In this issue Acute Pathology Costing Practice Makes Perfect for the FRCPath Analyte Monographs are Fun Peter and Vincent Down on the Farm ACBNI Spring Meeting Focus on Autoimmunity The Association for Clinical Biochemistry & Laboratory Medicine | Issue 640 | August 2016 ACB News
Transcript
In this issue
Acute PathologyCosting
Practice Makes Perfect for the FRCPath
AnalyteMonographsare Fun
Peter and Vincent Down on the Farm
ACBNI Spring Meeting
Focus on Autoimmunity
The Association for Clinical Biochemistry & Laboratory Medicine | Issue 640 | August 2016
ACBNews
About ACB NewsThe Editor is responsible for the finalcontent. Views expressed are not necessarily those of the ACB. EditorProfessor Jonathan BergDepartment of Clinical BiochemistryCity HospitalDudley RoadBirmingham B18 7QHTel: 07792-912163/0121-507-5353Fax: 0121-507-5290Email: [email protected]
Associate Editors Mrs Sophie BarnesDepartment of Clinical Biochemistry12th Floor, Lab BlockCharing Cross HospitalFulham Palace RoadLondon W6 8RFEmail: [email protected]
Dr Gina Frederick Pathology Laboratory, Level 5Royal Derby HospitalUttoxeter RoadDerby DE22 3NEEmail: [email protected]
Mr Ian HanningDepartment of Clinical BiochemistryHull Royal InfirmaryAnlaby RoadHull HU3 2JZEmail: [email protected]
Dr Derren Ready Microbial DiseasesEastman Dental Hospital University College London Hospitals (UCLH) 256 Gray’s Inn Road London WC1X 8LD Email: [email protected]
Front cover: A break frompractising an FRCPath mock inBirmingham for Clinical Scientistand Specialist Registrar Trainees
ACB Response to NHS Improvement’s Letterto NHACS TrustsDr Gwyn McCreanor, ACB President, on behalf of the ACB Council
4 | General News
ACB News | Issue 640 | August 2016
All NHS Trust CEOs and Chairs received a letterfrom NHS Improvement on 28th June 2016outlining the financial position for 2016/17and describing actions to be taken toeradicate a substantial proportion of thedeficit. One of the three areas highlighted foraction is ‘Back office and PathologyConsolidation – Carter Implementation’. The Sustainability and Transformation leadsare being asked to develop proposals toconsolidate back office and Pathology servicesby the end of July 2016. This is anunreasonably short timescale for sensibleplans to be developed. Many PathologyDepartments are already working in networksor developing plans around clinicalcollaboration. Imposing this four weekdeadline to develop plans may damage theongoing planning processes and rushing toproduce plans is more likely to cost moneythan deliver savings. Pathology is not a backoffice function, it is a clinical serviceembedded in patient pathways. ACB membersare highly trained clinical professionals whodeliver excellent healthcare to our patients in
Primary and Secondary Care. Many of ourmembers are out on wards and in clinicsdelivering patient care and interpretingdiagnostic investigations for our clinicalcolleagues. Pathology across the country hasalready made significant savings, not least theefficiencies delivered by managing a hugeincrease in workload at marginal costsresulting in a decrease in the actual cost perresult. There is no evidence that consolidationis the way forward for Pathology.Consolidation is certainly not the best way todrive efficiencies as demonstrated by the factthat Cambridge University Hospitals (CUH) hasjust announced that they will pull out of thePathology Partnership. The partnership had adeficit of £15 million last year and £4.5 millionin the previous year. Withdrawal from thepartnership will cost CUH £5 million and takeabout a year to complete. The ACB urges NHSImprovement to withdraw this request andsupport departments with their current plans.One size will not fit all services as local patientdemographics and clinical needs dictatedifferent service delivery models. �
Sudoku This month’s puzzleLast month’s solution
ACB News | Issue 640 | August 2016
6 | General News
Practice Makes PerfectThere is nothing that scares our Trainees morethan the thought of the FRCPath PracticalExam. That mix of short answer questions andthen the “wet”, and not so wet, practical leadto some of the best stories of wow andpressure from all our careers. For the last twelve years the Clinical
Biochemistry Department at Sandwell & WestBirmingham Hospital has been organising aone day mock practical day. Every time thelaboratory does it the message goes out that itwill be the last time . . . but then thosepleading phone calls start coming in and weend up doing it again. In July eight Traineesput themselves through the experience and
even offered to fill the front cover of ACBNews in their very short lunchtime break. Best of luck to you all! �
ACB Scotland National Autumn MeetingMonday 24th OctoberSteele Lecture Theatre, Perth Royal Infirmary10.00-10.30 Registration10.30-12.00 Members’ Papers & John King Award10.30-11:00 Demand Optimisation in Primary Care
Dr Mark Lum11:00-11.30 What Happens to Phoned Results?
