Introduction of the Client Encik Ahmad (not his real name) is a 56-year-old Malay man living in Km. 12 Air Molek, Melaka. He is admitted in General Hospital Malacca on 09 January 2011 at 10:20 AM at male medical ward 3-4. For the past 2 days he was complaining of shortness of breath upon exertion, orthopneic, sore throat and is havinga productive cough with whitish sputum. The wife was worried of these symptoms because his medical history, decided to go to Hospital Malacca. Upon examining, his physician advised him to be admitted to undergo further investigation. Encik Ahmad has no chest pain, palpitation, syncope attach, loss of consciousness, diarrhoea, abdominal pain, nausea, vomiting, headacheand no other upper respiratory and urinary tract infections. His sputum has no blood stain and tolerating orally well and passing out urine and bowel are normal. Clinical Examination On examination, Encik Ismail sitting blood pressure was 138/92 mmHg, his pulse and respiratory rates were 82 bpm and 16 breaths per min., respectively. His body temperature was 37.1°C; sPO2 was 96% on 3L/min nasal prong oxygen and blood glucose level of 17.6mmol/L. Encik Ismail was alert, conscious, can speak in full sentences, pink, and his hydration was good and not tachypneic. His Cardio Vascular System showed S 1 S 2 Dual Rhythm No Murmur, lung has bibasal crept more on right side, no rhenchi, air entry is equal for both sides. Jugular vein pressure His abdomen was soft System showed normal. Case Study on Pleural Effusion1 | Page
Transcript
Introduction of the Client
Encik Ahmad (not his real name) is a 56-year-old Malay man living in Km. 12 Air Molek, Melaka. He is admitted in General Hospital Malacca on 09 January 2011 at 10:20 AM at male medical ward 3-4. For the past 2 days he was complaining of shortness of breath upon exertion, orthopneic, sore throat and is havinga productive cough with whitish sputum. The wife was worried of these symptoms because his medical history, decided to go to Hospital Malacca. Upon examining, his physician advised him to be admitted to undergo further investigation.
Encik Ahmad has no chest pain, palpitation, syncope attach, loss of consciousness, diarrhoea, abdominal pain, nausea, vomiting, headacheand no other upper respiratory and urinary tract infections. His sputum has no blood stain and tolerating orally well and passing out urine and bowel are normal.
Clinical Examination
On examination, Encik Ismail sitting blood pressure was 138/92 mmHg, his pulse and respiratory rates were 82 bpm and 16 breaths per min., respectively. His body temperature was 37.1°C; sPO2 was 96% on 3L/min nasal prong oxygen and blood glucose level of 17.6mmol/L.
Encik Ismail was alert, conscious, can speak in full sentences, pink, and his hydration was good and not tachypneic. His Cardio Vascular System showed S1S2 Dual Rhythm No Murmur, lung has bibasal crept more on right side, no rhenchi, air entry is equal for both sides. Jugular vein pressure His abdomen was soft System showed normal.
Diagnosis
After a series of investigation, Encik Ismail was diagnosed with cardiomegaly, fluid overload in CCF secondary to non-compliance to fluid restriction and right and left pleural effusionsecondary to hypertension.
Medical History
Encik Ismail is a patient with complicated diseases. He is having hypertension for 1 year, an insulin dependent for 10 years, right side hemiparesis, and has ischemic heart failure with triple vessel disease. He has done angiogram clone in IJN and on follow up since November 2010.
He is on the following medication for the above diseases and claimed compliance to it but daughter said he is not complying with fluid restriction:
Case Study on Pleural Effusion1 | P a g e
Chest x-ray showing bilateral pleural effusion
1. S/C Humulin 30/70 2. T. Simvastatin 40 mg ON3. T. Aspirin 150 mg OD4. T. Isordil 10 mg TDS5. T. Vastarel 20 mg TDS6. T. Clinidogrel 75 mg OD7. T. Bisoprolol 1.25 mg OD8. T. Digoxin 0.0625 mg OD9. C. Gemtobrozil 300 mg ON10. T. Frusemide 40 mg BD
He also had a multiple admission due to chest pain at same hospital and his last admission was December 2010 of which he was treated with stable angina.
