See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/261881109 Miniscrew anchorage for the correction of midline discrepancies Article in Journal of clinical orthodontics: JCO · March 2014 Source: PubMed CITATION 1 READS 551 4 authors, including: Some of the authors of this publication are also working on these related projects: Accurate and Accelerated ASL View project Xue Feng Hohai University 51 PUBLICATIONS 525 CITATIONS SEE PROFILE Zhenhua Yang Fourth Military Medical University 27 PUBLICATIONS 656 CITATIONS SEE PROFILE All content following this page was uploaded by Zhenhua Yang on 13 December 2014. The user has requested enhancement of the downloaded file.
Transcript
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/261881109
Miniscrew anchorage for the correction of midline discrepancies
Article in Journal of clinical orthodontics: JCO · March 2014
Source: PubMed
CITATION
1
READS
551
4 authors, including:
Some of the authors of this publication are also working on these related projects:
Accurate and Accelerated ASL View project
Xue Feng
Hohai University
51 PUBLICATIONS 525 CITATIONS
SEE PROFILE
Zhenhua Yang
Fourth Military Medical University
27 PUBLICATIONS 656 CITATIONS
SEE PROFILE
All content following this page was uploaded by Zhenhua Yang on 13 December 2014.
The user has requested enhancement of the downloaded file.
Miniscrew Anchorage for the Correction of Midline Discrepancies
Dr. Dai Dr. Li Dr. Yang Dr. Feng
Dr. Feng is an Associate Professor, Drs. Yang and Dai are lecturers, and Dr. Li is a postgraduate student, Department of Orthodontics, School of Stomatology, Fourth Military Medical University, Xi’an, Shaanxi 710032, China. E-mail Dr. Feng at [email protected].
Midline discrepancies are commonly associ-ated with various types of malocclusion and,
from the patients’ perspective, are the most obvi-ous of all occlusal asymmetries.1 Interarch elastics and asymmetrical or sequential extractions are commonly recommended for midline correction; other proposed methods include cantilevers and asymmetrical palatal arches.2,3 Treatment is often complicated, however, by differential anchorage requirements and by such undesirable side effects as canting of the occlusal plane or loss of tip and torque from inappropriate mechanics.2
The following three cases illustrate the use of miniscrew anchorage to correct midline dis-crepancies in typical clinical scenarios.
Case 1
A 15-year-old male presented with the chief complaint of a buccally erupted ectopic maxillary right canine (Fig. 1). He had a symmetrical face and a straight profile. The molar relationship was Class II on the right side and Class I on the left, with a 2mm overjet and a 40% overbite. The max-illary midline was deviated to the right by 1.5mm due to the ectopically erupted canine. Cast analy-sis showed an arch-length discrepancy of 11mm in the upper arch and 4mm in the lower. The pano-ramic radiograph revealed the developing maxil-lary and mandibular third molars and no pathologies. Cephalometric analysis indicated a
Miniscrew Anchorage for the Correction of Midline Discrepancies
Fig. 1 Case 1. 15-year-old male patient with ectopically erupted upper right canine and upper midline deviation before treatment.
Fig. 2 Case 1. After five months of initial alignment, maxillary midline slightly deviated to left due to poor compliance with headgear wear; miniscrew inserted in right infrazygomatic crest as anchorage for midline correction.
171VOLUME XLVIII NUMBER 3
Feng, Yang, Dai, and Li
skeletal Class I relationship (ANB = 1.7°, Wits appraisal = −1mm) with a normodivergent growth pattern (SN-MP = 32°). The maxillary incisors were relatively upright (1-NA = 3mm), but the mandibular incisors were normal (IMPA = 91°).
Treatment objectives were to correct the maxillary midline discrepancy and the ectopic
position of the maxillary canine, establish a Class I molar relationship, relieve the upper crowding, and obtain a normal overjet and overbite. Considering the patient’s retrognathic profile, we believed nonextraction treatment was the best option.
A high-pull facebow was prescribed to dis-
Fig. 3 Case 1. Patient after 15 months of treatment.