Dr Jennifer Johnstone11:30-12:00 Development of an LC-MS Method for Biomarkers of Alcohol Ingestion
Dr Emma Dewar 12.10-13.00 Lunch13.00-14.30 AKI 13.00-13.30 Clinical Aspects of AKI
Dr Samira Bell13.30-14.00 Laboratory Aspects of AKI
Dr Ian Godber14.00-14.30 AKI: Current and Future Issues
Dr Bill Bartlett14.30-15.00 Coffee Break15.00-16.00 Renal15.00-15.30 Proteinuria 2016: Still Bad for You
Professor Neil Turner15.30-16.00 CKD in the Era of Realistic Medicine
Dr Mark MacGregor
Registration closes: Friday 7th October 2016Please register for this meeting via www.acb.org.uk
Public and Private Down on the Farm The second in our series of interviews withPeter Wilding and Vincent Marks can now beviewed online. They start by considering theMSc courses that both Guildford with VincentMarks, and Birmingham with Tom Whitehead,oversaw. Vincent points to the pleasure ofcoming to Focus meetings and seeing hisformer students leading the profession,though of course many have now retired!Two 1980s meetings on Point of Care Testing
at Guildford pioneered what is now amainstream part of every laboratory’s work.They were internationally popular and set the scene for what is now commonplace. Why have we moved so slowly with POCT?Peter points out that really glucose testing hasbeen the only real test and he suggests muchPOCT glucose testing in the modern hospital is unnecessary. Peter describes how he went to work for
Technicon Corporation and how he learnt justhow much professionalism and competencethere was in the commercial sector. Labsperhaps struggle to understand just howmuch effort commercial organisations take tobring products into the laboratory. Vincent ofcourse established several companies to
commercialise ideas. The Guildhay company inparticular supplied antisera first to hisGuildford research team and later to otherlaboratories. Vincent remembers how he gothold of a farm from an old mental healthhospital. He had sheep, donkeys and rabbitsto produce antibodies and when monoclonalscame along Vincent set up another companyto purify them. �
� To see the video just put ‘Public and Private down on the farm Youtube’ intoyour search engine.
Issue 640 | August 2016 | ACB News
General News | 7
Peter, Jonathan and Vincent look at the start of POCT and commercial work in 1980s clinical biochemistry
Click on this thumbnail to go to the video from thePDF edition
Lord Carter of Coles’ Review ofOperational Productivity andPerformance in English NHSAcute Hospitals: UnwarrantedVariations was published in February 2016 and sets out recommendations to improveefficiency in NHS Acute Hospitals
The Report states that they have developed anational set of benchmarks and indicators aspart of the model hospital that will allowTrusts to compare their services with theirpeers in terms of quality and cost. NHS Improvement have requested plans by
the end of July and as yet the benchmarks arenot available to allow this comparison. The Carter Report suggested a benchmark
for acute pathology costs of 1.6% as aproportion of Trust operating expenditure. For clarity, the sequence of the
recommendation is: 1. Does the in-house provision of acute
pathology at the Trust cost more than 1.6%of Trust operating expenditure? If no,great, no action required.
2. If the cost of in-house acute pathology isabove 1.6% of Trust operating expenditureat the moment, will it be reduced to 1.6%by April 2017? If yes, great (as above).
3. However, if not, the recommendation fromThe Review is that the Trust should prepareand agree plans for consolidation withothers by January 2017. The Review is, ofcourse, agnostic about whether theconsolidation should be with public orprivate providers, or a combination of both
4. Or finally, if the Trust doesn’t want toconsolidate, and can’t achieve a cost ofacute pathology of 1.6% of Trust operatingexpenditure, The Review recommendation
is that it should prepare and agree plansfor outsourcing provision of acutepathology by January 2017. Again, The Review is agnostic about whether theoutcome of any outsourced arrangementshould be to a public or private provider, or a combination of both.
Supporting Recommendations� Trusts introducing the Pathology QualityAssurance Dashboard (PQAD) by July 2016to assure themselves and others that thepathology service provided to them is, and remains, of appropriate quality andsafety, with NHS Improvement hosting thedashboard.
� HSCIC publishing a definitive list of NHSpathology tests and how they should becounted by October 2016, with NHSImprovement requiring Trusts to adopt the definitions from April 2017, and NHSImprovement publishing guidance notesfor forming collaborativejoint ventures and specifying managed equipment servicecontracts for local adaptation by October2016 (Carter, 2016).
There are no guidelines available forinclusion and exclusion criteria so following discussions with Phil Hudson who was involved in drawing up the Carter Report the ACB has draftedsuggested exclusions when calculating theacute pathology costs.
Exclusions� Blood and blood products (as althoughsome pathology services administer theprocurement of blood products,consumption and therefore cost iscontrolled elsewhere in the Acute Trust).
� Phlebotomy (as not all pathology servicesprovide acute phlebotomy).
� Consultants both Medical and Clinical
ACB News | Issue 640 | August 2016
8 | Council Matters
Guidance on the Calculationof Acute Pathology Costs
Scientists (as not all pathology services have consultants ‘on their pathologybooks’, and the programme is not (yet)proposing to attempt to measureconsultant productivity, or form a view on an appropriate quantum of resource for Trusts with similar clinical demands).
� Medical secretaries (usually sit withconsultants).
� Facilities (as not all Trusts charge ‘in-house’,‘construct’ or ‘hybrid’ pathology servicesdirectly for hard and soft facilities).
� Transport of Direct Access samples to theacute laboratories (as costs associated withDirect Access are covered below).
� Direct Access (DA) activity actual costs or
half of DA costs calculated from referencecost data whichever is the lesser.
� The costs associated with regionalscreening programmes.
� Anticoagulation, DVT, VTE services (as notall Trusts provide this service).
� Infection control (as not all pathologyservices provide infection control services tothe acute Trust).
� Mortuary and bereavement office (as notall pathology services provide this service).
� Point of care costs (as this does not alwayssit in pathology budget).