Surgical History
Encik Ahmad also has a bilateral basal knee amputation. His right leg was amputated 10 years ago while his left leg was amputated 4 years ago.
Family History
Both parents of Encik Ahmad have a medical history of diabetes mellitus and hypertension and heart problem. His brothers and sisters inherited the same. His wife is having hypertension and claimed that his children are all healthy.
Social History
Encik Ismail was previously working as Chef to Selangor Royal Family. He has 7 children and currently staying with his wife and 2 children. Other children are married, working and staying on their own. He is non-smoker, non-alcohol drinker and never use any prohibited drugs before. Due to his condition (right side hemiparesis and amputated legs) he is semi dependent in doing his activities of daily living. He also has financial support from the social welfare of RM150.00/month.
Food and Drug Allergies
Encik Ismail has noknown allergies.
Case Study on Pleural Effusion2 | P a g e
ASSESSMENT OF ACTIVITIES OF DAILY LIVING (ADL)
Case Study on Pleural Effusion3 | P a g e
Patient's Name : Encik AhmadRegistration No.: 679010
DATEACTIVITIES OF DAILY LIVING PATIENT'S PROBLEM
What pateint can or cannot perform by herself/himself ACTUAL/POTENTIAL
09.1.11 Maintaining a safe environment
to 14.1.11
Bed and bed side rail are always locked and up after each procedure/s.
Risk for injury related to right hemeparesis and loss of extremities.
Communication
Patient is able to talk clear and in full sentences.
Breathing
Patient is having short of breath especially during exertion.
Breathing pattern impairment related to pleural fluid build-up.
Eating and Drinking Risk for body nutrition excess related to high glucose level.
Patient can eat and drink by himself and is tolerating orally well.
Eliminating Patient is on bed pan and urinal Self care deficit: elimination
related to limited mobility as evidence by patient is having right hemeparesis and below knees amputation.
Personal cleaning and dressing Patient needs help in bathing, washing and
dressing himself due to right side hemeparesis.Bathing/hygiene deficit related to loss of ability to use the right arm and hand as evidence by patient is having right hemeparesis.
Controlling body temperature
Case Study on Pleural Effusion4 | P a g e
Patient is afebrile during his stay in the hospital Risk for infection related to pleural tapping.
Mobility Patient needs help in moving around. Wife always
around to help.Impaired physical mobility related to right hemeparesis and loss of extremities.
Sleep Sleep on and off due to cough. Disturbed sleep pattern
related to coughing and SOB.
Working and Playing
Patient's entertainment are reading newspaper, watching tv, sitting on wheelchair outside his house and doing physiotheraphy exercise.
Disturbed body image related to amputation of both lower legs
Sexuality Patient's wife still alive. Sexuality dysfunction
