Reversal of Anticoagulation CHS Pharmacy Education Series ProCE, Inc. www.ProCE.com 1 2019 Pharmacy Education Series May 15, 2019 Reversal of Anticoagulation Faculty Speakers: Jessica M. Rimsans, PharmD, BCPS Heather Weese, PharmD, MSHI, BCPS, BCPPS Submission of an online post‐test and evaluation is the only way to obtain CE credit for this webinar Go to www.ProCE.com/CHSRx Print your CE statement of completion online – Credit for live or enduring (not both) Deadline: June 14, 2019 Pharmacists and Pharmacy Technicians: CE credit uploaded to CPE Monitor – User must complete the “claim credit” step Online Evaluation, Self-Assessment and CE Credit Attendance Code Code will be provided at the end of today’s activity 2
Transcript
Reversal of AnticoagulationCHS Pharmacy Education Series
Submission of an online post‐test and evaluation is the only way to obtain CE credit for this webinar
Go to www.ProCE.com/CHSRx
Print your CE statement of completion online
– Credit for live or enduring (not both)
Deadline: June 14, 2019
Pharmacists and Pharmacy Technicians: CE credit uploaded to CPE Monitor
– User must complete the “claim credit” step
Online Evaluation, Self-Assessmentand CE Credit
Attendance Code
Code will be provided at the end of today’s activity 2
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 2
How to Ask a Question
Locate menu bar on your computer desktop
Click orange arrow button to open menu box
Type question into question box
Click Send
Do not close menu box
– This will disconnect you
from the Webcast
Please submit questions throughout
presentation
Click No!
Click
Enter question
3
Accessing PDF Handout Click the hyperlink that is
located directly above the question box
Do not close menu box
– This will disconnect you
from the Webcast
No!
Clickhyperlink
4
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 3
2019 Pharmacy Education Series
It is the policy of ProCE, Inc. to ensure balance, independence, objectivity and scientific rigor in all of its continuing education activities. Faculty must disclose to participants the existence of any significant financial interest or any other relationship with the manufacturer of any commercial product(s) discussed in an educational presentation. None of the presenters have any relevant commercial or financial relationships to disclose.
Disclosure: The information contained in the presentation is for Community Health System employees and hospital affiliates and is not for external distribution and/or use. The presentation may contain information that is proprietary, confidential, or legally privileged or protected. It is intended only for the use of Community Health System employees and hospital affiliates. Do not deliver, distribute or copy the presentation and do not disclose its contents or take any action in reliance on the information it contains outside of Community Health Systems and hospital affiliates.
Please note: The opinions expressed in this activity should not be construed as those of the CME/CE provider. The information and views are those of the faculty through clinical practice and knowledge of the professional literature. Portions of this activity may include unlabeled indications. Use of drugs and devices outside of labeling should be considered experimental and participants are advised to consult prescribing information and professional literature.
May 15, 2019Reversal of Anticoagulation
5
CE Activity Information & Accreditation
ProCE, Inc. (Pharmacist and Pharmacy Technician CE)This CE activity is jointly provided by ProCE, Inc. and CHSPSC, LLC. ProCE is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. ACPE Universal Activity Number 0221‐9999‐19‐161‐L01‐P/T has been assigned to this knowledge‐based live CE activity (initial release date 5‐15‐19). This CE activity is approved for 2.0 contact hours (0.2 CEU) in states that recognize ACPE providers. This CE activity is provided at no cost to participants. Successful completion of the online post‐test and evaluation at www.ProCE.com/CHSRx is required to receive CE credit. CE credit will be uploaded to NABP/CPE Monitor. No partial credit will be given.
Funding:This activity is self‐funded through CHSPSC.
6
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 4
