30
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014

2014 PCMH Standards: How CPCI Can Help with
Transformation
CHCANYS Quality Improvement Program November 20, 2014

Agenda
www.chcanys.org 2
• Review of PCMH 2014 Standards and Stage II MU Crosswalk
• PCMH Transformation and the CPCI

Today’s Presenters
www.chcanys.org 3
• Kathy Alexis, Director, Quality Improvement Program, CHCANYS
• Amy Grandov, Managing Director, NYS-HCCN, CHCANYS
• Heather Budd, VP of Clinical Transformation, Azara Healthcare

PCMH 2014: Key Changes
www.chcanys.org 4
• Additional emphasis on team-based care
• Care management focused on high-risk patients
• More focused, sustained Quality Improvement (QI) on patient experience, utilization, clinical quality
• Alignment with Meaningful Use stage 2
• Further integration of Behavioral Health
Adapted from NCQA’s Intro to PCMH: Foundational Concepts of the Medical Home

5
PCMH 2014 Content and Scoring (6 standards/27 elements)
1: Enhance Access and Continuity A. *Patient-Centered Appointment Access B. 24/7 Access to Clinical Advice C. Electronic Access
Pts 4.5 3.5 2
10
2: Team-Based Care A. Continuity B. Medical Home Responsibilities C. Culturally and Linguistically Appropriate
Services (CLAS) D. *The Practice Team
Pts 3 2.5 2.5 4
12
3: Population Health Management A. Patient Information B. Clinical Data C. Comprehensive Health Assessment D. *Use Data for Population Management E. Implement Evidence-Based Decision-
Support
Pts 3 4 4 5 4
20
4: Plan and Manage Care A. Identify Patients for Care Management B. *Care Planning and Self-Care Support C. Medication Management D. Use Electronic Prescribing E. Support Self-Care and Shared Decision-Making
Pts 4 4 4 3 5
20 5: Track and Coordinate Care A. Test Tracking and Follow-Up B. *Referral Tracking and Follow-Up C. Coordinate Care Transitions
Pts 6 6 6 18
6: Measure and Improve Performance A. Measure Clinical Quality Performance B. Measure Resource Use and Care Coordination C. Measure Patient/Family Experience D. *Implement Continuous Quality Improvement E. Demonstrate Continuous Quality Improvement F. Report Performance G. Use Certified EHR Technology
Pts 3 3 4 4 3 3 0 20
*Must Pass Elements Scoring Levels
Level 1: 35-59 points. Level 2: 60-84 points. Level 3: 85-100 points.

PCMH 2014 Standards and Related MU Stage 2 Alignment
11/20/2014 www.chcanys.org 6

PCMH 1: Patient-Centered Access
7
Intent of Standard The practice provides access to team-based care for both routine and urgent needs of patients/families/care-givers at all time.
A. Patient-centered appointment access B. 24/7 Access to clinical advice C. Electronic access
Adapted from NCQA’s Intro to PCMH: Foundational Concepts of the Medical Home

PCMH 1: MU Stage II Alignment
8
PCMH 1 Element C: Electronic Access aligns to: • Core 7: Provide patients the ability to view online,
download and transmit their health information within four business days of the information being available to the EP
• Core 8: Provide clinical summaries for patients for each office visit
• Core 17: Use secure electronic messaging to communicate with patients on relevant health information
https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/Stage2_MeaningfulUseSpecSheet_TableContents_EPs.pdf

PCMH 2: Team-Based Care Meaningful Use Alignment • No alignment
www.chcanys.org 9
Intent of Standard The practice provides continuity of care using culturally and linguistically appropriate, team-based approaches.
A. Continuity B. Medical Home Responsibilities C. CLAS D. The Practice Team
Adapted from NCQA’s Intro to PCMH: Foundational Concepts of the Medical Home
PCMH 3: Population Health Management
www.chcanys.org 10
Intent of Standard The practice uses a comprehensive health assessment and evidence-based decision support based on complete patient information and clinical data to manage the health of its entire patient population.
A. Patient Information B. Clinical Data C. Comprehensive Health Assessment D. Use Data for Population Management E. Implement Evidence-Based Decision Support
Adapted from NCQA’s Intro to PCMH: Foundational Concepts of the Medical Home

