59
Fundamentals of Human Neuropsychology, Sixth Edition Chapter 27 Lecture PPT Prepared by Gina Mollet, Adams State College Bryan Kolb & Ian Q. Whishaw’s
| Date post: | 03-Dec-2015 |
| Category: |
Documents |
| Upload: | tiankaunang |
| View: | 213 times |
| Download: | 0 times |

Fundamentals of Human Neuropsychology,Sixth Edition
Chapter 27Lecture PPT
Prepared by Gina Mollet, Adams State College
Bryan Kolb & Ian Q. Whishaw’s

Cha
pter
27
Psychiatric and Related Disorders

Portrait: Losing Touch with Reality
• Mrs. T.– Symptoms of schizophrenia beginning at age
16– Began with self-consciousness and
progressed to delusions and hallucinations– Hallucinations led to bizarre and dangerous
behavior
• PET scans of schizophrenia indicate abnormal blood flow in the prefrontal cortex

The Brain and Behavior
• The mind-body problem– Dualists– Monists
• Psychiatric or behavioral disorders have a biological, anatomical, or genetic basis

Schizophrenia
• DSM-IV R – Delusions or beliefs that distort reality– Hallucinations– Disorganized speech, senseless rhyming– Disorganized, agitated behavior– Blunted emotions, loss of interest and drive

Structural Abnormalities in Schizophrenic Brains
• Less than average weight
• Enlarged ventricles
• Reduction in the number of neurons in the prefrontal cortex
• Abnormal cellular structure in the prefrontal cortex and hippocampus
• Hypofrontality during card sorting


Biochemical Abnormalities in Schizophrenic Brains
• Dopaminergic function– Anti-psychotics
• Act on the dopamine synapse
• Glutamate
• GABA


Types of Schizophrenia
• Type I: Acute Schizophrenia– Positive symptoms– More responsive to neuroleptics (anti-
psychotics)
• Type II: Chronic Schizophrenia– Negative symptoms– Structural abnormalities in the brain

Schizophrenia As a Disorder of Development
• Develops during late adolescence
• Slow emergence of brain abnormalities
• Combination of genetics and environment– No single gene– More likely to have experienced a
combination of adverse events

Neuropsychological Assessment
• Poor performance on long-term verbal and nonverbal memory
• Poor frontal-lobe functioning
• May not perform well on any test

Mood Disorders
• Clinical Depression– Prolonged feelings of worthlessness and guilt– Behavioral slowing– Disrupted eating and sleeping
• Mania– Excessive euphoria– Hyperactivity
• Bipolar disorder– Periods of depression and mania

Neurochemical Aspects of Depression
• Reduction of monoamines• Brain-derived neurotrophic factors (BDNF)
– Downregulated by stress– May affect functioning of monoamine
synapses
• Hypothalamic-Adrenal system (HPA-axis)– Oversecretion of cortisol; chronic stress– Widespread influence on cerebral functioning– Kills granule cells in the hippocampus


Neurochemical Aspects of Depression
• Fluoxetine– SSRI– Stimulates BDNF and neurogenesis in the
hippocampus

Blood Flow and Metabolic Abnormalities in Depression
• Decreased activity in: – Dorsolateral and medial prefrontal regions
• Reduced memory and attention
• Increased activity in: – Orbital regions
• An attempt to inhibit amygdala activity• An attempt to break persistent negative thoughts
– Amygdala• May increase HPA-axis activity
– Medial thalamus

Blood Flow and Metabolic Abnormalities in Depression
• Sleep-cycle– May be altered due to lowered serotonin
levels
• Thyroid-hormone – Decrease in production may influence mood

Neurobiological Aspects of Bipolar Disorder
• Decrease in gray matter in the temporal lobe and cerebellum– Decrease correlates with number of episodes
• Sensitization Model– Bipolar patients are sensitive to stress and
drugs– Episodes of mood disorder change the brain

Snapshot: Cortical Metabolic and Anatomical Abnormalities in Mood Disorders
• Drevets and colleagues– PET images of unipolar and bipolar patients
• 12% decrease in blood flow to the subgenual area• Bipolars exhibit an increase in blood flow during
the manic phase
– MRI images of unipolar and bipolar patients• Reduction in gray matter volume in the left
subgenual area


