40
5900 Southwest Parkway | Building 2, Suite 200, Austin, TX 78735 Tel: (512) 366 ‐3745 Fax: (866) 315‐2353 www.healthsure.com Prepared by: 2018 BENEFITS ENROLLMENT GUIDE

5900 Southwest Parkway | Building 2, Suite 200, Austin, TX 78735Tel: (512) 366 ‐3745 Fax: (866) 315‐2353 www.healthsure.com
Prepared by:
2018 BENEFITS ENROLLMENT GUIDE

Table of Contents
Contacts Page 1
Benefit Basics Page 2
Monthly Premium Contributions Page 3
Medical Insurance Page 4
Prescription Drug Benefit Schedule Page 13
Dental Insurance Page 14
Vision Insurance Page 15
Basic Life & Voluntary Life Insurance Coverage Page 16
Short & Long Term Disability Page 18
Critical Illness Page 19
Accident Page 21
Cancer Page 23
Flexible Spending Accounts Page 25
Employee Assistance Program Page 27
Will Prep Services Page 28
Wellness Program Page 29
401K Savings and Profit Sharing Program Page 31
Important Notices Page 35
1

Contacts
Peterson Human Resources PlanSource Online Enrollment
https://benefits.plansource.com
User name: (up to 6 characters of last name, last 4 of social security)
Sandra PattersonHR Benefits Coordinator
830‐258‐7441
[email protected] Password: Your birthdate in YYYYMMDD format
Medical Dental
WebTPA ‐ Group #2012PRMC
www.webtpa.com
800‐953‐2015
WebTPA – Group #2012PRMC
PPO PHCS Plan
www.webtpa.com
800‐678‐7427
Guardian Flexible Spending Accounts (FSA)
Vision, Life, Disability, Critical Illness, Cancer & Accident
Pension Concepts & Administration
Group #: 00490572 Jan Holmes
www.guardiananytime.com [email protected]
888‐600‐1600 806‐745‐9781 X 4
Employee Assistance Program Will Prep Services
Work Life Matters Available to members enrolled in voluntary life
800‐386‐7055 877‐433‐6789
www.ibhworklife.com www.ibhwillprep.com
User Name: Matters User Name: WillPrep
Password: wlm70101 Password: GLIC09
Wellness Revolution Retirement – Mass Mutual
Viverae www.retiresmart.com
www.PRMCWellness.com 800‐743‐5274
888‐848‐3723
2

Benefit Basics
Qualified Life Event
Peterson Regional Medical Center offers a comprehensive suite of benefits to promote health and financial security for you and your family. This booklet provides you with a summary of your benefits. Please review it carefully so you can choose the coverage that’s right for you.
As a Peterson employee, you are eligible for benefits if you work at least 30 hours per week.
Benefits are effective on the first day of the month following 60 days of full‐time employment.
If the spouse of an eligible employee is eligible for coverage through their employer, they are not eligible to participate in this plan.
Generally, you may change your benefit elections only during the annual enrollment period. However, you may change your benefit elections during the year if you experience a qualified life event, including:• Marriage• Divorce or legal separation• Death of your spouse or dependent child• Birth of your child• Adoption of or placement for adoption of your
child• Change in employment status of employee,
spouse or dependent child• Qualification by the Plan Administrator of a child
support order for medical coverage• Entitlement to Medicare or MedicaidYou must notify Human Resources within 30 days of the qualified life event. Depending on the type of event, you may be asked to provide proof of the event.
If you do not contact Human Resources within 30 days of the qualified event, you will have to wait until the next annual enrollment period to make changes (unless you experience another qualified life event).
For more information about your benefits, please contact your HR Department.
Notice of Privacy PracticesPeterson Regional Medical Center understands that information about you and your health is personal and we are committed to protecting this information. Peterson Regional Medical Center maintains a Notice of Privacy Practices that explains how we may disclose your health information. The Notice of Privacy Practices also describes your rights and our obligations regarding the use and disclosure of this information
Plans at a Glance
This brochure is intended to provide a convenient summary of benefit plans. It is not intended to be a legal document. If there are any inconsistencies between the information in this brochure and the plan Summary of Benefit documents or contracts, the plan documents and contracts will prevail.
Terms and Descriptions
The information in this Enrollment Guides is presented for illustrative purposes and is based on information provided by the employer. The text contained in this Guide was taken from various summary plan descriptions and benefit information. While every effort was taken to accurately report your benefits, discrepancies or errors are always possible. In case of discrepancy between the Guide and the actual plan documents, the actual plan documents will prevail. If you have any questions about your Guide, contact your Human Resources Department.
Reasonable & Customary (R&C) and /or Usual & Customary (U&C)
When using out‐of‐network providers for medical or dental benefit, payments from insurance carriers are based on what is considered reasonable. Everything not included as reasonable is considered the member’s responsibility to pay to the provider, and the member is not credited for any of these expenses towards their deductible or coinsurance maximums.
Benefit Payments
For benefits received in the Network, you are responsible only for your co‐payment or deductible amount and coinsurance. Your provider will file the claim. Benefits for Non‐Network visits are payable on a reimbursement basis only. You can be subject to additional charges over the reasonable and customary allowed amount.
3

MEDICAL BENEFITS - BASE PLAN
BASE PLANPRMC NETWORK
PROVIDERS NON-NETWORK
PROVIDERS Lifetime Maximum Unlimited
MAXIMUM BENEFIT AMOUNT: Aggregate
Annual Limit Unlimited
DEDUCTIBLE, PER CALENDAR YEAR - THE TIER 1 AND TIER 2 DEDUCTIBLE AMOUNTS ACCUMULATE TOGETHER, NOT SEPARATELY
BASE PLAN Per Covered Person $3,000 $3,000 N/A
Per Family Unit $6,000 $6,000 N/A
MAXIMUM OUT-OF-POCKET AMOUNT, PER CALENDAR YEAR - TTHHEE OOUUTT--OOFF--PPOOCCKKEETT AAMMOOUUNNTTSS FFOORR TIER 1 AND TIER 2 NNEETTWWOORRKKSS AACCCCUUMMUULLAATTEE TTOOGGEETTHHEERR..
Any applicable Prescription Drug Plan copayments and/or coinsurance percentages are integrated with the Medical Plan’s Out-of-Pocket Maximums.
BASE PLAN Per Covered Person $6,850 $6,850 N/A
Per Family Unit $13,700 $13,700 N/A
The Plan will pay the designated percentage of Covered Charges until out-of-pocket amounts are reached, at which time the Plan will pay 100% of the remainder of Covered Charges for the rest of the
Calendar Year unless stated otherwise. The following charges do not apply toward the out-of-pocket maximum and are never paid at 100%:
Cost containment penalties Amounts over Usual and Reasonable Charges
Non-covered expenses Othognathic Conditions & Surgery
Smoking Cessation Program COVERED CHARGES Benefits are payable as shown below. However, to the extent that a service is specifically described in the Summary of Benefits and Coverage and it is not specifically addressed below, benefits will be payable at the levels shown in the Summary of Benefits and Coverage.
PLEASE NOTE: THERE IS NO OUT-OF-NETWORK COVERAGE EXCEPT FOR EMERGENCY SITUATIONS, WHICH ARE PAYABLE BASED UPON USUAL AND
REASONABLE ALLOWANCES Hospital Services Note: The following services are NOT available at PRMC: Bariatric Surgery, Cardiac Catherizations
(interventional), Cardiac Surgery, Multiple Trauma, Neonatal ICU, Pediatric ICU, PET Scans and Neurosurgery.
Room and Board semiprivate room rate
100%, deductible waived 75% after deductible Not Covered
Intensive Care Unit 100%, deductible waived 75% after deductible Not Covered
Rehabilitation Facility 100%, deductible waived 75% after deductible Not Covered
Emergency Room (true emergency)
75%, deductible waived 75%, deductible waived 75%, deductible waived
Emergency Room (non-emergency)
75% after deductible 75% after deductible Not Covered
Urgent Care $30 copayment 75% after deductible Not Covered 23 Hour Observation 100%, deductible waived 75% after deductible Not Covered
Members must use PRMC for health services unless the service is not available at PRMC. If service is not available member must use an in-network provider.
5

BASE PLANPRMC NETWORK
PROVIDERS NON-NETWORK
PROVIDERS Radiation Therapy, Inhalation Therapy,
Chemotherapy 75% after deductible 75% after deductible
Not Covered
Outpatient Dialysis 75% after deductible 75% after deductible Not Covered Please see the Covered Charges section for more information on Outpatient Dialysis coverage.
Cardiac Rehabilitation 75% after deductible 75% after deductible Not Covered Outpatient Surgery 75% after deductible 75% after deductible Not Covered Independent Lab Not Available 75% after deductible Not Covered
Diagnostic Imaging/ X-ray Services
75% after deductible 75% after deductible Not Covered
Diagnostic Laboratory Services
75% after deductible 75% after deductible Not Covered
Sleep Studies 75% after deductible 75% after deductible Not Covered Mammograms (non-routine)
75% after deductible 75% after deductible Not Covered
Colonoscopy/ Sigmoidoscopy
(Routine or non-routine)
100% deductible waived
100% deductible waived
Not Covered
Pre-admission Testing 75% after deductible 75% after deductible Not Covered Note: Occupational, Speech and Physical Therapy visit maximums are separate.
Occupational Therapy 60 day Calendar Year
maximum 75% after deductible 75% after deductible Not Covered
Speech Therapy 60 day Calendar Year
maximum 75% after deductible 75% after deductible Not Covered
Physical Therapy 60 day Calendar Year
maximum 75% after deductible 75% after deductible Not Covered
Skilled Nursing Facility Must be within 7 days of
related Hospital confinement
Not Available 75% after deductible Not Covered
Physician Services Inpatient visits Not Available 75% after deductible Not Covered
Emergency room visit (true emergency)
75%, deductible waived 75%, deductible waived 75%, deductible waived
Emergency room visit (non emergency)
75% after deductible 75% after deductible Not Covered
Urgent Care – Physician visit
$30 copayment 75% after deductible Not Covered
Office visits Primary Care Physician
(PCP) $30 copayment $30 copayment Not Covered
Office visits Specialist $60 copayment $60 copayment Not Covered
All other services rendered during the
visit except laboratory test and x-rays
75% after deductible 75% after deductible Not Covered
Diagnostic Laboratory Services - office 75% after deductible 75% after deductible
Not Covered
6
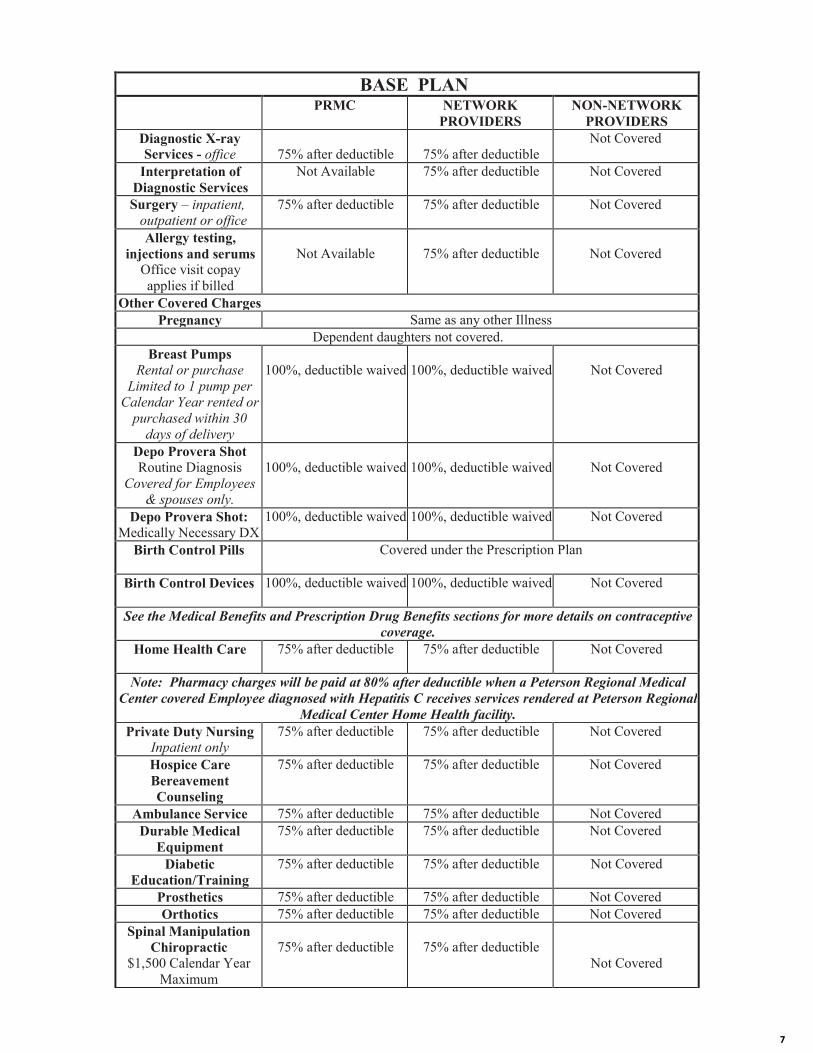
BASE PLANPRMC NETWORK
PROVIDERS NON-NETWORK
PROVIDERS Diagnostic X-ray Services - office 75% after deductible 75% after deductible
Not Covered
Interpretation of Diagnostic Services
Not Available 75% after deductible Not Covered
Surgery – inpatient, outpatient or office
75% after deductible 75% after deductible Not Covered
Allergy testing, injections and serums
Office visit copay applies if billed
Not Available 75% after deductible Not Covered
Other Covered Charges Pregnancy Same as any other Illness
Dependent daughters not covered. Breast Pumps
Rental or purchase Limited to 1 pump per
Calendar Year rented or purchased within 30
days of delivery
100%, deductible waived 100%, deductible waived Not Covered
Depo Provera Shot Routine Diagnosis
Covered for Employees & spouses only.
100%, deductible waived 100%, deductible waived Not Covered
Depo Provera Shot: Medically Necessary DX
100%, deductible waived 100%, deductible waived Not Covered
Birth Control Pills Covered under the Prescription Plan
Birth Control Devices 100%, deductible waived 100%, deductible waived Not Covered
See the Medical Benefits and Prescription Drug Benefits sections for more details on contraceptive coverage.
Home Health Care 75% after deductible 75% after deductible Not Covered
Note: Pharmacy charges will be paid at 80% after deductible when a Peterson Regional Medical Center covered Employee diagnosed with Hepatitis C receives services rendered at Peterson Regional
Medical Center Home Health facility. Private Duty Nursing
Inpatient only 75% after deductible 75% after deductible Not Covered
Hospice Care Bereavement Counseling
75% after deductible 75% after deductible Not Covered
Ambulance Service 75% after deductible 75% after deductible Not Covered Durable Medical
Equipment 75% after deductible 75% after deductible Not Covered
Diabetic Education/Training
75% after deductible 75% after deductible Not Covered
Prosthetics 75% after deductible 75% after deductible Not Covered Orthotics 75% after deductible 75% after deductible Not Covered
Spinal Manipulation Chiropractic
$1,500 Calendar Year Maximum
75% after deductible 75% after deductible Not Covered
7

