This continuing medical education activity is jointly provided by the American College of Obstetricians and Gynecologists. April 20-22, 2018 | Omni Grove Park Inn Resort | Asheville, NC North Carolina Obstetrical and Gynecological Society and NC Section of ACOG 2018 ANNUAL MEETING SUNDAY PRESENTATIONS
Transcript
This continuing medical education activity is jointly provided by the American College of Obstetricians and Gynecologists.
April 20-22, 2018 | Omni Grove Park Inn Resort | Asheville, NC
North Carolina Obstetrical and Gynecological Society and NC Section of ACOG
2018 ANNUAL MEETING
SUNDAY
PRESENTATIONS
Immediate Postpartum LARC: Inserting IUDs as Soon as the
Placenta is OutMatthew Zerden, MD, MPH, FACOG
OBGYN Hospitalist, WakeMed Health & Hospitals
Assistant Clinical Professor, UNC School of Medicine, OBGYN Dep’t
Associate Affiliate Medical Director, Planned Parenthood South Atlantic
1
Disclosures• I am a Trainer for the ACOG Immediate Postpartum LARC Program• I will be speaking about off‐label, but evidence‐supported, use ofintrauterine devices in the immediate postpartum• Currently not supported by FDA labeling
• I will be using brand names as I discuss the various types ofLevonorgestrel‐Intrauterine Systems (LNG‐IUS)
2
Objectives
• Counseling framework: shared decision‐making & reproductive justice• Impact of unintended pregnancy in the postpartum period• Unmet need for postpartum contraception• Understand and practice immediate postpartum (IPP) IUD insertion techniques
• Follow up instructions for postpartum IUDs
3
Shared decision‐making & reproductive justice
• “The economic, social and political power and resources to make healthy decisions about our bodies, sexuality and reproduction for ourselves, our families and our communities”• http://strongfamiliesmovement.org/assets/docs/ACRJ-A-New-
Vision.pdf
• The right to have children, the right to not have children, the right to raise children with dignity and in safety
4
Forced Sterilizations in NC
• Eugenics Board of North Carolina (EBNC) • 1933 by NC Legislature until 1977
• Sterilization: Tool to combat poverty/ welfare• “Mentally defective or feeble‐minded”• Evidence of racial bias• Restitution, 2012:
• $50,000 payments to verified North Carolina eugenics victims
(Price & Darity, 2010)
5
Forced Sterilizations in NC
6
Reproductive justice
• Evidence-based contraception counseling• Free of coercion• Culturally-sensitive, patient-centered counseling
• Break away from the traditional, provider informing the patient• Use of videos and apps
• Fulfilling sterilization requests• Evidenced- based counseling on lactational amenorrhea • Offering LARC: all evidence-based times of the postpartum• Ensuring access to LARC removal
7
Impact of unintended pregnancy in the postpartum
8
Unintended pregnancy
9
Pregnancy spacing is important for healthy families
• Maternal & infant benefits of interpregnancy intervals > 18 months• Many women unaware• Providers can engage patients with knowledge & planning• ACOG Committee Opinion #666, Optimizing Postpartum Care:
• “The optimal interval between delivery and subsequent pregnancy is 18 months to 5 years”
• “The greatest risk of low birth weight and preterm birth occurs when the interconception interval is less than 6 months”
Foster 2008; Salihu 2011; Grisaru‐Granovsky 2009
10
Unmet need for PP contraception
•Why is 6 week visit too late?• Ovulation may return at 3 weeks postpartum• 50% adolescents resume intercourse < 6 wks• Poor adherence to 6 week PP appointments
• 20‐40% of high‐risk patients never attend a PP visit• Even lower in under resourced areas, further contributing to health disparities
Speroff & Mishell, 2008; Tocce et al., 2013 Attanasio 2017 ; ACOG CO #666
11
What is immediate PP LARC?
• When LARC methods are available to women in the hospital after a delivery before discharge
• ACOG, CDC, WHO, and Cochrane reviews all agree that immediate postpartum (IPP) LARC is safe and effective
• Can be an ideal time to provide LARC methods for many women
12
What is immediate PP LARC?