There may be other exclusions and we can review the list as more informationemerges. �
Council Matters | 9
Issue 640 | August 2016 | ACB News
HCPC Lay Council MembersThe Health and Care Professions Council (HCPC) is seeking to appoint two lay members. Council members play a key role in setting strategy and policy and ensuring the HCPC fulfilsits statutory duties and responsibilities. Candidates require experience in corporategovernance, strategic planning and collective decision making and must have a good grasp of regulatory principles. As ambassadors for the HCPC, they will need the ability to form strong relationships and
uphold the principles of transparency and accountability. Candidates for this role must not beon the HCPC Register or engaged in practise, teaching, managing or researching in, one ofthe professions regulated by the HCPC. As a UK-wide regulator, HCPC encourages applicationsfrom individuals across England, Wales, Scotland and Northern Ireland.Elaine Buckley, Council Chair HCPC said: “The role of the Lay Council Member is one that is
highly valued by the HCPC Council and is extremely important for the effective governance ofthe organisation. We are looking for candidates with a broad range of skills who can supportthe work of the HCPC whilst contributing a different perspective. I look forward to workingwith the successful candidates who will be joining the Council next January.”The deadline for applications is 9am on Monday 19 September and interviews will take
place between 2nd and 4th November 2016. The successful candidate will begin their newrole from Monday 2nd January 2017.
For more information and how to apply, visit: www.hcpc-uk.org/aboutus/council/councilappointments or email [email protected]
10 | Practice FRCPath Style Calculations
ACB News | Issue 640 | August 2016
A medical team is considering a change of screening strategy for a disease X. The traditional test A has a sensitivity of 95% and specificity of 60% for disease X. A new test B has beenintroduced which has an increased specificity 75% for this disease but a reduced sensitivity of75%. Calculate the positive and negative predictive values for each test for a population inwhich X has a true prevalence of 10%.
FRCPath, Autumn 2001
The positive predictive value of a test (PV+) is the proportion of positive results which are truepositives whereas the negative predictive value (PV-) is the proportion of negative results whichare true negatives:
PV(+) = TP PV(-) = TN TP + FP TN + FN
The problem can be solved by calculating the individual values for TP, FP, TN and FN andsubstituting them into the above expressions. However, there is a quicker alternative.
TP is the proportion of positive results obtained for the diseased population which can beobtained by multiplying the sensitivity by the proportion of diseased individuals:
TP = Sensitivity x Prevalence
FP is the proportion of positive results for individuals without disease which can be obtained bymultiplying the proportion of disease-free individuals (1 - prevalence) by (1 - specificity) – sincespecificity is the proportion of negative results in the disease-free population (1 - specificity)must be the proportion of positive results in this group:
FP = (1 - specificity) x (1 - prevalence)
TN is the proportion of negative results for individuals who are disease free and is simply theproduct of specificity and (1 - prevalence):
TN = Specificity x (1 - prevalence)
FN is the proportion of negative results for individuals with the disease and is obtained bymultiplying the proportion of diseased individuals (prevalence) by (1 - sensitivity) – sincesensitivity is the proportion of positive results in the diseased population (1 - sensitivity) must bethe proportion of negative results in this group:
FN = (1 - sensitivity) x Prevalence
Substitution of these values into the expressions for positive predictive values yields thefollowing:
PV(+) = Sensitivity x Prevalence (Sensitivity x Prevalence) + {(1 – specificity) x (1 – prevalence)}
PV(-) = Specificity x (1 - prevalence) {(Specificity x (1 - prevalence)} + {(1 - sensitivity) x Prevalence}
Deacon’s Challenge No 183 - Answer
Note that sensitivity, specificity and prevalence are given as proportions rather thanpercentages.
Therefore for test A the sensitivity is 0.95 and specificity 0.6. For test B both the sensitivity andspecificity are 0.75. The prevalence of disease (given as 10%) becomes 0.1.
For test A:
PV(+) = 0.95 x 0.1 = 0.095 = 0.21(0.95 x 0.1) + {(1 - 0.6) x (1 - 0.1)} 0.095 + 0.36
PV(-) = 0.6 x (1 - 0.1) = 0.54 = 0.99{0.6 x (1 - 0.1)} + {(1 - 0.95) x 0.1} 0.54 + 0.005
For test B:
PV(+) = 0.75 x 0.1 = 0.075 = 0.25(0.75 x 0.1) + {(1 - 0.75) x (1 - 0.1)} 0.075 + 0.225
PV(-) = 0.75 x (1 - 0.1) = 0.675 = 0.96{0.75 x (1 - 0.1)} + {(1 - 0.75) x 0.1} 0.675 + 0.025
Practice FRCPath Style Calculations | 11
Issue 640 | August 2016 | ACB News
Question 184A new assay is being devised for the measurement of phenytoin. In an assessment ofrecovery, aliquots of a solution of phenytoin sodium (1 mg in 1 mL) are added to separate 1 mL aliquots of a serum sample and the aliquots mixed then re-assayed with the followingresults:
Aliquot Added aliquot of Apparent phenytoinphenytoin standard (µL) concentration measured
by new assay (µmol/L)
A 0 40B 10 80C 20 125D 30 176
Calculate the recovery for aliquots A, B, C and D and give an explanation for the patternobserved (Mol. W. of phenytoin sodium 274)
FRCPath, Autumn 2001
Here are some tips on how to take a nationalaudit forward based on our experience:
1. Once a subject for a national audit hasbeen identified, please contact the ACBNational Audit Group (ACBNAG) forapproval and advice as to how to proceedto the next stage. You can either contactyour Regional Audit Lead (see list of NAGmembers from link on ACB website) ore-mail the chair of NAG:[email protected]
Creating the Audit Questionnaire
2. The audit questionnaire should bedesigned to allow responders to completeit in a timely fashion. Aim to use tick boxesand give options that can be easily selectedwhere possible. Actively avoid ambiguity inquestions. Do not ask multiple questionswithin a single question: avoid e.g. ‘howoften and in which patients does yourlaboratory perform test X?’ Review somepreviously published audits for ideas. If particular information is required (e.g. specific assay information/laboratorystats) then highlight this at the start of thequestionnaire.
