Synthesis Presentation Group B2 Tonya Adelman Natalie Hawkins Michael Herbert Musediq Ismail- Rasheed Sanghee Lee Renee Sandusky Providing Culturally Competent Care to Minority youth with mental health issues
Transcript
Synthesis Presentation
Group B2Tonya AdelmanNatalie HawkinsMichael HerbertMusediq Ismail-RasheedSanghee LeeRenee Sandusky
Providing Culturally Competent Care to Minority youth with
An estimated 15 million youth, or 1 in 5 children and adolescents, are currently suffering from a mental disorder. Sadly, however, only about 7% of those in need receive appropriate mental health care.
Furthermore, over two-thirds of white children receive necessary mental health care, but only about half of minority children will receive the same needed care.
Strategies for addressing mental health disparities among youth are urgently needed to help lessen the impact of the devastating and lasting effects. For example, untreated depression in the minority youth population has been associated with suicide, school dropout, pregnancy, substance abuse, and depression in adulthood.
Why Is This Important?
Population DefinitionOur population of minority youths are defined as follows:
• Minority ethnic groups:o African-Americans (blacks)o Asian-Americanso Hispanics or Latinoso Native Hawaiian and other Pacific Islandso American Indians/Alaskan Natives.
• Youths defined as people under 24 years of age. • Children defined as persons aged <18 years• Adolescents are persons aged 12–17 years
• Mental disorders:o In children, mental disorders are described as "serious deviations from
expected cognitive, social, and emotional development" and include conditions meeting criteria described by the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision (DSM-IV-TR) (5) or the International Classification of Diseases (ICD)
Americans • 24.8 Hispanics, and • 12.5% Asian Americans
(IES, 2007)
Averaged freshman graduation rate for public high school students, by race/ethnicity:
School year 2006–07
• 13%–20% of the population under age 18 experience a mental disorder in any given year.
• In 2006, the cost of mental disorders among people under 24 years of age was estimated at $247 billion annually.
• During 2007-2010, studies found:o a 24% increase in inpatient mental health and substance
abuse admissions among children o an increase in use of psychotropic medications for teenagers.
• In 2010, mood disorders were the most common diagnoses for all hospital stays among children in the U.S.
• In 2011, substance use disorders affected 1.7 million adolescents aged 12–17 years.
(CDC, 2013)
Population Health Assessment
• Attention-deficit/hyperactivity disorder (ADHD, 6.8%)o The prevalence was highest among black and white children
and lower among Hispanic children.
• Conduct Disorder (3.5%)o The highest prevalence was found among black children.
• Anxiety disorder (3.0%)o Black children were less likely than white children to have
had anxiety or have current anxiety.
• Depression (2.1%)o Black adolescents were less likely to have had a major
depressive episode than white adolescents.
• Autism spectrum disorders (ASD, 1.1%)o The prevalence tends to be lower among minority children.
(CDC, 2013)
Population Health Assessment
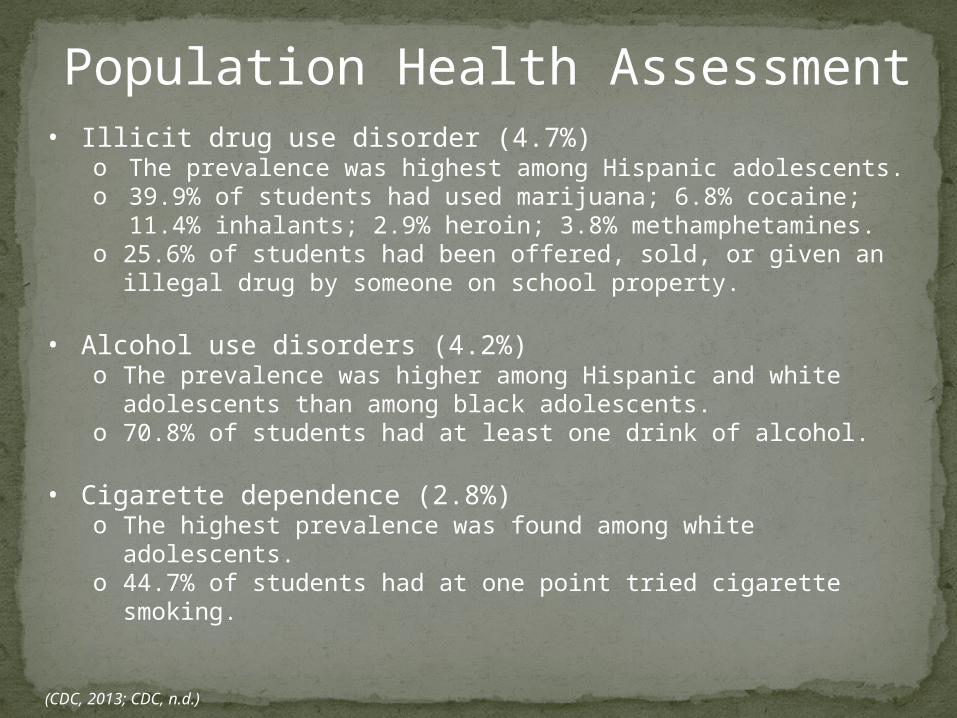
• Illicit drug use disorder (4.7%)o The prevalence was highest among Hispanic adolescents.o 39.9% of students had used marijuana; 6.8% cocaine; 11.4%
inhalants; 2.9% heroin; 3.8% methamphetamines.o 25.6% of students had been offered, sold, or given an illegal drug
by someone on school property.