Definitions: timing of LARC placement1. Immediate postplacental – placement within 10 minutes of delivery of
placenta2. Immediate postpartum – placement during hospital admission for delivery3. Postpartum – placement within 6 weeks of delivery4. Interval placement – placement 6 weeks or later following delivery
• Should be offered as an effective option for postpartum contraception• Can reduce unintended pregnancy & lengthen interpregnancy intervals • Women should be counseled prenatally about IPP LARC, including:
• Advantages • Risks of expulsion • Contraindications & alternatives to allow for informed decision making
14
IPP LARC Satisfaction & Continuation Rates
• Most women like & continue their LARC method from IPP• 74% IUD placed IPP – no expulsions & IUD in place @ 1 year• 84% w/ implant placed IPP had the implant @1 year• Elective discontinuation: IUDs & implants IPP = interval placement
• ACOG Practice Bulletin #186, LARC:• Mechanism of Action: Thickening of cervical mucous• Most women ovulate normally • Diminished menstrual bleeding from local effect of LNG on endometrium
• 99.8% effective; the one‐year typical use failure rate is 0.2 per 100 women
20
Copper IUD
• ACOG Practice Bulletin #186, LARC: • Mechanism of Action: Inhibition of sperm migration and viability• Mechanism of action for pregnancy prevention occurs before fertilization• Most common adverse effects: abnormal bleeding & pain• 99.2% effective; the one‐year typical use failure rate is 0.8 per 100 women
21
Radiopaque 68 mg Etonogestrel implant
• ACOG Practice Bulletin #186, LARC• Mechanism of Action: Primary: ovulation suppression • Additional: thickening of cervical mucus & alteration of endometrial lining • Changes in bleeding patterns are common, include amenorrhea or infrequent, frequent, or prolonged bleeding
• Placed in upper arm; comparable in size to a match stick• 99.9% effective; the 1‐yr typical use failure rate is 0.05 /100 women
• Uterine anomaly or fibroids • Dependent on severity of anomaly and/or fibroids
• Active gynecologic malignancy• Allergy to any component of the IUD • Severe anemia or Wilson’s disease (for copper IUD)
• Breast cancer (for LNG IUS) • Pelvic tuberculosis
• IPP Contraindications• Peripartum chorioamnionitis, endometritis, or puerperal sepsis
• Prolonged rupture of membranes (>18 hours)
• Unresolved post‐partum hemorrhage
23
IPP LARC & Infection: Key Takeaways
• ACOG Committee Opinion #670, IPP LARC, states that: “In the absence of puerperal sepsis, IPP IUD insertion is not associated with increased risks of bleeding or infection.”
• Minimal data on IPP IUD and endometritis • ACOG has no official guidance on treating IPP IUD & endometritis• Although rare, if endometritis develops after IPP IUD insertion, treat per your usual clinical practice
24
IPP LARC & Expulsion Rates: Key Takeaway
ACOG Committee Opinion #670, IPP LARC, states that:• “Despite the higher expulsion rate of immediate postpartum IUD placement over interval placement, evidence from clinical trials and from cost‐benefit analyses strongly suggest the superiority of immediate placement in reduction of unintended pregnancy, especially for those at greatest risk of not having recommended postpartum follow‐up”
25
Expulsion, con’t
• Expulsion rates for IPP IUD insertions > interval or postabortion, vary by study.• Expulsion range: 10–27% (73‐90% of women retain the device)• Experience of provider matters • Counsel appropriately, including what to look for
• If suspected expulsion, contact provider & use a back‐up contraception
• Many barriers to interval LARC placement,• Often, pros of IPP insertion outweigh the disadvantages
26
CDC Recs: IPP LARC & Breastfeeding
27
IPP LARC & Breastfeeding, ACOG PB #186 & CO #670:
• Copper IUD lacks hormones, no effect on breastfeeding. CDC Cat 1. • LNG‐IUD: Systematic review: progestin‐only contraceptives do not appear to adversely affect … successfully initiation or continuation of breastfeeding (Phillips, 2016)• No impact on infant’s growth and development
• IPP LNG‐IUD & implant CDC / MEC Cat 2 in breastfeeding• Theoretical concerns: exogenous progesterone preventing lactogenesis, but best data suggest no effect on breastfeeding or infant outcomes
28
IPP LARC & Breastfeeding, Key points:
• ACOG CO #670, IPP LARC:“Given available evidence, women considering immediate postpartum hormonal LARC should be counseled about the theoretical risk of reduced duration of breastfeeding, but that preponderance of the evidence has not shown a negative effect on actual breastfeeding outcomes.”
The risk of perforation may be increased if LILETTA is inserted when the uterus is fixed retroverted or not completely involuted during the post‐partum period. Delay LILETTA insertion a minimum of six weeks or until involution is complete following a delivery or a second trimester abortion.
