Page 1
MSc Crisis and Security Management
Faculty of Governance and Global Affairs
Leiden University – Campus The Hague
Master Thesis
“Resilient Healthcare Catering to Resilient Communities:
An Examination of Peru’s Healthcare System and its Degree
of Resilience”
Course: Master Thesis Crisis and Security Management
Supervisor: Drs. G.M. (Jelle) van Buuren
Second Reader: Dr. Anouk L. van Leeuwen
Student: Francesca Barco
s1644858
[email protected]
Date: August 11th, 2016
Page 2
2
Acknowledgements
"When they go low, we go high”
Michelle Obama
Developing this thesis was a long process at the end of a long journey. It would have
never been possible without a few people:
My supervisor, Jelle van Buuren, for his support, patience and advice. Thank you
from the bottom of my heart!
My parents, Alessandra and Gianfranco, and all my family, for allowing me the
audacity of dreaming big since I was very little. I love you very much.
The people I truly love, for being by my side, fighting for me and with me. You are
my world.
My previous teachers Hillary, Vilma, Tex and Farhang, and those who helped me
with this thesis. You all gave me the opportunity to get here, I hope I made you proud.
And finally, myself, for the resilience.
Now, on to the next big thing!
Page 3
3
Table of contents
INTRODUCTION 5
RELEVANCE OF THE STUDY.............................................................................................................7THESIS OUTLINE................................................................................................................................9
2. BODY OF KNOWLEDGE 11
2.1 RESILIENCE: A COMPLEX AND DYNAMIC CONCEPT...........................................................122.2 RESILIENCE AND CRISIS: EXACERBATING THE PROCESS..................................................162.3 COMMUNITY RESILIENCE: SHAPING THE PROCESS............................................................242.4 COMMUNITY RESILIENCE AND HEALTHCARE, RESILIENT HEALTHCARE FOR
COMMUNITIES..................................................................................................................................272.6 CHAPTER CONCLUSION...........................................................................................................29
3. RESEARCH DESIGN AND METHODOLOGY 30
3.1 RESEARCH QUESTIONS.............................................................................................................303.2 RESEARCH DESIGN: SINGLE CASE STUDY.............................................................................333.3 OPERATIONALIZATION............................................................................................................343.4 TRIANGULATION OF METHODS...............................................................................................403.5 VALIDITY....................................................................................................................................41
4. THE CASE: PERU 42
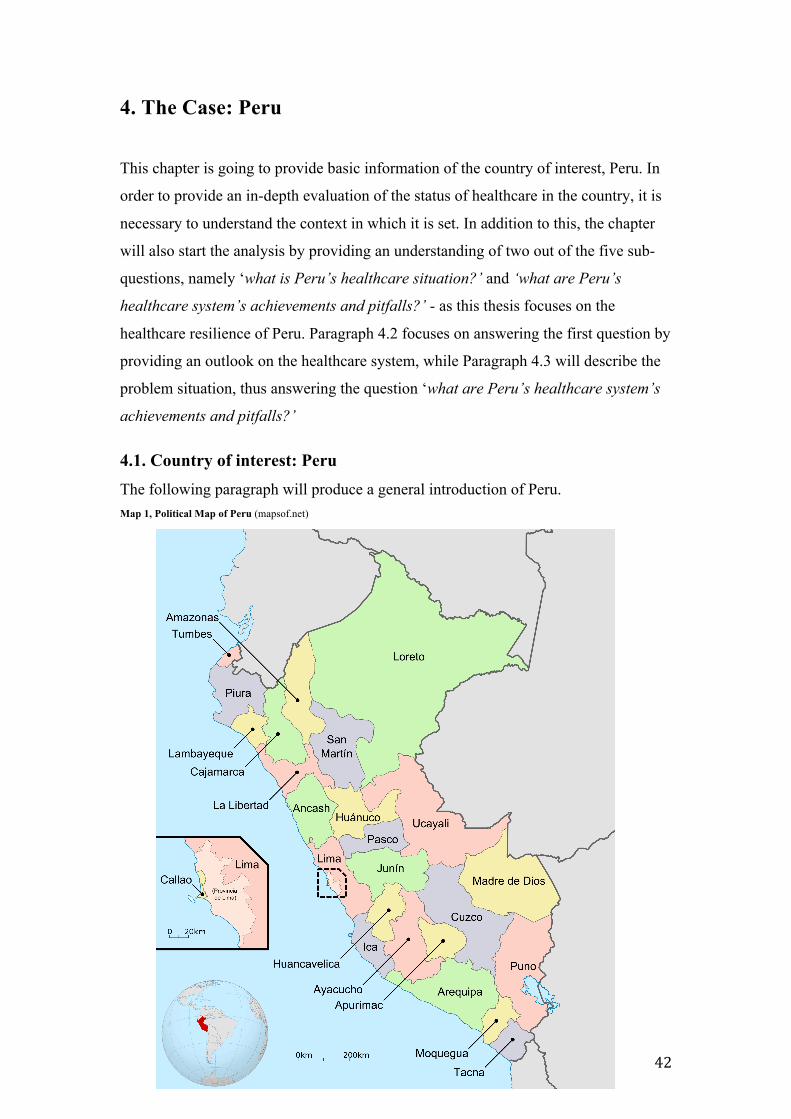
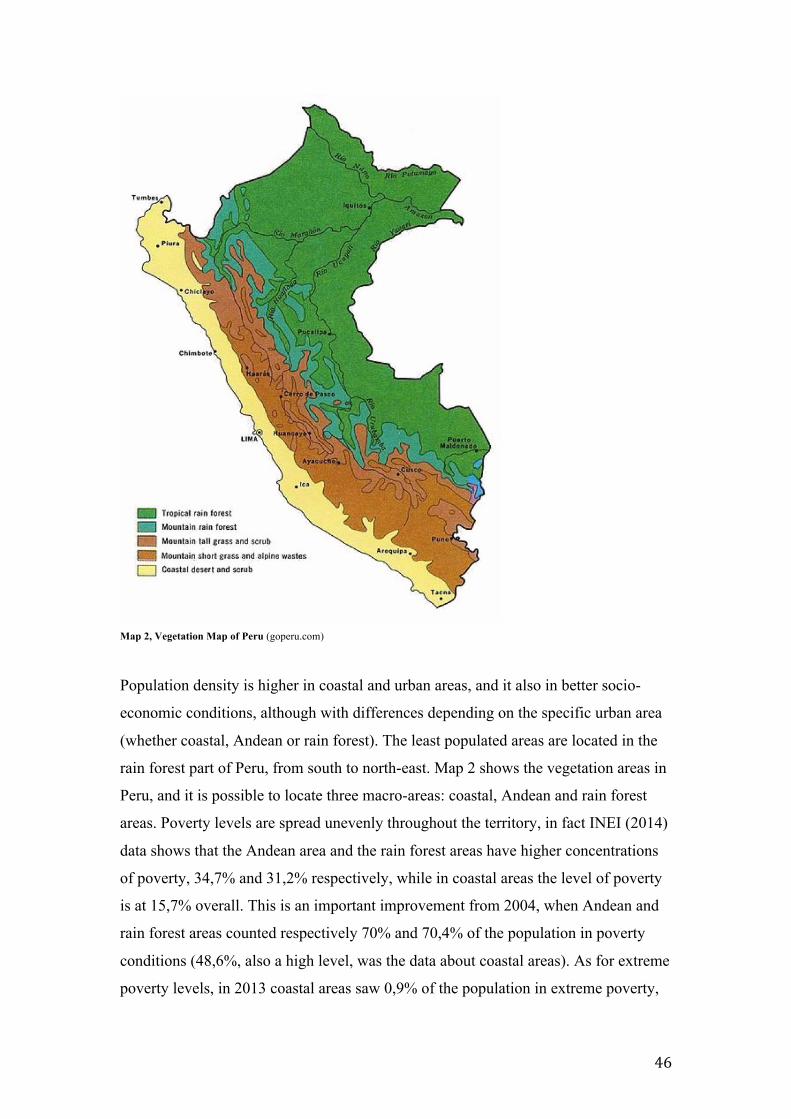
4.1. COUNTRY OF INTEREST: PERU..............................................................................................424.1.1 REGIONS AND POVERTY LEVELS THROUGHOUT THE TERRITORY...........................................454.2 THE CASE: PERU’S HEALTHCARE SYSTEM...........................................................................484.3 PROBLEM SITUATION: ACHIEVEMENTS AND PITFALLS OF PERU’S HEALTHCARE
SYSTEM..............................................................................................................................................494.3.1 INFRASTRUCTURE DISTRIBUTION......................................................................................................494.3.2 HEALTH WORKERS..................................................................................................................................514.3.3 BLOOD DONATIONS................................................................................................................................544.4 CHAPTER CONCLUSION...........................................................................................................55
5.RESULTS 56
5.2 HOW RESILIENT IS PERU’S HEALTHCARE SYSTEM FROM BOTH A TOP-DOWN AND A
BOTTOM-UP PERSPECTIVE?...........................................................................................................585.2.1 EMERGENCY RESPONSE PLANS IN HEALTH EMERGENCIES......................................................58
Page 4
4
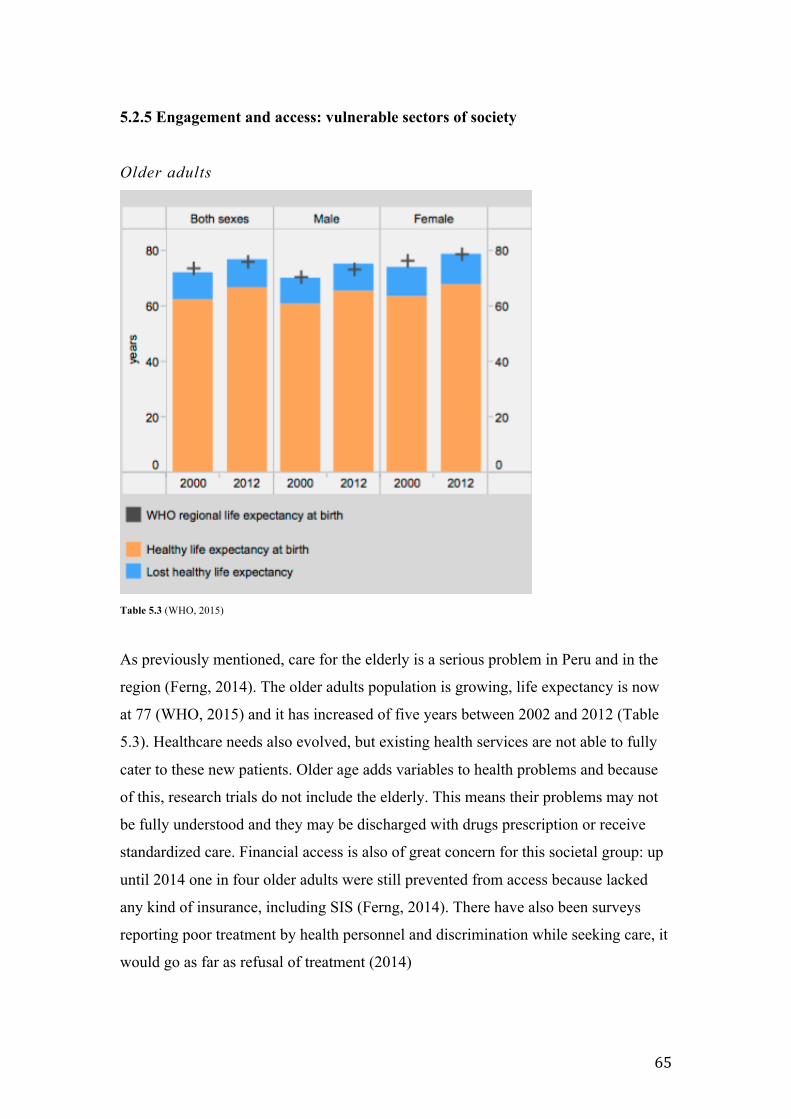
5.2.2 CRITICAL INFRASTRUCTURE PROTECTION AND SAFE HOSPITALS..........................................595.2.3 ACCESS: SIS – SEGURO INTEGRAL DE SALUD...............................................................................615.2.4 ENGAGEMENT: RELIANCE ON THE HEALTHCARE SYSTEM........................................................625.2.5 ENGAGEMENT AND ACCESS: VULNERABLE SECTORS OF SOCIETY..........................................655.5 CHAPTER CONCLUSION...........................................................................................................68
6. CONCLUSION AND DISCUSSION 71
6.1 TO WHAT EXTENT IS PERU’S HEALTHCARE SYSTEM RESILIENT AND HOW CAN THIS
DEGREE OF RESILIENCE BE EXPLAINED?....................................................................................716.2 POLICY RECOMMENDATIONS..................................................................................................736.3 FINAL REMARKS - SUGGESTIONS FOR FURTHER RESEARCH AND LIMITATIONS OF THIS
STUDY.................................................................................................................................................74
BIBLIOGRAPHY 76
JOURNAL ARTICLES........................................................................................................................76BOOKS AND BOOK CHAPTERS.......................................................................................................83GOVERNMENT AND ORGANIZATIONS’ DOCUMENTS, REPORTS.............................................86LAWS AND BILLS..............................................................................................................................91DATASETS..........................................................................................................................................91WEBSITES..........................................................................................................................................93MAPS..................................................................................................................................................95
Page 5
5
Introduction
While discussing the belle époque, Ward Wilson (2014) found consistent parallels in
several countries around the globe. Deep economic crisis, a widening gap between the
poorest and wealthiest sectors of society and overcrowding in metropolises
heightening risk and criminality made communities and states more insecure in the
1890s and 1910s, but today these are still matters subject of debate and policymaking
decisions worldwide. A factor that was overlooked then is how these relate to disaster,
when it hits. After decades of failed treaties and conventions, in December 2015 the
United Nations Climate Change Conference (COP 21 or CMP 11) in Paris made a
breakthrough in matters of environmental policy, putting the world’s worsening
environmental conditions at the top of the political agenda. At the time of writing, it is
yet to be seen if the Agreement will be ratified by enough states to become reality, but
it has the potential to benefit socio-environmental systems and subsystems that are
struggling to thrive. Coupled with the Hyogo Framework for Action 2005–2015:
Building the resilience of nations and communities to disasters, we can notice an
attention to the wellbeing of peoples in the circumstances they live in, therefore
paving the way to implement solutions that can empower communities when facing
crisis. Nonetheless, these measures are not pre-emptive but forced by the worsening
circumstances to which all regions of the world are increasingly exposed. The next
decades are going to be affected by disruption and disaster therefore it is necessary to
tackle the problem with real strategies involving all areas of crisis management.
But what does this all mean? The Paris Climate talks, the Hyogo Framework and
exposure to disaster? There is an element pulling together these rather distant topics
and it is resilience: resilience as an outlet for real change in facing crisis, which is a
constant threat in present and future endeavours for wealthy and not-so-wealthy
countries; and resilience as a way to adapt to the environment around people and
boost recovery from disaster, overall promising stronger adaptability in the future.
Resilience has become the answer to worsening climate conditions and disaster, but
what is it exactly? What does it entail? The concept is not easily quantifiable and
cannot be isolated to be studied. Instead, it has to be analysed in relation to the
context in which it originates.
Page 6
6
In recent decades, resilience has become a go-to concept for policymakers and in
crisis management discourse. While previous approaches sought a top-down type of
resolution for disruption within communities, currently more attention is paid to what
people can do in the present and the future, when the threat of climate change will be
reality for many populations around the globe, the poorest in particular. Resilience is
becoming more and more a concept on its own, not just a tool for bureaucracies and
the security apparatus of a country. At the same time the concept suffers from gaps in
the knowledge, as it adapts to the circumstances of crisis affecting an individual or a
community and cannot be studied on its own. Moreover the practical applications of
resilience vary greatly from one occasion to the other, contributing to a continuous
revision of its theoretical connotations. Contemporary thinking frames resilience as an
element of a sustainable future, but not all agree on the extent of its importance
compared to other matters or actors in it and at times it is used by organizations and
institutions as a buzzwords. As per Christoplos et al. (2012) “the need to choose
different indicators for measuring resilience per se, in order to understand if
adaptation has been achieved, seems not to have been considered in most planning
processes “, therefore research on resilience is of great value because it contributes to
expanding its understanding and the understanding of the role other elements play in
resilient contexts.
The concept is increasingly incorporated into development policy focusing on
sustainable future planning and decreasing vulnerability to risk. It initially developed
from a number of ideas in the body of literature: ecosystem stability and biology
(Holling, 1973); engineering, psychology and behavioural sciences (Norris, 2010; Lee
et al., 2009); urban and regional development (Simmie and Martin, 2010); and
disaster risk reduction. For communities, too, it has become source of empowerment
when these are included in governance. There is ideological tension between
grassroots movements and more liberal policymakers in what resilience comprises of,
and this is likely to continue in future decades. But what exactly is required from
resilience? The perpetuation of security? Security is a social construction. Following
the English School’s concept of securitization, security is not unitary and can be seen
under various aspects, making Environmental and Societal security have an impact on
the overall security of the people of a nation or even a system of nations (Buzan, de
Wilde and Wæver, 1997). According to this point of view, the referent of security is
the individual (Owen, 2004) who has to count on his or her own resilience to survive
Page 7
7
and recover in critical situations. Consequently, the threats to the security of
individuals include problems that may not always be foreseeable, such as disease
outbreaks, poverty, crime, natural disasters, abuses to human rights after conflict, etc.
(2004).
Relevance of the study In the context of this thesis, resilience is defined as the capacity of a system,
community or society potentially exposed to hazards to adapt, by resisting or
changing in order to reach and maintain an acceptable level of functioning and
structure (United Nations’ International Strategy for Disaster Risk Reduction, 2005)
and it will be thoroughly analysed throughout the literature review. The idea behind
this thesis project originates from the consideration that although crises are not
exclusive to global warming, their occurrence will not be halted by it, rather, it will
increase. Therefore, are countries prepared? Are communities going to be able to
‘bounce back’ from disasters? How is it possible to put resilience in practice? These
questions led to finding the final question leading this research, with specific
reference to the case at hand: to what extent is Peru’s healthcare system resilient and
how can this degree of resilience be explained?
The theoretical ambiguity of the concept, especially when it falls into in particular
areas of study, makes it difficult to analyse it. Consequently the first achievement for
this thesis was to find workable indicators that could be applied to the case at hand.
Without clear indicators problem-solving becomes impossible both for the researcher
and the policymaker, therefore having ad-hoc indicators was a solution for academic
purposes but also for potential policy recommendations. For this reason, this
assessment of Peru’s healthcare resilience is based on indicators developed
specifically for this thesis that are not only answering the main research question, but
also proposing further research and policy alternatives.
