28
250 Fractionated Radiation Therapy for Malignant Brain Tumors Youmans Neurological surgery 13/09/2559 George M. Cannon Minesh P. Mehta
| Date post: | 20-Jan-2017 |
| Category: |
Health & Medicine |
| Upload: | neurosurgery-vajira |
| View: | 31 times |
| Download: | 1 times |
250 Fractionated Radiation Therapy for Malignant Brain Tumors
Youmans Neurological surgery13/09/2559
George M. CannonMinesh P. Mehta
Outline• Brain metastasis• Malignant glioma• Anaplastic Astrocytoma• Anaplastic Oligodendroglioma• Primary CNS lymphoma• Malignant meningeal tumor• Primitive Neuroectodermal Tumors• Germ Cell Neoplasms
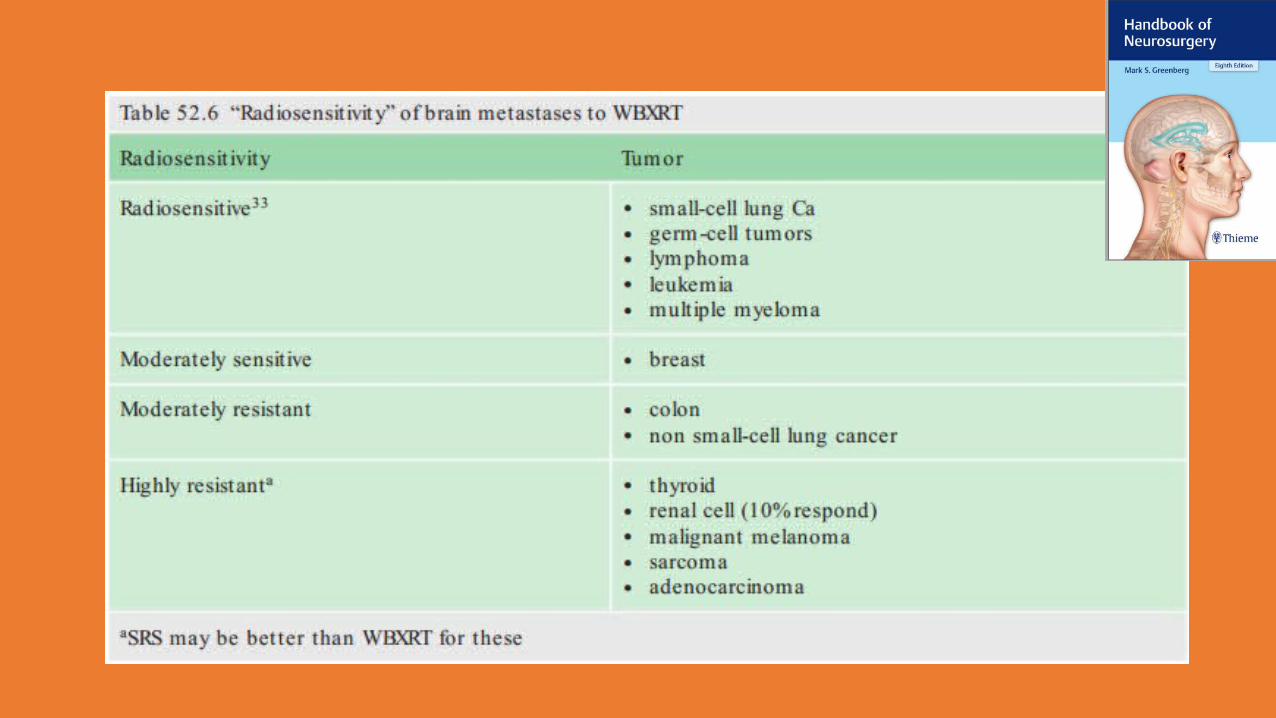
Brain metastasis
• Most common : lung, breast, melanoma• Less common : primary tumors of the gastrointestinal tract and
