DIEGO REY, DDSADRIANA CAMPUZANO, DDSPETER NGAN, DMD
Modified Alt-RAMEC Treatment of Class III Malocclusion in Young Patients with Down Syndrome
Dr. Campuzano Dr. NganDr. Rey
Dr. Rey is Associate Professor and Chair and Dr. Campuzano is an Assistant Professor, Department of Orthodontics, Institute of Health Sciences, CES University, Medellín, Colombia. Dr. Ngan is Professor and Chair, Department of Orthodontics, West Virginia University, Morgantown, WV. E-mail Dr. Rey at [email protected].
Anatomically, DS patients tend to display inadequate orofacial development, leading to a flattened bridge of the nose and bones of the mid-face, and a prognathic mandible, resulting in Class III dental and skeletal relationships.3,4 Their over-all musculature is hypotonic; muscular weakness and anterior positioning give the appearance of an abnormally long and large tongue (relative macro-glossia). Poor facial esthetics and difficulty in eat-ing and swallowing can lead to medical and social problems that are essential to address in the early stages of development.5 Many dental conditions common to children with DS are well suited for orthodontic intervention and should be considered for correction at the appropriate time.6
Although several orthodontic treatment op-
Down syndrome (DS) is a genetic disorder caused by the presence of an extra copy of
chromosome 21, occurring once in every 600 births.1 It is characterized by some degree of cog-nitive disability and by easily recognizable physi-cal features. Thanks to recent medical advances, children with DS now have a longer life expec-tancy, which has led more parents to seek dental services such as orthodontic treatment for the typ-ical malocclusion.2 DS patients can be challenging for clinicians to manage, however, since they re-quire full commitment and collaboration from their parents or caregivers in maintaining oral hygiene and caring for their appliances.3 Detailed education of the parents and weekly appointments may be necessary to ensure proper motivation.
Modified Alt-RAMEC Treatment of Class III in Patients with Down Syndrome
Fig. 1 6-year-old female Down syndrome patient with concave profile, maxillary and malar hypoplasia, everted lower lip, mesial-step occlusal relationship, and anterior and posterior crossbites before treatment.
115VOLUME XLIX NUMBER 2
Rey, Campuzano, and Ngan
anterior crossbite and poor upper-jaw growth. Clinical examination showed a concave profile with malar and maxillary hypoplasia, a retrusive maxilla, mandibular protrusion, counterclockwise rotation of the mandible, and deficient lower facial height. The deciduous teeth were in mesiocclusion, with anterior and posterior crossbites, a deep over-bite, and retroclined upper incisors (Fig. 1). Ceph-alometric evaluation (Table 1) indicated a skeletal Class III growth pattern (ANB = −2.0°, Wits ap-praisal = −11.6mm) and a flat mandibular plane (FMA = 15.3°). The upper and lower incisors were both retroclined, with an overjet of −3.5mm.
Treatment objectives were to protract the maxilla for enhanced malar projection and antero-posterior growth, to resolve the crossbite, and to improve the facial profile. Options included the conventional protocol of rapid palatal expansion combined with a Delaire facemask.16 Another al-ternative was to use Class III elastics, anchored by mini-implants between the maxillary molars and the mandibular symphysis, to achieve the ortho-pedic effects needed for skeletal Class III correc-tion.17,18 Other possibilities were to wait until after
tions have been suggested for DS patients in early childhood,7 few authors have focused on the reso-lution of midface deficiency.8 Rapid palatal ex-panders have been used to provide space for align-ing crowded teeth and correcting posterior crossbite while improving nasal patency.7 Maxil-lary protraction or facemask devices have been employed in conjunction with expanders to resolve skeletal anteroposterior jaw discrepancies.9-12 Liou and Tsai proposed the use of an alternate maxillary expansion and constriction (Alt-RAMEC) protocol to disarticulate the maxillary sutures and thus fa-cilitate forward movement of the maxilla.13 This method has been shown to be effective in manag-ing cleft lip and palate patients with midface defi-ciencies.8 The present article describes the treat-ment of young DS patients with maxillary deficiencies using the Alt-RAMEC protocol and maxillary protraction.
Diagnosis and Treatment Plan
A 6-year-old female was brought in for eval-uation by her mother, with the chief concerns of
Modified Alt-RAMEC Treatment of Class III in Patients with Down Syndrome
the pubertal growth spurt and camouflage the malocclusion by extracting the lower first premo-lars, or to wait until the cessation of growth and perform maxillary advancement surgery.19,20 The parents did not want to wait that long to begin treatment, however, and they declined the use of mini-implants because of the cost.