related to right hemeparesis and BKA
Dying NIL NIL
PLEURAL EFFUSION
Case Study on Pleural Effusion5 | P a g e
Introduction of Disease
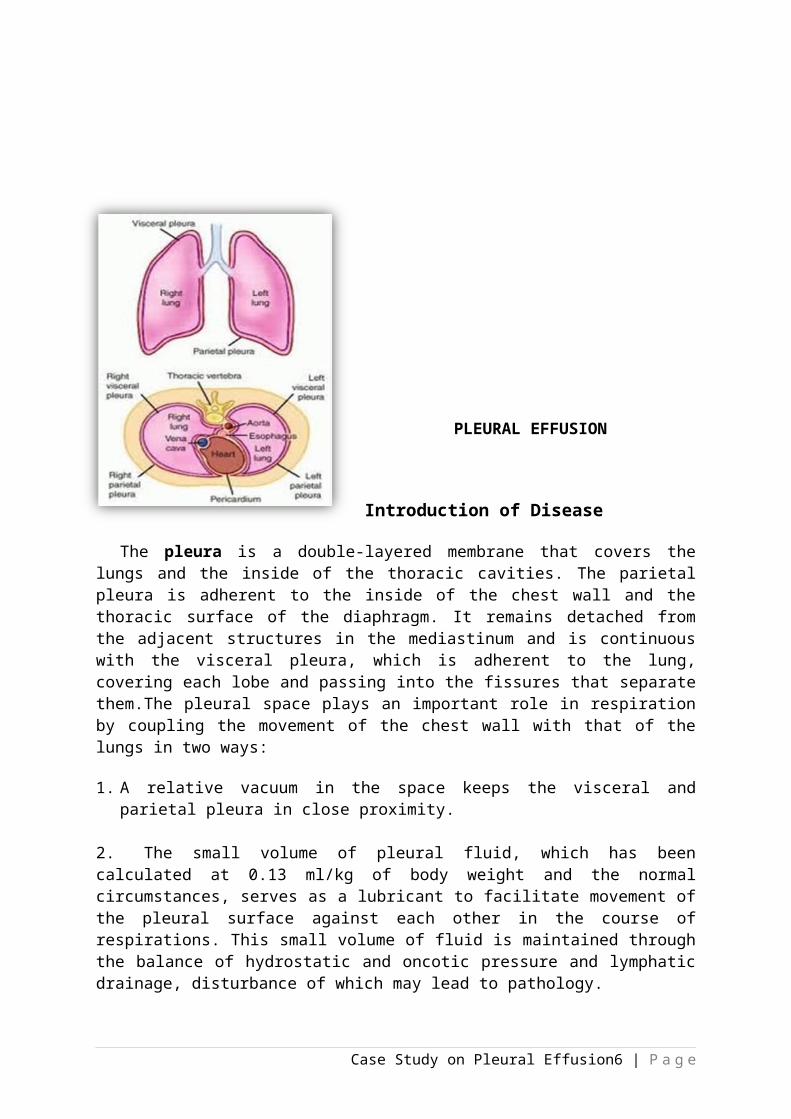
The pleura is a double-layered membrane that covers the lungs and the inside of the thoracic cavities. The parietal pleura is adherent to the inside of the chest wall and the thoracic surface of the diaphragm. It remains detached from the adjacent structures in the mediastinum and is continuous with the visceral pleura, which is adherent to the lung, covering each lobe and passing into the fissures that separate them.The pleural space plays an important role in respiration by coupling the movement of the chest wall with that of the lungs in two ways:
1. A relative vacuum in the space keeps the visceral and parietal pleura in close proximity.
2. The small volume of pleural fluid, which has been calculated at 0.13 ml/kg of body weight and the normal circumstances, serves as a lubricant to facilitate movement of the pleural surface against each other in the course of respirations. This small
volume of fluid is maintained through the balance of hydrostatic and oncotic pressure and lymphatic drainage, disturbance of which may lead to pathology.
An abnormal collection of this pleural fluid in the pleural spaces more than 0.13 ml/kg of body weight is called,pleural effusion.This can either be a result from a systemic disorders or local diseases. Systemic disorders include heart failure, liver or renal diseases and connective disorders, like rheumatoid arthritis and systemic lupus erythematosus (SLE). Local diseases include pneumonia, atelectasis, tuberculosis, lung cancer, and trauma.
Pleural Effusion is not often a primary disease process; it is usually a secondary to other processesas mentioned above.
Pathophysiology
Case Study on Pleural Effusion6 | P a g e
Pleural effusion is an indicator of an underlying disease process that may be pulmonary or non-pulmonary in origin, acute or chronic.
Normally, pleural fluid has the following characteristics:
Clear ultrafiltrate of plasma that originates from the parietal pleura pH 7.60-7.64 protein contain less than 2% (1-2g/dL) fewer than 1000 WBCs per cubic millimetre
glucose contain similar to that of plasma lactate dehydrogenase (LDH) less than 50%
of plasma sodium, potassium and calcium concentration
similar to that of the interstitial fluid
Excess pleural fluid can either be in the form of exudate and transudate. Exudate, is a protein-rich fluid, developed when the blood vessels leak caused by inflammation of the pleura and when the patient is having infection or systemic inflammation.
Transudate on the other hand, is formed when the pressure is high or plasma protein content is low in the blood vessels, the fluid leaks into the
pleural space. It is commonly caused by heart failure and may also accompany renal failure, nephritis, liver failure and malignancy.
