Goals of the Program: • Serve more people in their homes and communities • Integrate physical health and long‐term Medicare and Medicaid services • Enhance fiscal accountability • Promote quality and innovation among providers 1
Transcript
Goals of the Program:• Serve more people in their homes and communities• Integrate physical health and long‐term Medicare and Medicaid services
• Enhance fiscal accountability• Promote quality and innovation among providers
1
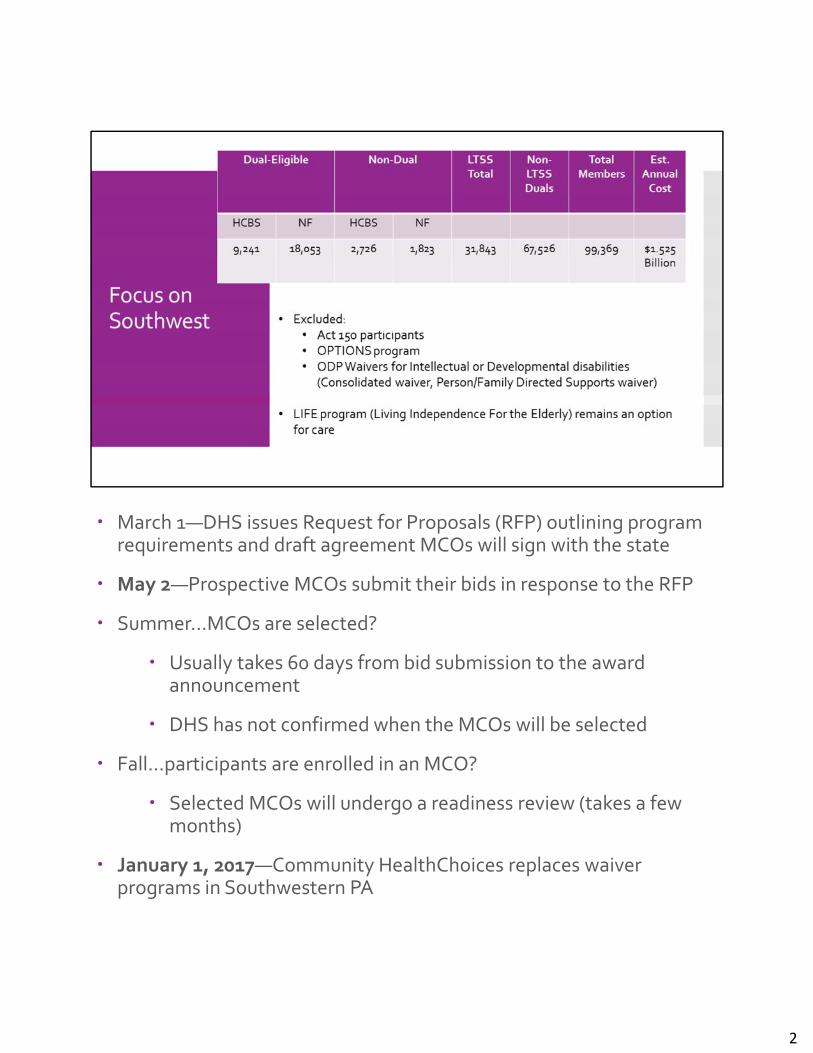
March 1—DHS issues Request for Proposals (RFP) outlining program requirements and draft agreement MCOs will sign with the state
May 2—Prospective MCOs submit their bids in response to the RFP
Summer…MCOs are selected?
Usually takes 60 days from bid submission to the award announcement
DHS has not confirmed when the MCOs will be selected
Fall…participants are enrolled in an MCO?
