting) hypertension who havesevere hypertension or superimposed preeclampsia due to a hypertensive response to intubation andpossible increased risk or laryngeal edema. Women with HDP may have an increased likelihood o di cult or ailed intubation than the general population. SOMANZ guidelines note that generalanesthesia may be indicated by etal or maternal conditions, and requires early anesthesia noti cation,aspiration prophylaxis, and attenuation o pressor responses.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 44/56
d. Analgesia
SOMANZ guidelines recommend early insertion o an epidural catheter or pain i there is nocontraindication, so that the option or regional anesthesia can be maintained i conditions changerapidly. Epidural analgesia is a use ul adjunct or hypertension control and or improving renal anduteroplacental fow, since epidural analgesia can blunt pain-induced increases in blood pressurethat can be exaggerated in women with preeclampsia. SOMANZ guidelines recommend patientcontrolled entanyl or remi entanil analgesia i epidural is not possible. SOGC and SOMANZguidelines recommend avoiding non-steroidal anti-infammatory drugs (NSAIDs) post partum i hypertension is di cult to control, or i there is oliguria, elevated creatinine or platelets less than50 x 109/L. Tese agents are commonly given or analgesia and can contribute to hypertension,elevated creatinine or renal ailure.
e. Fluid balance
Women with preeclampsia have reduced plasma volume and routine uid restriction in all such women
may not be appropriate. Optimizing uid balance prior to delivery is essential, and uid balanceshould be care ully monitored in women with HDP. Fluid management or these patients, including
an intravenous (IV) uid bolus prior to administration o regional anesthesia, should be directed by an
anesthesiologist with expertise in this area.
Preeclampsia is associated with vasospasm, hemoconcentration, capillary leak and alteration in the normal volume expansion seen in pregnancy, complicating fuid management in women with preeclampsia. Women with preeclampsia have reduced plasma volume, associated with reduced serum albumin.62 Some women with preeclampsia are at increased risk or pulmonary edema, which has been associated with excess fuid administration, and pulmonary edema is a major cause o maternal mortality in thispopulation. Tere is no clear evidence or optimal fuid management in women with preeclampsia.
Te ACOG practice bulletin or chronic hypertension notes that women with chronic (preexisting)hypertension and cardiovascular or renal disease may be more susceptible to fuid overload andpulmonary edema, and there ore require particular attention to fuid balance. ACOG and NICEguidelines recommend hourly intake and output monitoring be ore delivery, and note that invasivemonitoring is rarely needed.
Women with preeclampsia are at risk or hypotension ollowing regional anesthesia/analgesia(both spinal and epidural) because they are intravascularly depleted, and steps should be taken toavoid this complication. Fluid management or these patients, including an IV fuid bolus prior toadministration o regional anesthesia, should be directed by an anesthesiologist with expertise in thisarea. Te anesthesiologist should also be responsible or management o any hypotension ollowingregional anesthesia and should provide appropriate monitoring guidelines.
ACOG-AAP Guidelines or Perinatal Care note that intrapartum oliguria is common, especially with oxytocin usage, and recommend up to three boluses o 500 cc o crystalloid i urine output is lessthan 30 cc/hr or 2 consecutive hours during labor. I oliguria persists, more accurate determination o volume status may be required.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 45/56
Recommendations or postpartum oliguria vary across guidelines. SOGC guidelines recommendtolerating oliguria (<15 mL/hr) or at least the rst six hours post partum in women withoutpreexisting renal disease or rising creatinine. ACOG-AAP guidelines note, however, that postpartumoliguria is usually due to hypovolemia and recommend initial volume replacement or oliguria with500 cc o crystalloid over 20 minutes; with consideration o packed red blood cells i oliguria persists
and the woman is anemic.
