Neurosurgery department, Vajira hospital
Evaluation and Management Craniocervical Dissociation Atlantoaxial Rotatory Subluxation Transverse Ligament Injury
Chapter 313 and 314
YOUMANS Neurological Surgery sixth edition
Craniocervical Dissociation
Anatomy of craniovertebral junction
✤ Ligaments of craniovertebral junction (CVJ)
✤ Skull to atlas group
✤ Articular capsule ligaments
✤ Anterior and posterior atlanto-occipital ligament
✤ Lateral atlanto-occipital ligament
✤ Cruciate ligament
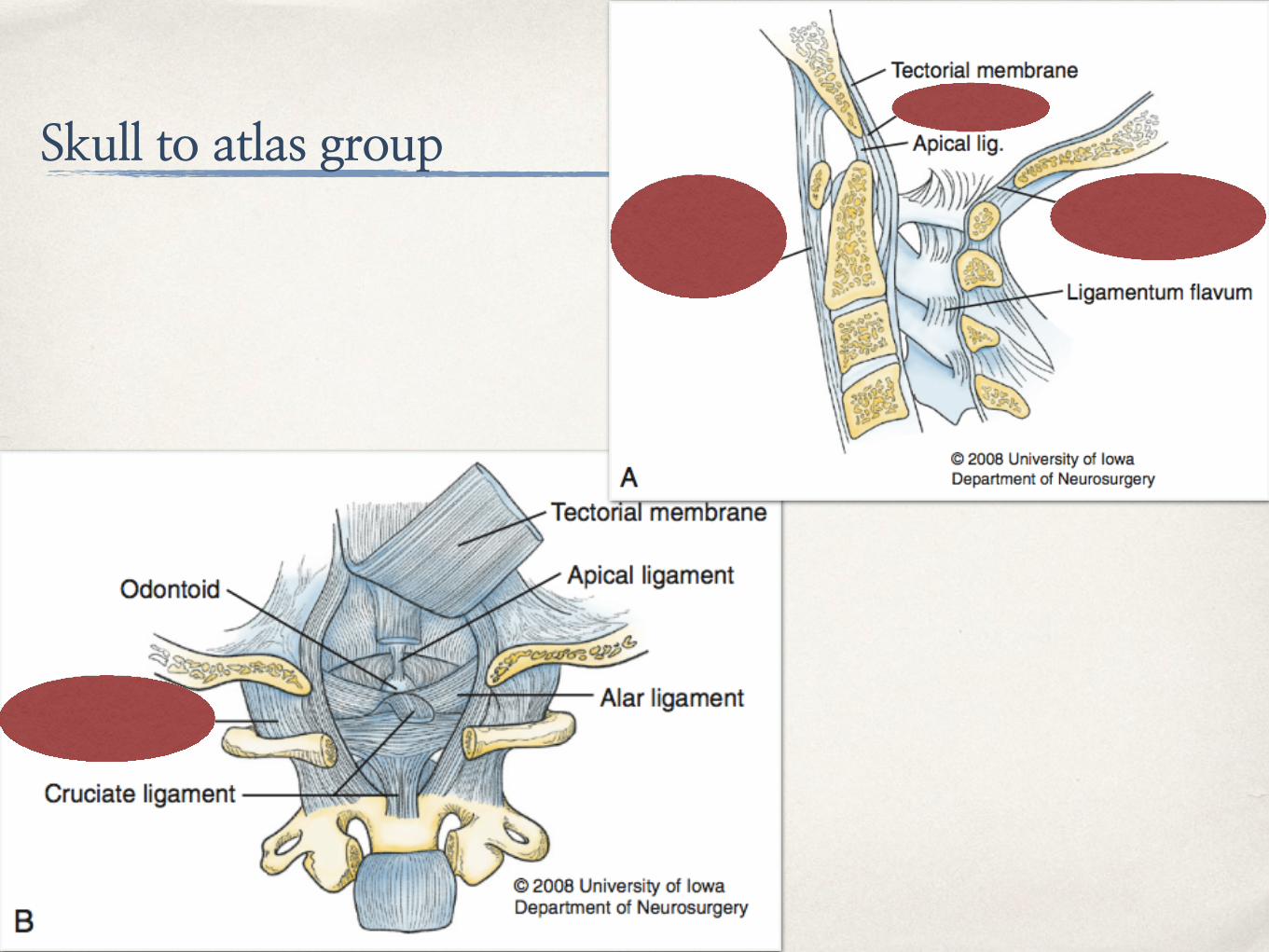
Skull to atlas group
Anatomy of craniovertebral junction
✤ Ligaments of craniovertebral junction (CVJ)
✤ Skull to axis group
✤ Alar ligament
✤ Tectorial membrane
✤ Apical dental ligament
✤ Ligamentum nuchae
Skull to axis group
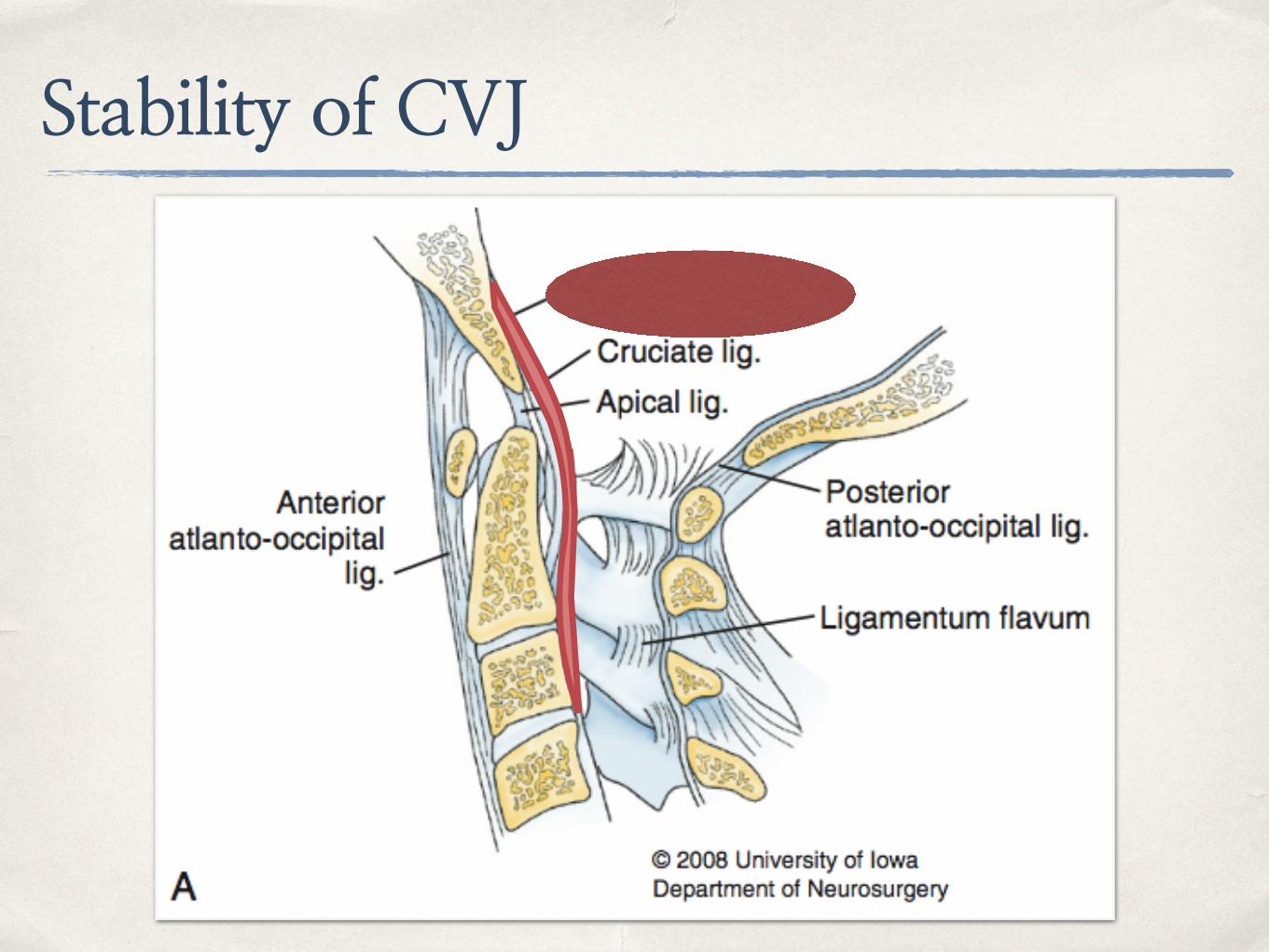
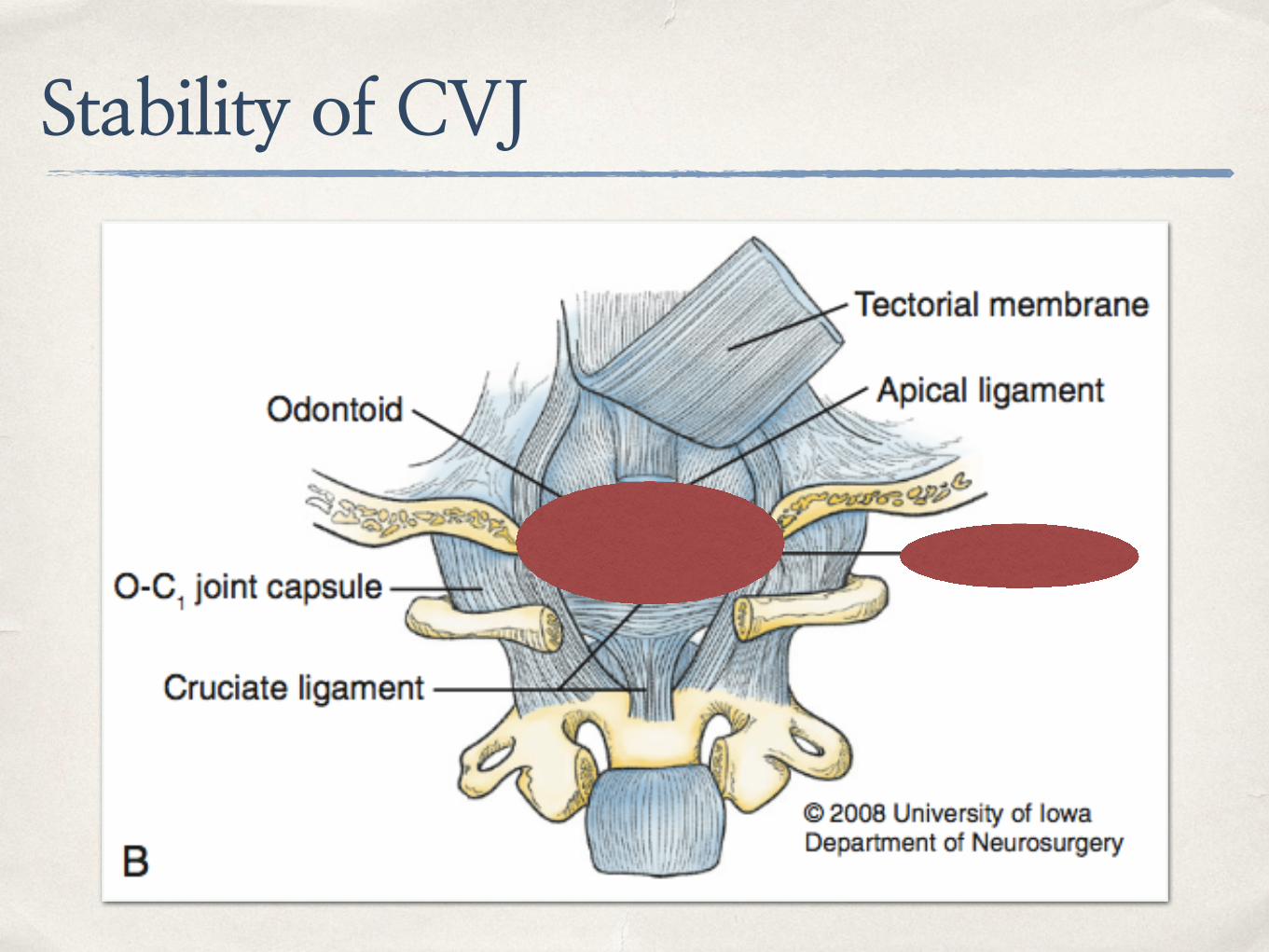
Stability of CVJ
✤ Mainly from skull to axis group of ligaments
✤ Alar ligament
✤ Connect odontoid process to occipital condyles and lateral mass of atlas
✤ Control axial rotation of neck and limit lateral flexion and AP translation
✤ Tectorial membrane (continuation of PLL)