Reversal of Anticoagulation
Jessica Rimsans, PharmD, BCPS
Hemostatic Antithrombotic Stewardship
Brigham and Women’s Hospital, Boston, MA
Community Health Systems & ProCE
7
Conflicts of Interest
Speaker has no conflicts of interest
Disclosures
There will be off‐label and/or investigational
discussion
8
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 5
Pharmacist Objectives
At the conclusion of this activity, participants will be able to:
1. Discuss the differences in bleeding profiles of the direct acting oral anticoagulants (DOACs) and vitamin K antagonists (VKAs).
2. Compare strategies to reverse anticoagulant‐induced life threatening bleeding or for emergency surgery.
3. Develop a periprocedural management plan for patients on oral anticoagulants (AC).
9
Pharmacy Technician Objectives
At the conclusion of this activity, participants will be able to:
1. Understand the urgency of life threatening major bleeding.
2. List current available medications used to reverse bleeding caused by oral anticoagulants.
3. Describe how reversal agents such as PCC, idarucizumab, and andexanet are stored, prepared, and administered.
10
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 6
DOACs vs Vitamin K Antagonists
• Proposed benefits of DOACs• rapid onset of action
• ease of administration
• overall less bleeding (less major bleeding, less ICH*)
• lack of routine laboratory monitoring required
• at least non‐inferior efficacy compared with VKAs
• However, spontaneous and traumatic bleeding events do occur requiring urgent/emergent reversal
*ICH: intracranial hemorrhage Barra M, et al. Am J Med. 2016;129, 1198‐1204.
11
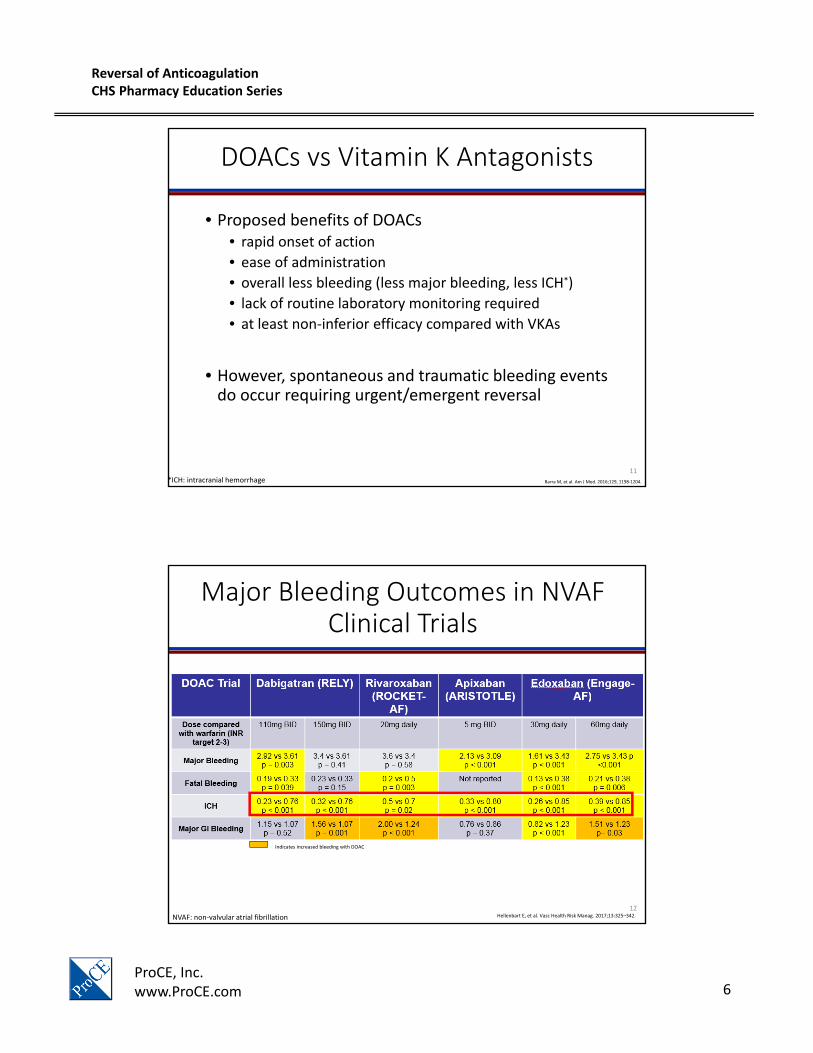
Major Bleeding Outcomes in NVAF Clinical Trials
Indicates increased bleeding with warfarin
Indicates increased bleeding with DOAC
Bleeding outcomes reported as DOAC vs warfarin (titrated to target INR 2‐3); % per year
Hellenbart E, et al. Vasc Health Risk Manag. 2017;13:325–342. NVAF: non‐valvular atrial fibrillation12
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 7
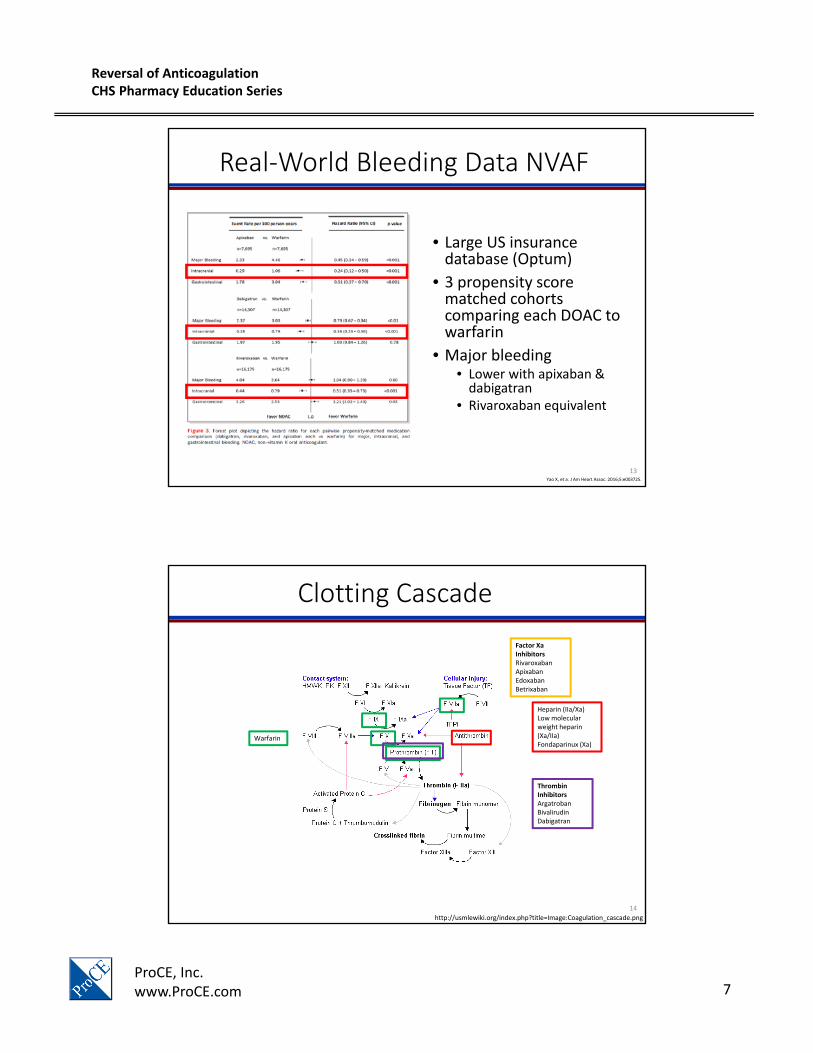
Real‐World Bleeding Data NVAF
• Large US insurance database (Optum)
• 3 propensity score matched cohorts comparing each DOAC to warfarin
• Major bleeding• Lower with apixaban & dabigatran
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 8
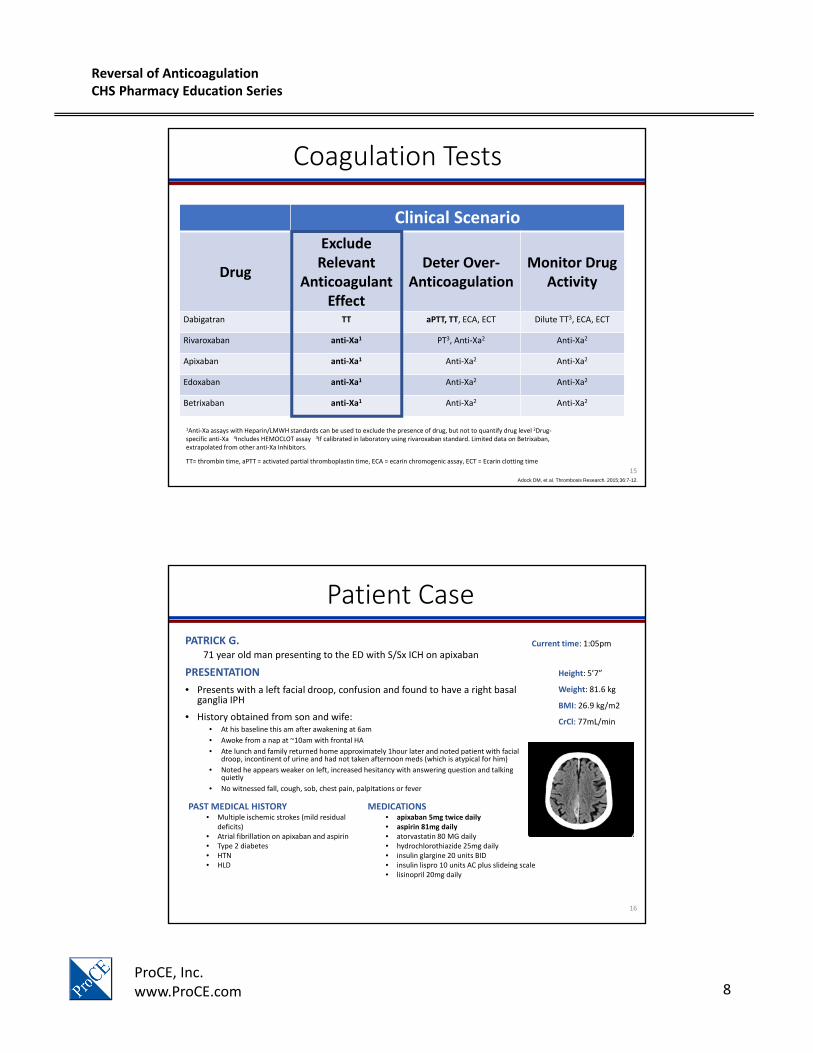
Coagulation Tests
Adock DM, et al. Thrombosis Research. 2015;36:7-12.
1Anti‐Xa assays with Heparin/LMWH standards can be used to exclude the presence of drug, but not to quantify drug level 2Drug‐specific anti‐Xa 3Includes HEMOCLOT assay 3If calibrated in laboratory using rivaroxaban standard. Limited data on Betrixaban, extrapolated from other anti‐Xa Inhibitors.
TT= thrombin time, aPTT = activated partial thromboplastin time, ECA = ecarin chromogenic assay, ECT = Ecarin clotting time
PATRICK G.71 year old man presenting to the ED with S/Sx ICH on apixaban
PRESENTATION
• Presents with a left facial droop, confusion and found to have a right basal ganglia IPH
• History obtained from son and wife: • At his baseline this am after awakening at 6am
• Awoke from a nap at ~10am with frontal HA
• Ate lunch and family returned home approximately 1hour later and noted patient with facial droop, incontinent of urine and had not taken afternoon meds (which is atypical for him)
• Noted he appears weaker on left, increased hesitancy with answering question and talking quietly
• No witnessed fall, cough, sob, chest pain, palpitations or fever
Height: 5’7”
Weight: 81.6 kg
BMI: 26.9 kg/m2
CrCl: 77mL/min
Current time: 1:05pm
PAST MEDICAL HISTORY• Multiple ischemic strokes (mild residual
deficits)• Atrial fibrillation on apixaban and aspirin• Type 2 diabetes• HTN• HLD
MEDICATIONS• apixaban 5mg twice daily• aspirin 81mg daily• atorvastatin 80 MG daily• hydrochlorothiazide 25mg daily• insulin glargine 20 units BID• insulin lispro 10 units AC plus slideing scale• lisinopril 20mg daily
16
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 9
Patient Case
PATRICK G.71 year old man presenting to the ED with S/Sx ICH on apixaban
ED COURSE
• Review of Systems (notable) by PA• Neurological: Positive for facial asymmetry, speech difficulty, weakness and headaches.
