Optimizing Patients for Surgery Optimizing Patients for Surgery Rl f th PAT i i Rl f th PAT i i Role of the PAT nurse in assessing Role of the PAT nurse in assessing patient risk patient risk Tanya Cowder, RN, CNS Sue Burns, RN Avis Hayden, PhD
Transcript
Optimizing Patients for SurgeryOptimizing Patients for Surgery
R l f th PAT i iR l f th PAT i iRole of the PAT nurse in assessing Role of the PAT nurse in assessing patient riskpatient risk
Tanya Cowder, RN, CNSSue Burns, RN
Avis Hayden, PhDy ,
PAT: Pre‐Anesthesia
Teaching
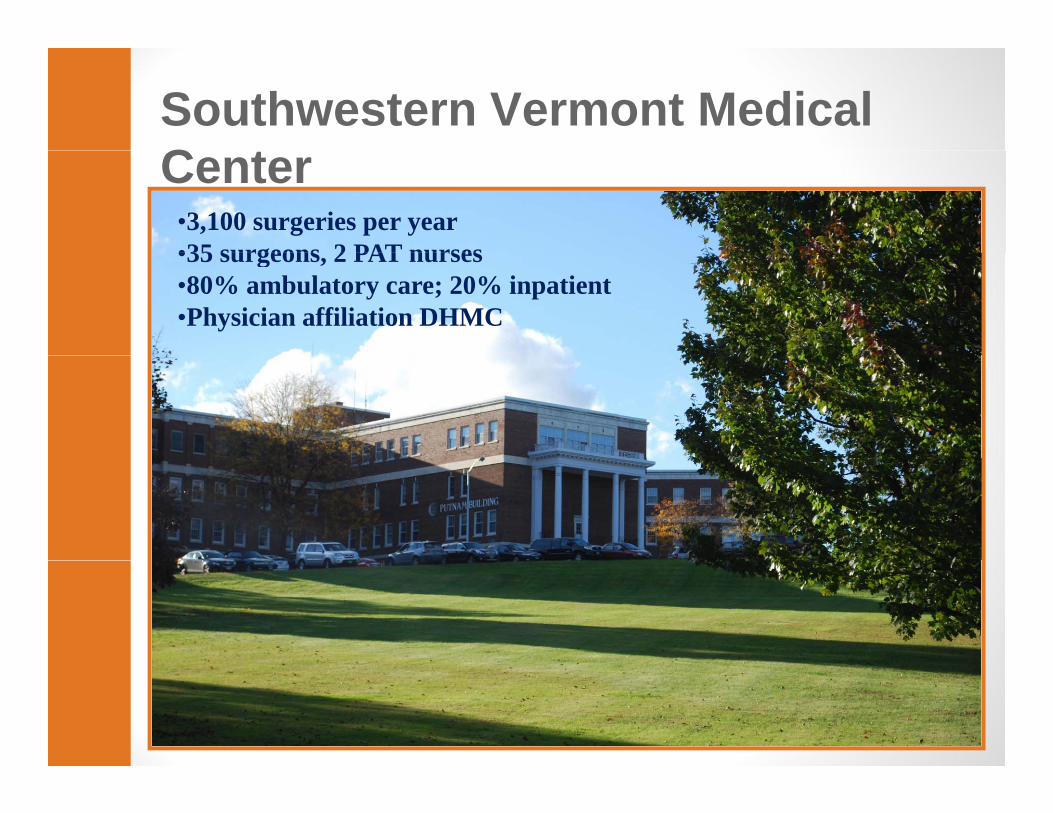