Neurobiological Aspects of Bipolar Disorder
• Sensitization Model– Genetically predisposed individuals may be
more sensitive– There is a link between psychomotor-
stimulants and mania– Bipolars are at high risk for drug abuse and
may be especially sensitive to the effects

Vitamins, Minerals, and Food
• Kaplan and colleagues– Mood symptoms may be related to:
• Inborn errors in metabolism• Alterations in gene expression• Epigenetic alterations in genes• Long-latency effects of nutritional abnormalities

Psychiatric Symptoms of Cerebral Vascular Disease
• Post-stroke patients– 25-50% experience depression– About 25% experience generalized anxiety
disorder– Catastrophic reactions– 11-50% experience pathological affect

Psychosurgery
• Destruction of a region of the brain to alleviate psychiatric symptoms
• Neurosurgery– Brain surgery intended to repair damage to
alleviate symptoms
• Egas Moniz– Prefrontal lobotomy

Psychosurgery
• Modern Psychosurgery– 13 targets– Smaller lesions– Rarely performed– Does not replace abnormal activity with
normal activity


Motor Disorders
• Hyperkinetic – Increase motor activity
• Hypokinetic– Loss of movement

Hyperkinetic Disorders
• Huntington’s chorea– Genetic disorder– Intellectual deterioration and abnormal
movements– Begins as a reduction of activity and a
restriction of interest– Involuntary movements begin about a year
later


Hyperkinetic Disorders
• Huntington’s chorea– Movements
• Entail whole limbs • Irregular, no pattern• Affect head, face, trunk and limbs
– Behavioral Symptoms• Personality changes• Cognitive impairments• Anxiety, depression, mania, and schizophrenic-like
psychoses

Hyperkinetic Disorders
• Huntington’s chorea– Brain abnormalities
• Shrinkage of the cortex• Atrophy of the basal ganglia• Imbalance among the various neurotransmitter
systems– Death of GABA and ACh neurons in the basal ganglia
• Poor performance on memory and frontal-lobe tests


Tourette’s Syndrome
• Three stages– 1. Multiple tics– 2. Inarticulate cries are added to the tics– 3. Articulate words
• Echolalia: Repeating what others say• Coprolalia: Obscene or lewd speech
• Age of onset: 2-15• Not associated with neuroses, psychoses,
or other disorders

Tourette’s Syndrome
• Subcortical origin– Small cells in the basal ganglia
• Treatment– Antidopaminergic drugs– Norepinephrine receptor agonists
• Abnormalities in cognitive functions supported by the right hemisphere


Hypokinetic Disorders
• Parkinson’s Disease– Degeneration of the substantia nigra– Loss of dopamine– Variety of symptoms that vary from patient to
patient– Symptoms resemble changes in motor activity
that occur with age

Hypokinetic Disorders
• Parkinson’s Disease– Rigidity– Tremor– Akinesia– Postural disturbances

Hypokinetic Disorders
• Parkinson’s Disease: Positive Symptoms– Resting tremor– Muscular rigidity
• Cogwheel rigidity
– Involuntary movements• Akathesia
– Cruel restlessness
• Oculogyric crisis– Involuntary turns of the head and eyes to the side

Hypokinetic Disorders
• Parkinson’s Disease: Negative Symptoms– Disorders of posture
• Disorder of fixation• Disorder of equilibrium
– Disorders of righting– Disorders of locomotion
• Festination
– Disorders of speech– Akinesia

Hypokinetic Disorders
• Progression of Parkinsonism– Begins with tremors in the hand– Face becomes masklike and movement slows– 10-20 years of progression – On-again-off-again quality

Causes of Parkinsonism
• Idiopathic– Familial– Part of the aging process– Viral origin
• Postencephalitic– Occurs after encephalitis

Causes of Parkinsonism
• Drug Induced– Ingestion of major tranquilizers– Contaminant of synthetic heroin (MPTP)– Environmental toxins
• Depletion of dopamine

Treatment of Parkinson’s Disease
• Physical therapy
• Pharmacological therapy– Increase dopamine function– Block cholinergic system
• Stem-cell research
• Deep brain stimulation (DBS)