• Alcohol use disorders (4.2%)o The prevalence was higher among Hispanic and white
adolescents than among black adolescents.o 70.8% of students had at least one drink of alcohol.
• Cigarette dependence (2.8%)o The highest prevalence was found among white adolescents.o 44.7% of students had at one point tried cigarette smoking.
(CDC, 2013; CDC, n.d.)
Population Health Assessment
• 28.5% of high school students reported that they had felt sad or hopeless. o The prevalence was higher among Hispanic students
than white or black students.
Table 1Felt Sad or Hopeless Among Students in Grades 9-12
(in %), 2011
Sex Black AI/AN Asian Hispanic White
Male 18.0 22.8 25.9 24.4 20.7
Female 31.4 50.0 33.5 41.4 34.3
Total 24.7 35.9 29.4 32.6 27.2
Population Health Assessment
Note. From High School Youth Risk Behavior Survey Data, 2011, CDC.
(CDC, 2011)
• Suicide was the second leading cause of death among adolescents aged 12–17 years.
• In 2010, the overall suicide rate for adolescents aged 10-19 years was 4.5 suicides per 100,000 persons.o White children and non-Hispanic children of other races had
higher rates of suicide than black and Hispanic children.o The most common mechanisms of injury were
hanging/suffocation and firearms.
• Among children who died by suicide, o 35.5% had a diagnosed mental disorder at the time of deatho 26.4% were under treatment for a current mental disorder at
the time of death.
(CDC, 2013)
Population Health Assessment
• Suicide attempts for Hispanic girls, grades 9-12, were 70% higher than for white girls, in 2011
• American Indian/Alaska Native (AI/AN) girls have death rates at almost four times the rate for white girls.
Table 2Age-Adjusted Death Rates for Suicide: Ages 15 -
19, 2011
Sex Black AI/AN Asian Hispanic White
Male 7.0 31.1 7.5 9.0 14.0
Female 1.8 10.7 4.2 2.8 3.5
Total 4.5 20.7 5.9 6.0 8.9
Population Health Assessment
Note. From Web-based Injury Statistics Query and Reporting System (WISQARS), 2012, CDC.
(CDC, 2013)
Risk Factors for Mental Illness
Individual and family risk factors:
• History of mental disorders, e.g.,
depression, ADHD, autism spectrum
• Physical and sexual abuse
• Involvement with drugs, alcohol or tobacco
• Parental criminality, substance abuse,
psychiatric disorders
• Unwillingness to seek help because of
stigma
• Repeated experiences of discrimination;
chronic exposure to racism
(Dyson, n.d.)
Social and environmental:
• Low socioeconomic status
• Large families and overcrowding
• Unsafe neighborhoods
• Foster care placement
• High rates of unmet mental
health needs
• Diminished economic
opportunities
• Lack of adequate services within
local communities
Risk Factors for Mental Illness
Cultural and ethnic:
• Difficulty with assimilation
• Lack of cultural role models
• Misdiagnosis based on various
cultural presenting symptoms
• General mistrust of the healthcare
system
• Shame and stigma
Risk Factors for Mental Illness
Risk Factors for Mental Illness
The healthcare system itself creates additional risk
factors for minority populations such as:
• a lack of required training on cultural components and etiquette
• a lack of a diverse workforce
• a lack of knowledge and awareness of cultural differences among
providers
We will be addressing this final issue for the remainder of the presentation.