Moreover, the following processes play a role in the increased production of pleural fluid:
Altered permeability of the pleural membranes(e.g., inflammation, malignancy, pulmonary embolus)
Reduction in intravascular oncotic pressure(e.g., hypoalbuminemia, cirrhosis)
Increase capillary permeability or vascular disruption(e.g., trauma, malignancy, inflammation, infection, pulmonary infarction, drug hypersensitivity, uraemia, pancreatitis)
Increase capillary hydrostatic pressure in the systemic and/or pulmonary circulation (e.g., CHF, superior vena cava syndrome)
Reduction of pressure in the pleural space, preventing full lung expansion(e.g., extensiveatelectasis, mesothelioma)
Decrease lymphatic drainage or complete blockage, including thoracic duct obstruction or rupture (e.g., malignancy, trauma)
Increase peritoneal fluid, with migration across the diaphragm via lymphatic or structural defect (e.g., cirrhosis, peritoneal dialysis)
Case Study on Pleural Effusion7 | P a g e
Movement of fluid from pulmonary oedema across the visceral pleura
Persistent increase in pleural fluid oncotic pressure from an existing pleural effusion, causing for the fluid accumulation
The net result of the effusion formation is a flattening or inversion of the diaphragm, mechanical disassociation of the visceral and parietal pleura, and a restrictive ventilatory defect.
Possible Signs and Symptoms
The most common manifestations, regardless of the type of fluid in the pleural space or its causes, are shortness of breath and chest pain because of large pleural effusion that compresses the adjacent lung tissue. However, some people with pleural effusion have no symptoms at all. When the parietal pleura is irritated, the patient may have mild pain that quickly passes or, sometimes, a sharp, stabbing pleuritic type of pain. Pain is often relieved by formation of an effusion, as the fluid reduces friction between inflamed visceral and parietal pleura. Some patients also will have a dry and unproductive cough. Tapping on the chest will show that the usual crisp sounds have become dull, and on listening with a stethoscope the normal breath sounds are muted. If the pleura is inflamed, there may be a scratchy sound called a “pleural friction rub."
Table 2. Possible and Actual Signs and Symptoms POSSIBLE ACTUAL COMPLAINT OF THE
PATIENTDry and unproductive cough Dyspnoea
Pleuritic pain OrthopneicDyspnoea Sore throat
Dullness over chest wall Productive coughDecreased or absence of breath sound
Pleural friction rub
Possible Diagnostic Procedure and Laboratory Tests
Chest Radiograph (x-ray).A chest X-ray is a radiology test that involves exposing the chest briefly to radiation to produce an image of the chest and the internal organs such as the heart, lungs, and blood vessels. Doctor may order a chest x-ray if you have symptoms like persistent cough, chest injury, chest pain, coughing up blood and difficulty in breathing. It can be done also for patient having signs oftuberculosis, lung cancer, or other chest or lung disease.
A seriesof chest x-ray may be used to evaluate or monitor changes found on a previous chest x-ray.
Although the treatment is beneficial to the patient, it poses certain risks or complications and or side effects like cancer and other defects; nausea, sneezing,
vomiting, itching, hives or anaphylaxis may occur if allergic to iodine; and kidney problem due the toxic effect of the dye.
Thoracic Computed Tomography (CT). An imaging method that uses x-rays to create cross-sectional pictures of the chest and upper abdomen. These cross-sectional images of the area being studied can then be examined on a computer monitor, printed or transferred to a CD. It also provides greater clarity and reveals more details than regular x-ray examination of the body e.g., brain, chest, spine, and abdomen. The test may be used to better view the structures inside the chest.
A thoracic CT may be done: Chest CT scan showing loculated pleural effusion and right lung
After a chest injury
When a tumour or mass (clump of cells) is suspected
To determine the size, shape, and position of organs in the chest and upper abdomen
To look for bleeding or fluid collections in the lungs or other areas
All procedure using radiation and dyes poses the same complications and side effects though it varies from person to person.
Thoracentesis. A procedure is used to remove fluid from the space between the lungs and the chest wall called the pleural space. It is done by inserting a needle (sometimes a plastic catheter) into the chest wall and the pleural fluid is aspirated. The procedure is performed to remove the fluid, prevent the fluid from building up again and treating the cause of the fluid build-up.
The procedure can also be performed if you have the following conditions:
Asbestos-related pleural effusion
Collagen vascular disease
Drug reactions
Hemothorax
Pancreatitis
Pneumonia
Pulmonary embolism
Pulmonary veno-occlusive disease
Thyroid disease
Collapse of the lung (pneumothorax)
The risks for thoracentesis include excessive loss of blood, fluid re-accumulation,infection, pulmonary oedema, and respiratory distress. So far no serious complications have been reported.