12. Postpartum and ollow-up
a. Postpartum evaluation/surveillance
Close monitoring o women with HDP is essential in the postpartum period. Many women with
preeclampsia can deteriorate postpartum. Preeclampsia and eclampsia can develop in the postpartum
period, and blood pressure in women with chronic (preexisting) hypertension is o ten unstable or 1-2
weeks postpartum. Blood pressure should be monitored at least every 4 hours postpartum, and women
should not be discharged until blood pressure has been well controlled or at least 24 hours. The ollow-up plan or monitoring o women with HDP should be clear in discharge instructions. Peak postpartum
blood pressure occurs between days 3-5 a ter birth. Blood pressure should be measured at least once in
the 3-5 day postpartum period.
Tough close ollow up is essential, there is no clear evidence or the requency o post partum ollow-up visits or women with HDP. Frequency should be clinically driven, and occur at least at the samerequency as antenatal visits. Prior to discharge, NICE guidelines recommend a written care plan toinclude who will provide ollow-up care and the requency o BP monitoring needed.
Close monitoring o blood pressure is essential in the post partum period; many women with
preeclampsia can deteriorate postpartum, and preeclampsia and eclampsia can develop in the postpartum period. Blood pressure in women with chronic (preexisting) hypertension is o ten unstableor 1-2 weeks post partum. Blood pressure, proteinuria and other adverse conditions may worsen inthe rst ew days post partum, especially in women with severe disease. Women should be evaluatedin the rst ew days post partum or symptoms such as headache and epigastric pain, as well as bloodpressure and evidence o adverse conditions. NICE guidelines recommend monitoring daily or therst two days a ter birth, with particular attention to monitoring high-risk women such as those withantenatal preeclampsia with preterm delivery, high BUN or uric acid levels.
Peak postpartum blood pressure occurs between day 3 -5 a ter birth, and hypertension may developde novo in this time rame; blood pressure should be measured at least once in this time rame. SOGCrecommends maternal surveillance at least once in the rst three days postpartum or women withpreeclampsia and as indicated i treatment is changed, with continuation o monitoring every otherday until blood pressure is normal.
Postpartum surveillance should include con rmation that the end-organ dys unction o preeclampsiahas resolved. NICE guidelines recommend monitoring platelet count, transaminases, and serumcreatinine in the 48-72 hours a ter birth or women with preeclampsia, to be repeated as clinically indicated. Derangement should resolve at 6 weeks post partum.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 46/56
b. Postpartum antihypertensive therapy
Tere is no reliable data to guide whether or not to continue antenatal antihypertensive therapy and which agent is pre erred.
Antihypertensive therapy may be restarted postpartum, especially in women with severe preeclampsia
and those who have delivered preterm according to SOGC guidelines. WHO guidelines recommendcontinuing antihypertensive treatment postpartum in women treated with antihypertensive drugsantenatally and treating women with severe postpartum hypertension with antihypertensive drugs. While there is generally consensus that severe hypertension should be treated to keep blood pressure< 160/110 mmHg, there is insu cient evidence or treating non-severe hypertension postpartum. Te JNC report suggests consideration o withholding antihypertensives or breast eeding women withblood pressure 140-159/90-99 mmHg, with close monitoring or the rst ew months while nursing.For women with gestational hypertension on antihypertensives, NICE guidelines recommendreducing and stopping antihypertensive treatment i possible, with consideration o reduction o antihypertensives i blood pressure is < 140/90 mmHg. For women with gestational hypertension who
were not previously treated with antihypertensives, NICE guidelines recommend initiating therapy postpartum or blood pressure higher than 149/99 mmHg.
For chronic (preexisting) hypertension, NICE guidelines suggest that target blood pressures shouldbe the same as long term targets or the general population, with aim to keep blood pressure lessthan 140/90 mmHg. Tis target is the same as the de nition o control in the JNC report or generalpopulations. Comorbid conditions should be considered in the treatment o non-severe hypertension.SOGC guidelines suggest that antihypertensive therapy may be used to treat non-severe post partumhypertension, particularly in women with comorbidities, and that in certain populations (diabetes,chronic kidney disease or prior stroke) a lower target o < 130/80 mmHg may be indicated.