172 JCO/MARCH 2014
Miniscrew Anchorage for the Correction of Midline Discrepancies
talize the upper right molars at the beginning of treatment, while an open-coil spring was placed between the upper right first premolar and lateral incisor to gain space for the buccally erupted canine and correct the upper midline. Unfor-tunately, the patient did not comply with headgear wear, and after initial leveling and alignment, the maxillary midline had deviated slightly to the left to accommodate the ectopic right canine (Fig. 2). We then placed a miniscrew in the infrazygomat-ic crest on the right side and attached a closed-coil spring from the miniscrew to a hook on the upper
archwire. After four months, the midlines were coincident and the molar relationship was Class I. Treatment was completed in 15 months (Fig. 3).
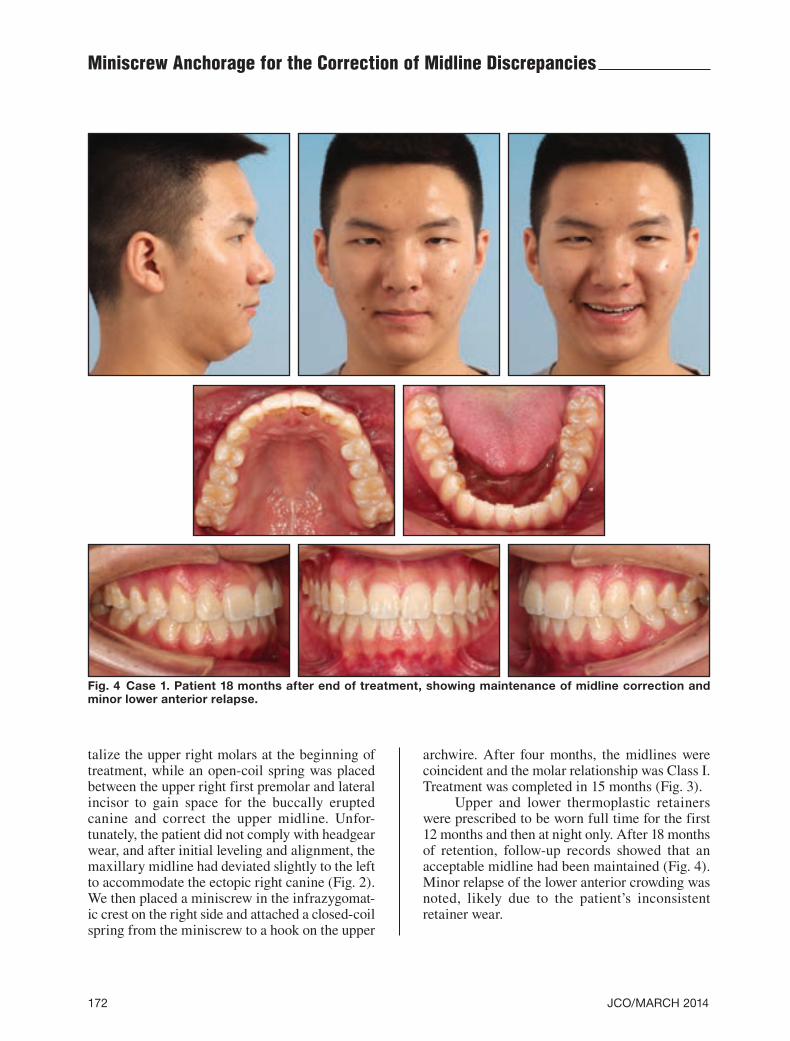
Upper and lower thermoplastic retainers were prescribed to be worn full time for the first 12 months and then at night only. After 18 months of retention, follow-up records showed that an acceptable midline had been maintained (Fig. 4). Minor relapse of the lower anterior crowding was noted, likely due to the patient’s inconsistent retainer wear.
Fig. 4 Case 1. Patient 18 months after end of treatment, showing maintenance of midline correction and minor lower anterior relapse.
173VOLUME XLVIII NUMBER 3
Feng, Yang, Dai, and Li
Case 2
A 14-year-old female presented with the chief complaint of malaligned teeth (Fig. 5). Her face was asymmetrical; a frontal radiograph revealed that the chin was deviated to the left, with the
lower midline deviated correspondingly. The patient had a Class III molar relationship on both sides, an anterior edge-to-edge occlusion, and a posterior crossbite on the left side. Cephalometric analysis showed a Class III growth tendency (ANB = −0.5°, Wits appraisal = −3.5mm).
Fig. 5 Case 2. 14-year-old female patient with deviated chin and lower midline before treatment.
174 JCO/MARCH 2014
Fig. 6 Case 2. A. Midlines remain noncoincident after six months of treatment. B. Overjet and overbite significantly increased and midlines coincident after six months of activation on left side and nine months on right, using miniscrew anchorage for retraction.