genitourinary system, lymphomas, sarcomas, and prostate cancer• Median survival time of untreated patients with brain metastases is
approximately 1 month

Fractionation Trials
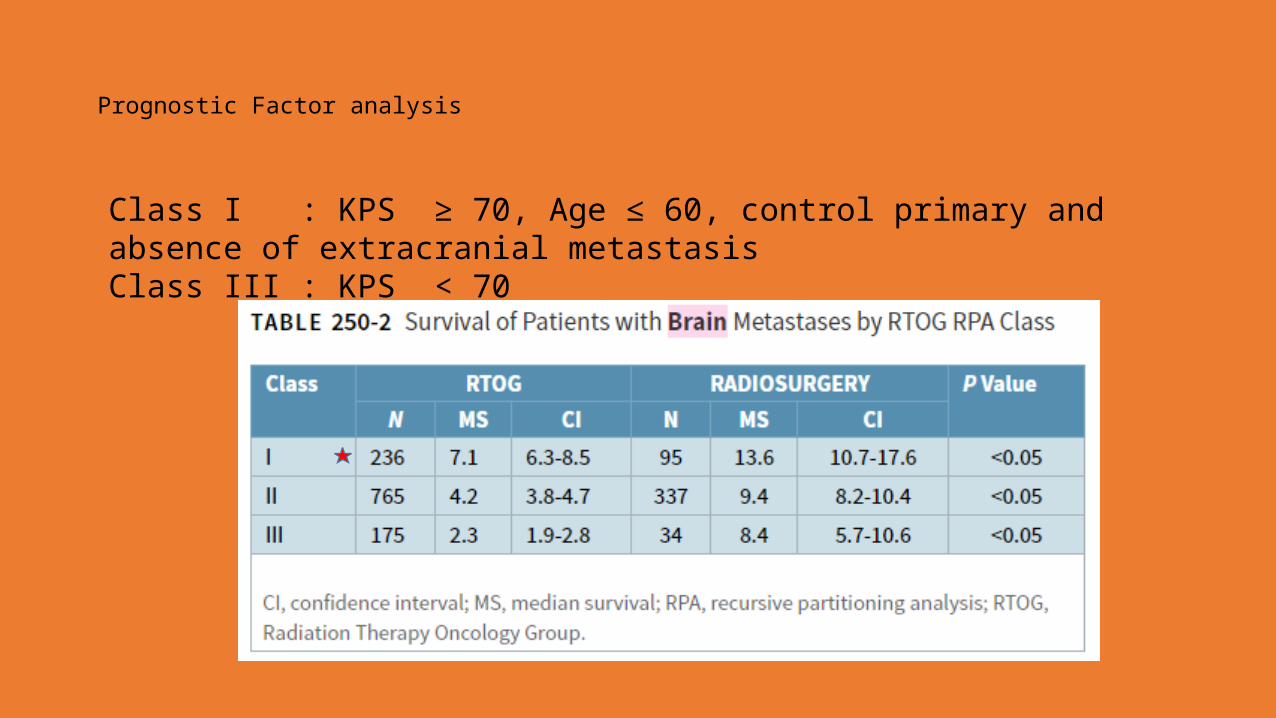
Prognostic Factor analysis
Class I : KPS ≥ 70, Age ≤ 60, control primary and absence of extracranial metastasisClass III : KPS < 70
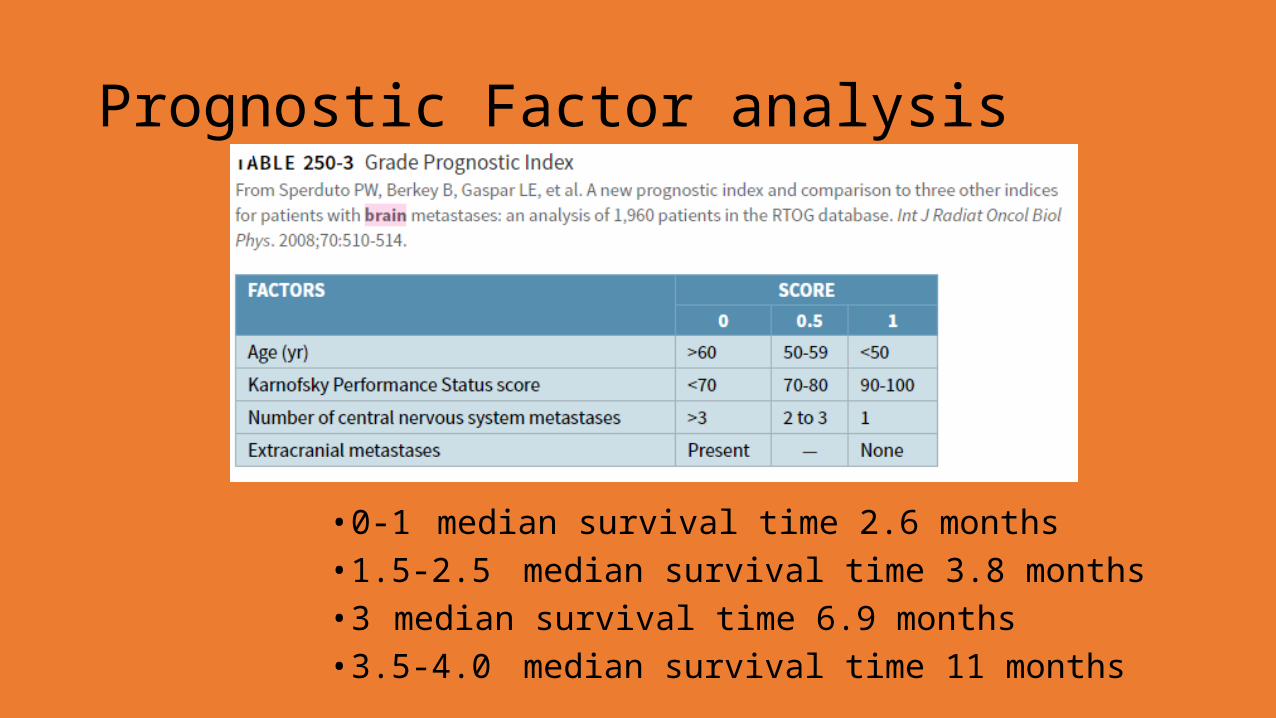
Prognostic Factor analysis
• 0-1 median survival time 2.6 months• 1.5-2.5 median survival time 3.8 months• 3 median survival time 6.9 months• 3.5-4.0 median survival time 11 months

Role of Adjuvant Whole-Brain Radiotherapy
no significant difference in overall survival between the two groups, even though the study was not powered to detect a survival difference
Side Effects of Whole-Brain Radiotherapy• Acute side effect• fatigue, hair loss, particularly along the midline and vertex, erythema, and
otitis
• Months to years side effect• Impairment of neurocognitive function
• Survived longer than 1 yrs• Neurotoxicity with progressive dementia, ataxia and urinary incontinence
• Neurocognitive function factor• presence of brain metastases, neurosurgical interventions, chemotherapy,
and other neurotoxic therapies such as steroids and anticonvulsants
Reirradiation of Brain metastasis• Aggressive, primary treatment interventions to provide durable local
control is obviously preferable to being backed into this unfortunate situation of recurrent intracranial disease with limited treatment options.