Pleural Fluid Analysis. An examination ofthe fluid aspirated/collected from the pleural space during thoracentesis and to look for cancerous or malignant cells, cellular makeup, chemical content and tiny organisms that can cause the diseases.
Complete Blood Count. This is used as a broad screening test to check for disorders as anemia, infection, and many other diseases. It is actually a panel of tests that examines different parts of the blood which includes the following (Lab Test Online):
White blood cell (WBC) count is a count of the actual number of white blood cells per volume of blood. Both increases and decreases can be significant.
White blood cell differential looks at the types of white blood cells present. There are fivedifferent types of white blood cells e.g., neutrophils, lymphocytes, monocytes, eosinophil, and basophils. Each has its own function in protecting us from infection.
Red blood cell (RBC) count. It is a count of the actual number of red blood cells per volume of blood. Both increases and decreases can point to abnormal conditions.
Hemoglobin measures the amount of oxygen-carrying protein in the blood.
Hematocrit measures the percentage of red blood cells in a given volume of whole blood.
The platelet count is the number of platelets in a given volume of blood. Both increases and decreases can point to abnormal conditions of excess bleeding or clotting.
Mean platelet volume (MPV) is a machine-calculated measurement of the average size of your platelets. New platelets are larger, and an increased MPV occurs when increased numbers of platelets are being produced. MPV gives your doctor information about platelet production in your bone marrow.
Mean corpuscular volume (MCV) is a measurement of the average size of your RBCs. The MCV is elevated when your RBCs are larger than normal (macrocytic), for example in anemia caused by vitamin B12 deficiency. When the MCV is decreased, your RBCs are smaller than normal (microcytic) as is seen in iron deficiency anemia or thalassemia.
Mean corpuscular haemoglobin (MCH) is a calculation of the average amount of oxygen-carrying haemoglobin inside a red blood cell. Macrocytic RBCs are large so tend to have a higher MCH, while microcytic red cells would have a lower value.
Mean corpuscular hemoglobin concentration (MCHC) is a calculation of the average concentration of hemoglobin inside a red cell. Decreased MCHC values (hypochromia) are seen in conditions where the hemoglobin is abnormally diluted
inside the red cells, such as in iron deficiency anemia and in thalassemia. Increased MCHC values (hyperchromia) are seen in conditions where the hemoglobin is abnormally concentrated inside the red cells, such as in burn patients and hereditary spherocytosis, a relatively rare congenital disorder.
Red cell distribution width (RDW) is a calculation of the variation in the size of your RBCs. In some anemias, such as pernicious anemia, the amount of variation (anisocytosis) in RBC size (along with variation in shape – poikilocytosis) causes an increase in the RDW.
Actual Diagnostic Procedure and Laboratory Test
Upon admission, the physician ordered a full blood count test and other relevant haematology test for Encik Ahmad. The following tables showed the results of the laboratory
investigations. He had chest x-ray which revealed no pneumothorax. He was also ordered for
thoracentesis and pleural fluid analysis and was performed on 11 January 2011. They aspirated about
500 ml., of clear fluid and a sample was send for laboratory analysis. Based on the result, the type of
pleural fluid of Encik Ahmad was transudate caused by CCF.Please refer to the table for the fluid
analysis result.