BASE PLANPRMC NETWORK
PROVIDERS NON-NETWORK
PROVIDERS Mental Disorders and Substance Abuse
Inpatient 100%, deductible waived 75% after deductible Not Covered
Outpatient Treatment Facility
Not Available 75% after deductible Not Covered
Partial Day Treatment Facility
Not Available 75% after deductible Not Covered
Office visits Not Available $60 copayment Not Covered Preventive Care See the Covered Charges section for more details on Preventive Care benefits.
Routine Well Adult Care
100% deductible waived
100% deductible waived
Not Covered
Includes: Standard Preventive Care, office visits, pap smear, mammogram, prostate screening, gynecological exam, routine physical examination, x-rays, laboratory tests, hearing tests,
immunizations/flu shots, bone density scans, stress tests,colonoscopies, sigmoidoscopies and diagnostic procedures.
Frequency limits for mammogram……………………….One per Calendar Year Frequency limits for routine colonoscopy……………… . A routine colonoscopy is available
for a Covered Person age 50 or older, once per 130 months (or more frequently if recommended by a Physician, provided that such person has a positive family history).
Frequency limits for routine sigmoidoscopy…………… . A routine sigmoidoscopy is available for a Covered Person age 50 or older, once per 60 months (or more frequently if recommended
by a Physician, provided that such person has a positive family history).
Shingles vaccine will be covered through the Occupational Health Nurse at 100%. Please call 830-285-7459 to make an appt to get the vaccine. Shingles vaccines received anywhere else will not be covered.
Routine Well Child Care
100% (if services available)
100% deductible waived
Not Covered
Includes: Standard Preventive Care, office visits, routine physical examination, laboratory tests, x-rays, immunizations and other preventive care and services required by applicable law if provided by
a Panel/Network/Participating Provider through age 18. Hearing Exams
(with diagnosis) Routine hearing exams covered under Preventive Care
75% after deductible (if services available)
75% after deductible Not Covered
Smoking Cessation Services Outpatient
Limited to 2 courses per Calendar Year
100% deductible waived
100% deductible waived
Not Covered
Diabetes Education outpatient
100%, deductible waived 100%, deductible waived Not Covered
Jaw Joint/TMJ Office visit
Not Available 75% after deductible Not Covered
Jaw Joint/TMJ Diagnostic Testing
75%after deductible 75% after deductible Not Covered
Jaw Joint/TMJ Inpatient/Outpatient Surgery Physician
Charges
Not Available 75% after deductible Not Covered
TMJ Inpatient/Outpatient facility charges paid the same as any other Illness
8

BUY-UP PLANPRMC NETWORK
PROVIDERS NON-NETWORK
PROVIDERS Lifetime Maximum Unlimited
MAXIMUM BENEFIT AMOUNT: Aggregate
Annual Limit Unlimited
DEDUCTIBLE, PER CALENDAR YEAR - THE TIER 1 AND TIER 2 DEDUCTIBLE AMOUNTS ACCUMULATE TOGETHER, NOT SEPARATELY
BUY-UP PLAN Per Covered Person $2,000 $2,000 N/A
Per Family Unit $4,000 $4,000 N/A
MAXIMUM OUT-OF-POCKET AMOUNT, PER CALENDAR YEAR - TTHHEE OOUUTT--OOFF--PPOOCCKKEETT AAMMOOUUNNTTSS FFOORR TIER 1 AND TIER 2 NNEETTWWOORRKKSS AACCCCUUMMUULLAATTEE TTOOGGEETTHHEERR..
Any applicable Prescription Drug Plan copayments and/or coinsurance percentages are integrated with the Medical Plan’s Out-of-Pocket Maximums.
BUY-UP PLAN Per Covered Person $6,850 $6,850 N/A
Per Family Unit $13,700 $13,700 N/A
The Plan will pay the designated percentage of Covered Charges until out-of-pocket amounts are reached, at which time the Plan will pay 100% of the remainder of Covered Charges for the rest of the
Calendar Year unless stated otherwise. The following charges do not apply toward the out-of-pocket maximum and are never paid at 100%:
Cost containment penalties Amounts over Usual and Reasonable Charges
Non-covered expenses Othognathic Conditions & Surgery
Smoking Cessation Program COVERED CHARGES Benefits are payable as shown below. However, to the extent that a service is specifically described in the Summary of Benefits and Coverage and it is not specifically addressed below, benefits will be payable at the levels shown in the Summary of Benefits and Coverage.
PLEASE NOTE: THERE IS NO OUT-OF-NETWORK COVERAGE EXCEPT FOR EMERGENCY SITUATIONS, WHICH ARE PAYABLE BASED UPON USUAL AND
REASONABLE ALLOWANCES Hospital Services Note: The following services are NOT available at PRMC: Bariatric Surgery, Cardiac Catherizations
(interventional), Cardiac Surgery, Multiple Trauma, Neonatal ICU, Pediatric ICU, PET Scans and Neurosurgery.
Room and Board semiprivate room rate
100%, deductible waived
$2,000 copayment, then 50% after deductible NOTE: Copayment
waived and coinsurance increased to 75% if
services not available at PRMC.
Not Covered
Intensive Care Unit 100%, deductible waived
$2,000 copayment, then 50% after deductible NOTE: Copayment
waived and coinsurance increased to 75% if
services not available at PRMC.
Not Covered
MEDICAL BENEFITS - BUY UP PLAN
Members must use PRMC for health services unless the service is not available at PRMC. If service is not available member must use an in-network provider.
9
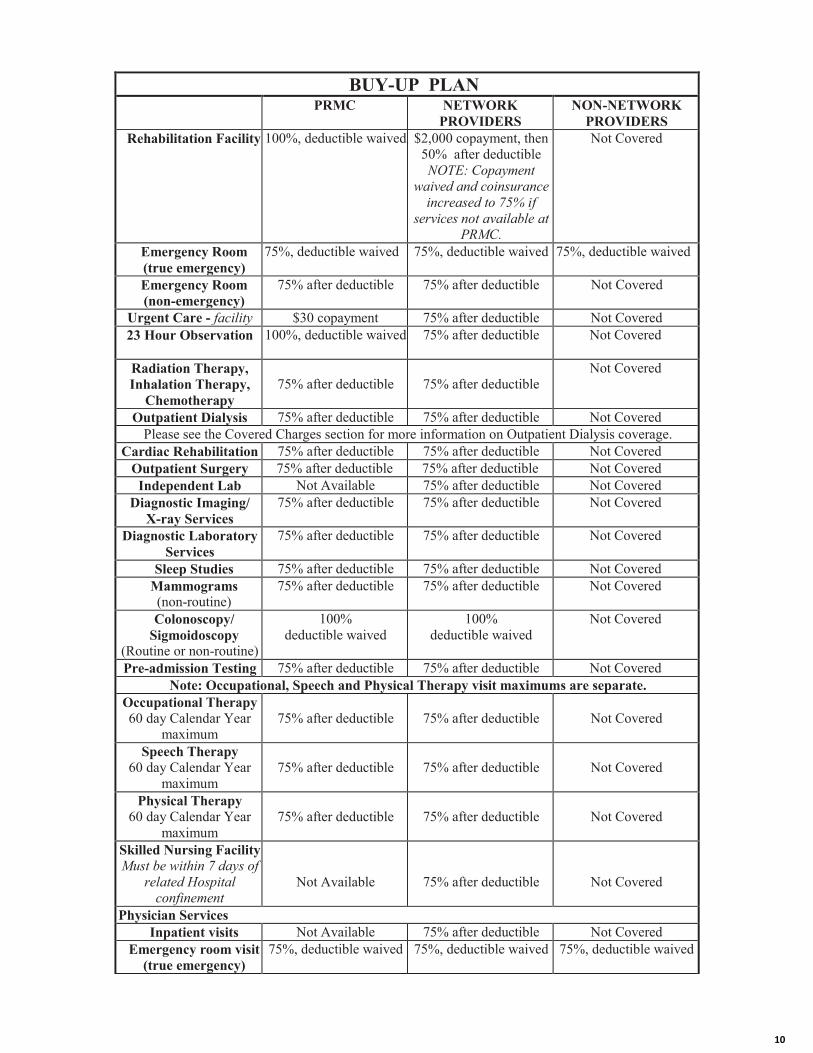
BUY-UP PLANPRMC NETWORK
PROVIDERS NON-NETWORK
PROVIDERS Rehabilitation Facility 100%, deductible waived $2,000 copayment, then
50% after deductible NOTE: Copayment
waived and coinsurance increased to 75% if
services not available at PRMC.
Not Covered
Emergency Room (true emergency)
75%, deductible waived 75%, deductible waived 75%, deductible waived
Emergency Room (non-emergency)
75% after deductible 75% after deductible Not Covered
Urgent Care - facility $30 copayment 75% after deductible Not Covered 23 Hour Observation 100%, deductible waived 75% after deductible Not Covered
Radiation Therapy, Inhalation Therapy,
Chemotherapy 75% after deductible 75% after deductible
Not Covered
Outpatient Dialysis 75% after deductible 75% after deductible Not Covered Please see the Covered Charges section for more information on Outpatient Dialysis coverage.
Cardiac Rehabilitation 75% after deductible 75% after deductible Not Covered Outpatient Surgery 75% after deductible 75% after deductible Not Covered Independent Lab Not Available 75% after deductible Not Covered
Diagnostic Imaging/ X-ray Services
75% after deductible 75% after deductible Not Covered
Diagnostic Laboratory Services
75% after deductible 75% after deductible Not Covered
Sleep Studies 75% after deductible 75% after deductible Not Covered Mammograms (non-routine)
75% after deductible 75% after deductible Not Covered
Colonoscopy/ Sigmoidoscopy
(Routine or non-routine)
100% deductible waived
100% deductible waived
Not Covered
Pre-admission Testing 75% after deductible 75% after deductible Not Covered Note: Occupational, Speech and Physical Therapy visit maximums are separate.
Occupational Therapy 60 day Calendar Year
maximum 75% after deductible 75% after deductible Not Covered
Speech Therapy 60 day Calendar Year
maximum 75% after deductible 75% after deductible Not Covered
Physical Therapy 60 day Calendar Year
maximum 75% after deductible 75% after deductible Not Covered
Skilled Nursing Facility Must be within 7 days of
related Hospital confinement
Not Available 75% after deductible Not Covered
Physician Services Inpatient visits Not Available 75% after deductible Not Covered
Emergency room visit (true emergency)
75%, deductible waived 75%, deductible waived 75%, deductible waived
10