3. The standards against which the audit isbeing completed must be clearly statedfrom the outset (if there are no extantaudit standards, consensus standards maybe created internally).
4. Where possible, the impact of the current(and future) state on patient outcomesmust be clearly stated – why are weauditing?
5. Once the audit questionnaire is designed itis useful to seek feedback and suggestionsfrom your Regional audit group beforesubmitting to ACBNAG.
6. Once completed, the questionnaire should
then be sent to ACBNAG for final approval. 7. The ACB Office can assist in converting
audit from MS Word onto Survey Monkey®(ACB have a subscription). Depending onthe size of the audit questionnaire this canbe time-consuming and therefore the ACB should be contacted early in theprocess to allow sufficient time for thisprocess. Contact the ACB Office [email protected] in advance tohighlight the audit.
8. The audit questionnaire should becompleted in the trial version on SurveyMonkey® and checked thoroughly beforethe final link is circulated nationally.
9. A PDF version of the audit (which allowselectronic completion) should also beprepared and circulated with the SurveyMonkey® link as some may not have accessto Survey Monkey®. This also allows theoption for the questionnaire to be printedand completed by hand and posted to theACB Office.
Distributing the Questionnaire
10. All national audits must be circulated viathe ACB Office.
11. A short email letter should be drafted and sent to the ACB for circulation withthe audit questionnaire. This shouldinclude a brief description of the audit, who should be completing the audit (e.g. one response required from eachlab/site, whether it needs input fromother colleagues such as Haematology/Immunology etc.) It should also highlightany data that will need to be prepared inadvance to enable completion (e.g.method insert information, laboratorystatistics, clinical data).
12. Advice should be sought from the ACB
12 | Scientific Committee
ACB News | Issue 640 | August 2016
Conducting a National Audit;Hints and Tips from the ACBNational Audit GroupGareth McKeeman and Annette Thomas, Cardiff
Office regarding the distribution lists.Depending on requirements auditquestionnaires may be sent to Heads ofDepartments only, or all ACB members.They can also be distributed through theRegional audit leads.
13. It is useful to keep regular contact withthe ACB Office to assess response ratesduring the audit window. Further emailsmay also need to be sent as reminders.Regional leads should be able to assist intargeting areas to improve response rates.
Presenting and Disseminating theAudit Findings
14. There is an opportunity to present anddisseminate the findings from the audit at the annual ACB audit meeting. This meeting is organised either as astand-alone meeting or as part of aparallel session at the ACB Focus NationalMeeting. The presentation should beconfined to 40 minutes with an overviewof the aims of the audit, thestandards/guidelines audited against, the findings and any recommendationsfor service improvement.
15. All replies should be treated anonymously.In presenting or publishing the data, the
number in each group should be sufficientto ensure that individual laboratoriescannot be identified.
16. A summary report of the audit should becompleted using the ACBNAG audittemplate (available to download from theACB audit page link as above) andsubmitted to the audit webmaster foraddition to the National Audit Grouppage on the website.
17. Anyone undertaking a national audit isencouraged to publish their work in theAnnals of Clinical Biochemistry.
18. The Royal College of Pathologists alsopublishes high-quality auditshttps://www.rcpath.org/profession/clinical-effectiveness/quality-improvement/clinical-audit.html
Approval of Recommendations from a National Audit
19. Any recommendations must be approvedby the ACB Scientific Committee throughthe chair of ACBNAG.
Completed regional and national audits areavailable at the ACB website along with usefulinformation on clinical audits, the audit cycleand a suggested template. �
Scientific Committee | 13
Issue 640 | August 2016 | ACB News
14 | Meeting Reports
ACB News | Issue 640 | August 2016
The ACBNI’s Annual Spring Meeting on 15thApril 2016 was a great success and challengedus to think around both our day-to-daypractice and our future service delivery. Wewelcomed multidisciplinary speakers andrepresentatives from our users to gain insightsinto the world outside our laboratories.
Modernising Pathology Services
Dr Michael McBride, Chief Medical Officer forNorthern Ireland, opened the meeting byencouraging us to embrace the challenges ofmodernising pathology services and to usethem to help influence the wider health andsocial care services in Northern Ireland. Herecognised that Pathology is facing challengessuch as growing demand and financialconstraint and stressed that we need to workin collaboration, not competition, to moveforward. He praised the Northern IrelandPathology Network and acknowledged thework already carried out to standardisepractice across the region. He suggested that‘standardisation is the platform forinnovation’. Finally, he presented examples ofhow Northern Ireland is leading the way inprecision medicine with its involvement inCatapult and the 100,000 Genomes project.These initiatives are working to deliveraccurate diagnosis and targeted treatment forbetter patient outcomes.
Human Factors in Health Care
Dr Richard Corry, Consultant Anaesthetist,educated the audience on the topic of humanfactors in healthcare. He stated that allhumans make mistakes and we need to acceptthat. To reduce human error, we need tochange our procedures not our people. Hetalked about the fragility of our workingmemory, how it relates to our performanceand how our performance varies on a day-to-day basis. We need to build our systems
around the health care professional on a badday. He outlined the reasons behind humanerror and highlighted ‘distraction errors’ and‘lookalike errors’. Simple measures can be putin place to minimise these risks such as using‘do not disturb’ vests when dispensingpharmacy medications. Addressing humanfactors in health care is of upmost importancein delivering a quality service.