Table 3. Full Blood Count Test
TYPES OF INVESTIGATION
DATE TIME RESULT UNITREFERENCE
RANGE HEMATOLOGY 9/1/2011 22:23 Full Blood Count Haemoglobin L 121 .0 g/L 130. 0- 170. T.W.B.C 6.5 10^9/L 4. 0-10 .0 Platelets 218 10^9/L 150- 410 T.R.B.C L 4.31 10^12/L 4.50 -5. 50 HCT L 35.6 g 40.0 -50. 0 MCU 83 f L 83 -101 MCH 28 .0 P g 27. 0- 32 .0 MCHC 34. 0 g/d L 31. 5- 34. 5 RDW-CV H 14.5 g 11. 6-14. 0 Lmphocytes# 1.2 10^3/u L 1. 0-3.0 Neutrophil# 4.5 10^3/u L 2. 0-7 .0 Monocytes# 0. 6 10^3/u L 0. 2- 1. 0 Eosinophil# 0. 1 10^3/u L 0 .0- 0. 05 Basophil# L 0. 0 Lmphocytes g L 19.1 20. 0- 40. 0 Neutrophil g 69. 3 40. 0- 80. 0 Monocytes g 10. 0 g 2. 0- 10. 0 Eosinophil g 1 .2 g 1. 0- 6. 0
HEMATOLOGY - COA 9/1/2011 22:23 PT/APTT Protrombin Time 11.8 sec 9.1-12.1 PT Test 10.3 sec PT Control 1.15 sec PR 1.15 sec I.N.R APTT APTT Test 34. 0 sec 21.4-36.8
Case Study on Pleural Effusion14 | P a g e
APTT Control 28. 0 sec APTT / Ratio 1. 21 sec
HEMATOLOGY - COA PROTHROMBIN TIME 11/1/2011 17:18
PT Test H 14.8 sec 9.1- 12.1
PT Control 10.3
P.R 1.44
I.N.R 1.44 APTT
APTT Test 36 .0 sec 21.4 -6.8
APTT Control 28 .0
APTT / Ratio 1.29
Table 7. Pleural Fluid Analysis
TYPES OF INVESTIGATION
DATE TIME RESULT UNITREFERENCE
RANGE PLEURAL FLUID Pleural Fluid Biochesmistry
11/1/2011 13:34
Protien (Pleural Fluid)
28
(transudate)
<30 Transudate)
>30 (Exudate)
LDH (Pleural Fluid) 184 <200 Transudate)
(transudate)
>200 (Exudate)
Possible Treatment
Thoracentesis. A procedure is used to remove fluid from the space between the lungs and the chest wall called the pleural space. It is done by inserting a needle (sometimes a plastic catheter) into the chest wall and the pleural fluid is aspirated. The procedure is performed to remove the fluid, prevent the fluid from building up again and treating the cause of the fluid build-up.
Under Water Seal Drainage (also called Chest Tube/Chest Drain/Tube Thoracostomy/Intercostal Drain) is a flexible plastic tube that is inserted through the side of the chest into the pleural space. It is used to remove air (pneumothorax) or fluid (pleural effusion, blood, chyle), or pus (empyema) from the intrathoracic
space(Wikipedia). Chest tubes are normally inserted under a local anaesthetic or under a general anaesthetic if the patient is undergoing chest surgery.
The two common complications are the risk of infection and pain. Good hygiene practices including hand washing before contact with the patient will help minimize the infection risk. There can be a degree pain of which differs from patient to patient and should be discussed with the concern doctors and nurses.
Pleurectomy (also known as recurrent pleural effusion). Thisis a surgical procedure to remove part of the pleura, the lining around the lungs. It is usually done to treat mesothelioma, a rare form of lung cancer most often related to asbestos exposure. It is performed under general anaesthesia. An incision is made above the affected area and the pleural layers are removed. Additional affected lung tissue may also be removed during the surgery. Stitches are made once the surgery is complete and the incision is cleaned and bandaged.
There is a risk for bleeding or infection after a pleurectomy. Patients should be on the lookout for symptoms like fever, drainage from the incision, or redness and swelling around the area of the incision. Once the patient returns home, he or she can usually resume normal activity within a week. It may take longer to gain the energy to perform vigorous tasks.
Actual Treatment Received by the Patient
During his admission, Encik Ahmad was given nebulizer with salbutamol, continue to take his old medication for his other diseases e.g., hypertension, diabetes mellitus, heart medication and etc. Aside from that he was ordered to undergo thoracentesis to confirm his diagnosis. He finished the procedure successfully with 500 ml. of blood stain pleural fluid aspirated. Pleural fluid sample was sent for analysis and result showed transudate type of
fluid due to CCF.
His other medications are listed in the table below.
Table 8. Medication, its action, indication and side effects.NAME ACTIONS INDICATIONS SIDE EFFECTS
T. Simvastatin 40mg(ON)
To lower bad cholesterol (LDL) and triglycerides in the blood while increasing the level of good cholesterol (HDL)
Lower bad cholesterol and triglyceride in the blood
Constipation, stomach pain, nausea and headache
T.Aspirin 150mg (OD)
Reducing substances in the body that cause pain, fever, and inflammation.