BUY-UP PLANPRMC NETWORK
PROVIDERS NON-NETWORK
PROVIDERS Emergency room visit
(non emergency) 75% after deductible 75% after deductible Not Covered
Urgent Care – Physician visit
$30 copayment 75% after deductible Not Covered
Office visits Primary Care Physician
(PCP) $25 copayment $25 copayment Not Covered
Office visits Specialist $50 copayment $50 copayment Not Covered
All other services rendered during the
visit except laboratory test and x-rays
75% after deductible 75% after deductible Not Covered
Diagnostic Laboratory Services - office 75% after deductible 75% after deductible
Not Covered
Diagnostic X-ray Services - office 75% after deductible 75% after deductible
Not Covered
Interpretation of Diagnostic Services
Not Available 75% after deductible Not Covered
Surgery – inpatient, outpatient or office
75% after deductible 75% after deductible Not Covered
Allergy testing, injections and serums
Office visit copay applies if billed
Not Available 75% after deductible Not Covered
Other Covered Charges Pregnancy Same as any other Illness
Dependent daughters not covered. Breast Pumps
Rental or purchase Limited to 1 pump per
Calendar Year rented or purchased within 30
days of delivery
100%, deductible waived 100%, deductible waived Not Covered
Depo Provera Shot Routine Diagnosis
Covered for Employees & spouses only.
100%, deductible waived 100%, deductible waived Not Covered
Depo Provera Shot: Medically Necessary DX
100%, deductible waived 100%, deductible waived Not Covered
Birth Control Pills Covered under the Prescription Plan
Birth Control Devices 100%, deductible waived 100%, deductible waived Not Covered
See the Medical Benefits and Prescription Drug Benefits sections for more details on contraceptive coverage.
Home Health Care 75% after deductible 75% after deductible Not Covered
Note: Pharmacy charges will be paid at 80% after deductible when a Peterson Regional Medical Center covered Employee diagnosed with Hepatitis C receives services rendered at Peterson Regional
Medical Center Home Health facility.
11

BUY-UP PLANPRMC NETWORK
PROVIDERS NON-NETWORK
PROVIDERS Private Duty Nursing
Inpatient only 75% after deductible 75% after deductible Not Covered
Hospice Care Bereavement Counseling
75% after deductible 75% after deductible Not Covered
Ambulance Service 75% after deductible 75% after deductible Not Covered Durable Medical
Equipment 75% after deductible 75% after deductible Not Covered
Diabetic Education/Training
75% after deductible 75% after deductible Not Covered
Prosthetics 75% after deductible 75% after deductible Not Covered Orthotics 75% after deductible 75% after deductible Not Covered
Spinal Manipulation Chiropractic
$1,500 Calendar Year Maximum
75% after deductible 75% after deductible Not Covered
Mental Disorders and Substance Abuse
Inpatient
100%, deductible waived
$2,000 copayment, then 50% after deductible NOTE: Copayment
waived and coinsurance increased to 75% if
services not available at PRMC.
Not Covered
Outpatient Treatment Facility
Not Available 75% after deductible Not Covered
Partial Day Treatment Facility
Not Available 75% after deductible Not Covered
Office visits Not Available $50 copayment Not Covered Preventive Care See the Covered Charges section for more details on Preventive Care benefits.
Routine Well Adult Care
100% deductible waived
100% deductible waived
Not Covered
Includes: Standard Preventive Care, office visits, pap smear, mammogram, prostate screening, gynecological exam, routine physical examination, x-rays, laboratory tests, hearing tests,
immunizations/flu shots, bone density scans, stress tests,colonoscopies, sigmoidoscopies and diagnostic procedures.
Frequency limits for mammogram……………………….One per Calendar Year Frequency limits for routine colonoscopy……………… . A routine colonoscopy is available
for a Covered Person age 50 or older, once per 130 months (or more frequently if recommended by a Physician, provided that such person has a positive family history).
Frequency limits for routine sigmoidoscopy…………… . A routine sigmoidoscopy is available for a Covered Person age 50 or older, once per 60 months (or more frequently if recommended
by a Physician, provided that such person has a positive family history).
Shingles vaccine will be covered through the Occupational Health Nurse at 100%. Please call 830-285-7459 to make an appt to get the vaccine. Shingles vaccines received anywhere else will not be covered.
Routine Well Child Care
100% (if services available)
100% deductible waived
Not Covered
12

BUY-UP PLANPRMC NETWORK
PROVIDERS NON-NETWORK
PROVIDERS Includes: Standard Preventive Care, office visits, routine physical examination, laboratory tests, x-
rays, immunizations and other preventive care and services required by applicable law if provided by a Panel/Network/Participating Provider through age 18.
Hearing Exams (with diagnosis) Routine hearing exams covered under Preventive Care
75% after deductible (if services available)
75% after deductible Not Covered
Smoking Cessation Services Outpatient
Limited to 2 courses per Calendar Year
100% deductible waived
100% deductible waived
Not Covered
Diabetes Education outpatient
100%, deductible waived 100%, deductible waived Not Covered
Jaw Joint/TMJ Office visit
Not Available 75% after deductible Not Covered
Jaw Joint/TMJ Diagnostic Testing
75% after deductible 75% after deductible Not Covered
Jaw Joint/TMJ Inpatient/Outpatient Surgery Physician
Charges
Not Available 75% after deductible Not Covered
TMJ Inpatient/Outpatient facility charges paid the same as any other Illness Orthognathic
Conditions and Surgery 50% after deductible (if services available)
50% after deductible Not Covered
Note: Outpatient X-ray and Laboratory services for Orthognathic Conditions will be covered as specified under “DIAGNOSTIC X-RAY AND LABORATORY SERVICES”.
Medical Weight Loss Surgery
$30,000 Lifetime maximum (including
complications)
Not Available 75% after deductible Not Covered
Organ Transplants 75% after deductible (if services available)
Interlink In-Network Benefit:
75% after deductible
Not Covered
Covered transplants include: Heart, lung, Bone Marrow, Liver, Heart/Lung, Pancreas, Kidney, Kidney/Pancreas, and Multivisceral/Small Bowel. Please see the transplant section in the Covered
Charges section for more details on transplant benefits and limitations.
13

PRESCRIPTION DRUG BENEFIT SCHEDULE
SCOTT & WHITE PRESCRIPTION SERVICES
APPLIES TO BASE AND BUY-UP PLANS
Any applicable Prescription Drug Plan deductible, copayments and/or coinsurance percentages are integrated with the Medical Plan’s Out-of-Pocket Maximums.
$50 Calendar Year deductible applies to Preferred & Non-Preferred Brand Name Drugs
Pharmacy Option (33 Day Supply) Generic Drugs $10 copayment
Preferred Brand Name Drugs $55 copayment Non- Preferred Brand Name
Drugs $85 copayment
Specialty Drugs $80 copayment High Dollar Copayment (cost over $500)
Preferred Brand Name Drugs 15% Non- Preferred Brand Name
Drugs 25%
Mail Order Option (100 Day Supply) Generic Drugs $20 copayment
Brand Name Drugs $110 copayment Non- Preferred Brand Name
Drugs Not Applicable
Refer to the Prescription Drug Section for details on the Prescription Drug benefit.
14

DENTAL CARE BENEFIT SCHEDULE
DENTAL CARE BENEFIT
DENTAL CARE DEDUCTIBLE, PER CALENDAR YEAR
Per Covered Person $50 Per Family Unit $150
Calendar Year Deductible applies to these classes of services: Class B Services - Basic and Class C Services - Major
MAXIMUM BENEFIT AMOUNT BENEFIT
For Class A – Preventive, Class B - Basic and Class C - Major Services
Per Covered Person per Calendar Year
$1500
For Class D - Orthodontia (benefit available for Dependents under age 19)
Lifetime maximum per Covered Person $1500
Implants
Lifetime maximum per Covered Person $3,000 COVERED CHARGES
Dental Percentage Payable Class A Services - Preventive
Class B Services - Basic (6 month waiting period) Class C Services- Major (12 month waiting period)
Class D Services - Orthodontia
100% 80% 50% 50%
Note: The waiting period applies only to Late Enrollees from the Covered Person’s effective date of dental coverage before dental benefits are payable (a Late Enrollee is a person who enrolls other than
during the initial enrollment period or a special enrollment period as provided under the eligibility requirements of the Plan.)
15

About Your Benefits:
Eye care is a vital component of a healthy lifestyle. With vision insurance, having regular exams and purchasing contacts or glasses issimple and affordable. The coverage is inexpensive, yet the benefits can be significant! Guardian provides rich, flexible plans thatallow you to safeguard your health while saving you money. Review your plan options and see why vision insurance may be a greatbenefit for you.
Vision Benefit Summary
Visit any doctor with your Full Feature plan, but save by visiting any of the 50,000+ locations in the nation's largest visionnetwork.
Group Number: 00490572
Your Vision Plan Full Feature
Your Network is VSP Choice Network
Your Semi-monthly premium $ 4.78You and spouse $ 9.56You and child(ren) $ 8.23You, spouse and child(ren) $ 13.01Copay
Exams Copay $ 10
Materials Copay (waived for elective contact lenses) $ 25
Sample of Covered Services You pay (after copay if applicable):
In-network Out-of-network
Eye Exams $0 Amount over $55
Single Vision Lenses $0 Amount over $40
Lined Bifocal Lenses $0 Amount over $80
Lined Trifocal Lenses $0 Amount over $80
Lenticular Lenses $0 Amount over $80
Frames 80% of amount over $130¹ Amount over $65
Contact Lenses (Elective) Amount over $130 Amount over $105
Contact Lenses (Medically Necessary) $0 Amount over $210
Contact Lenses (Evaluation and fitting) 15% off UCR No discounts
Cosmetic Extras Avg. 20-25% off retail price No discounts
Glasses (Additional pair of frames and lenses) 20% off retail price** No discounts
Laser Correction Surgery Discount Up to 15% off the usual charge or 5%
off promotional price
No discounts
Service Frequencies
Exams Every calendar year
Lenses (for glasses or contact lenses)‡‡ Every calendar year
Frames Every two calendar years‡‡‡
Network discounts (cosmetic extras, glasses and contact lensprofessional service)
Limitless within 12 months of exam.
Dependent Age Limits 26
Visit www.GuardianAnytime.com and click on “Find a Provider”
16

