38
2017 AJAS Annual Conference MASTERClass

2017 AJAS Annual Conference
MASTERClass

AJAS Master Class
Innovations in Jewish End-of-Life Care
End-of-Life Care for Jewish Community
Should be informed by and incorporate the following:
• Cultural norms in Jewish community
• Jewish vs. Western medical ethics
• Endorsement by Religious and Lay community
• Jewish providers, liaisons and navigators
• Jewish clinical team members
• Cultural sensitivity training
• Incorporation of Halachic Pathway
Barriers/Challenges to Access
• Hospice ‘philosophy’
• Lack of awareness of Jewish laws and customs
• Exclusion of appropriate stakeholders in decision
making
• Jewish Values and Jewish Medical Ethics
• Cultural norms around seeking aggressive medical care
• Cultural norms around advance care planning
• Loss of hope, hastening death
Recommendations Leading to Best Practice
• Community based model – multi-pronged approach
• Lay, religious, healthcare leadership
• Education/outreach – professional, community
• Synagogue involvement
• Funding support
• Governance/Leadership support
• Infrastructure – human resources
• Value neutral staff
• Marketing
• Communication, communication, communication

AJAS MasterclassInnovations in Jewish End-of-Life Care

Education
•Professionals
•Community
•Synagogue
7
Center for Jewish End of Life Care
History
Lessons learned
•Focus Groups
•Snackable
•Changeable
8
To Operate or Not to Operate Hospice?Sivitz Jewish Hospice
Jewish Association on AgingPittsburgh, PA
AJAS MasterClass: Innovations in Jewish Palliative & End of Life Care
April 5, 2017Deborah Winn-Horvitz
Mary Anne Foley
Objectives
1. Understand how to include Board and Community Leaders in discussions related to a mission critical program
2. Learn how one hospice program redesigned for financial success
3. Understand ways to differentiate your program in a crowded market
10
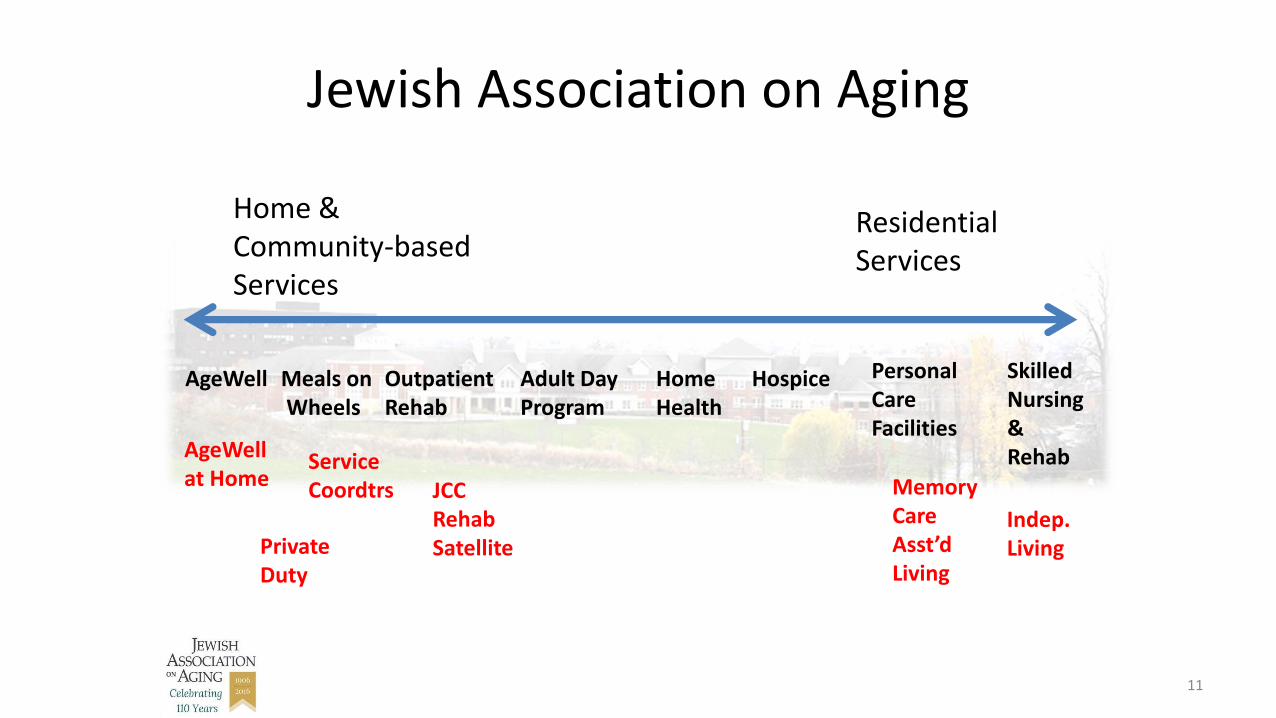
Jewish Association on Aging
