Tiirkisli Ncltrosiirgerlj 8: 110 - 113, 1998 5tereotactically-Guided Craniotomy Hemangioma: Teclinical for a Note Smin~: Tecli11 icnl Nole Cavernous Stereotaktik Hemanjioma Kraniotomi Olgusunda Tekniginin Bir Kavernöz Kullanilmasi: Teknik Not ALI SAVAS, NiHAT EGEMEN, ÇAGlAR BERK Ankara University School of Medicine Department of Neurosurgery, Ankara, Turkey Abstract: Stereotaxy-guided surgery offers significant advantages in the treatment of lesions that cannot be localised reliably because of their sm all size andi or la ek of evident landmarks. A stereotactically-guided craniotomy and microsurgical resection technique was described for excision of a cavernous hemangioma. The technique provided ad vantages in better surgical orientation, precise localization and less invasiveness to the normal brain tissue when compared to the conventional free-hand neurosurgical techniques. Key Word s: Cavernous angioma, minimally invasive, stereotactic craniotomy. INTRODUCTION Almost all neurosurgeons realise the accuracy and advantages of stereotaxy for performing biopsies from brain tumorso On the other hand, stereotactical techniques have alsa been used in assistance in performing craniotomies and microsurgical resection of brain tumors (3, 4, 7). Basically, two kinds of stereotactic systems have been used in order to facilitate microsurgical resection of brain tumors: (1) frameless stereotactic systems; (2) frame based 110 Özet: Stereotaktik teknIklerle desteklenmis mikrosirürji, küçük çapli ve bulunmalarinda yol gösterici izlerin yetersizligi nedeniyle cerrahi lokalizasyon problemi olan lezyonlarda önemli avantajlar saglamaktadir. Bu makalede, bir kavernöz henianjiomali olguda kullanilan stereotaksi rehberliginde kraniotomi ve mikrosirürjikal rezeksiyon teknigi tanimlanmaktadir. Bu teknik, stereotaktik yöntemlerin kullanilmadigi konvansiyonel girisimlerle kiyaslandiginda, daha iyi cerrahi oryantasyon, kesin lokalizasyon ve normal beyin dokusuna daha az zarar verilmesini saglamak gibi avantajlar sunmaktadir. Anahtar Sözcükler: Kavernöz anjioma, minimal invaziv, stereotaktik kraniotomi. stereotactic system.s. Because of its accuracy and easy- to-use frame based stereotactic systems are useful for obtaining accurate approach to most of the lesions in the brain. A cavernous angioma is one of four the commonly oceurring types of cerebral vaseular malformations 0, 2, 5). They of ten oecur in eortieal and subeortieal regions. Frequently, theyare located near the Rolandic area, basal ganglia, pons and cerebellar hemispheres. Because they may often be
OlgusundaTekniginin Bir KavernözKullanilmasi: Teknik Not
ALI SAVAS, NiHAT EGEMEN, ÇAGlAR BERK
Ankara University School of Medicine Department of Neurosurgery, Ankara, Turkey
Abstract: Stereotaxy-guided surgery offers significantadvantages in the treatment of lesions that cannot belocalised reliably because of their sm all size andi or la ekof evident landmarks. A stereotactically-guidedcraniotomy and microsurgical resection technique wasdescribed for excision of a cavernous hemangioma. Thetechnique provided ad vantages in better surgicalorientation, precise localization and less invasiveness tothe normal brain tissue when compared to theconventional free-hand neurosurgical techniques.
Key Word s: Cavernous angioma, minimally invasive,stereotactic craniotomy.
INTRODUCTION
Almost all neurosurgeons realise the accuracyand advantages of stereotaxy for performing biopsiesfrom brain tumorso On the other hand, stereotacticaltechniques have alsa been used in assistance inperforming craniotomies and microsurgical resectionof brain tumors (3, 4, 7). Basically, two kinds ofstereotactic systems have been used in order tofacilitate microsurgical resection of brain tumors: (1)frameless stereotactic systems; (2) frame based
110
Özet: Stereotaktik teknIklerle desteklenmis mikrosirürji,küçük çapli ve bulunmalarinda yol gösterici izlerinyetersizligi nedeniyle cerrahi lokalizasyon problemi olanlezyonlarda önemli avantajlar saglamaktadir. Bumakalede, bir kavernöz henianjiomali olguda kullanilanstereotaksi rehberliginde kraniotomi ve mikrosirürjikalrezeksiyon teknigi tanimlanmaktadir. Bu teknik,stereotaktik yöntemlerin kullanilmadigi konvansiyonelgirisimlerle kiyaslandiginda, daha iyi cerrahi oryantasyon,kesin lokalizasyon ve normal beyin dokusuna daha azzarar verilmesini saglamak gibi avantajlar sunmaktadir.
stereotactic system.s. Because of its accuracy and easyto-use frame based stereotactic systems are usefulfor obtaining accurate approach to most of the lesionsin the brain.