Direct Patient Access to Results
Dr Donagh McDonagh, Associate MedicalDirector for General Practice in Belfast Trust,discussed some of the issues around directpatient access to results. He highlighted thecomplex nature of some tests and theirinterpretation and stressed that information isnot the same as knowledge. The question ofwho is responsible for action or follow up wasraised. GPs are often the first port of call. Hediscussed the practicalities of deciding howmuch access to give and how to implementlimits in access where necessary. He describedsocial class effects and how direct patient
ACBNI Annual SpringMeeting 2016Gillian Hamilton
Dr Michael McBride, Mrs Margaret McDonnell andProfessor Maurice O’Kane
Meeting Reports | 15
Issue 640 | August 2016 | ACB News
Dr Peter Sharpe, Ms Julie McCullough, Professor Stephen Halloran, Mrs Margaret McDonnell, Professor JimBonham, Dr Jenny Hamilton, and Dr Tom Trinick OBE
access to results tends to benefit the middleclasses and not the deprived classes. Hequestioned whether it really did lead topatient empowerment.
Colorectal Cancer Screening
Professor Stephen Halloran outlined thesuccesses, challenges and opportunities incolorectal cancer (CRC) screening. Majorchallenges for the programme are to increaseuptake and to ensure that the test methodused selects the appropriate patients forcolonoscopy. Uptake is dependent onsocioeconomic status and is almost 50% lowerin the most deprived populations. A better testis needed. The current guaiac faecal occultblood test (gFOBt) requires three specimensand cannot be automated, is subject tointerferences, is qualitative and is affected byoperator variability. A pilot was carried out inEngland in 2014 using the faecalimmunochemical test (FIT) which measures theconcentration of human haemoglobin in asingle specimen and is less susceptible tointerferences. Interestingly, uptake increased
in all population groups and most significantlyin the deprived population with an 8%increase. An increase in positivity was alsoobserved. As the capacity of colonoscopyreferral cannot be increased, carefulconsideration of the cut-off to use is required.A cut-off of 20 µg haem/g faeces, equivalentto the current gFOBt method, would increasepositivity from 1.7% to 7.9%. The cut-offwould need to be increased to 180 µg haem/gto be equivalent to current referral rates.Increasing the cut-off would lead to morecancers detected per colonoscopy but wouldmiss more cancers in women and in the olderpopulation. Professor Halloran concluded byproposing the use of variable cut-offs togetherwith assessment of personal risk in amultivariate risk score. He described this as anopportunity to personalise population-basedscreening.
Neonatal Screening
Professor Jim Bonham, Sheffield Children’sHospital, talked about the future of neonatalscreening. Since the introduction of
phenylketonuria (PKU) screening using theGuthrie method in 1969 significant advances intechnology, in particular tandem massspectrometry, have opened up the possibilityof identifying many other treatable raredisorders. The challenge was to expand theexisting newborn screening programme in away that does not create anxiety for familiesand can be delivered within existing clinicalresources. Following a successful pilot study in2008, four conditions (GA1, MSUD, IVA, HCU)were added to the existing screening panel inEngland (CHT, Sickle cell, CF, PKU, andMCADD). Possible candidates for addition tothe programme in the next five years areLCHADD, Tyrosinaemia type 1, CAH, SCID andDuchenne muscular dystrophy. Looking to thefuture, there are exciting new developmentsincorporating Next Generation DNAsequencing. The Wellcome Trust andDepartment of Health are funding a threeyear project to study both clinical and geneticinformation to improve newborn screeningoutcomes. Professor Bonham concluded byfocusing on how we support patients. Withthe increasing amount of informationbecoming available we need to understandthe best way to make this accessible to
patients. The aim is to produce a mobile Appproviding full information support.
Constitutional Delay in Growth andPuberty
Dr Philip Johnston, Consultant inEndocrinology & Diabetes, spoke on theapproach to the male with constitutional delayin growth and puberty (CDGP). The factorsthat control the timing of puberty aregenetics, epigenetics, environmental factorsand endocrine disruptors. Delayed puberty isdefined as the absence of signs of sexualmaturation by an age more than 2 to 2.5standard deviation values above the mean ofthe population (traditionally, breastdevelopment by age 13 years in girls andtesticular development by age 14 in boys).Constitutional delay accounts for 53% of cases. CDGP is a transient state ofhypogonadotrophic hypogonadism (HH)associated with prolongation of the childhoodphase of growth, delayed skeletal maturation,delayed and attenuated pubertal growth spurtand relatively low insulin-like growth factor-1secretion. It is often combined with familialshort stature. In the pre-pubertal male,testosterone replacement can be used to
16 | Meeting Reports
ACB News | Issue 640 | August 2016
Professor Stephen Halloran
induce pubertal development, accelerategrowth and relieve psychosocial complaints.CDGP is a diagnosis of exclusion. In particular,the distinction between CDGP and idiopathicHH requires careful clinical observation asbiochemical investigations do not alwaysdiscriminate. However, a testicular volume <4 mL and testosterone <1.7 nmol/L suggeststhe need for further studies.
