2015 EAST AFRICA EVIDENCE SUMMIT JULY 8-9, 2015 | NAIROBI, KENYA WORKING WITH VILLAGE HEALTH TEAMS (VHTS) TO INCREASE ORAL REHYDRATION SALT (ORS) USE IN UGANDA: A RANDOMIZED CONTROL TRIAL ZACHARY WAGNER, JOHN BOSCO ASIIMWE, DAVID LEVINE & WILLIAM DOW
Transcript
2 0 1 5 E A S T A F R I C A E V I D E N C E S U M M I T J U LY 8 - 9 , 2 0 1 5 | N A I R O B I , K E N Y A
WORKING WITH VILLAGE HEALTH TEAMS (VHTS) TO INCREASE ORAL REHYDRATION SALT (ORS) USE IN UGANDA: A RANDOMIZED CONTROL TRIAL ZACHARY WAGNER, JOHN BOSCO ASIIMWE, DAVID LEVINE & WILLIAM DOW
Motivation
• Diarrheal diseases are the second leading cause of child mortality under-5 (Liu et al. 2012)
• In Uganda, under 5 child mortality is 90 per 1000. Diarrhea accounts for 13% total children’s deaths
• Diarrhea is preventable. It is also cheaply treatable through the use of oral rehydration salts (ORS) (Spandorfer et al. 2005, Munos, Walker, and Black 2010)
• In Eastern Uganda, the location of the proposed study, under 40% of diarrheal cases are treated with ORS (UDHS 2011).
Background
• Working with VHTs may increase use ORS, which is key in reducing under-5 mortality in Uganda
• In 2001, government of Uganda established VHTs in an effort to increase ORS use and other health interventions in rural areas
• VHTs were brought on board due to: - Severe shortage of trained health
worker (Dambisya and Matinhur, 2012)- Health worker to population ratio in Uganda is low 1:1298 compared to recommended World
Health Organization (WHO) of 1:439 (MoFPE, 2013).
Literature Review
• Basinga, et al., 2010 – research on incentives• WHO,2007 – essential health services cannot be
provided by people working on a voluntary basis• Dambisya et al., 2012 – on diarrhoea case
management in low income countries • Wagner et al., 2014 – inconvenience for
mothers/caregivers to visit the VHTs
Location of Study
Area of Study
Intervention
• VHTs are community-based and community-run health services in Uganda
• They are not trained medical health worker• They work on voluntary basis• They are ‘self’ selected and informally confirmed by
the village leader (local council chairperson)• They are expected to be trained in 5 days (training
manual by MoH available) on a range of health care service including disease prevention & treatment
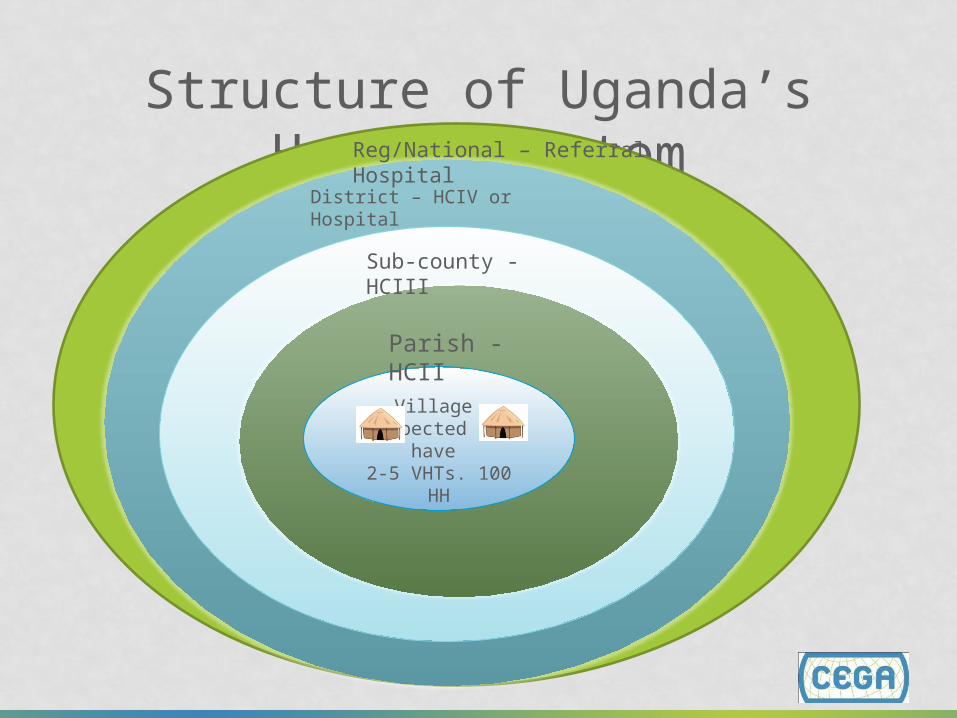
Structure of Uganda’s Health System
Village expected to have 2-5 VHTs. 100 HH
Parish - HCII
Sub-county - HCIII
District – HCIV or Hospital
Reg/National – Referral Hospital
VHT Tasks/Roles • Community mobilization and empowerment: home
visits, health records, community meetings, distribution of medical supplies.
• Health surveillance and simple treatments: disease surveillance (disease outbreaks), illness treatment, hospital referrals and monitoring of child growth
handwashing, use treated mosquito nets, immunization
Challenges
• High levels of attrition seen among VHT workers (MoH, 2013).
- Villages with presence of VHTs dropped from 78% (FY2011/12) to 55% FY2012/13
• Attrition due to being overworked and receiving no compensation (voluntary basis)
• Attrition is also due to lack of medical supplies (ORS) at the health facility
Goal of Study
This study aims to address barriers related to low ORS use, by:
- Training VHTs on proper ORS use- Educating mothers on proper ORS use- Work with VHTs to directly distribute ORS to households- Provide financial incentives to VHTs to
improve performance
Design
• Clustered randomized controlled trial - Select a region with high incidence of
diarrhoeal: Eastern region (diarrhoeal incidence 33% vs national rate is 23% (UBOS, 2012))
- Select one district within the Eastern region- Randomly select 4 sub-counties from selected district - Randomly select 68 eligible villages; 34
villages/clusters allocated to treatment 34 to control• Sample size 1,000 households; 14 households per
village
Treatment
• Treatment: Training + delivery of ORS+ ZINC to households with children under 5 (with financial compensation to VHTs for delivery)
• Control: Training of VHTs
Research Questions
• Does offering financial incentives to VHTs to deliver ORS at home increase ORS use?
• Does home delivery of ORS by VHTs reduce the time when diarrhea treatment is initiated, once a diarrhea episode starts?
Empirical Specification
•𝑌𝑖t health outcome for each selected HH i.e ORS use, time to ORS initiation, and whether ORS is stocked•Treat is a dummy for the treated=1; 0 otherwise •Post is a dummy for the intervention period i.e endline=1 and 0 otherwise•X is a vector of households characteristics (assets proxy for wealth, HH size, education level of the mother or caretaker and distance to HC) •v captures village fixed-effects •u is the individual’s error term
Yitv=δ0+Treat.Postitvδ3 +Xitvβ+Vv+uitv
Next Steps
• Conduct Formative Research- Work with the ministry of health, local health
officials, village leaders, VHTs, NGOs and mothers/caregivers to craft the intervention and assessacceptance and appropriateness of incentive
• Ensure political feasibility and buy-in of study• List villages • Average pay per VHT will be 15US$ per month (figure
based on village level wages); discuss possibility to offer different levels of incentives?