A cavernous angioma is one of four thecommonly oceurring types of cerebral vaseularmalformations 0, 2, 5). They of ten oecur in eortiealand subeortieal regions. Frequently, theyare locatednear the Rolandic area, basal ganglia, pons andcerebellar hemispheres. Because they may often be
Turkis/i Neurosiirgery 8: 110 - 113, 1998
just an incidental finding, surgical excision is notrecommended in all patients but especially forpatients with medically intractable epilepsy and inthose with previous hemorrhage. Magneticresonance imaging (MRI) technology offers a morereliable diagnosis of this vascular malformationentity, and the incidance of diagnosing of cavernousangiomas has greatly iilereased since the introductionof MR!. Since these lesions are usually smaIl andmay be located in eloquent regions in the brain,essentials of surgery for cavernomas are precision inlocalisation and minimal operatiye trauma to thesurrounding brain tissue. Conventional surgicaltechniques may be insufficient for accuratelocalisation of these lesions, and cavernousmalformations may be more safely excised usingstereotactic localisation techniques.
We report a patient with cerebral cavernoushemangioma removed by stereotacticaiiy-guidedcraniotomy and microsurgical resection; and thetechnique is described in detai1.
MATERIAL AND METHODS
Patient
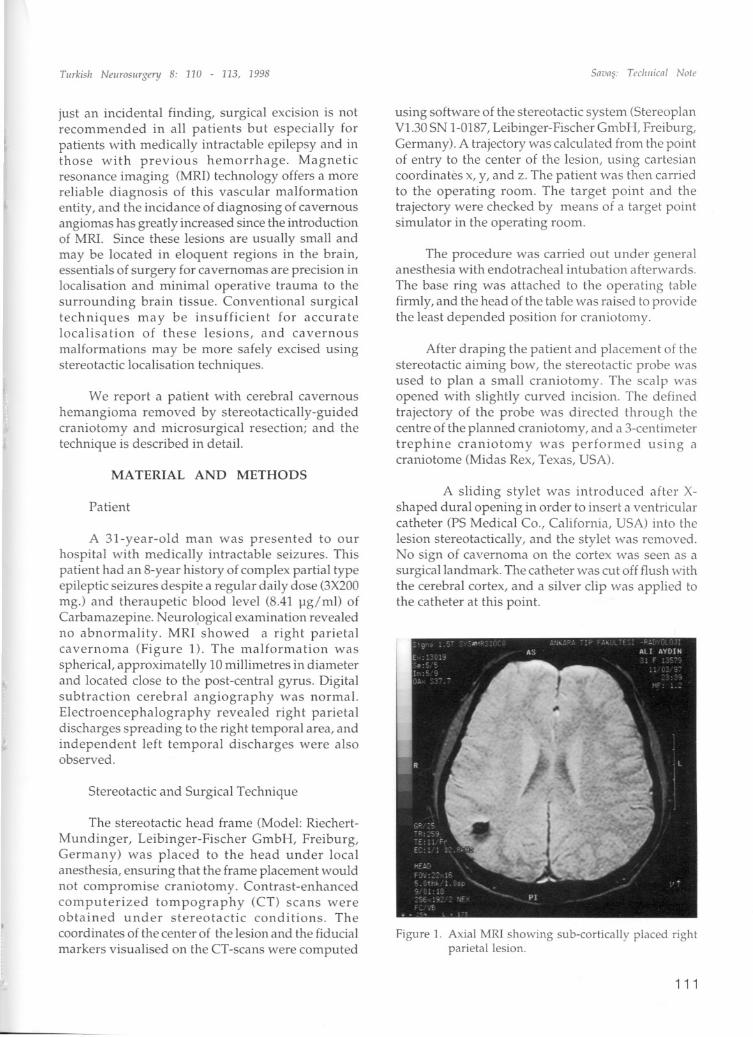
A 31-year-old man was presented to ourhospital with medicaiiY intractable seizures. Thispatient had an 8-year history of complex partial typeepileptic seizures despite a regular daily dose (3X200mg.) and theraupetic blood level (8.41 )lg/ml) ofCarbamazepine. Neurological examination revealedno abnormality. MRI showed a right parietalcavernoma (Pigure 1). The malformation wasspherical, approximatelly 10 millimetres in diameterand located elose to the post-central gyrus. Digitalsubtraction cerebral angiography was normaL.Electroencephalography revealed right parietaldischarges spreading to the right temporal area, andindependent left temporal discharges were alsoobserved.