The relevance of this study is therefore both academic and societal. From an academic
point of view, finding suitable indicators to conduct this type analysis is challenging,
but allows using theoretical inputs while delving in the most technical aspects of the
matter, finalizing objective parameters and providing insight into the case.
From a societal standpoint, this research tackles the matter of healthcare availability
Page 8
8
providing data and information of use for future improvements and policy changes.
Knowledge from the evidence can be used for practical matters enhancing capacity
for both policy makers and crisis managers, as the underlining belief of this thesis is
that the successfulness of crisis relief derives from the efficiency of the sectors
contributing to it. As we will also study in the next chapter, using this mechanism in
policy would allow the possibility of going beyond the status quo and engage in social
change and development.
The case of Peru’s healthcare system was picked for availability of information and
peculiar national situation: it is a developing country, it is demographically unique
and it has a variety of ecosystems throughout its territory, but at the same time
healthcare expenditure by the government is very low and spread unevenly. Resilient
healthcare is a pillar of crisis recovery and as such, for communities hit by an
emergency, therefore the complexity of Peru’s case serves the topic well and is a
starting point for further developments and studies.
The idea behind this thesis was informed by a variety of sources. First and foremost,
an increased debate on the media and in academia of the possible, damning effects
climate-change. As important was my fascination with Latin America, a continent
often forgotten by Western academia. Moreover the influence resilience has in top-
down and bottom-up action in crisis settings is not going to diminish in time,
especially since it has been adopted by a variety of international institutions and
organizations. Finally, community resilience in the aftermath of natural disasters was
not one of the first subjects to arise when discussing crisis management in class, even
though the harrowing experiences of Haiti in 2010, Hurricane Katrina in 2005 and the
Zika epidemic in the Americas in more recent times have shown how relevant to the
topic can low-income communities be in such critical times. Health problems after
crisis were not often tackled, too, even though these can often take place in refugee
camps, or makeshift camps.
I personally believe natural disasters and climate-related disruptive events are going
to become the most dangerous threat to our and future generations, therefore it
deserves smart and forward-thinking planning to be tackled – starting from
healthcare. Resilience in times of crisis may be a hot topic for policymakers and
media outlets when dealing with war and revolutions, but neglecting it when
discussing disasters and its serious consequences is short-sighted and
Page 9
9
counterproductive.
Thesis outline
In the following chapters the thesis will cover theoretical doubts over what resilience
is and how it takes shape in practical contexts such as healthcare, and then it will
provide the analysis of the case, Peru, with the help of the main research question and
consequent sub-questions.
Chapter 2 is an investigation on resilience that goes from a general outlook on the
concept to the specifics of resilient healthcare. The conceptualization starts with
definitions and the relation of resilience to crisis management, exploring critiques and
ramifications into the crisis realm. It then moves into the ‘top-down’ and ‘bottom-up’
debate, giving an overview of the complex tension between the two points of view
and offering examples of how bottom-up resilience can improve communities’
conditions after crisis. In order to introduce healthcare resilience, the chapter will also
take into account community resilience. Finally, the chapter ends on resilient
healthcare, considered to be a pillar for community resilience and the ‘bounce back’
property of the concept.
Chapter 3 introduces the specifics of the research design and methodology starting
from the research questions. Following, the analysis of a single case study (Peru’s
healthcare system) is going to be motivated and indicators are going to be presented
in order to operationalize all concepts and then proceed with explaining triangulation
of methods and validity.
Chapter 4 functions both as a case introduction and initial analysis of data. As a
matter of fact, the contextual insights on Peru as a country and as a case study will be
presented, but this in the outlook of the case also being part of two of the sub-
questions, the particular downfalls and achievements of the country’s healthcare
system are going to be described.
Chapter 5 presents the results of the data researched and the answer to the remaining
sub-questions. The debate looks at government plans, technical analyses by third part
Page 10
10
examiners such as WHO and PAHO, and it keeps into account the peculiarities of
Peru, as a nation and as an ensemble of realities, often very different from each other.
Chapter 6 is devoted to a summary providing the conclusive remarks on the research,
an answer to the leading research question and the recommendations for improvement
of the sector in order to make it resilient.
Page 11
11
2. Body of knowledge
The following chapter is going to present a discussion on resilience. This is a
contested concept in public administration and crisis management because its
definition and peculiarities vary according to the context in which it works. Although
the concept has gained popularity, the lack of a clear definition brings to an overall
absence of an operative framework for assessing its progress asking for it to be
framed within a context in order to be understood. For this reason this chapter is
starting from the general understanding of the concept in relation to the realm of crisis
management, touching on the various approaches by academia and eventually going
into detail on the matter of healthcare as a functional component of community
resilience. In going from the general concept to a more particular area, this chapter
aims at tackling the increasing popularity of the term and the differences we may
encounter from one discipline to another. In a second moment, this theoretical
framework will approach community resilience in order to decide which ‘side’ of the
concept is more useful to the overall analysis: top-down or bottom-up? This is going
to allow further debate on healthcare resilience as the main topic of this research is
Peru’s healthcare system’s active contribution to the empowerment of communities
and effectiveness of resilience to prepare for future crises that are likely to struck
South America. Successful crisis relief requires functioning infrastructure catering to
its needs. Of the many components of community resilience, healthcare is of interest
because it has immense societal value by being an agent of change in both crisis and
‘normal’ settings. At the same time, the problems that one healthcare system
encounters can differ profoundly from another one, making this research dynamic
because it demands for the analyst to delve deep into what the indicators for the study
are, as we will see in the end of the chapter with an assessment of the variables
suggested by the literature that can provide an answer to the research question.
Page 12
12
2.1 Resilience: a complex and dynamic concept Due to worsening climate change, the globe is entering a phase of ‘ongoing
emergency’, calling for an acceptance of life as a permanent process of continual
adaptation in light of more frequent and complex hazardous events (Evans and Reid,
2013). The need of resilience as a response to almost perpetual contingency requires
looking for its implications in specific spheres of security politics and policy. For this
reason it is necessary to trace “this transformation of an ensemble of difficulties into
problems to which diverse solutions are proposed” (Foucault, 2003: 47) in order to
find an organic strategy for the utilization of resilience in securitizing at-risk
communities and countries.
From the Latin ‘resilio’ and ‘resiliere’, to rebound, to recoil or to spring back, the
term ‘resilience’, or ‘resiliency’, originally derives from engineering where it was
used to indicate the elastic quality of a certain a substance (Joseph, 1994), and from
biology and psychiatry (Boin et al.,). Resilience is a concept “for which both its
appeals and frustration come from the elasticity of its meaning” (Brown and Kulig,
1996/97: 29). As a matter of fact, the concept carries a variety of meanings depending
on the context in which it is used, causing disagreement on a single and uniform
definition among scholars and critics, who in turn argue against the ambiguity of the
term (Folke, 2006; Hunter, 2012; McAslan, 2010, 2011; Tanner et al., 2009).
Theorists have often pointed at the shortcomings of resiliency, Rigsby (1994) argued
that the underlining assumption of success in resilience may lead to simplistic
predictions when analysing risk. Others directed their critique to the ambiguity of the
definition, pointing out that it may not be a single construct (Gordon and Song, 1994).
Resilience is clearly a complex and dynamic subject of study, which is far reaching
and evolves with the progress of research. Nonetheless its essence stems in the ability
to bounce back from distress, change and/or disruption, which is not dissimilar from
the definition by Webster’s New Twentieth Century Dictionary of English Language
(1958): “the ability to bounce or spring back after being stretched or constrained or
recovering strength or spirit.” Resilience therefore encapsulates the capacity of a
system, community or society that are potentially exposed to hazards to adapt by
resisting or changing in order to reach and maintain an acceptable level of functioning
and structure (United Nations’ International Strategy for Disaster Risk Reduction,
2005).
Page 13
13
2.1.1 Resilience: shaping the concept through the context
In context, the term is shaped by the researcher, who filters it through the use of
adjectives and nouns to shape its essence and orient it towards new fields of study.
There is a number of contexts in which resilience is used, business, science,
engineering, etc. In this case, human resilience, institutional resilience and social-
ecological resilience are worth mentioning in order to provide examples of the
concept assuming new meaning in different fields. Human resilience ensures focus on
individuals and communities when coping with adversity and on their adaptive and
learning capabilities. Furedi (2008) for example perceives as resilient those groups
and people showing natural propensity in coping with contingency, although this must
not be taken as an innate quality, rather a “developmental process that incorporates
the normative self-righting tendencies of individuals” (Masten, 2001). Institutional
resilience, on the other hand, studies the anticipation and level of absorbance of shock
for institutions, which need to maintain their functions and identity in contingency.
Finally, social-ecological resilience places human society in its habitat. It is
preoccupied with the interaction between people and the environment or ecosystem
surrounding them, and how they can sustain their livelihoods through disaster
(Walker et al., 2004).
2.1.2 Epistemic regimes and ramifications
The emergence of resilience as concept and construct to be used as solution to
disruptive events should be studied from the perspective of these emergencies, in
relation to crisis (Aradau, 2014). In order to understand her point, Aradau finds three
epistemic regimes (ignorance/secrecy; risk/uncertainty; surprise/novelty) that present
different views on problematizing contingency and “are underpinned by different
assumptions about what can be known, how knowledge can be acquired and how
contingency can be ‘tamed’” (Aradau, 2014: 76).
The assumption underpinning the epistemic regime ‘ignorance/secrecy’ is that what is
unknown can be discovered and made transparent, therefore rendered tangible.
Ignorance and secrecy are examined in relation to knowledge, for this reason lack of it
gives access to ‘depth’ - the opposite on ‘surface’, non-knowledge (2014).
The ‘risk/uncertainty’ regime works thanks to the idea that knowledge “depends upon
Page 14
14
the existence of parallel worlds” instead of surface and depth. In modelling a parallel
reality, mimicking the one we live in, risk management can frame uncertainty. To do
so, though, it requires governing contingency through patterns and multiples without
focusing on a single event.
Events are a constant potential when discussing the ‘surprise/novelty’ epistemic
regime. Surprise is inevitable and a continuous process, making the unknown integral
to the world, although it cannot be visible or made visible through either taming non-
knowledge or drawing patterns. Contingency becomes part of reality through
resilience. Surprise has different meanings also in the other regimes, but in this it
paves the way for resilience. In resilient individuals and communities we find that the
process stimulates growth, giving additional skills than prior to the contingency
(Richardson et al., 1990: 34; Higgins, 1994: 1), making it a construct involving
exposure to disruptive events and a positive outcome in adaptation and adjustment
(Luther and Cicchetti, 2000).
Once again, the relationship with resilience and change is common to various fields,
although the subject of study varies and brings to different conclusion on the concept
itself.
Castelden et al. (2011), find that the many definitions of the concept share common
components, regardless of their originating discipline, and proceed to pinpoint them:
• Communication is the first major feature of a significant amount of literature,
bringing as example the United States’ Coast Guard’s actions during
Hurricane Katrina. With the establishing of number of communication
channels and a solid coordination effort with all levels of government
guaranteed effectiveness (Baker and Refsgaard, 2007).
• Learning (education, knowledge) is vital in preparedness in front of crises, as
the 1994 California earthquake showed. Compared to the 1989 earthquake in
Armenia, which caused 25000 fatalities, in California only 61 died due to the
seismic shocks (Gilbert, 2008).
• Adaptation, showed by Project Lyttleton after the 2011 Christchurch
earthquake in Aotearoa, New Zealand. The activists supported the town of
Lyttletown engaging in food security activities and supporting decisions
through open democracy when isolated from the rest of the country (Bond and
Page 15
15
Cretney, 2014: 24).
• Risk awareness, which stimulated community hazard awareness activities and
Civil Protection Clubs in Portugal after a period of floods, landslides and
forest fires (Mendes and Tavares, 2009).
• Social capital (trust, social cohesion), often prompted by loss of trust in
authorities (Castelden et al., 2011).
• Good governance, as opposed to poor governance, is essential in emergency
planning, especially decentralization and giving responsibility to local level
authorities (Fundter et al., 2008).
• Planning/preparedness, measures concerning warning systems, relief
operations and evacuation organization and regular drills all contribute to the
resilience of potentially vulnerable communities (Castelden et al., 2011; Chen
et al., 2008).
• Redundancy, the multiplication of critical components to emergency planning
such as the case of communication insures functioning in highly critical
situations.
• Economic capacity and diversification is significant in building resilience,
especially in agricultural communities, as the diversification in agriculture
since the 1970s in the Sahel region has showed (Chhibber and Laajaj, 2008).
• Population physical and mental health plays an important role in community
resilience, as we will see later on in this chapter, and enhancing vital
infrastructure to sustain disruption has to be a priority in policy, especially in
countries that are subject to climate change-related contingency (McDaniels et
al., 2008).
This information is to be used as a magnifying lens to understand the topic of the
research. In this analysis, the dimension of adversity is to be intended within the
realm of crisis management while positive outcomes are relative to Peru’s healthcare
system’s degree of contribution to the resilience of communities. Resilience is
therefore premised upon a vulnerable subject’s ability to internalize conditions of on-
going contingency by re-emerging from them (Evans and Reid, 2013), a quality that
to some is proper of a “healthy system” (Boin and McConnell, 2007; Longstaff,
2005).
Page 16
16
2.2 Resilience and crisis: exacerbating the process Firstly developed within the field of system ecology in the 1970s, resilience has
evolved as an operational strategy in risk management and as a frequent discourse of
resource management, especially in the public administration sphere. As previously
mentioned, the United Nations International Strategy for Disaster Risk Reduction
(UNISDR)’s Report of the World Conference on Disaster Reduction 2005 associates
the concept with crisis: “The ability of a system, community or society exposed to
hazards to resist, absorb, accommodate to and recover from the effects of a hazard in
a timely and efficient manner, including through the preservation and restoration of its
essential basic structures and functions . . . determined by the degree to which the
community has the necessary resources and is capable of organizing itself both prior
to and during times of need.” (2005). The concept has become undoubtedly popular
and as we will see it is often associated with a ‘bounce back’ property of individuals
and communities. As a matter of fact this sub-chapter is intended to open to the
debate on community resilience itself, but it also has to explore top-down approaches
to the matter and crisis.
Resilient practices often tend to stem from informal solutions found with the available
means in the aftermath of disaster or significant change, something Kendra and
Wachtendorf identify as “creative thinking, flexibility and the ability to improvise”
(2002: 52), considered vital in sudden disruption. According to Adger et al. (2011),
disregarding the resilience of a system when dealing with risk can lead to counter
productive responses that undermine long-term development. Crisis management
governance tends to only recognize resilience when this serves policymakers’ purpose
(Furedi, 2008), but the discipline is in need to understand and facilitate resilience to
promote healthy systems capable of facing newly emerging situations (Longstaff,
2005).
With the threat of transboundary crisis within inter-related areas of social life,
promoting resilience becomes a necessary strategy to the basic methods of crisis
management. Modern societies rely on infrastructures in order to deliver “public
services, enhance quality of life, sustain private profits and spur economic growth”
(Boin and McConnell, 2007) but these are particularly sensitive in disasters. The
breakdown of critical infrastructure is not always predictable with precision, nor are
Page 17
17
its consequences. Regardless, it is still a matter that deserves preparation both by
policymaker and the public. Top-down approaches and traditional crisis management
contingency planning are limited in critical infrastructure breakdowns (2007).
Managing a crisis from a resilient perspective increases the chances for a strong
recovery, especially if this involves all strata of society and goes beyond emergencies.
Furthermore, contingency planning is too often done overconfidently when in fact it
requires to go beyond what Clarke (1999) calls ‘fantasy documents’, fundamentally
incomplete lessons-learned studies looking to shift the authority in the hands of few
(‘t Hart, Rosenthal and Kouzmin, 1993) and reiterating the status quo by halting the
natural course of resilience mechanisms. Disasters and emergencies do not necessarily
guarantee significant change of previous systems, nor learning, (Birkland, 1997; Boin
et al., 2006) but can convey a change of course in policies, procedures, legitimacies
and even cultures (Baumgartner and Jones, 1993). Clearly, galvanizing society to
embrace resilience is more difficult when emotions such as fear are not persistent,
leading the management of risk solely in the hands of governments. Administrative
and societal capacities have to be harmonious in order to cope and to avoid
politicization, therefore the promotion of resilience is the tool to do so (Boin,
McConnell, 2007). As a matter of fact, the effectiveness of response in the first hours
and days in the aftermath of a crisis is critically determined by citizens on site, by first
responders and by operational administrators (Barton, 1969; Dynes, 1970; Drabek,
1986), proving the level of good governance present in risk management. A quick
recovery from disruption therefore should be seen as a property of a system capable
of decentralization and subsidence (Longstaff, 2005). As a matter of fact the United
Nations Development Programme’s motto for its 2030 development goals is
“Empowered Lives. Resilient Nations”, the goal to end poverty and hunger also
implies to manage disaster risk from a resilient point of view.
2.2.1 Addressing disaster risk with a reformed approach
The Hyogo Framework for Action 2005-2015 drafted by the United Nations
International Strategy for Disaster Risk Reduction, recognizes that climate variability
strongly impacts on disaster risk. Climate change is undeniably becoming a major
issue for policymakers since its threat has the potential to hinder the efforts to reach a
more sustainable future. The special report “Managing the Risks of Extreme Events
Page 18
18
and Disasters to Advance Climate Change Adaptation” of the Intergovernmental
Panel on Climate Change (2012) indicated that there is margin for integration in
disaster risk management and adaptation-oriented policies through careful
coordination across several domains on both sides (2012: 439). Adaptive capacity is
characterized by dynamism, with economic and natural resources, social dynamics,
technology, institutions and governance influencing it (Parry et al., 2007). With
changing climate extremes resilient and sustainable development as illustrated by the
Sustainable Development Goals could benefit from a systematic questioning of pre-
established paradigms and assumption in disaster risk management. Reducing disaster
risk and adapting to climate change are critical elements for ensuring the
sustainability of economies, societies and the environment in the long term (Wilbanks
and Kates, 2010).
Addressing disaster risk with a reformed approach that enhances coping mechanisms
while addressing multiple perspectives and obstacles favors the developing of new
patterns of response. The challenges that both disaster risk management and climate
change pose are related, from “reassessing and potentially transforming the goals,
functions, and structure of institutions and governance arrangements;” (IPCC, 2012:
440) to “creating synergies across temporal and spatial scales;” (2012: 440) and
“increasing access to information, technology, resources, and capacity” (440). Where
climate change is supposedly going to hit the hardest, the challenges for disaster risk
management become more demanding, since the level of adaptive capacity across
administrative, social and physical areas of each country (O’Brien et al., 2006).
Furthermore, important for our overall analysis is also the level of wealth of a
country, which potentially factors in determining adaptive capacity in practical
matters such as infrastructure protection and healthcare availability (Moss et al., 2010;
Ford and Ford, 2011). Other factors that influence adaptive capacity are the ability of
identifying problems and vulnerabilities under significant pressure, the best practice
of previously learned scientific notions and the implementation of projects and
programs (Moser and Ekstrom, 2010).