Laboratory Tests in Neuroblastoma
Dr Robert Johnston, Consultant PaediatricOncologist, spoke on the use of laboratorytests in neuroblastoma. Neuroblastoma is themost common extracranial solid tumour inchildren and accounts for 15% of all paediatriccancer deaths. It occurs almost exclusively ininfants and children. Presenting featuresinclude bone pain, fever, hypertension,anaemia, watery diarrhoea, Horner Syndromeand subcutaneous skin nodules. Diagnosisrequires unequivocal pathologic diagnosisfrom tumour tissue by light microscopy orbone marrow (BM) aspirate (or trephine) withunequivocal tumour cells and demonstrationof elevated urine or serum catecholamines ormetabolites. The major catecholaminemetabolites of interest are vanillylmandelic
acid (VMA), homovanillic acid (HVA) anddopamine. Catecholamine secretion isincreased in 90% of children withneuroblastoma but false positive and falsenegative results are possible. A newer markeremerging is MYCN amplification inneuroblastoma (NBL). This is a genetic markerof long term prognosis and is a marker of pooroutcome in low stage disease. It can identifypatients at high risk and can help to stratifyfor treatment.
Laboratory Services in a War Zone
Dr Tom Trinick OBE, Consultant ChemicalPathologist and General Physician, gave arealistic view of laboratory services in a warzone. He presented examples of acutemedicine on the front line with limitedlaboratory resources. It certainly put ourproblems into perspective!
Familial Hypercholesterolaemia
Dr Peter Sharpe, Consultant ChemicalPathologist, spoke on familial hypercholest-erolaemia (FH). FH is the most commondominantly inherited disorder. It is mostfrequently due to mutations in the geneaffecting the Low-Density Lipoprotein (LDL)
Meeting Reports | 17
Issue 640 | August 2016 | ACB News
receptor that clears LDL particles from plasma.In heterozygotes, total cholesterol is typically7.5 to 11 mmol/L. Untreated, there is a 50%risk of death by age 60 in males and age 70 infemales. Tendon xanthomata is virtuallypathognomic. Homozygote FH is rare(1:1,000,000) with cholesterol levels typically18 to 25 mmol/L. Patients develop ischaemicheart disease (IHD) in childhood and untreatedmost die of IHD in their mid 20s. In NorthernIreland there is a FH genotyping screeningcriteria in place to select patients for genetictesting based on the Wales FH scoring criteria.This takes account of family history, LDL,cholesterol, triglycerides, clinical history andtendon xanthomata/premature corneal arcus.The current aim of management of adultheterozygotes is to achieve LDL <50% baselineusing statins plus additional agents asnecessary (NICE). ESC/EAS guidelines suggest aLDL target of <2.5 mmol/L in adults and <1.8mmol/L in diabetics or those with establishedcoronary heart disease (CHD). This is not yet inplace in Northern Ireland. Dr Sharpe finishedby presenting promising data on the use of
Evolocumab as a new cholesterol reducingagent. Julie McCullough, a FH Specialist Nurse,
outlined the FH cascade testing service inNorthern Ireland and the role of the SpecialistNurse Team. The programme is regionallystandardised and involves close collaborationbetween the Regional Genetics Centre and thelipid clinics in each trust. It is patient focusedand detailed protocols ensure that the patientis kept well informed at every stage. The totalnumber of patients identified in NorthernIreland by 31st March 2015 was 1034, almost29% of the predicted total. Of the 187 at-riskpatients tested in the last year, 78 wereidentified with FH (42%). The cascadedetection rate has more than doubled in thefirst year following the introduction of thenew FH Nurse team. Throughout the meeting we saw evidence
of the ‘modernising pathology’ described inour opening talk. The meeting highlighted the benefits of working in collaboration,exploring new technologies, and putting thepatient first. �
18 | Meeting Reports
ACB News | Issue 640 | August 2016
Meeting Reports | 19
Issue 640 | August 2016 | ACB News
The 4th Autoimmune Focus Meeting,organised by Werfen, was held on 19th May2016 at the Hilton Metropole Hotel inBirmingham, attracting over 120 delegates.The meeting was opened with a briefintroduction given by Richard Hames, whointroduced the two chairs of the meeting;Professor Berne Ferry (ConsultantImmunologist, Churchill Hospital, Oxford) andDr Sadia Noorani (Consultant Immunologist,Sandwell & West Birmingham Hospital).
Coeliac Disease
Professor Berne Ferry began the lectures witha presentation on Coeliac Disease (CD),concentrating on three main areas: The pathology of CD and its diagnosis andtreatment, the NICE Guidelines for Coeliac2015, and the difficulties in monitoring thisdisease.
The ‘gold standard’ for diagnosis of CD is theduodenal biopsy, but there are difficultiesrelating to accurately obtaining/reading biopsysamples. As such, serological diagnosis of CDremains of huge importance.The current NICE guidelines NG20
(September 2015) offer recommendations forthe recognition, serological testing andmonitoring of CD. The relevant key points forlaboratories were identified and highlightedby Professor Ferry, bringing attention to theupdates in this latest version – particularlyaround Endomysial antibody testing. Adiscussion of the pros and cons of the differentantibodies used in CD diagnosis followed.The talk was brought to a close with
comments on the challenges of monitoringCD. As serological testing for CD does notcorrelate well with disease activity, or predict
Focus on AutoimmunityAnaya Connolly, Northampton General Hospital
Delegates had the opportunity to view and discuss a number of scientific posters from UK based study groups
long-term risk, the ability to monitor CDremains under-addressed.Dr Ronnie Chee (Consultant Immunologist,
Royal Free Hospital, London) gave a talk onRefractory Coeliac Disease (RCD), focusing onmechanisms and management.RCD was defined as patients that have
persisting symptoms of CD for >12 months, on a strict gluten free diet after all othercauses of villous atrophy have been excluded.Dr Chee explained the classification of the
two types of RCD (I and II) was based upon thepercentage of normal/abnormal intraepitheliallymphocytes (IELs) present (determined mostaccurately by flow cytometry). Clinically RCDI isless severe, whereas RCDII is frequently thefirst step towards malignant lymphomaltransformation of IELs to EnteropathyAssociated T-cell Lymphoma (EATL), which hasa very poor prognosis, with 5 year survivalaround 20%. Dr Chee closed the lecture with adiscussion around the treatment strategies forRCDI, RCDII and EATL.