Selected MCOs will undergo a readiness review (takes a few months)
January 1, 2017—Community HealthChoices replaces waiver programs in Southwestern PA
2
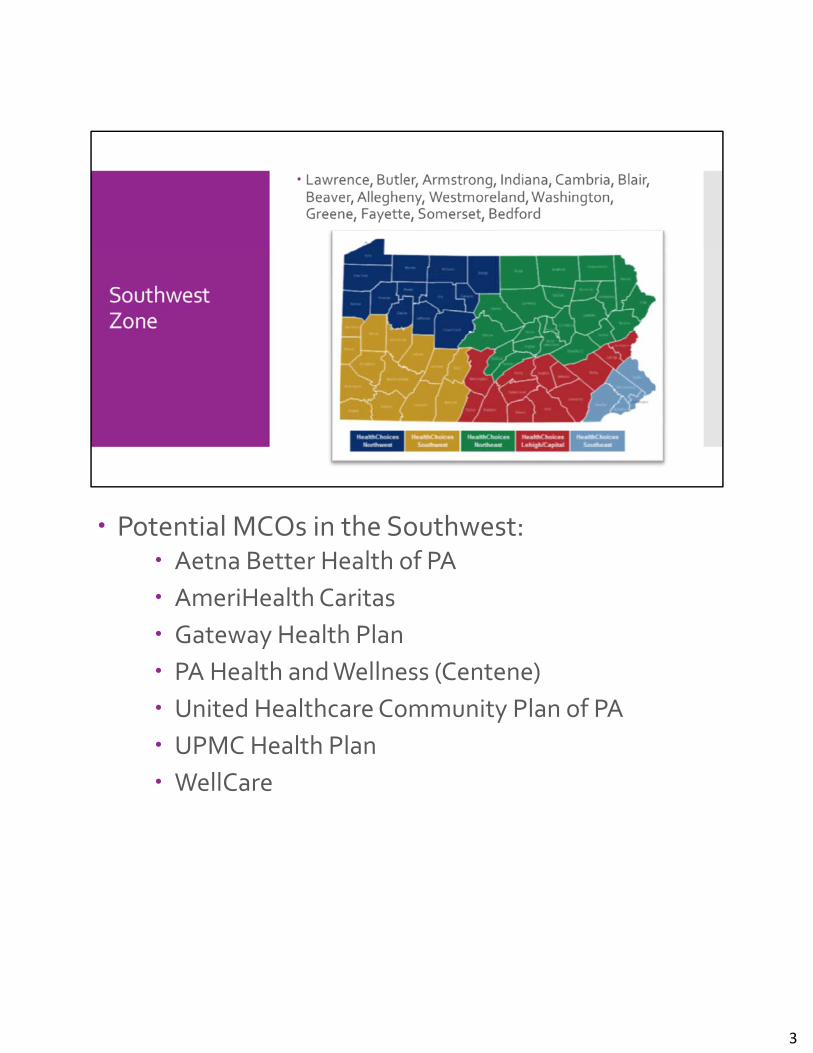
Potential MCOs in the Southwest: Aetna Better Health of PA
AmeriHealth Caritas
Gateway Health Plan
PA Health and Wellness (Centene)
United Healthcare Community Plan of PA
UPMC Health Plan
WellCare
3
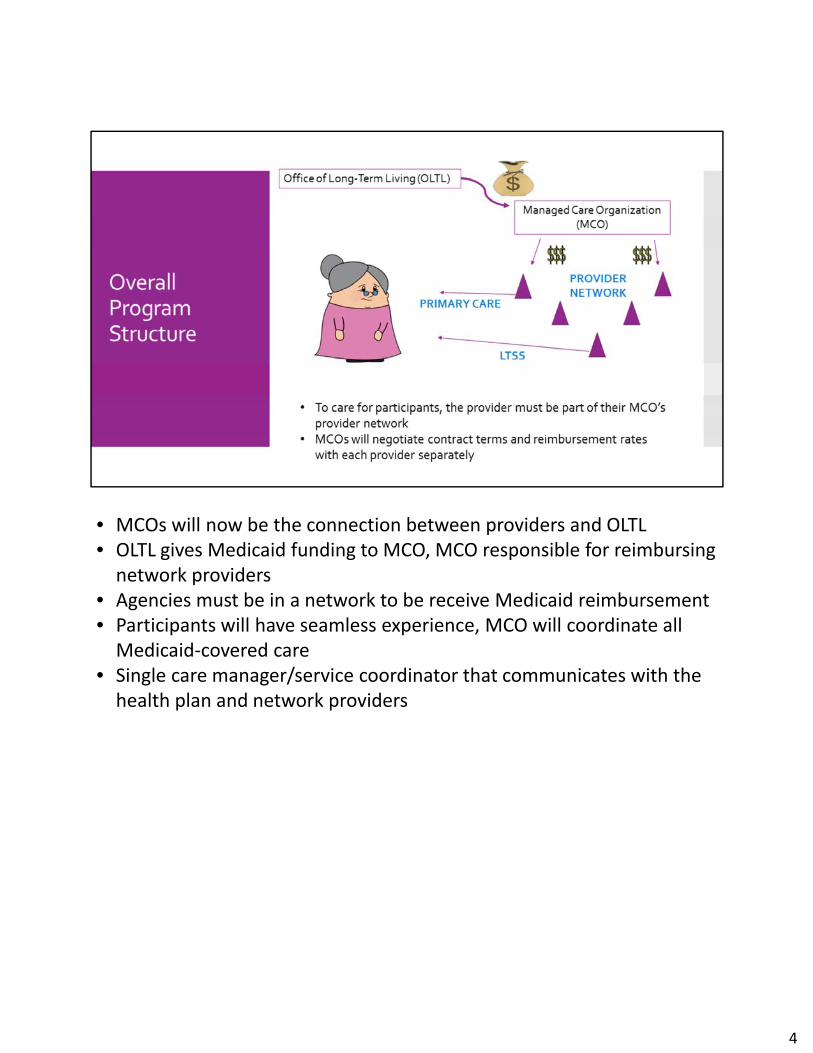
• MCOs will now be the connection between providers and OLTL• OLTL gives Medicaid funding to MCO, MCO responsible for reimbursing network providers
• Agencies must be in a network to be receive Medicaid reimbursement• Participants will have seamless experience, MCO will coordinate all Medicaid‐covered care
• Single care manager/service coordinator that communicates with the health plan and network providers
4
• Instead of fee‐for‐service, MCOs will receive PM/PM to cover all services for their members