Southwestern Vermont Medical C tCenter
•3,100 surgeries per year•35 surgeons 2 PAT nurses•35 surgeons, 2 PAT nurses•80% ambulatory care; 20% inpatient•Physician affiliation DHMC
Objectives for Today:Objectives for Today:
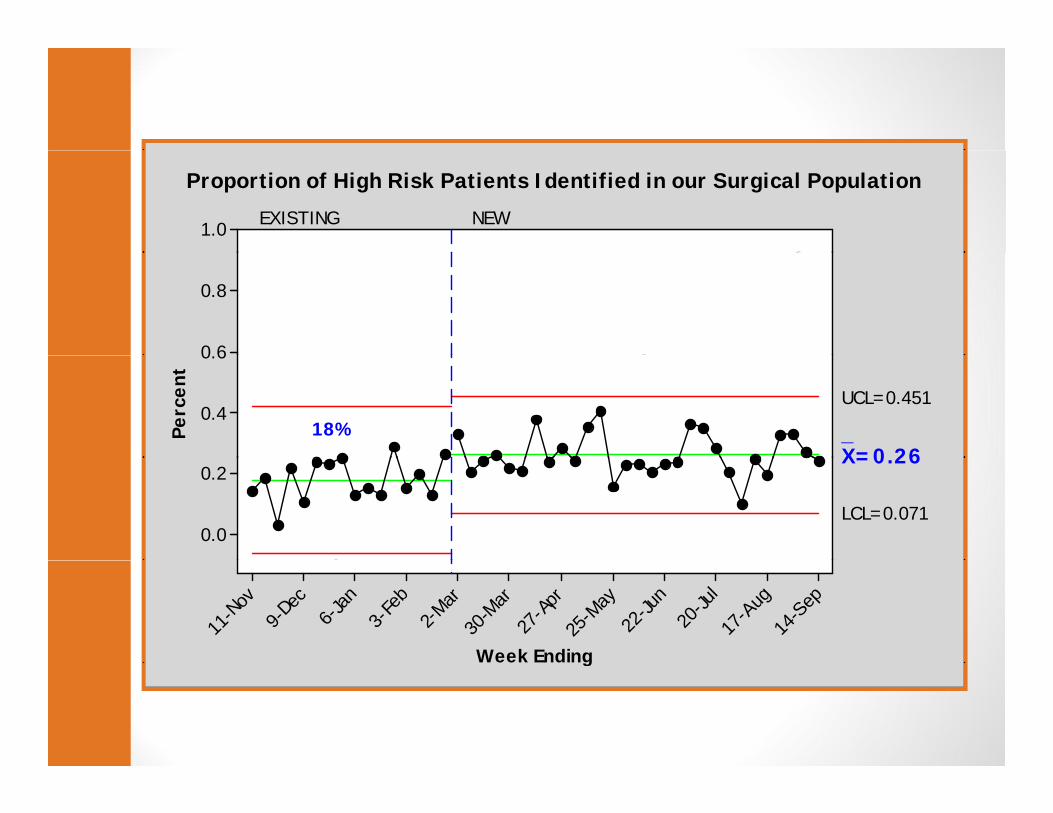
•Factors leading to change•Factors leading to change•Key elements of new processy p•Expanded role of PAT nurse•Outcomes, data•Next steps•Next steps
Frank’s StoryFrank s Story
InterviewsInterviews•Chief Medical Officer•Patient Safety Specialist•Anesthesiologists•Anesthesiologists•Internists & PCP’s•Surgeons•Nurses•Nurses•Support Staffpp