Negative for light‐headedness.
• All other systems reviewed and are negative
• Neurology Exam• Worsening LLE weakness, new L facial and likely rest was deficient at baseline, suspect a
delta‐NIHSS of 3.
• CT shows an IPH, likely hypertensive with superimposed coagulopathy from both apixaban and aspirin
• Imaging• CT/CTA notable for basal ganglia hemorrhage
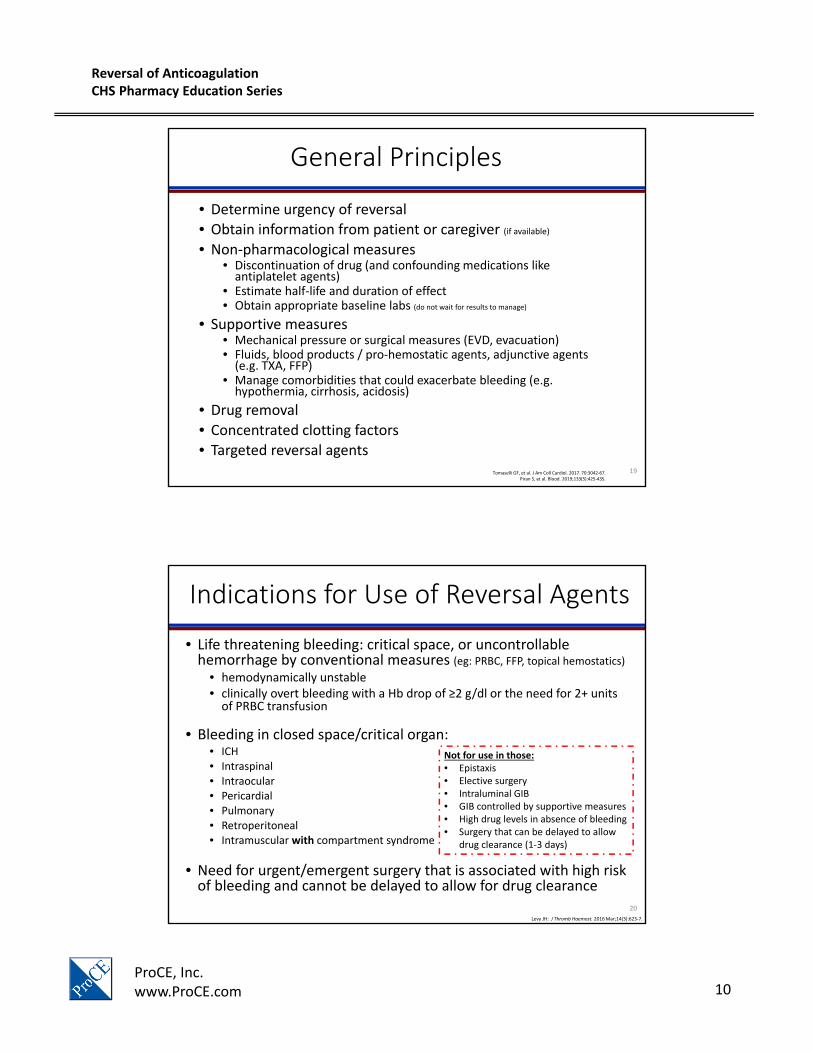
• Manage comorbidities that could exacerbate bleeding (e.g. hypothermia, cirrhosis, acidosis)
• Drug removal
• Concentrated clotting factors
• Targeted reversal agentsTomaselli GF, et al. J Am Coll Cardiol. 2017. 70:3042‐67.
Piran S, et al. Blood. 2019;133(5):425‐435.
19
Indications for Use of Reversal Agents
• Life threatening bleeding: critical space, or uncontrollable hemorrhage by conventional measures (eg: PRBC, FFP, topical hemostatics)
• hemodynamically unstable• clinically overt bleeding with a Hb drop of ≥2 g/dl or the need for 2+ units of PRBC transfusion
• Bleeding in closed space/critical organ:• ICH• Intraspinal• Intraocular• Pericardial• Pulmonary• Retroperitoneal• Intramuscular with compartment syndrome
• Need for urgent/emergent surgery that is associated with high risk of bleeding and cannot be delayed to allow for drug clearance
Levy JH: J Thromb Haemost. 2016 Mar;14(3):623‐7.
Not for use in those: • Epistaxis• Elective surgery• Intraluminal GIB• GIB controlled by supportive measures• High drug levels in absence of bleeding • Surgery that can be delayed to allow
drug clearance (1‐3 days)
20
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 11
Major Bleeding – Critical Sites
Critical Site Potential Signs/Symptoms Potential Consequences
Tomaselli GF, et al. J Am Coll Cardiol. 2017. 70:3042-67.EKG = electrocardiogram
21
Oral Anticoagulation Reversal Options
FDA Approved Options
• Idarucizumab for dabigatran reversal only
• Andexanet alfa for apixaban and rivaroxaban only
• 4PCC VKA‐reversal only
Off Label / Alternative Options
• 3PCC • 4PCC• aPCC (Factor VIII inhibitor bypassing activity)
• Recombinant activated factor VII• Plasmapheresis• Hemodialysis for dabigatran reversal only
• Activated charcoal
Also may use Vitamin K and Fresh Frozen Plasma (FFP) for Warfarin reversalVitamin K and FFP will not overcome/reverse DOAC effect
22
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 12
Concentrated Clotting Factors
• Prothrombin Complex Concentrates (PCC)• Four factor PCC (4PCC)
• Contains non‐activated vitamin K‐dependent coagulation Factors II, VII, IX, and X and antithrombotic Proteins C and S* (and a small amount of heparin)
• Three factor PCC (3PCC)• Contains non‐activated factors II, IX, X and trace amounts of factor VII
• Requires concomitant administration of FFP for source factor VII
• Activated Prothrombin Complex Concentrates (aPCC)• Four factor aPCC
• Contains mainly non‐activated factors II, IX, X and activated factor VII
• Activated recombinant factor VII (rVIIa)• Contains only activated factor VII
Nutescu EA, et al. Am J Health Syst Pharm. 2013;70(21):1914‐29.
23
Anticoagulation reversal in the setting of life threatening major bleeding
VKA Reversal
24
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 13
Guideline Recommendations ‐ VKA Reversal
Frontera JA, et al. Crit Care Med 2016; 44:2251‐2257.Tomaselli GF, et al. J Am Coll Cardiol. 2017;70(24):3042‐3067.
Critical Care Guidelines2016
Expert Consensus Decision Pathway 2017
Recommend discontinuation of VKA if ICH is present/suspected Agreement
Recommend urgent reversal of VKA in patients with ICH (exceptions for risk vs benefit assessment*)
Agreement
Recommend administration of vitamin K
a.) Dose: 10mg IV x1 w/follow‐up INR
b.) If INR ≥ 1.4 within 23‐48 hrs, suggest redosing
Agreement
Not specifically addressed for ICH
Recommend 3PCC or 4PCC over FFP
a.) Recommend 4PCC over 3PCC
b.) PCC dosing should be weight based and vary according to admission INR and type of PCC used
Agreement
Guidance for INR/weight‐based dosing or low fixed‐dose option (1500 units
for ICH)
25
Management of Warfarin‐Related Life Threatening Bleeding
• FDA approval 4PCC• Reversal of life threatening
bleeding or requiring surgery on patients taking warfarin
• Package label dosing: 25‐50 units/kg based on INR
• Off label fixed low dose: 1500 units for ICH (or 2000 units*)
• Risk of thromboembolic events is not clear
• Recommended dose = 10mg slow IV Push
• IV over PO
• Slower onset, but sustained effect
• Combination with 4PCC
Lubetsky A, et al. Arch Intern Med. 2003;163:2469‐2473.