Home & Community-based Services
Residential Services
Meals onWheels
Outpatient Rehab
Adult DayProgram
Home Health
Hospice Personal Care Facilities
Skilled Nursing & Rehab
AgeWell
AgeWellat Home
Service Coordtrs
Private Duty
JCC Rehab Satellite
Memory Care Asst’dLiving
Indep. Living
11
History of Sivitz Jewish Hospice
• Developed and opened 20 years ago, by the Sivitz Family
• Historically a financially stable program
– Strong census despite competition
– Overall quality excellent
12
Regulatory Changes Impacting Hospice Providers
• January 2011: Face to Face Ruling went into effect
• October 2012: Medicare Hospice Claims with increased scrutiny• LOS: Routine & GIP• LTC/SNF: Debility• LOS: Alzheimer’s, Debility or COPD
• October 2013: Final ruling: Debility and Adult Failure to Thrive
• July 2013: First Mandatory reporting requirements
• March 2014: Hospice and Medication Part D
• July 2014: First penalties imposed on reimbursement
13
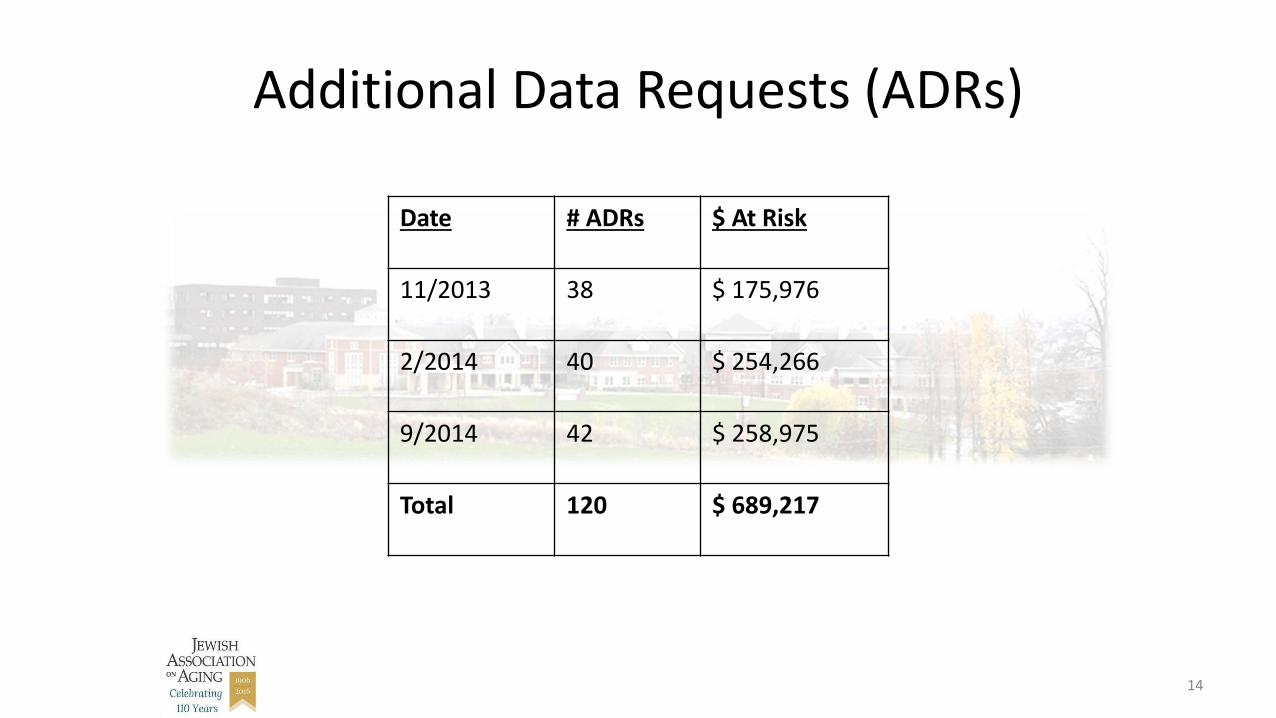