✤ Connect dorsal surface of odontoid process to ventral surface of foramen magnum
✤ Limit hyperextension of neck
✤ Odontoid process to foramen magnum limits hyperflexion of neck
Mechanism of injury
✤ Mechanisms
✤ Hyperextension
✤ Hyperflexion
✤ Lateral flexion
✤ Combined forces
Mechanism of injury
✤ Most common is hyperextension combined with extreme lateral flexion
✤ Hyperextension cause rupture of tectorial membrane
✤ Extreme lateral flexion cause alar ligament injury
✤ Anterior dislocation of cranium to cervical spine
✤ Children are susceptibility to AOD because of
✤ Less stiffness of ligaments
✤ Larger head to body ratio
Clinical findings✤ Most common causes are high-speed motor vehicles accident and
pedestrians injury
✤ Wide range of injury from dead to minor injury
✤ Brainstem injury
✤ Cranial nerve deficit
✤ Spinal cord injury
✤ Cervical nerve roots injury
✤ Anterior spinal a., vertebral a. or carotid a. injury
Clinical findings✤ Steel rules of third at C1 spinal canal
✤ Odontoid process
✤ Spinal cord
✤ CSF space
✤ Cruciate paralysis
✤ Weakness of hands and arms with sparing of lower extremities
✤ True mechanism is still unknown but there are theories