Women with preeclampsia usually require longer antihypertensive therapy than women withgestational hypertension, but requirements vary. Although hypertension usually resolves by 6 weekspostpartum in gestational hypertension, it may persist up to 3 months or longer in severe preeclampsia.
Women who are breast eeding should be o ered in ormation regarding antihypertensive agents.SOGC guidelines note that antihypertensive agents are usually acceptable or breast eeding women,although all agents are excreted in breast milk. However, there is little data on long term e ects orthe e ect o maternal antihypertensive therapy on low birthweight or preterm in ants. Labetaloland propranolol are pre erred i beta blockers are indicated. Te JNC recommends against ACE/ ARB therapy based on reports o adverse etal and neonatal e ects and insu cient evidence o sa ety. NICE guidelines cite insu cient evidence on the sa ety o ARBs, amlodipine, and ACEinhibitors other than enalapril and captopril, although other guidelines indicate the acceptability o enalapril, captopril and quinapril during breast eeding. Diuretics can decrease lactation, and shouldbe avoided in breast eeding women. NICE guidelines recommend discontinuation o methyldopa i it is prescribed or women with chronic (preexisting) hypertension during pregnancy within 2 days o birth, with resumption o antenatal treatment to avoid the risk o depression.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 47/56
c. Follow up review/testing
Long term treatment o women with HDP should be reviewed at 2 weeks post partum or those whoremain on antihypertensives. NICE recommends a medical review or women with HDP who remainon antihypertensives two weeks a ter discharge, since many women with gestational hypertension may actually have a preexisting hypertensive disorder. SOGC guidelines recommend that women withsevere preeclampsia, especially those who presented or delivered be ore 34 weeks, should be screenedor pre-existing hypertension, underlying renal disease and thrombophilia.
SOGC guidelines recommend ollow-up o women with chronic (preexisting) hypertension thatincludes urinalysis, serum sodium, potassium and creatinine, asting glucose, asting total cholesterol,HDL cholesterol, LDL cholesterol, triglycerides and 12 lead EKG i not done previously. SOGCguidelines note that previously normotensive women with a hypertensive disorder in pregnancy may bene t rom assessment o cardiovascular risk markers.
NICE guidelines recommend a specialist or women with gestational hypertension who still needantihypertensives at their postnatal review or have ongoing proteinuria or other non- resolved abnormalindices. SOMANZ guidelines recommend that women with HDP should have annual blood pressurechecks and cardiovascular risk assessment, including lipids and glucose, at least every ve years.
d. Risk communication/li estyle counseling
Women with HDP should be advised o the risk or recurrent HDP and o uture cardiovascular risk. It is
important to note that ACOG recommends that all health encounters during a woman’s reproductive
years, particularly those that are part o preconception care, should include counseling on appropriate
health behaviors to optimize pregnancy outcomes and prevent maternal mortality.
Women should be advised o the risk or uture hypertensive disorders using plain language. All women with HDP are at risk or uture preeclampsia, and are at increased risk o uture hypertensionand its complications. Hypertension recurs in 20-50% o subsequent pregnancies o women withHDP, particularly in women with early onset o hypertension in pregnancy, a history o chronic(preexisting) hypertension, or hypertension persisting beyond 5 weeks postpartum.38
Te risk o recurrent preeclampsia is based on severity, gestation at onset, and additional maternal risk actors (chronic (preexisting) hypertension, diabetes). NICE guidelines advocate advising women withpreeclampsia o the risk o uture gestational hypertension and preeclampsia, which is more likely or women with severe preeclampsia, HELLP syndrome, eclampsia, or complications that led to birthbe ore 34 or 28 weeks.
