1
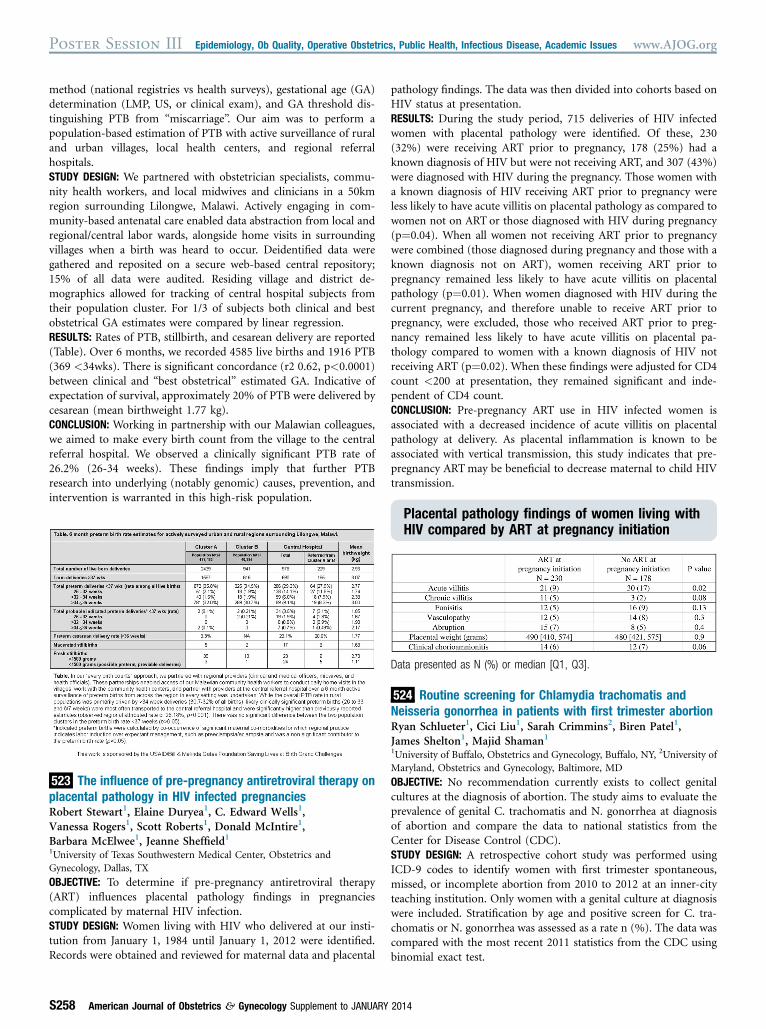
method (national registries vs health surveys), gestational age (GA) determination (LMP, US, or clinical exam), and GA threshold dis- tinguishing PTB from “miscarriage” . Our aim was to perform a population-based estimation of PTB with active surveillance of rural and urban villages, local health centers, and regional referral hospitals. STUDY DESIGN: We partnered with obstetrician specialists, commu- nity health workers, and local midwives and clinicians in a 50km region surrounding Lilongwe, Malawi. Actively engaging in com- munity-based antenatal care enabled data abstraction from local and regional/central labor wards, alongside home visits in surrounding villages when a birth was heard to occur. Deidentified data were gathered and reposited on a secure web-based central repository; 15% of all data were audited. Residing village and district de- mographics allowed for tracking of central hospital subjects from their population cluster. For 1/3 of subjects both clinical and best obstetrical GA estimates were compared by linear regression. RESULTS: Rates of PTB, stillbirth, and cesarean delivery are reported (Table). Over 6 months, we recorded 4585 live births and 1916 PTB (369 <34wks). There is significant concordance (r2 0.62, p<0.0001) between clinical and “best obstetrical” estimated GA. Indicative of expectation of survival, approximately 20% of PTB were delivered by cesarean (mean birthweight 1.77 kg). CONCLUSION: Working in partnership with our Malawian colleagues, we aimed to make every birth count from the village to the central referral hospital. We observed a clinically significant PTB rate of 26.2% (26-34 weeks). These findings imply that further PTB research into underlying (notably genomic) causes, prevention, and intervention is warranted in this high-risk population. 523 The influence of pre-pregnancy antiretroviral therapy on placental pathology in HIV infected pregnancies Robert Stewart 1 , Elaine Duryea 1 , C. Edward Wells 1 , Vanessa Rogers 1 , Scott Roberts 1 , Donald McIntire 1 , Barbara McElwee 1 , Jeanne Sheffield 1 1 University of Texas Southwestern Medical Center, Obstetrics and Gynecology, Dallas, TX OBJECTIVE: To determine if pre-pregnancy antiretroviral therapy (ART) influences placental pathology findings in pregnancies complicated by maternal HIV infection. STUDY DESIGN: Women living with HIV who delivered at our insti- tution from January 1, 1984 until January 1, 2012 were identified. Records were obtained and reviewed for maternal data and placental pathology findings. The data was then divided into cohorts based on HIV status at presentation. RESULTS: During the study period, 715 deliveries of HIV infected women with placental pathology were identified. Of these, 230 (32%) were receiving ART prior to pregnancy, 178 (25%) had a known