• Providers will receive reimbursement out of this one pot of money• Capitation calculation focuses on characteristics of that Medicaid population
• What is the age of the population?• How many are dual eligibles?• How many are considered nursing facility clinically eligible?
• NOTE: All waiver participants today must be NFCE in order to be in a waiver
5
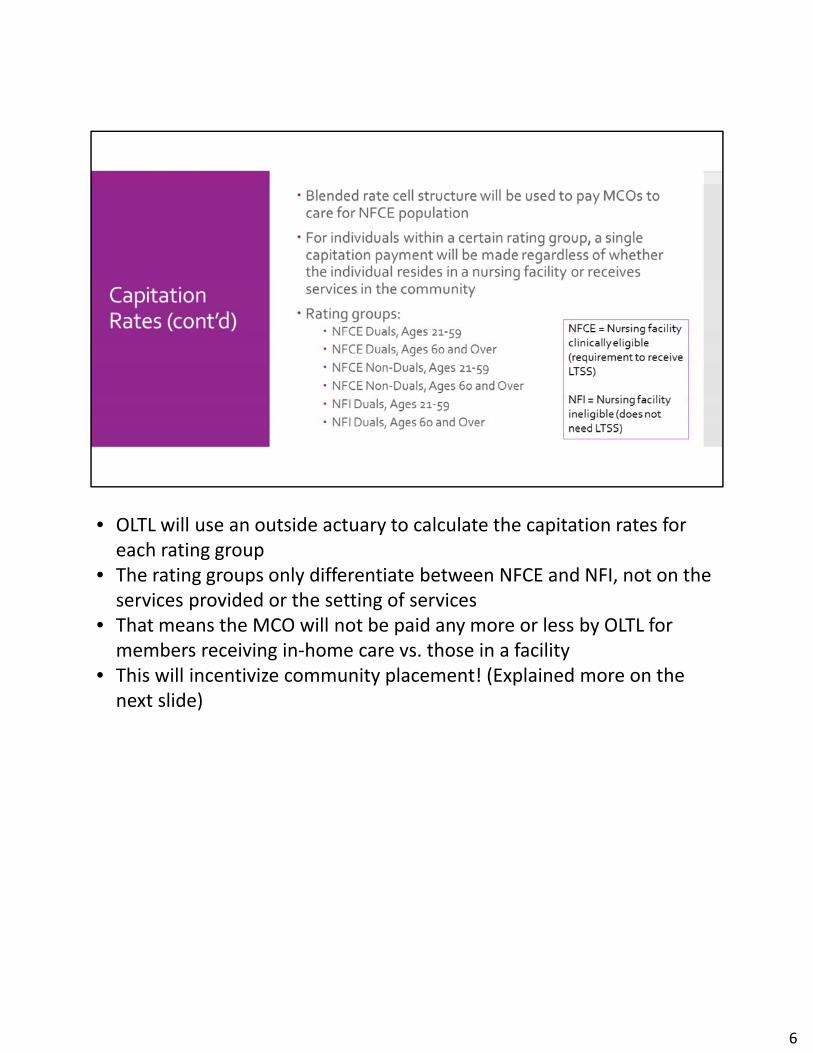
• OLTL will use an outside actuary to calculate the capitation rates for each rating group
• The rating groups only differentiate between NFCE and NFI, not on the services provided or the setting of services
• That means the MCO will not be paid any more or less by OLTL for members receiving in‐home care vs. those in a facility
• This will incentivize community placement! (Explained more on the next slide)
6
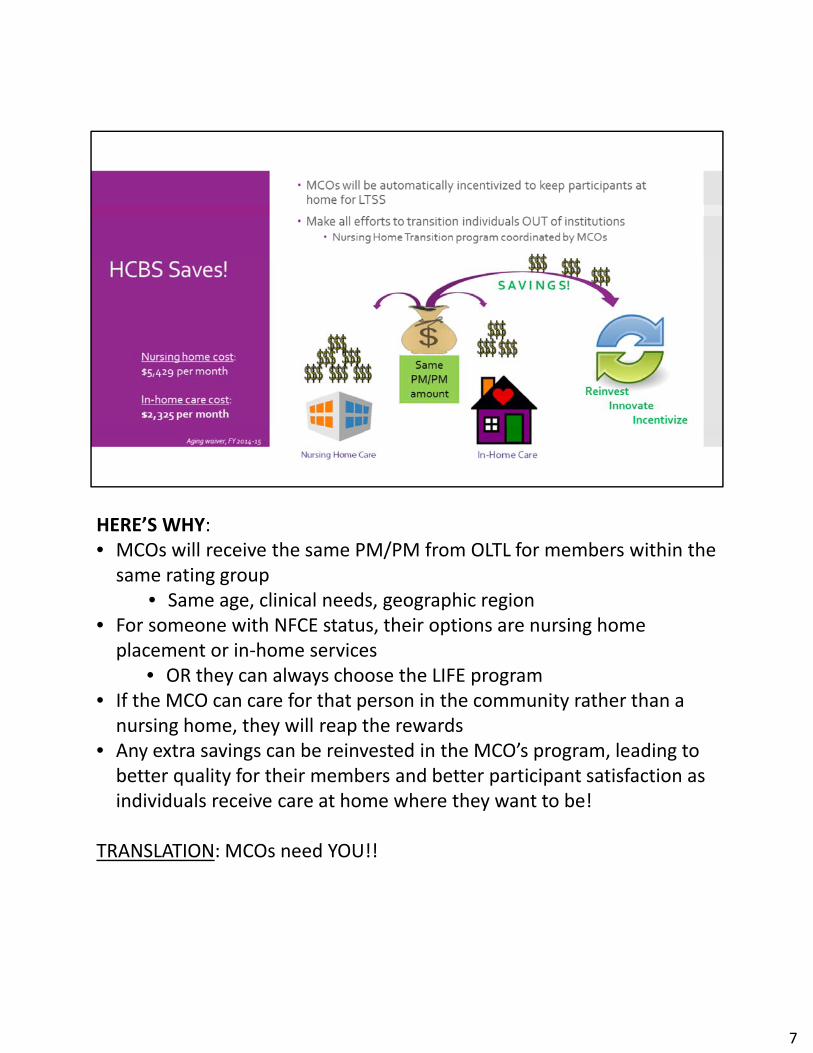
HERE’S WHY:• MCOs will receive the same PM/PM from OLTL for members within the same rating group
• Same age, clinical needs, geographic region• For someone with NFCE status, their options are nursing home placement or in‐home services
• OR they can always choose the LIFE program• If the MCO can care for that person in the community rather than a nursing home, they will reap the rewards
• Any extra savings can be reinvested in the MCO’s program, leading to better quality for their members and better participant satisfaction as individuals receive care at home where they want to be!
TRANSLATION: MCOs need YOU!!
7
• The continuity of care period is not a strict cutoff date• MCOs may choose to keep providers in network even if contracts aren’t yet finished
• But this is your only guaranteed window of time when services can continue according to current care plans
Ask your MCO—Will your company contract with current service coordinators?