✤ Selective damage to neural areas
✤ Injury to ventral corticospinal tracts
Radiology
✤ Assessment of lateral C-spine plain film for AOD
✤ Basilar line of Wackenheim
✤ Line from posterior surface of clivus to caudal extension
✤ Normal line is attached to posterior tip of odontoid process and not altered by flexion and extension
Wackenheim’s line
Radiology
✤ Assessment of lateral C-spine plain film for AOD
✤ Dens-basion interval
✤ Normal range is below 5mm in adult and 10mm in infant
✤ Unreliable due to wide range of variability in normal population
Radiology
✤ Assessment of lateral C-spine plain film for AOD
✤ Craniovertebral relationships distances (Powers ratio)
✤ BC/OA ratio more than 1.0 indicate AOD (normal is 0.77)
✤ Unreliable in congenital anomaly or atlas fracture
Basion
Posterior arch of C1
Opisthion
Anterior arch of C1
Powers ratio
Radiology
✤ Assessment of lateral C-spine plain film for AOD
✤ Basion-posterior axial line interval (BAI) and basion-dental interval (BDI) (Harris rule-of-12)
✤ Abnormal is more than 12mm (~95%)
✤ Universally acceptable and most accuracy
✤ BDI is unreliable in age below 13 years
BAI
BDI
Harris rule-of-12
Children atlantooccipital dissociation (AOD) By Pang and colleagues
✤ Condylar-C1 interval (CCI)
✤ Distance between occipital condyle to lateral mass of C1
✤ Assess by CT scan
✤ Normal value is 1.28mm (sensitivity 100%)
PANG ET AL. NEUROSURGERY | VOLUME 61 | NUMBER 5 | NOVEMBER 2007
Classification of craniocervical dissociation
✤ Assess by lateral C-spine plain film or CT scan
✤ 3 types
✤ Type I : Anterior displacement of occiput to atlas
✤ Type II : Longitudinal distraction with seperation of occiput to atlas
✤ Type III : Posterior displacement of occiput to atlas
Classification of craniocervical dissociation
Type I Type II Type III
Treatment considerations
✤ Emergency considerations
✤ Awareness of craniocervical dissociation
✤ Cardiopulmonary support
✤ Spinal immobilisation
✤ Surgical removal of hematoma at CVJ (rare condition) if hematoma associated with neurological deficit
Treatment considerations
✤ Skull traction
✤ Recommended in patients of Type I and III dislocation with neurological deficit
✤ Fluoroscopic-guided for applied traction is recommended
✤ Traction weight below 5 lb.