Life Benefit SummaryGroup Number: 00490572
About Your Benefits:
Your family depends on you in many ways and you’ve worked hard to ensure their financial security. But if something happened to
you, will your family be protected? Will your loved ones be able to stay in their home, pay bills, and prepare for the future. Life
insurance provides a financial benefit that your family can depend on. And getting it at work is easier, more convenient and more
affordable than doing it on your own. If you have financial dependents- a spouse, children or aging parents, having life insurance is a
responsible and a smart decision. Enroll today to secure their future!
What Your Benefits Cover:
BASIC LIFE VOLUNTARY TERM LIFE
Employee Benefit Your employer provides Basic Life
Coverage for all full time
employees in the amount of 200%
of your annual salary, to a
maximum of $350,000.
$10,000 increments to a
maximum of $500,000. See Cost
Illustration page for details.
Accidental Death and Dismemberment Your Basic Life coverage includes
Accidental Death and
Dismemberment coverage equal
to one times the employee's life
benefits.
Employee, Spouse & Child(ren)
coverage. Maximum 1 times life
amount.
Spouse‡ Benefit N/A $5,000 increments to a maximum
of $250,000. See Cost Illustration
page for details.
Child Benefit N/A Your dependent children age 14
days to 26 years.
$1,000 increments to a maximum
of $10,000. Subject to state limits.
See Cost Illustration page for
details.
Guarantee Issue: The ‘guarantee’ means you are not required to
answer health questions to qualify for coverage up to and including
the specified amount, when you sign up for coverage during the initial
enrollment period.
Guarantee Issue coverage up to
$350,000 per employee
We Guarantee Issue coverage up
to:
Employee $200,000.
Spouse $50,000.
Dependent children $10,000.
Premiums Covered by your company if you
meet eligibility requirements
Increase on plan anniversary after
you enter next five-year age
group
Portability: Allows you to take your coverage with you if you
terminate employment.
No Yes, with age and other
restrictions
Conversion: Allows you to continue your coverage after your group
plan has terminated.
Yes, with restrictions; see
certificate of benefits
Yes, with restrictions; see
certificate of benefits
17
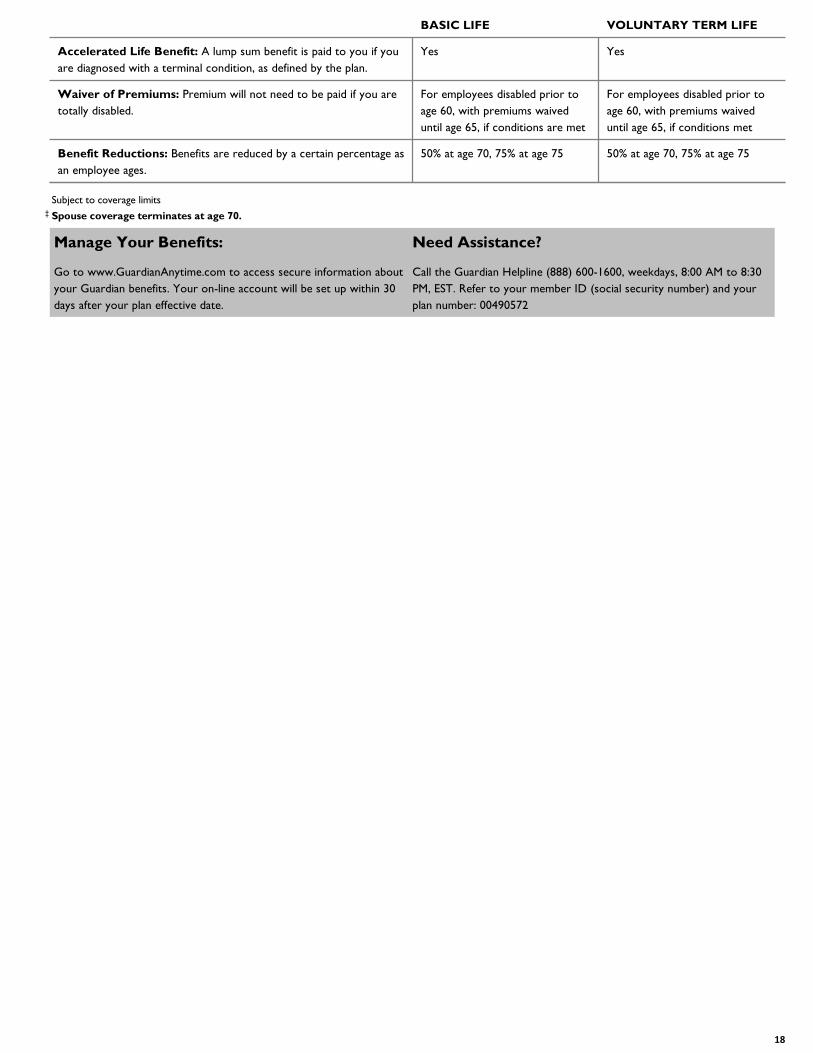
BASIC LIFE VOLUNTARY TERM LIFE
Accelerated Life Benefit: A lump sum benefit is paid to you if you
are diagnosed with a terminal condition, as defined by the plan.
Yes Yes
Waiver of Premiums: Premium will not need to be paid if you are
totally disabled.
For employees disabled prior to
age 60, with premiums waived
until age 65, if conditions are met
For employees disabled prior to
age 60, with premiums waived
until age 65, if conditions met
Benefit Reductions: Benefits are reduced by a certain percentage as
an employee ages.
50% at age 70, 75% at age 75 50% at age 70, 75% at age 75
Subject to coverage limits� Spouse coverage terminates at age 70.
Manage Your Benefits:
Go to www.GuardianAnytime.com to access secure information about
your Guardian benefits. Your on-line account will be set up within 30
days after your plan effective date.
Need Assistance?
Call the Guardian Helpline (888) 600-1600, weekdays, 8:00 AM to 8:30
PM, EST. Refer to your member ID (social security number) and your
plan number: 00490572
18

About Your Benefits:
You probably have insurance for your car or home, but what about the source of income that pays for it? You rely on your
paycheck for so many things, but what if you were suddenly unable to work due to an accident or illness? How will you put food
on the table, pay your mortgage or heat your home? Disability insurance can help replace lost income and make a difficult time a
little easier. Protect your most valuable asset, your paycheck-enroll today!
What Your Benefits Cover:
Disability Benefit Summary
Group Number: 00490572
Short-Term Disability Long-Term Disability
Plan 1 Plan 2.
Coverage amount60% of salary to maximum
$1500/week
60% of salary to maximum
$1500/week
60% of salary to maximum
$6000/month
Maximum payment period: Maximum length of
time you can receive disability benefits.13 weeks 9 weeks
Social Security Normal
Retirement Age
Accident benefits begin: The length of time you
must be disabled before benefits begin.Day 8 Day 30 Day 91
Illness benefits begin: The length of time you must
be disabled before benefits begin.Day 8 Day 30 Day 91
Evidence of Insurability: A health statement
requiring you to answer a few medical history
questions.
Health Statement not
required
Health Statement not
required
Health Statement not
required
Minimum work hours/week: Minimum number of
hours you must regularly work each week to be
eligible for coverage.
Planholder Determines Planholder Determines Planholder Determines
Pre-existing conditions: A pre-existing condition
includes any condition/symptom for which you, in the
specified time period prior to coverage in this plan,
consulted with a physician, received treatment, or
took prescribed drugs.
Not Applicable Not Applicable12 months look back; 12
months after exclusion
Premium waived if disabled: Premium will not
need to be paid when you are receiving benefits.Yes Yes Yes
UNDERSTANDING YOUR BENEFITS—DISABILITY (Some information may vary by state)
l Disability (long-term): For first two years of disability, you will receive benefit payments while you are unable to work in
your own occupation. After two years, you will continue to receive benefits if you cannot work in any occupation based on
training, experience and education.
l Earnings definition: Your covered salary excludes bonuses and commissions.
19

Critical Illness Benefit Summary
Group Number: 00490572
About Your Benefits:
It takes a lot to beat a serious illness. Unfortunately, it can also cost a lot. When you or a family member suffers a serious illness like
a stroke or heart attack, Critical Illness Insurance can help with expenses that medical insurance doesn't cover like deductibles or
out of pocket costs, or services like experimental treatment. Critical Illness supplements your medical and your disability income
insurance. The lump sum benefit is paid when you need it most, upon diagnosis, so you can rest assured that you will have funds to
offset upcoming out of pocket costs, and that you'll have the flexibility to elect treatments with less worry about the cost. Review
your options and enroll today!
What Your Benefits Cover:
Option 1 Option 2
Benefit Amount(s)Employee may choose a lump sum benefit of
$5,000 to $50,000 in $5,000 increments.
Employee may choose a lump sum benefit of
$5,000 to $50,000 in $5,000 increments.
CONDITIONS
Cancer 1st OCCURRENCE 2nd OCCURRENCE 1st OCCURRENCE 2nd OCCURRENCE
Invasive Cancer Not Applicable Not Applicable 100% 50%
Carcinoma In Situ Not Applicable Not Applicable 30% 0%
Benign Brain Tumor Not Applicable Not Applicable 75% 0%
Skin Cancer Not Applicable Not Applicable $250 per lifetime Not Covered
Vascular
Heart Attack 100% 50% 100% 50%
Stroke! 100% 50% 100% 50%
Heart Failure## 100% 50% 100% 50%
Coronary Arteriosclerosis# 30% 0% 30% 0%
Other
Organ Failure*** 100% 50% 100% 50%
Kidney Failure** 100% 50% 100% 50%
ADDITIONAL CONDITIONS 1st OCCURRENCE ONLY 1st OCCURRENCE ONLY
Accute Respiratory Distress Syndrome 30% 30%
Addison's Disease 30% 30%
ALS (Lou Gehrig's Disease) 100% 100%
Alzheimer's Disease 50% 50%
Coma 100% 100%
Huntington's Disease 30% 30%
Loss of Hearing 100% 100%
Loss of Sight 100% 100%
Loss of Speech 100% 100%
Multiple Sclerosis 30% 30%
Parkinson's Disease 100% 100%
Permanent Paralysis 50% for 1 limb, 100% for 2 limbs 50% for 1 limb, 100% for 2 limbs
Severe Burns 100% 100%
20

Option 1 Option 2
Childhood Conditions 1st OCCURRENCE ONLY 1st OCCURRENCE ONLY
Cerebral Palsy 100% 100%
Cleft Lip/Palate 100% 100%
Club Foot 100% 100%
Cystic Fibrosis 100% 100%
Down's Syndrome 100% 100%
Muscular Dystrophy 100% 100%
Spina Bifida 100% 100%
Type 1 Diabetes 100% 100%
Spouse Benefit
May choose a lump sum benefit up to $50,000.
Please see your cost illustration for a full list of
available benefit amounts.
May choose a lump sum benefit up to $50,000.
Please see your cost illustration for a full list of
available benefit amounts.
Child Benefit- children age Birth to 26 years 25% of employee's lump sum benefit 25% of employee's lump sum benefit
Benefit Reductions: Benefits are reduced by
a certain percentage as an employee ages50% at age 70 50% at age 70
Guarantee Issue: The ‘guarantee’ means you
are not required to answer health questions to
qualify for coverage up to and including the
specified amount, when you sign up for
coverage during the initial enrollment period.
We Guarantee Issue up to:
Less than age 70 $20,000
For a spouse:
Less than age 70 $20,000
For a child: All Amounts
Health questions are required if the
elected amount exceeds the Guarantee
Issue, as well as for all applicants age 70+
regardless of elected amount.
We Guarantee Issue up to:
Less than age 70 $20,000
For a spouse:
Less than age 70 $20,000
For a child: All Amounts
Health questions are required if the
elected amount exceeds the Guarantee
Issue, as well as for all applicants age 70+
regardless of elected amount.
Portability: Allows you to take your Critical
Illness coverage with you if you terminate
employment.
Included Included
Pre-Existing Condition Limitation: A
pre-existing condition includes any condition
for which you, in the specified time period
prior to coverage in this plan, consulted with a
physician, received treatment, or took
prescribed drugs.
3 months prior/6 months treatment free/12
months after
3 months prior/6 months treatment free/12
months after
Cancer Vaccine Benefit Not Applicable $50 per lifetime for receiving a cancer vaccine
Occupational HIV/Hepatitis Benefit100% of employee benefit for the first
occurrence.
100% of employee benefit for the first
occurrence.
WELLNESS BENEFIT
Employee Per Year Limit $50 $50
Spouse Per Year Limit $50 $50
Child Per Year Limit $50 $50
• ! Stroke: Stroke must be severe enough to cause neurological deficits at least 30 days after the event.
• ## Heart Failure: An insured must be placed on an organ transplant list in order to be eligible for the Heart failure benefits.
• # Coronary Arteriosclerosis: Coronary Arteriosclerosis must be severe enough to require a coronary artery bypass graft.
• *** Organ Failure: Organ failure includes both lungs, liver, pancreas or bone marrow and requires the insured to be placed on an organ
transplant list.
• ** Kidney Failure: An insured must be placed on an organ transplant list in order to be eligible for the Kidney failure benefits.
21