Additional Data Requests (ADRs)
Date # ADRs $ At Risk
11/2013 38 $ 175,976
2/2014 40 $ 254,266
9/2014 42 $ 258,975
Total 120 $ 689,217
14
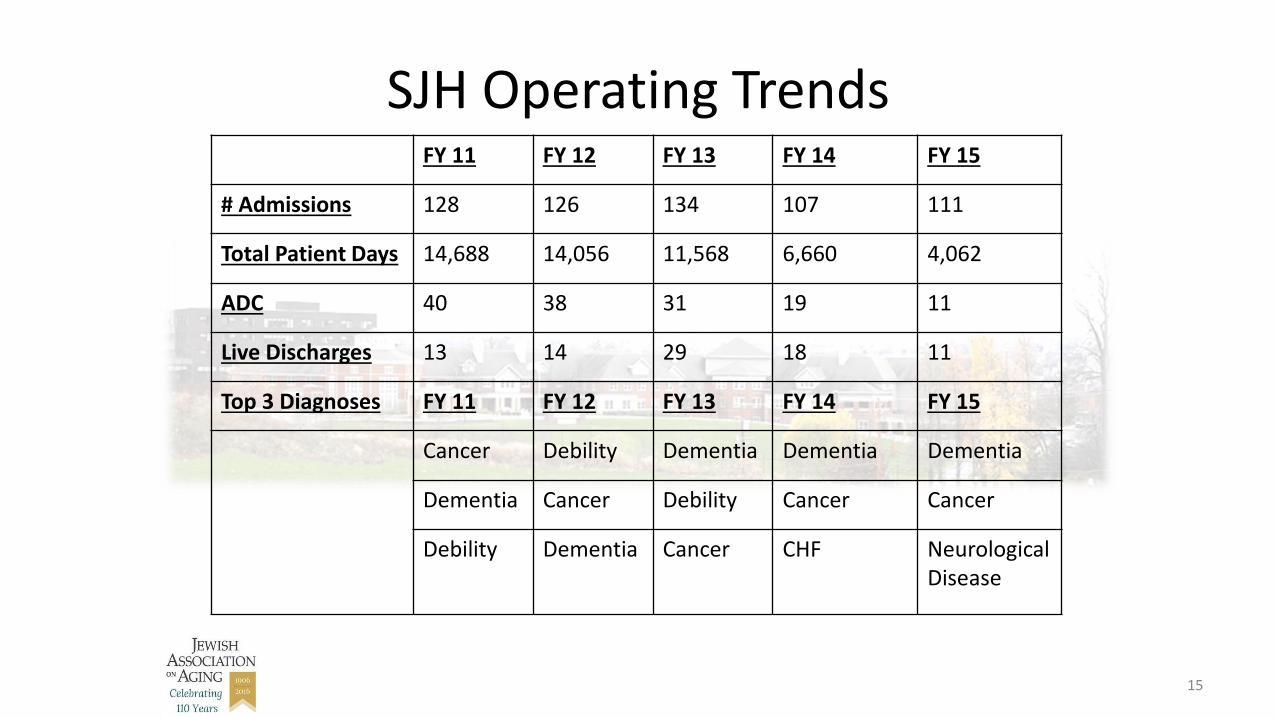
SJH Operating TrendsFY 11 FY 12 FY 13 FY 14 FY 15
# Admissions 128 126 134 107 111
Total Patient Days 14,688 14,056 11,568 6,660 4,062
ADC 40 38 31 19 11
Live Discharges 13 14 29 18 11
Top 3 Diagnoses FY 11 FY 12 FY 13 FY 14 FY 15
Cancer Debility Dementia Dementia Dementia
Dementia Cancer Debility Cancer Cancer
Debility Dementia Cancer CHF Neurological Disease
15
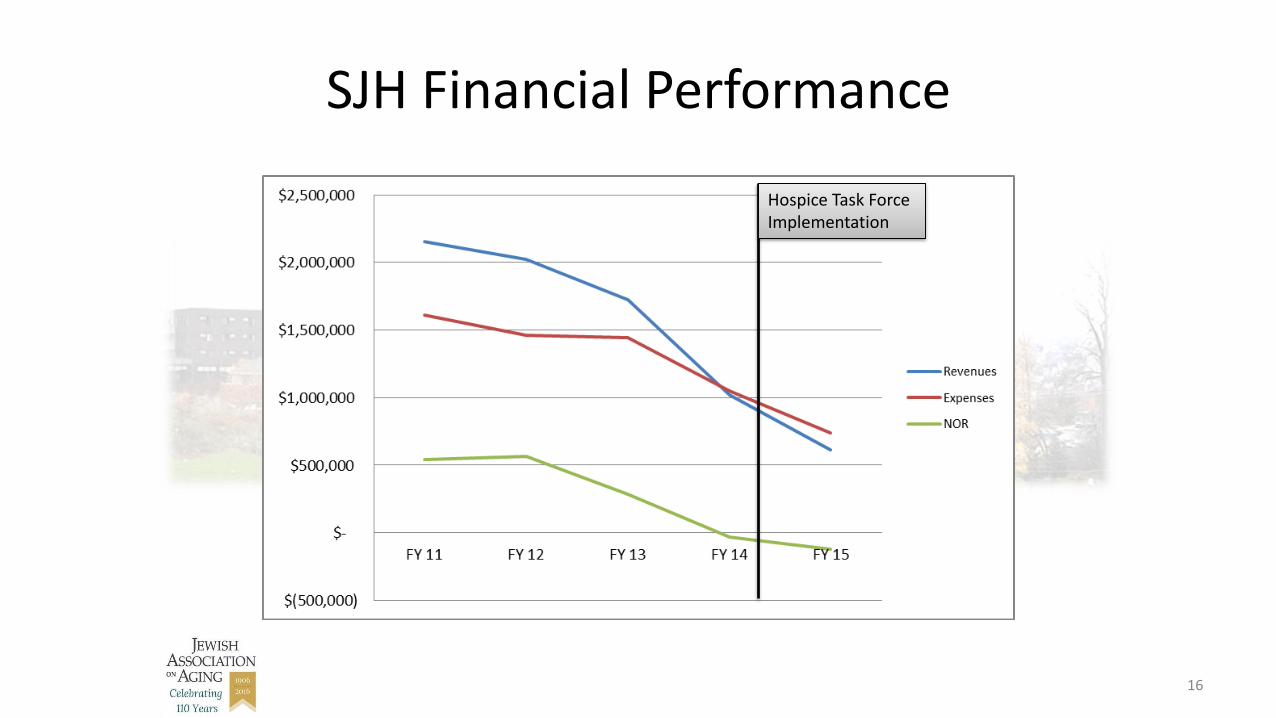
SJH Financial Performance
Hospice Task Force Implementation
16
JAA Board Of Directors: Call For Action
• Hospice Task Force developed to conduct a deep dive evaluation of Sivitz Jewish Hospice
– Implemented September 2014
– Members: Board representatives including Board Quality Committee Chair; Community Leaders and JAA Senior Management
– SWOT analysis completed
– Questioned: What makes us Jewish?