Psychological Aspects of Parkinson’s Disease
• Cognitive functions– Generalized behavior slowing– Show symptoms similar to individuals with
frontal lobe or basal ganglia lesions– Impaired on the WAIS

Dementia
• DSM-IV-R– Memory and other cognitive deficits– Impairment in social and occupational
functioning
• Degenerative dementias– Intrinsic to the nervous system– Affects the CNS selectively
• Nondegenerative dementias– Diverse etiologies


Dementia
• Alzheimer’s disease– Most prevalent form of dementia– Neuritic Plaques
• Found in the cortex• Positively correlated with cognitive decline• Amyloid surrounded by degenerative cellular
fragments
– Paired Helical Filaments• Found in the cortex and hippocampus

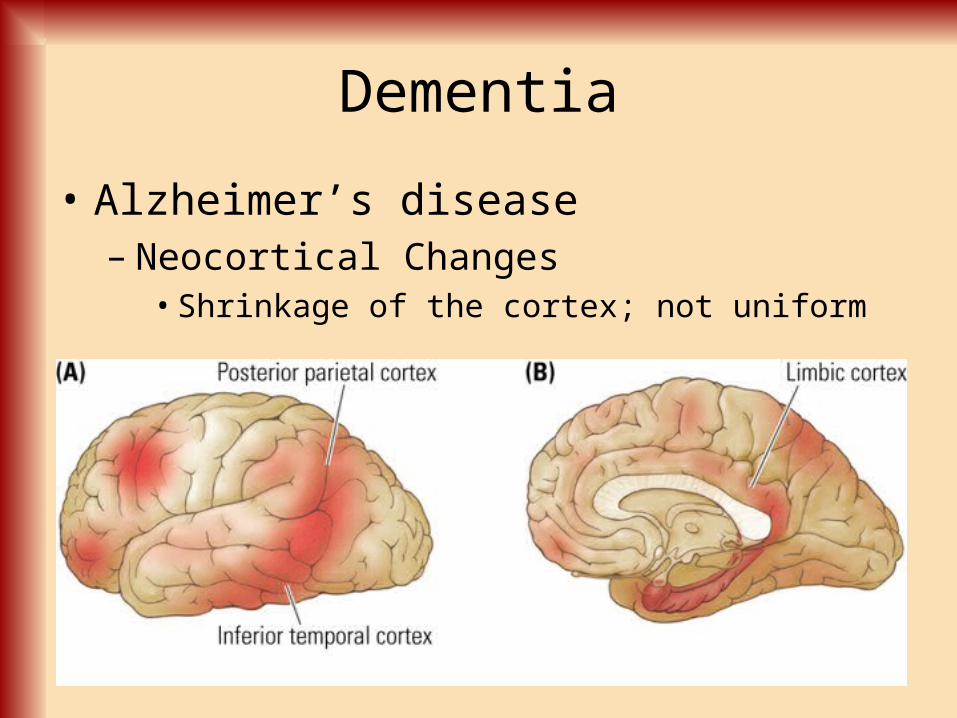
Dementia
• Alzheimer’s disease– Neocortical Changes
• Shrinkage of the cortex; not uniform

Dementia
• Alzheimer’s Disease– Paralimbic cortex changes
• Degeneration of the limbic system and entorhinal cortex
– Cell changes• Shrinking of neurons• Loss of dendritic aborizations


Dementia
• Alzheimer’s Disease– Neurotransmitter changes
• Reduction in two or more transmitter systems• ACh, Noradrenaline, DA, 5-HT, and glutamate
receptors

Putative Causes of Alzheimer’s Disease
• Genetics
• Trace Metals– Increased concentration of aluminum
• Immune Reactions– Antibrain antibodies that cause neuronal
degeneration

Putative Causes of Alzheimer’s Disease
• Blood Flow– Decrease in blood flow to the brain
• Abnormal Proteins– Increased production of abnormal proteins
that accumulate in the brain

Clinical Symptoms and the Progression of Alzheimer’s Disease• Gradual progression
– Recent memory– Remote memory– Ability to recognize family members
• Impairments on the WAIS• Impaired on nearly all tests of memory
– Names of objects and distinguishing among objects in a category
• Language impairments