Accident Benefit Summary
About Your Benefits:
Accidents happen every day. Did you know almost 39 Million emergency room visits a year are due to an injury?¹ If you wereinjured from an accident, chances are you will have expenses that you were not anticipating-will you be prepared? AccidentInsurance can help you deal with those expenses. Benefit payments can help you with your medical deductibles and co-pays, andcover household expenses like groceries, mortgage payments and childcare, which can begin to pile up if you have to take sometime off from work. You are guaranteed coverage, so please enroll today!1Injury Facts, 2011 Edition, National Safety Council.
Group Number: 00490572
What Your Benefits Cover:
ACCIDENT
COVERAGE - DETAILS
Your Semi-monthly premium $9.46
You and Spouse $14.71
You and Child(ren) $12.40
You, Spouse and Child(ren) $17.65
Accident Coverage Type On and Off Job
Portability - Allows you to take your Accident coverage with you if you terminate
employment. Ported Accident plan terminates at age 70.
Included
ACCIDENTAL DEATH AND DISMEMBERMENT
Benefit Amount(s)
Employee $25,000
Spouse $12,500
Child $5,000
Catastrophic LossQuadriplegia, Loss of speech & hearing (both ears),
Loss of Cognitive function: 100% of AD&D
Hemiplegia & Paraplegia: 50% of AD&D
Common Carrier 200% of AD&D benefit
Common Disaster 200% of Spouse AD&D benefit
Dismemberment - Hand, Foot, SightSingle: 50% of AD&D benefit
Multiple: 100% of AD&D benefit
Dismemberment - Thumb/Index Finger Same Hand, Four Fingers Same Hand, All
Toes Same Foot
25% of AD&D benefit
Seatbelts and Airbags Seatbelts: $10,000 & Airbags: $15,000
Reasonable Accommodation to Home or Vehicle $2,500
WELLNESS BENEFIT - Per Year Limit $50
Child(ren) Age Limits Children age birth to 26 years
FEATURES
Accident Emergency Room Treatment $175
Accident Follow-Up Visit - Doctor $50 up to 6 treatments
Air Ambulance $1,000
Ambulance $150
Appliance - Wheelchair, leg or back brace, crutches, walker, walking boot that
extends above the ankle or brace for the neck.
$125
22

FEATURES (Cont.)
Blood/Plasma/Platelets $300
Burns (2nd Degree/3rd Degree)9 sq inches to 18 sq inches: $0/$2,000
18 sq inches to 35 sq inches: $1,000/$4,000
Over 35 sq inches: $3,000/$12,000
Burn - Skin Graft 50% of burn benefit
Child Organized Sport - Benefit is paid if the covered accident occurred while your
covered child is participating in an organized sport that is governed by an
organization and requires formal registration to participate.
20% increase to child benefits
Chiropractic Visits $25 per visit up to 6 visits
Coma $10,000
Concussions $75
Dislocations Schedule up to $4,400
Diagnostic Exam (Major) $150
Emergency Dental Work $300/Crown, $75/Extraction
Epidural pain management $100, 2 times per accident
Eye Injury $300
Family Care $20/day up to 30 days
Fracture Schedule up to $5,500
Hospital Admission $1,000
Hospital Confinement $225/day - up to 1 year
Hospital ICU Admission $2,000
Hospital ICU Confinement $450/day - up to 15 days
Initial Physician's office/Urgent Care Facility Treatment $75
Joint Replacement (hip/knee/shoulder) $2,500/$1,250/$1,250
Knee Cartilage $500
Laceration Schedule up to $400
Lodging - The hospital must be more than 50 miles from the insured's residence. $125/day, up to 30 days for companion hotel stay
Occupational or Physical Therapy $25/day up to 10 days
Prosthetic Device/Artificial Limb1: $500
2 or more: $1,000
Rehabilitation Unit Confinement $150/day up to 15 days
Ruptured Disc With Surgical Repair $500
SurgerySchedule up to $1,250
Hernia: $150
Surgery - Exploratory or Arthroscopic $250
Tendon/Ligament/Rotator Cuff1: $500
2 or more: $1,000
Transportation - Benefit is paid if you have to travel more than 50 miles one way to
receive special treatment at a hospital or facility due to a covered accident.
$500, 3 times per accident
X - Ray $30
UNDERSTANDING YOUR BENEFITS:
• Common Carrier – Benefit is paid if an insured's death occurs due to an accident while riding as a fare-paying passanger in a
public conveyance. If this is paid, we do not pay the Accidental Death benefit.
• Common Disaster – Benefit is paid if both you & your spouse die in a covered accident or separate covered accidents
within the same 24 hour period.
• Reasonable Accomodation – Benefit is payable if a modification is required to an insured's place of residence or vehicle due
to an Accidental Dismemberment or Catastrophic loss.
This handout is for illustrative purposes only and is an approximation. If any discrepancies between this handout and your paycheck stub exist, your paycheck stub prevails.
23
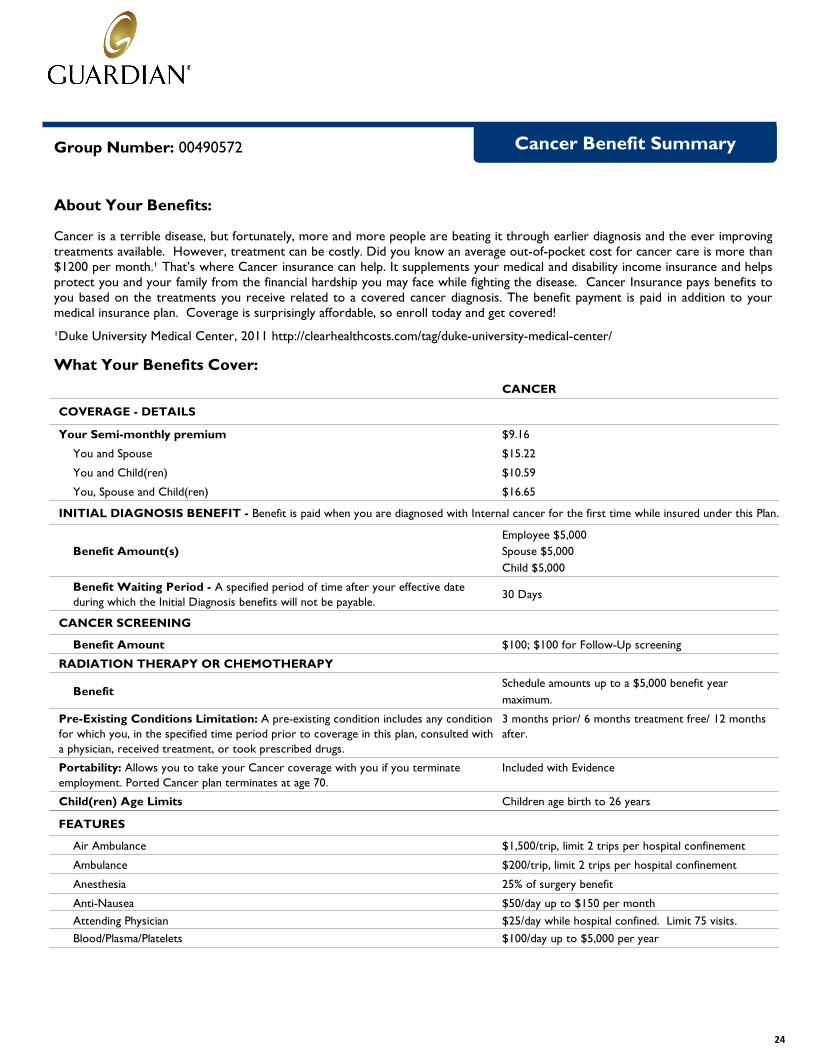
Cancer Benefit Summary
About Your Benefits:
Cancer is a terrible disease, but fortunately, more and more people are beating it through earlier diagnosis and the ever improvingtreatments available. However, treatment can be costly. Did you know an average out-of-pocket cost for cancer care is more than$1200 per month.¹ That’s where Cancer insurance can help. It supplements your medical and disability income insurance and helpsprotect you and your family from the financial hardship you may face while fighting the disease. Cancer Insurance pays benefits toyou based on the treatments you receive related to a covered cancer diagnosis. The benefit payment is paid in addition to yourmedical insurance plan. Coverage is surprisingly affordable, so enroll today and get covered!
¹Duke University Medical Center, 2011 http://clearhealthcosts.com/tag/duke-university-medical-center/
Group Number: 00490572
What Your Benefits Cover:
CANCER
COVERAGE - DETAILS
Your Semi-monthly premium $9.16
You and Spouse $15.22
You and Child(ren) $10.59
You, Spouse and Child(ren) $16.65
INITIAL DIAGNOSIS BENEFIT - Benefit is paid when you are diagnosed with Internal cancer for the first time while insured under this Plan.
Benefit Amount(s)
Employee $5,000
Spouse $5,000
Child $5,000
Benefit Waiting Period - A specified period of time after your effective date
during which the Initial Diagnosis benefits will not be payable.30 Days
CANCER SCREENING
Benefit Amount $100; $100 for Follow-Up screening
RADIATION THERAPY OR CHEMOTHERAPY
BenefitSchedule amounts up to a $5,000 benefit year
maximum.
Pre-Existing Conditions Limitation: A pre-existing condition includes any condition
for which you, in the specified time period prior to coverage in this plan, consulted with
a physician, received treatment, or took prescribed drugs.
3 months prior/ 6 months treatment free/ 12 months
after.
Portability: Allows you to take your Cancer coverage with you if you terminate
employment. Ported Cancer plan terminates at age 70.
Included with Evidence
Child(ren) Age Limits Children age birth to 26 years
FEATURES
Air Ambulance $1,500/trip, limit 2 trips per hospital confinement
Ambulance $200/trip, limit 2 trips per hospital confinement
Anesthesia 25% of surgery benefit
Anti-Nausea $50/day up to $150 per month
Attending Physician $25/day while hospital confined. Limit 75 visits.
Blood/Plasma/Platelets $100/day up to $5,000 per year
24

FEATURES (Cont.)
Bone Marrow/Stem Cell
Bone Marrow: $7,500
Stem Cell: $1,500
50% benefit for 2nd transplant. $1,000 benefit if a
donor
Experimental Treatment $100/day up to $1,000/month
Extended Care Facility/Skilled Nursing care $100/day up to 90 days per year
Government or Charity Hospital $300 per day in lieu of all other benefits
Home Health Care $50/visit up to 30 visits per year
Hormone Therapy $25/treatment up to 12 treatments per year
Hospice $50/day up to 100 days/lifetime
Hospital Confinement$300/day for first 30 days; $600/day for 31st day
thereafter per confinement
ICU Confinement$400/day for first 30 days; $600/day for 31st day
thereafter per confinement
Immunotherapy $500 per month, $2500 lifetime max
Inpatient Special Nursing $100/day up to 30 days per year
Medical Imaging $100/image up to 2 per year
Outpatient and family member lodging - Lodging must be more than 50 miles from
your home.
$75/day, up to 90 days per year
Outpatient or Ambulatory Surgical Center $250/day, 3 days per procedure
Physical or Speech Therapy $25/visit up to 4 visits per month, $400 lifetime max
ProstheticSurgically Implanted: $2,000/device, $4,000 lifetime max
Non-Surgically: $200/device, $400 lifetime max
Reconstructive Surgery
Breast TRAM Flap $2,000
Breast reconstruction $500
Breast Symmetry $250
Facial reconstruction $500
Second Surgical Opinion $200/surgery procedure
Skin Cancer
Biopsy Only: $100
Reconstructive Surgery: $250
Excision of a skin cancer: $375
Excision of a skin cancer with flap or graft: $600
Surgical Benefit Schedule amount up to $4,125
Transportation/Companion Transportation - Benefit is paid if you have to travel
more than 50 miles one way to receive treatment for internal cancer.
$0.50/mile up to $1,000 per round trip/equal benefit
for companion
Waiver of Premium - If you become disabled due to cancer that is diagnosed after
the employee's effective date, and you remain disabled for 90 days, we will waive the
premium due after such 90 days for as long as you remain disabled.
Included
UNDERSTANDING YOUR BENEFITS :
• Cancer – Cancer means you have been diagnosed with a disease manifested by the presence of a malignant tumor
characterized by the uncontrolled growth and spread of malignant cells in any part of the body. This includes leukemia,
Hodgkin's disease, lymphoma, sarcoma, malignant tumors and melanoma. Cancer includes carcinomas in-situ (in the natural or
normal place, confined to the site of origin, without having invaded neighboring tissue). Pre-malignant conditions or conditions
with malignant potential, such as myelodyplastic and myeloproliferative disorders, carcinoid, leukoplakia, hyperplasia, actinic
keratosis, polycythemia, and nonmalignant melanoma, moles or similar diseases or lesions will not be considered cancer.
• Experimental Treatment – Benefits will be paid for experimental treatment prescribed by a doctor for the purpose of
destroying or changing abnormal tissue. All treatment must be NCI listed as viable experimental treatment for Internal
Cancer.
25