17
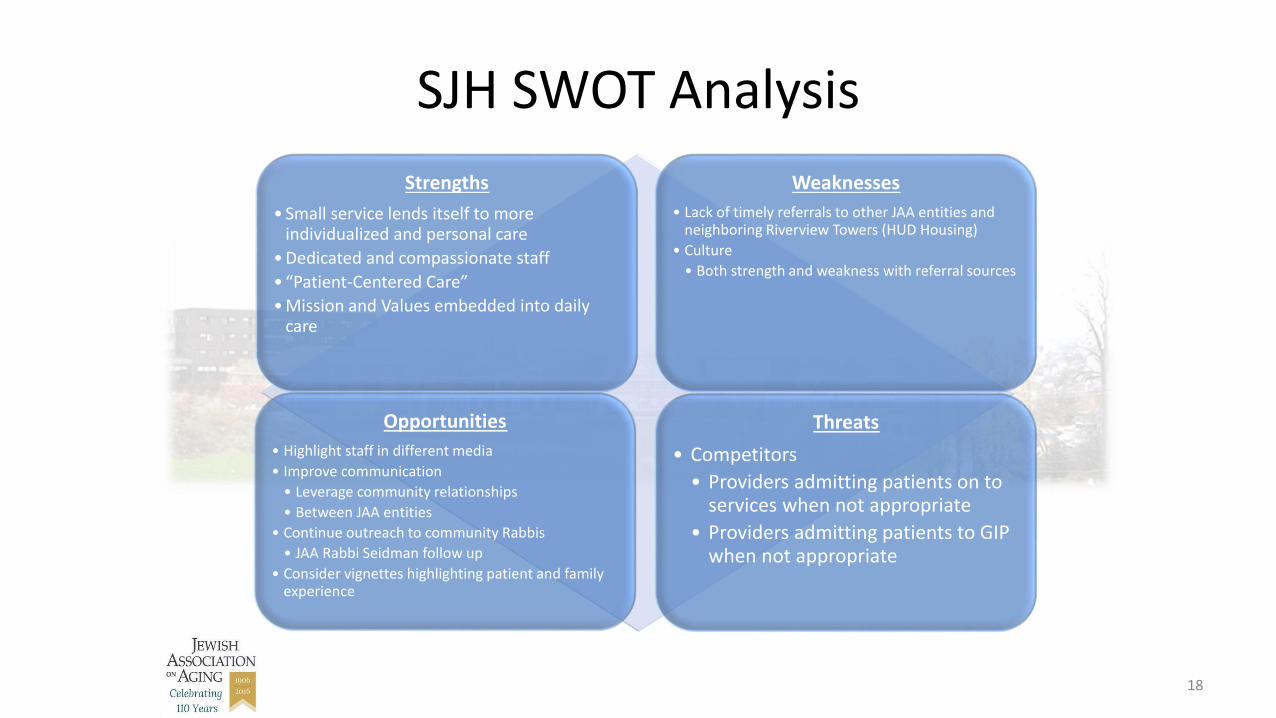
SJH SWOT Analysis
Strengths
• Small service lends itself to more individualized and personal care
• Dedicated and compassionate staff
• “Patient-Centered Care”
• Mission and Values embedded into daily care
Weaknesses
• Lack of timely referrals to other JAA entities and neighboring Riverview Towers (HUD Housing)
• Culture
• Both strength and weakness with referral sources
Opportunities
• Highlight staff in different media
• Improve communication
• Leverage community relationships
• Between JAA entities
• Continue outreach to community Rabbis
• JAA Rabbi Seidman follow up
• Consider vignettes highlighting patient and family experience
Threats
• Competitors
• Providers admitting patients on to services when not appropriate
• Providers admitting patients to GIP when not appropriate
18
Maintain Independence or Merge?