Vitamin K4PCC (Kcentra®)
Other options include: 3PCC +/‐ FFP or rFVIIa if 4PCC not available
26
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 14
Warfarin Reversal Agents
Nutescu EA, et al. Am J Health Syst Pharm. 2013;70(21):1914‐29.Frontera JA, et al. Crit Care Med. 2016; 44:2251–2257.
Hanke AA, et al. Br J Anaesth. 2013;110(5):764‐72.
Drug Onset of Effect Duration of Effect
Vitamin K (PO) 24 hours Days
Vitamin K (IV) 8‐12 hours Days
FFP Immediate post infusion 12‐24 hours
4PCC* Immediate post infusion 12‐24 hours
• Re‐dosing may be required based on INR post‐reversal and sustained decline in the 1st 24‐48 hours post ICH to prevent hematoma expansion
*Potentially higher thrombotic rate vs FFP (reported at 1.8%)
27
4PCC Dosing for VKA Reversal – Variable dosing
Sarode R, et al. Circulation. 2013;128:1234‐124.
Baseline INR
4PCC dose
Plasma dose
2‐ < 425
units/kg10 mL/kg
4‐635
units/kg12 mL/kg
> 650
units/kg15 mL/kg
Max doses
5000 units
1500 mLs
• Phase IIIb, multicenter, open‐label, noninferiority trial, nonsurgical patients • Variable dosing based on presenting INR and patient weight
Outcomes4PCC(n = 98)
Plasma (n=104)
Difference (95% CI)
Effective Hemostatic Efficacy (No, %)
71 (72.4)
68 (65.4) 7.1 (‐5.8 to 19.9)
Rapid INR Reduction*
61 (62.2)
10 (9.6)52.6 (39.4 to
65.9)
Adverse Events
Thromboembolic Events
8 (7.8) 7 (6.4) N/A
Related thromboembolic Events
4 (3.9) 3 (2.8) N/A
Serious adverse events
32 (31.1)
26 (23.9) N/A
*INR ≤1.3 at 0.5 h after end of infusion
28
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 15
4PCC Dosing for VKA Reversal– Fixed Dosing
• Low fixed‐dose options (ACC 2017 Guideline Recommendations)• 1,000 units for any major bleed, 1500 units for ICH
• Multiple evaluations of fixed dosing from 1000 units to 1500 units
• Retrospective analysis from University of New Mexico 2018
Astrup G, et al. J Thromb Thrombolysis. 2018;45:300–305.
Outcomes Result
INR ≤ 1.5 post 4PCC 74.3% (26/35)
INR ≤ 1.5 post 4PCC – initial INR > 5
60% (6/10)
INR ≤ 2.0 post 4PCC 100% (30/30)
Thromboembolic Events 0
• 37 patients reviewed• Fixed dose 1500 units; median 20 units/kg• Indication for reversal
• Emergent bleeding 78.4%• ICH 45.9%• GI 13.5%
• Urgent surgery 18.9%• Initial INR (median) = 3.06 (range 1.17 to > 16)• Concomitant Medications
• Vitamin K 81.1%• FFP 24.3%
One patient required 2nd dose of 4PCC 2 days after initial dose
29
Anticoagulation reversal in the setting of life threatening bleeding
Dabigatran
30
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 16
Guideline Recommendations ‐ Oral DTI Reversal
Frontera JA, et al. Crit Care Med 2016; 44:2251‐2257.Tomaselli GF, et al. J Am Coll Cardiol. 2017;70(24):3042‐3067.
Cuker A, et al. Am J Hematol. 2019 Mar 27. [Epub ahead of print] Review.
Critical Care Guidelines2016
Expert Consensus Decision Pathway
2017
AC Forum Consensus Document 2019
Recommend discontinuation of DTI when ICH is present or suspected
Agreement Agreement
Recommend obtain time and amount of last dose, renal function and medication interactions to estimate degree of anticoagulation
Agreement Agreement
Suggest activated charcoal (50g) to intubated ICH with enteral access or low risk for aspiration within 2 hours of ingestion
Agreement (within 2‐4 hours of
ingestion)
Agreement
Recommend idarucizumab (5g IV in 2 doses)
a.) dabigatran administered within 3‐5 half‐lives and no evidence of renal failureb.) renal insufficiency leading to drug exposure beyond 3‐5 half‐lives
Agreement Agreement
Suggest 4PCC (50 units/kg) or aPCC (50 units/kg) if ICH if idarucizumab is not available
Agreement aPCC 50 units/kg
Suggest redosing idarucizumab and/or hemodialysis if evidence of ongoing clinically significant bleeding
Not addressed Agreement
31
Idarucizumab (Praxbind®)
• FDA Approved October 2015• Human monoclonal antibody fragment that binds free and thrombin‐bound dabigatran
• 300 x higher affinity for dabigatran than dabigatran has for thrombin
• Renally eliminated
• Indication• Emergency surgery / urgent procedures
• Life‐threatening or uncontrolled bleeding
• Dose• 5gm dose administered as 2.5gm x2 IV bolus within 15 minutes
• May require repeat dosing due to dabigatran Vd (rare)
• Cost – approximately $3500 per dose
Gm: grams; VD: Volume of distributionArbit B, et al. Int J of Cardiol. 2016;223: 244–250.
32
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 17
RE‐VERSE AD Trial
• Design: Multicenter, prospective, open‐label study
• Objective: Does 5 grams idarucizumab reverse the anticoagulant effect of dabigatran
• Group A: Uncontrolled bleeding (n= 301)
• GI bleeding (n = 137, 45.5%)• ICH (n =98, 32.6%)
• Group B: urgent procedure (n = 202)
Pollack CV, et al. N Engl J Med. 2017;377:431‐441.33
RE‐VERSE AD Endpoints
• Median maximum percentage reversal of dabigatran was 100% by either ecarin clotting time (ECT) or dilute thrombin time (dTT)
• Group A: median time to the cessation of bleeding was 2.5 hours
• Group B: periprocedural hemostasis was assessed as normal in 93.4% of the patients
• At 90 days:
• Thrombotic events occurred in 6.3% Group A and 7.4% in Group B
• Mortality rate was 18.8% and 18.9% in Group A and Group B respectively
• No serious adverse safety signals
• 8 patients required 2nd dose of idarucizumab
Pollack CV, et al. N Engl J Med. 2017;377:431‐441.