Flexible Spending AccountsFlexible Spending Accounts (FSAs) are
designed to save you money on your
taxes. They work in a similar way to a
savings account. Each pay period, funds
are deducted from your pay on a pre-tax
basis and are deposited to your Health
Care and/or Dependent Care FSA. You
then use your funds to pay for eligible
health care or dependent care expenses.
Please note, in order to receive
employer contributions to an HSA
account, or contribute yourself, you
cannot participate in the Health Care
FSA.
Account Type Eligible ExpensesAnnual Contribution
LimitsBenefit
Health Care FSA
Most medical, dental and vision care expenses that are not covered by your health plan (such as copayments, coinsurance, deductibles, eyeglasses and doctor-prescribed over the counter medications)
Minimum contribution-$500Maximum contribution-$2,550 per year
Saves on eligible expenses not covered by insurance; reduces your taxable income
Dependent Care FSA
Dependent care expenses (such as day care, after school programs or elder care programs) so you and your spouse can work or attend school full-time
Maximum contribution is $5,000 per year ($2,500 if married and filing separate tax returns)
Reduces your taxable income
Important Information About FSAs
Your FSA elections will be in effect
from January 1st through December
31st. Claims incurred between January
1st and March 31st may be submitted
under the previous plan year. If you do
not use all of the funds in your FSA by
then, you forfeit any unused funds.
Please plan your contributions
carefully. Note that FSA elections do
not automatically continue from year
to year; you must actively enroll each
year.
The Advantages of an FSA
With an FSA, the money you
contribute is never taxed—not when
you put it in
the account, not when you are
reimbursed with the funds from the
account, and not when you file your
income tax return at the end of the
year.
Save on Your Taxes
Here is an example of how much you
might save when you use the FSAs to
pay for your predictable health care
and dependent care expenses.
With FSA Without FSA
Your taxable income $50,000 $50,000
Pre-tax contribution to Health Care and Dependent Care FSA $2,000 $0
Federal and Social Security taxes* $11,701 $12,355
After-tax dollars spent on eligible expenses $0 $2,000
Spendable income after expenses $36,299 $35,645
Tax savings with the Medical and Dependent Care FSA $654
*This is an example only, and may not reflect your actual experience. It assumes a 25% federal income tax rate marginal rate and a 7.7% FICA marginal rate. State and local taxes vary, and are not included in this example. However, you will also save on any state and local taxes as well.
26

FSA/HSA Eligible and Non-Eligible Expenses
FSA/HSA Eligible Health Care Expenses Please note that this list is not intended to be comprehensive tax advice. For more detailed
information, please consult IRS Publication 502 or see your tax advisor.
Acupuncture Psychiatric care, psychologists, Alcoholism treatment Home health and/or hospice care psychotherapists, counselors
Hospital services Radial keratotomy Ambulance (ground or air) Insulin Schools (special, relief, or handicapped)
Laboratory fees Blind services and equipment LASIK/LASEK eye surgery Car controls for handicapped* Medical alert (bracelet, necklace) Surgical fees Chiropractor services Television or telephone for the hearing
Nursing services impaired Contact lenses Obstetrical expenses Therapy treatments* Crutches, wheelchairs, walkers Occlusal guards
medical care; limits apply) aid animal & care, lip reading expenses, Optometrists
Vitamins* Dental treatment Orthopedic services Weight loss programs* Dentures Osteopaths X-rays
Oxygen/oxygen equipment ailment or
Doctor’s fees Physical exams (except for employment-
related physicals) Physical therapy
Important Notice About Over-the-Counter (OTC) Medications
OTC medications require a doctor’s prescription to be eligible for FSA/HSA reimbursement. For that reason, OTC
medications cannot be purchased using the mySourceCard® unless dispensed by a pharmacy the same as
a standard prescription (with an Rx number). If a manual claim is submitted for purchase of an OTC medication,
both a copy of the prescription and the purchase receipt must be included to receive reimbursement.
Non-medicated OTC products (diabetes test strips, saline solution, bandages, etc.) do not require a prescription.
You can use either the mySourceCard® to purchase these items or submit the purchase receipt for reimbursement
Under PPACA (health reform
law), the Maximum
Annual Election is capped at $2,600 per employee.
FSA/HSA Eligible OTC Medications and Products
COPY OF PRESCRIPTION AS WELL AS DETAILED ELIGIBLE FOR REIMBURSEMENT WITH RECEIPT REQUIRED FOR REIMBURSEMENT: suppositories, etc.) DETAILED RECEIPT ONLY (NO PRESCRIPTION
Eczema & psoriasis remedies REQUIRED): Eye drops, ear drops, nasal sprays Breast pumps for nursing mothers
syrups, cough drops, nasal sprays, medicated First aid kits Braces & supports
rubs, etc.) Hydrogen peroxide, rubbing alcohol CPAP equipment & supplies Antacids & acid controllers (tablets, liquids,
capsules) Medicated bandaids & dressings Durable medical equipment (power chairs,
ointments walkers, wheelchairs, etc.)
Pain relievers (aspirin, ibuprofen, kits, thermometers, blood pressure acetaminophen, naproxen, etc.) monitors, etc.)
Non-medicated bandaids, rolled bandages & Wart removal remedies, corn patches dressings
Baby care (diaper rash ointments, teething gel, Reading glasses
All OTC items listed are examples
2018 FORM FURNISHED BY PENSION CONCEPTS AND ADMINISTRATION, INC.
27

WorkLifeMatters
Your Confidential Employee Assistance Program – Helping find balance between work and homelife.
WorkLifeMatters provides guidance for personal issues that you might be facing and information about other concerns thataffect your life, whether it’s a life event or on a day-to-day basis.
• Unlimited free telephonic consultation with an EAP counselor available 24/7 at 800-386-7055
• Referrals to local counselors — up to three sessions free of charge
• State-of-the-art website featuring over 3,400 helpful articles on topics like wellness, training courses, and a
legal and financial center
WorkLifeMatters can offer help with:
Education Dependent Care & Care Giving Legal and financial▪ Admissions testing & procedures ▪ Adoption Assistance ▪ Basic tax planning▪ Adult re-entry programs ▪ Before/after school programs ▪ Credit & collections▪ College Planning ▪ Day Care/Elder Care ▪ Debt Counseling▪ Financial aid resources ▪ Elder care ▪ Home buying▪ Finding a pre-school ▪ In-home services ▪ Immigration
Lifestyle & Fitness Management Working Smarter▪ Anxiety & depression ▪ Career development▪ Divorce & separation ▪ Effective managing▪ Drugs & alcohol ▪ Relocation
For more information about WorkLifeMatters, go to www.ibhworklife.com; User Name: Matters; Password: wlm70101
WorkLifeMatters Program services are provided by Integrated Behavioral Health, Inc., and its contractors. Guardian does not provide any part of WorkLifeMattersProgram services. Guardian is not responsible or liable for care or advice given by any provider or resource under the program. This information is for illustrativepurposes only. It is not a contract. Only the Administration Agreement can provide the actual terms, services, limitations and exclusions. Guardian and IBH reservethe right to discontinue the WorkLifeMatters Program at any time without notice. Legal services provided through WorkLifeMatters will not be provided in connectionwith or preparation for any action against Guardian, IBH, or your employer.
28

WillPrep Services
Special bonus for participants in voluntary life plan
Your employer has worked with Guardian to make WillPrep Services available to eligible members with Voluntary Lifeplans. Keeping an up-to-date will is essential to ensuring that your assets are distributed as you intended, no matter thesize of your estate. You may be avoiding creating a will because you believe you can’t afford the time or legal expense.Now you can with WillPrep Services.
WillPrep Services offer support and guidance to help you properly prepare the documents necessary to preserve yourfamily’s financial security. WillPrep has a range of services including online planning documents, a resource library andaccess to professionals* to help with issues related to:
Advanced Health CareDirectives
Financial Power of Attorney Wills and Living Wills
Estate Taxes Guardianship andConservatorship
Resource Library
Executors & Probate Healthcare Power of Attorney Trusts
For more information about WillPrep Services, go to www.ibhwillprep.com; User name: WillPrep; Password: GLIC09or call 1-877-433-6789
*The Option of an attorney prepared will is available for a small fee.WillPrep Services are provided by Integrated Behavioral Health, Inc., and its contractors. The Guardian Life Insurance Company of America(Guardian) does not provide any part of WillPrep Services. Guardian is not responsible or liable for care or advice given by any provider or resourceunder the program. This information is for illustrative purposes only. It is not a contract. Only the Administration Agreement can provide the actualterms, services, limitations and exclusions. Guardian and IBH reserve the right to discontinue the WillPrep Services at any time without notice. Legalservices will not be provided in connection with or preparation for any action against Guardian, IBH, or your employer.
29

2018 WELLNESS PROGRAM
LIVE BETTER TODAYThe Wellness Revolution will reward you for making healthy choices. Get the motivation you need to improve your health, and the education and support to make wellness a lifestyle.
This is your chance to reach personal health goals and learn what improvements you can make to avoid future health problems. This document explains how you can take control of your health today. Have fun!
Who can participate in the program?Beginning 1/1/18, all health plan‐covered employees are eligible to log on to www.PRMCWellness.com to start the program.
Is my health information confidential?All programs are confidential and in compliance with the Health Insurance Portability and Accountability Act (HIPAA). Any information shared with the Viverae® team will not be disclosed, except in accordance with HIPAA laws. Your Protected Health Information (PHI) will not be shared with your employer.
HOW TO REGISTERStep 1
» Visit www.PRMCWellness.com
» Click New User Registration
» Enter your last name and date of birth (DOB)
» Enter your identifier: SNN
» Enter the registration code: petersonrmc
Step 2
» Create a user name (5 – 25 characters)
» Create a password (8 – 12 characters) using letters (upperand/or lowercase), numerals and/or special characters (such as@$%&#)
» Select a security question and answer, then click Save
TEXT MESSAGE REMINDERSwww.PRMCWellness.com can text you healthy reminders:
» Complete Member Health Assessment (MHA) and BiometricScreening
» Screening appointment date and time
» Important challenge sign‐up dates and Targeted Programdeadlines
Note: Opt‐in on www.PRMCWellness.com to receive text message reminders. Standard text messaging
rates apply.
GETTING STARTED
www.PRMCWellness.com
Start at this site to learn where your health stands. Take action on health risks to develop a healthy lifestyle.
Member Health Assessment (MHA)The MHA consists of questions about specific lifestyle habits. Your MHA responses are analyzed to show your risk level and generate a Health Index. You can complete your MHA at www.PRMCWellness.com
Biometric ScreeningBiometric screenings provide vital information about your overall health, including cholesterol (total, LDL, and HDL), triglycerides, cardiac risk, glucose, blood pressure, height, weight, Body Mass Index (BMI), and waist measurement. If you are unable to attend a Biometric Screening event, you may fulfill the screening requirement by visiting your physician.
Contact the Viverae Health Center at 888‐VIVERAE (848‐3723) with any questions or concerns about the Viverae.
Preventive CareSelf‐report completion of 3 preventive care exams at www.PRMCWellness.com. Exams must be dated between 11/19/17 – 11/17/18.
DOWNLOAD THE VIVERAE APP
Get ready to experience wellness on the go with the new Viverae wellness mobile app! Now, you can take the wellness experience with you no matter the time or place.
Download the Viverae mobile app in the Apple Store (iOS 9 and higher) or in the Google play Store (4.4 or higher).
30