✤ If clinical improved >> decrease weight to 1-2 lb. or halo vest applied
✤ Contraindication in Type II dislocation and rotatory subluxation
Treatment considerations
✤ Surgical management
✤ Posterior fusion of occiput to C2 is recommended in most cases of AOD
✤ Main injury is ligaments and stability cannot maintain after external fixation
✤ Should be done after medically stable
✤ Some surgeon recommended posterior fusion without skull traction first
Atlantoaxial Rotatory Subluxation and Transverse Ligament Injury
Anatomy and Biomechanics of Atlantoaxial joint
✤ Atlantoaxial joint is mainly functionally as neck rotation
✤ Facet joint of C1-2 is horizontal
✤ Stability of C1-2 joint is from ligamentous structures
✤ Transverse ligament : Prevent excessive translation of atlas to axis
✤ Alar ligament : Limit rotation of atlas on axis and secondary translation stabiliser (from transverse ligament)
✤ Vertebral artery runs in transverse foramenSchmidek & Sweet operative neurosurgical techniques
Diagnosis
✤ Sign and symptom of AARS
✤ “Cock-robin” position of neck : head tilted one side and rotated to contralateral side with flexion of neck
✤ Occipital pain from compression of occipital nerve or C2 nerve root
✤ Posterior fossa syndrome from stretching or kinking of vertebral arteries