ISO 15189
John Ringrow (Senior Assessment Manager,UKAS) began this talk with an insight into thetransition to ISO 15189 from CPA. The fourmain areas that came out of the gap analysisbetween UKAS and CPA were highlighted:
verification/validation, traceability, uncertaintyof measurement, and clinical staffcompetence. He estimated that all laboratorieswill be ISO 15189 accredited by March 2018, as more decision makers are currently beingtrained.Ravina Hira-Kazal (Clinical Scientist and
Immunology Laboratory Manager, BarnetHospital) gave her experience of goingthrough the ISO 15189 inspection, coveringthe non-conformance notices that were raisedon an individual basis. They coveredretrospective validation, unjustifiablestatements in SOPs, clinical competence andIQC statistical reviews.Steven Rimmer (Clinical Scientist, Heart of
England NHS Trust, Birmingham) offered hisexperience of the UKAS inspection. He gave aninsight into the requirements for robustdocumentation, encouraging staffengagement, staff training, audits andcontinual improvement. He indicated that thefirst visit by UKAS focused on ensuringlaboratory processes are being followed(overview), and the second visit focused moreon specifics.
ANA and DFS70
Dr Eckart Mummert (Clinical Science Liaison,Inova Diagnostics, San Diego) gave a talk on
20 | Meeting Reports
ACB News | Issue 640 | August 2016
Meeting and discussion opportunities for delegates
the importance of ANA measurement, andissues that arise due to the presence of ANAsin the healthy population.The detection of ANAs is important in the
exclusion or diagnosis of autoimmune disease,and in particular the connective tissuediseases. ANA requests are made (mostly fromprimary care) for a wide range of symptoms,meaning there is a low pre-test probability ofa CTD.He indicated that the detection of high
numbers of false positives leads to increasedcosts for the NHS, in terms of referrals, follow-up testing, and inappropriatetreatment, highlighting the importance of determining new methods for reducingANA false positives.Anti-DFS-70 (dense fine speckled) was
introduced as an ANA found mostly in thehealthy population. It is very frequent in anumber of inflammatory conditions, and veryrare in systemic autoimmune rheumaticdiseases. It can therefore be used as exclusionmarker, reducing follow up testing/referrals.Focusing further on DFS70, Dr Sadia Noorani
(Consultant Immunologist, Sandwell andBirmingham Hospitals) spoke of an MScproject that aimed to establish incidence ofanti-DFS70 in the population. This will beachieved by assessing positives and negativesand their association with SARD, to determineif DFS70 testing would be beneficial. Testingincluded screening using QUANTA Lite HEp2slides with confirmatory testing performed onthe BIO-FLASH chemiluminescence system. The study is on-going.The talk was summarised by indicating the
potential for DFS70 having a role in reducingrepeat CTD testing, rheumatology visits andfurther testing, but more data needs to begathered.
Scleroderma and Myositis
Dr Harsha Gunawardena (ConsultantRheumatologist, Bristol) gave an insight into the clinical associations of myositis-scleroderma overlap antibodies.
A historical perspective of scleroderma andmyositis was given, highlighting the limiteduse of the classification criteria used in clinicaldiagnosis. It was suggested that usingantibodies to stratify patients was a muchbetter tool due to the vast array of clinicalphenotypes associated with this disease.Specific autoantibodies can be useful indetermining risk of development of particularorgan manifestations. Many laboratoriesreport weakly positive ANAs as negative, but it was suggested that this is notparticularly useful to clinicians as myositispatients often have weakly positive ANAs.Kim Fligelstone (Patient Representative,
Scleroderma and Raynaud’s UK) offered us aninsight into her personal journey withscleroderma. She told the meeting of thechallenges that this disease caused on dailylife. It highlighted the wide range of clinicalsymptoms that can occur, and the impact thatlaboratory testing can have.The meeting was informative and interesting
and gave the opportunity for networkingamongst clinical and laboratory professionals.It provided a platform for dissemination ofnew and updated information within theremit of autoimmunity. �
Meeting Reports | 21
Issue 640 | August 2016 | ACB News
Ravina Hira-Kazal, Clinical Scientist and LaboratoryManager at Barnet Hospital – one of three speakersreviewing ISO 15189 accreditation experiences. The scientific sessions were chaired by Professor BerneFerry and Dr Sadia Noorani