Fig. 7 Case 2. Patient after 25 months of treatment (continued on next page).
Miniscrew Anchorage for the Correction of Midline Discrepancies
A
B
175VOLUME XLVIII NUMBER 3
Feng, Yang, Dai, and Li
Fig. 7 (cont.) Case 2. Patient after 25 months of treatment.
Fig. 8 Case 2. Patient 13 months after end of treatment.
176 JCO/MARCH 2014
Miniscrew Anchorage for the Correction of Midline Discrepancies
Treatment objectives were to correct the facial asymmetry and midline discrepancy, expand the upper arch to resolve the posterior crossbite and relieve the crowding, retract the lower ante-rior teeth to obtain a normal overjet and overbite, and establish a Class I molar relationship. Given the age of the patient, a nonsurgical treatment plan was devised.
Rapid maxillary expansion was prescribed for the initial stage of treatment, followed by face-mask protraction to induce forward growth of the maxilla. After six months of orthopedic treatment, the posterior crossbite was corrected, but the mid-lines were still not coincident (Fig. 6A).
Miniscrews were then inserted bilaterally in the lower buccal interradicular regions, between
Fig. 9 Case 3. 21-year-old male patient with severe overjet and midline discrepancy before treatment.
177VOLUME XLVIII NUMBER 3
Feng, Yang, Dai, and Li
the first and second molars, and closed-coil springs were attached from the miniscrews to hooks mesi-al to the canines. The miniscrew on the right failed after eight weeks and was reinserted between the second premolar and first molar. After another six months of activation on the left side and an addi-tional three months on the right, the midlines were coincident and the overjet and overbite had in-creased substantially (Fig. 6B). The skeletal devi-ation remained, with the chin still shifted to the left (Fig. 7).
Vacuum-formed clear retainers were pre-scribed for retention. An ideal midline and normal overbite and overjet were observed 13 months after debonding (Fig. 8).
Case 3
A 21-year-old male presented with the chief complaint of upper anterior protrusion and a devi-ated lower midline (Fig. 9). The molar relationship was Class III on the right side and Class I on the left, with a 6mm overjet and 40% overbite. All four first premolars and the lower right second premo-lar had been extracted during previous orthodontic therapy; the lower midline was deviated to the
right by 2.5mm and the upper midline to the left by 1mm. Cephalometric analysis indicated a Class II skeletal pattern (ANB = 5°, Wits appraisal = +3.5mm).
Treatment objectives were to correct the upper and lower midline discrepancies, establish a Class I canine relationship, and retract the upper anterior teeth to obtain a normal overjet. After five months of initial alignment, miniscrews were inserted in the upper infrazygomatic crest between the first and second molars on both sides and in the lower left buccal interradicular region between the first and second molars (Fig. 10A). Closed-coil springs were attached between the miniscrews and the archwire hooks. After 10 months of retraction, the overjet was significantly reduced, but the upper midline was still not coordinated with the lower midline (Fig. 10B). With an additional four months of activation in the upper right and lower left quad-rants, the midlines were aligned (Fig. 10C). The patient was debonded after a total 20 months of treatment (Fig. 11).