8
When can I get started?• Get familiar with prospective MCOs today• Sign letters of intent as they are presented to you• Begin collecting and analyze internal data NOW to prepare to sell your agency
• Bids due May 2 to OLTL…Negotiations between MCOs and OLTL…
…Selected plans announced Summer 2016…
• Once MCOs are announced, contracts can be signed, but remember you have 180‐day continuity of care period
9
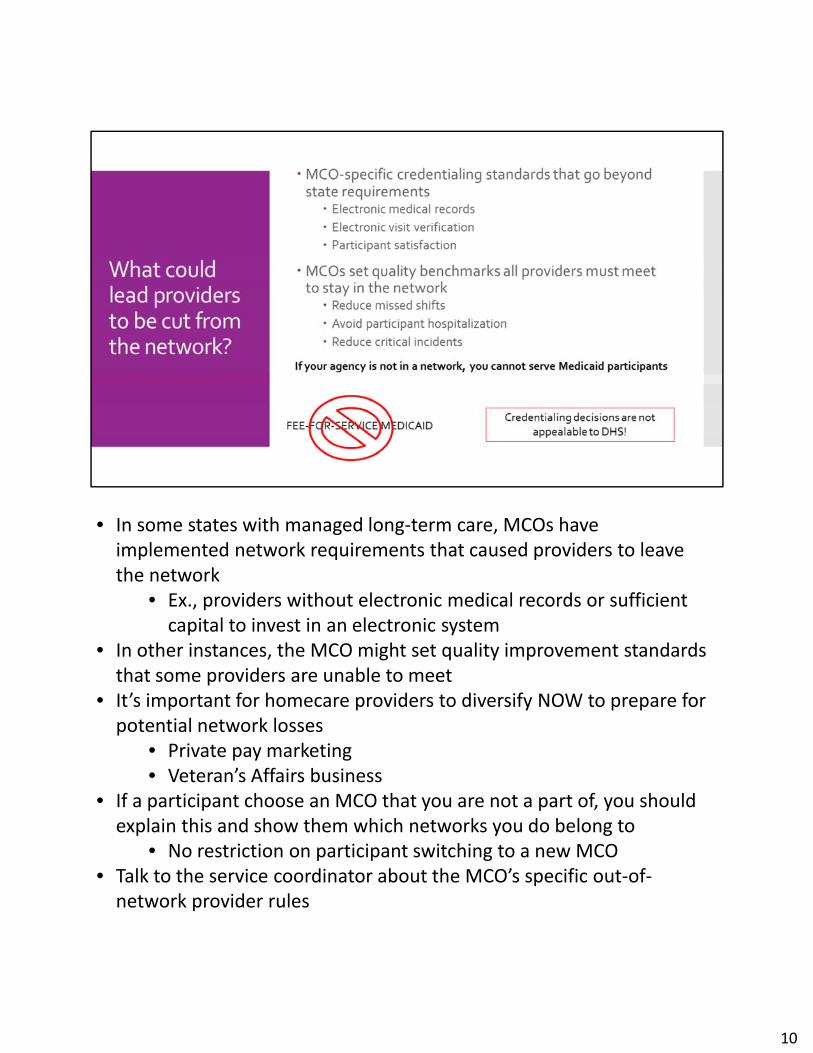
• In some states with managed long‐term care, MCOs have implemented network requirements that caused providers to leave the network
• Ex., providers without electronic medical records or sufficient capital to invest in an electronic system
• In other instances, the MCO might set quality improvement standards that some providers are unable to meet
• It’s important for homecare providers to diversify NOW to prepare for potential network losses
• Private pay marketing• Veteran’s Affairs business
• If a participant choose an MCO that you are not a part of, you should explain this and show them which networks you do belong to
• No restriction on participant switching to a new MCO • Talk to the service coordinator about the MCO’s specific out‐of‐network provider rules
10
Maximus will continue to enroll brand new participants Aging Well PA, LLC will take on clinical eligibility determination (NFCE assessment)