• Valuation performed by 3rd party
• Evaluation of Sale/Merger opportunities
• How would Jewish culture be maintained?
19
Task Force Decision – Maintain Independence
Why?
20

21
Staff Education Volunteer Training
Bereavement Recognition
Community Expectations
What makes us Jewish?
How Did We Revitalize SJH?
• Expense reduction
• Increase marketing & exposure
– Closure series
• Improved internal referral processes and relationships
• Enhance volunteer programs
22
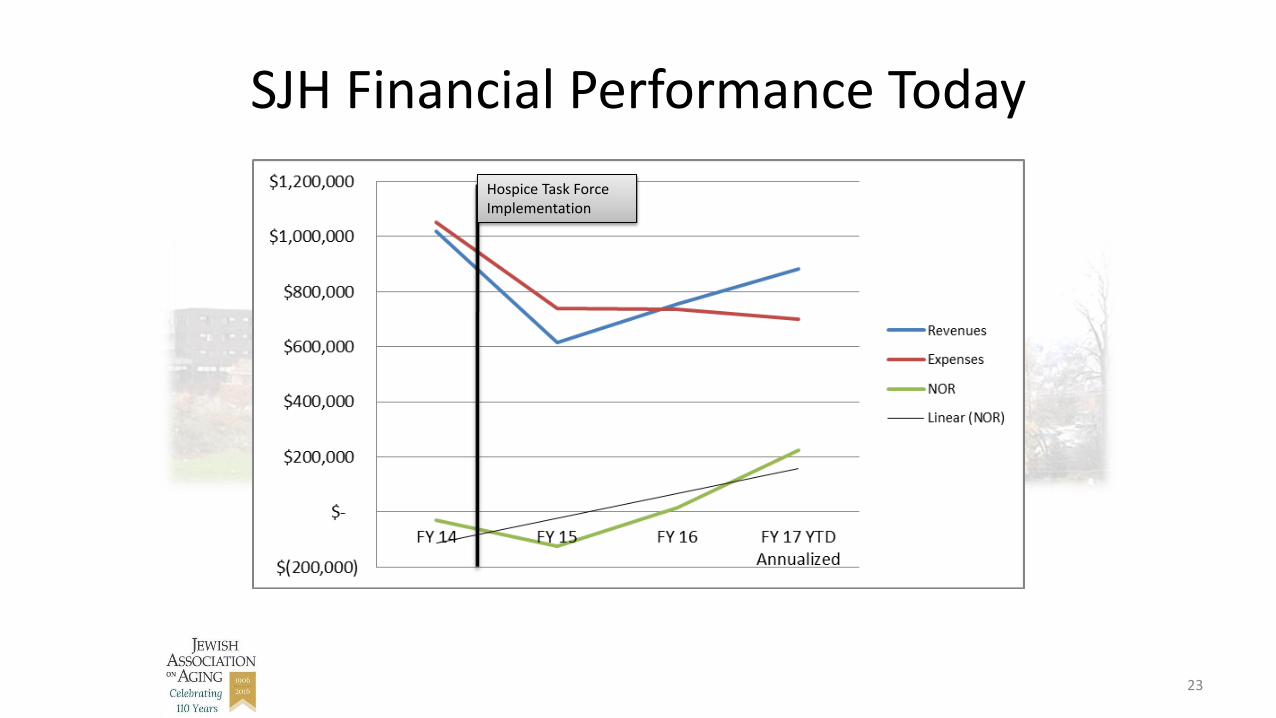
SJH Financial Performance Today
23
Hospice Task Force Implementation
SJH Today
• Preferred Provider within JAA continuum
• Staff retention
• No ADRs
• Hospice item set = 100%
• Deficiency free surveys
• Working more closely with Jewish Community Rabbis
• Partnership with Hillman Cancer Center
• 20th anniversary celebration
24
SJH Future Plans
25
• MCCM Recipient
– Phase II
• Staff certification
• AgeWell collaboration bereavement support for caregivers
AJAS Masterclass:
Montefiore Inpatient Hospice
Seth Vilensky
April 5, 2017
Montefiore Hospice: History
• Founded in 1992 – NCJW
• First Jewish Hospice agency in the state of Ohio
• Endowment through Jules and Ruth Vinney Philanthropic Fund, 2011

Montefiore Hospice: Today
Full service hospice agency
• Palliative care consult service
• Hospice at home
• Hospice in nursing home/assisted living
• Inpatient hospice unit – 6 beds
45 – 50 patient average daily census

• Medical Director
• Nurses, Aides, Social Workers, Chaplains, Bereavement
• Music, Art, Massage, Reiki therapists
• Volunteers
Montefiore Hospice: Team
Why build an Inpatient Hospice Unit?