We therefore proposed a treatment plan in-volving the use of Alt-RAMEC13-15 to disarticulate the maxillary sutures, followed by maxillary pro-traction with a facemask to correct the anteropos-terior jaw discrepancy. Apprised of the reported effectiveness of this procedure in early child-hood,13,14 as well as the potential complications and risks of treatment, the parents signed an informed-consent agreement. The family was made aware of the importance of cooperation in achieving a successful outcome.
Treatment Progress
A Hyrax* rapid palatal expander was bonded in place, and .045" buccal wires were extended from the acrylic forward to the canine areas, end-ing in hooks for the attachment of elastics from the facemask (Fig. 2). The expansion/constriction protocol was modified from the recommendation of Liou and Tsai13 as follows (Table 2): The patient was instructed to activate the appliance one-
quarter turn in the morning and one-quarter turn in the evening for the first week (expansion), then to turn the jackscrew backward at the same rate during the second week (constriction). This alter-nation was continued for five weeks, ending in an expansion week.
After the expansion/constriction protocol, a facemask with adjustable forehead padding, chin cup, and anterior bar was placed, and a force of 400-500g per side was delivered using ³⁄16", 14oz elastics (Fig. 3). To avoid opening the bite as the maxilla was protracted, the elastics were attached to the hooks near the maxillary canines with a downward and forward pull of 30° to the occlusal plane. The patient was instructed to wear the pro-traction facemask 10-12 hours a day for 12 months, until the molars were overcorrected to a Class II relationship.15 A lower-anterior inclined plane was then placed for three weeks to increase the angula-tion of the upper incisors (Fig. 4).
Fig. 2 Bonded Hyrax* expander with posterior biteplane and protraction hooks for attachment of elastics from facemask.
Fig. 3 Facemask with elastics pulling 30° forward and downward from occlusal plane.
*Registered trademark of Dentaurum, Inc., Newtown, PA; www.dentaurum.com.
117VOLUME XLIX NUMBER 2
Rey, Campuzano, and Ngan
facial esthetics in DS patients.25 Oral hygiene dur-ing this regimen was fairly poor, however, and the technique does not address anteroposterior skeletal problems. González and colleagues reported pos-itive results in a Class III DS patient using ortho-dontic camouflage treatment after extraction of the lower first premolars.26
In 2005, Liou and Tsai proposed the Alt-RAMEC protocol to disarticulate the maxillary sutures and enhance forward movement of the maxilla by means of protraction springs.13,14 This procedure resulted in more than 5mm of maxillary protraction, compared to only 2mm using one-time expansion and protraction. Wang and colleagues also found much greater opening of the maxillary sutures with the Alt-RAMEC protocol, although it did require more than five weeks of expansion and constriction.27 On the other hand, Do-deLatour and colleagues observed no difference in forward movement of the maxilla between the Alt- RAMEC and one-time expansion protocols.28 This pilot study used a different expansion/constriction device from the one described by Liou and Tsai,13 however, and required patient cooperation in wear-ing the facemask.