The wealthiest countries with a strong record on addressing risk can benefit from
addressing these challenges, too. Since there are several coefficients influencing
adaptive capacity and vulnerability, wealth can also not factor in it depending on the
situation. Extreme events may also impact wealthy countries severely (Salagnac,
2007) since every socioeconomic system has to be considered “as vulnerable as its
Page 19
19
weakest link” (IPCC, 2012).
Resilience has the potential of complementing negotiation and decision-making
processes in climate change response. The concept is already being incorporated into
disaster risk management policy for reduction and adaptation, slowly becoming the
guiding principle of the most advanced responses in developed and developing
countries (Cutter et al., 2008). Resilience thinking strengthens analyses on adaptation
and climate change since adaptation is part of a trajectory towards change (Nelson et
al., 2007). The concept of resilience provides different key approaches to adaptation
to extremes: a holistic framework for socio-ecological systems in need of evaluating
hazards; emphasis on how to deal with them; exploring options for dealing with future
disruptive events; and identifying factors able to build strong responses (Berkes,
2007; Obrist et al., 2010). Resilience may also present shortcomings in dealing with
crisis when the concept is misinterpreted and the status quo is perpetuated without
giving space to support, learning and inclusiveness in decision-making. Every single
stressor influencing an interconnected socio-ecological system deserves identification
while enhancing the ability of said system to absorb shock and adapt while improving
(IPCC, 2012: 454). Furthermore, as difficult as this may seem, particularly in
developing countries, dealing with specific types of risk without an integrated picture
of the system complexity does neither produce long-term stability nor resilience
(Walker et al., 2002; Lebel et al., 2006).
Ultimately, although it requires careful analysis and measures, using resilience proves
productive in crisis management, as it handles change without unnecessary fears and
responsabilizing citizens (Boin and McConnell, 2007). Disaster risk management and
resilience can work in synergy, especially when dealing with threats such as climate
change – which contributes to social, economic and environmental disruption. There
is no single approach to achieve this cooperation in the field, but a reconciliation of
long- and short-term goals, an in depth analysis of potential stressors, the introduction
of resilience in socio-economic systems, support for an adaptive response,
responsibilization of citizens and promotion of resilient thinking are contributing
factors that can improve response to natural disasters and adaptation to change. Full
security is not achievable and resilience accepts it by fostering survival, adaptation
and a ‘bouncing forward’ capacity, as ecological systems do.
Page 20
20
2.2.2 Top-down resilience and the status quo: a paradox in policy-making
After being an increasingly studied subject in the 1990s and also due to the effect of
the 9/11 attacks, resilience has become prominent in security responses and in the
discourse of agencies in charge of it (Walker and Cooper, 2011). Building resilience
is now the go-to catchphrase that institutions use to prepare for a critical future. The
subject of this analysis, the healthcare system’s contribution to enforcing resilience in
communities in order to face future threats coming from climate change, requires
looking at the concept both from its the bottom up and the top down aspects.
Liberalism and neoliberalism represent the top down side of the concept and often are
the underlining ideologies upon which modern states are built, therefore also the
starting point from which policies are assembled. For this reason there is a need to
examine the relationship between resilience and liberalism in-depth.
While the concept is often used and misused in global governance it is also true that
“the science of complex adaptive systems has become a theoretical reference point for
the full spectrum of contemporary risk interventions” (Walker and Cooper, 2011: 3).
Furedi (2008) uses this peculiarity to tackle the issue of vulnerability-led response,
which often fosters insecurity. Doing a comparison between official discourse and the
literature – which sees it as the capability to confront shock (Kendra and
Wachtendorf, 2002: 11) - Furedi (2008) points out that resilience is often presented in
pair with possibilistic thinking, leading to a paradoxical situation in which we
cultivate helplessness but do not give enough relevance to risk calculation. Resilience
demands a rejection of the pre-conceived notion of security to shape a more nuanced
one. Naturally, humans aim at survival, at enduring in all circumstances. We must
accept that life and survival are continuous and non-fixed processes and that dangers
are often outside our control, therefore we partake in a world where we continuously
have to adjust and permanently struggle in order to survive threats that are now seen
as endemic (Evans and Reid, 2013). Vulnerability has not to be seen with fear, but as
a reality we must adapt to. To absorb change and continue life we learn from
catastrophes in order to improve responsiveness and adaptability to future disasters.
By doing so, we accept our fundamental vulnerability and overcome the idea of it in
itself. Life is not securable and, regardless of how much Liberalist theory tries to
prove the contrary, we are never free from danger. Liberal regimes, adopting
vulnerability-led responses, do not internalize the unchanging condition of surprise.
Page 21
21
To explain this, Reid uses ecology, stating that “exposure to threats is a constitutive
process in the development of living systems, and thus the problem for them is never
simply how to secure themselves but how to adapt to them. Such capacities for
adaptation to threats are precisely what ecologists argue determines the ‘resilience’ of
any living system” (2012: 71). Every hazardous event is to be recovered from, but in
policy there is little absorbance of it, indeed the instances in which institutions expand
their capacity of planning ahead and engage with contingency are rare (Boin and
McConnell, 2007; Clarke, 1999). Overall, in official text the bottom up role of
communities, especially the poorest ones, in resilient processes is downplayed if not
completely forgotten. Only if communities accept being subjectivised they can be
agents of their own change (Reid, 2012) and become able to “make sustainable
management decisions that respect natural resources and enable the achievement of a
sustainable income stream” (UNEP 2004: 5). However oftentimes resilient
individuals “do not look to states to secure their wellbeing because they have been
disciplined into believing in the necessity to secure it for themselves” (Reid, 2012:
69). The question become then: are top-down resilience practices completely
inefficient? Or can they cater to communities looking to adapt and ‘bounce back’
from crisis?
Policymakers that over-use the concept of resilience but displace the role of the public
and communities forget the real protagonists of disruptive events and subsequent
adaptation. Maintaining that resilience is an exceptional measure serving constant
vulnerability within the public and focusing policies on the helpless society is
misleading and fosters insecurity among the same group of people that is resilient.
Resilience embraces change, it does not promise security. An important example of
how resilience is in place within communities comes from the 2011 Christchurch
earthquake in Aotearoa, New Zealand: activists from grass-roots organization ‘Project
Lyttelton’ experienced disaster first hand in a semi-isolated area and were able to
support the community of Lyttelton, in the Canterbury region. The central
government was not able to reach the location, therefore the community group
dedicated to environmental causes and social change, showed resilience in managing
the aftermath of the crisis from within the community (Cretney and Bond, 2014: 24).
After the situation was restored, Project Lyttelton was able to continue in the
development and transferring of skills by founding the ‘Harbour Resilient Project’,
Page 22
22
aimed at improving resilience in a region were seismic activity is particularly strong
(2014: 24). This example regards a Western country, where liberal policymaking
dictates crisis management measures that could not be put in place as soon as the
earthquake hit as the Lyttelton area was disconnected from the rest of society due to
damages in transport routes. This case of a community tackling the aftermath of a
crisis with “its own” resilient measures demonstrates “contingency is not tamed, but
incorporated, literally lived with” (Aradau, 2014: 77).
Resilience is a radical concept that should not be misused in order to maintain the
status quo of institutions because it essentially does not entail the existence of one.
Embedding resilience in liberal crisis management policy makes it inherently non-
radical. This is also a problem stemming from its increasing popularity, making it a
concept of both grass-roots and top-down approaches to the extent of some scholars
discouraging groups from adopting the concept and its framework (MacKinnon and
Derickson, 2012). Regardless, it is being applied to various types of social
environment, from rural to urban settings, from highly developed to low-income
countries. Theoretical advances look to include adaptation and transformation into
Social Ecological Systems (SES) resilience (Bond and Cretney, 2014), therefore
providing ground for a new definition of the concept, looking to ‘bounce forward’
after a crisis (Magis, 2010). Incorporating the idea of adapting capacity finds solid
proof in situations like the previously described Lyttelton earthquake, but other
situations can differ substantially depending on a variety of factors. As a matter of
fact “adaptive capacity involves a framework that acknowledges the multiple, ever-
changing nature of systems and the need to prepare for uncertainty and make changes
in response to disruptions” (Bond and Cretney, 2014). Nonetheless, even when adding
adaptive capacity to the concept, resilience can still be serving the establishment or
re-establishment of the status quo. The case of resilience articulated as desire for
focusing on the recovery of social systems and infrastructure after disruptions is an
example (Engle, 2011), especially after a crisis, when it serves as an opportunity to
implement selective neoliberal projects (Walker and Cooper, 2011). This use of
resilience is aimed at justifying “actions that increase inequality and disadvantage
marginalized communities through the use of market-driven rationale” (Bond and
Cretney, 2014). Because neoliberal ideologies are not confined to their original
economic and political spheres but influence all aspects of subjectivities and societal
issues, one should expect to find it in several disciplines, including social studies,
Page 23
23
security and crisis management even if not all concepts in these disciplines pertain to
the neoliberal realm. Perpetuating neoliberal discourses hinders the dynamism
embedded in the concept of resilience, favouring a capitalistic take on the notion that
is aimed at maintaining existing structures of power (Joseph, 2013). Resilient
communities work within the system they are in, adapting and responding to
contingency in order to overcome it, not to maintain the status quo that may or may
not favour them, depending on the case. The question therefore is whether the
outcomes of state-sponsored resilience are indeed beneficial to different types of
communities with different needs. Limitedly and depending on what exactly the
programs aim for, leading to the questions formulated by Cote and Nightingale
(2012): resilience of what and for whom?
Resilience “evidences most clearly how liberal power is confronting the realities of its
own self-imposed political foreclosure as the reality of finitude is haunted by infinite
potentiality” (Evans and Reid, 2013: 91). This paradox is particularly difficult to
accept in liberal regimes, as it plays on a multitude of levels, first and foremost in
human subjectivity.
Page 24
24
2.3 Community resilience: shaping the process Orienting this analysis towards community resilience - and healthcare in particular -
requires an emphasis on the role of community in itself, both in geographical and
cultural terms. Individuals form communities and the social relationships they create
within them constitute resilient behaviour that manifests at times of disruption and
change. In “disabling of the political habits, tendencies and capacities of peoples and
replacing them with adaptive ones” (Evans and Reid, 2013: 85), actors learn from
catastrophes to become more responsive during future ones. ‘Community resilience’
is defined by Magis as “the existence, development, and engagement of community
resources by community members to thrive in an environment characterized by
change, uncertainty, unpredictability, and surprise” (2010).
The term ‘community’ usually refers to a social entity, group of people living in a
certain geographical area, often sharing common values, norms and culture and who
arrange themselves according to a structure developed overtime (IFRC, 2014). The
term may also refer to a group on a local or international level with specific interests
(2014). By sharing habitat and or culture, communities are also groups of people
exposed to the same threats, whether these are man-made or not (2014). The
vulnerability of communities varies with the community itself, with several factors
(physical, technological, financial, natural, etc.) contributing to it. Moreover,
communities also contain a variety of social groups differing significantly. In general,
individuals are part of several communities throughout their lives, whether they live
in a specific place, are part of a certain minority, etc. Some groups in communities,
depending on their vulnerability, may be less resilient than others. Communities also
depend on the environment they live in, with their resilience being undermined by
disturbance in markets or ecological conditions. The diversity of the ecosystem
communities live in determines social systems making them more or less vulnerable
depending on the case. Change of course is constant in the environment and in
society, but in cases of resource-dependence, resilience is going to be more difficult to
achieve in case of crisis. The factors influencing differences and vulnerability are
interconnected as well, requiring for a multidisciplinary approach when doing an
analysis. For this reason, the concept of ‘community resilience’ raises as many
concerns as the concept of resilience in itself. Many note that an ensemble of resilient
Page 25
25
individuals does not necessarily make a resilient community because the latter is more
than the sum of its parts (Pfefferbaum et al., 2005; Rose, 2004). Of course, enabling
individuals and offering them access is the first step to strengthen a community, but
viewing resilience on an individual level is insufficient and does not allow it to
significantly improve, rather, it requires attention on a societal level to empower all
against crisis (Seccombe, 2002). When a community as a whole is resilient, the
potential for adaptation in physical, social and economic spheres of society increases
because “people in communities are resilient together, not merely in similar ways”
(Brown and Kulig, 1996/97: 43). A resilient community is likely to be empowered
facing disruption while a vulnerable one is not (IFRC, 2014). Moreover, the lessons
that are learned from the efforts to face crisis are vital over time and foster self-
sufficiency when external aid is limited or delayed (Price-Robertson and Knight,
2012).
When the idea of ‘resilient community’ arises, the National Strategy for Disaster
Resilience (NEMC, 2009) finds that the following features are at its core:
• functioning well while under stress;
• successful adaptation;
• self reliance; and
• social capacity.
Therefore the members of a community that work together are interconnected in order
to enable ways to function after facing a traumatic event are to be considered resilient.
Maguire and Hagan (2007) find three properties to social resilience (community
resilience): resistance, recovery and creativity. The more resilient is a community, the
more these properties are manifested. Referring to resistance as a property entails
communities’ efforts to withstand a crisis and its consequences without crossing a
threshold meaning these would have to undergo long-term changes (2007).
Commonly associated terms are also “bounce back” to pre-disasters level of
functioning and “pulling through”, both equating to the recovery property of social
entities that are resilient (Kimhi and Shamai, 2004). Very resilient communities not
only return to a pre-disaster point of equilibrium, but also adapt to the new
circumstances while learning from their experience, showing a degree of creativity
throughout the recovery process (Maguire and Hagan, 2007). The three properties of
Page 26
26
resilience are strongly linked, making resilient communities able not only to prepare
and anticipate disruption but also to absorb and recover from the shock afterwards.
All in all, community resilience is multifaceted and changes from one social entity to
the other, with the possibility of finding more vulnerable groups within an otherwise
resilient community. It is essentially the ability to “utilise community resources to
transform and respond to change in an adaptive way” (Maguire and Cartwright, 2008:
8), therefore gain strength as a result of dealing with adversity (Brown and Kulig,
1996/97). Studies showed that community resilience is a process (Kulig and Hanson,
1996) overseeing the enhancement of community cohesion when influenced by a
number of different components ranging proactive members, a community problem-
solving process in place and community leadership (Kulig et al., 2008). As a
theoretical framework, community resilience provides an explanation for how
communities operate as collectives, interacting and creating a “sense of belonging”
(Kulig et al., 2008) which leads to expressing a “sense of community”, contributing to
problem-solving and the ability to deal with disruption (2008).
Page 27
27
2.4 Community resilience and healthcare, resilient healthcare for
communities
After exploring resilience as a concept, associating it with crisis, reviewing the
relationship between bottom up and top down approaches and understanding the
qualities of communities resilience, it is necessary to delve into what facilitates the
development of community resilience. As previously mentioned, Castelden et al.
(2011) found that several components are proper to the concept whether they are
communication, good governance or economic capacity. This section looks into
healthcare as a component of resilience. The choice of this component over others
derives from the fact that healthcare availability is an agent of change, especially for
developing countries and/or communities in crisis. A community can be resilient and
provide for itself in many ways, but certain needs such as health provision demand for
more than just a community effort, they demand available and functioning services.
Moreover the promotion of resilient healthcare for communities brings scientific
knowledge to the realm of decision-making, which can make its best decision when it
has the most cunning data available.
The health status of a community undoubtedly factors into its overall resilience and
vulnerability (2011). According to the European Union (2014) it is vital for modern
health systems to always be accessible and effective, especially in times of crisis. To
remain sustainable and build resilience, they have to be fiscally responsible and to pay
attention to non-fiscal factors such as environmental change, lack of expertise in
certain areas, surges in demand, even with limited resources (2014). To meet
authorities and their crisis management plans, communities can become more resilient
by using the resources in place. If a healthcare system is in place, communities can
contribute in managing a crisis, if there is no system or it is not prepared, it is
necessary to identify the issue for planners to match external resources. According to
Keim (2008: 515) “community-based risk-reduction activities lessen human
vulnerability to the vagaries of natural disasters, especially those activities that
integrate public health”. To address and increase disaster resilience in communities,
local public health is a key agent able to build and maintain human resilience when
facing hazard and vulnerability. Adaptation after a disaster starts at the community
level, therefore public health is essential in the resilience of the community itself. In
providing health services, local healthcare systems reduce burdens such as disease
Page 28
28
that increase vulnerability and enhance safety in strengthening the resilience of the
community against crisis (2008). In promoting “healthy people, healthy homes and
healthy communities” (Shobha et al., 2003) vulnerability can decrease since healthier
individuals are more likely to ‘bounce back’ from disasters and disaster morbidity.
With healthy homes there is a lower risk of structural damage and increased safety,
therefore healthy communities become sustainable and have overall minimalized
exposure to crisis and its consequences. Enhancing healthcare resilience from both an
institutional and a community’s perspectives equates to enhancing adequate
preparedness to hazard, especially in regions were climate change-related events are
frequent. Ultimately “resilience fits the complexities of healthcare more effectively
than principles of high reliability. In essence, resilience represents a shift from seeing
humans as a pathological feature of a healthcare system to one where they contribute
actively to ‘safe’ work and greater patient safety” (Jeffcott et al., 2009).
Page 29
29
2.6 Chapter Conclusion How does resilient healthcare place within the academic discussion on resilience?
This chapter has answered the question by exploring general knowledge on resilience,
resilience within crisis management, the top-down and bottom-up approaches to the
concept and finally studying community resilience and a most vital component of it:
healthcare. Nonetheless, further questions have to be asked in order to understand the
topic and the case. Moreover, the complexity of the notion, paired with crisis and
resilient healthcare require for an in-depth research on indicators capable of linking
the theory to the case and conduct the analysis appropriately. The literature does not
find a complete set of indicators for this subject as it can do with food security for
example. For this reason in Chapter 3 indicators developed ad-hoc will be described
starting from an exploration of the theoretical understanding of resilience and
complementing the search for indicators through an initial expert interview.
A healthcare system is to be understood in general, from its achievements and its
pitfalls, therefore it is important to question every aspect of it. Moreover, in pairing
resilience with crisis we have to delve deep into the practical matters of the problem,
and in the case of healthcare, ask whether the sector, in the given country, can face
disruption. With a sector unable to work under stress, community resilience is
hindered. Lastly, communities have to be able to respond to the healthcare system,
access it, engage with it, otherwise they may not turn to it when crisis hits. All in all,
resilience is “an ideological project that is informed by political and economic
rationalities which offer very particular accounts of life as an ontological problem”
(Evans and Reid, 2013: 92). Whether from a grass-roots or a top-down point of view,
the key to security is in the resilience of people (Toulmin, 2009). It does not
automatically mean protection but it entails adaptation to disruption, not helplessness
in front of it. Insecurity must be accepted as permanent and the concept of resilience
promotes the adaptability of the actors that do not politically strive for a world free
from danger, because they know it is utopic. To some extent, resilience in general and
healthcare in community resilience in particular force us to question what it means to
live when “crisis is the mother of history” (Lilla, 2007).