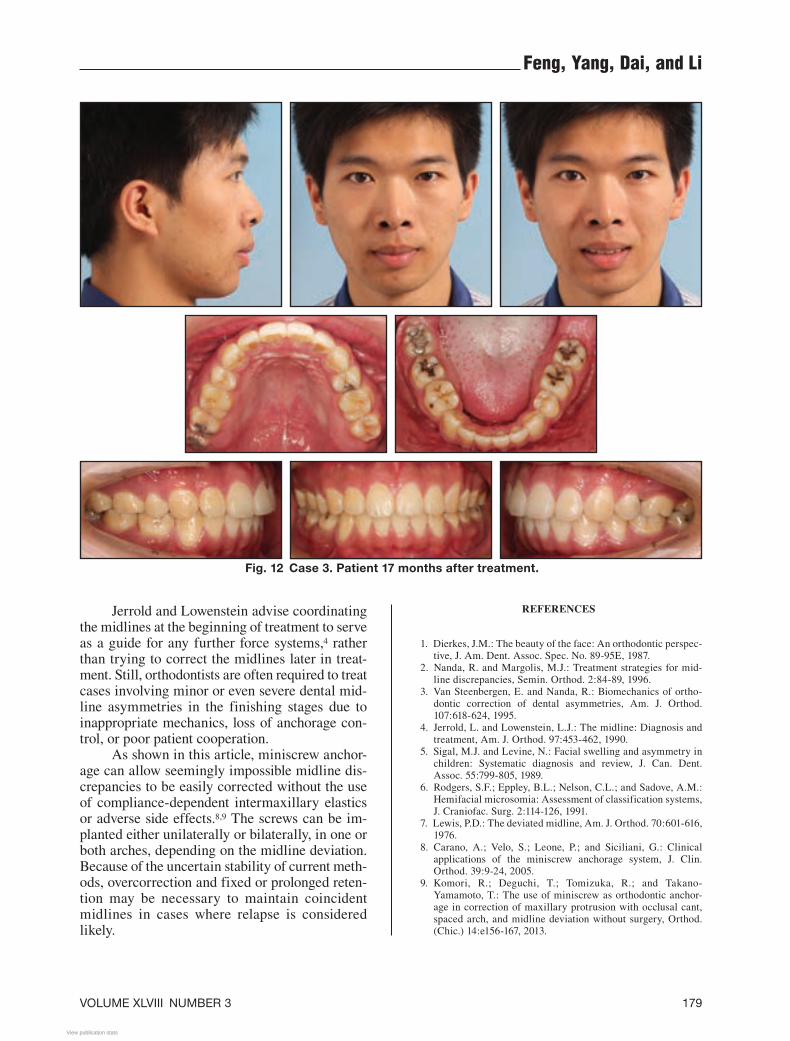
Vacuum-formed clear retainers were pre-scribed for retention. Seventeen months later, a recurrence of the midline discrepancy was noted and the canine relationship had partially relapsed
Fig. 10 Case 3. A. After five months of leveling and alignment, miniscrews inserted in upper infrazygomat-ic crest between first and second molars on both sides and in lower left buccal region between first and second molars. B. 10 months later, overjet significantly reduced, but additional midline correction need-ed. C. Coincident midlines after four more months of retraction in upper right and lower left quadrants.
B
A
C
178 JCO/MARCH 2014
Miniscrew Anchorage for the Correction of Midline Discrepancies
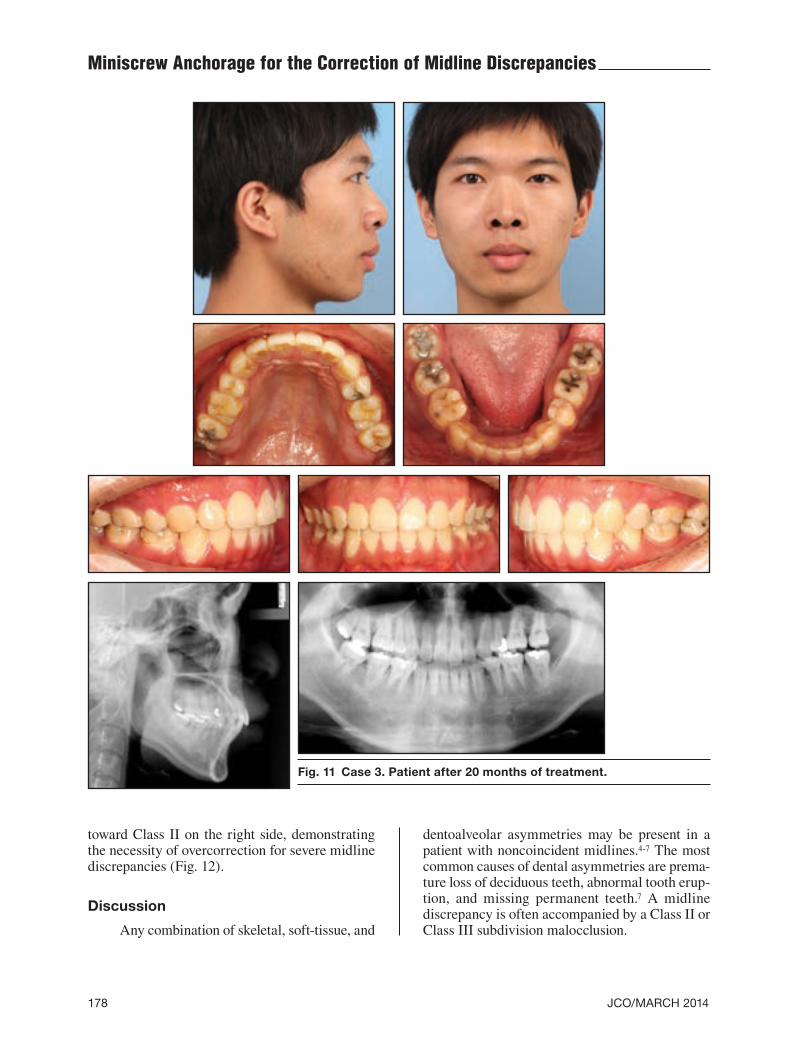
Fig. 11 Case 3. Patient after 20 months of treatment.