In another study, Isci and colleagues mea-sured differences between the two protraction protocols in Class III patients with an average age of 11½.29 In the rapid palatal expansion group, the jackscrew was activated .2mm twice a day for a week. In the expansion/constriction group, subjects alternated .2mm of opening twice a day for a week with .2mm of closing twice a day for the next
Treatment Results
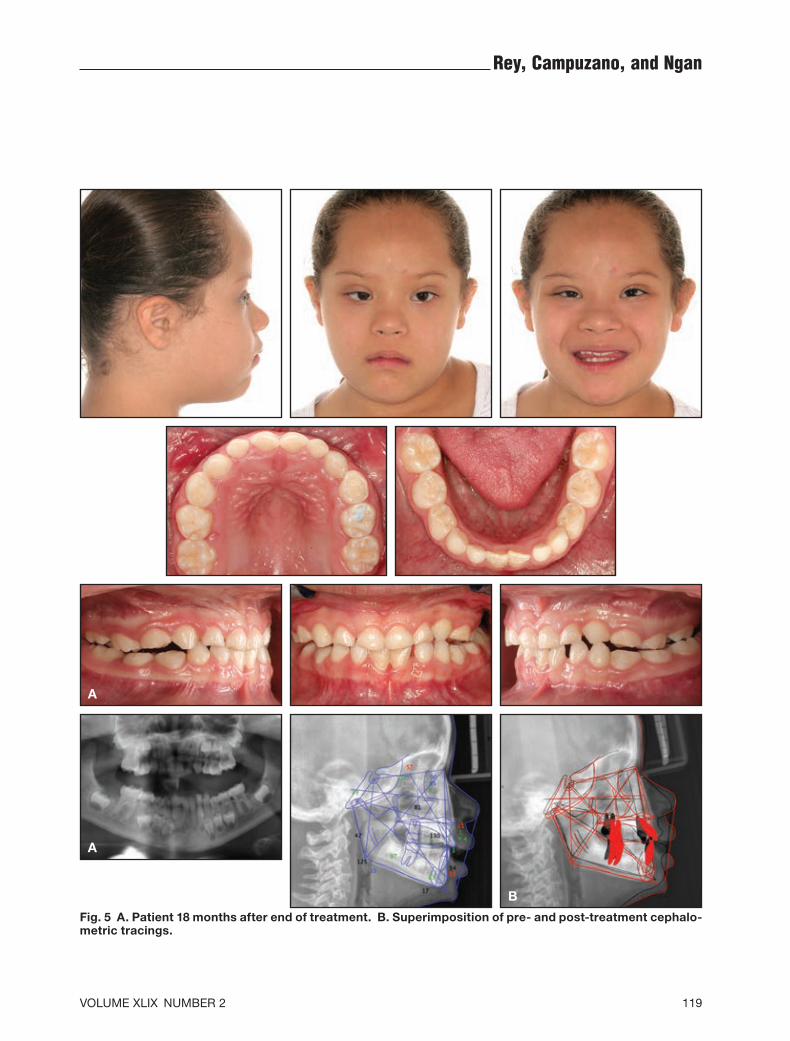
Eighteen months after treatment, the patient exhibited adequate overbite and overjet and good facial balance (Fig. 5A). A significant improve-ment was observed in the soft-tissue convexity of the profile, with the midface projected forward, the lip position normalized, and the lower facial height increased. Cephalometric analysis con-firmed that the posterior occlusion had improved to a straight terminal plane (Fig. 5B, Table 1). The anterior crossbite was corrected, as were the an-gulation of the upper incisors (99.5° to 122.9°) and lower incisors (80.3° to 86.7°). Significant skeletal changes were also observed: A point advanced by 4.2mm, the maxilla increased in size by 5mm, SNA improved by 3.6°, B point was retracted by 2.3mm, SNB was reduced by 4°, mandibular rota-tion remained stable, and the anterior facial height and Wits appraisal improved substantially.
Discussion
Some 65% of DS patients present with Class III malocclusions due to maxillary hypoplasia.6 Most of these malocclusions are severe,21,22 making it even more important to consider early orthope-dic treatment.13 Several methods have been pro-posed to enhance perioral muscle function, breath-ing, swallowing, and chewing.6,23,24 Pietrzak and Kowalska recommended the use of removable plates, as described by Castillo-Morales,23,24 fol-lowed by Schwarz plates to improve speech and
Modified Alt-RAMEC Treatment of Class III in Patients with Down Syndrome
tion without dental effects, a clockwise mandibular rotation with slight inclination of the lower inci-sors, an increased vertical dimension, and a sig-nificant improvement in facial profile and poste-rior displacement of the chin.30
The treatment protocol used for the DS pa-tient shown here was originally proposed by Fran-chi and colleagues.15 We preferred to treat the patient at a younger age, however, to reduce the risk of periodontal problems from the Alt-RAMEC protocol. In addition, the treatment would be less effective after the pubertal growth spurt due to ossification of the circummaxillary sutures.15 The results of our case were similar to those observed by Franchi and colleagues in non-DS patients. In the two cases reported by Franchi and colleagues,15 SNA increased by an average 4.4°, compared to our increase of 3.6°; on the other hand, Liou14 and Isci and colleagues29 reported increases of only 3.4°. Franchi and colleagues measured an average decrease of 3.5° in SNB; both Liou and Isci and colleagues noted decreases of 1.6°, whereas our patient showed a more substantial decrease of 4°. Franchi and colleagues found an average advance-ment in A point of 3.6mm, compared to 4.2mm of advancement in our case, while Liou reported 5.8mm of advancement and Isci and colleagues 3mm. We also noted an improvement of 10mm in the Wits appraisal, which improved by an average of only 3.2mm in Franchi and colleagues’ study. Franchi and colleagues observed an average 1.9° clockwise mandibular rotation, while our patient’s jaw remained stable.