34
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 18
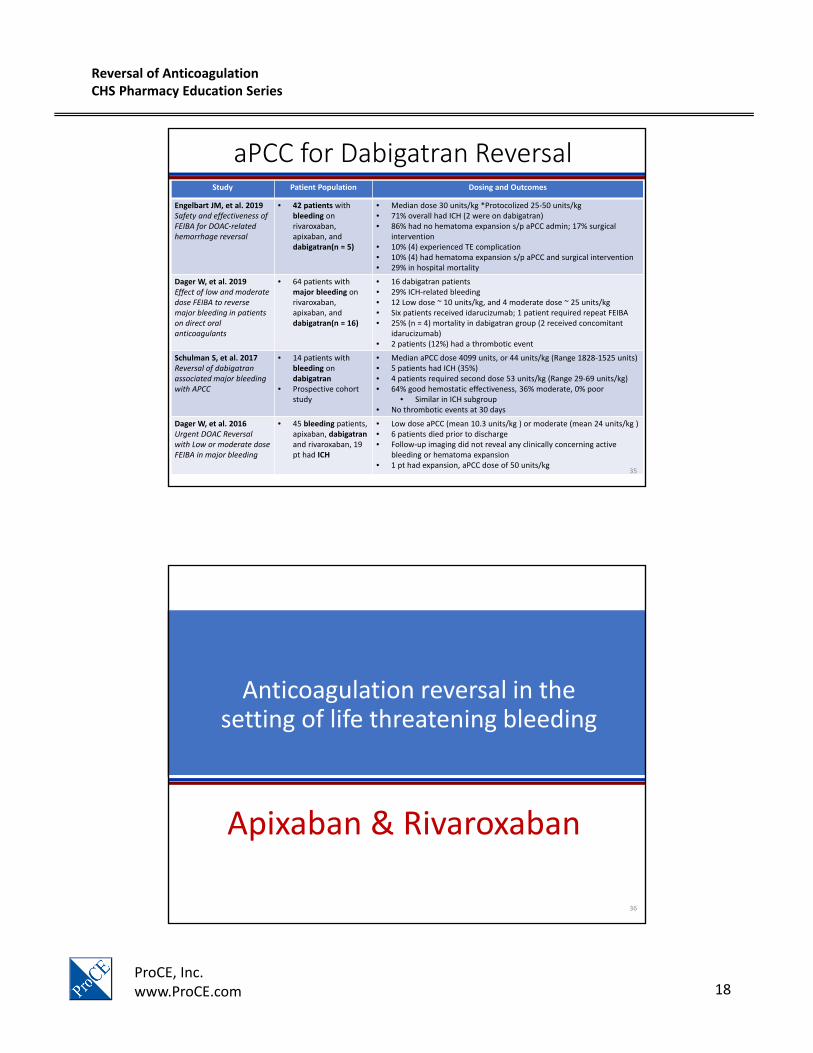
aPCC for Dabigatran ReversalStudy Patient Population Dosing and Outcomes
Engelbart JM, et al. 2019Safety and effectiveness of FEIBA for DOAC‐related hemorrhage reversal
• 42 patients with bleeding on rivaroxaban, apixaban, anddabigatran(n = 5)
• Median dose 30 units/kg *Protocolized 25‐50 units/kg • 71% overall had ICH (2 were on dabigatran)• 86% had no hematoma expansion s/p aPCC admin; 17% surgical
intervention • 10% (4) experienced TE complication• 10% (4) had hematoma expansion s/p aPCC and surgical intervention• 29% in hospital mortality
Dager W, et al. 2019Effect of low and moderate dose FEIBA to reverse major bleeding in patientson direct oral anticoagulants
• 64 patients with major bleeding on rivaroxaban, apixaban, anddabigatran(n = 16)
• 16 dabigatran patients • 29% ICH‐related bleeding• 12 Low dose ~ 10 units/kg, and 4 moderate dose ~ 25 units/kg• Six patients received idarucizumab; 1 patient required repeat FEIBA • 25% (n = 4) mortality in dabigatran group (2 received concomitant
idarucizumab)• 2 patients (12%) had a thrombotic event
Schulman S, et al. 2017Reversal of dabigatran associated major bleeding with APCC
• 14 patients with bleeding on dabigatran
• Prospective cohort study
• Median aPCC dose 4099 units, or 44 units/kg (Range 1828‐1525 units)• 5 patients had ICH (35%)• 4 patients required second dose 53 units/kg (Range 29‐69 units/kg) • 64% good hemostatic effectiveness, 36% moderate, 0% poor
• Similar in ICH subgroup• No thrombotic events at 30 days
Dager W, et al. 2016Urgent DOAC Reversal with Low or moderate dose FEIBA in major bleeding
• 45 bleeding patients, apixaban, dabigatranand rivaroxaban, 19 pt had ICH
• Low dose aPCC (mean 10.3 units/kg ) or moderate (mean 24 units/kg ) • 6 patients died prior to discharge• Follow‐up imaging did not reveal any clinically concerning active
bleeding or hematoma expansion• 1 pt had expansion, aPCC dose of 50 units/kg
35
Anticoagulation reversal in the setting of life threatening bleeding
Apixaban & Rivaroxaban
36
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 19
Guideline RecommendationsOral Xa Inhibitor Reversal
Frontera JA, et al. Crit Care Med 2016; 44:2251‐2257.Tomaselli GF, et al. J Am Coll Cardiol. 2017;70(24):3042‐3067.
Cuker A, et al. Am J Hematol. 2019 Mar 27. [Epub ahead of print] Review.
Critical Care Guidelines2016
Expert Consensus Decision Pathway 2017
Recommend discontinuation of factor Xa inhibitor when ICH is present or suspected
Agreement
Recommend obtain time of last dose of factor Xa inhibitor and medication interactions to estimate anticoagulation exposure
Agreement
Suggest activated charcoal (50g) to intubated ICH with enteral access or low risk for aspiration within 2 hours of ingestion
Agreement (within 2‐4 hours of ingestion)
Suggest 4PCC (50 units/kg) or aPCC (50 units/kg) if ICH within 3‐5 terminal half‐lives of drug or in the context of liver failure
Administer 4PCC 50 units/kg IV
If 4PCC not available, consider aPCC 50 units/kg IV
Suggest 4PCC or aPCC over rFVIIa due to lower risk of thromboembolic events
Not addressed
37
Guideline RecommendationsOral Xa Inhibitor Reversal