33
Package insert: ParaGard®
34
Package insert: ParaGard®
35
Insertion video
• https://cfweb.acog.org/district_ii/larc/section4.html• Video
• Minute 6
36
Post‐Placental IUD Insertion Equipment
• Two forceps: 1 for cervical traction, 1 for device placement • Kelly Placental forceps vs. Ring/Ovum forceps
• Some type of vaginal retraction• Betadine, radiopaque surgical sponge, scissors• Light source• Ultrasound recommended, not required• IUD & inserter
37
Importance of Fundal Placement
38
IUD Forceps method• Place atraumatic (ring) forceps on anterior lip of cervix • Grasp IUD w/forceps but do NOT close the ratchets • Insert forceps through cervix • Place non‐forceps hand on abdomen, palpating fundus • Move the IUD‐holding forceps to fundus • Open forceps, release IUD • Slowly remove the forceps, keeping them slightly open • Cut the strings flush with external os
• Strings will lengthen with uterine involution, may require trimming
39
IUD Manual Insertion Method
• Grasp IUD between your 2nd and 3rd fingers• Insert hand to the fundus• Use other hand to palpate the fundus abdominally to confirm
• Slowly open fingers & remove them from uterus• Cut the strings flush with the external os
• Strings will lengthen with uterine involution, may require trimming
40
IUD Inserter Method
• Follow manufacture instructions for loading the IUD • Move flange all the way back to handle • Move inserter to appropriate place in uterus
• Angle of uterus can change postpartum, especially LUS
• Ensure fundal placement • If available, use ultrasound to confirm
• Deploy IUD per standard instructions • Cut the strings flush with the external os
41
IUD Tips: post‐vaginal delivery
• Put on new sterile gloves before beginning• Retrieve the ultrasound prior to delivery, if possible• Ensure appropriate bleeding,
• Confirm uterine tone & complete placental removal via placental examination
• Use ring forceps to apply cervical traction, if needed• If difficulty reaching fundus, lower hand & adjust retractor ‐ change angle of insertion to navigate LUS
• Repair bleeding lacerations first, leave non‐bleeder to repaired after
42
Post‐placental IUD placement at the time of cesarean delivery
• Perform routine external massage and internal sweep to ensure all placental tissue is removed
• Grasp body of the IUD with forceps, hand or inserter • Strings of an LNG IUD should be trimmed to about 10 cm. Strings of the Paragard copper IUD do not need to be trimmed.
• Place the IUD at the fundus• Carefully point strings to cervix/vagina • Close the hysterotomy – take care to not incorporate the strings into the closure
43
Following up after insertion
• Many will need a follow‐up appointment to have strings trimmed• Offering, but not mandating, a string check is important
• Instruct patient:• Not to mess with strings if bothersome• If experiences usual bleeding +/‐ cramping different from lochia make an appointment for possible partial expulsion
• Inspect pads for evidence of expelled IUD• Remind her provider that an IUD placed postpartum• Notify provider of abnormal symptoms or device expulsion
44
Resource
• ACOG Video: https://cfweb.acog.org/district_ii/larc/section4.html• http://resources.jhpiego.org/• CHOICE Study counseling videos (not specific to postpartum):
• In English: https://www.youtube.com/watch?v=u9SHoy1C3tU&feature=youtu.be• Or in Spanish: https://www.youtube.com/watch?v=HgenzQUCugg&feature=youtu.be
• Bedsider: https://www.bedsider.org/methods• CDC Medical Eligibility Criteria
References• Price GN, Darity Jr WA. The economics of race and eugenic sterilization in North Carolina: 1958–1968. Economics & Human Biology. 2010 Jul 1;8(2):261‐72.
• Grisaru‐Granovsky S, Gordon ES, Haklai Z, Samueloff A, Schimmel MM. Effect of interpregnancy interval on adverse perinatal outcomes—a national study. Contraception. 2009 Dec 1;80(6):512‐8.
• Foster DG, Biggs MA, Ralph LJ, Arons A, Brindis CD. Family planning and life planning: reproductive intentions among individuals seeking reproductive health care. Women's Health Issues. 2008 Oct 31;18(5):351‐9.
• Gordon, Linda (2003). The Moral Property of Women: A History of Birth Control Politics in America. Urbana: University of Illinois Press.
• Grisaru‐Granovsky S, Gordon ES, Haklai Z, Samueloff A, Schimmel MM. Effect of interpregnancy interval on adverse perinatal outcomes‐‐a national study. Contraception. 2009 Dec;80(6):512‐8. Epub 2009 Jul 22.
• Attanasio & Kozhimannil. Health care engagement and follow‐up after perceived discrimination in maternal care. Med care 2017. 55 830
• Cohen R, Sheeder J, Arango N, Teal SB, Tocce K. Twelve‐month contraceptive continuation and repeat pregnancy among young mothers choosing postdelivery contraceptive implants or postplacental intrauterine devices. Contraception. 2016 Feb 1;93(2):178‐83.