Is used to treat mild to moderate pain, and to reduce fever or inflammation. It is sometimes used to
Black, bloody or tarry stool, severe nausea, vomiting , headache, coughing up blood
Case Study on Pleural Effusion16 | P a g e
Pleurectomy/decortication: Appearances of the decorticated lung after the visceral and parietal pleurae have been resected
(with diaphragm intact).
treat/prevent heart attacks, strokes, and
T. Isosorbide Dinitrate 10mg (TDS)
Dilates (widens) blood vessels, making it easier for blood to flow and easier for the heart to pump.
Prevent attack of chest pain
Headache, dizziness, palpitation, low blood pressure and weakness
T.Vasteral 20mg (TDS)
Preventive treatment of episode of angina pectoris.
Angina pectosis Gastrointestinal upset, nausea abd vomiting
T. Clopidogrel 75mg (OD)
Keeps the platelets in your blood from coagulating (clotting) to prevent unwanted blood clots that can occur with certain heart or blood vessel conditions.
Used to prevent blood clots after a recent heart attack or stroke, and in people with certain disorders of the heart or blood vessels.
Hypertension Diarrhea, headache, short of breath and dizziness
T. Digoxin 0.0625gm(OD)
It helps make the heart beat stronger and with a more regular rhythm.
Used to treat atrial fibrillation, a heart rhythm disorder of the atria (the upper chambers of the heart that allow blood to flow into the heart).
Nausea, vomiting, headache, abdominal pain and skin rashes
C. Gemfibrozil 300mg (OD)
Helps reduce cholesterol and triglycerides (fatty acids) in the blood
Treat very high cholesterol and triglyceride levels in people with pancreatitis. It also use to to lower the risk of stroke, heart attack, or other heart complications in people
Abdominal pain, diarrhea, nausea, myalgia and rashes
Case Study on Pleural Effusion17 | P a g e
with high cholesterol and triglycerides who have not been helped
T.Frusemide 40mg (BD)
Reduce the amount of water in body also treat hypertension
Reduce the amount of water in body also treat hypertension
Skin rashes, oedema, eye or eyesight problem, itching, pain and inflammation
Possible Complications
Pleural effusions compromise lung function by preventing its full expansion for breathing. If the effusion is not treated and underlying diseases causing effusion, lung scarring and permanent decrease in lung function will be developed. Fluid that remains for a prolonged period of time is also at risk for becoming infected and forming an abscess called an empyema.
Diagnostic and therapeutic procedures like thoracentesis, pneumothorax is a potential complication. It is also called a collapsed lung, where there is the collection of air in the pleural space that causes part or all of a lung to collapse. This build-up of air puts pressure on the lung, decreasing lung expansion and difficulty in breathing.
Case Study on Pleural Effusion18 | P a g e
Case Study on Pleural Effusion19 | P a g e
Case Study on Pleural Effusion20 | P a g e
Case Study on Pleural Effusion21 | P a g e
Discharge Plan of Pleural Effusion
Encik Ahmad was discharge on 14 January 2011. He was alert, conscious and had good hydration. His blood pressure was 139/87 mmHg, pulse of 69 bpm, respiratory rate of 20 breath per minute andsPO2 of 97% on room air, body temperature of 37.0°C and blood glucose level of 15.1 mmol/L. He had no more complaint of chest pain and SOB. His physician and staff nurses reiterated their advicesespecially on restriction of fluid intake and others.
The following were the discharge plan for Encik Ahmed:
A. Follow-up Care
He was advised to come to hospital after 1 month time for regular check-up. Follow other medical appointmentin orthopaedic clinic and IJN. He was informed that regular check-up isnecessary to help ensure that any changes in his health are noted and treated if needed. If any health problems between check-ups are encountered, contact his doctor immediately or come to the hospital.
B. Medication
Comply with the treatment regimen. Use medication as ordered and complete the entire prescription. Provide schedule as when to take the medication. Do under dose or overdose by cutting breaking the medicine using hands. This will lessen the efficacy of the medicine and will only prolong the disease process.