Frontera JA, et al. Crit Care Med 2016; 44:2251‐2257.Tomaselli GF, et al. J Am Coll Cardiol. 2017;70(24):3042‐3067.
Critical Care Guidelines2016
Expert Consensus Decision Pathway 2017
Recommend discontinuation of factor Xa inhibitor when ICH is present or suspected
Agreement
Recommend obtain time of last dose of factor Xa inhibitor and medication interactions to estimate anticoagulation exposure
Agreement
Suggest activated charcoal (50g) to intubated ICH with enteral access or low risk for aspiration within 2 hours of ingestion
Agreement (within 2‐4 hours of ingestion)
Suggest 4PCC (50 units/kg) or aPCC (50 units/kg) if ICH within 3‐5 terminal half‐lives of drug or in the context of liver failure
Administer 4PCC 50 units/kg IV
If 4PCC not available, consider aPCC50 units/kg IV
Suggest 4PCC or aPCC over rFVIIa due to lower risk of thromboembolic events
Not addressed
2018 ACC Updated Guidance for Anticoagulation Reversal
First line (when available) for apixaban and rivaroxaban Andexanet alfa
2019 AC Forum Guidance Document
First line (when available) for apixaban and rivaroxaban Andexanet alfa
If not available, 4PCC Fixed Dose 2000 units for life threatening bleeding
38
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 20
Andexanet Alfa (Andexxa®)
Coagulation factor Xa (recombinant), inactivated‐zhzo (Andexxa®), is a recombinant modified human factor Xa decoy protein that is catalytically inactive but that retains the ability to bind factor Xa inhibitors in the active site with high affinity
• ICH 70%• Median dose 2000 units (1500‐2000u); 25
units/kg
• Hemostatic effectiveness 69%, 73% in ICH• 61.5% of ineffective hemostasis was in ICH• 32% mortality (27 pts, 74% were ICH)• 4% thromboembolism (3 pts)
Arachchillage et al, 2019• Major bleeding (ICH/GIB) on Fxai (n=80)
• 4PCC 2000 units (range 1000‐4500 units)• Effectiveness: ~75% for FXAi, no difference in
rebleeding
Sin et al, 2016• Major bleeding (11) and surgery (3) on Fxai (n=14)
• 6 patients received a 2nd dose (2 ICH 50 units/kg)• 5 thromboembolic events (8%); 3 LD and 2 HD• 9 patients died within 30 days (14%)• 12 of 28 ICH patients received low dose
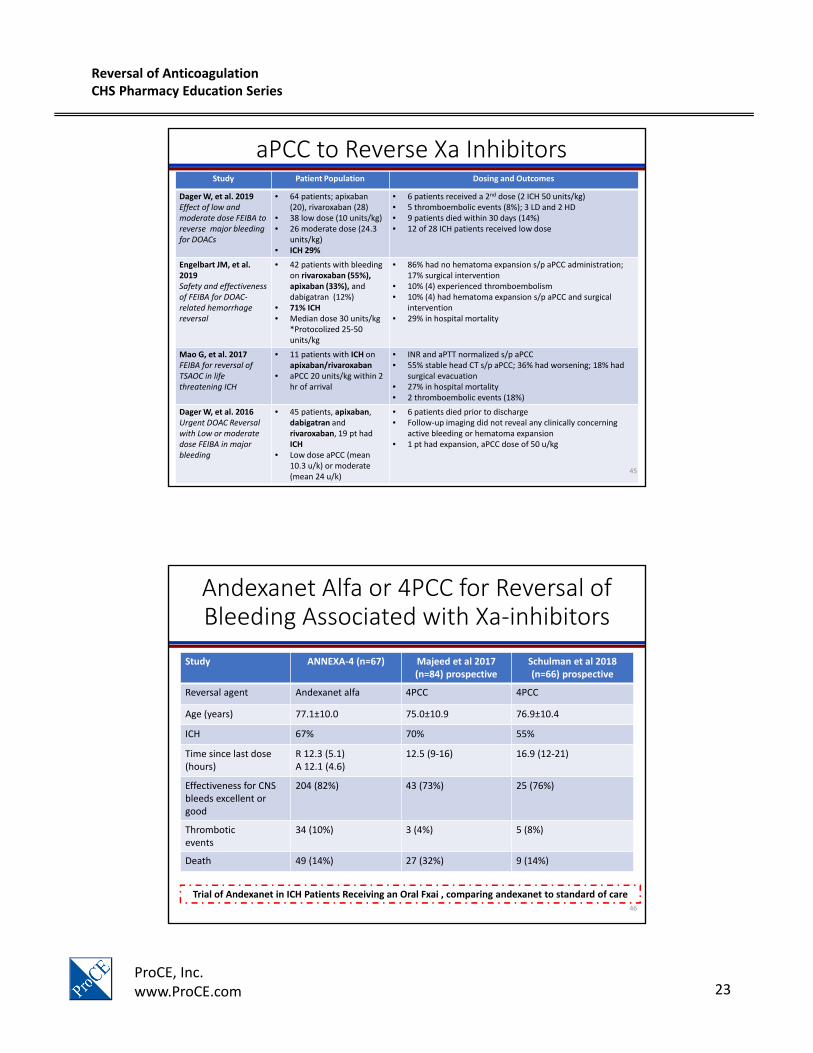
Engelbart JM, et al. 2019Safety and effectiveness of FEIBA for DOAC‐related hemorrhage reversal
• 42 patients with bleeding on rivaroxaban (55%), apixaban (33%), and dabigatran (12%)
• 71% ICH• Median dose 30 units/kg
*Protocolized 25‐50 units/kg
• 86% had no hematoma expansion s/p aPCC administration; 17% surgical intervention
• 10% (4) experienced thromboembolism• 10% (4) had hematoma expansion s/p aPCC and surgical
intervention• 29% in hospital mortality
Mao G, et al. 2017FEIBA for reversal of TSAOC in life threatening ICH
• 11 patients with ICH on apixaban/rivaroxaban
• aPCC 20 units/kg within 2 hr of arrival
• INR and aPTT normalized s/p aPCC• 55% stable head CT s/p aPCC; 36% had worsening; 18% had
• 6 patients died prior to discharge• Follow‐up imaging did not reveal any clinically concerning
active bleeding or hematoma expansion• 1 pt had expansion, aPCC dose of 50 u/kg
45
Andexanet Alfa or 4PCC for Reversal of Bleeding Associated with Xa‐inhibitors
Study ANNEXA‐4 (n=67) Majeed et al 2017 (n=84) prospective
Schulman et al 2018 (n=66) prospective
Reversal agent Andexanet alfa 4PCC 4PCC
Age (years) 77.1±10.0 75.0±10.9 76.9±10.4