PCMH 3: MU Stage II Alignment
www.chcanys.org 11
PCMH 3 Element A: Patient Information aligns to: • Core 3: Record the following demographics: preferred language,
sex, race, ethnicity, date of birth
PCMH 3 Element B: Clinical Data aligns to: • Core 4: Record and chart changes in vital signs • Core 5: Record smoking status for patients 13 years old or older • Menu 2: Record electronic notes in patient records • Menu 4: Record patient family health history as structured data
https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/Stage2_MeaningfulUseSpecSheet_TableContents_EPs.pdf
PCMH 3: MU Alignment
www.chcanys.org 12
PCMH 3 Element D Use Data for Population Management aligns to: • Core 11: Generate lists of patients by specific conditions to
use for quality improvement, reduction of disparities, research, or outreach
PCMH 3 Element E Implement Evidence-Based Decision Support aligns to: • Core 6: Use clinical decision support to improve performance
on high-priority health conditions
https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/Stage2_MeaningfulUseSpecSheet_TableContents_EPs.pdf

PCMH 4: Care Management and Support
www.chcanys.org 13
Intent of Standard The practice systematically identifies individual patients and plans, manages and coordinates care, based on need.
A. Identify Patients for Care Management B. Care Planning and Self-Care Support C. Medication Management D. Use Electronic Prescribing E. Support Self-Care and Shared Decision-Making
Adapted from NCQA’s Intro to PCMH: Foundational Concepts of the Medical Home

PCMH 4: MU Stage II Alignment
www.chcanys.org 14
PCMH 4 Element C Medication Management aligns to: • Core 14: The EP who receives a patient from another setting of care or
provider of care or believes an encounter is relevant should perform medication reconciliation.
PCMH 4 Use Electronic Prescribing aligns to: • Core 1: Use computerized provider order entry (CPOE) for medication,
laboratory and radiology orders directly entered by any licensed healthcare professional who can enter orders into the medical record per state, local and professional guidelines.
• Core 2: Generate and transmit permissible prescriptions electronically (eRx).
• Core 6: Use clinical decision support to improve performance on high-priority health conditions
https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/Stage2_MeaningfulUseSpecSheet_TableContents_EPs.pdf
PCMH 4: MU Stage II Alignment
www.chcanys.org 15
PCMH 4 Element E Support Self-Care and Shared Decision-Making aligns to: • Core 13: Use clinically relevant information from Certified EHR
Technology to identify patient-specific education resources and provide those resources to the patient
https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/Stage2_MeaningfulUseSpecSheet_TableContents_EPs.pdf

PCMH 5: Care Coordination and Care Transitions
www.chcanys.org 16
Intent of Standard The practice systematically tracks, test and coordinates care across specialty care, facility based care and community organizations.
A. Track and follow-up B. Referral Tracking and Follow-up C. Coordinate Care Transitions
Adapted from NCQA’s Intro to PCMH: Foundational Concepts of the Medical Home

PCMH 5: MU Stage II Alignment
www.chcanys.org 17
PCMH 5 Element A Track and Follow-up aligns to: • Core 1 : Use computerized provider order entry (CPOE) • Core 10: Incorporate clinical lab-test results into Certified EHR
Technology as structured data • Menu 3: Imaging results consisting of the image itself and
any explanation or other accompanying information are accessible through CEHRT
https://www.cms.gov/Regulations-and-
Guidance/Legislation/EHRIncentivePrograms/Downloads/Stage2_MeaningfulUseSpecSheet_TableContents_EPs.pdf
PCMH 5: MU Stage II Alignment
www.chcanys.org 18
PCMH 5 Element B Referral Tracking & Follow-up AND Element C Coordinate Care Transitions both align to: • Core 15: The EP who transitions their patient to another
setting of care or provider of care or refers their patient to another provider of care should provide a summary care record for each transition of care or referral
https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/Stage2_MeaningfulUseSpecSheet_TableContents_EPs.pdf

PCMH 6: Performance Measurement and Quality Improvement
www.chcanys.org 19
Intent of Standard The practice uses performance data to identify opportunities for improvement and acts to improve clinical quality, efficiency and patient experience.
A. Measure Clinical Quality Performance B. Measure Resource Use and Care Coordination C. Measure Patient/Family Experience D. Implement Continuous Quality Improvement E. Demonstrate Continuous Quality Improvement F. Report Performance G. Use Certified EHR Technology Adapted from NCQA’s Intro to PCMH: Foundational Concepts of the Medical Home