Women with preeclampsia have a greater tendency to develop chronic hypertension than women with normotensive pregnancies. Tere are large scale epidemiologic studies showing women withgestational hypertension and especially preeclampsia to have increased risk o developing chronichypertension, renal disease and cardiovascular and cerebrovascular morbidity and mortality. Dueto the long term risk o women with HDP, speci c cardiovascular risk actors should be addressedand recommendations made or addressing them with dietary and li estyle modi cation, includingDASH diet, exercise, maintenance o ideal body weight and avoidance o tobacco. American Heart

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 48/56
AssociationGuidelines for the Prevention of Cardiovascular Disease in Womennote that relative to other women, women with preeclampsia have been shown to have nearly a two old increase in risk orischemic heart disease, stroke and venous thromboembolic disease in the ve to teen years a ter thepregnancy.63Tese guidelines suggest that the physiologic changes o pregnancy may unmask early or preexisting endothelial dys unction and vascular or metabolic disease, and there ore recommend
postpartum re erral to a primary care physician or cardiologist or women with preeclampsia ormanagement o cardiovascular risk actors.
Women should be counseled regarding amily planning to prevent pregnancy. Hospital sta andhealth care providers should ensure all women have a method o birth control prior to discharge romthe hospital post partum. Women should be in ormed that intervals between pregnancies o < 2 yearsor > 10 years are both associated with recurrent preeclampsia. Higher BMI categories are associated with increased complications and adverse outcomes, including risk or HDP. Overweight womenshould be encouraged to attain healthy BMI to decrease uture pregnancy risk and improve long termhealth. Tere is strong epidemiologic evidence that weight gain between pregnancies is associated with an increased risk or preeclampsia, even in non-obese women. Avoidance o interpregnancy weight gain or high-risk women is recommended in SOGC guidelines. For those with severe obesity,surgical management has reduced the risk o gestational hypertension in subsequent pregnancies in asmall group o women, as noted in SOGC and IOM guidelines. It is important to note that ACOGrecommends that all health encounters during a woman’s reproductive years, particularly thosethat are a part o preconception care, should include counseling on appropriate health behaviors tooptimize pregnancy outcomes and prevent maternal mortality.
13. Continuous Quality Improvement
SOMANZ guidelines recommend that hospitals monitor outcomes o women with HDP, includingmaternal mortality, composite severe adverse maternal outcomes, perinatal mortality, and rate o NICU admission o term babies.

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 49/56
Glossary of acronyms
ACE angiotensin-converting enzyme
ACOG American Congress o Obstetricians and Gynecologists
AAP American Academy o Pediatrics
ARB Angiotensin Receptor Blocker
HDP Hypertensive Disorders in Pregnancy
IOM Institute o Medicine
IUGR Intrauterine Growth Restriction
IV Intravenously
JNC Joint National Committee
LMWH Low-molecular-weight Heparin
MgSO Magnesium sul ate
MMR Maternal Mortality Review
NHBPEP National High Blood Pressure Education Program
NICE Royal College o Obstetricians and Gynaecologists National Institute orHealth and Clinical Excellence
NSAIDs Non-Steroidal Anti-in ammatory DrugsNYSDOH New York State Department o Health
SOGC Society o Obstetricians and Gynaecologists o Canada
SOMANZ Society o Obstetric Medicine o Australia and New Zealand

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 50/56

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 51/56
Endnotes Berg CJ Callaghan WM Syverson C Henderson Z. Pregnancy-related mortality in the United States - . Obstet Gynecol ;
( ): - .
Roberts JM Pearson G Cutler J Lindheimer M. Summary o the NHLBI Working Group on Research on Hypertension in Pregnancy.Hypertension ; : - .
Kuklina EV Ayala C Callaghan WM. Hypertensive Disorders and Severe Obstetric Morbidity in the United States. Obstet Gynecol ;( ): - .
Kuklina et.al. Obstet Gynecol ; ( ).
IOM (Institute o Medicine) and NRC (National Research Council). . Weight Gain during Pregnancy: Reexamining the Guidelines.Washington DC: the National Academies Press. http://www.nap.edu. Accessed December .
American College o Obstetricians and Gynecologists (ACOG). Chronic hypertension in pregnancy. Practice Bulletin number . ObstetGynecol ; ( Part ): - .