Population Strengths and ChallengesChallenges:• Less access to available mental health services
o Rates of use of mental health services by Hispanics are low due to lack of community- based services and language barriers
• Are less likely to receive needed mental health careo Inadequate access to care because of living in rural areas which results
in less culturally competent providers in these areas
• Often receive poorer quality careo African American adolescents are more likely to be referred to the
juvenile justice system rather than the mental health treatment system
• Are significantly under-represented in mental health professions
Strengths:• Societal/environmental factors such as Hispanics having strong
support systems which translates to better support for depression and suicide
• Many minorities have an advantage of bilingualism
Ecological ModelCultural competence includes aspects of:
• Commitment to diversity as a valued component of
organizational strategy.
• Dedication to achieving a workforce that is reflective of
the communities and regions that are served, and is
demonstrated through the behaviors of the entire
organization.
• Working to eliminate mental health care disparities with
healthcare reform.
• Having the ability to speak more than one language gives
minorities an advantage to increased communication with
healthcare providers.
Selection of Intervention and Purpose Intervention:
Enhance cultural awareness and encourage culturally
competent care.
Why is addressing cultural communication important?
• The inability of healthcare providers to connect with young
patients is a form of health care disparity.
• Minorities generally receive lower levels of “interpersonal
care” than whites.
• Elimination of health disparities is a Healthy People 2020 goal.
• Individualized mental health care is considered a right.
(Stewart, Simmons, & Habibpour, 2012)
Intervention Specifics
• Target: Health care providers working with desired
populations.
• Location: Large medical centers and other institutions
catering to minority clienteles.
• Intervention will primarily be conducted via training and
• In one year, at least 85% of providers at local institutions
will have taken at least one class in culturally competent
care.
• At the end of the one-year period, 85% of providers who
have taken classes will take a brief examination that covers
selected aspects of culturally-competent care.
• At least 85% of participating institutions will designate an
official responsible for improving cultural competency at
their facility.
Outcome Objectives:
• Outcome 1: Patients will be satisfied with
communication in their cultural style as evidenced by
85% satisfaction on a survey that assesses whether or
not they are satisfied with their provider’s
communication style.
• Outcome 2: Culturally diverse patients will experience
greater participation in the health care system as
evidenced by a statistically significant increase in
resource utilization.
Plan For Process Evaluation
Factors and data analyzed throughout the evaluation
process:
Evaluating intervention materials:
• The content and accuracy of the cultural competency education and
training
o Providers and administrators will asses if topics are applicable
• Provider and Patient surveys
o For Provider: the Cultural Self-Efficacy Scale (NYSPI, 2010)
o For Patient: Client Cultural Competence Inventory
• Provider Examination at the end of program
Who is being tracked through the intervention activities:
• Patients (their usage and demographic data)
• Providers (who has attended training)
• Institutions and administrators (who is participating and
establishing protocols)
Who is conducting the intervention analysis:
• researchers, student researchers
• Statisticians
Identify possible program areas for Improvement:
• Continuous analysis of data, questioning, and ideas that inform
program process (quality control measures)
Plan For Process Evaluation
Plan For Outcome Evaluation
Measure Short Term Outcome Objectives
For short term objectives such as patient satisfaction at the end of the study:
• Measure the change between the initial patient satisfaction survey assessed before the provider received cultural competence training and their experience with their healthcare provider at the end of the study.
Data collection and evaluation will be done at the end program for outcome 1 and one year later for outcome 2.
Measure Long Term Outcome Objectives
Long-term objectives involves behavioral changes which are more challenging to quantify.
• This requires comparing and evaluating minority youth patients mental healthcare usage data during the year after the study was completed versus the initial baseline that was collected at the beginning of the program.
• Unfortunately changing behavior and attitudes can take an extremely long time and creating a direct link between long-term patient outcomes and changes in behavior and given interventions can be difficult to prove.