EARNING POINTS
Earn points for completing program activities in the Wellness Revolution and earn rewards. Manage all your program activities and log points at www.PRMCWellness.com.
Complete your MHA, biometric screening, preventive care and earn a total of 300 points by 11/17/18 to earn your cash reward.
ADDITIONAL ACTIVITIES
For more points or support in your wellness program, you have plenty of available resources. Participating in Wellness Revolution allows you to do the following:
» Register for quarterly Employer Challenges PRMC is hosting
» Take an Online Course or join a Targeted Program to addressspecific lifestyle concerns
» Connect your health app or device and track your progress
» Participate in or start a Peer Challenge
CHALLENGES
Challenges let you earn extra points in the program while managing risk factors or lifestyle changes.
Sign up for Employer and Peer Challenges. Log activity and view your status. View challenge details (past and present) and sign up for new challenges from the Challenges section.
FREQUENTLY ASKED QUESTIONS
What is the Viverae Health Center?
The Viverae Health Center is a health and wellness resource that is available for Viverae members. It is staffed by a variety of highly trained customer care representatives and health professionals, including clinicians, exercise specialists, and registered nurses and dietitians.
How do I contact the Viverae Health Center?
There are two ways to contact the Health Center: via secure email message or by phone.
» You can send a secure message to your coach by selecting theInbox link at the top of the screen
» To call toll‐free, please dial 888‐VIVERAE (848‐3723)
The Viverae Health Center hours are as follows:
» Monday – Thursday: 7 a.m. – 7:30 p.m. CT
» Friday: 7 a.m. – 6 p.m. CT
» Saturday – Sunday: Closed
» Closed holidays
2018 WELLNESS REVOLUTIONASSESSMENTS (REQUIRED) POINT VALUE
Member Health Assessment (MHA) 25
Biometric Screening 25
PREVENTIVE CARE COMPLIANCE (REQUIRED) POINT VALUE
Preventive Care Compliance (Complete 3) 25
TOBACCO POINT VALUE
TobaccoTobacco‐Free: Negative Online Attestation 25 each / 25
maxTargeted Program – Breaking Free from Tobacco
HEALTH METRICS / TARGETED ACTIONS POINT VALUE
Body Mass
Index /
Waist
Measurement
BMI: Less than 25.0
50
OR Waist Measurement:
Less than 35 inches (Females)
Less than 40 inches (Males)
OR Any Improvement (from 2016 Biometrics)
Action: Targeted Program – Reaching Your
Healthy Weight
Total
Cholesterol
Less than 200 mg/dL
50OR Any Improvement (from 2016 Biometrics)
Action: Online Course – Lipids: Managing Your
Risk
Blood Pressure
Systolic: Less than 120 mmHG AND
Diastolic: Less than 80 mmHG
50OR Any Improvement (from 2016 Biometrics)
Action: Targeted Program – Tackling Your
Stress
Glucose
Fasting: Less than 100 mg/dL
50
OR Non‐Fasting or Unknown: Less than 140
mg/dL
OR Any Improvement (from 2016 Biometrics)
Action: Online Course – Healthy Eating: Mindful
& Portion Control
ACTIVITIES – Q1 (1/1/18 – 3/31/18) (Complete 2 of the 3) POINT VALUE
(Option 1) Employer Challenge: (Weight Management) WEIGH 2
WIN
(Option 2) 250,000 Steps (Apps & Devices)
(Option 3) 250,000 Steps (Apps & Devices)
25 each / 50
max
ACTIVITIES – Q2 (4/1/18 – 6/30/18) (Complete 2 of the 3) POINT VALUE
(Option 1) Employer Challenge – (Nutrition Challenge) HYDR8TE
(Option 2) 250,000 Steps (Apps & Devices)
(Option 3) 250,000 Steps (Apps & Devices)
25 each / 50
max
ACTIVITIES – Q3 (7/1/18 – 9/30/18) (Complete 2 of the 3) POINT VALUE
(Option 1) Employer Challenge: (Nutrition Challenge) 5‐ A –DAY
(Option 2) 250,000 Steps (Apps & Devices)
(Option 3) 250,000 Steps (Apps & Devices)
25 each / 50
max
ACTIVITIES – Q4 (10/1/18 – 11/17/18) (Complete 2 of the 3) POINT VALUE
(Option 1) Employer Challenge: (Stress Management Challenge)
TAKE 5
(Option 2) 250,000 Steps (Apps & Devices)
(Option 3) 250,000 Steps (Apps & Devices)
25 each / 50
max
PROGRAM GOAL 300 POINTS
31

Sid Peterson Memorial Hospital 401(k) Savings and Profit Sharing Plan
J O I N I N G T H E P L A N
Who is eligible to join the plan?
The following employees may join the plan - Non-Union to make any employee contributions except: Employees covered by a collective bargaining agreement Non-resident aliens with no U.S. earned income Leased employees Peterson Med. excluded from Match & ERYou need to be age 18 and work for at least 90 day(s) to elect any employee contributions.
The following employees may join the plan - Non-Union to receive any employer contributions except: Employees covered by a collective bargaining agreement Non-resident aliens with no U.S. earned income Leased employees Peterson Med. excluded from Match & ERYou need to be age 18 and work for at least 12 month(s) to receive any employer contributions.
When will I join the plan?
Your participation in the plan will begin when you reach the service levels required by the plan. Your payrolldeductions will start as soon as possible after your entry date.
M A K I N G C O N T R I B U T I O N S
What is my “pay” under the plan?
Your plan contains a definition of “pay” for calculating contribution amounts. Your plan may use differentdefinitions of “pay” for other purposes. To learn more about what types of compensation are used by the plan,read your Summary Plan Description.
These are the highlights of your plan. For additional information, read your Summary Plan Description or ask to see the plan document. If any information here conflicts with the terms of your plan, the plan language governs.
32

PLAN HIGHLIGHTS
How much may I contribute to the plan?
The contribution(s) that you may make to the plan are displayed below:
DEFERRED SALARY CONTRIBUTIONS
Through payroll deduction you will make Deferred Salary contributions of 2.00% of your pay. You may changethis percentage and make Deferred Salary contributions up to the maximum amount allowed by law. Thesecontributions consist of pre-tax dollars and earnings on these contributions grow tax-deferred. If you do not wantto make Deferred Salary contributions, you may decline enrollment by completing a Participation form.
You may increase or decrease the amount of your contributions quarterly. You may stop your contributions anytime.
The Internal Revenue Service (IRS) limits the total amount of pre-tax contributions you may make each calendaryear. For 2017, this limit is $18,000. However, if you reach age 50 anytime during the calendar year or are over50, you may make additional pre-tax contributions above and beyond normal plan and legal limits. For 2017, youcan make up to $6,000 in additional contributions.
ROLLOVER CONTRIBUTIONS
You may be able to roll over your existing retirement savings into this plan. Consolidating your retirementsavings can help you continue benefiting from tax-deferred growth - despite any disruptions that may occurduring your working life. Maintaining one retirement account also makes it easy for you to track your retirementsavings. To learn more about making Rollover contributions to this plan, call 1-888-526-6905 and a RetirementSpecialist will assist you.
Will the company contribute?
The company contribution(s) that you may receive are displayed below:
COMPANY MATCH CONTRIBUTIONS
Each year, your company may make Company Match contributions. These contributions will grow tax-deferred.Read your Summary Plan Description for more details.
PROFIT SHARING CONTRIBUTIONS
Each year, your company decides whether to make a Profit Sharing contribution. Your share of the contribution isbased on your pay compared to the pay of all plan participants. These contributions grow tax-deferred.
Your Profit Sharing contributions will be calculated based on your pay for the entire plan year. You receiveProfit Sharing contributions if you work over 1,000 hours in a plan year and are employed on the last day of the
33

PLAN HIGHLIGHTS
plan year. Participants who retire, die or become disabled during the plan year also receive Profit Sharingcontributions.
M A N A G I N G Y O U R A C C O U N T
How will I know how much is in my account?
You will receive a personal statement periodically. You may also use your Personal Identification Number (PIN)to access your account by calling 1-800-74FLASHSM (35274) or accessing The JourneySM atwww.retiresmart.com, 24 hours a day, 365 days a year. You can check your account balance, secure investmentperformance information, obtain loan information and apply for a loan, make investment changes, or requestadditional information about the plan.
How are my contributions invested?
You give investment directions for all of your account, choosing from the investment options your plan provides.
Until you make an investment selection, all of your contributions will be invested into a retirement date basedinvestment option determined by your date of birth and a projected retirement age of 65. You may giveinvestment directions for your account, choosing from the investment options your plan provides. You maychange your investment choices daily. You may transfer your existing balance to other investment options dailysubject to certain restrictions.
To make choosing your investment options easier, your contributions are placed in one or more groups as follows:
Employee Source Group – Deferred Salary
Employer Source Group – Company Match, Profit Sharing
If you call 1-800-74FLASHSM (35274) or access The JourneySM at www.retiresmart.com, these group names arereferenced.
Sid Peterson Memorial Hospital 401(k) Savings and Profit Sharing Plan is intended to constitute an ERISA§404(c) plan. This means that you "exercise control" over the investments in your account. From the investmentoptions available under your plan, you can choose which investments to put your money in now and you canswitch into different investments as your needs change. Complying with ERISA §404(c) may relieve planfiduciaries of liability for any investment losses to your account that are the result of your investment choices.
As a plan participant, you are entitled to request certain information about your plan’s investments, including: theannual operating expenses of each investment; financial statements, reports, or other materials relating to theplan’s investments; a list of assets contained in each investment portfolio; the value of those assets and fund unitsor shares; and the past and current performance of each investment.
34

PLAN HIGHLIGHTS
How does vesting (ownership) apply to my account?
Plans set a “vesting schedule” to determine what percentage of ownership you can apply to your account at specificpoints in time. You are always 100% vested in any Deferred Salary contributions, plus earnings. Your plan’s vestingschedule applies to the following contributions, plus earnings:Company Match, Profit Sharing
Yrs. ofService
VestedPct.
0 0%2 20%3 40%4 80%5 100%
Your years of service for vesting purposes begin on your date of hire.
If you die, become disabled or reach normal retirement age, you will become 100% vested in all contributions your company makes to the plan, plus earnings. T A K I N G A D I S T R I B U T I O N : When may I withdraw money from the plan? The plan is designed to help you save for retirement. So, the IRS has placed restrictions on when you may withdraw money from the plan. You may withdraw money from your account at: Termination
You may receive your vested account balance. Additional requirements may apply.
Normal Retirement
Age 65
Disability Retirement: Disability is determined based on the company’s personnel policy. Death
Your account balance will be paid to your designated beneficiaryYour plan may allow withdrawals of certain contributions and earnings while you are employed. Your Summary Plan Description provides more details about distributions, including important tax information and information on the forms of benefit your plan offers.May I take out loans from the plan?You may borrow money from the plan by taking up to one loan. Your maximum loan balance may not exceed the lesser of: one half of your vested account balance or $50,000.00. You may not initiate a loan for less than $1,000.00. Your loan is secured by your remaining account balance.You must repay all loans within 5 years. The interest rate on your loan will be the prime rate +2.00%. You pay back the principal and interest directly to your account by establishing an Automated Clearing House (“ACH”) Agreement with your bank. The ACH remittance frequency is required monthly, and you may elect to have the debit to your account occur on either the 3rd of the month, or the 15th of the month.If you don’t repay your loan, the IRS considers the unpaid amount to be a taxable payment made to you.
35

Important InformationHIPAA PRIVACY RIGHTS
The Health Insurance Portability and Accountability Act (HIPAA) provides you certain rights to privacy concerning your health information. The regulations designate certain types of information as Protected Health Information (PHI).
Health care providers, medical processionals and health plans, including Peterson health plan representatives, are restricted in their use of PHI to purposes of treatment, payment, and health care operations and as required by national public health activities. Written authorization is required to use or disclose your PHI pertaining to your medical, dental, prescription drug, employee assistance program and health care operations and as required by national public health activities. Written authorization is required to sue or disclose your PHI pertaining to your medical, dental, prescription drug, employee assistance program and health care spending accounts outside of these purposes.
You may receive a form requesting your authorization to use your PHI for another purpose. Should you grant this authorization, your PHI is still protected from use and disclosure by any party other than the one(s) to whom you grant written authorization, and from use and disclosure by authorized parties for any purpose other than the one you specifically authorized.
PROTECTED HEALTH INFORMATION
(PHI)PHI includes information that could be used to identify you as an individual in electronic, printed or spoken forms that relates to (1) past, present or future health, physical or mental condition, (2) provision of health care, or (3) past, present or future payment for the provision of health care.
HIPAA gives you the right to: Receive notice of the health plan’s uses and disclosures of your PHI, your privacy rights and the health plan’s legal duties regarding your PHI; Obtain access to your own PHI; Amend your PHI; Receive an accounting of non-exempt uses and disclosures of your PHI over the past six years upon request; and Received communications by an alternative means or at an alternate location upon request. For information regarding HIPAA privacy rules, refer to your Summary Plan Description.
THE WOMEN’S HEALTH AND CANCER RIGHTS ACT
Do you know that your plan, as required by the Women’s Health and Cancer Rights Act of 1998, provides benefits for mastectomy –related services including all stages of reconstruction and surgery to achieve symmetry between the breast, prosthesis, and complications resulting from a mastectomy including lymphedema? Contact the Human Resources Department for more information.
If you have had or are going to have a mastectomy, you may be entitled to certain benefits under the Women’s Health and Cancer Rights Act of 1998 (WHCRA). For individuals receiving mastectomy-related benefits, coverage will be provided in a manner determined in consultation with the attending physician and the patient for:
• All stages of reconstructions of the breast on whichthe mastectomy was performed;
• Surgery and reconstruction of the other breast toproduce a symmetrical appearance;
• Prostheses; and• Treatment of physical complications of the
mastectomy, including lymphedema.
These benefits will be provided subject to the same deductibles and co-insurance applicable to other medical and surgical benefits provided under the Peterson Health Plan.
36