It is important to note that the few published studies of the Alt-RAMEC protocol have been inconsistent in terms of age, type of device, hours
week, repeating the procedure over four weeks. Each patient was then instructed to wear a face-mask with a force of 700g per side 16-18 hours a day, followed by three months of Class III elastics. Corroborating the findings of Liou and Tsai,13 as well as the present report, the expansion/constric-tion group showed a 4.13mm advancement of A point vs. 2.33mm in the rapid palatal expansion group. Both groups exhibited clockwise mandib-ular rotation and increased anterior facial height.29
Yen analyzed the effects of the Alt-RAMEC protocol in a sample of adolescent patients with cleft lip and palate.8 Activation and deactivation of the Hyrax expansion screw were performed over nine weeks. Maxillary protraction springs were not used because the author felt they fractured too easily and produced anterior bite opening in most cases. Instead, each patient was instructed to wear a facemask at night and Class III elastics during the day to retain the nighttime protraction effects. The facemask was worn until an overcorrected Class II molar relationship was achieved. In 24 of 30 patients, the treatment produced an 8-9mm overjet, along with rotation of the occlusal plane and dentoalveolar compensation.8
Another modification of the Alt-RAMEC protocol, using skeletal anchorage to minimize dental side effects, was introduced in 2011 by Kaya and colleagues.30 The expansion/constriction pro-tocol was performed with an activation of .5mm per day for eight weeks. Miniplates were then surgically inserted for attachment of the elastics to the facemask, so that the force would be directed between the lateral incisors and upper canines. The authors found significant forward movement of the maxilla, a slight counterclockwise maxillary rota-
Fig. 4 After 12 months of protraction, lower inclined plane placed to increase inclination of upper incisors.
119VOLUME XLIX NUMBER 2
Rey, Campuzano, and Ngan
Fig. 5 A. Patient 18 months after end of treatment. B. Superimposition of pre- and post-treatment cephalo-metric tracings.
A
A
B
120 JCO/FEBRUARY 2015
Modified Alt-RAMEC Treatment of Class III in Patients with Down Syndrome
of use, and other variables. Nevertheless, all stud-ies except the one by Do-deLatour and colleagues28 have shown superior correction of Class III mal-occlusion due to maxillary hypoplasia, as com-pared to the combination of rapid palatal expansion and facemask therapy. Future researchers should consider using a well-defined protocol with large samples at similar ages, either in normal patients or in patients with DS, to obtain reliable results on which clinical practices can be based.
REFERENCES
1. Petersen, M.B. and Mikkelsen, M.: Nondisjunction in trisomy 21: Origin and mechanisms, Cytogenet. Cell Genet. 91:199-203, 2000.
2. Outumuro, M.; Abeleira, M.T.; Caamaño, F.; Limeres, J.; Suarez, D.; Diz, P.; and Tomas, I.: Maxillary expansion thera-py in children with Down syndrome, Pediat. Dent. 32:499-504, 2010.
3. Rada, R.; Bakhsh, H.H.; and Evans, C.: Orthodontic care for the behavior-challenged special needs patient, Spec. Care Dent., published online July 23, 2014.
4. Faulks, D.; Collado, V.; Mazille, M.N.; Veyrune, J.L.; and Hennequin, M.: Masticatory dysfunction in persons with Down’s syndrome, Part 1: Aetiology and incidence, J. Oral Rehab. 35:854-862, 2008.
5. Faulks, D.; Mazille, M.N.; Collado, V.; Veyrune, J.L.; and Hennequin, M.: Masticatory dysfunction in persons with Down’s syndrome, Part 2: Management, J. Oral Rehab. 35:863-869, 2008.
6. Musich, D.R.: Orthodontic intervention and patients with Down syndrome, Angle Orthod. 76:734-735, 2006.
7. De Moura, C.P.; Vales, F.; Andrade, D.; Cunha, L.M.; Barros, H.; Pueschel, S.M.; and Clemente, M.P.: Rapid maxillary ex-pansion and nasal patency in children with Down syndrome, Rhinol. 43:138-142, 2005.
8. Yen, S.L.: Protocols for late maxillary protraction in cleft lip and palate patients at Children’s Hospital Los Angeles, Semin. Orthod. 17:138-148, 2011.
9. Baccetti, T.; Franchi, L.; and McNamara, J.A. Jr.: Treatment and posttreatment craniofacial changes after rapid maxillary expansion and facemask therapy, Am. J. Orthod. 118:404-413, 2000.
10. Ngan, P.; Yiu, C.; Hu, A.; Hägg, U.; Wei, S.H.; and Gunel, E.: Cephalometric and occlusal changes following maxillary ex-pansion and protraction, Eur. J. Orthod. 20:237-254, 1998.