Page 30
30
3. Research Design and Methodology
In the following chapter there is going to be a presentation of the research design and
methodology employed in this thesis. The research question and sub-questions will be
introduced together with a brief description of the case. Finally, the methodology used
in the case study analysis is going to be explained before proceeding in using it
throughout the next chapter.
3.1 Research questions This research was developed through a guiding research question:
To what extent is Peru’s healthcare system resilient and how can this degree of
resilience be explained?
Furthermore, the following sub-questions were also formulated in order to better
answer the main research question:
1. How does resilient healthcare place within the academic discussion on
resilience?
2. What is Peru’s healthcare situation?
3. What are Peru’s healthcare system’s achievements and pitfalls?
4. How resilient is Peru’s healthcare system from both a top-down and a bottom-
up perspective?
The following section is designed to further explain the main research question and
sub-questions, but especially, to show how they are going to be answered. Each one
will be presented in how it relates to the research and with the indicators that were
assigned to it. In order to increase the understanding of the questions, an
operationalization of terminology will be offered, so that the main themes of the
thesis will be explained clearly. There will be no operationalization of sub-question
1, how does resilient healthcare place within the academic discussion on resilience?
due to the fact that it is a theoretical matter that was covered in the theoretical
framework.
Page 31
31
3.1.1 Main research question
In order to answer the main research question, “to what extent is Peru’s healthcare
system resilient and how can this degree of resilience be explained?” it is necessary
to use the aforementioned sub-questions. Nonetheless, it is useful to adopt a unique
definition for resilience that encapsulates the themes of this analysis - healthcare
system and community resilience. The United Nations’ International Strategy for
Disaster Risk Reduction then, will serve the purpose, as it states that resilience is “the
ability of a system, community or society exposed to hazards to resist, absorb,
accommodate to and recover from the effects of a hazard in a timely and efficient
manner, including through the preservation and restoration of its essential basic
structures and functions” (2005).
3.1.2 Sub-question 2 Sub-question two, ‘what is Peru’s healthcare situation’ is going to be answered
throughout Chapter 4. The chapter is going to present the context of the case, Peru’s
healthcare system, and provide data in order to understand the background of the
overall analysis. This favors the discussion that is going to permeate the answer to the
following sub-questions.
3.1.3 Sub-question 3
The third sub-question, ‘what are Peru’s healthcare system’s achievements and
pitfalls?’ furthers the investigation launched by the first. Continuing Chapter 4,
‘Problem situation’, the question will open to a discussion where the ‘achievements’
and ‘pitfalls’ presented in the case description are going to be examined objectively
according to WHO rules and regulations (found in the IHR). The indicators used are
going to be reflecting the level of access to healthcare for all and the availability of
blood donations.
3.1.4 Sub-question 4 The fourth and final question is a complete analysis on the resilience of healthcare in
Peru. It is composed by a main sub-question: ‘how resilient is Peru’s healthcare
system from both a top-down and a bottom-up perspective?’
This sub-question demands for us to look deep into any policy or technical issues that
a crisis may present: are there plans to tackle it in the healthcare system? Are facilities
capable of withstanding it? Is the nation sufficiently covered? Are all types of
Page 32
32
communities able to access healthcare services when in need?
Because of this, in Chapter 5 ‘Results’ it will be possible to understand the reasoning
behind the answer to the sub-question through the use of the following indicators:
Equal Access to healthcare, Emergency Response Plans in Health Emergencies,
Critical infrastructure protection and “safe hospitals”, Cooperation with non-state
healthcare providers and healthcare-oriented NGOs, Sustainability in blood donations
and Citizens’ engagement in healthcare.
The analysis will be developed over two chapters. The first describes the case and the
‘problem situation’ offering a familiarization to the first and second sub-questions and
providing in-depth information to use in order to understand the complex situation of
Peru’s healthcare system. The situation of the system, its pitfalls and achievements
are embedded into social, economic and historical happenings that have to be
explained to the reader. The second, more analytical, chapter uses indicators to
answer the third and fourth question thoroughly and provide further perspective to the
first two. The indicators will be described in this chapter and associated to one or
more sub-questions.
Page 33
33
3.2 Research design: single case study Every thesis requires a research design in order to conceptualize the problem and
understand how far the findings can reach (Grinnell and Stothers, 1988: 219). The
problem of healthcare resilience is multifaceted and differs from region to region, if
not from state to state, therefore this specific research concentrates on a single case in
which the unit of analysis is the healthcare system in Peru.
The choice of a single case study is due to the specificity of the phenomenon itself. As
Goode and Hatt (1952) state, “the case study … is a way of organizing social data so
as to preserve the unitary character of the social object being studied”. A case study,
according to Swanborn (2010), entails the manifestation of the social subject in its
natural surroundings, within an established time period. It focuses on details
(indicators) attached to the social process and finds the researcher starting from a
broad research question and using theories and data analysis to find an answer
through several data sources, some or which may be engaged with confronting the
case itself (Swanborn). In order to collect information, the process requires a theory to
guide it, even the most primitive. In this research, the primitive theory that opens the
collection of data and its subsequent analysis is the aforementioned United Nations’
International Strategy for Disaster Risk Reduction’s definition of resilience and the
belief that in community resilience, healthcare is substantial in order to ‘bounce back’
from a disaster.
Peru was picked as a case because it is the third country most vulnerable to the impact
of climate change (UNDPLAC, 2015) it experiences climate variations due to El Niño
and overall has unique geographic peculiarities. Moreover its society is multi-ethnic
and presents differences in the socioeconomic sphere, with extreme poverty levels
still high in the most rural areas of the country. The development of the nation is also
going at a fast pace but government spending is not always focused on areas of
welfare. The country is matchless in matters of resilient healthcare in the Latin
American region, therefore its complexity serves the topic as much as the topic serves
its complexity.
The following section presents a rationale for the use of each indicator in the analysis.
Page 34
34
3.3 Operationalization
3.2.1 Indicators
The process of finding the correct indicators was one of trail and error. At first
literature addressed concerns over what aspect of healthcare was the most important
to tackle, whether it was disease prevention, first aid healthcare or general guidelines
for medical safety in a country. Eventually the focus shifted on the fact that the focus
healthcare provision used in this thesis is a component of community resilience,
leading to the development of public administration and crisis management-related
indicators. Although these tackle different aspects of the healthcare system, they are
to be portrayed as all part of a system that is in place to provide to communities. For
this reason, the first indicator at the basis of this research is the subscription to
International Health Regulations. As it will be explained in the following paragraphs
these Regulations are in place to safeguard public health from disease outbreak – and
what better than a resilient health system to do so? Resilience is a practical
application of the regulations in the healthcare environment, especially to tackle any
outbreak and/or crisis to prevent dramatic spread of disease. On the other hand
indicators such as emergency response plans in health emergencies and critical
infrastructure protection and “safe hospitals” were distilled after an examination of
WHO, PAHO, Red Cross and UN guidelines on health management and crisis
management. As a matter of fact these are the most technical indicators that directly
address the substantial role of coordination and infrastructure preparedness for crisis
scenarios. The following paragraphs will go in depth on the peculiarities of the chosen
technical indicators. The remaining four indicators, equal access to healthcare,
cooperation with non-state healthcare agencies, sustainability in blood donations and
citizens’ engagement in healthcare were developed after an expert interview focused
on exploring aspects of healthcare in Peru that were not as highlighted on official text.
Luigina Prosocco of COMIVIS was very kind in answering this thesis sub-questions
for an initial interview and provided insight in the state of healthcare in the country
which lead to confirming some indicators (equal access to healthcare, cooperation
with non-state healthcare agencies, citizens’ engagement in healthcare) that had
already been approached and adding a seventh to the list, sustainability in blood
donations, which is also technical and related to crisis management.
Page 35
35
Once again, the indicators used in this analysis are:
- Adhesion to International Health Regulations
- Equal Access to healthcare
- Emergency response plans in health emergencies
- Critical infrastructure protection and “safe hospitals”
- Cooperation with non-state healthcare providers and healthcare-oriented
NGOs
- Sustainability in blood donations
- Citizens’ engagement in healthcare
In the following section indicators are going to be explained through literature,
information provided by datasets and expert interviews.
Adhesion International Health Regulations
The International Health Regulations are a framework to govern the response to
public health emergencies posing an international threat (Wilson et al., 2008). The
first International Health Regulations were drafted in 1851 as the International
Sanitary Regulations, after cholera epidemics around Europe showed the need for
international cooperation in matters concerning health. After the World Health
Organization was born in 1948, a new series of Regulations were drafted as the
International Health Regulations in 1969. These concerned notifiable diseases such as
cholera, plague and yellow fever and presented a series of limitations in the
cooperation among countries that caused the 1995 World Health Assembly to revise
them. By 2005, a new and more organic set of Regulations was proposed and it
became binding in June 2007 in 194 State Parties.
In introducing the concept of “public health emergency of international concern”
(WHO, 2005), the revised Regulations provide guidance to protect travel and trade in
the international community from the spread of health emergencies. They also require
from each state the development of health surveillance and response systems (Wilson
et al., 2008). To implement the IHR (WHO, 2005), State Parties are required to fully
respect human rights, dignity and fundamental freedoms through the guidance of the
WHO Constitution and aiming at universal application to protect all from disease.
State Parties have the right to legislate and implement legislation in upholding the
Page 36
36
Regulations (2005).
The security of populations is in synergy with their ability to thrive, therefore
strengthening health regulations is necessary to avoid permanent damages to the re-
habilitation period after a crisis. This is also one of the main critiques to the IHR,
which are seen as subordinating health to economic and security concerns (Wilson et
al., 2008). Public health officials agree on the importance of collective action in
managing the spread of disease and compliance is of utmost importance, especially
for developing countries that may require assistance or lack in strong legal
mechanisms.
Using the International Health Regulation as an indicator provides a solid foundation
on which to build the analysis on whether Peru’s healthcare system is resilient enough
to support communities through crisis. By halting the spread of diseases and
protecting international travel and trade, they limit the long-term damages that health
crises can have, especially on the poorest communities.
Equal Access to Healthcare
In recent decades evidence has shown that the socioeconomic status of a person does
have an influence on their ill health (Mustard et al., 1997; Gordon et al., 1992;
Wilkins et al., 1989). The issue becomes especially challenging in developing
countries, where there may be two-tier health systems and medicines are less
affordable by less privileged income groups – widening the gap between the wealthy
and the poor. Selecting Equal Access as an indicator in the analysis provides further understanding
on the distribution of health resilient and less health resilient communities around
Peru. Understanding where the healthcare system may lack when catering to the
population is essential to answer the main research question and make final policy
recommendations, too.
Emergency Response Plans in Health Emergencies
The gap between income groups particularly shows in emergencies, as the poorest
sectors of the population suffer disproportionately. The enormous economic costs of
post-crisis relief and International Health Regulations demand for appropriate crisis
management, which includes emergency response plans, “effective national and
international capacities, intersectoral collaboration, the promotion of equity, the
Page 37
37
protection of human rights, and the advancement of gender equality” (WHO, 2013).
Drafting a plan to tackle emergencies is vital to prepare communities and the
healthcare system. If communities can count on the healthcare system in a post-crisis
environment, they can ‘bounce back’ and be resilient.
Emergency Response Plans in Health Emergencies Infrastructure Protection and
“Safe Hospitals”
Whenever the concept of “safe hospitals” is mentioned, it exemplifies the
infrastructures that will not collapse after a disaster and will remain open to patients,
providing urgent care and services in critical times. A natural disaster is likely to
disrupt the functioning of several types of infrastructure in an urban or semi-urban
setting, including healthcare facilities. For example, with the 2007 Pisco earthquake,
most health facilities in the city and in the surrounding areas of Cañete, Chincha and
Ica were damaged as a consequence to the quake (Rios and Zavala, 2008). Eight
hospitals suffered several damages and three hospitals were destroyed (2008). To
ensure the safety of health facilities in crisis a wide range of actions has to be put in
place: training for healthcare personnel, the hardening of health facilities,
implementation of resilience and redundancy and technological advance in safety
provision. All these efforts imply the necessity of a strong investment in the cause by
politicians and stakeholders. World Health Day 2009 focused on this crucial matter,
sending three main messages: the need for all health facilities to withstand disaster;
the need for all health facilities to function throughout any emergency; and the need
for all health workers to be trained and be ready to respond to disaster situations.
This indicator is undoubtedly essential to measure the practical resilience of health
facilities in Peru in times of crisis and it is going to provide insight in the country’s
healthcare system’s deficiencies.
Cooperation with private non-State healthcare providers and healthcare-
oriented NGOs
Peru has a two-tier healthcare system, basic care is funded by the government but
those who can afford it can also access secondary tiers of care with better quality of
services. This is not an a-typical situation, most countries have a two-tier system of
care, but it may create inequality in access for all citizens, and differences in quality
Page 38
38
of care and distribution in the territory depending on how the public healthcare system
is managed and how many public funds go into it.
In addition to this, nongovernmental organizations have for a long time being
involved in healthcare provision. The most famous in doing this are of course Doctors
Without Borders and the International Red Cross, but smaller NGOs also provide
services focusing on particular aspects of care or work to link communities to
governments. Furthermore, NGOs “have exhibited a special capacity to work within
the community in response to expressed needs. They have a flexibility and freedom to
respond in innovative and creative ways to a wide range of requests and situations”
(WFPHA, 1978).
As part of the research will also consist of interviews to experts of NGOs involved in
healthcare, the contribution of non-State entities to the healthcare situation is Peru can
make a difference in the overall resilience of communities, making this a necessary
indicator in the analysis.
Sustainability in blood donation
Victims of disaster reaching hospitals are always in need of urgent care and this also
demands for blood availability, as patients could be wounded, or need to undergo
surgery. In order to comply with international directives, blood donations in a country
have to be at least 2% to cater to the national demand, but to achieve such milestone it
is necessary to launch awareness campaigns to achieve more donations to not incur in
the problem of having to buy it from private blood banks.
This indicator was suggested during the interview with Luigina Prosocco, expert on
the field working with the Italian NGO COMIVIS. It is useful in order to understand
the preparedness of Peru in case of crisis and for first aid purposed.
Citizens’ engagement in healthcare
The poorest sectors of society are often marginalized when shaping health policy and
practice of developing countries. Moreover, traditional healing methods within certain
communities can distance citizens from public healthcare when the latter is not
accessible, therefore sustainable change in healthcare practice can only be of impact
when all citizens can have their voices heard. In order to attract citizens to public
healthcare, they have to be conscious of health rights, provision of services and be
completely equal before the law and in practice. Ensuring that all communities
Page 39
39
understand and approach public healthcare services is of utmost importance in any
system, hence the necessity to enlist this as an indicator. This is not to state that
traditional methods are ‘bad’ or ‘inadequate’, but they should be one of the options
rather than the only one whose mechanisms are trusted.
Page 40
40
3.4 Triangulation of methods
3.4.1 Data collection and data exploitation The following section presents the data sources used for the analysis. In qualifying the
ad-hoc indicators, the data was sourced to be thorough in the research and allow an
exploration into the various dimensions of the matter such as poor communities,
healthcare mishaps and institutional plans.
Initial expert interview
In order to ensure a balanced analysis on the healthcare system in Peru, an expert was
consulted. Luigina Prosocco, who is working with the Italian NGO “Comunità
Missionaria di Villaregia per lo Sviluppo” (COMIVIS), Villareggia’s Community
Mission for Development, was very kind in answering the thesis’ sub-questions with
her insight, these are general questions that allow for an understanding on each
indicator. These lead to confirming previously conceived indicators and creating a
seventh, sustainability in blood donations. The expert interview will be occasionally
referred at in the following chapters but it is important to understand it was an initial
assessment and data was found through desktop analysis.
Desktop analysis
Starting from International Health Regulations, there is going to be a research on data
through reports by various sources. Looking into the Peruvian healthcare system is
going to give the opportunity detect the problems this has in enforcing any
Regulations.
To understand the state of Equal Access, articles and reports from PAHO and WHO
are going to be used, as the information is quite organic and a variety of matters are
also tackled. As we will see the matter of access is divided into what are also the
achievements and pitfalls of Peru’s healthcare system, therefore there will also be
insight on the status of health coverage of the citizens with data provided by
government sources and articles.
For emergency response plans in health emergencies region-wide reports from PAHO
are going to be used. Data on critical infrastructure protection and "safe hospitals" is
going to be tracked down mostly looking at regional reports.
Cooperation with non-state entities and citizens’ engagement in healthcare are
indicators that can provide quite a lot of insight, especially regarding more local
Page 41
41
situations. This indicator is going to be researched through articles and data in reports,
as the matter of Communities Engagement. Data on blood donations availability is
going to be researched through government guidelines and reports, and articles from
external sources.
3.5 Validity The single case study approach offers strong internal validity when using a variety of
data sources such as government reports, international organizations reports and
articles to gather insightful information (Bryman, 2012). Of course as this is a
qualitative type of research focusing only on Peru, the results are not going to be
externally valid or applicable on a wider scale outside of the country in question.
However this case study can offer a ‘theoretical generalization’ thanks to the insights
provided by the indicators. It may be possible to apply the same indicators to similar
studies and understand more about the topic of healthcare and resilience.
Page 42
42
4. The Case: Peru
This chapter is going to provide basic information of the country of interest, Peru. In
order to provide an in-depth evaluation of the status of healthcare in the country, it is
necessary to understand the context in which it is set. In addition to this, the chapter
will also start the analysis by providing an understanding of two out of the five sub-
questions, namely ‘what is Peru’s healthcare situation?’ and ‘what are Peru’s
healthcare system’s achievements and pitfalls?’ - as this thesis focuses on the
healthcare resilience of Peru. Paragraph 4.2 focuses on answering the first question by
providing an outlook on the healthcare system, while Paragraph 4.3 will describe the
problem situation, thus answering the question ‘what are Peru’s healthcare system’s
achievements and pitfalls?’
4.1. Country of interest: Peru The following paragraph will produce a general introduction of Peru. Map 1, Political Map of Peru (mapsof.net)
Page 43
43
The following sub-chapter is an overview of the country of Peru, our case study. The
country is going to be presented to the reader in its physical and societal peculiarity in
order to better understand the chapters and sub-chapters to follow. Data on the
political organization and socioeconomic advance of the country are substantial to
comprehend the references to uneven spread of health workers and infrastructure, or
to highlight the level of engagement of certain communities compared to others. As
previously explained in 3.2 Research design: single case study the choice of analysing
this country stemmed from its unparalleled characteristics and this section is
necessary to understand the final assessment and answer to the research question.