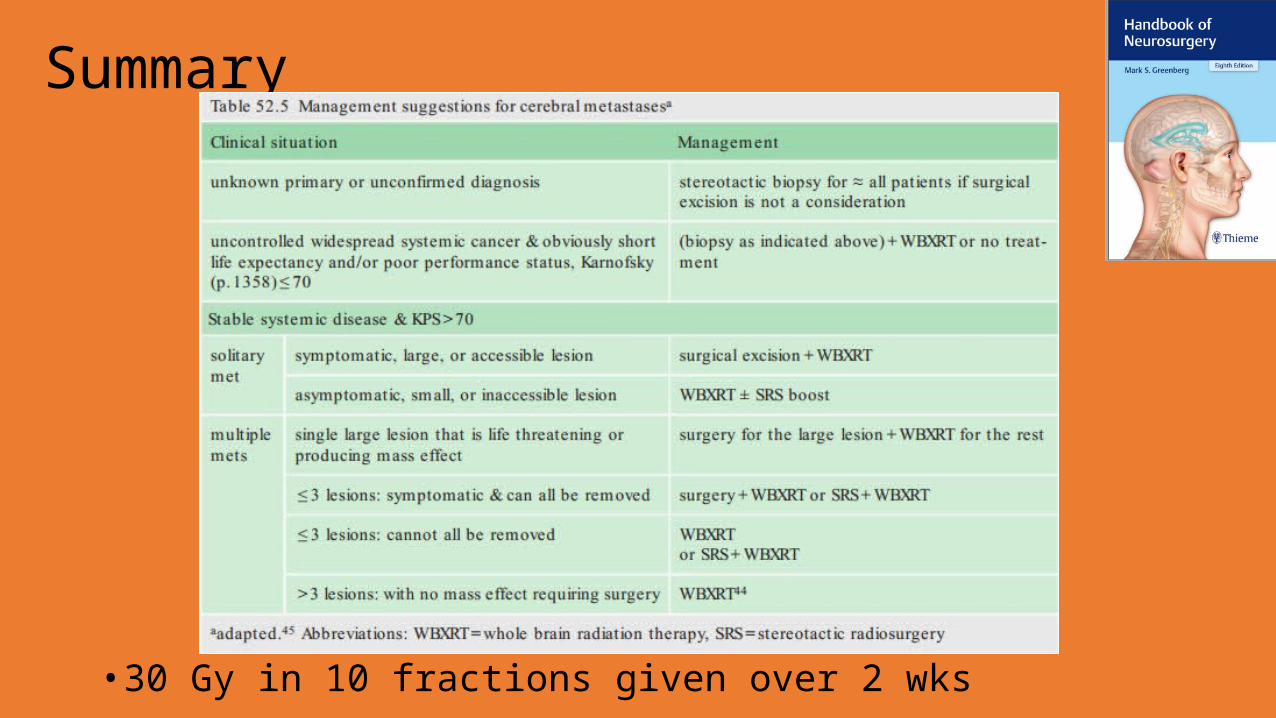
Summary
• 30 Gy in 10 fractions given over 2 wks
Glioblastoma multiforme• Diffusely infiltrative the brain parenchyma• Can’t complete microscopic surgical excision• Grade IV
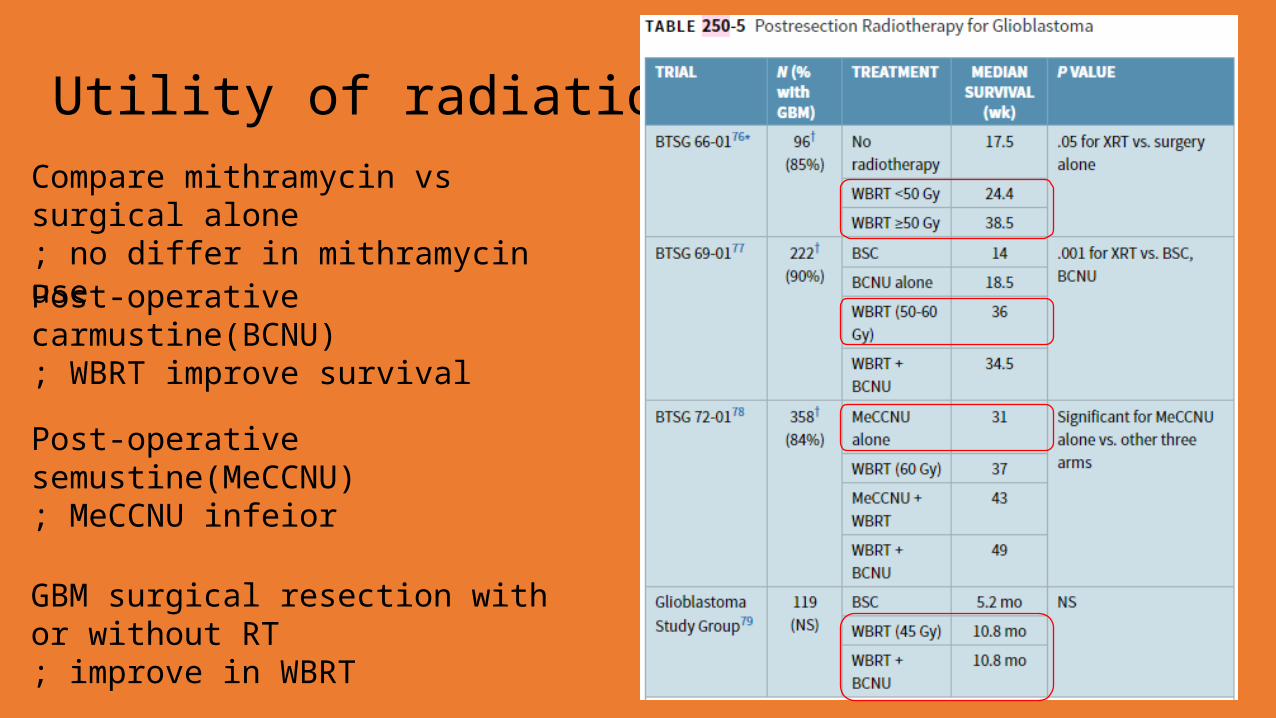
Utility of radiation therapyCompare mithramycin vs surgical alone; no differ in mithramycin use
Post-operative carmustine(BCNU); WBRT improve survival
Post-operative semustine(MeCCNU); MeCCNU infeior
GBM surgical resection with or without RT; improve in WBRT
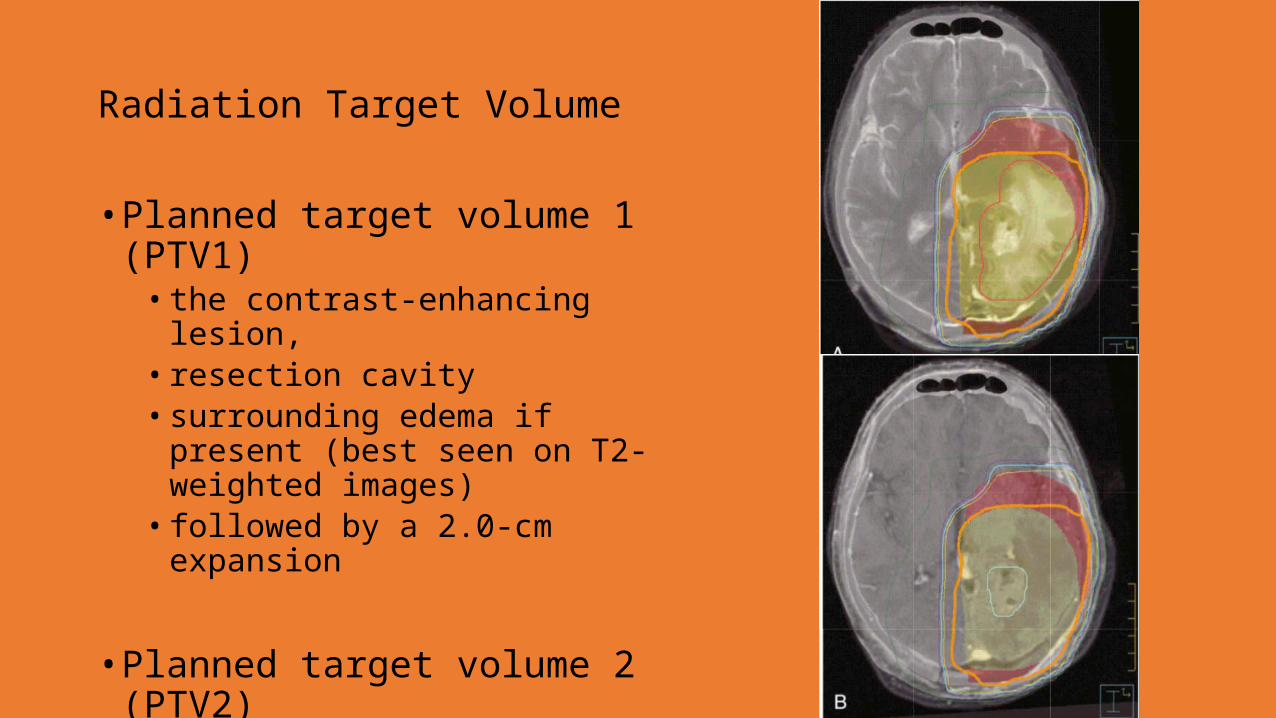
Radiation Target Volume
• Planned target volume 1 (PTV1)• the contrast-enhancing lesion,• resection cavity• surrounding edema if present (best
seen on T2-weighted images)• followed by a 2.0-cm expansion
• Planned target volume 2 (PTV2)• After 46 Gy of radiation• the contrast-enhancing lesion with a
2.5-cm expansion
Recurrence Patterns
• The recurrent tumor that surpassed the outside surface of the PTV was still predominantly centered within the tumor bed• Central or in-field

Dose Escalation
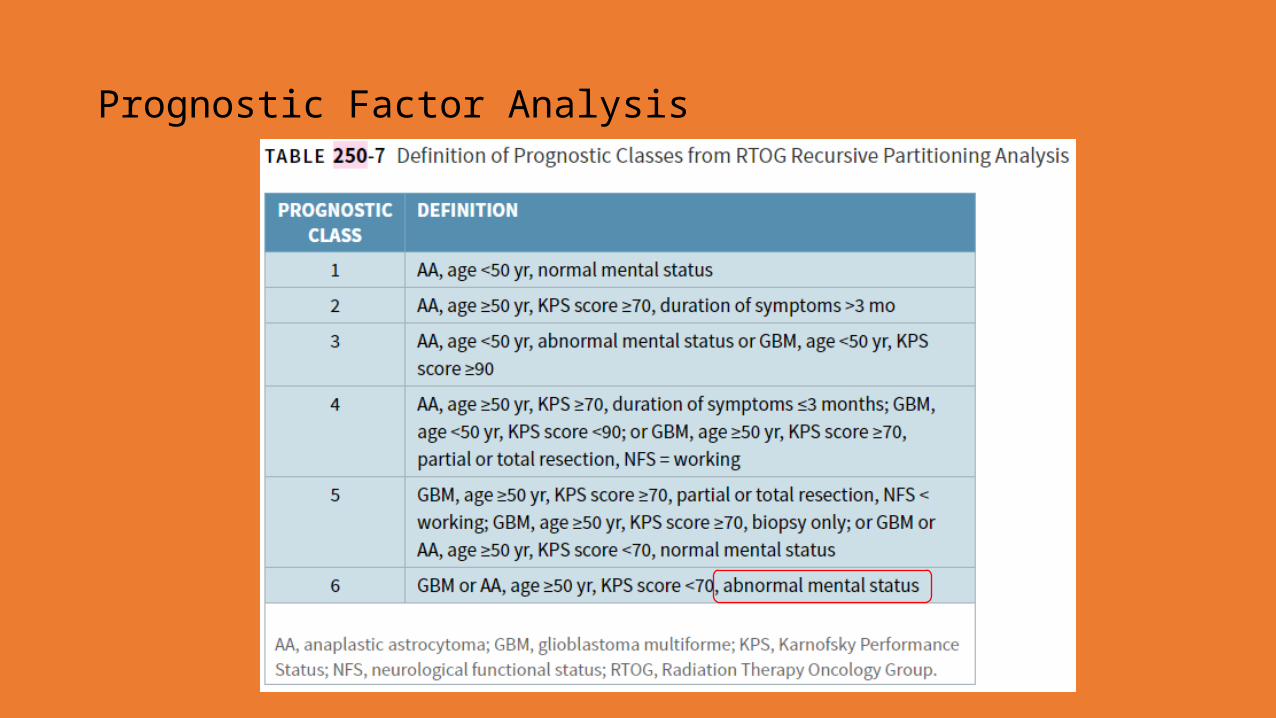