Plan For Outcome Evaluation
Alegria, M., Vallas, M., & Pumariega, A. (2010). Racial and ethnic disparities in pediatric mental health. Child and Adolescent Psychiatric Clinics of North America 19(4), 759-774. doi:10.1016/j.chc.2010.07.001
American Psychological Association. (n.d.) Children’s Mental Health. Retrieved from https://www.apa.org/pi/families/children-mental-health.aspx
Centers for Disease Control and Prevention (CDC). (2011). High School Youth Risk Behavior Survey Data. Retrieved from http://nccd.cdc.gov/youthonline/App/Default.aspx
CDC (2011). Mental Illness Surveillance Among Adults in the United States. Retrieved from http://www.cdc.gov/mmwr/preview/mmwrhtml/su6003a1.htm?s_cid=su6003a1_w
CDC. (2012). Web-based Injury Statistics Query and Reporting System (WISQARS). Retrieved from http://www.cdc.gov/injury/wisqars/index.html
CDC. (2013). Mental Health Surveillance Among Children--United States, 2005-2011. Retrieved from http://www.cdc.gov/mmwr/pdf/other/su6202.pdf
CDC. (n.d.). Youth Risk Behavior Surveillance System: 2011 National Overview. Retrieved from http://www.cdc.gov/healthyyouth/yrbs/pdf/us_overview_yrbs.pdf
Dyson, A. (n.d.). [Picture of a child surrounded by three hands]. Retrieved from http://www.theage.com.au/national/reforms-target-youth-mental-health-problems-20090312-8whl.html
Heron, M. (2013). Deaths: Leading causes for 2010. National Vital Statistics Reports, 62(6), 17-91. Retrieved from http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_06.pdf
Institute For Education Sciences (IES). (2007). Status and trends in the education of racial and ethnic minorities. Retrieved from http://nces.ed.gov/pubs2010/2010015/figures/figure_18_2.asp.
References
Kumpfer, K. L., Alvarado, R., Smith, P., & Bellamy, N. (2002). Cultural sensitivity and adaptation in family-based prevention interventions. Prevention Medicine 3(3), 241-246. Retrieved from http://rulearning.rush.edu/bbcswebdav/pid-251504-dt-content-rid-2284162_1/courses/14SPCON-NSG-524-W1/13SUCON-NSG-524-1_ImportedContent_20130429044423/Kumpfer%2C%202002.pdf
New York State Psychiatric Institute (NYSPI). (2010). Cultural Competence Assessment Tools. Retrieved from http://www.nyspi.org/culturalcompetence/what/pdf/NYSPI-CECC_CulturalCompetenceAssessment.pdf
Pumareiga, A. J., Rogers, K., & Rothe, E. (2005). Culturally competent systems of care for children’s mental health: Advances and challenges. Community Mental Health Journal 41(5), 539-555. doi:10.1007/s10597-005-6360-4
Ngo, V., Asarnow, J., Lange, J., Jaycox, L., Rea, M., Landon, C., . . . Miranda, J. (2009). Outcomes for youths from racial-ethnic minority groups in a quality improvement intervention for depression treatment. Psychiatric Services, 60(10), 1357-1364. doi:10.1176/appi.ps.60.10.1357
Thomas, J., Temple, J., Perez, N., & Rupp, R. (2012). Ethnic and gender disparities in needed adolescent mental health care. Journal of Health Care for the Poor and Underserved, 22(1), 101-110. doi:10.1353/hpu.2011.0029
United Nations Educational, Scientific, and Cultural Organization. (n.d.). Youth-Definition. Retrieved from http://www.unesco.org/new/en/social-and-human-sciences/themes/youth/youth-definition/
U.S. Census Bureau. (2010). Racial and Ethnic Minority Populations. Retrieved from http://www.cdc.gov/minorityhealth/populations/REMP/definitions.html
US Department of Health and Human Services, Office of Minority Health. (2012). Mental Health and Hispanics. Retrieved from http://minorityhealth.hhs.gov/templates/content.aspx?lvl=3&lvlID=9&ID=6477
US Department of Health and Human Services, Substance Abuse and Mental Health Services Administration. (2012). Results from the 2012 National Survey on Drug Use and Health: Mental Health Findings. Retrieved from http://www.samhsa.gov/data/NSDUH/2k12MH_FindingsandDetTables/2K12MHF/NSDUHmhfr2012.htm#ch2
US Department of Health and Human Services, Substance Abuse and Mental Health Services Administration. (n.d.) Key Features of Risk and Protective Factors.Retrieved from http://captus.samhsa.gov/prevention-practice/prevention-and-behavioral-health/key-features-risk-protective-factors/1