Important InformationNEWBORN AND MOTHER’S HEALTH
PROTECTION ACT
Group health plans and health insurance issuers generally may not, under Federal law, restrict benefits for any hospital length of stay in connection with childbirth for the mother or newborn child to less than 48 hours following a vaginal delivery, or less than 96 hours following a cesarean section. However, Federal law generally does not prohibit the mother’s or newborn’s attending provider, after consulting with the mother, from discharging the mother or her newborn earlier than 48 hours (or 96 hours as applicable). In any case, plans and issuers may not, under Federal law, require that a provider obtain authorization from the plan or the insurance issuer for prescribing a length of stay not in excess of 48 hours (or 96 hours).
PATIENT PROTECTION
Peterson generally allows the designation of a primary care provider. You have the right to designate any primary care provider who participates in our network and who is available to accept you or your family members. For children, you may designate a pediatrician as the primary care provider.
You do not need prior authorization from Peterson or from any other person (including a primary care provider) in order to obtain access to obstetrical or gynecological care from a health care professional in our network who specializes in obstetrics or gynecology. The health care professional, however, maybe required to comply with certain procedures, including obtaining prior authorization for certain services, following a pre-approved treatment plan or procedures for making referrals.
For information on how to select a primary care provider or for a list of participating primary care providers or health care professionals who specialize in obstetrics or gynecology, contact the Human Resources Department.
HIPAA SPECIAL ENROLLMENT RIGHTS
Loss of Other Coverage – If you are declining enrollment for yourself and/or dependents (including your spouse) because of other health insurance or group health plan coverage, you may be able to enroll yourself and/or your dependents in this plan if you or your dependents’ in this plan if you or your dependents
lose eligibility for that other coverage or if the employer stops contributing towards your or your dependents’ other coverage. To be eligible for this special enrollment opportunity, you must request enrollment within 30 days after your other coverage ends or after the employer stops contributing towards the other coverage.
New Dependent as a Result of Marriage, Birth, Adoption, or Placement for Adoption – If you have a new dependent as a result of marriage, birth, adoption, or placement for adoption, you may be able to enroll your dependents. To be eligible for this special enrollment opportunity, you must request enrollment within 30 days after the marriage, birth, adoption or placement for adoption. Contact your plan administrator to request a special enrollment.
MAKING ENROLLMENT CHANGES DURING
THE YEAR:
In most cases, your benefit elections will remain in
effect for the entire plan year (January 1st, 2018 - December 31st, 2018) During the annual enrollment period, you have the opportunity to review your benefit elections and make changes for the coming year.
• You may only make changes to your elections duringthe year if you have one of the following statuschanges:
• Marriage, divorce or legal separation (if your staterecognizes legal separation);
• Gain or loss of an eligible dependent for reasonssuch as birth, adoption, court order, disability, death;reaching the dependent child age limit; or
• Significant changes in employment or employer –sponsored benefit coverage that affect you or yourspouse’s benefit eligibility.
• Your benefit change must be consistent with yourchange in family status.
IRS regulations require that for enrollment due to the qualifying events above, change forms must be submitted with in 30 days of that qualifying event. Contact your Human Resources office for information on completing these forms.
37

38

Premium Assistance Under Medicaid and the Children’s Health Insurance Program (CHIP)
If you or your children are eligible for Medicaid or CHIP and you’re eligible for health coverage from your employer, your state may have a premium assistance program that can help pay for coverage, using funds from their Medicaid or CHIP programs. If you or your children aren’t eligible for Medicaid or CHIP, you won’t be eligible for these premium assistance programs but you may be able to buy individual insurance coverage through the Health Insurance Marketplace. For more information, visit www.healthcare.gov.
If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, contact your State Medicaid or CHIP office to find out if premium assistance is available.
If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible
for either of these programs, contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, ask your state if it has a program that might help you pay the premiums for an employer-sponsored plan.
If you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must allow you to enroll in your employer plan if you aren’t already enrolled. This is called a “special enrollment” opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, contact the Department of Labor at www.askebsa.dol.gov or call 1-866-444-EBSA (3272).
If you live in one of the following states, you may be eligible for assistance paying your employer health plan premiums. The following list of states is current as of July 31, 2016. Contact your State for more information on eligibility –
ALABAMA – Medicaid FLORIDA – Medicaid
Website: http://myalhipp.com/ Phone: 1-855-692-5447
Website: http://flmedicaidtplrecovery.com/hipp/ Phone: 1-877-357-3268
ALASKA – Medicaid GEORGIA – Medicaid
The AK Health Insurance Premium Payment Program Website: http://myakhipp.com/ Phone: 1-866-251-4861 Email: [email protected] Medicaid Eligibility: http://dhss.alaska.gov/dpa/Pages/medicaid/default.aspx
Website: http://dch.georgia.gov/medicaid - Click on Health Insurance Premium Payment (HIPP)Phone: 404-656-4507
ARKANSAS – Medicaid INDIANA – Medicaid
Website: http://myarhipp.com/ Phone: 1-855-MyARHIPP (855-692-7447)
Healthy Indiana Plan for low-income adults 19-64 Website: http://www.hip.in.gov Phone: 1-877-438-4479 All other Medicaid Website: http://www.indianamedicaid.com Phone 1-800-403-0864
COLORADO – Medicaid IOWA – Medicaid
Medicaid Website: http://www.colorado.gov/hcpf Medicaid Customer Contact Center: 1-800-221-3943
Website: http://www.dhs.state.ia.us/hipp/ Phone: 1-888-346-9562
KANSAS – Medicaid NEW HAMPSHIRE – Medicaid
Website: http://www.kdheks.gov/hcf/ Phone: 1-785-296-3512
Website: http://www.dhhs.nh.gov/oii/documents/hippapp.pdf Phone: 603-271-5218
KENTUCKY – Medicaid NEW JERSEY – Medicaid and CHIP
Website: http://chfs.ky.gov/dms/default.htm Phone: 1-800-635-2570
Medicaid Website: http://www.state.nj.us/humanservices/ dmahs/clients/medicaid/ Medicaid Phone: 609-631-2392 CHIP Website: http://www.njfamilycare.org/index.html CHIP Phone: 1-800-701-0710
LOUISIANA – Medicaid NEW YORK – Medicaid
Website: http://dhh.louisiana.gov/index.cfm/subhome/1/n/331 Phone: 1-888-695-2447
Website: http://www.nyhealth.gov/health_care/medicaid/ Phone: 1-800-541-2831
MAINE – Medicaid NORTH CAROLINA – Medicaid
Website: http://www.maine.gov/dhhs/ofi/public-assistance/index.html Phone: 1-800-442-6003 TTY: Maine relay 711
Website: http://www.ncdhhs.gov/dma Phone: 919-855-4100
MASSACHUSETTS – Medicaid and CHIP NORTH DAKOTA – Medicaid
Website: http://www.mass.gov/MassHealth Phone: 1-800-462-1120
Website: http://www.nd.gov/dhs/services/medicalserv/medicaid/ Phone: 1-844-854-4825
39

MINNESOTA – Medicaid OKLAHOMA – Medicaid and CHIP
Website: http://mn.gov/dhs/ma/ Phone: 1-800-657-3739
Website: http://www.insureoklahoma.org Phone: 1-888-365-3742
MISSOURI – Medicaid OREGON – Medicaid
Website: http://www.dss.mo.gov/mhd/participants/pages/hipp.htm Phone: 573-751-2005
Website: http://healthcare.oregon.gov/Pages/index.aspx http://www.oregonhealthcare.gov/index-es.html Phone: 1-800-699-9075
MONTANA – Medicaid PENNSYLVANIA – Medicaid
Website: http://dphhs.mt.gov/MontanaHealthcarePrograms/HIPP Phone: 1-800-694-3084
Website: http://www.dhs.pa.gov/hipp Phone: 1-800-692-7462
NEBRASKA – Medicaid RHODE ISLAND – Medicaid
Website: http://dhhs.ne.gov/Children_Family_Services/AccessNebraska/Pages/accessnebraska_index.aspx Phone: 1-855-632-7633
Website: http://www.eohhs.ri.gov/ Phone: 401-462-5300
NEVADA – Medicaid SOUTH CAROLINA – Medicaid
Medicaid Website: http://dwss.nv.gov/ Medicaid Phone: 1-800-992-0900
Website: http://www.scdhhs.gov Phone: 1-888-549-0820
SOUTH DAKOTA - Medicaid WASHINGTON – Medicaid
Website: http://dss.sd.gov Phone: 1-888-828-0059
Website: http://www.hca.wa.gov/free-or-low-cost-health-care/program-administration/premium-payment-program Phone: 1-800-562-3022 ext. 15473
TEXAS – Medicaid WEST VIRGINIA – Medicaid
Website: http://gethipptexas.com/ Phone: 1-800-440-0493
Website: http://www.dhhr.wv.gov/bms/Medicaid%20Expansion/Pages/default.aspx Phone: 1-877-598-5820, HMS Third Party Liability
UTAH – Medicaid and CHIP WISCONSIN – Medicaid and CHIP
Website: Medicaid: http://health.utah.gov/medicaid CHIP: http://health.utah.gov/chip Phone: 1-877-543-7669
Website: https://www.dhs.wisconsin.gov/publications/p1/p10095.pdf Phone: 1-800-362-3002
VERMONT– Medicaid WYOMING – Medicaid
Website: http://www.greenmountaincare.org/ Phone: 1-800-250-8427
Website: https://wyequalitycare.acs-inc.com/ Phone: 307-777-7531
VIRGINIA – Medicaid and CHIP
Medicaid Website: http://www.coverva.org/programs_premium_assistance.cfm Medicaid Phone: 1-800-432-5924 CHIP Website: http://www.coverva.org/programs_premium_assistance.cfm CHIP Phone: 1-855-242-8282
To see if any other states have added a premium assistance program since July 31, 2016, or for more information on special enrollment rights, contact either:
U.S. Department of Labor U.S. Department of Health and Human Services Employee Benefits Security Administration Centers for Medicare & Medicaid Services www.dol.gov/ebsa www.cms.hhs.gov1-866-444-EBSA (3272) 1-877-267-2323, Menu Option 4, Ext. 61565
Paperwork Reduction Act Statement
According to the Paperwork Reduction Act of 1995 (Pub. L. 104-13) (PRA), no persons are required to respond to a collection of information unless such collection displays a valid Office of Management and Budget (OMB) control number. The Department notes that a Federal agency cannot conduct or sponsor a collection of information unless it is approved by OMB under the PRA, and displays a currently valid OMB control number, and the public is not required to respond to a collection of information unless it displays a currently valid OMB control number. See 44 U.S.C. 3507. Also, notwithstanding any other provisions of law, no person shall be subject to penalty for failing to comply with a collection of information if the collection of information does not display a currently valid OMB control number. See 44 U.S.C. 3512.
The public reporting burden for this collection of information is estimated to average approximately seven minutes per respondent. Interested parties are encouraged to send comments regarding the burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to the U.S. Department of Labor, Employee Benefits Security Administration, Office of Policy and Research, Attention: PRA Clearance Officer, 200 Constitution Avenue, N.W., Room N-5718, Washington, DC 20210 or email [email protected] and reference the OMB Control Number 1210-0137.
OMB Control Number 1210-0137 (expires 12/31/2019)
40

