• Woo I, Seifert S, Hendricks D, Jamshidi RM, Burke AE, Fox MC. Six‐month and 1‐year continuation rates following postpartum insertion of implants and intrauterine devices. Contraception. 2015 Dec 1;92(6):532‐5.
• Goldthwaite LM, Shaw KA. Immediate postpartum provision of long‐acting reversible contraception. Current Opinion in Obstetrics and Gynecology. 2015 Dec 1;27(6):460‐4.Woo, Contraception, 2015;
• Crockett AH, Pickell LB, Heberlein EC, Billings DL, Mills B. Six‐and twelve‐month documented removal rates among women electing postpartum inpatient compared to delayed or interval contraceptive implant insertions after Medicaid payment reform. Contraception. 2017 Jan 1;95(1):71‐6.
• Curtis KM. US medical eligibility criteria for contraceptive use, 2016. MMWR. Recommendations and Reports. 2016;65.
46
References• Phillips SJ, Tepper NK, Kapp N, Nanda K, Temmerman M, Curtis KM. Progestogen‐only contraceptive use among breastfeeding women: a systematic
review. Contraception. 2016 Sep 1;94(3):226‐52.
• Speroff L, Mishell DR. The postpartum visit: it's time for a change in order to optimally initiate contraception. Contraception. 2008 Aug 1;78(2):90‐8.
• Attanasio L, Kozhimannil KB. Health Care Engagement and Follow‐up After Perceived Discrimination in Maternity Care. Medical care. 2017 Sep 1;55(9):830‐3.
• Tocce K, Sheeder J, Arango N, Teal S. Immediate postpartum LARC in adolescents: Implants versus IUDs. Contraception. 2013 Sep 1;88(3):437‐8.
• ACOG Committee Opinion #666, Optimizing Postpartum Care
2. Discuss an educational model for training and practice
Rebecca Meekins, MDFellow, FPMRSDuke University Medical Center
4
5
Perineal Anatomy
5
6
Perineal Anatomy
6
7
Perineal Anatomy
7
8
Perineal Anatomy
8
9
Perineal Anatomy
EAS
9
10
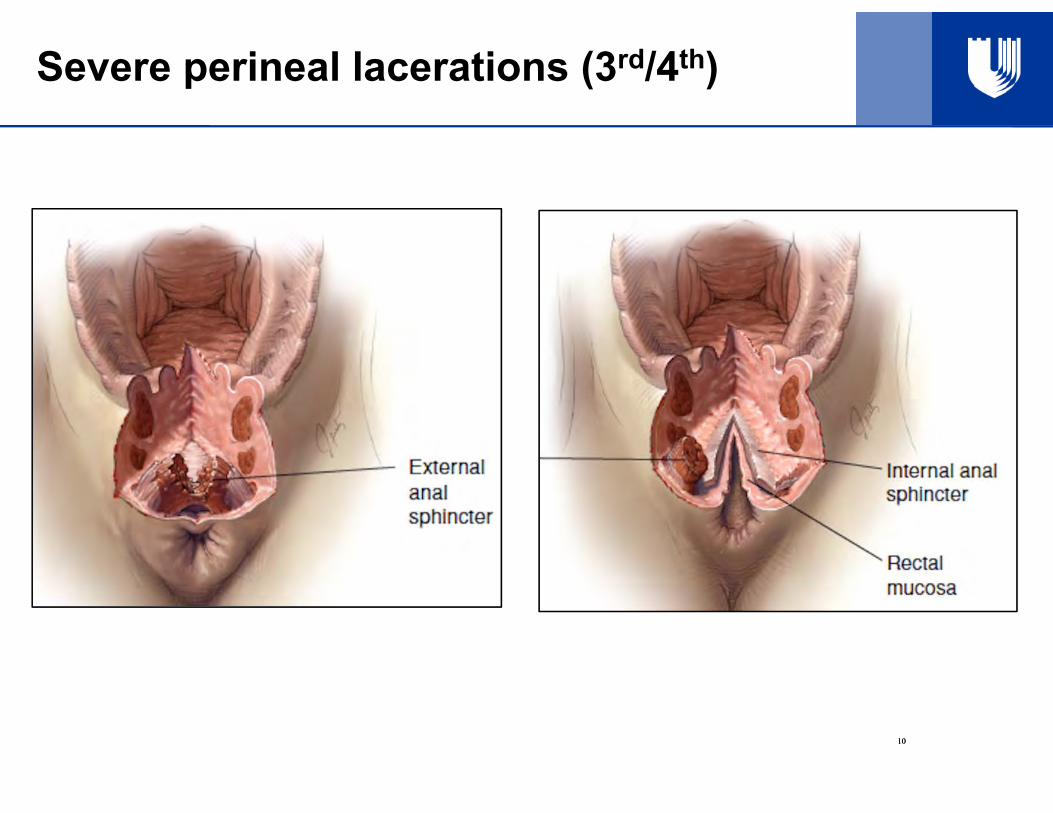
Severe perineal lacerations (3rd/4th)
10
11
Anal sphincter – endoanal US
Dobben et al. AJR 2008; 190: 671-68211
12
Suture Choice
• Rectal mucosa
o 4-0 or other fine suture
o Absorbable (Vicryl/Polysorb/Monocryl)
o Running vs interrupted with knots in lumen Prefer running but either ok as long as you are not
bunching the rectal mucosa
o Second layer of muscularis imbricating over first (to also re-attach IAS)
12
13
Suture Choice
• Internal anal sphincter
o Can be challenging to identifyo Close with second layer of rectal musculariso 3-0 delayed absorbable (Vicryl or PDS)
• External anal sphincter
o Williams et al. 2006 No significant differences in outcomes regardless of
suture choice (Vicryl vs PDS) or method (overlap vsend to end)
13
14
Antibiotic Choice
• At time of repair
o Antibiotics (2nd generation cephalosporin) reduced wound complications