C. Exercise
Case Study on Pleural Effusion22 | P a g e
Exercise keeps you healthy. It is good for the heart and lungs and promotes blood circulation. Start with range of motion (ROM) exercises, it is a good choice e.g., stretching and flexing the joints. Decrease activities if you feel pain and tired. Do deep breathing and coughing exercise to lessen the pain sensation and promote lung expansion. Do it gradually. Ask your doctor to help you plan the best exercise program for you. It is best to start slowly and do more as you get stronger.
D. Treatment
Treatment of pleural effusion is always based on the underlying condition and whether the effusion is causing symptoms like difficulty in breathing or SOB. However, removal of fluid is always the first choice if fluid build-up is in large volume, preventing it from accumulating again and or addressing the underlying cause of the fluid build-up. Removal of fluid promotes lung expansion and easy breathing.
E. Health Teaching
Good personal hygiene is very important factor in daily living to keep us from getting infection.
Hand washing. Correct technique must be applied especially after using the bathroom and before eating any food. Hand washing still the most effective way of eliminating microorganisms.
Shower daily. Keep yourself clean daily to prevent accumulation of microorganisms on your skin.
Use a deodorant spray instead of antiperspirant. Antiperspirants block sweat glands which can cause an infection.
Brush teeth two to three times a day.Oral hygiene is the most effective way in preventing the spread of infection.
Perineum care. Clean perineum area properly each time you pass urine and bowel.
F. Diet
Limit intake of food loaded with salt e.g., salted fish, eggs, sauces, seasoning and vegetables. Salt causes water retention in people with heart failure and result to edema in lungs, ankles, and abdomen. Be smart in buying food, read label of nutritional value in packed food.
Eat variety of healthy foods from all the food groups e.g., whole grains, green leafy vegetables, apples, soy,oats, olive oils, salmons and almonds Eating healthy foods may help you feel better and have more energy. You may need to make diet changes
Case Study on Pleural Effusion23 | P a g e
depending on your underlying diseases. Eat small-frequent meal and snacks rather than 1 big meal to boost your metabolism.
Drink Fluids:Restrict fluid intake from 800 – 1000 mls. per day or as prescribed by your physician to avoid fluid overload which causes SOB and dyspnea. Choose healthy like water, fresh fruit juices, and milk rather than caffeinated/carbonated drinks which is loaded with sugar.
Rest:Limit your activities in a day to reduce oxygen consumption.
G. Seek Care Immediately If You Have:
Pleuritic pain. An early signs of effusion.
Trouble breathing.
Increasing dyspnea or SOB
Cough and hemoptysis
Bibliography
Chest Ultrasound. (2008, August 8). Retrieved January 13, 2011, from Care First Blue Cross Blue Shield: http://carefirst.staywellsolutionsonline.com/RelatedItems/92,P0774
Chest x-ray. (2010, August 20). Retrieved January 13, 2011, from Heart, Lung and Blood Substitute Disease and Condition Index: http://www.nhlbi.nih.gov/health/dci/Diseases/cxray_whatis.html
Complete Blood Count Test. (2010, November 24). Retrieved January 23, 2011, from Lab Tests Online: http:labtestonline.org/understanding/analytes/cbc/test.html
Burke, P. L. (2008). Medical Surgical Nursing (6th ed.). New Jersey, USA: Pearson Education International.
Dugdale, D. C. (2010, September 15). Pleural Effusion. Retrieved January 22, 2011, from Medicine Plus: http://www.nlm.nih.gov/medicineplus/ency/article/000086.htm
Grant, A. W. (2006). Anatomy and Physiology in Health and Illness (10th ed.). London: Churchill Livingstone.
Jegtvig, S. (2008, February 28). Ten Foods for a Healthy Heart. Retrieved January 23, 2011, from About.com: http://www.nutrition.about.com/od/fooffun/a/healthy_heart.htm
Pleural Effusion. (2010, February 4). Retrieved January 14, 2011, from Medicine Net.Com: http://medicine.com/pleural_effusion/page5.htm
Case Study on Pleural Effusion24 | P a g e
johnroks. (n.d.). Hemothorax/Pnuemothorax. Retrieved January 23, 2011, from Scribd.com: htto://www.scribd.com/doc/17471582/nursing-care-plan-for hemothroax-pneumothorax