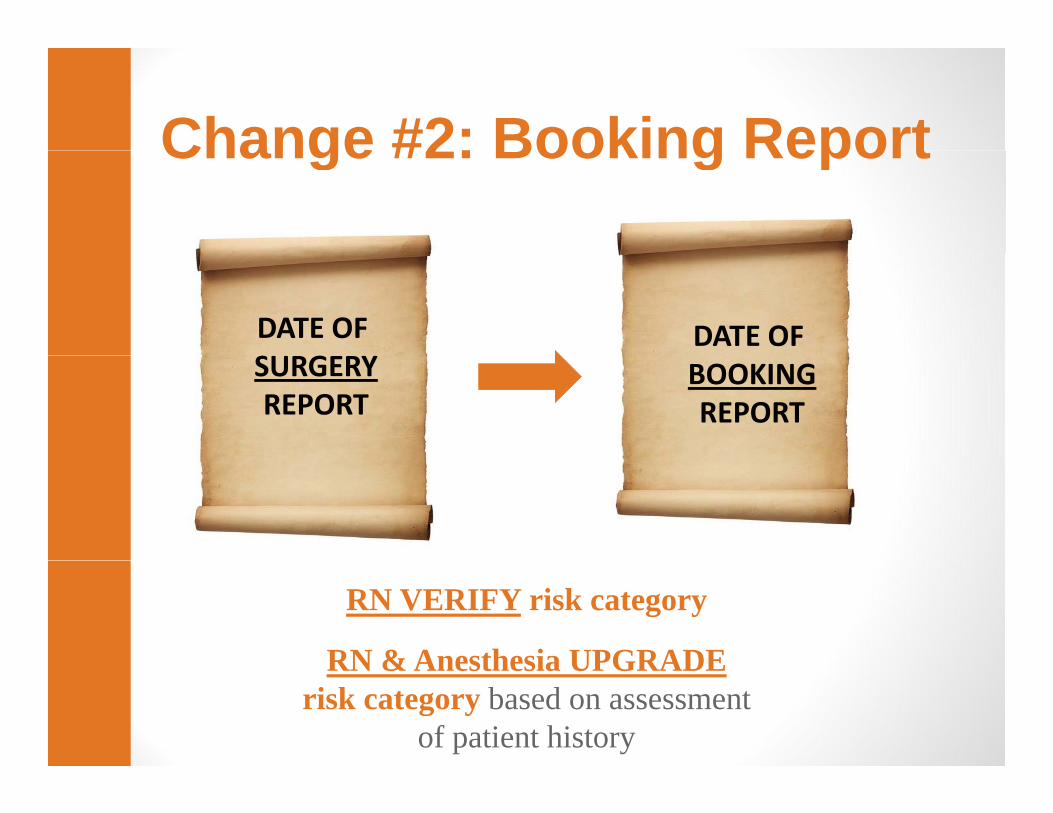
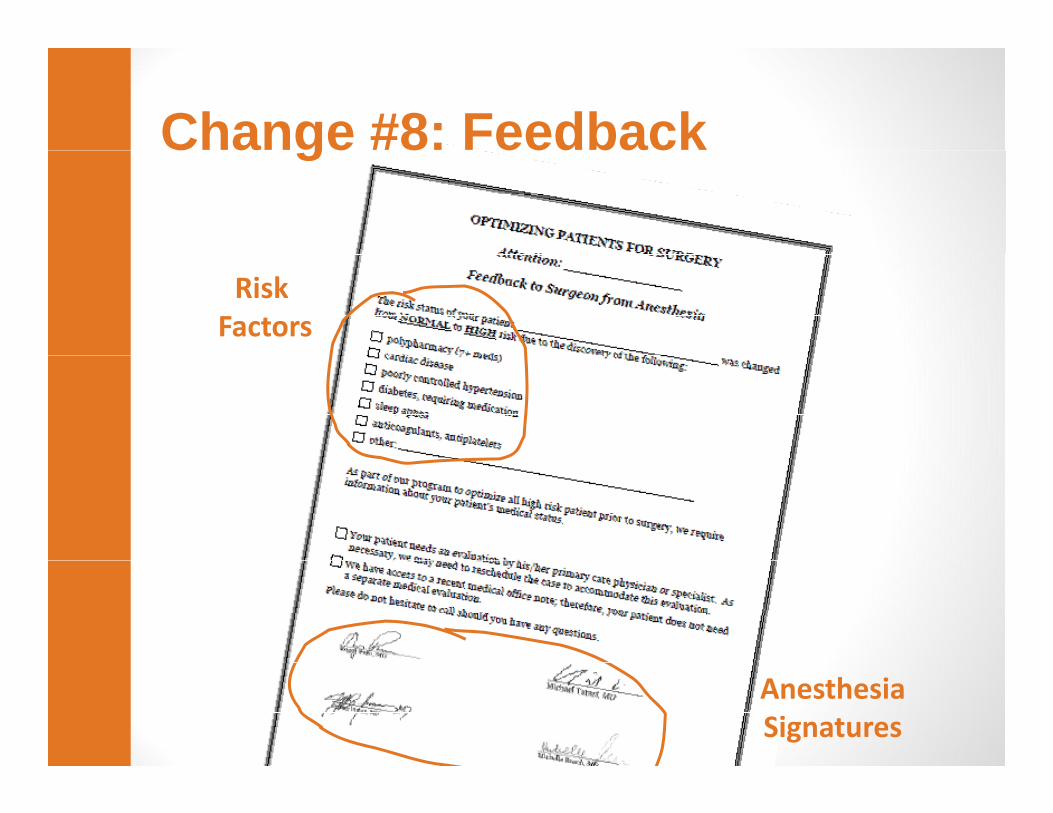
RN & Anesthesia UPGRADERN & Anesthesia UPGRADErisk category based on assessment
of patient history
Change #3: Medical EvalChange #3: Medical Eval
•HIGH RISK
•NORMAL RISK•NORMAL RISK
Change #4: Clinical InformationChange #4: Clinical Information
Orders, Consent, H&P
Assemble chart
Change #5: Medical EvalChange #5: Medical Eval