o Postpartum: not routinely administered
14
15
Antibiotic Choice
• Why cephalosporin?Single RCT!
Bowel surgery: 2nd or 3rd generation cephalosporin
OBGYN surgery: 1st or 2nd generation cephalosporin
2nd generation cephalosporin = Cefotetan or cefoxitin
Severe PCN allergy -> IV Clindamycin
15
16
OASIS Repair
• Move to the OR and give antibioticsPrep the perineum
Rectal exam Determine extent of laceration Watch for button-hole defects in mucosa
Anal mucosa Running, non-locking 3-0/4-0 Vicryl
16
17
OASIS Repair
IAS:• Running, nonlocking 3-0 Polysorb• Imbricating second layer is sometimes possible
EAS:• Identify and grasp with Allis clamps • Dissect around to mobilize if needed• End-to-End vs Overlapping are both acceptable
Literature is mixed regarding outcomes Bottom line: perform the procedure you are most comfortable with
17
18
End to End vs Overlapping
18
19
Perineal Body
• Transition stitch to crown stitch vs.• Interrupted crown stitch
19
20
Simulation of 4th degree lac repair
• INSERT pictures of beef tongue model in (steps to create and final model)
20
21
References
1. Williams A1, Adams EJ, Tincello DG, Alfirevic Z, Walkinshaw SA, Richmond DH. How to repair an anal sphincter injury after vaginal delivery: results of a randomised controlled trial. BJOG. 2006 Feb;113(2):201-7.
2. Fernando RJ, Sultan AH, Kettle C, Thakar R. Methods of Repair for obstetric anal sphincter injury. Cochrane Database Syst Rev. 2013.
3. Farrell SA, Flowerdew G, Gilmour D, Turnbull GK, Schmidt MH, Baskett TF, Fanning CA. Overlapping compared with end-to-end repair of complete third-degree or fourth-degree obstetric tears: three-year follow-up of a randomized controlled trial. Obstet Gynecol. 2012;120(4):803.
4. ACOG Practice Bulletin 165- Prevention and Management of Obstetric Lacerations at Vaginal Delivery
5. Duggal N, Mercado C, Daniels K, Bujor A, Caughey AB, El-Sayed YY. Antibiotic prophylaxis for prevention of postpartum perineal wound complications: a randomized controlled trial. Obstet Gynecol 2008; 111: 1268-73
6. Stock L, Basham E, Gossett DR, Lewicky-Guapp C. Factors associated with wound complications in women with obstetric anal sphincter injuries (OASIS). Am J Obstet Gynecol 2013; 208: 327.e1-6
7. Buppasiri P, Lumbiganon P, Thinkhamrop J, Thinkhamrop B. Antibiotic prophylaxis for third- and fourth degree perinealtear during vaginal birth. Cochrane Database of Systematic Reviews 2014, Issue 10. Art No.: CD005125
8. Kettle C, Dowswell T, Ismail KM. Continuous and interrupted suturing techniques for repair of episiotomy or second-degree tears. Cochrane Database Syst Rev. 2012;11:CD000947. Epub 2012 Nov 14.