o A new company comprised of many current Area Agencies on Aging MCO will perform comprehensive needs assessment and annual reassessments
(currently done by service coordination entities)o Develop person‐centered service plan
The current NFCE assessment tool (also known as the level of care determination) is being redesigned for 2017
o DHS will use the InterRAI‐Homecare tool, a nationally tested and validated assessment
o An excerpt of the InterRAI will make up the new “clinical eligibility determination” instrument
o 5 Areas Assessed: Walking, Eating, Elimination, Cognition, ADLo Built‐in scoring logic, removes subjectivity
Once a participant enters the CHC program, the MCO will use the full InterRAI tool to complete the comprehensive needs assessment
11
12
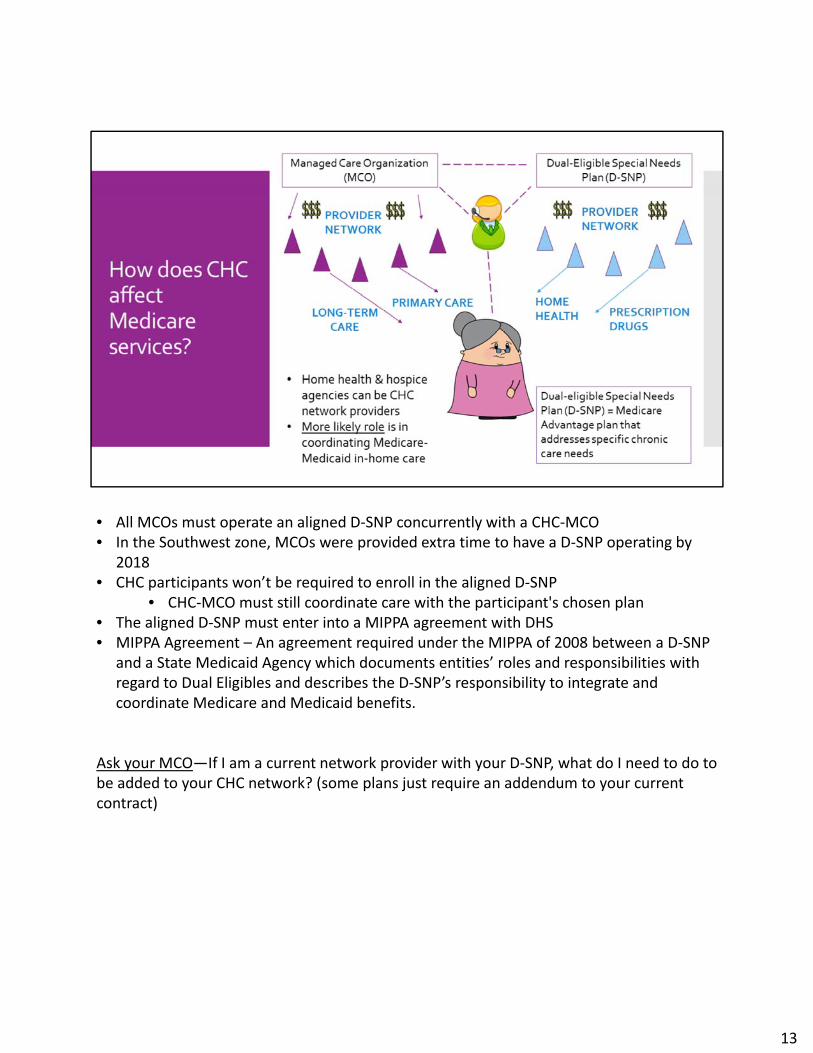
• All MCOs must operate an aligned D‐SNP concurrently with a CHC‐MCO• In the Southwest zone, MCOs were provided extra time to have a D‐SNP operating by
2018 • CHC participants won’t be required to enroll in the aligned D‐SNP
• CHC‐MCO must still coordinate care with the participant's chosen plan• The aligned D‐SNP must enter into a MIPPA agreement with DHS• MIPPA Agreement – An agreement required under the MIPPA of 2008 between a D‐SNP
and a State Medicaid Agency which documents entities’ roles and responsibilities with regard to Dual Eligibles and describes the D‐SNP’s responsibility to integrate and coordinate Medicare and Medicaid benefits.