• Market opportunity
• Full-service program
• Milt and Tamar Maltz
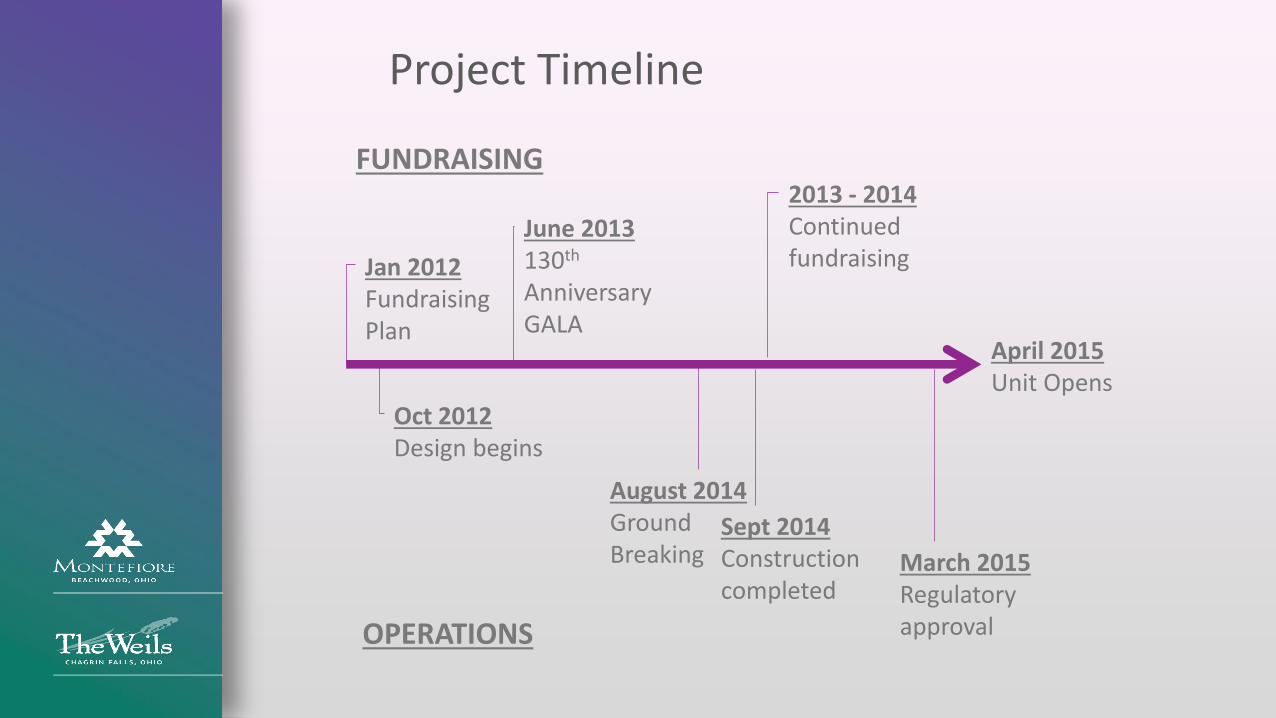
Project Timeline
Jan 2012FundraisingPlan
April 2015Unit Opens
Oct 2012Design begins
August 2014 Ground Breaking
June 2013130th
Anniversary GALA
2013 - 2014Continued fundraising
Sept 2014 Constructioncompleted
March 2015 Regulatory approval
FUNDRAISING
OPERATIONS


Project Funding
• Total Project Cost: $3.0m
• Total $ raised: $3.0m• Maltz Foundation: $1.5m• Additional fundraising: $1.5m
The Maltz Hospice House
• Virtual Tour
Differentiators