Prognostic Factor Analysis

Prognostic Factor Analysis
Methylguanine-deoxyribonucleic acid methyltransferase (MGMT) methylation has also proved to be a powerful predictor of survival in patients receiving RT and TMZ
Anaplastic Astrocytoma
• Grade III astrocytoma• Median survival in the 2- to 3-year range• Partial brain fields• GTV(Gross total volume) : hypodense edema or T2 abnormality,
contrast-enhancing volume• CTV(Clinical target volume): 2- to 3-cm margin of tissue surrounding
the GTV. • The initial volume is typically treated to 46 Gy and the boost volume
to 60 Gy• Median survival decreased with more aggressive therapy• RT + CMT did not achieve better compare with RT alone
Anaplastic Oligodendroglioma
• Chemotherapy potentially improves PFS, but the effect on survival is not statistically obvious• Patients with 1p and 19q deletions had significantly better outcomes• MGMT promoter methylation : TMZ
Primary central nervous system lymphoma• lymphoma confined to the CNS• Dissemination through the craniospinal axis• Radiosensitive tumor• 40-50 Gy total• Chemotherapy • Younger than 60 yrs,better prognois
Malignant Meningeal Tumors
• Hemangiopericytoma• Slow but progressive radiographic response to ionizing radiation• Significant metastasis : liver, lung, bone and soft tissue• Effetiveness is dubious [Greenberg]
• Malignant meningioma• Aggressive surgical resection followed by postoperative high-dose RT• 5 Yr survival less thans 20%• GTV : expan 1.5-2 cm.• 55-60 Gy [Greenberg]
Primitive Neuroectodermal Tumors
• sheets of small round blue cells with scant cytoplasm• supratentorial PNET, pineoblastoma, medulloblastoma, and
ependymoblastoma• “standard risk” or “high risk”• age, Chang M stage, location, and extent of resection
• Standard-risk patients : • Chang M0 stage disease (no evidence of microscopic or macroscopic
dissemination along the craniospinal axis)• posterior fossa origin• age older than 3 years• less than 1.5-cm2 tumor residual after surgery
Primitive Neuroectodermal Tumors• Craniospinal RT at recommended doses of 36 Gy to the craniospinal
axis and a posterior fossa boost to 54 Gy • 35-40 Gy to whole craniospinal axis + 10-15 Gy boost to tumor
bed(usually posterior fossa) [Greenberg]• Combination chemotherapy given with craniospinal RT continues to
be pursued
Germ Cell Neoplasms
• CNS germinomas have been managed with craniospinal RT• Nongerminomatous germ cell tumors of the CNS, survival is
significantly poorer, and both surgical resection and chemotherapy are the primary modalities of treatment
Complication• Acute : occur during and immediately after completion of a course of
external beam• Acute skin reaction : dry desquamation, erythema• Temporary alopecia• Fatigue• Flash of light• Serous otitis media• Uncommon : Nausea, increase intracranial hypertension
Complication• Subacute : several week of month after complete RT• Lethargy and somnolence• Children : acute somnolence syndrome• N/V, ataxia, dysphagia, cerebellar ataxia• Keratoconjunctivitis• Radiation necrosis : PET or MRS
Complication• Late complication : several month to years• Unclear because short-term survivor• Impairment of intellectual function : memory and mathmetical ability• Dementia, ataxia, confusion

