Ask your MCO—If I am a current network provider with your D‐SNP, what do I need to do to be added to your CHC network? (some plans just require an addendum to your current contract)
13
• Administrative integration is expected to evolve over the life of the CHC program• This includes, but is not limited to, an integrated assessment and care coordination
process that spans all Medicaid and Medicare services.• MCOs were asked to address their plans for coordinating Medicare services in their bids
DHS contractor Truven Health Analytics recommends CHC strategy:“Go slow” approach to alignment, recognizing that it has taken more time than expected in other states
14
CHC Covered LTSS Benefits Include:• Personal Assistance Services• Home Health Services • Hospice• Participant‐Directed Services• Respite• Adult Daily Living • Assistive Technology• Personal Emergency Response System• Residential Habilitation• Exceptional DME • Home Adaptations • Home Delivered Meals • TeleCare• Vehicle Modifications• Non‐Medical Transportation
Ask your MCO‐‐Will you cover assisted living facilities? What other services will you pay for besides those on this list? Will your plan require nursing supervision of aides?
15
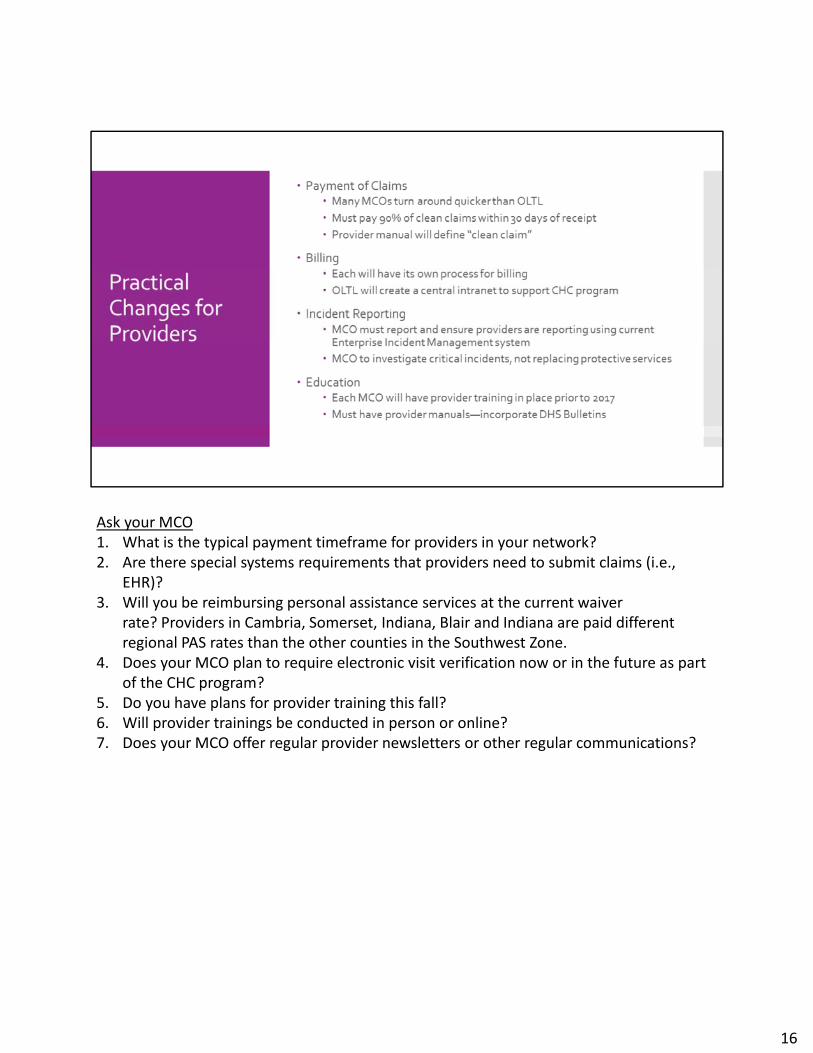
Ask your MCO1. What is the typical payment timeframe for providers in your network?2. Are there special systems requirements that providers need to submit claims (i.e.,
EHR)?3. Will you be reimbursing personal assistance services at the current waiver
rate? Providers in Cambria, Somerset, Indiana, Blair and Indiana are paid different regional PAS rates than the other counties in the Southwest Zone.
4. Does your MCO plan to require electronic visit verification now or in the future as part of the CHC program?
5. Do you have plans for provider training this fall?6. Will provider trainings be conducted in person or online?7. Does your MCO offer regular provider newsletters or other regular communications?