Stereotactic and Surgical Technique
The stereotactic head frame (Model; RiechertMundinger, Leibinger-Pischer GmbH, Preiburg,Germany) was placed to the head under localanesthesia, ensuring that the frame placement wouldnot compromise craniotomy. Contrast-enhancedcomputerized tompography (CT) seans wereobtained under stereotactic conditions. Thecoordinates of the center of the lesion and the fiducial
markers visualised on the CT-seans were computed
SaL'as: Teel/iiiml Note
using software of the stereotactic system (StereoplanVL.30SN 1-0187,Leibinger- Pischer GmbH, Preiburg,Germany). A trajectory was calculated from the pointof entry to the center of the lesion, using cartesiancoordinates x, y, and z. The patient was then carriedto the operating room. The target point and thetrajectory were checked by means of a target pointsimulator in the operating room.
The procedure was carried out under generalanesthesia with endotracheal intubation afterwards.The base ring was attached to the operating tablefirmly, and the head of the tabie was raised to providethe least depended position for craniotom.y.
After draping the patient and placement of thestereotactic aiming bow, the stereotactic probe wasused to plan a smaIl craniotomy. The scalp wasopened with slightly curved incision. The definedtrajectory of the probe was directed through thecentre of the planned craniotomy, and a 3-centimetertrephine craniotomy was performed using acraniotome (Midas Rex, Texas, USA).
A sliding stylet was introduced after Xshaped dural opening in order to insert a ventricularcatheter (PS Medical Co., California, USA) into thelesion stereotactically, and the stylet was removed.No sign of cavernoma on the cortex was seen as asurgical landmark. The catheter was cut off flush withthe cerebral cortex, and a silver elip was applied tothe catheter at this point.
A convenient sulcus was split microsurgically,and the direction of the subcortical incision was
made following the trajectory of the catheter. Thegliotic surrounding tissue stained by hemosiderinand the hemangioma came into view, and themaltormation was removed using standardmicrosurgical technique and instrumentation,including Leyla retractors (Aesculap, Tuttlingen,Germany) mounted on the operating table. Theoperation was concluded in the standart fashion, thedura was closed in waterthight fashion, no epiduraldrain was placed. and the stereotactic apparatus wasremoved.
Post-Operative Course
The postoperative course of the patient wasuneventful. He was discharged from the hospitalwithout any abnormal neurological findings 3 daysaf ter the surgery. Pathological examinationconfirmed the diagnosis of cavernous hemangioma.Post-operative MRI showed total removal of themaHormation with minimal operatiye changes in thesurrounding tissues (Figure 2). Post-operativeelectroencephalographies revealed well-Iocalisedright temporal sharp waves, and a remarkablereduction. in frequency of epileptic seizures wasobserved in 5 months' follow-up.
Figure 2. Post-operative MRI demonstrating the totalremoval of the hemangioma and minimal postoperative changes in the surraunding braintissue.
112
Savas: Teel/IiIcal Nafe
DISCUSSION
The use of stereotactic methods to localise a
visible region of cerebral morphology for surgicalpurposes is called "morphologic stereotaxy". In thissurgical discipline, pathologic structures are readilyvisualised with appropriate imaging and their x, y, z(Cartesian) coordinates are usual1y calculatedaccording to a stereotactic head frame using thecomputer technology. Surgery is planned, and thenperformed according to these calculations. Therecently developed method s for localising any pointon the digital imaging modalities, such as computedtomography (CT), magnetic resonance imaging(MRI) and digital angiography (DSA), with respectto the stereotactic head frame have provided that anyintracranial point could be accessed surgically withgreat accuracy.
The stereotactic systems may be used not onlyfor stereotactic biopsies or similar procedures madethrough a burr-hole but alsa for microsurgicalresectian of the cerebral lesions via smal1craniotomies (6). Such assistance is beneficial,particularly for subcortical1y or deeply locatedlesions or those near eloquent or functionallyimportant nervous structures. Stereotactic systemsused for excision of the cerebrallesions may basicallybe divided into two: (1) Frameless systems, and (2)Frame based systems.
The frameless stereotactic systems have beenobviating the need for conventional head frames buttheyare still evolving. In frameless stereotacticsystems, the digital imaging modalities, such as CT,MRI, and DSA, and pasitran emmision tomography(PET) seans are obtained as three dimensionalvolumetric data bases. Usually, fiducial markers areattached to the patient's skin, and each digital imagepoints are registered according to the markers. Thisregistration can employ information about the spatiallocalisation of any target or selected volume, whichis obtained preoperatively, or postoperatively.Preoperative planning the frameless systems takesplace in the operating theatre in interactive fashionwithin the intended operating field; they may be usedto mark the normal anatamical structures providingthe surgeon with a much more realistic setting tounderstand the surgical anatomy; and their rangeof usage will be more unlimited since they don'tcause any mechanical restriction when compared toframe based systems. There is no doubt that thesesystems will emerge as extremely useful in their ownright and serve a bridge into the next era of surgical
Tiirkis/r Neiirosiirgery 8: 110 - 113, 1998
technology (3). The most importantdisadvantages of these systems may be summarisedas following: Theyare very expensive and notavailable in most of neurosurgieal elinies; their usagelimited only in neuronavigation duringmierosurgieal resections.