ICH 67% 70% 55%
Time since last dose(hours)
R 12.3 (5.1)A 12.1 (4.6)
12.5 (9‐16) 16.9 (12‐21)
Effectiveness for CNS bleeds excellent or good
204 (82%) 43 (73%) 25 (76%)
Thromboticevents
34 (10%) 3 (4%) 5 (8%)
Death 49 (14%) 27 (32%) 9 (14%)
Trial of Andexanet in ICH Patients Receiving an Oral Fxai , comparing andexanet to standard of care 46
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 24
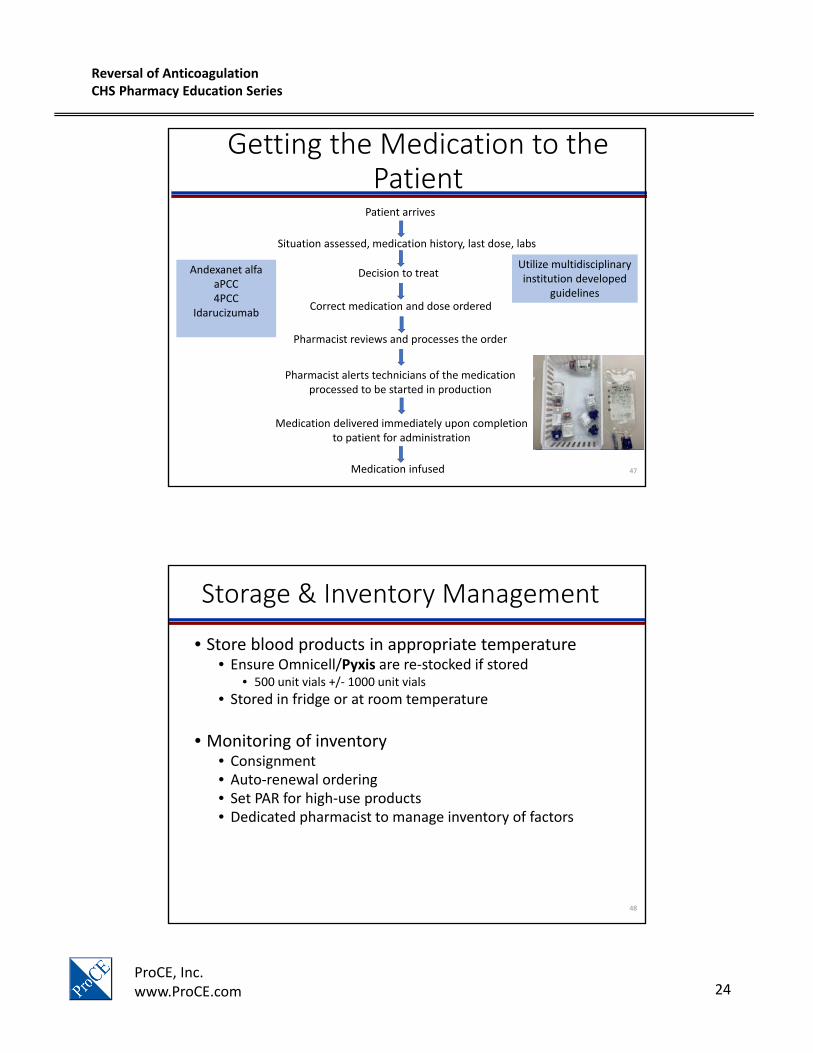
Getting the Medication to the Patient
Patient arrives
Situation assessed, medication history, last dose, labs
Decision to treat
Correct medication and dose ordered
Pharmacist reviews and processes the order
Pharmacist alerts technicians of the medication processed to be started in production
Medication delivered immediately upon completion to patient for administration
Medication infused
Andexanet alfaaPCC4PCC
Idarucizumab
Utilize multidisciplinary institution developed
guidelines
47
Storage & Inventory Management
• Store blood products in appropriate temperature• Ensure Omnicell/Pyxis are re‐stocked if stored
• 500 unit vials +/‐ 1000 unit vials
• Stored in fridge or at room temperature
• Monitoring of inventory • Consignment • Auto‐renewal ordering• Set PAR for high‐use products• Dedicated pharmacist to manage inventory of factors
48
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 25
Preparation & Administration Considerations
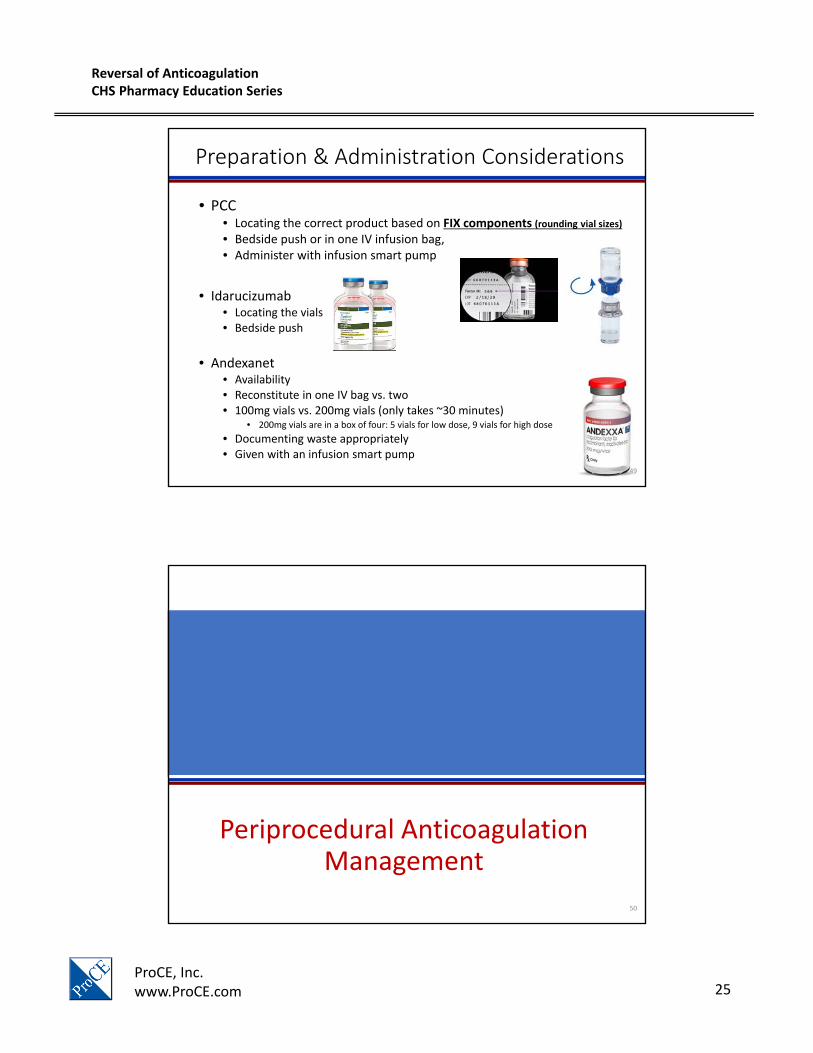
• PCC• Locating the correct product based on FIX components (rounding vial sizes)• Bedside push or in one IV infusion bag,• Administer with infusion smart pump
• Idarucizumab• Locating the vials • Bedside push
• Andexanet• Availability• Reconstitute in one IV bag vs. two• 100mg vials vs. 200mg vials (only takes ~30 minutes)
• 200mg vials are in a box of four: 5 vials for low dose, 9 vials for high dose
• Documenting waste appropriately• Given with an infusion smart pump
49
Periprocedural Anticoagulation Management
50
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 26
Guideline Recommendations – 2017 ACC
General Approach to Management:
• Estimate thromboembolic risk• Different registries exist to aid (eg: NVAF vs.
Valves)
• Estimate bleeding risk• Dependent on bleed and surgical approach as
well as patient specific characteristics (eg: age, renal or hepatic dysfunction)
• Determine timing of anticoagulant interruption
• Determine whether to use IV anticoagulant bridging
Picture from: Doherty JU, et al. J Am Coll Cardiol. 2017 Feb 21;69(7):871‐89851
Guideline Recommendations – DOAC
• Low risk procedures• Continue DOAC
• Time procedure at ‘trough’
• Moderate to High risk procedures• Duration of hold dependent on CrCl and intermediate or high bleed risk
• Restarting DOAC post procedure • No bridge required for DOACs
• May start with a short acting agent 1st
such as CI UFH monitor for hemostasis
CI UFH: continuous infusion unfractionated heparin
Doherty JU, et al. J Am Coll Cardiol. 2017 Feb 21;69(7):871‐89852
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 27
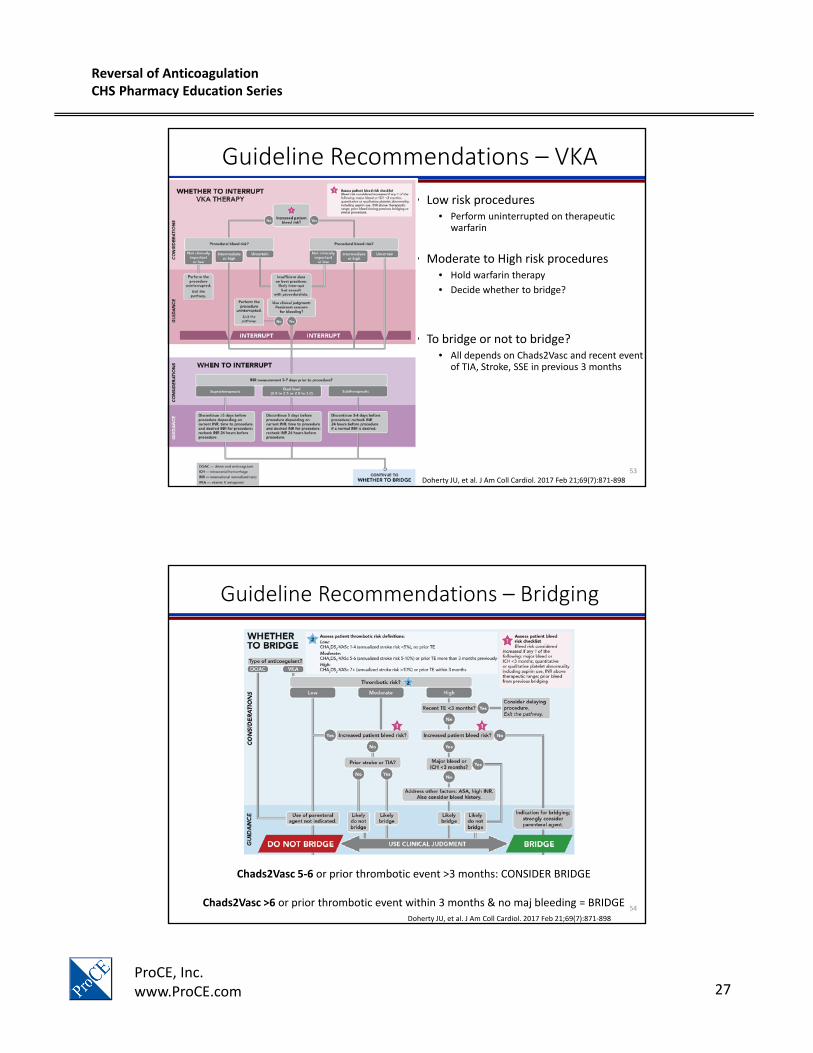
Guideline Recommendations – VKA
• Low risk procedures• Perform uninterrupted on therapeutic
warfarin
• Moderate to High risk procedures• Hold warfarin therapy
• Decide whether to bridge?