16
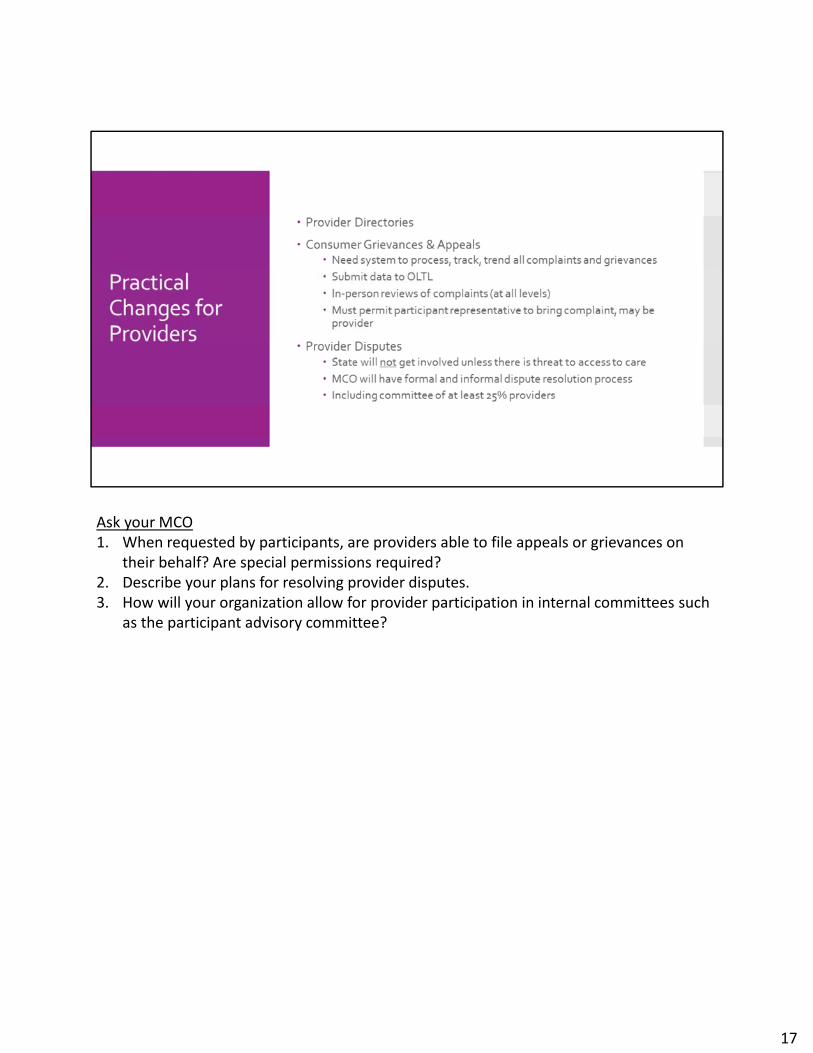
Ask your MCO1. When requested by participants, are providers able to file appeals or grievances on
their behalf? Are special permissions required?2. Describe your plans for resolving provider disputes.3. How will your organization allow for provider participation in internal committees such
as the participant advisory committee?
17
• HEDIS measures analyze the health plan’s performance in areas such as:• Controlling high blood pressure• Flu vaccinations for adults 18‐64• Getting care quickly• Network management• Network directory accuracy • Utilization management• Quality improvement activities
• NCQA = National Committee for Quality Assurance, a private, 501(c)(3) not‐for‐profit organization dedicated to improving health care quality
• Accredited health plans face a rigorous set of more than 60 standards and must report on their performance in more than 40 areas in order to earn NCQA’s seal of approval
18
• PHA has introduced the MCOs to our learning management system, My Learning Center, as a potential tool for workforce innovation as well as MCO staff and network provider training
• Network providers should position themselves as partners to help MCOs meet the objectives in their quality management plans
Ask your MCO—Can you share with us your response to the RFP dealing with Workforce Innovation that improves the recruitment, retention and skills of direct care workers?























![in ^ c j b b d 8in ^ a V j F GZXdkZgn - AHCIin ^ a V j F in ^ c j b b d 8 GZXdkZgn Allegheny HealthChoices, Inc.8]d^XZh The Allegheny County HealthChoices Program 1999 - 2009 Improving](https://static.documents.pub/doc/80x56/5f4b867e91fcb5401e41df7e/in-c-j-b-b-d-8in-a-v-j-f-gzxdkzgn-ahci-in-a-v-j-f-in-c-j-b-b-d-8-gzxdkzgn.jpg)