Keith Johnson started his laboratory career inthe early 1960s as a Laboratory Technician atLeeds General Infirmary. At that time it was aUniversity-run Department led by ProfessorG.H. Lathe and it was he who inspired Keith’sinterest in neonatal bilirubin – an interest hemaintained for all his working life.After Leeds General Infirmary, Keith worked
at Bradford Royal Infirmary, followed by aperiod at St James’s Hospital in Leeds. He thenbecame a Biochemist and moved to Dewsburywhere he worked for the rest of his career.Apart from being very active in his
laboratory work Keith also contributed tomany external aspects of Clinical Chemistry. In his early career he was an active member ofthe Yorkshire Regional Committee for ClinicalBiochemistry, an organisation which allowedexchange of ideas and practice betweenlaboratories in the Region. With input fromthe members of this organisation, and inconjunction with the Computer Department atthe Regional Headquarters, Keith developedYRQAS – the Yorkshire Regional QualityAssurance Scheme. This was probably aforerunner of the national schemes.Keith’s keen interest in the quality assurance
of bilirubin developed into a national schemefor paediatric/neonatal bilirubin. Hisenthusiasm and efforts in this pioneeringscheme no doubt improved the quality ofinvestigations in many laboratories andconsequently the care and treatment of many babies and children across the UK.Alongside this he advocated strongly for acomprehensive diagnostic service, particularly in children, to avoid the lengthydelays sometimes seen in the identification of inherited disorders. This is something thathe continued to develop throughout hiscareer.Keith also ran a Regional Discussion Group
for many years and was active in teaching andtutoring at the Leeds Polytechnic.Despite serious illness Keith continued to be
active and involved in quality assurance untilvery recently. This demonstrated hiscommitment, not just to Clinical Chemistry, his life’s chosen topic, but also to the fact thathe avidly wanted Clinical Chemistry to be ofgood quality.He was always a pleasure to work with and
was unstinting in his help for others. �DMR
22 | Obituary
ACB News | Issue 640 | August 2016
Committed PaediatricBilirubin Pioneer
24 | Crossword
ACB News | Issue 640 | August 2016
Last month’s solution
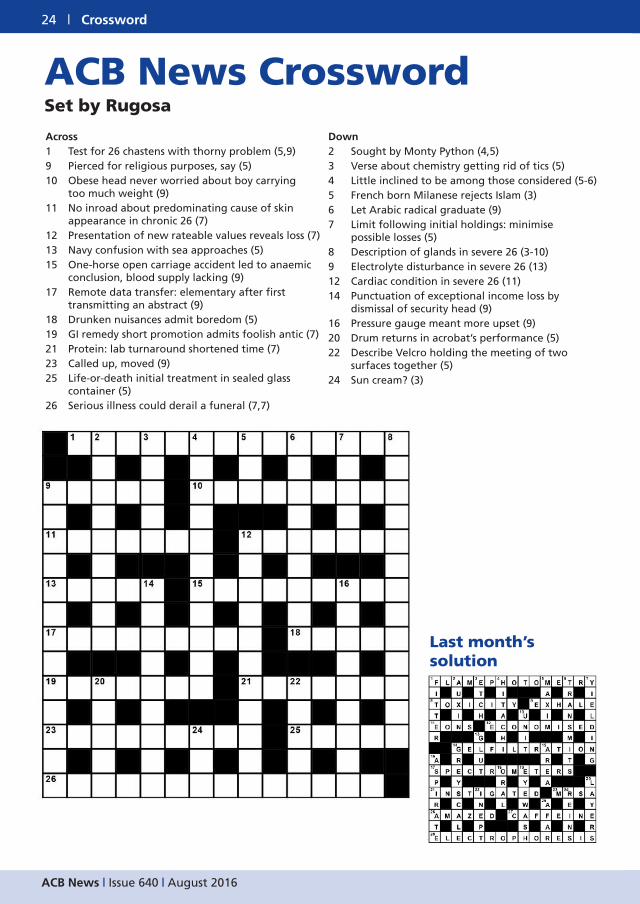
Across 1 Test for 26 chastens with thorny problem (5,9)9 Pierced for religious purposes, say (5)10 Obese head never worried about boy carrying
too much weight (9)11 No inroad about predominating cause of skin
appearance in chronic 26 (7)12 Presentation of new rateable values reveals loss (7)13 Navy confusion with sea approaches (5)15 One-horse open carriage accident led to anaemic
conclusion, blood supply lacking (9)17 Remote data transfer: elementary after first
transmitting an abstract (9)18 Drunken nuisances admit boredom (5)19 GI remedy short promotion admits foolish antic (7)21 Protein: lab turnaround shortened time (7)23 Called up, moved (9)25 Life-or-death initial treatment in sealed glass
container (5)26 Serious illness could derail a funeral (7,7)
Down2 Sought by Monty Python (4,5)3 Verse about chemistry getting rid of tics (5)4 Little inclined to be among those considered (5-6)5 French born Milanese rejects Islam (3)6 Let Arabic radical graduate (9)7 Limit following initial holdings: minimise
possible losses (5)8 Description of glands in severe 26 (3-10)9 Electrolyte disturbance in severe 26 (13)12 Cardiac condition in severe 26 (11)14 Punctuation of exceptional income loss by
dismissal of security head (9)16 Pressure gauge meant more upset (9)20 Drum returns in acrobat’s performance (5)22 Describe Velcro holding the meeting of two
surfaces together (5)24 Sun cream? (3)
ACB News CrosswordSet by Rugosa
Situations Vacant | 25
Issue 640 | August 2016 | ACB News
26 | Situations Vacant
ACB News | Issue 640 | August 2016
To advertise your vacancy contact:ACB Administrative Office,
Email: [email protected]: 26th of the month prior to the month of publication
Training Posts: When applying for such posts you should ensure that appropriate supervision and training support will be available to enable you to proceed towards HCPC registration and the FRCPath examinations.
For advice, contact your Regional Tutor.
The Editor reserves the right to amend or reject advertisements deemed unacceptable to the Association.