In Spanish ‘Perú’, in Quechua ‘Piruw’ and in Aymara ‘Piruw’, the Republic of Peru is
located in Latin America, specifically on the western coast facing the Pacific Ocean.
It borders with Ecuador and Colombia in the north, Chile in the south and in the east
by Brazil and Bolivia. Its geographical location made it a uniquely biodiverse
country, with landscapes raging from Andean peaks from north to south, to coastal
regions in the west and the Amazon rainforest in the east. The peculiarity of Peru’s
geography makes the country vulnerable to a wide range of disaster situations,
requiring an in-depth analysis over its crisis management abilities.
The Republic of Peru is a Presidential representative democratic republic governed
through a multi-party system and divided into twenty-five regions. The developing
country has suffered from periods of unrest and both internal and external conflict,
but 2011 data showing high Human Development Index score of .752 and a lowering
of the national poverty level to 25.8% (Gestión, 2013; UNDP, 2015). The twenty-five
regions and one province (Lima) have each its own elected government with its
president and its council serving four-years long terms (Ley N° 27867, Ley Orgánica
de Gobiernos Regionales, Article N° 11.). In an effort to improve popular
participation, regional governments were given powers over regional development,
the execution of investments projects, the management of public property and
administration and promotion of activities related to the economy (Ley N° 27867, Ley
Orgánica de Gobiernos Regionales, Article N° 10.). Lima is managed by a city
council (Ley N° 27867, Ley Orgánica de Gobiernos Regionales, Article N° 66.).
The main economic activities are mining, manufacturing, agriculture and fishing and
exports factor largely on the country’s income. According to the World Bank, the fast
growing economy of Peru positioned it as the 39th largest economy in the world with
Page 44
44
classification as upper middle income (BBC, 2012), although radical reforms in
previous decades tackling growth and egalitarian distribution of income did not
completely solve its social divides (Thorp and Bertram, 1978). As of 2010, 31.3% of
the population is poor and 9.8% live in extreme poverty (Instituto Nacional de
Estadística e Informática, 2010: 38).
There are around 31 million inhabitants in Peru, placing the country fifth in the most
populous countries in South America. The most populated areas is Lima, overall 76%
of the population lives in urban areas and the remaining 24% in rural areas (Instituto
Nacional de Estadística e Informática, 2008). The population is relatively young, with
28,9% of 15 or less years old, 62,3% between 15 and 64 years (legal working age) of
age and only 8,7% over 65 (INEI, 2013).
Peru is a multiethnic country and the demographic outlook of the nation includes
natives of the American continent (Amerindians), descendants of European
colonizers, Africans and Asians. According to DNA testing, on average 79.1%
Peruvians are Native Americans, 19.8% are European and the remaining 1.1% from
the African continent (Montinaro et al., 2015). The main language spoken is Spanish
but a high number of Peruvians can speak native languages such as Quechua.
In paragraph 4.1.1 the regions are going to be listed together with additional
information on the poverty levels in each geographical area. This because
communities that require resilient approaches in dealing with crisis are often not the
richest and find themselves in precarious conditions.
Page 45
45
4.1.1 Regions and poverty levels throughout the territory
The following is a list of the regions (or departments) of Peru, as it is also illustrated
in Map 1.
• Amazonas
• Ancash
• Apurímac
• Arequipa
• Ayacucho
• Cajamarca
• Callao
• Cuzco
• Huancavelica
• Huánuco
• Ica
• Junín
• La Libertad
• Lambayeque
• Lima
• Loreto
• Madre de Dios
• Moquegua
• Pasco
• Piura
• Puno
• San Martín
• Tacna
• Tumbes
• Ucayali
Page 46
46
Map 2, Vegetation Map of Peru (goperu.com)
Population density is higher in coastal and urban areas, and it also in better socio-
economic conditions, although with differences depending on the specific urban area
(whether coastal, Andean or rain forest). The least populated areas are located in the
rain forest part of Peru, from south to north-east. Map 2 shows the vegetation areas in
Peru, and it is possible to locate three macro-areas: coastal, Andean and rain forest
areas. Poverty levels are spread unevenly throughout the territory, in fact INEI (2014)
data shows that the Andean area and the rain forest areas have higher concentrations
of poverty, 34,7% and 31,2% respectively, while in coastal areas the level of poverty
is at 15,7% overall. This is an important improvement from 2004, when Andean and
rain forest areas counted respectively 70% and 70,4% of the population in poverty
conditions (48,6%, also a high level, was the data about coastal areas). As for extreme
poverty levels, in 2013 coastal areas saw 0,9% of the population in extreme poverty,
Page 47
47
while Andean and rain forest areas saw respectively 9,2% and 6,1% of the population
in conditions of extreme poverty. Nonetheless, this is an improvement from 2004,
when levels of extreme poverty were higher in all areas: 4,6% in the coast, 32,1% in
the Andes and 23,6% in the rain forest area.
Page 48
48
4.2 The Case: Peru’s healthcare system Peru abides by International Health Regulations set by the WHO in 2005. Peru’s
healthcare system is a decentralized, two-tier sector administered by five different
entities. The two major ones are the Ministry of Health (MINSA) and EsSalud, and
the remaining three entities are the Armed Forces (FFAA), the National Police (PNP)
and the private sector (Alcalde-Rabanal et al., 2011). The public health sector,
MINSA, is largely financed through indirect taxation, it offers health services to
people without health insurance in exchange of a fee and through the Seguro Integral
de Salud (SIS), a service of utmost importance in creating equality and access as it
establishes basic health coverage for all, especially the poorest (2011). In 2009,
universal healthcare became a reality thanks to the Ley Marco de Aseguramiento
Universal en Salud, which guarantees basic health coverage for all in order to cater to
all the health problems that citizens suffer from (Wilson et al., 2009). Social security
is divided into two sub-systems: EsSalud or private practice. The former caters to
employed citizens with a health plan, it aims at providing universal insurance
coverage, improving public and private partnerships in healthcare provision,
especially through technologic advance, and improving public investment in the
healthcare system so that regional inequalities will disappear (Cetrángolo et al.,
2013).
Private practice is divided into for-profit and non-profit entities. With ‘private for-
profit’ we address any type of private hospital, private insurer or private practive, but
it also includes traditional medicine providers such as shamans and healers, among
others (2011). The non-profit group is made of NGOs, Catholic Church-funded care
and citizens groups. These receive funding by multiple donors and governments.
The health systems of the Armed Forces (FFAA) and the National Police (PNP) cater
to members of the military or the police and to their families.
The system is articulated and presents a varying degree of coordination and overlap,
with health workers working more than one job in more than one subsector (WHOb).
In 2016 the government published laws on SuSalud, the entity in charge of
standardizing the quality of healthcare provision nationally (DL1158) and with focus
on primary care (DL1166). These laws can be key in achieving adequate health
services for all.
Page 49
49
4.3 Problem situation: achievements and pitfalls of Peru’s healthcare
system
4.3.1 Infrastructure distribution
The Peruvian healthcare system suffers from lack of funding, as it has the lowest total
health care expenditure as per cent of GDP in South America (WHO, 2013). In 2012,
for example, only 39.6% of the allocated budget was actually used due to
“administrative bottlenecking” and local governments’ failure in administering the
funds (Málaga, 2012). Table 4.1 shows the gap between regional investment in
healthcare and Peruvian. The spending has started showing consistent increase only
since 2005 (year in which the International Health Regulations were reformed and the
Hyogo Framework for Action was agreed upon) but it has not grown as dramatically
as the rest of the region.
Table 4.1 (WHO, 2015)
Page 50
50
Table 4.2 (INEI)
Ministry of Health hospitals are spread differently throughout the country, with
90% in urban areas, &% in marginal urban areas and only 3% in rural areas (Rios
and Zavala, 2008). In order to have further understanding of the differences in the
provision of healthcare among regions, Table 4.2 presents the distribution of
health infrastructure throughout the country.
It is possible to notice uneven distribution of health establishments between Lima
and other, poorer regions. Loreto, for example, is the largest region in the country
as it extends over the Amazon Basin, the poverty rate is at 70% but citizens can
only count on 14 hospitals, 85 health centers and 347 health posts. Apurimac,
where the poverty rate is 78%, is smaller than Loreto but also presents a lack in
hospitals.
Page 51
51
4.3.2 Health workers The overall health worker population of Peru has increased despite of migration
outwards in recent years. According to a WHO report, “Peru reported the presence of
a mechanism to share data and inform policy-makers, and fairly good performance in
retaining its health workers in rural areas. It could further improve its HRH planning
and information system, and intensify efforts in securing additional investment in
HRH from both domestic and international sources.” (WHOc). The World Health
Organization (WHOc) congratulated Peru for it renewed efforts in redistributing
health personnel, but an availability gap still exists, leading to health vulnerability in
certain geographical areas. In 2007 the gap was estimated to be “between 8,446 to
15,363 for doctors, between 10,541 to 19,393 for nurses, and between 6,884 to 14,855
for midwives” (WHOc). Moreover, the WHO also states that “a recent publication
estimated that the overall deficit of specialist doctors with regard to offer is about
45%, with important variations at sub-national level” (WHOc).
Table 4.3 (WHOc)
Page 52
52
The following charts allow to understand the inequalities in the distribution of per
doctors and nurses in each region compared to the inhabitants they attend to.
Table 4.4 (INEI)
Table 4.5 (INEI)
Page 53
53
Consequent to inequalities in infrastructure distribution, doctors and nurses cannot
always provide services at high standards for all people of all regions, as in some they
have too many people to attend to. The implementation of SIS increased the demand
for health providers, but these are unequally distributed throughout the territory, Lima
and the coastal area have in fact the highest densities, while regions such Loreto,
Piura, Cajamarca and San Martin (some of the poorest) have the lowest in the country
(Ministerio de Salud, 2011). The estimated 24% of the population is still living in
rural areas, vulnerable to neglection and disadvantages in access, but also to the worst
health and social inequalities afflicting the developing country.
A plan to distribute health workers and continue in offering coverage to the poorest
region is making demographic differences disappear (WHOb). The Institutional
Strategic Plan 2008-2011 of the Ministry of Health of Peru seeks to integrate state,
government, and healthcare sector policies (WHO, 2013). This will be vital both for
personell and infrastructure improvements. As Luigina Prosocco of COMIVIS
explained in her interview, so far waiting times are very long and there is little
communication between public hospitals, which consequently leads to loss of time
and possible fatal losses.
In conclusion to the matter of health workers, care for the elderly is one of the sectors
suffering the most. Older adults do not receive proper geriatric care, as it is barely
taught in the only six (of the thirty four) Peruvian medical schools offering courses on
the discipline, and there is little coordination across all levels, as well as little
awareness over the necessity of continuative care (Ferng, 2014).
Page 54
54
4.3.3 Blood donations
One of the pitfalls found in the interview with Luigina Prosocco of COMIVIS was the
scarcity and unorganization of blood donations. According to the Peruvian Ministry
of Health, MINSA, 86% of blood donations are collected in Lima and only 0.5% of
Peruvians donate their blood (MINSA). In order to comply with international
directives, blood donations in a country have to be at least 2% to cater to the national
demand. Currently, Peru requires 600’000 units of blood to cover its internal demand,
but in 2013 it only had 185’000 (MINSA). More often than not, patients seek blood
by themselves, endangering their situation by buying blood that may not be safe, as
often those outlets that sell blood do not undergo efficient testing and collect it from
anybody in need of money to survive poverty. For example, in 2004 and 2005, Peru
did not screen blood units for HIV (PAHO, 2008), therefore endangering patients
Only 5% of all blood donations in Peru come from volunteer donors, making the
country one with the lowest indicators in Latin America (Chase, 2014). According to
Dr. Loayaza, interviewed by the online publication Peru This Week, there are two
main problem areas in supplying blood: self-suffiency, which is lacking as it does not
correspond to international standards, and a lack of volunteer donors, who give the
highest quality of blood thanks to health checks and scrutiny (Chase, 2014).
Page 55
55
4.4 Chapter Conclusion All in all, Peru is at a “demographics crossroads” and is facing a number of problems
in the administration of the health system. Public expenses on healthcare are
drastically reduced while private citizens are spending more and more, especially on
medicines and medical exams (Cetrángolo et al., 2013). Infrastructure and human
resources are not up to standards and are distributed unevenly, as the previous
paragraphs have shown. In the next chapter, access and emergency plans will be
further studied from a national and a community perspective, but in this past chapter
we focused more on the system in general, gave an idea of what could prove to be
resourceful in the future (the SIS insurance) and what the pitfalls are so far. Uneven
distribution of infrastructure, uneven distribution of health workers, dangerously low
blood donations, matters causing inefficiency and further inequality in healthcare
resilience.
Page 56
56
5.Results
As discussed in Chapter 4, Peru has a two-tier healthcare system adhering to
International Health Regulations and allowing access to all sectors of society through
the SIS insurance system. Private healthcare includes traditional medicine and NGOs
providing services around the country, but the most health-efficient area is
undoubtedly Lima and the surrounding Metropolitan area. Funding for the healthcare
sector has increased over the past years, but it is still scarce compared to other
countries in the region and it spreads unevenly in the country. With 2016 laws on
healthcare standardization, the national government has taken important steps in
ensuring provision nation-wide and to give access to primary care. The main findings
in the pitfalls of the system resulted from the examination of data proposed by the
interview and they are, in summary: - Infrastructure lacking in non-urban and poor areas
- Health personnel spread unevenly and struggling to attend to patients in the
least-served areas
- Serious scarcity of blood donations, a vital element of disaster recovery
The universal health coverage plan (SIS) was also mentioned as an achievement and it
will be further studied in this chapter.
Although from general data it may not be recognised instantly the impact that these
main pitfalls has on the country’s healthcare system is consistent, as we will see later.
Regional and class divides are evident in country data from the Institute for Research
and they mostly show when discussing at-risk groups such as the elderly and poorer
women (as in subchapter 5.4.2 Engagement and access: vulnerable sectors of society).
As also discussed in the interview with Luigina Prosocco of COMIVIS, the overall
greatest achievement of the system is the development of SIS, the national insurance
plan that provides healthcare for any citizen in need. Although with its own structural
problem, the plan has proved efficient in catering to the needs of Peruvians and is an
important tool to insure equal access to healthcare.
Understanding the resilience level of Peru’s healthcare system catering to
communities in face of crisis requires an in-depth analysis on the sub-questions
established in previous chapters. The first, ‘what is healthcare resilience?’ was
Page 57
57
thoroughly explained in the Theoretical Framework, while the chapter on the Case
offered detailed picture of questions two and three – respectively ‘what is Peru’s
healthcare situation’ and ‘what are Peru’s healthcare system’s achievements and
pitfalls?’ also summarized in the previous paragraph. The following sub-chapter will
discuss in depth the remaining sub-question:‘how resilient is Peru’s healthcare
system from both a top-down and a bottom-up perspective?’ All indicators are going
to be used in the explanation of data results, but there is going to be an extensive
discussion dedicated to the remaining four indicators used in this research:
Emergency Response Plans in Health Emergencies Safe Hospitals, Equal Access and
Engagement. A final paragraph is going to provide a complete summary of all the
findings, which is going to allow a conclusion to this thesis with consequent policy
recommendations.
Page 58
58
5.2 How resilient is Peru’s healthcare system from both a top-down and a
bottom-up perspective?
The following sub-chapter is going to present data on emergency planning by the
Peruvian government and on advances in making Peru’s hospitals safe. The indicators
used tackle the question both from a bottom-up and a top-down perspective. Data was
acquired through research on institutional websites and was introduced by the
interview with Luigina Prosocco of COMIVIS. Paragraph 5.2.1 will evaluate the
plans of the government to respond to health emergencies while the second paragraph
(5.2.2) is going to concentrate on Safe Hospitals, presenting data by the PAHO and
the interview. Paragraphs 5.2.3, 5.2.4 and 5.2.5 look into engagement and access. The
basic element to go understand these two indicators is to be found in free healthcare
provision, the SIS program, in 5.2.3. Paragraph 5.2.4 analyses engagement in time
and among various groups of society. Finally 5.2.5 takes into account the most
vulnerable groups to conclude on the indicators Access and Engagement.
5.2.1 Emergency Response Plans in Health Emergencies
In case of disaster, nearby hospitals and health facilities are among the first public
services to provide care and because of this, they have to remain functional. In the
aftermath of disasters, hospital failure can worsen the situation and cause major life
loss for the population. In disasters, hospitals are not only critical in emergency, but
also in the recovery process, as they monitor disease outbursts and continue in caring
for the victims. According to UNISDR studies, “The long-term impact of the loss of
public health services on the Millennium Development Goals exceeds the impact of
delayed treatment of trauma injuries” (2009). They have key roles in preventing
outbreaks, public health prevention campaigns, drive innovation through research and
be a focal point in strengthening communities (2009).
According to Resolución Ministerial Nº 517-2004/MINSA (Ministry’s of Health
Resolution 517-2004), there are three different types of alerts in case of a Health
Authority-declared emergency: Green Alert, Yellow Alert and Red Alert (MINSA,
2004). The declaration is made to insure care for all those affected, adequate
protection of infrastructure and the operative effectiveness of health establishments
(2004). The magnitude and intensity of the foreseeable event decide whether to call a
Green, a Yellow or a Red Alert.
Page 59
59
The Green Alert is established when the Office for Defense of the Health Ministry has
proof of a possible adverse event through monitoring and complementary sources.
The event would ostracize the safety of citizens, therefore health infrastructure have
to put into practice emergency plans and be ready (2004). A Yellow Alert is
established when the Office for Defense of the Health Ministry receives information
over an imminent or high probability adverse event that require healthcare entities to
actualize their contingency plans and prepare patients and infrastructure for the
execution of specific tasks aimed at safety and security. Demands for healthcare
provision are likely to rise in such events, therefore the Yellow Alert requires to act
on previously approved contingency plans. The last type of alert, the Red Alert, is
established when the population suffered directly and indirectly from damages caused
by an adverse event and demand for healthcare provision is high. As the other two
alerts, it is also called after the Office for Defense of the Health Ministry has received
proof of serious conditions affecting citizens and the fatality of events requiring
immediate care for patients with the help of previously approved contingency plans.
After the 2007 earthquake in Pisco, approval ratings of then President Alan Garcia
soared because of the perceived effectiveness of the government in tackling the crisis
and covering hospitals’ needs (UNISDR, 2009).
