2
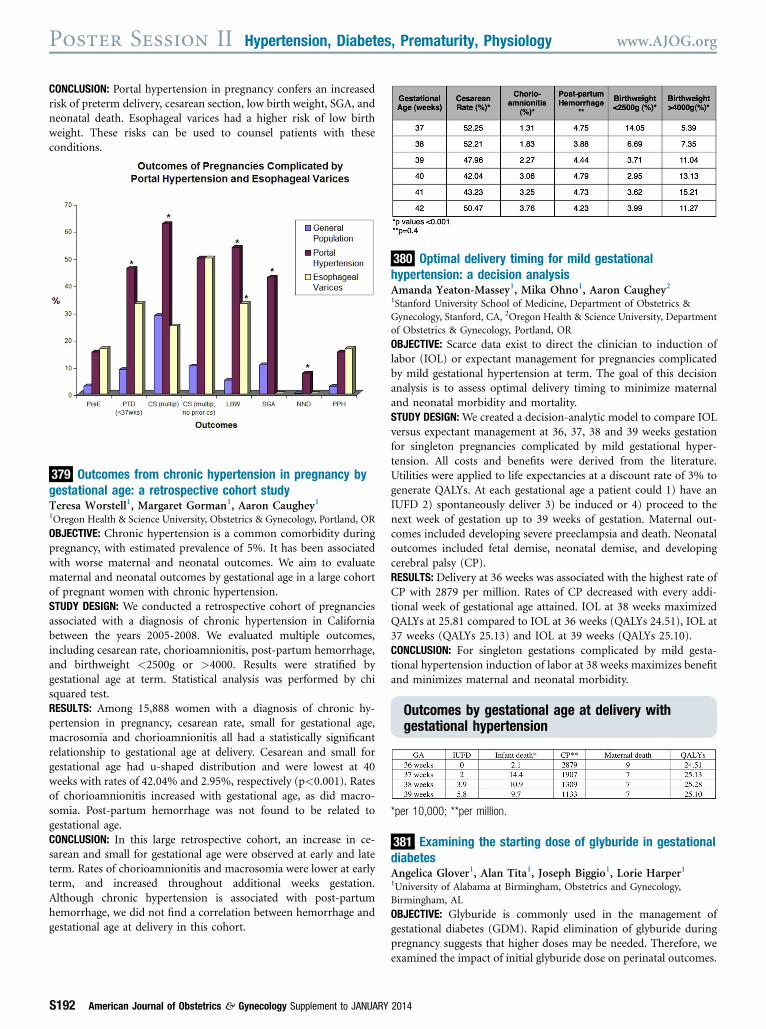
CONCLUSION: Portal hypertension in pregnancy confers an increased risk of preterm delivery, cesarean section, low birth weight, SGA, and neonatal death. Esophageal varices had a higher risk of low birth weight. These risks can be used to counsel patients with these conditions. 379 Outcomes from chronic hypertension in pregnancy by gestational age: a retrospective cohort study Teresa Worstell 1 , Margaret Gorman 1 , Aaron Caughey 1 1 Oregon Health & Science University, Obstetrics & Gynecology, Portland, OR OBJECTIVE: Chronic hypertension is a common comorbidity during pregnancy, with estimated prevalence of 5%. It has been associated with worse maternal and neonatal outcomes. We aim to evaluate maternal and neonatal outcomes by gestational age in a large cohort of pregnant women with chronic hypertension. STUDY DESIGN: We conducted a retrospective cohort of pregnancies associated with a diagnosis of chronic hypertension in California between the years 2005-2008. We evaluated multiple outcomes, including cesarean rate, chorioamnionitis, post-partum hemorrhage, and birthweight <2500g or >4000. Results were stratified by gestational age at term. Statistical analysis was performed by chi squared test. RESULTS: Among 15,888 women with a diagnosis of chronic hy- pertension in pregnancy, cesarean rate, small for gestational age, macrosomia and chorioamnionitis all had a statistically significant relationship to gestational age at delivery. Cesarean and small for gestational age had u-shaped distribution and were lowest at 40 weeks with rates of 42.04% and 2.95%, respectively (p<0.001). Rates of chorioamnionitis increased with gestational age, as did macro- somia. Post-partum hemorrhage was not found to be related to gestational age. CONCLUSION: In this large retrospective cohort, an increase in ce- sarean and small for gestational age were observed at early and late term. Rates of chorioamnionitis and macrosomia were lower at early term, and increased throughout additional weeks gestation. Although chronic hypertension is associated with post-partum hemorrhage, we did not find a correlation between hemorrhage and gestational age at delivery in this cohort. 380 Optimal delivery timing for mild gestational hypertension: a decision analysis Amanda Yeaton-Massey 1 , Mika Ohno 1 , Aaron Caughey 2 1 Stanford University School of Medicine, Department of Obstetrics & Gynecology, Stanford, CA, 2 Oregon Health & Science University, Department of Obstetrics & Gynecology, Portland, OR OBJECTIVE: Scarce data exist to direct the clinician to induction of labor (IOL) or expectant management for pregnancies complicated by mild gestational hypertension at term. The goal of this decision analysis is to assess optimal delivery timing to minimize maternal and neonatal morbidity and mortality. STUDY DESIGN: We created a decision-analytic model to compare IOL versus expectant management at 36, 37, 38 and 39 weeks gestation for singleton pregnancies complicated by mild gestational hyper- tension. All costs and benefits were derived from the literature. Utilities were applied to life expectancies at a discount rate of 3% to generate QALYs. At each gestational age a patient could 1) have an IUFD 2) spontaneously deliver 3) be induced or 4) proceed to the next week of gestation up to 39 weeks of gestation. Maternal out- comes included developing severe preeclampsia and death. Neonatal outcomes included fetal demise, neonatal demise, and developing cerebral palsy (CP). RESULTS: Delivery at 36 weeks was associated with the highest rate of CP with 2879 per million. Rates of CP decreased with every addi- tional week of gestational age attained. IOL at 38 weeks maximized QALYs at 25.81 compared to IOL at 36 weeks (QALYs 24.51), IOL at 37 weeks (QALYs 25.13) and IOL at 39 weeks (QALYs 25.10). CONCLUSION: For singleton gestations complicated by mild gesta- tional hypertension induction of labor at 38 weeks maximizes benefit and minimizes maternal and neonatal morbidity. Outcomes by gestational age at delivery with gestational hypertension *per 10,000; **per million. 381 Examining the starting dose of glyburide in gestational diabetes Angelica Glover 1 , Alan Tita 1 , Joseph Biggio 1 , Lorie Harper 1 1 University of Alabama at Birmingham, Obstetrics and Gynecology, Birmingham, AL OBJECTIVE: Glyburide is commonly used in the management of gestational diabetes (GDM). Rapid elimination of glyburide during pregnancy suggests that higher doses may be needed. Therefore, we examined the impact of initial glyburide dose on perinatal outcomes. Poster Session II Hypertension, Diabetes, Prematurity, Physiology www.AJOG.org S192 American Journal of Obstetrics & Gynecology Supplement to JANUARY 2014