diagnosis of HIV but were not receiving ART, and 307 (43%) were diagnosed with HIV during the pregnancy. Those women with a known diagnosis of HIV receiving ART prior to pregnancy were less likely to have acute villitis on placental pathology as compared to women not on ART or those diagnosed with HIV during pregnancy (p¼0.04). When all women not receiving ART prior to pregnancy were combined (those diagnosed during pregnancy and those with a known diagnosis not on ART), women receiving ART prior to pregnancy remained less likely to have acute villitis on placental pathology (p¼0.01). When women diagnosed with HIV during the current pregnancy, and therefore unable to receive ART prior to pregnancy, were excluded, those who received ART prior to preg- nancy remained less likely to have acute villitis on placental pa- thology compared to women with a known diagnosis of HIV not receiving ART (p¼0.02). When these findings were adjusted for CD4 count <200 at presentation, they remained significant and inde- pendent of CD4 count. CONCLUSION: Pre-pregnancy ART use in HIV infected women is associated with a decreased incidence of acute villitis on placental pathology at delivery. As placental inflammation is known to be associated with vertical transmission, this study indicates that pre- pregnancy ART may be beneficial to decrease maternal to child HIV transmission. Placental pathology findings of women living with HIV compared by ART at pregnancy initiation Data presented as N (%) or median [Q1, Q3]. 524 Routine screening for Chlamydia trachomatis and Neisseria gonorrhea in patients with first trimester abortion Ryan Schlueter 1 , Cici Liu 1 , Sarah Crimmins 2 , Biren Patel 1 , James Shelton 1 , Majid Shaman 1 1 University of Buffalo, Obstetrics and Gynecology, Buffalo, NY, 2 University of Maryland, Obstetrics and Gynecology, Baltimore, MD OBJECTIVE: No recommendation currently exists to collect genital cultures at the diagnosis of abortion. The study aims to evaluate the prevalence of genital C. trachomatis and N. gonorrhea at diagnosis of abortion and compare the data to national statistics from the Center for Disease Control (CDC). STUDY DESIGN: A retrospective cohort study was performed using ICD-9 codes to identify women with first trimester spontaneous, missed, or incomplete abortion from 2010 to 2012 at an inner-city teaching institution. Only women with a genital culture at diagnosis were included. Stratification by age and positive screen for C. tra- chomatis or N. gonorrhea was assessed as a rate n (%). The data was compared with the most recent 2011 statistics from the CDC using binomial exact test. Poster Session III Epidemiology, Ob Quality, Operative Obstetrics, Public Health, Infectious Disease, Academic Issues www.AJOG.org S258 American Journal of Obstetrics & Gynecology Supplement to JANUARY 2014