Frame based systems have still remained thegold standard in terms of preeision and aeeuraey ofloealisation. Stereotaetie frames are available in mostof the referenee neurosurgieal elinies and used invarious purposes. Additionally, theyare eheaper incomparison to the frameless systems. The describedteehnique can be performed with almost all kinds ofeommercial stereotaetie fram.e systems, and theproeedure requires no speeially designed equipment.With this teehnique, standard neurosurgiealretraetors (such as Leyla retraetors, ete.), in any sizeaccording to the neurosurgeon's preferenee and thesize and loealisation of the lesion, can be usedfollowing the stereotactieally plaeed teflon eatheteras a guide. The are-mounted stereotaetie eylindriealretraetors and dilators, whieh were described andfrequently used by Kelly, may be mueh moretraumatie to the brain tissue when compared to theteehnique described above.
On the other hand, the greatest limitation of theframe based stereotaetie methods in eraniotomy andreseetion of brain lesions is that the frame attaehedto the patient's skull is restrietive and bul kyproviding only a restricted and temporary referenee.Sinee mostly the frames are usually plaeed more orless in parallel to the orbitomeatal plane and elose toskull base, usage of the teehnique may be morediffieult in lesions with temporal lobe, posteriorfossa, oeeipitopolar or frontopolar loealisation.However, no diffieulty may be expeeted in lesionsloeated in parietal lobe, frontoparietal andparietooeeipital regions, and in lesions with deepbrain loealisation. As additional disadvantages, theaiming are is usually eumbersome in front of theneurosurgeon's view and onlyone target point andtrajectory are seleeted at a time.
Cavernous hemangioma (cavernoma) is one ofthe four major clinieopathologieal eategories ofvaseular malformations of the nervous system.Sinee most of the eavernomas may remainelinieally silent, surgieal removal of thesemalformations is eontroversial in some cases. On
the other hand, these tumors may be small sized,loeated subeortieally or in eloquent areas, and theremay be no evident landmarks on the brain surfaee
Snions: Tec/rilicnl Nafe
to aid surgieal orientation. Precise loealisation andminimal surgieal trauma to the surrounding neuraltissue, whieh may be provided with the help ofstereotactieal guidanee optimal1y, are essentials ofmierosurgieal reseetion of eavernomas 0, 2, 5). Wethink that with modern neurosurgieal teehniques,ineluding stereotaetie loealisation, there will be fewerdiffieulties in surgieal removal of these lesions, andthus postoperative results will beeome mueh moresa tisfaetory.
The described teehnique provides preciseloealisation during surgery, smaller and moreaeeurate eraniotomies and sealp ineisions, and shorterhospital stays. Stereotaxy-guided mierosurgery withframe based systems al10ws easy and safe reseetionof smal1, subeortieally plaeed eerebral lesions, e.g.eavernous hemangiomas.
Correspondence: Ali SavasPK 243, Kavakhdere06693 Ankara, TurkeyFax: 312-419 3684
1. Cas ey A TH, Thomas DGT, Harkness WF:Stereotactical1y-guided craniotomy for cavernousangiomas presenting with epilepsy. Acta Neurochir137: 34-37, 1995
2. Esposito V, Oppido PA, Delfini R, Cantore G: A simplemethod for stereotactic microsurgical excision of smail,deep-seated cavernous angiomas. Neurosurgery 34:515-519,1994
4. Kelly PJ:CTjMRI-based computer-assisted volumetricstereotactic resection of intracranial lesions, inSchmideck HH, Sweet WH (eds), Oper,ii i, I'
Neurosurgical Techniques, volume 1, third edii",:Philadelphia:WB Saunders, 1995: 619-635
5. Kunz U, Goldmann A, Bader C, Oldenkott P:Stereotactic and ultrasound guided minimal invasivesurgery of subcortical cavernomas. Min Inv Neurosurg37: 17-20, 1994
















![Case Report Cavernous Hemangioma of the Skull and ...downloads.hindawi.com/journals/crinm/2015/716837.pdf · etiology for brain tumors like meningiomas and cavernous hemangiomas,gliomas,andsarcomas[].Radiation-induced](https://static.documents.pub/doc/80x56/608fef3819cb3a1b7677deab/case-report-cavernous-hemangioma-of-the-skull-and-etiology-for-brain-tumors.jpg)