• To bridge or not to bridge?• All depends on Chads2Vasc and recent event
of TIA, Stroke, SSE in previous 3 months
Doherty JU, et al. J Am Coll Cardiol. 2017 Feb 21;69(7):871‐89853
Guideline Recommendations – Bridging
Chads2Vasc 5‐6 or prior thrombotic event >3 months: CONSIDER BRIDGE
Chads2Vasc >6 or prior thrombotic event within 3 months & no maj bleeding = BRIDGE Doherty JU, et al. J Am Coll Cardiol. 2017 Feb 21;69(7):871‐898
54
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 28
PAUSE Trial• The Perioperative Anticoagulant Use for Surgery Evaluation (PAUSE) Study
• Prospective study of 3,000 NVAF patients (23 sites) undergoing elective procedures requiring interruption to AC therapy
• 33.5% high bleeding risk surgery/procedure
• 1257 apixaban, 1082 rivaroxaban, 668 dabigatran
• Strategy for holding AC resulted in:
• minimal or no residual DOAC level at the time of surgery
• low rates of perioperative major bleeding (<2%)
• low rates of acute thrombotic events (<1%)
Thromb Haemost. 2017 Dec;117(12):2415-242455
Conclusions
• Regardless which reversal agent is given, life threatening major bleeding is associated with high morbidity and mortality.
• When considering anticoagulation reversal, decide if appropriate, and obtain a thorough patient history including OAC/last dose, evaluate risk of bleeding vs risk of thrombosis, get appropriate labs.
• Guideline Reversal Recommendations: • VKA reversal: 4PCC & IV Vitamin K
• Oral DTI reversal: Idarucizumab aPCC 25‐50 units/kg (lower doses observed in the literature)
• Provides guidance and evidence‐based support for reversal or management of bleeding complications
• Includes:– Adverse Drug Event reporting requirements– Critical Bleeding Management Flowchart– Guidance for Reversal of:
• Vitamin K Antagonists• Heparin • Low Molecular Weight Heparin and Pentasaccharides• Thrombolytics• Direct Thrombin Inhibitors• Factor Xa Inhibitors• Antiplatelets
63
Format for RecommendationDrug Class Being Reversed
Recommended reversal agents and important information
64
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 33
Format for Recommendation
• Table with Considerations, Management and Monitoring recommendations:
– Clinical Protocols and Guidelines ‐> AnticoagReversal Protocol
66
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 34
Order Set
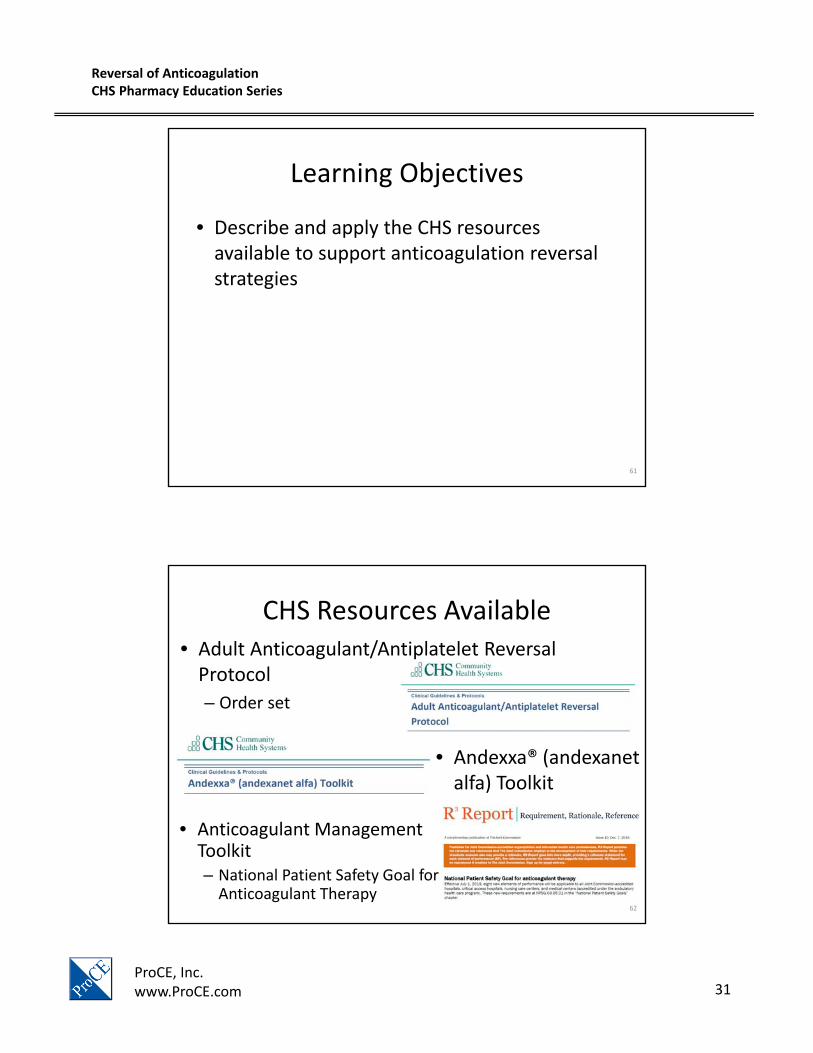
• Anticoagulant Reversal, Adult
• Organized by drug with appropriate reversal agents, doses, and routes listed
• Guidance for choosing the most appropriate reversal agent is also provided
*entire order set not represented67
Andexxa® (andexanet alfa) Toolkit
• Supports the use of Kcentra as the preferred product over Andexxa for the reversal of rivaroxabanand apixabanassociated bleeding
68
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 35
Toolkit Highlights
• Efficacy– Andexxa:
• Healthy volunteers (ANNEXA‐A and ANNEXA‐R)
• Patients with acute major bleeding (ANNEXA‐4)
– Kcentra:• Patients with acute major bleeding:
– Hemostasis
– Hemorrhage progression
• Safety– Thromboembolic complications
69
CHS Strategy
• Kcentra will be recommended as the preferred product available for urgent reversal of factor Xa inhibitor associated bleeding
– FEIBA – second line if Kcentra unavailable
70
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 36
Rationale
• Currently available literature on Andexxa® (andexanet alfa) does not examine outcomes data and the current published study in acute bleeding is limited to a single study of 254 patients for efficacy evaluation.
• Current study of andexanet alfa does not include an active comparator such as 4F‐PCC.
• Currently available literature concerning safety (ANNEXA‐4) identifies a 10% risk of thrombotic events including myocardial infarction, stroke, and venous thromboembolism in patients who have received andexanet alfa (34 out of 352 patients).
• Cost of Andexxa® therapy is substantial with an initial acquisition cost of up to $55,000 and a cost of between $24,750 and $49,500 per treatment regimen.
• Exclusion of Andexxa® from formulary is widespread with many other hospitals, including large, academic medical centers and not‐for profit and for‐profit health system electing to not stock Andexxa® at this time.
• Literature regarding comparative agents in similar patient populations is inconclusive regarding the superiority of Andexxa® over traditionally recommended therapies.
71
Who isn’t stocking
• States and Major Medical Centers
• No major medical centers in:
– Alabama
– Alaska
– New Mexico
– Tennessee
72
Reversal of AnticoagulationCHS Pharmacy Education Series
– Parenteral anticoagulants (heparin, enoxaparin, fondaparinux, argatroban, and bivalirudin)
• In depth recommendations for – Perioperative management
– Transitioning between anticoagulants
74
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 38
Toolkit Location
• PENDING APPROVAL FROM CLINICAL PHARMACY COUNCIL
75
Anticoagulation Reversal – CHS Resources and Recommendations
Heather Weese, PharmD, MSHI, BCPS, BCPPS
Senior Director, Pharmacy Services
76
Reversal of AnticoagulationCHS Pharmacy Education Series
ProCE, Inc.www.ProCE.com 39
77
Disclosure: The information contained in the presentation is for Community Health System employees and hospital affiliates and is not for external distribution and/or use. The presentation may contain information that is proprietary, confidential, or legally privileged or protected. It is intended only for the use of Community Health System employees and hospital affiliates. Do not deliver, distribute or copy the presentation and do not disclose its contents or take any action in reliance on the information it contains outside of Community Health Systems and hospital affiliates.
Heather Weese, PharmD, MSHI, BCPS, BCPPS
Senior Director, Pharmacy Services
Community Health Systems
Update on Current Pharmacy Initiatives and Strategies