M di l bl• Medical problems• Medication list• Would delaying the procedure allow to better control any of theallow to better control any of the following:
H A1C 7• HgA1C over 7• Poorly controlled hypertension or heart disease• Active infections• Sleep apnea• Anticoagulant therapy
• Process• Post op co-management• Short notice booking
SummarySummary
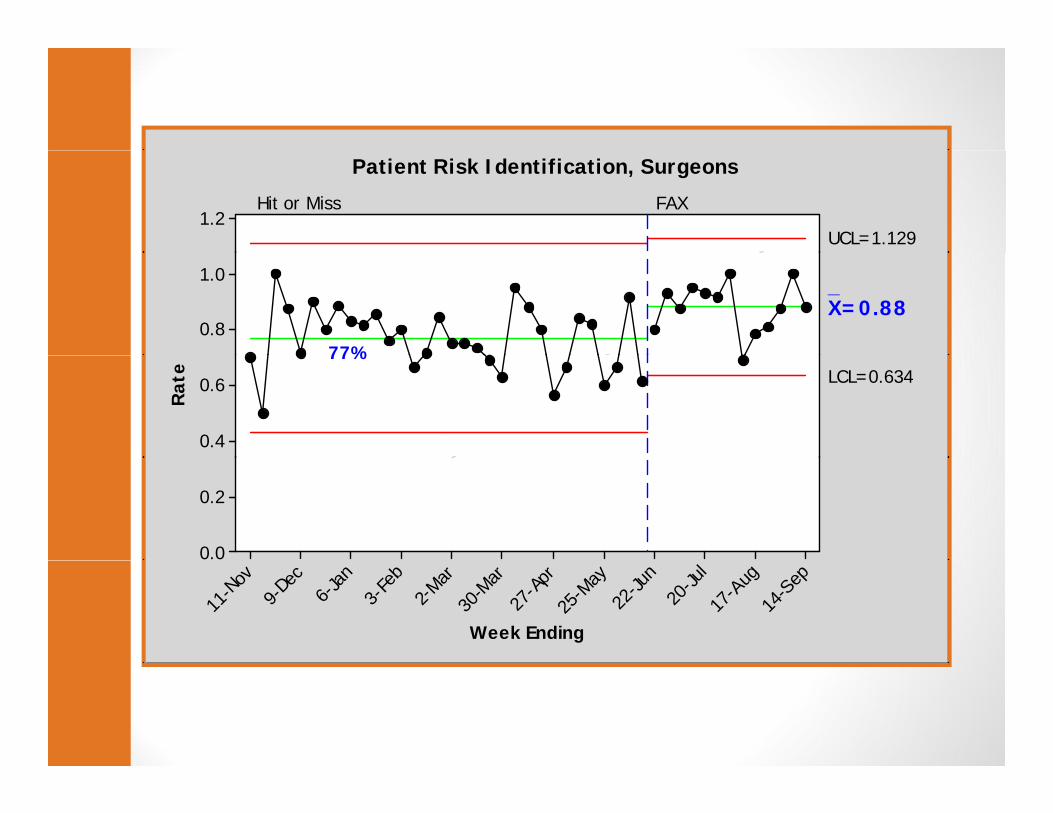
• Identified a problem•Identified a problem•Interviewed key stakeholders•Reviewed literature•Developed a new process•Developed a new process•Used data to keep the process on track
•After 1 yr – reliable processAfter 1 yr reliable process