5.2.2 Critical infrastructure protection and Safe Hospitals
Between the years 1981 and 1996, “a total of 93 hospitals and 538 health centers were
significantly damaged as a result of natural disasters in Latin America and the
Caribbean” (PAHO, 2000). This means that the region is geographically vulnerable to
disasters and consequently also are its hospitals, which are often destroyed by
earthquakes, or hurricanes, or floods, mining the resilience of communities and
causing enormous direct and indirect economic losses for the system, populations and
governments. Moreover, a damaged health infrastructure does not recover at the same
pace as other services, as buildings may stand still but they may be rendered incapable
of functioning. This relates to the study of Peruvian healthcare resilience because the
technical functioning of infrastructure protection is at the very basis of a resilient
healthcare system catering to communities. Moreover, the vulnerability of Peru to
disaster was highlighted in previous chapters (e.g. 3.2) therefore understanding the
capability of infrastructure becomes vital.
Page 60
60
The WHO, the World Disaster Reduction Campaign on Hospitals Safe from Disaster
and the PAHO launched a campaign in 2009 to raise awareness over the necessity of
protecting lives in disaster through the structural resilience of health infrastructures.
In order to do so, facilities and services require to be functioning at any circumstance
and to develop strong emergency management skills in health workers and
institutions. They need to be Safe Hospitals. A Safe Hospital is a concept introduced
by the Hyogo Framework for Action 2005-2015, which deems it to be any health
facility able to maintain access to all its services and work at maximum capacity
under stress provoked by disasters or emergencies (UNISDR, 2005). They have to be
able to protect life, investment and operations (UNISDR, 2005). The PAHO
developed a Safety Index score to determine in which category a facility falls and
whether it needs intervention. The categories are: Category A, for facilities that are
suitable to withstand crisis and to continue working while also protecting its
occupants at any time; Category B, for facilities that can withstand disaster but are at
risk and; Category C, for facilities unable to protect the life of their occupants during
disasters (PAHOa). The PAHO states that the Index is to be applied in a regional pilot
involving Peru’s hospitals, too, as preliminary results show consistent vulnerability in
infrastructural elements and equipment. Another elements found by the PAHO in
improving Safe Hospitals was the necessity of strong political commitment by
institutions. Technical and legal progress can only be achieved through institutional
methods in order to guarantee investments of resources and action, but so far, as
previously explained, the expenditure on healthcare in Peru is low.
Also thanks to the approval of the Andean Strategic Plan for Preparedness and
Response in 2005, in 2011 the PAHO reported improvements by creating a National
Safe Hospitals Committee, a national policy on safe hospitals and started the
evaluation of vulnerable facilities (preventionweb.net, 2011). In 2016, “Peru’s
Ministry of Health, working with EsSalud, the Health Social Security Service; the
Health Department of the Armed Forces and Police; and the private sector, updated
the nation’s Safe Hospitals Policy to cover a five-year period, through 2021” (PAHO,
2016). At the time of writing, the update to the Safe Hospitals Policy is yet to gain
approval nationally, but so far the country has evaluated 90% of public hospitals
(2016). The assessment allowed the implementation of measures to improve safety
conditions and non-structural components (2016). Hospitals in the Lima Metropolitan
area and nationwide were assessed for their vulnerability and five have ranked in
Page 61
61
category C (PAHO, 2016), requiring consistent investments. Furthermore, according
to the PAHO there was also progress thanks to the work of health professionals
applying the Hospital Safety Index which found necessary to “update design
standards in primary care facilities, hospitals and other health facilities to meet safe
hospitals criteria; incorporate non-structural safety measures; and in the use of base
isolation and seismic trigger systems, as part of the National Building Code” (2016).
The interview with Luigina Prosocco of COMIVIS gave testimony of infrastructural
vulnerability. When generally asked whether Peru’s healthcare sector was capable of
withstanding crisis, the answer was negative: “I sincerely think it cannot, as the
majority of hospitals are old and could collapse with an earthquake. In previous years,
green areas near hospitals were reserved to become field hospitals in case of disasters,
but some of those have now become commercial areas”. Coupling this with blood
banks lacking donors and uneven spread of infrastructures and personnel, even the
smallest disaster can become fatal for large parts of the population.
5.2.3 Access: SIS – Seguro Integral de Salud
The health coverage for the unemployed, the poorest or informally employed in Peru
is called SIS, Seguro Integral de Salud. It has been developed throughout the past
decade and it offers access to basic health service and, as Luigina Prosocco from the
organization COMIVIS stated, chronic diseases like diabetes are not covered, waiting
times are long and medicines are not always available. The bureaucratic process to
obtain the insurance and structural problems (reaching facilities, etc.) prove stressful,
especially in non-urban areas. Nonetheless, it has recently opened to more patients
affected by disease, especially to those suffering from cancer that cannot afford better
care, paving the way to improvements to the sector and equal access. According to the
head of the SIS programme, Julio Acosta Polo, in 2016 there were 17 million citizens
using the SIS insurance programme (MINSA/SIS, 2016). Funding for the program
increased between 2012 and 2015, from 47.91 Peruvian Soles (13.05€) per patient to
91.91 Peruvian Soles (25.04€) per patient (2016). Only in 2015, 65 million medical
services were provided to more than half the population. By also caring for cancer
patients, the SIS program was able to provide 306’000 medical examinations (2016),
working not only with those affected but also providing more access and increasing
awareness on the subject. In terms of access, these data shows that the SIS insurance
Page 62
62
program is no longer just a tool for the poorest sectors of society, as there are three
types of insurance products - Free, Independent and Entrepreneur (for small business
owners) - catering to a variety of social groups (2016). Without previous socio-
economic screening, pregnant mothers, newborns, children until 5 years of age, pupils
of public kindergartens and of public primary schools (2016). As we will see further
in the paragraph, this openness improved the overall conditions of mothers and
women in general, bridging societal gaps (WHOd).
The real question behind the SIS program is not whether it can be effective, it already
shows slow but steady advance in care provision for many, but whether it is
sustainable. With the rise of SIS users, the government-sponsored EsSalud
programme also improved but failed to attract users. Instead of paying their own
EsSalud insurance, citizens prefer to seek care in private clinics, which have shorter
waiting times (La República, 2016). If citizens’ health investments are not into the
public, the SIS programme will eventually prove unsustainable, with serious
consequences for the population.
5.2.4 Engagement: Reliance on the healthcare system
Before delving into the specifics of engagement and reliance on the system, it is
important to point out that another indicator in this research – blood availability – is
significant in understanding that the population is disengaged and not accustomed to
the healthcare system enough to participate in donations. This is not a positive signal.
In order to understand the level of engagement of citizens to public healthcare, PAHO
and WHO databases were consulted. Although this approach may not be orthodox
compared to other types of research such as interviews, the data gives a good picture
of how much citizens have become reliant on the healthcare system in Peru in their
daily life. Reliance is an important factor that has to be met by hospital security in
case of disaster, as previously discussed.
Table 5 uses PAHO data in showing the general increase in access to improved
sanitation infrastructure in Peru from 1990 to 2008. The light pink indicates the
general trend, the maroon the rural population’s trend and the orange the urban
population’s trend. It is particularly important to notice the rural population’s
dramatic increase in using sanitation facilities since 1990, which is reaching 50%. Of
course, it is always preferable for rural communities to go beyond this level of access.
Page 63
63
Table 5 (PAHOb) Thanks to WHO Global Health Observatory visualizations, it was possible to
understand how much the increase in sanitation facilities impacted on various groups
of citizens and if they were able to bridge gaps in healthcare use and approach safe
health services in the period between 1996 and 2012 (WHOd).
Table 5.1 (WHOd)
As shown in Table 5.1, women of all social groups are more and more able to tackle
reproductive health matters. What is of utmost importance is the increasingly narrow
gap between social groups, a consequence of equal access opportunities
Page 64
64
Table 5.2 (WHOd)
Table 5.2 also shows improvements, especially in antenatal care coverage, although
not as significant as Table 6 when it comes to the poorest communities. There is a
serious gap in maternal health interventions, especially in births with skilled health
personnel present. Although the situation has undoubtedly improved since 1996,
when only 20% of the poorest mothers were giving birth with health personnel, they
were still at 60% in 2012, compared to the almost 100% of the three richest social
groups. Although births are not necessarily attributable to resilience in itself, these
data shows that there are still gaps to bridge in catering healthcare to the poorest
communities (also found in rural or semi-rural regions) and vulnerable members of
society (poor women), therefore it eventually has incidence on the overall capabilities
to recover after crisis.
Page 65
65
5.2.5 Engagement and access: vulnerable sectors of society
Older adults
Table 5.3 (WHO, 2015)
As previously mentioned, care for the elderly is a serious problem in Peru and in the
region (Ferng, 2014). The older adults population is growing, life expectancy is now
at 77 (WHO, 2015) and it has increased of five years between 2002 and 2012 (Table
5.3). Healthcare needs also evolved, but existing health services are not able to fully
cater to these new patients. Older age adds variables to health problems and because
of this, research trials do not include the elderly. This means their problems may not
be fully understood and they may be discharged with drugs prescription or receive
standardized care. Financial access is also of great concern for this societal group: up
until 2014 one in four older adults were still prevented from access because lacked
any kind of insurance, including SIS (Ferng, 2014). There have also been surveys
reporting poor treatment by health personnel and discrimination while seeking care, it
would go as far as refusal of treatment (2014)
Page 66
66
Poorer women
Table 5.4 (WHO, UNICEF, UNFPA, World Bank Group, and United Nations Population Division Maternal Mortality
Estimation Inter-Agency Group, 2015)
Table 5.4 shows the improvements made in recent years to reduce casualties in
maternal health in Peru. The steep decrease since 1990 shows important advance, but
considering the data examined on the availability of healthcare facilities throughout
the country and the information on gaps between social groups in accessing maternal
health services, the matter of poor women and health had to be further investigated
through the lenses of access and engagement. According to the 2009 Amnesty
International report “Fatal Flaws: Barriers to Maternal Health in Peru”, Peru has one
of the highest rates of maternal mortality in the South American region and this
incidence mostly plagues the poorest women in rural areas or indigenous women.
Official figures show that between 185 and 240 women out of 100’000 die when
giving birth (Amnesty International, 2009). The reasons behind this serious issue
include lack in access or impossibility to communicate with health staff for
Indigenous women that do not speak Spanish. As we have seen earlier in this chapter,
there is still a divide between social groups when it comes to births assisted by health
workers, with the poorest sectors stopping at 60% compared to the nearly 100% of the
richest ones. Amnesty (2009) also reports that up until 2007 around 60% of
indigenous communities did not have access to health facilities. Moreover, although
the national government took steps such as better infrastructure and teaching
Page 67
67
indigenous languages to tackle these issues, they are not always implemented – for
example, health staff is still lacking the government-planned training and since 2000
waiting houses have increased, but not necessarily in rural areas, that need the most
(2009). At least until 2009, Amnesty found the government policies and initiatives to
be uncoordinated, lack of implementation and monitoring and no clear responsibility
or accountability.
Page 68
68
5.5 Chapter Conclusion This analysis started in examining the overall situation of Peru’s healthcare system. It
is a two-tier, underfunded system showing signs of improvement in certain areas (SIS
insurance service) but lacking in more local contexts. This is problematic for
vulnerable sectors of society, who may find difficulties in engaging with the system
or accessing it at all. Emergency response plans for health emergencies are in place,
but Peruvian infrastructure is not going to be able withstand the damages of a disaster,
as sub-chapter 5.2.2 showed. Data on cooperation with non-state health entities was
more difficult to find, but the initial interview, the description of the two-tier system
and reports by organizations provided interesting takes on the problems examined,
giving validation to the analysis in itself. The sub-questions were answered
thoroughly and the following table provides a summary of the findings on the
indicators. There are three labels on the table, they employed to understand the degree
of resilience for each indicator: ‘status weak’, ‘status sufficient’, ‘status strong’. The
indicators labelled as ‘weak’ show worrying data that require serious effort from the
government to solve issues that have the potential to be damaging to the population.
The label ‘sufficient’ instead shows a progressing situation in which there is still work
to be done but there are solid basis for resilience to operate. The label ‘strong’
signifies a good state of affairs for the indicator.
In the concluding chapter it will be possible to draw conclusions and make policy
recommendations.
Indicator Status weak Status
sufficient
Status strong Explanation
Adhesion to
International
Health
Regulations
X The country
adheres to
International
Health
Regulations
Equal Access to
healthcare
X There are
mechanisms in
place to access
Page 69
69
healthcare (SIS)
but not all
communities are
provided with
services or are
attended by
competent staff
Emergency
Response Plans
in Health
Emergencies
X Health-
Authority-
declared
emergency
warning system
implemented
Critical
infrastructure
protection and
“safe hospitals”
X Hospitals in the
country are not
safe but
improvements
are being put in
place, with hopes
for better
infrastructure
protection in the
next years
Cooperation
with non-state
healthcare
providers and
healthcare-
oriented NGOs
X There is a
presence of non-
state health
agencies
throughout the
territory
Page 70
70
Sustainability in
blood donations
X Blood donations
are scarce in the
country and
often hospitals
have to use
private and
possibly unsafe
blood banks
Citizens’
engagement in
healthcare
X Although data
shows important
improvements in
the last decade,
the most
vulnerable
sectors of society
are disengaged
and suffer the
most the
inefficiency of
Peru’s healthcare
system.
Page 71
71
6. Conclusion and Discussion In applying a set of concrete indicators in order to understand the degree of resilience
of the case at hand this study was able to explore the empirical field of resilience
research. Assessing the degree of resilience in Peru’s healthcare system proved useful
from both an academic and a social perspective, as it created a framework for analysis
through the formulation of indicators and also used it to find whether this component
of community resilience is able to withstand crisis and overall aid the population.
The concept of resilience is complex to define and presents different points of view
depending on the context in which it is used and who is using it. This thesis took into
account community resilience as a strategy to face crisis but went further into the
issue by finding what allows a community to be resilient and finally focused on the
matter of resilient healthcare. Resiliency in healthcare provision is a component of
community healthcare and it is a matter that is acquiring prominence in crisis
management but studying it presented difficulties as indicators are not as easy to find
as in subjects like food resilience, etc. Ad-hoc indicators were then developed to
proceed with a thorough research that could take into account both bottom-up and
top-down approaches to the concept while also making the study relevant from an
academic and social perspective.
6.1 To what extent is Peru’s healthcare system resilient and how can this
degree of resilience be explained?
This thesis fundamentally tested the resilience of Peru’s healthcare system by asking
to what extent it can support communities through crisis with resilience and why, and
found a series of data on the system that somewhat mirrored the socioeconomic
cleavages within the country. Developing countries can be reaching for the most
advanced solutions in certain areas (usually urban centers) and be still lacking the
most basic services in more rural and underdeveloped areas. Peru is in fact a
developing country that has improved greatly in the last decades under many aspects,
also in healthcare provision but the degree of resilience of the system is nonetheless
medium-low because while plans are being developed, funding is becoming less
scarce and while Peru adheres to international health regulations, bottom-up type of
indicators such as citizens’ engagement in healthcare, or availability of blood
donations, or access to healthcare throughout the territory prove that further
Page 72
72
improvements are needed urgently. The development of the SIS insurance system
covering the needs of citizens freely was a fundamental change that in time proved
helpful for many, but the substantial differences between healthcare provision in rural
areas and urban centers remains worrying. These could be affected deeply by disaster
but services would not be able to cater to the victims properly.
These problems undoubtedly originate in both funding scarcity and governance, but
the poverty levels varying from region to region also have an impact on the matter.
Data shows that even advanced solutions such as the universal health insurance
system have failed to attract personnel in areas with concentrations of vulnerable
communities therefore jeopardizing the health of groups such as pregnant women,
who may risk the worse consequences when giving birth. Elderly care is also lacking
attention in the country, with consistent disregard for older people and their health
problems, showing flaws in the medical approach to their conditions. Lack of funding
is also evident in the safety of infrastructure, which is scoring at the lowest levels on
the Hospital Safety Index. Without proper investment in infrastructure, hospitals and
health centers may not be able to support the ailing population in future crises and
also run the risk of collapsing, lowering communities’ chances of recovery and
‘bouncing back’ after an emergency. The problem regarding blood donations is
ultimately attributable to lack of good governance – the population must be made
aware of the issue and solutions must be found discourage blood-for-money donations
in which the lowest classes may partake to earn more but that are not as safe as
donations through public hospitals.
So, to what extent is Peru’s healthcare system resilient and how can this degree of
resilience be explained? Although it has started a long process of improvement, the
extent of resilience in Peru is not yet enough to withstand crisis, especially in the
Andean and rain forest areas where rural populations are often in poverty and suffer
immensely from lack of services. With very different indicators came very different
reasons why the degree of resilience of the system is medium-low. Overall - although
geographic peculiarities can pose physical obstacles to the improvement of conditions
- the problems present in the country’s healthcare system are due to a lack of
economic resources and a homogeneous spread of them throughout the territory. We
have seen poverty levels have improved in the past decades but they were not yet
satisfactory. It is with social investments from the government that communities can
be empowered and be fully resilient, that health facilities can provide the best care
Page 73
73
and crisis can be recovered and ‘bounced back’ from. If funding continues to increase
and central and regional governments expand their efforts to offer concrete health
coverage to the population, the situation will change for the better, as the data from
previous decades showed in this analysis.
6.2 Policy recommendations The following recommendations are offered to insure improvements for Peru’s
healthcare system. As noted in previous chapters, the country is still lacking in its
catering to citizens’ need. The degree of resilience encountered in studying the
country health system is medium to low because while there are areas in which the
government has improved its provision of healthcare services, others present worrying
data that impact on communities throughout the country, especially the ones with
lower incomes in rural areas.
• Infrastructure protection requires a vast investment by the Peruvian
government in order to make hospitals safe and score an A on the Hospitals
Safety Index. This has to be at the top of the agenda in order to insure resilient
healthcare to all.
• Maintenance of the SIS health coverage and strengthening of this service. It is
substantial for citizens to be offered universal health coverage and for the
government to implement measures to insure sustainability in the future and
make sure it will not fail due to lack of economic resources in the future.
Bureaucratic processes and service efficiency (e.g. waiting times) also need to
be simplified for the sake of citizens’ access. The service has proved to be
effective but it requires a serious effort by institutions to continue in providing
care.
• It is substantial to increase awareness on the importance of blood donations.
As Peru is in a particularly challenging situation when it comes to disaster, the
country must be able to sustain the request for blood – especially in times of
crisis. A maybe extreme but effective strategy would be to crack down on
money-for-blood systems that are under scrutinized and can seriously bring
damage to the health of blood receivers. This could be done while embarking
on a campaign to sensitise the public, especially in rural areas, to donate.
Involving communities in blood donation – which usually also consist in
Page 74
74
health checks for donors – could prove useful in engaging all sectors of
society in public healthcare and improve reliance in it.
• Granting access to healthcare also means giving all citizens equal opportunity
in reaching it. Rural communities in the Andean and rainforest areas must be
able to be attended to by competent staff within safe and available health
infrastructure. While the latter requires considerable investment by the
government, the former can be triggered with incentives for practitioners and
enhancing social mobility. Furthermore increasing the availability to study
medicine for citizens living in these areas could bring about a new generation
of carers returning to their regions after their studies and working with their
communities of origin.