PCMH 6: MU Stage II Alignment (1 of 2)
www.chcanys.org 20
PCMH 6 Element G Use Certified EHR Technology aligns to: • Core 9: Protect electronic health information created or
maintained by the Certified EHR Technology through the implementation of appropriate technical capabilities Core 12: reminders for preventive/follow-up care
• Core 16: Capability to submit electronic data to immunization registries or immunization information systems except where prohibited, and in accordance with applicable law and practice.
• Menu 1: Capability to submit electronic syndromic surveillance data to public health agencies except where prohibited, and in accordance with applicable law and practice. https://www.cms.gov/Regulations-and-
Guidance/Legislation/EHRIncentivePrograms/Downloads/Stage2_MeaningfulUseSpecSheet_TableContents_EPs.pdf

PCMH 6: MU Stage II Alignment (2 of 2)
www.chcanys.org 21
PCMH 6 Element G Use Certified EHR Technology aligns to (cont): • Menu 5: Capability to identify and report cancer cases to a
public health central cancer registry, except where prohibited, and in accordance with applicable law and practice.
• Menu 6: Capability to identify and report specific cases to a specialized registry (other than a cancer registry), except where prohibited, and in accordance with applicable law and practice.
• Clinical Quality Measures
https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/Stage2_MeaningfulUseSpecSheet_TableContents_EPs.pdf

www.chcanys.org 22
Using CPCI as a Tool to Transform Your Practice
© Azara Healthcare 2014
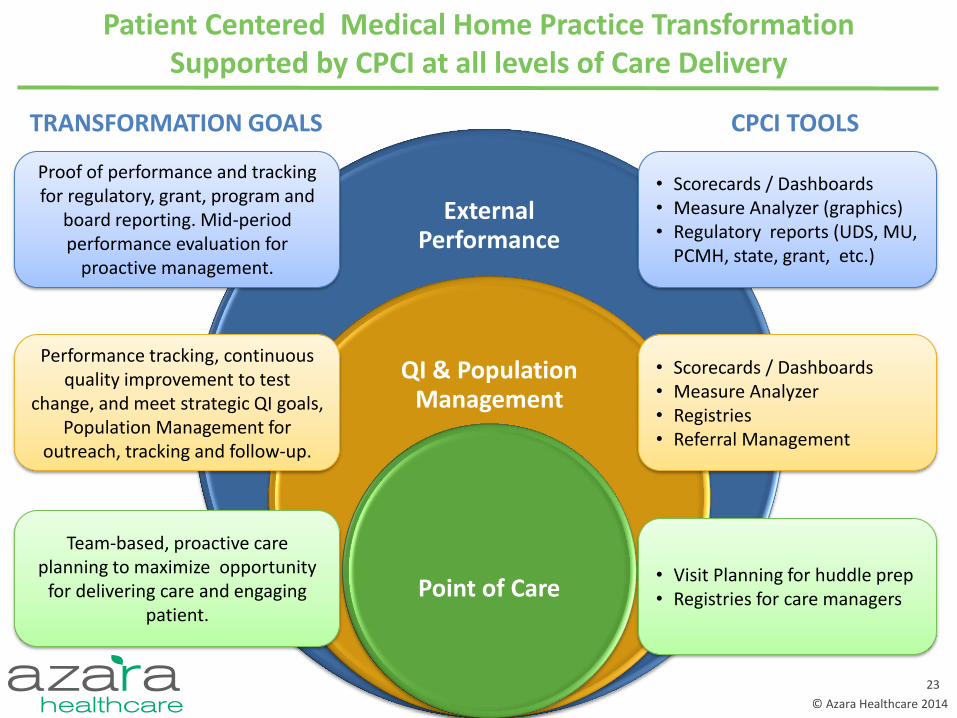
Patient Centered Medical Home Practice Transformation Supported by CPCI at all levels of Care Delivery
23
External Performance
QI & Population Management
Point of Care
Team-based, proactive care planning to maximize opportunity
for delivering care and engaging patient.
Performance tracking, continuous quality improvement to test
change, and meet strategic QI goals, Population Management for
outreach, tracking and follow-up.
• Visit Planning for huddle prep • Registries for care managers
• Scorecards / Dashboards • Measure Analyzer • Registries • Referral Management
Proof of performance and tracking for regulatory, grant, program and
board reporting. Mid-period performance evaluation for
proactive management.
• Scorecards / Dashboards • Measure Analyzer (graphics) • Regulatory reports (UDS, MU,
PCMH, state, grant, etc.)
TRANSFORMATION GOALS CPCI TOOLS