11. Vaughn, G.A.; Mason, B.; Moon, H.B.; and Turley, P.K.: The effects of maxillary protraction therapy with or without rapid palatal expansion: A prospective, randomized clinical trial, Am. J. Orthod. 128:299-309, 2005.
12. Turley, P.K.: Managing the developing Class III malocclusion with palatal expansion and facemask therapy, Am. J. Orthod. 122:349-352, 2002.
13. Liou, E.J. and Tsai, W.C.: A new protocol for maxillary pro-traction in cleft patients: Repetitive weekly protocol of alter-nate rapid maxillary expansions and constrictions, Cleft Pal. Craniofac. J. 42:121-127, 2005.
14. Liou, E.J.: Effective maxillary orthopedic protraction for growing Class III patients: A clinical application simulates distraction osteogenesis, Prog. Orthod. 6:154-171, 2005.
15. Franchi, L.; Baccetti, T.; Masucci, C.; and Defraia, E.: Early Alt-RAMEC and facial mask protocol in Class III malocclu-sion, J. Clin. Orthod. 45:601-609, 2011.
16. Delaire, J.: Maxillary development revisited: Relevance to the orthopaedic treatment of Class III malocclusions, Eur. J. Orthod. 19:289-311, 1997.
17. De Clerck, H.; Cevidanes, L.; and Baccetti, T.: Dentofacial ef-fects of bone-anchored maxillary protraction: A controlled study of consecutively treated Class III patients, Am. J. Orthod. 138:577-581, 2010.
18. De Clerck, E.E. and Swennen, G.R.: Success rate of miniplate anchorage for bone anchored maxillary protraction, Angle Orthod. 81:1010-1013, 2011.
19. Jacobs, C.; Jacobs-Müller, C.; Hoffmann, V.; Meila, D.; Erbe, C.; Krieger, E.; and Wehrbein, H.: Dental compensation for moderate Class III with vertical growth pattern by extraction of the lower second molars, J. Orofac. Orthop. 73:41-48, 2012.
20. De Paula, L.K.; Ruellas, A.C.; Paniagua, B.; Styner, M.; Turvey, T.; Zhu, H.; Wang, J.; and Cevidanes, L.H.: One-year assessment of surgical outcomes in Class III patients using cone beam computed tomography, Int. J. Oral Maxillofac. Surg. 42:780-789, 2013.
21. Abdul Rahim, F.S.; Mohamed, A.M.; Nor, M.M.; and Saub, R.: Malocclusion and orthodontic treatment need evaluated among subjects with Down syndrome using the Dental Aesthetic Index (DAI), Angle Orthod. 84:600-606, 2014.
22. Bauer, D.; Evans, C.A., BeGole, E.A.; and Salzmann, L.: Severity of occlusal disharmonies in Down syndrome, Int. J. Dent., published online Aug. 15, 2012.
23. Hoyer, H. and Limbrock, G.J.: Orofacial regulation therapy in children with Down syndrome, using the methods and appli-ances of Castillo-Morales, ASDC J. Dent. Child. 57:442-444, 1990.
24. Schuster, G. and Giese, R.: Retrospective clinical investiga-tion of the impact of early treatment of children with Down’s syndrome according to Castillo-Morales, J. Orofac. Orthop. 62:255-263, 2001.
25. Pietrzak, P. and Kowalska, E.: Possibilities of orthodontic-or-thopaedic treatment in patients with Down syndrome, based on review of literature and on own observations, Pediat. Pol. 87:626-632, 2012.
26. González, L.M. and Rey, D.: Orthodontic treatment of a pa-tient with Down syndrome, Rev. CES Odont. 26:136-143, 2013.
27. Wang, Y.C.; Chang, P.M.; and Liou, E.J.: Opening of circum-maxillary sutures by alternate rapid maxillary expansions and constrictions, Angle Orthod. 79:230-234, 2009.
28. Do-deLatour, T.; Ngan, P.; Martin, C.A.; Razmus, T.; and Gunel, E.: Effect of alternate maxillary expansion and con-traction on protraction of the maxilla: A pilot study, Hong Kong Dent. J. 6:72-82, 2009.
29. Isci, D.; Turk, T.; and Elekdag-Turk, S.: Activation-deactivation rapid palatal expansion and reverse headgear in Class III cases, Eur. J. Orthod. 32:706-715, 2010.
30. Kaya, D.; Kocadereli, I.; Kan, B.; and Tasar, F.: Effects of facemask treatment anchored with miniplates after alternate rapid maxillary expansions and constrictions: A pilot study, Angle Orthod. 81:639-646, 2011.