• Vulnerable sectors of society such as low income and indigenous women and
older adults deserve better care. Poorer women have to be enabled access and
the policy steps taken by the government (Amnesty International, 2009) must
be put into practice and providers must be made accountable for them.
The older population is growing compared to previous decades and their
health issues may differ greatly from the ones of younger adults. It is
important to not overlook this sector of society and increasing attention to the
elderly by implementing courses for practitioners and simplifying access to
care for them.
6.3 Final remarks - Suggestions for further research and limitations of this
study This research was a long process of trial and error that required finding different
indicators for different aspects of healthcare in a developing country such as Peru.
Fortunately, the interview with Luigina Prosocco also provided insights for the
indicator on blood sustainability and confirmation for others, which was added
following her answering my sub-questions. The final indicators were very valuable in
showing interesting and useful data for the research and allowed in-depth analysis on
the national and local healthcare situation in Peru. They were also valuable because
they provided a point of view on both the top-down and bottom-up aspects of
healthcare. Further researchers could take on one of the indicators and analyse them
Page 75
75
on the field, as reliable data was initially difficult to find and required a long process.
Delving into the most technical aspects of healthcare resilience (e.g. critical
infrastructure protections) could be very interesting for enhancing capacity in the
system. On the other hand, studying local cases of access and citizens engagement
would also be interesting to further understand if and how a community is resilient
without a strong system available. Finally, research on the importance of traditional
medicine for poorer communities would also be of use to implement new methods of
engagement and care in the country.
The indicator “Critical infrastructure protection and ‘safe hospitals’” was the most
difficult to analyse due to shortage of data. Information is still very fragmented and it
was through the Peruvian national research institute (INEI) and PAHO and/or WHO
databases that most of the information was found. The indicator “Cooperation with
non-state healthcare providers and healthcare-oriented NGOs” proved to be not as
satisfactory as it was hoped, and if this thesis had to be rewritten or revisited, it would
definitely be incorporated. Nonetheless, it is an important indicator to understand a
two-tier healthcare system, therefore if possible it would be advisable to do research
on it – possibly in the field.
This research topic is surely vast and it would have been interesting to investigate it
further and on the field, going into Peruvian hospitals and understanding whether
there are more indicators to take into account and also looking into private healthcare
provision, especially traditional medicine which has a large following among
Peruvians. Nonetheless, the results discussed in the previous chapter were
constructive and the majority of the ad-hoc indicators could be taken into account in
future studies on resilience and healthcare.
Page 76
76
Bibliography
Journal Articles Adger, W. N., Brown, K., Nelson, D. R., Berkes, F., Eakin, H., Folke, C., Galvin, K.,
Gunderson, L., Goulden, M., O'Brien, K., Ruitenbeek, J. and Tompkins, E. L. (2011).
“Resilience implications of policy responses to climate change”, WIREs Climate
Change, Vol. 2, Issue 5, (September/October 2011), pp. 757–766.
Alcalde-Rabanal, J.E., Lazo-González, O., Nigenda, G. (2011). “Sistema de salud de
Perú”, Salud Pública de Mexico, Vol. 53, pp. S243-S254.
Aradau, C. (2014). “The promise of security: resilience, surprise and epistemic
politics”, Resilience: International Policies, Practices and Discourses, Vol. 2, Issue
2, pp. 73-87.
Baker, D., Refsgaard, K. (2007). “Institutional development and scale matching in
disaster response management”, Ecological Economics, Vol. 63, Issue 2-3, pp. 331–
43.
Berkes, F., (2007). “Understanding uncertainty and reducing vulnerability: Lessons
from resilience thinking. Natural Hazards, Vol. 41, Issue 2, pp. 283-295.
Biggs, D., Biggs, R., Dakos, V., Scholes, R. J. and M. Schoon, M. (2011). “Are we
entering an era of concatenated global crises?”, Ecology and Society, Vol. 16, Issue 2,
[online] Available at: http://www.ecologyandsociety.org/vol16/iss2/art27/ [Accessed
April 20th, 2016]
Arjen, B. (2004). “Lessons from Crisis research”, International Studies Review,
Vol.6, Issue 1, pp.165-194.
Boin, A. and McConnell, A. (2007). “Preparing for Critical Infrastructure
Breakdowns: The Limits of Crisis Management and the Need for Resilience”, Journal
of Contingencies and Crisis Management, Vol. 15 No.1, (March 2007), pp. 50-59.
Page 77
77
Boin, A., McConnell, A. and ‘t Hart, P. (2006). “Inertia or Change? Crisis-induced
Challenges for Political Leaders”, Refereed paper presented to the Australasian
Political Studies Association Conference, University of Newcastle 25–27 September
2006, [online] http://www.newcastle.edu.au [Accessed May 2nd, 2016]
Brown, D., & Kulig, J. (1996/97). “The concept of resiliency: Theoretical lessons
from community research”. Health and Canadian Society, Vol. 4, pp. 29–52.
Castleden, M., McKee1, M., Murray, V., Leonardi, G. (2011). “Resilience thinking in
health protection”, Journal of Public Health, Vol. 33, Issue 3, pp. 369–377.
Chen, S., Ferng, J., Wang, Y., Wu, T., Wang, J. (2008). “Assessment of disaster
resilience capacity of hillslope communities with high risk for geological hazards”,
Engineering Geology, Vol. 98, Issue 3-4, pp. 86–101.
Chhibber, A., Laajaj, R. (2008). “Disasters, climate change and economic
development in Sub-Saharan Africa: lessons and directions”, Journal of African
Economies, Vol. 17, Issue suppl. 2, pp. ii7–ii49.
Clarke, S. (1999). “Perceptions of organizational safety: implications for the
development of safety culture”, Journal of Organizational Behavior, Vol. 20, Issue 2,
(March 1999), pp. 185–198.
Cote, M., Nightingale, A. J. (2012). “Resilience Thinking Meets Social Theory
Situating Social Change in Socio-Ecological Systems (SES) Research”, Progress in
Human Geography, Vol. 36, Issue 4, pp. 475–489.
Cretney, R., Bond, S. (2014). “Bouncing back’ to capitalism? Grass-roots
autonomous activism in shaping discourses of resilience and transformation following
disaster”, Resilience: International Policies, Practices and Discourses, Vol. 2, Issue
1, pp. 18-31.
Cutter, S. L., Barnes, L., Berry, M., Burton, C., Evans, E. Tate, E., Webb, J. (2008).
“A place-based model for understanding community resilience to natural disasters”,
Page 78
78
Global Environmental Change, Vol. 18, Issue 4, pp. 598-606.
Evans, B. Reid, J. (2013). “Dangerously exposed: the life and death of the resilient
subject”, Resilience: International Policies, Practices and Discourses, Vol. 1, Issue 2,
pp. 83-98.
Folke, C. (2006). “Resilience: the emergence of a perspective for social-ecological
systems analyses”, Global Environmental Change, Vol. 16, pp. 253-67.
Furedi, F. (2008). “Fear And Security: A Vulnerability-Led Policy Response”, Social
Policy & Administration, Vol. 42, Issue 6, (December 2008), pp. 645–661.
Fundter, D., Jonkman, B., Beerman, S., Goemans, C. L., Briggs, R., Coumans, F.,
Lahaye, J. W., Bierens, J. (2008). “Health impacts of large-scale floods: governmental
decision-making and resilience of the citizens”, Prehospital and Disaster Medicine,
Vol. 23, pp. 70–3.
Gilbert, M. (2008). “Bridging the gap: building local resilience and competencies in
remote communities”, Prehospital and Disaster Medicine, Vol. 23, pp. 297–300.
Gordon N. H., Crowe J. P., Brumberg D. J., Berger N. A. (1992). “Socioeconomic
factors and race in breast cancer recurrence and survival”, American Journal of
Epidemiology, Vol. 135, Issue 6, pp. 609-618.
Holling, C. S. (1973). “Resilience and Stability of Ecological Systems,” Annual
Review of Ecology and Systematics, Vol. 4, pp. 1–23.
Hunter, C. (2012). Is resilience still a useful concept when working with children and
young people? (CFCA Paper 2). Melbourne: Australian Institute of Family Studies.
Keim, M. (2008). “Building Human Resilience. The Role of Public Health
Preparedness and Response As an Adaptation to Climate Change”, American Journal
of Preventive Medicine 2008, Vol. 35, Issue 5, pp. 508–516.
Kimhi, S., Shamai, M. (2004). “Community resilience and the impact of stress: adult
response to Israel’s withdrawal from Lebanon”. Journal of Community Psychology,
Vol. 32, Issue 4, pp. 439-451.
Page 79
79
Kulig, J. C., Edge, D. S., Joyce, B. (2008). “Understanding Community Resiliency in
Rural Communities Through Multimethod Research”, Journal of Rural and
Community Development, Vol. 3, Issue 3.
Jeffcott, S. A., Ibrahim, J. E., Cameron P. A. (2009). “Resilience in healthcare and
clinical handover”, Quality and Safety in Health Care, Vol. 18, Issue 4, (August
2009), pp. 256-260.
Joseph, J. (2013). “Resilience as Embedded Neoliberalism: A Governmentality
Approach”, Resilience: International Policies, Practices and Discourses, Vol. 1,
Issue 1, pp. 38–52.
Lebel, L., Anderies, J. M., Campbell, B., Folke, C., Hatfield-Dodds, S., Hughes T. P.,
Wilson, J. (2006). “Governance and the capacity to manage resilience in regional
social-ecological systems”, Ecology and Society, Vol. 11, Issue 1, pp. 1-21.
Lee, E.K.O., Shen, C., Tran, T. V. (2009). “Coping with Hurricane Katrina:
psychological distress and resilience among African Americans evacuees”, Journal of
Black Psychology, Vol. 35, Issue 1, pp. 5-23.
Luthar, S. S., Cicchetti, D. (2000). “The construct of resilience: Implications for
interventions and social policies”, Development and Psychopathology, Vol. 12, Issue
4, pp. 857-885.
MacKinnon, D., Derickson, K. D. (2012). “From Resilience to Resourcefulness: A
Critique of Resilience Policy and Activism”, Progress in Human Geography, Vol. 37,
Issue 2, (August 2012), pp. 253–270.
Magis, K. (2010). “Community Resilience: An Indicator of Social Sustainability”,
Society & Natural Resources, Vol. 23, Issue 5, pp. 401–416.
Maguire, B., Hagan, P. (2007). “Disasters and communities:
understanding social resilience”, The Australian Journal of Emergency Management,
Vol. 22, Issue 2, (May 2007), pp. 16-20.
Page 80
80
Masten, A.S. (2001). “Ordinary magic: Resilience processes in development”,
American Psychologist, Vol. 56, Issue 3, pp. 227-238.
Meadowcroft, J. (1997). “Planning for sustainable development: insights from the
literatures of political science”. European Journal of Political Research, Vol. 31,
Issue 4, pp. 427-454.
Montinaro, F., Busby, G. B. J., Pascali, V. L., Myers, S., Hellenthal, G., Capelli, C.
(2015). “Unravelling the hidden ancestry of American admixed populations”, Nature
Communications, Vol. 6, (March 2015).
Moser, S., Ekstrom, J. A., (2010). “A framework to diagnose barriers to climate
change adaptation”, Proceedings of the National Academy of Sciences, Vol. 107,
Issue 51, pp. 22026-22031.
Moss, R.H., Edmonds, J. A., Hibbard, K. A., Manning, M. R., Rose, S.K. , van
Vuuren, D.P. , Carter, T.R., Emori, S., Kainuma, M., Kram, T., Meehl, G.A.,
Mitchell, J.F.B., Nakicenovic, N., Riahi, K., Smith, S. J., Stouffer, R. J., Thomson, A.
M., Weyant, J. P., Wilbanks, T. J. (2010). “A new paradigm for the next generation of
climate change scenarios”, Nature, Vol. 463, pp. 747-756.
Mustard, C. A., Derkson, S., Berthelot, M., Wolfson, M., Roos, L.L. (1997). “Age-
specific education and income gradients in morbidity and mortality in a Canadian
province”, Social Science and Medicine, Vol. 45, Issue 3, pp. 383-397.
Nelson, D.R., Adger, W.N., Brown, K. (2007). “Adaptation to environmental change:
contributions of a resilience framework”, Annual Review of Environment and
Resources, Vol. 32, pp. 395-419.
O’Brien, K. L., Eriksen, S., Sygna, L., Næss, L.O. (2006). “Questioning
complacency: climate change impacts, vulnerability, and adaptation in Norway”,
Ambio, Vol. 35, Issue 2, pp. 50-56.
Page 81
81
Obrist, B., Pfeiffer, C., R. Henley, R. (2010). “Multi-layered social resilience: a new
approach in mitigation research”, Progress in Development Studies, Vol. 10, Issue 4,
pp. 283-293.
Owen, T. (2004), "Challenges and opportunities for defining and measuring human
security", Human Rights, Human Security and Disarmament, Disarmament Forum,
Issue 2, (June 2004).
Price-Robertson, R., Knight, K. (2012). “Natural disasters and community resilience:
A framework for support”, CFCA Paper, Issue 3, Melbourne: Australian Institute of
Family Studies.
Reid, J. (2012). “The Disastrous and Politically Debased Subject of Resilience”,
Development dialogue, Vol. 58, (April 2012), pp. 67-80.
Richardson, G.E., Neiger, B.L., Jensen, S., Kumpfer, K.L. (1990). “The resiliency
model”, Health Education, Vol. 21, Issue 6, pp. 33-39.
Rios, J. F., Zavala, C. A. (2008). Impact Of The Pisco-Peru Earthquake Of August
15th 2007 On Health Facilities. In: WCEE (World Conference for Earthquake
Engineering), 14th World Conference. Beijing, China, 12-17 October 2008.
Rose, A. (2004). Defining and measuring economic resilience to disasters. Disaster
Prevention and Management, 13, 307–314.
Salagnac, J. (2007). “Lessons from the 2003 heat wave: a French perspective”,
Building Research and Information, Vol. 35, Issue 4, pp. 450-457.
Seccombe, K. (2002). “Beating the Odds” Versus “Changing the Odds”: Poverty,
Resilience, and Family Policy” , Journal of Marriage and Family, Vol. 64, Issue 2,
(May 2002), pp. 384-394.
Shobha S. L. R., O’Fallon M. A., Dearry A. (2003). “Creating healthy communities,
healthy homes, healthy people: initiating a research agenda on the built
Page 82
82
environment and public health”, American Journal of Public Health, Vol. 93, pp.
1446–50.
Simmie, J., Martin, R. (2010). “The economic resilience of regions: towards an
evolutionary approach”, Economy and Society, Vol. 3, Issue 1, pp. 27-43.
Swart, R., Robinson, J. Cohen, S. (2003). “Climate change and sustainable
development: expanding the options”, Climate Policy, Vol. 3, Suppl. 1, (November
2003), pp. S19–S40.
‘t Hart, P. (1993). “Symbols, Rituals and Power: The Lost Dimension in Crisis
Management”, Journal of Contingencies and Crisis Management, Vol. 1, Issue 1, pp.
36–50.
‘t Hart, P., Rosenthal, U., Kouzmin, A. (1993). “Crisis Decision Making: The
Centralization Thesis Revisited”, Administration and Society, Vol. 25, Issue 1, pp.
12–45.
Walker, B., Carpenter, S., Anderies, J., Abel, N., Cumming, G. S., Janssen, M., Lebel,
L., Norberg, J., Peterson, G.D., Pritchard, R. (2002). “Resilience management in
social-ecological systems: a working hypothesis for a participatory approach”,
Conservation Ecology, Vol. 6, Issue 1, Art. 14.
Walker, B., Holling, C. S., Carpenter, S. R., Kinzig., A. (2004). “Resilience,
adaptability and transformability in social–ecological systems”, Ecology and Society,
Vol. 9, Issue 2, Art. 5.
Walker, J., Cooper, M. (2011). “Genealogies of Resilience: From Systems Ecology to
the Political Economy of Crisis Adaptation”, Security Dialogue, Vol. 42, Issue 2, pp.
143–60.
Wilbanks, T.J. (1994). “’Sustainable development’ in geographic context”, Annals of
the Association of American Geographers, Vol. 84, Issue 4, pp. 541-557.
Page 83
83
Wilbanks, T., Kates, R. (2010). “Beyond adapting to climate change: embedding
adaptation in responses to multiple threats and stresses”, Annals of the Association of
American Geographers, Vol. 100, Issue 4, pp. 719-728.
Wilson, L.,Velásquez, A., Ponce, C. (2009). “La Ley Marco de Aseguramiento
Universal en Salud en el Perú: análisis de beneficios y sistematización del proceso
desde su concepción hasta su promulgación”, Salud Pública di Mexico, Vol. 53,
Suppl. 2, pp. 207-217.
Books and Book chapters
Barton, A.H. (1969). Communities in Disaster: A Sociological Analysis of Collective
Stress Situations. New York: Doubleday.
Baumgartner, F.R., Jones, B.D. (1993). Agendas and Instability in American Politics.
Chicago: University of Chicago Press.
Birkland, T.A. (1997). After Disaster: Agenda Setting, Public Policy, and Focusing
Events. Washington DC: Georgetown University Press.
Boin, R.A. (2005), “From Crisis to Disaster: Toward an Integrative Perspective”. In
Perry, R., Quarantelli, E.L., ed. (2005). What is a Disaster? New Answers to Old
Questions. Philadelphia: Xlibris Press, pp. 153–172.
Boin, A., Comfort, L. K., Demchak, C. C. (2010). Designing Resilience: Preparing
for Extreme Events. Pittsburgh: University Press.
Buzan, B., de Wilde, J. and Wæver, O. (1997). Security: A New Framework for
Analysis. Boulder (Colorado): Lynne Rienner Publishers Inc.
Clarke, L. (1999). Mission Improbable: Using Fantasy Documents to Tame Disaster.
Chicago: University of Chicago Press.
Page 84
84
Drabek, T.E. (1986). Human System Responses to Disaster: An Inventory of
Sociological Findings. New York: Springer
Ford, J.D., Ford L.B., ed. (2011). Climate Change Adaptation in Developed Nations:
From Theory to Practice. Dordrecht, The Netherlands: Springer.
Foucault, M. (quoted in Rabinow, P.) (2003). Anthropos Today. Reflections on
Modern Equipment, Princeton, NJ: Princeton University Press.
Goode, W. J., Hatt, P. K. (1952). Methods in Social Research. New York: McGraw-
Hill.
Gordon, E.W., Song, L.D. (1994). “Variations in the experience of resilience”. In
M.C. Wang & E.W. Gordon (Eds.). Educational resilience in inner-city America:
Challenges and prospects. Hillsdale, NJ: Lawrence Erlbaum Associates, pp. 27-43
Higgins, G.O. (1994). Resilient adults: Overcoming a cruel past. San Francisco, CA:
Jossey-Bass.