© Azara Healthcare 2014
Putting the Visit Planning Report into Daily Practice: Team Based Care Visit Planning Responsibilities
24
© Azara Healthcare 2014
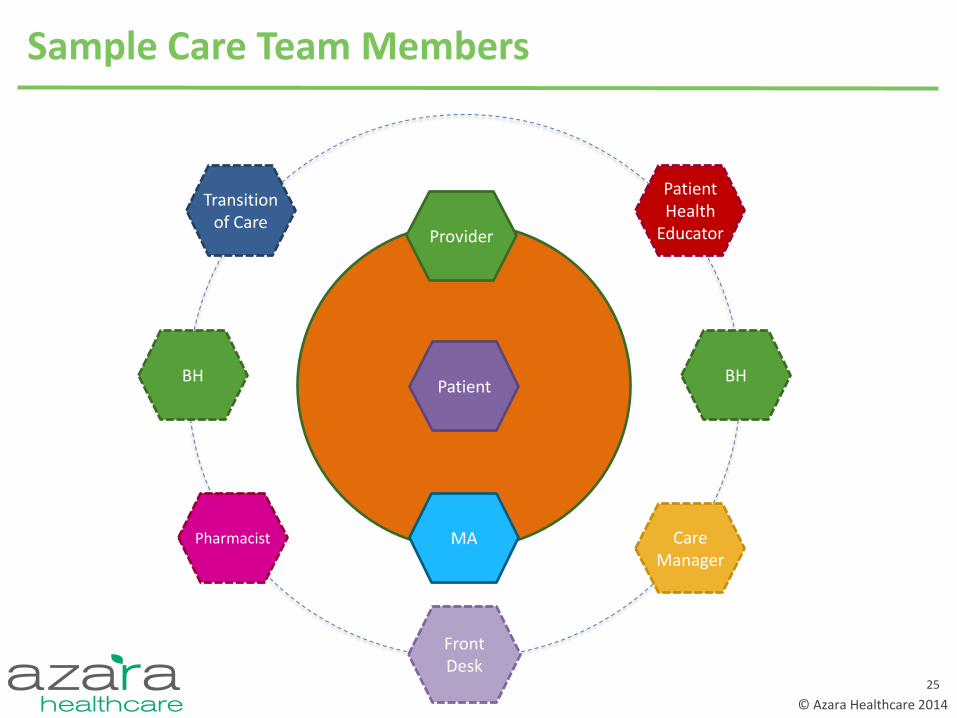
Sample Care Team Members
Provider
MA
Patient
Front Desk
Care Manager
BH
Pharmacist
Patient Health
Educator
BH
Transition of Care
25

© Azara Healthcare 2014
Visit Planning Responsibilities
MA 1. Run Azara DRVS Visit Planning Report for scheduled patients daily and for
walk-in patients if there is time.
2. Identify missing data for Diagnostics or Labs. If scanned only results exist, enter in EHR as structured data (especially Mammogram, Pap, Colonoscopy).
3. Assist Provider with completing alerts for patients, supported by standing orders. Enter reminders in the secondary chief complaint field. Primary chief complaint still used for true chief complaint. Order labs and diagnostics as needed (supported by standing orders).
4. Cancel pre-ordered labs for patients who cancel or no-show by the end of each session.
Front Desk 1. Check what has been ordered for the patient in order to charge the correct
co-pay at check in and avoid needing to send patient out to FD during visit.
26

© Azara Healthcare 2014
Visit Planning Responsibilities Health Educator/ Care Manager / Pharmacy/ BH/ Other
1. Huddle with MA to determine high risk patients to see face-to-face or offer additional education or care coordination.
2. Share any special patient circumstances with the team.
Provider 1. Delegate standing order tasks to appropriate support team members. Visit
Planning Report provides technology foundation for trust. 2. Ensure huddles are happening. May take many forms but at the very least
there should be some conversation with your MA about the plan for patients- a quick team meeting, or passing check in. Essential for MAs to feel supported when acting on Standing Orders.
3. Delete secondary chief complaint items not addressed in visit. All
1. Data Hygiene: Report data errors so they can be addressed and fixed. Workflows and inputs change overtime. Azara will find root cause and update. Send an email with details to [email protected].
27
www.chcanys.org 28
PCMH Update Timeline PCMH 2011
• PCMH 2011 survey tools are no longer available for purchase
• December 31, 2014 last date to submit PCMH 2011 Corporate survey tools
• March 31, 2015 last date to submit PCMH 2011 survey tools
PCMH 2014 Available • Standards and Guidelines • Survey tools
Adapted from NCQA’s Intro to PCMH: Foundational Concepts of the Medical Home

11/20/2014 www.chcanys.org 29
Resources
Order the PCMH 2014 Online Application from NCQA

© Azara Healthcare 2014

