Magee LA Helewa M Moutquin J-M et al. Society o Obstetricians and Gynaecologists o Canada (SOGC). Clinical Practice Guideline-Diagnosis Evaluation and Management o the Hypertensive Disorders o Pregnancy. J Obstet Gynaecol Can ; ( Supplement ):S -S .
Kirkpatrick DH Burkman RT. Does standardization o care through clinical guidelines improve outcomes and reduce medical liability?Obstet Gynecol ; : - .
Menzies J Magee LA Li J et al. Instituting surveillance guidelines and adverse outcomes in preeclampsia. Obstet Gynecol ; : - .
Von Dadelszen P Sawchuck D McMaster R et.al. or the Translating Evidence Based Surveillance and Treatment Strategies (TESS) Group.The active implementation o pregnancy hypertension guidelines in Brit ish Columbia. Obstet Gynecol ; : - .
Institute o Medicine. Committee on Quality o Health Care in America. Crossing the quality chasm: a new health system or the stcentury. Washington DC: the National Academies Press . http://www.nap.edu. Accessed December .
Institute o Medicine. Committee on Quality o Health Care in America. Crossing the quality chasm: a new health system or the stcentury. Washington DC: the National Academies Press .
Martin JN Thigpen BD Moore RC et al. Stroke and severe preeclampsia and eclampsia: a paradigm shi t ocusing on systolic bloodpressure. Obstet Gynecol ; ( ): - .
Hermida RC Ayala DE Iglesias M. Predictable blood pressure variability in healthy and complicated pregnancies. Hypertension ;: - .
American College o Obstetricians and Gynecologists. Chronic hypertension in pregnancy. Practice Bulletin number . Obstet Gynecol; ( Part ): - .
Committee on Obstetric Practice. Committee Opinion no. : Emergent therapy or acute onset severe hypertension with preeclampsiaor eclampsia. Committee Opinion No. . Obstet Gynecol ; ( ): - .
Magee LA Helewa M Moutquin J-M et al. Society o Obstetricians and Gynaecologists o Canada (SOGC). Clinical Practice Guideline-Diagnosis Evaluation and Management o the Hypertensive Disorders o Pregnancy. J Obstet Gynaecol Can ; ( Supplement ):
S -S . Wrobel MJ Figge JJ Izzo JL. Hypertension in diverse populations: a New York State Medicaid clinical guidance document. J Am Soc
Hypertens ; ( ): - .
Committee on Obstetric Practice. Committee Opinion no. : emergent therapy or acute onset severe hypertension with preeclampsiaor eclampsia. Committee Opinion No. . Obstet Gynecol ; ( ): - .
Martin et al. Obstet Gynecol ; ( ).
Martin et al. Obstet Gynecol ; ( ).
Bergel E Carroli G Althabe F. Ambulatory versus conventional methods or monitoring blood pressure during pregnancy. CochraneDatabase o Syst Rev Issue . Art. No. CD .
American College o Obstetricians and Gynecologists. Chronic hypertension in pregnancy. Practice Bulletin number . Obstet Gynecol; ( Part ): - .
Magee LA Helewa M Moutquin J-M et al. Diagnosis evaluation and management o the hypertensive disorders o pregnancy. J ObstetGynaecol Can ; ( Suppl):S - .
Turner JA. Diagnosis and management o pre-eclampsia: an update. Int J Women’s Health ; : - .
Chronic hypertension in pregnancy. Practice Bulletin No. . American College o Obstetricians and Gynecologists (ACOG). Obstetrics andGynecology ; : - .
Rowe T Senikas V Pothier M Fairbanks J editors. Diagnosis Evaluation and Management o the Hypertensive Disorders o Pregnancy.Society o Obstetricians and Gynaecologists o Canada (SOGC). Journal o Obstetrics and Gynaecology Canada ; ( ): S -S .