Kendra, J., Wachtendorf, T. (2002). Elements of resilience in the World Trade
Center attack, Preliminary report published by the Disaster Research Center,
Newark, DE: University of Delaware.
Kulig, J., Hanson, L. (1996). Discussion and expansion of the concept of resiliency:
summary of a think tank. Lethbridge, AB: University of Lethbridge, Regional Centre
for Health Promotion & Community Studies.
Kumar, R. (1996). Research Methodology. A step-by-step guide for beginners.
Australia: Addison Wesley Longman.
Joseph, J. (1994). The Resilient Child. New York, NY: Insight Books.
Longstaff, P.H. (2005). Security, Resilience and Communication in Unpredictable
Environments such as Terrorism, Natural Disasters and Complex Technology.
Harvard University: Program on Information Resources Policy, Center for
Information Policy Research.
Page 85
85
McAslan, A. (2010). Resilience: Understanding it origins, meaning and utility.
Adelaide: Torrens Resilience Institute.
McAslan, A. (2011). Community resilience: Understanding the concept and its
application. Adelaide: Torrens Resilience Institute.
Maguire, B., Cartwright, S. (2008). Assessing a community's capacity to manage
change: A resilience approach to social assessment. Canberra: Bureau of Rural
Sciences.
Mendes J, Tavares, A. (2009). “Building resilience to natural hazards. Practices and
policies on governance and mitigation in the central region of Portugal”. In Martorell,
S., Soares, C. G., Barnett, J., ed. (2009). Safety, Reliability and Risk Analysis: Theory,
Methods and Applications. London: Taylor and Francis.
Norris, F. (2010). Behavioral Science Perspectives on Resilience. CARRI Research
Paper 10. Oak Ridge, TN: Community and Regional Resilience Institute.
Parry, M. L., Canziani, O. F., Palutikof, J. P. (2007). “Technical summary”. In Parry,
M.L., Canziani, O.F., Palutikof, J.P., van der Linden, P. J., Hanson, C. E., ed. (2007).
Climate Change 2007: Impacts, Adaptation and Vulnerability. Contribution of
Working Group II to the Fourth Assessment Report of the Intergovernmental Panel on
Climate Change. Cambridge: University Press, , pp. 23-78.
Pfefferbaum, B., Reissman, D., Pfefferbaum, R., Klomp, R., Gurwitch, R. (2005).
“Building resilience to mass trauma events”. In Doll, L., Bonzo, S., Mercy, J., Sleet,
D. ed. (2005). Handbook on injury and violence prevention interventions. New York:
Kluwer Academic Publishers.
Posner, R.A. (2004). Catastrophe: Risk and Response. Oxford: University Press.
Page 86
86
Rigsby, L. (1994). “The Americanization of resilience. Deconstructing research
practice”. In Wang, M., Gordon, E., ed. (1994). Educational resilience in inner-city
America. Hillsdale, NJ: Lawrence Erlbaum, pp. 85-94.
Rosemary, T., Bertram, G. (1978). Peru 1890–1977: growth and policy in an open
economy. New York: Columbia University Press.
Rosenthal, U., Boin, A., Comfort, L. K., ed. (2001). Managing Crises: Threats,
Dilemmas, Opportunities. Springfield, IL: Charles C. Thomas.
Swanborn, P. (2010). Case Study Research: What, Why and How? London: Sage.
‘t Hart, P., Boin, A. (2001). “Between Crisis And Normalcy: The Long Shadow of
Post- Crisis Politics”. In Rosenthal, U., Boin, A., Comfort, L. K., ed. (2001)
Managing Crises: Threats, Dilemmas, Opportunities. Springfield, IL: Charles C.
Thomas.
Tanner, T., Mitchell, T., Polack, E., Guenther, B. (2009). Urban governance for
adaptation: Assessing climate change resilience in ten Asian cities (IDS Working
Paper 315). Brighton: Institute of Development Studies, University of Sussex.
Toulmin, C. (2009). Building Resilience for an Interdependent World: Why the
Environment Matters and What DFID Should Do About It. London: IIED.
Webster (1958). Webster’s New Twentieth Century Dictionary of English Language.
Boston, US: Houghton Mifflin Harcourt
Government and Organizations’ Documents, Reports Amnesty International, (2009). Peru: Fatal Flaws - Barriers To Maternal Health In
Peru. London: Amnesty International Publications. [PDF] Available at
https://www.amnesty.org/en/documents/AMR46/008/2009/en/ [Accessed July 23rd,
2016]
Page 87
87
Cetrángolo, O., Bertranou, F., Casanova, L., Casalí, P. (2013). El sistema de salud del
Perú: situación actual y estrategias para orientar la extensión de la cobertura
contribu va. Lima: OIT/Oficina de la OIT para los Países Andinos.
Christoplos, I., Novaky, M., Aysan, Y. (2012). Resilience, Risk and Vulnerability at
Sida - Final Report. Stockholm, Sweden: swedish International Development
Cooperation Agency. [PDF] Available at
http://www.sida.se/contentassets/5de4b5ba77044012af09ba3eb53f3a5f/resilience-
risk-and-vulnerability-at-sida---final-report_3406.pdf [Accessed August 19th, 2016]
European Union (2014). Communication From The Commission On effective,
Accessible and Resilient Health Systems. Brussels, Belgium: European Commission.
[PDF] Available at
http://ec.europa.eu/health/healthcare/docs/com2014_215_final_en.pdf [Accessed July
20th, 2016]
International Federation of Red Cross and Red Crescent Societies (IFRC), (2014).
IFRC Framework for Community Resilience. Geneva: International Federation of Red
Cross and Red Crescent Societies. [PDF] Available at
http://www.ifrc.org/Global/Documents/Secretariat/201501/1284000-
Framework%20for%20Community%20Resilience-EN-LR.pdf [Accessed July 12th,
2016]
Intergovernmental Panel on Climate Change (IPCC), (2007). In Pachauri, R. K.
Reisinger, A., ed. (2007). Climate change 2007: synthesis report. Contribution of
Working Groups I, II and III to the Fourth Assessment Report of the
Intergovernmental Panel on Climate Change. Geneva, Switzerland: IPCC.
Intergovernmental Panel on Climate Change (IPCC), (2012). In Field, C. B., Dokken,
D. J., Plattner, G., Barros, V., Ebi, K. L., Allen, S. K., Stocker, T. F., Mastrandrea, M.
D., Tignor, M., Dahe, Q., Mach, K. J., Midgley, P. M., ed. (2012). Managing the
Risks of Extreme Events and Disasters to Advance Climate Change Adaptation.
Page 88
88
Special Report of the Intergovernmental Panel on Climate Change. Cambridge:
University Press.
Millennium Ecosystem Assessment (MEA). (2005). Ecosystems and human well-
being: synthesis. Washington, D.C.: Island Press.
Ministerio de Salud de Peru (MINSA), (2010). Dona Sangre, ¡Salva Vidas! –
Situación Actual. [online] Available at
http://www.minsa.gob.pe/portada/Especiales/2010/donasangre/?op=3 [Accessed
August 6th, 2016]
Ministerio de Salud de Peru (MINSA), (2011). Recursos Humanos En Salud Al 2011
Evidencias para la toma de decisiones. Lima, Peru: Dirección General de Ges ón del
Desarrollo de Recursos Humanos. [PDF] Available at
http://www.bvsde.paho.org/texcom/cd046043/serieRHUS14.pdf [Accessed July 20th,
2016]
Ministerio de Salud de Peru/Seguro Integral de Salud (MINSA/SIS), (2016). Al
cumplir 14 años de creación, el Seguro Integral de Salud garantiza la salud del 53%
de los peruanos. Lima, Peru: Oficina General de Imagen Institucional y
Transparencia. [online] Available at
http://www.sis.gob.pe/Nuevo/vistas/Frm_NotaPrensa.aspx?np=120 [Accessed July
30th, 2016]
National Emergency Management Committee, (2009). National Strategy for Disaster
Resilience: Building our nation's resilience to disasters. Canberra: COAG.
National Research Council (NRC), 1999. Our Common Journey: A Transition
Towards Sustainability. Washington, D.C.: National Research Council, National
Academies Press.
Pan American Health Organization (PAHO)a. Hospital Safety Index. What Is the
Hospital Safety Index? [online] Available at
Page 89
89
http://www.paho.org/disasters/index.php?option=com_content&view=category&layo
ut=blog&id=907&Itemid=884&lang=en [Accessed July 29th, 2016]
Pan American Health Organization (PAHO) (2000). Principles of Disaster Mitigation
in Health Facilities. Washington D. C.: Emergency Preparedness and Disaster Relief
Coordination Program Pan American Health Organization Regional Office of the
World Health Organization. [PDF] Available at http://www.disaster-
info.net/safehospitals_refdocs/documents/english/PrinciplesOfDisasterMitig.pdf
[Accessed July 26th, 2016]
Pan American Health Organization (PAHO) (2008). Provisional Agenda Item 4.13
CE142/20. Blood Transfusion Safety: Progress Report. Washington D. C.: Pan
American Health Organization. [PDF] Available at
http://www1.paho.org/english/gov/ce/ce142-20-e.pdf [Accessed August 2nd, 2016]
Pan American Health Organization (PAHO) (2016). Peru Updates its National Policy
on Safe Hospitals. [online] Available at
http://www.paho.org/disasters/newsletter/index.php?option=com_content&view=artic
le&id=539%3Aperu-updates-its-national-policy-on-safe-
hospitals&catid=257%3Aissue-121-june-2016-member-
countries&Itemid=349&lang=en [Accessed July 26th, 2016]
United Nations Environment Programme (UNEP) (2004), Exploring the Links:
Human Well-Being, Poverty and Ecosystem Services. Nairobi: UN Publications.
United Nations International Strategy for Disaster Risk Reduction (UNISDR), (2005).
Hyogo Framework for Action 2005–2015: Building the resilience of nations and
communities to disasters. United Nations International Strategy for
Disaster Reduction, Geneva, Switzerland.
United Nations Office for Disaster Risk Reduction (UNISDR), (2009). Making the
Case for Hospitals Safe From Disasters. [PDF] Available at
Page 90
90
https://www.unisdr.org/2009/campaign/pdf/wdrc-2007-2008-making-the-case.pdf
[Accessed July 19th, 2016]
World Federation of Public Health Associations (WFPHA) (1978). Non-
Governmental Organizations and Primary Health Care.Position Paper – Passed by
the WFPHA General Assembly – 1978. [PDF] Available at
http://www.wfpha.org/tl_files/doc/resolutions/positionpapers/global/NGO&PrimaryH
ealthCare.pdf [Accessed July 19th, 2016]
World Health Organization (WHO) (2005). International Health Regulations.
Geneva, Switzerland: World Health Organization. Available at
http://apps.who.int/iris/bitstream/10665/246107/1/9789241580496-eng.pdf?ua=1
[Accessed July 1st, 2016]
World Health Organization (WHO) (2013). Work Force Alliance – Country Case
Studies: Annex 12 Peru. [PDF] Available at
http://www.who.int/workforcealliance/knowledge/resources/MLHWCountryCaseStud
ies_annex12_Peru.pdf?ua=1 [Accessed July 21st, 2016]
World Health Organization (WHO)a. Emergency Response Framework. Geneva,
Switzerland: World Health Organization. [PDF] Available at
http://www.who.int/hac/about/erf_.pdf [Accessed July 13th, 2016]
World Health Organization (WHO)b. Global Health Workforce Alliance – Peru.
[online] Available at http://www.who.int/workforcealliance/countries/per/en/
[Accessed July 21st, 2016]
World Health Organization (WHO), The United Nations Children's Emergency Fund
(UNICEF), United Nations Fund for Population Activities (UNFPA), World Bank
Group, United Nations Population Division Maternal Mortality Estimation Inter-
Agency Group (2015). Maternal mortality in 1990-2015. [PDF] Available at
http://www.who.int/gho/maternal_health/countries/per.pdf?ua=1 [Accessed August
1st, 2016]
Page 91
91
World Resources Institute (WRI), United Nations Development Programme (UNDP),
United Nations Environment Programme (UNEP), World Bank (2008). World
Resources 2008: Roots of Resilience—Growing the Wealth of the Poor. Washington:
World Resources Institute. [PDF] Available at
https://www.wri.org/sites/default/files/pdf/world_resources_2008_roots_of_resilience
_front.pdf [Accessed May 4th, 2016]
WRI; UNDP; UNEP; World Bank (2008). World Resources 2008: Roots of
Resilience—Growing the Wealth of the Poor. Washington: World Resources Institute,
262 http://www.wri.org/publication/world-resources-2008- roots-of-resilience
Laws and Bills Ley Orgánica de Gobiernos Regionales N° 27867 (Article N° 11). Lima, Peru.
Ley Orgánica de Gobiernos Regionales N° 27867, (Article N° 10). Lima, Peru.
Ley Orgánica de Gobiernos Regionales, N° 27867 (Article N° 66). Lima, Peru.
Ministerio de Salud de Peru (MINSA), (2004). Resolución Ministerial No. 517-
2004/MINSA. [PDF] Available at
http://www.minsa.gob.pe/ogdn/cd1/pdf/NLS_15/resolucion.pdf [Accessed August
1st, 2016]
Datasets Instituto Nacional de Estadística e Informática (INEI). Población en situación de
pobreza, según ámbitos geográficos. [online] Available at
https://www.inei.gob.pe/estadisticas/indice-tematico/sociales/ [Accessed July 30th,
2016]
Page 92
92
Instituto Nacional de Estadística e Informática (INEI). Población en situación de
pobreza, según ámbitos geográficos. [online] Available at
https://www.inei.gob.pe/estadisticas/indice-tematico/sociales/ [Accessed July 30th,
2016]
Instituto Nacional de Estadística e Informática (INEI). Población en situación de
pobreza extrema, ámbitos geográficos. [online] Available at
https://www.inei.gob.pe/estadisticas/indice-tematico/sociales/ [Accessed July 30th,
2016]
Instituto Nacional de Estadística e Informática (INEI). Número de habitantes por
cada médico, según departamento. [online] Available at
https://www.inei.gob.pe/estadisticas/indice-tematico/sociales/ [Accessed July 30th,
2016]
Instituto Nacional de Estadística e Informática (INEI). Número de habitantes por
cada enfermera(os) por cada habitante, según departamento. [online] Available at
https://www.inei.gob.pe/estadisticas/indice-tematico/sociales/ [Accessed July 30th,
2016]
Instituto Nacional de Estadística e Informática (INEI) (2008). Perfil
sociodemográfico del Perú. Lima: INEI, 2008. [PDF] Available at
https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1136/l
ibro.pdf [Accessed July 22nd, 2016]
Instituto Nacional de Estadística e Informática (INEI) (2010) Evolución de la Pobreza
en el Perú al 2010. Lima, Peru: INEI. [PDF] Available at
http://siteresources.worldbank.org/INTPERUINSPANISH/Resources/Presentacion_R
esultados_POBREZA_2010_18_Mayo_2011.pdf [Accessed July 22nd, 2016]
Instituto Nacional de Estadística e Informática (INEI) (2013). Encuesta Demográfica
y de Salud Familiar 2013 – Resumen Ejecutivo. Lima, Peru: INEI. [PDF] Available at
Page 93
93
https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1151/
pdf/Resumenejecutivo.pdf [Accessed July 22nd, 2016]
PAHOb. Health Intelligence Platform
http://phip.paho.org/views/PerfilesPais2014/CoberturaySaniamiento?:iid=1?:embed%
3Dyes&:embed=yes&:comments=n&:display_count=no&:showVizHome=no
World Health Organization (WHO) (2015). Peru: WHO statistical profile. [PDF]
Available at http://www.who.int/gho/countries/per.pdf [Accessed July 31st, 2016]
World Health Organization (WHO)c. Peru. [PDF] Available at
http://www.who.int/workforcealliance/countries/Peru_En.pdf?ua=1 [Accessed July
21st, 2016]
World Health Organization (WHO)d. Global Health Observatory (GHO) data. Peru:
Country Profiles. [online] Available at
http://www.who.int/gho/countries/per/country_profiles/en/ [Accessed July 31st, 2016]
Websites BBC, (2012). Peru Country Profile. BBC. [online] Available at
http://news.bbc.co.uk/2/hi/americas/country_profiles/1224656.stm [Accessed May
5th, 2016]
Chase, R. (2014). Peru needs more blood donors. Peru This Week. [online] Available
at http://www.peruthisweek.com/news-peru-needs-more-blood-donors-103088
[Accessed July 15th, 2016]
Ferng, M. (2014). Peru: Health System Unresponsive to Aging Population. Pulitzer
Center. [online] Available at http://pulitzercenter.org/reporting/south-america-peru-
health-care-elderly [Accessed July 29th, 2016]
Gestión, (2013). INEI: Pobreza se reduce a 25.8% en Perú y 509 mil personas dejaron
de ser pobres en 2012. Gestión. [online] Available at http://gestion.pe/economia/inei-
Page 94
94
pobreza-se-reduce-258-peru-y-509-mil-personas-dejaron-pobres-2012-2065578
[Accessed August 1st, 2016]
La República, (2016). ¿El SIS, el seguro que podría cambiar el sector salud en Perú?
La República. [online] Available at http://larepublica.pe/sociedad/785789-el-sis-el-
seguro-que-podria-cambiar-el-sector-salud-en-peru [Accessed August 3rd, 2016]
Lilla, M. (2007). Mr. Casaubon in America. The New York Review of Books. [online]
Available at http://www.nybooks.com/articles/2007/06/28/mr-casaubon-in-america/
[Accessed April 15th, 2016]
Málaga, I. (2012). En el 2012 solo se ejecutó el 39,6% del presupuesto social
destinado a salud. El Comercio. [online] Available at
http://elcomercio.pe/economia/peru/2012-solo-se-ejecuto-396-presupuesto-social-
destinado-salud_1-noticia-1514660 [Accessed July 16th, 2016]
Preventionweb.net (2011). Peru sets an example for safe hospitals.
Preventionweb.net. [online] Available at
http://www.preventionweb.net/news/view/20780 [Accessed July 28th, 2016]
UNDPLAC, (2015). Improving Resilience in Peru. Women empowerment and
climate change adaptation in the hills of Lima. [online] Available at
https://undplac.exposure.co/improving-resilience-in-peru [Accessed August 19th,
2016]
Page 95
95
Maps Goperu.com. Vegetation Map of Peru. [online] Available at
http://goperu.about.com/od/planningandpacking/ss/Maps-Of-Peru.htm#step4
[Accessed August 10th, 2016]
Mapsof.net. Map of Peru’s regions and departments. [online] Available at
http://mapsof.net/peru/peru-regions-and-departments [Accessed July 26th, 2016]