toward Class II on the right side, demonstrating the necessity of overcorrection for severe midline discrepancies (Fig. 12).
Discussion
Any combination of skeletal, soft-tissue, and
dentoalveolar asymmetries may be present in a patient with noncoincident midlines.4-7 The most common causes of dental asymmetries are prema-ture loss of deciduous teeth, abnormal tooth erup-tion, and missing permanent teeth.7 A midline discrepancy is often accompanied by a Class II or Class III subdivision malocclusion.
179VOLUME XLVIII NUMBER 3
Feng, Yang, Dai, and Li
REFERENCES
1. Dierkes, J.M.: The beauty of the face: An orthodontic perspec-tive, J. Am. Dent. Assoc. Spec. No. 89-95E, 1987.
2. Nanda, R. and Margolis, M.J.: Treatment strategies for mid-line discrepancies, Semin. Orthod. 2:84-89, 1996.
3. Van Steenbergen, E. and Nanda, R.: Biomechanics of ortho-dontic correction of dental asymmetries, Am. J. Orthod. 107:618-624, 1995.
4. Jerrold, L. and Lowenstein, L.J.: The midline: Diagnosis and treatment, Am. J. Orthod. 97:453-462, 1990.
5. Sigal, M.J. and Levine, N.: Facial swelling and asymmetry in children: Systematic diagnosis and review, J. Can. Dent. Assoc. 55:799-805, 1989.
6. Rodgers, S.F.; Eppley, B.L.; Nelson, C.L.; and Sadove, A.M.: Hemifacial microsomia: Assessment of classification systems, J. Craniofac. Surg. 2:114-126, 1991.
7. Lewis, P.D.: The deviated midline, Am. J. Orthod. 70:601-616, 1976.
8. Carano, A.; Velo, S.; Leone, P.; and Siciliani, G.: Clinical applications of the miniscrew anchorage system, J. Clin. Orthod. 39:9-24, 2005.
9. Komori, R.; Deguchi, T.; Tomizuka, R.; and Takano-Yamamoto, T.: The use of miniscrew as orthodontic anchor-age in correction of maxillary protrusion with occlusal cant, spaced arch, and midline deviation without surgery, Orthod. (Chic.) 14:e156-167, 2013.
Jerrold and Lowenstein advise coordinating the midlines at the beginning of treatment to serve as a guide for any further force systems,4 rather than trying to correct the midlines later in treat-ment. Still, orthodontists are often required to treat cases involving minor or even severe dental mid-line asymmetries in the finishing stages due to inappropriate mechanics, loss of anchorage con-trol, or poor patient cooperation.
As shown in this article, miniscrew anchor-age can allow seemingly impossible midline dis-crepancies to be easily corrected without the use of compliance-dependent intermaxillary elastics or adverse side effects.8,9 The screws can be im-planted either unilaterally or bilaterally, in one or both arches, depending on the midline deviation. Because of the uncertain stability of current meth-ods, overcorrection and fixed or prolonged reten-tion may be necessary to maintain coincident midlines in cases where relapse is considered likely.
Fig. 12 Case 3. Patient 17 months after treatment.













![Miniscrew Applications in Orthodontics · 2020. 12. 21. · ‘microscrews’, ‘miniscrew implants’. and ‘mini-implants’ [13,19-21]. In this chapter, we refer to them as miniscrews.](https://static.documents.pub/doc/80x56/6148d5dc2918e2056c22f27f/miniscrew-applications-in-orthodontics-2020-12-21-amicroscrewsa-aminiscrew.jpg)