Morris RK Riley RD Doug M et al. Diagnostic accuracy o spot urinary protein and albumin to creatinine ratios or detection o signi cantproteinuria or adverse pregnancy outcome in patients with suspected pre-eclampsia: systematic review and meta-analysis. BMJ ;
:e .
National Kidney Foundation. KDOQI Clinical Practice Guidelines or Chronic Kidney Disease: Evaluation Classi cation and Strati cation.Am J Kidney Dis :S -S (suppl )
Morris RK Riley RD Doug M et al. BMJ ; :e .

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 52/56
Turner JA. Int J Womens Health ; .
Turner JA. Int J Womens Health ; .
Valensise H Vasapollo B Gagiardi G Novelli GP. Early and late preeclampsia: two di erent maternal hemodynamic states in the latentphase o the disease. Hypertension ; ( ): - .
Turner JA. Int J Womens Health ; .
Report o the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Am J Obstet Gynecol; ( ):S -S .
Magee LA Helewa M Moutquin J-M et.al. J Obstet Gynaecol Can ; ( Suppl).
Royal College o Obstetricians and Gynaecologists. National Institute or Health and Clinical Excellence (NICE) Clinical Guideline-Hypertension in Pregnancy: the Management o Hypertensive Disorders during Pregnancy. August . http://publications.nice.org.uk/hypertension-in-pregnancy-cg Accessed December .
ACOG Committee on Practice bulletins--Obstetrics. Diagnosis and Management o Preeclampsia and Eclampsia. Obstet Gynecol ;( ): - .
Magee LA Helewa M Moutquin J-M et al. J Obstet Gynaecol Can ; ( Suppl).
Morris RK Riley RD Doug M et al. BMJ ; :e .
National Kidney Foundation. Am J Kidney Dis :S -S (suppl )
Morris RK Riley RD Doug M et al. BMJ ; :e .
National High Blood Pressure Education Program National Heart Lung and Blood Institute. The Seventh Report o the Joint NationalCommittee on Prevention Detection Evaluation and Treatment o High Blood Pressure. U.S. Department o Health and Human ServicesNational Institutes o Health. NIH Publication No. - . August . http://www.nhlbi.nih.gov/guidelines/hypertension/jnc ull.htmAccessed December .
World Health Organization. WHO recommendations or prevention and treatment o pre-eclampsia and eclampsia. WHO Press GenevaSwitzerland. . http://www.who.int/reproductivehealth/publications/maternal_perinatal_health/rhr_ _ /en/index.html AccessedDecember .
Magee LA Helewa M Moutquin J-M et al. J Obstet Gyn Can ; ( Suppl).
Magee LA Helewa M Moutquin J-M et al. J Obstet Gynaecol Can ; ( Suppl).
World Health Organization. WHO Press Geneva Switzerland. .
IOM (Institute o Medicine) and NRC (National Research Council). . Washington DC: the National Academies Press.
Committee on Obstetric Practice. ACOG committee opinion. Exercise during pregnancy and the postpartum period. Number January. American College o Obstetricians and Gynecologists. Int J Gynecol Obstet ; ( ): - .
Li D-K Yang C Andrade S et al. Maternal exposure to angiotensin inhibitors in the rst trimester and risk o mal ormations in o spring: aretrospective cohort study. BMJ ; : d .
Magee LA Helewa M Moutquin J-M et al. J Obstet Gynaecol Can ; ( Supplement ).
National High Blood Pressure Education Program National Heart Lung and Blood Institute. The Seventh Report o the Joint NationalCommittee on Prevention Detection Evaluation and Treatment o High Blood Pressure. U.S. Department o Health and Human ServicesNational Institutes o Health. NIH Publication No. - . August . http://www.nhlbi.nih.gov/guidelines/hypertension/jnc ull.htmAccessed December .
Nabhan AF Elsedawy MM. Tight control o mild-moderate preexisting or non-proteinuric gestational hypertension. Cochrane Database o Syst Rev ; Jul ;( ): CD .