• Design and ‘home-like’ feel
• Location
• Team and staffing ratio• 1 RN• 1 STNA• Medical Director• Chaplain, social worker, integrative therapies,
volunteers
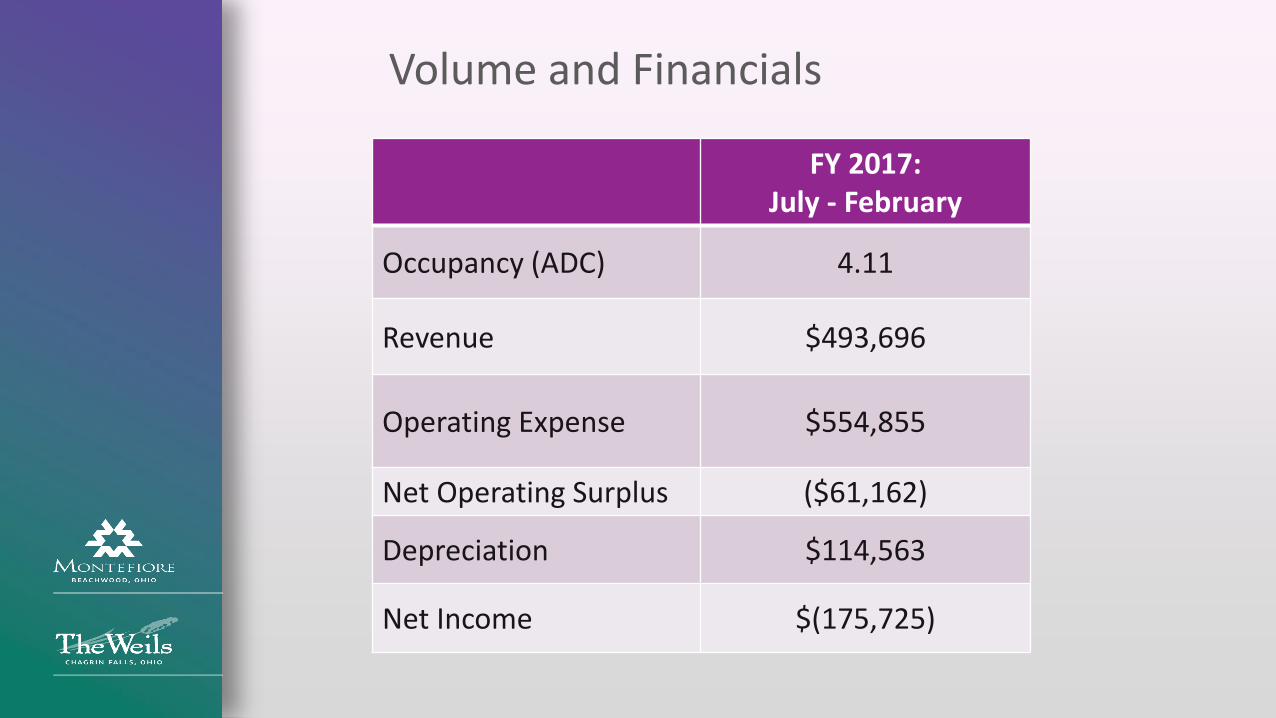
Volume and Financials
FY 2017:July - February
Occupancy (ADC) 4.11
Revenue $493,696
Operating Expense $554,855
Net Operating Surplus ($61,162)
Depreciation $114,563
Net Income $(175,725)

Lessons Learned
1. Patient mix: residential vs GIP
2. Medical supervision
3. Staffing a 6-bed unit
4. Marketing advantage
5. Community benefit


