Diagnosis
tidsskriftet.no
Diagnosis
✤ Imaging
✤ Open-mouth plain film show asymmetrical of lateral of C1 to odontoid process
✤ Lateral plain film show lateral mass of C1 projecting anterior to odontoid process >> “wink” sign
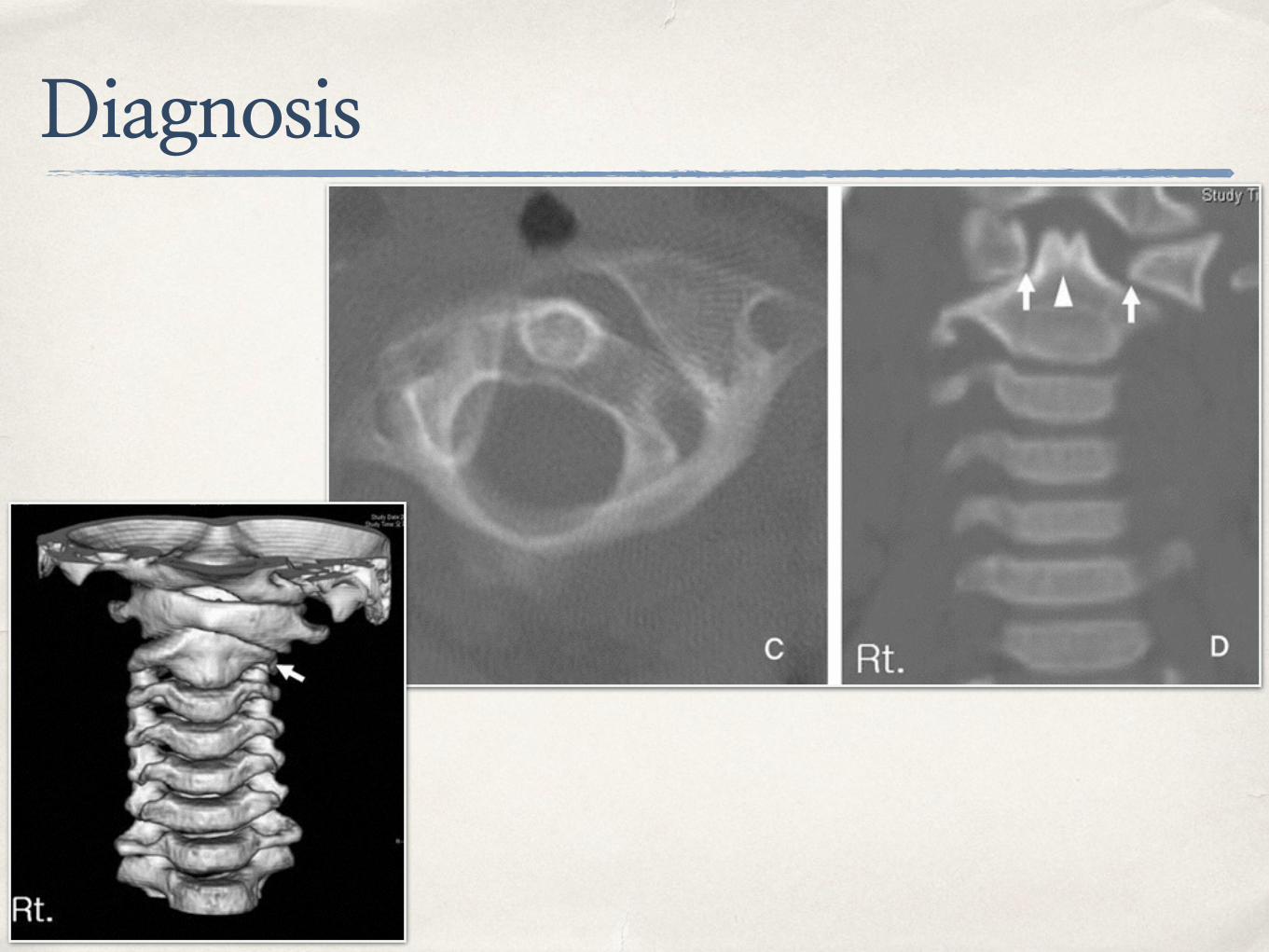
Diagnosis
✤ Imaging
✤ Cervical spine CT is recommended for diagnosis of AARS
✤ Contrast injection for evaluating of vertebral artery
✤ MRI can be used for evaluating of transverse ligament and cord compression
Classification system
✤ Fielding system (1977)
✤ Type I : Intact odontoid and transverse ligament with disrupt of alar ligament
✤ Type II : Anterior translation of atlas on axis 3-5mm with disrupt of transverse ligament
✤ Type III : Anterior translation of atlas on axis > 5mm with disrupt of transverse ligament
✤ Type IV : Posterior displacement of atlas on axis and odontoid process is injured
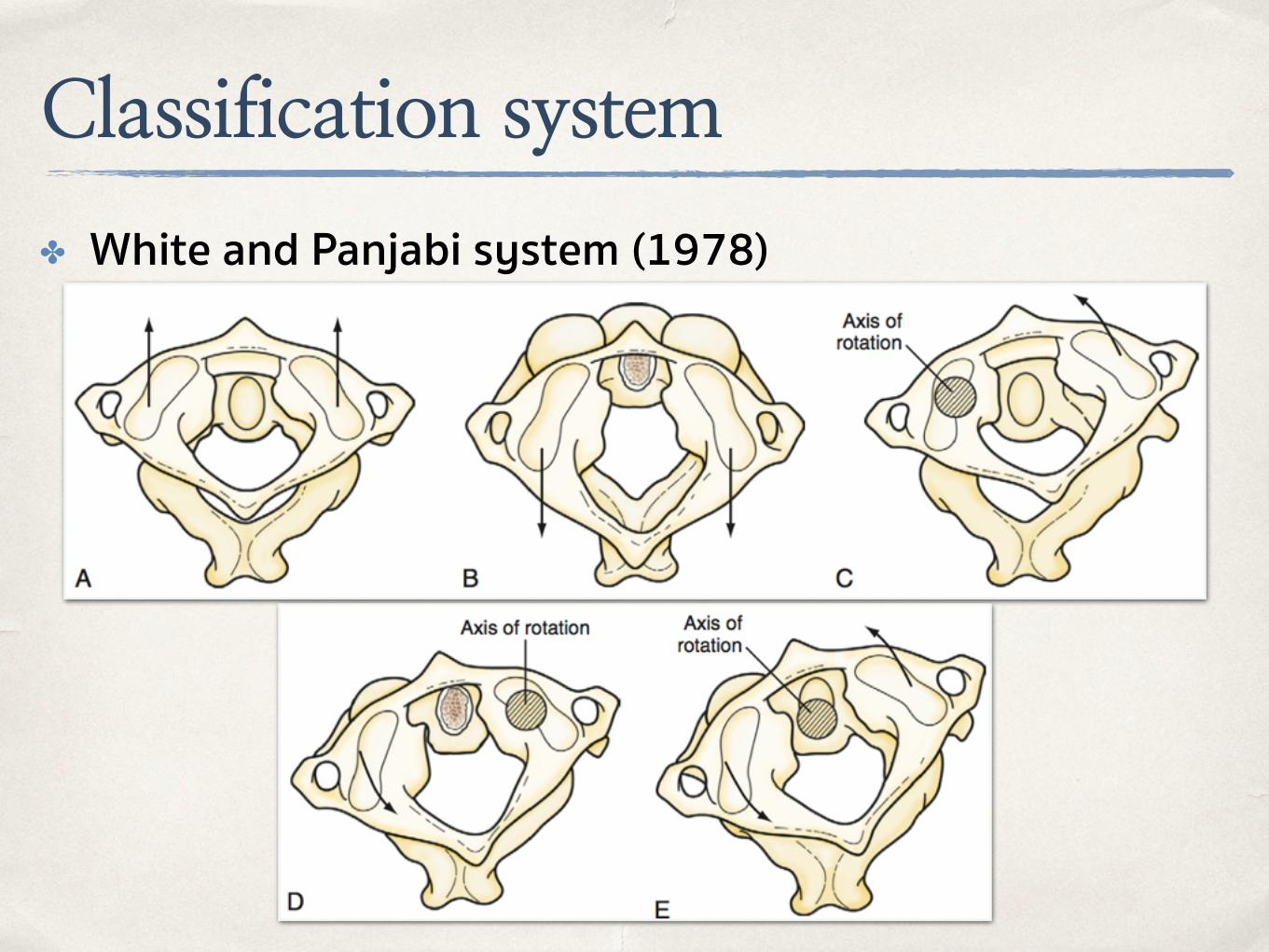
Classification system
✤ White and Panjabi system (1978)
Classification system
Grisel’s Syndrome✤ Nontraumatic atlantoaxial subluxation (rare condition)
✤ Caused by infection process or head and neck procedure
✤ Edema (inflammation process) and relaxation of ligamentous structures
✤ In children with Down’s syndrome and Klippel-Feil syndrome increase risk of Grisel’s syndrome
✤ Management