Committee on Obstetric Practice. Obstet Gynecol ; ( ): - .
National High Blood Pressure Education Program National Heart Lung and Blood Institute. August .
Mah GT Tejani AM Musini VM. Methyldopa or primary hypertension (review). Cochrane Database o Syst Rev ; ( ):CD .
Seely EW Ecker J. Chronic hypertension in pregnancy. NEJM ; ( ): - .
Seely EW Ecker J. NEJM .
Clark SL Hankins GDV. Preventing maternal death: clinical diamonds. Obstet Gynecol ; ( Part ): - .
Royal College o Obstetricians and Gynaecologists. Reducing the risk o thrombosis and embolism during pregnancy and the puerperium.Green top guideline # a. November . http://www.rcog.org.uk/ les/rcog-corp/GTG aReducingRiskThrombosis.pd AccessedDecember .
Sibai BM. Diagnosis controversies and management o the syndrome o hemolysis elevated liver enzymes and low platelet count. ObstetGynecol ; : - .
Duley L Williams J Henderson-Smart DJ. Plasma volume expansion or treatment o pre-eclampsia. Cochrane Database Sys Rev ;( ):CD . Edited with no change to conclusions .
Mosca L Benjamin EJ Berra K et al. E ectiveness-based guidelines or the prevention o cardiovascular disease in women- update: aguideline rom the American Heart Association. Circulation ; : - .

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 53/56
Acknowledgements
New York State Department o Health
Marilyn Kacica, MD, MPHMedical Director Division o Family Health
Christopher Kus, MD, MPH Associate Medical Director Division o Family Health
Wendy Shaw, RN Associate Director Division o Family Health
Barbara Dennison, MDDirector Policy & ResearchTranslation Unit
James RaucciProgram Manager Maternal Mortality Review andPrevention
Judith White, RNHospital Nursing Services Consultant Bureau o Program Quality In ormationand Evaluation
Beverly Pasley (Retired)Director Quality Improvement UnitOfce o Quality and Patient Sa ety
NYS DOH Maternal Mortality Hypertension Subcommittee
Richard Aubrey, MD, MPHCoordinaor o Sa ety/QA o CNY-RPPUpstate Medical Center
Cynthia Chazotte, MDAmerican Congress o Obstetriciansand Gynecologists
Christina R. Christakis, MPPHealth Care Association o New York State
Joseph Izzo, MDPro essor and Chie ClinicalPharmacologySUNY Bu alo
Sandra McCalla, MDGreater New York Hospital Association
Donna Montalto, MPPExecutive Director American Congress o Obstetriciansand Gynecologists
Renee Samelson, MD, MPHMaternal Fetal Medicine Specialist Albany Medical Center
Lorraine Boyd, MD, MPHMedical Director Bureau o Maternal In ant andReproductive HealthNew York City Dept. o Health andMental Hygiene
Davic Crossland, MD, FCAPPresident New York State Society o Pathologists
Deborah Elliot, MBA, RNDeputy Executive Director New York State Nurses Association-Clinical
David Lehman, MD, PharmDUpstate University Hospital
Aleida Llanes-Oberstein, CNM,LM, MS, FACNMNew York State Association o LicensedMidwives
Daniel G. Murphy, MD, MBA, FACEPPresident New York American College o Emergency Physicians
Eileen Steinberg, MDNew York State Society o Anesthesiologists Inc.
Nikki SullivanProjects Manager New York State Medicaid PrescriberEducation Program
Wendy Wilcox, MDMaternal Fetal Medicine Specialist New York City Dept. o Health andMental Hygiene
Island Peer Review Organization (IPRO)
Jeanne Alicandro, MD, MPHMedical Director Managed Care
Paul Henfeld, MASenior Director

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 54/56

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 55/56

7/28/2019 2013 Hdp Guideline Summary
http://slidepdf.com/reader/full/2013-hdp-guideline-summary 56/56

