✤ Reduction by cervical traction with muscle relaxant
✤ Antibiotic prophylaxis in high risk group
✤ Surgical fusion if failed conservative treatment
Management of AARS
✤ Conservative treatment
✤ Cervical traction by Gardner-Wells tong or halo ring with conscious sedation
✤ Bone fracture must be ruled out before traction application
✤ Patient with minor ligamentous injury should be placed in halo vest for 3 months
✤ Failure of conservative treatment or gross instability, surgical fusion should be done
Management of AARS
✤ Surgical treatment
✤ Reducible deformity >> only posterior fixation with fusion
✤ Irreducible deformity >> Anterior decompression with posterior fusion
✤ Anterior decompression
✤ Transoral route with soft tissue and longus colli muscles stripped from bone with/without anterior arch of C1 resection
Posterior C1-2 fusion techniques
✤ Magerl and Seemann technique (1979)
✤ Transarticular screw fixation technique
✤ No need for halo immobilisation postoperative
✤ High risk for vertebral artery injury
Posterior C1-2 fusion techniques
✤ Harms and Melcher technique
✤ Lateral mass screw in C1
✤ Pedicular screw in C2
✤ Connect with rod
Posterior C1-2 fusion techniques
✤ Wright technique
✤ Translaminar fixation technique of C2
✤ Low risk for vertebral artery injury
C1
C2